

We read with interest the case report of Clarot et al (1) regarding a patient with intracranial hypotension (IH) after lumbar puncture who had giant cervical epidural veins as the sole MR finding. Having had experience with a similar case, we felt obliged to report on our observation and contribute to the validation of this finding, with the aim of rendering a difficult diagnosis easier.
A 34-year-old previously healthy woman presented in May 1996 with headache and neck pain. Spinal MR showed dilation of cervical epidural veins, especially visible from the C2 down to the C4 level anteriorly. On subsequent angiography, no vascular malformation was identified; venous drainage and jugular veins were normal, but epidural veins appeared markedly dilated at the upper cervical and spinal-medullary level (Fig 1). Further observation of the spinal MR study made it possible to identify meningeal ectasia at the level of the exiting spinal roots at C7–T1 (Fig 2). At the same level, increased signal was noticed on T2-weighted images in the paraspinal soft tissues, which was interpreted as cerebrospinal fluid. On this basis, spontaneous IH caused by CSF leakage was suspected. Brain MR showed thickened dura, but the patient refused a contrast-enhanced examination. Nevertheless, accurate measurement of brain position in the skull on midsagittal T1-weighted images gave results suggesting a significant rostrocaudal brain displacement (Fig 3). Cerebellar tonsils were 2 mm below the Chamberlain line, and the apex of the fourth ventricle was 3 mm below the Twining line. The symptoms and the MR images resolved after conservative therapy (ie, bed rest and hydration). On clinical follow-up 41 months later, the patient denied any relapse of symptoms.
In addition to confirming dilation of cervical epidural veins as a possible presentation of IH, we would like to draw attention to precise measurement of brain position in the skull on midsagittal MR images as an aid to the diagnosis of IH (2). We recently measured brain position relative to four anatomic landmarks in a series of eight patients affected by the syndrome of spontaneous IH, and in 89 healthy control subjects. We found that the two groups differed for all four measurements: 1) the position of the cerebellar tonsils measured relative to the Chamberlain line (a straight line drawn from the posterior lip of the bony hard palate posteriorly to the posterior lip of the foramen magnum), 2) the position of the apex of the fourth ventricle measured relative to the Twining line (a straight line drawn from the anterior tuberculum sellae posteriorly to the internal occipital protuberance), 3) the position of the third ventricle infundibular recess relative to the straight line drawn tangent to the floor of the anterior cranial fossa, and 4) the position of the third ventricle measured as the value of the superior-posterior angle between the bicommissural line (a straight line drawn from the anterior to the posterior commissure) and the straight line drawn tangent to the floor of the fourth ventricle. The difference was significant (P < .001) for three of the four measurements (1, 2, and 3).
To conclude, dural contrast enhancement (4) and other MR findings can be absent in some cases of IH, and we emphasise the possibility of confirming clinical suspicion by precise evaluation of the above-mentioned features.
fig 1.

A, MR angiogram obtained with an axial fast low-angle shot 2D sequence (40/9.8 [TR/TE]; flip angle, 35°). Cervical epidural veins are markedly dilated and give very high signal. Carotid and vertebral arteries give dark signal because of inferior saturation.
B, Oblique sagittal and coronal reconstructed images obtained with maximum intensity projection.
fig 2.
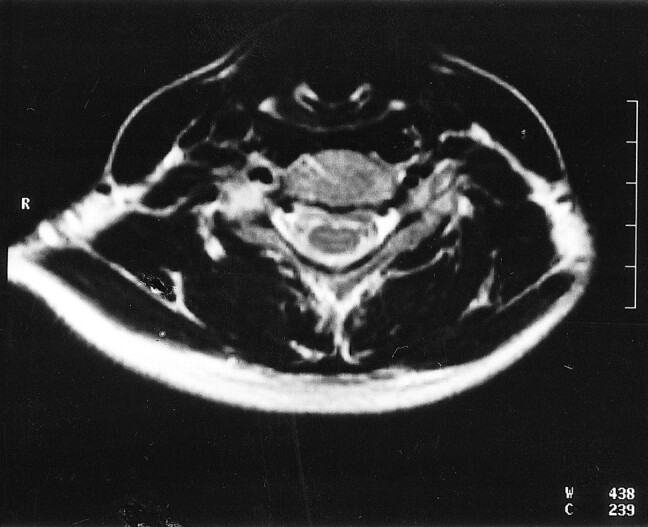
Axial T2-weighted turbo spin-echo sequence (3900/120) at C7–T1 level showing increased signal in the paraspinal soft tissues close to the right exiting root. This finding was interpreted as cerebrospinal fluid leakage.
fig 3.

Anatomic landmarks for measurement of vertical brain displacement on sagittal T1-weighted MR images (1, cerebellar tonsils; 2, fourth ventricle; 3, infundibular recess; 4/5, angle.
A, Symptomatic patient.
B, Same patient after a normal follow-up examination.
References
- 1.Clarot F, Callonnec F, Douvrin F, et al. Giant cervical epidural veins after lumbar puncture in a case of intracranial hypotension. AJNR Am J Neuroradiol 2000;21:787-789 [PMC free article] [PubMed] [Google Scholar]
- 2.Pannullo SC, Reich JB, Krol G, Deck MDF, Posner JB. MRI changes in intracranial hypotension. Neurology 1993;43:910-926 [DOI] [PubMed] [Google Scholar]
- 3.Messori A, Regnicolo L, Simonetti BF, Di Bella P, Logullo F, Salvolini U. Spontaneous intracranial hypotension syndrome: the value of brain measurements in MRI diagnosis . (in press) [DOI] [PubMed]
- 4.Mokri B, Atkinson JLD, Dodick DW, Miller GM, Piepgras DG. Absent pachimeningeal gadolinium enhancement on cranial MR despite symptomatic CSF leak. Neurology 1999;53:402-404 [DOI] [PubMed] [Google Scholar]