

Abstract
Summary: Aneurysmal bone cysts of the skull are rare, and orbital involvement of these cysts is even less frequent. We present CT, MR imaging, and histopathologic findings of an aneurysmal bone cyst of the orbit in a 13-year-old female adolescent. The tumor mainly involved the frontal bone. MR imaging findings of the aneurysmal bone cyst of the skull were highly suggestive of the diagnosis.
Aneurysmal bone cysts are uncommon benign, expansile, and lytic lesions that develop in childhood or early adulthood. An aneurysmal bone cyst usually occurs as a primary lesion. In one third of the cases reported in the literature, a preexisting condition or history of trauma is present. Pain and swelling are the main symptoms and usually last for as long as 6 months. Long bones are involved in more than half of the cases. Involvement of the spine and flat bones also has been reported (1, 2). Skull involvement is rare, occurring in less than 1% of all aneurysmal bone cysts (3). The orbit is much less frequently involved; a review of the literature revealed only 20 cases (3–7). Among them, we could find only two presentations with MR imaging findings, and these were not published in the radiologic literature (3, 4). We present CT and MR imaging findings in a case of aneurysmal bone cyst of the orbit that was confirmed by histopathologic analysis.
Case Report
A 13-year-old female adolescent had rapidly growing, painful swelling in her right frontal region and diplopia over a 2-month period. She had no history of trauma or surgery. Physical examination revealed a firm, fixed mass situated just superior and posterior to the right orbital rim. Exophthalmos was present on the right. The lateral gaze of the right eye was restricted, but visual acuity was normal. On coronal and axial CT scans, a multiloculated mass with fluid-fluid levels was found. Bone destruction was present in the superior, lateral, and posterior walls of the right orbit (Fig 1). T1- and T2-weighted imaging revealed variable signal intensities of fluid-fluid levels, consistent with blood degradation products. The walls of the cystic spaces and surrounding rim showed contrast enhancement. The mass was compressing the optic nerve and ocular muscles inferomedially (Fig 2). A cystic mass, approximately 4.5 × 3 × 3 cm in size and containing brown-yellowish fluid, was surgically removed. Histopathologic analysis revealed multiple blood-filled cystic spaces. The borders of these spaces were lined by osteoclast type multinucleated giant cells, bone, and fibrous tissue. Endothelial cells were not present. These findings were consistent with those of an aneurysmal bone cyst (Fig 3).
Fig 1.

Bone destruction in the superior, lateral, and posterior walls of the right orbit.
A, Coronal CT scan obtained with bone window settings shows an orbital mass causing bone destruction and displacing the orbital structures.
B, Axial non–contrast-enhanced CT scan shows multiloculated mass with fluid-fluid levels.
Fig 2.

Mass compressing the optic nerve and ocular muscles inferomedially.
A, Axial T1-weighted MR image (562/14/2 [TR/TE/excitations]), obtained before the administration of contrast material, shows a multiloculated mass in the right frontal region, which contains fluid-fluid levels with variable signal intensity.
B, Axial contrast-enhanced T1-weighted MR image (562/14/2) shows enhancement of the cyst walls.
C, Coronal T2-weighted MR image (4000/120/3) shows displacement of the optic nerve and ocular muscles by the mass.
D, Sagittal T2-weighted MR image (4000/120/3) shows multiple small cysts (diverticula) projecting from larger cysts.
Fig 3.
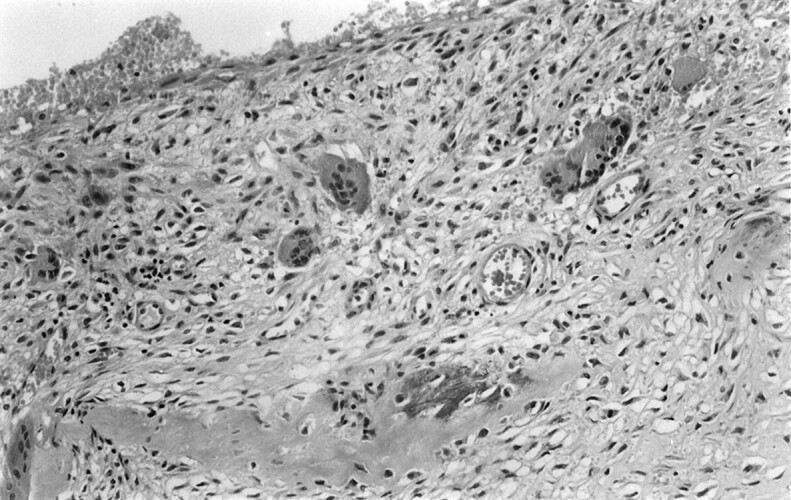
Histologic specimen shows multiple giant cells and bony spicula within the walls of the cystic spaces containing erythrocytes (hematoxylin-eosin stain, magnification ×20).
Discussion
Aneurysmal bone cysts were first described in 1942 as “peculiar blood-containing cysts of large size” (8). They are composed of blood-filled, anostomosing cavernous spaces, separated by cystlike walls. The precise nature and histogenesis of the aneurysmal bone cyst remain unclear (2). However, the aneurysmal bone cyst is considered to be the result of a specific pathophysiologic change, which is probably caused by trauma or an anomalous vascular process. In one third of the cases, a preexisting lesion is present. Giant cell tumor, chondroblastoma, chondromyxoid fibroma, nonossifying fibroma, osteoblastoma, fibrosarcoma, fibrous histiocytoma, osteosarcoma, and fibrous dysplasia have been reported as antecedent lesions (1, 2).
Radiologic findings reflect the pathophysiologic properties of an aneurysmal bone cyst. Initially, well-defined osteolysis and periosteal elevation are present. The lesion grows rapidly and causes progressive destruction. Radiographs typically show an eccentric lesion with an expanded, remodeled blown-out or ballooned bony contour of the bone. The word aneurysmal refers to this appearance. The expanded contour is the result of bone production by the periosteum. Lesions frequently have a delicate trabeculated appearance (1). At histologic examination, these lesions are large, septated sinusoids filled with blood and lined by endothelium and multinucleated giant cells. Small cysts called diverticula project from larger cysts (9, 10). Hemorrhage of variable age within the cysts are present, and the degradation of blood products causes fluid levels. On MR images, all these structures are surrounded by a well-defined low-signal-intensity rim (11). Later, a soap bubble appearance is seen as the lesion stabilizes. Finally, calcification and ossification occur, and the lesion turns into a dense mass.
CT is especially useful in the evaluation of the lesions located in the regions that cannot be adequately assessed by radiography. On CT scans, a well-defined expansile mass causing cortical interruption is seen. Fluid levels are observed in 35% of the cases, and dependent layers show increased attenuation (1).
MR imaging features of an aneurysmal bone cyst have been described in several studies (9, 10, 12, 13). The hypointense rim surrounding the lesion is an important finding and suggests a benign process. This rim is composed of fibrous tissue (1, 10, 13). A fluid-fluid level is another finding and is more readily seen on MR images than on CT scans (1). Cavities that contain fluid-fluid level are conspicuous on T1-weighted images. Because of the degradation of blood products, the signal intensity of these levels vary (9, 10). Fluid-fluid levels strongly suggest the presence of an aneurysmal bone cyst (9), but this finding has been reported to occur in association with various conditions and is not pathognomonic. Chondroblastoma, osteosarcoma, giant cell tumor, fibrous dysplasia, osteoblastoma, and tumoral calcinosis are examples of pathologic abnormalities with which fluid-fluid levels are found (14, 15). Although it is not specific, its presence indicates an aneurysmal bone cyst if other suggestive features exist (11). Another important MR imaging feature of an aneurysmal bone cyst is the presence of small cysts projected from larger cysts; these are called diverticula (9, 10). These structures contribute to the typical bubbly appearance. MR imaging features of calvarial lesions are not noticeably different from those of lesions occurring elsewhere in the body (3, 11).
Age, clinical course, and imaging findings in our patient suggested the diagnosis of aneurysmal bone cyst. Diverticula were seen on MR images. Although the hypointense rim was not obvious on T1-weighted images, fibrous tissue enhancement was observed. These MR imaging findings were considered typical for an aneurysmal bone cyst.
In conclusion, aneurysmal bone cyst should be in the differential diagnosis of rapidly growing calvarial masses in young patients. Although not pathognomonic, the presence of cysts and diverticula, fibrous tissue enhancement, and fluid-fluid levels with variable signal intensity on MR images strongly suggests the presence of an aneurysmal bone cyst. The multiplanar imaging capability of MR imaging is especially important in the evaluation of skull lesions for which the neighboring structures should be evaluated before surgical intervention.
References
- 1.Kransdorf MJ, Sweet DE. Aneurysmal bone cyst: concept, controversy, clinical presentation, and imaging. AJR Am J Roentgenol 1995;164:573–580 [DOI] [PubMed] [Google Scholar]
- 2.Martinez V, Sissons HA. Aneurysmal bone cyst: a review of 123 cases including primary lesions and those secondary to other bone pathology. Cancer 1988;61:2291–2304 [DOI] [PubMed] [Google Scholar]
- 3.Hunter JV, Yokoyama C, Moseley IF, Wright JE. Aneurysmal bone cyst of the sphenoid with orbital involvement. Br J Ophthalmol 1990;74:505–508 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hino N, Ohtsuka K, Hashimoto M, Sakata M. Radiographic features of an aneurysmal bone cyst of the orbit. Ophthalmologica 1988;212:198–201 [DOI] [PubMed] [Google Scholar]
- 5.Bealer LA, Cibis GW, Barker BF, Egelhoff JC, Freeman AI, Zwick DA. Aneurysmal bone cyst: report of a case mimicking orbital tumour. J Pediatr Ophthalmol Strabismus 1993;30:199–200 [DOI] [PubMed] [Google Scholar]
- 6.Dailey R, Gilliland G, McCoy GB. Orbital aneurysmal bone cyst in a patient with renal cell carcinoma. Am J Ophthalmol 1994;117:643–646 [DOI] [PubMed] [Google Scholar]
- 7.Lucarelli MJ, Bilyk JR, Shore JW, Rubin PA, Yaremchuk MJ. Aneurysmal bone cyst of the orbit associated with fibrous dysplasia. Plast Reconstr Surg 1995;96:440–445 [DOI] [PubMed] [Google Scholar]
- 8.Jaffe HL, Lichtenstein L. Solitary unicameral bone cyst with emphasis on the roentgen picture, the pathologic appearance, and the pathogenesis. Arch Surg 1942;44:1004–1025 [Google Scholar]
- 9.Beltran J, Simon DC, Levy M, Herman L, Weis L, Mueller CF. Aneurysmal bone cysts: MR imaging at 1.5 T. Radiology 1986;156:689–690 [DOI] [PubMed] [Google Scholar]
- 10.Munk PL, Helms CA, Holt G, Johnston J, Steinbach L, Neumann C. MR imaging of aneurysmal bone cysts. AJR Am J Roentgenol 1989;153:99–101 [DOI] [PubMed] [Google Scholar]
- 11.Shah GV, Doctor MR, Shah PS. Aneurysmal bone cyst of the temporal bone: MR findings. AJNR Am J Neuroradiol 1995;16:763–766 [PMC free article] [PubMed] [Google Scholar]
- 12.Hudson TM, Hamlin DJ, Fitzsimmons JR. Magnetic resonance imaging of fluid levels in an aneurysmal bone cyst and in anticoagulated human blood. Skeletal Radiol 1985;13:267–270 [DOI] [PubMed] [Google Scholar]
- 13.Zimmer WD, Berquist TH, McLeod RA, et al. Bone tumors: magnetic resonance imaging versus computed tomography. Radiology 1985;155:709–718 [DOI] [PubMed] [Google Scholar]
- 14.Tsai JC, Dalinka MK, Fallon MD, Zlatkin MB, Kressel HY. Fluid-fluid level: a nonspecific finding in tumours of bone and soft tissue. Radiology 1990;175:779–782 [DOI] [PubMed] [Google Scholar]
- 15.Vilanova JC, Dolz JL, Maestro de Leon JL, Aparicio A, Aldom J, Capdevila A. MR imaging of a malignant schwannoma and an osteoblastoma with fluid-fluid levels: report of two new cases. Eur Radiol 1998;8:1359–1362 [DOI] [PubMed] [Google Scholar]