

Abstract
OBJECTIVES:
To examine reductions in diarrhea-associated health care utilization after rotavirus vaccine implementation and to assess direct and indirect effectiveness of vaccination.
METHODS:
Retrospective cohort analysis of claims data of commercially insured US children aged <5 years. We examined annual pentavalent (RV5) and monovalent (RV1) rotavirus vaccine coverage. We compared rates of diarrhea-associated health care utilization in prevaccine (2001–2006) versus postvaccine introduction (2007–2011) years, compared rates of diarrhea-associated health care utilization in vaccinated versus unvaccinated children and compared rates in unvaccinated children in postvaccine versus prevaccine years.
RESULTS:
Among children aged <5 years, RV5 and RV1 rotavirus vaccine coverage rates reached 58% and 5%, respectively, by December 31, 2010. Compared with the average rate of rotavirus-coded hospitalizations in 2001–2006, rates were reduced by 75% in 2007–2008, 60% in 2008–2009, 94% in 2009–2010, and 80% in 2010–2011. Compared with unvaccinated children, in 2010–2011, the rate of rotavirus-coded hospitalizations was reduced by 92% among RV5 recipients and 96% among RV1 recipients. Rotavirus-coded hospitalization rate reductions among RV5 recipients versus unvaccinated children ranged from 87% among <1-year-olds to 81% among 4-year-olds. Compared with prevaccine rates in 2001–2006, rotavirus-coded hospitalization rates among unvaccinated children decreased by 50% in 2007–2008, 77% in 2009–2010, and 25% in 2010–2011.
CONCLUSIONS:
Implementation of rotavirus vaccines has substantially reduced diarrhea health care utilization in US children. Both rotavirus vaccines conferred high protection against rotavirus hospitalizations; RV5 conferred durable protection through the fourth year of life. Vaccination also conferred indirect benefits to unvaccinated children.
Keywords: rotavirus vaccines, United States, diarrhea, rotavirus, hospitalization
In February 2006, the Advisory Committee on Immunization Practices recommended the routine use of pentavalent rotavirus vaccine (RV5; RotaTeq, Merck and Co, Whitehouse Station, NJ) in US infants with 3 doses administered orally at 2, 4, and 6 months of age.1 In June 2008, the committee updated its recommendations to include the use of monovalent rotavirus vaccine (RV1; Rotarix, GSK Biologicals, Rixensart, Belgium).2 RV1 is a 2-dose vaccine administered orally at 2 and 4 months of age. Before vaccine introduction, rotavirus was the most common cause of severe gastroenteritis in children under 5 years of age in the United States, resulting in an estimated 20 to 60 deaths, 55 000 to 70 000 hospitalizations, and nearly half a million ambulatory medical visits each year.1,3,4
Since the introduction of rotavirus vaccines, diarrhea-associated health care utilization and medical expenditures in US children have decreased substantially.5-7 Moreover, indirect benefits from rotavirus vaccination have been observed in unvaccinated children and in adults.6,7 Although RV5 vaccine impact and effectiveness have been well described for the 2008–2009 rotavirus seasons, fewer data on the impact and effectiveness of vaccination in more recent rotavirus seasons are available. Furthermore, because of its later introduction, limited information is available regarding the effectiveness of RV1 in routine use in US children.
We previously evaluated direct and indirect effects of RV5 vaccination on diarrhea-associated health care utilization in US children during 2008 and 2009 using data from MarketScan insurance claims databases.5 To evaluate the long-term impact of rotavirus vaccination in US children <5 years of age, we updated our analysis with data for the 2010 and 2011 rotavirus seasons. Our objectives were to evaluate (1) rotavirus vaccine coverage and correlate vaccine coverage with changes in the rates of diarrhea associated hospitalizations, emergency department, and outpatient visits in postvaccine versus prevaccine introduction years; (2) effectiveness of both RV5 and RV1 in contemporaneous use and the duration of protection from RV5 vaccination; (3) indirect benefits from rotavirus vaccination; and (4) national reduction in health care utilization for diarrhea and associated costs after implementation of the rotavirus vaccine program.
METHODS
Data Source and identification of Diarrhea-Associated Health Care Events
Data from the 2001–2011 Truven Health MarketScan Commercial Claims and Encounters Database were analyzed.8 MarketScan data are derived from insurance claims and contain deidentified information from various public and private health plans. Medicaid recipients are not included.
Diarrhea-associated health care events were identified with the use of the following International Classification of Diseases, Ninth Revision, Clinical Modification codes: viral enteritis, 008.6–008.8 (including rotavirus, 008.61); bacterial enteritis, 001.0–005.9 (excluding 003.2) and 008.0–008.5; parasitic intestinal disease, 006.0–007.9 (excluding 006.3–006.6); presumed infectious diarrhea, 009.0–009.3; presumed noninfectious diarrhea, 558.9; and diarrhea not otherwise specified, 787.91. In addition to all-cause diarrhea events, rotavirus-coded events (coded 008.61) were also specifically examined. An event identified as the primary discharge diagnosis or 1 of 15 other possible discharge diagnoses for the inpatient-admissions table was classified as a hospitalization. An event identified in 1 of the 2 diagnosis fields in the outpatient-services table was classified as an outpatient visit. Events were classified as emergency department visits (ie, not hospitalizations or outpatient visits) if “urgent care facility” or “emergency room” was specified in either the inpatient-services table or the outpatient-services table. Patients evaluated ≥1 setting for the same diarrhea episode had their visit included for each setting in which they were evaluated for the single episode.
RV5 and RV1 Coverage
Using data from January 2006–June 2011, we assessed RV5 and RV1 coverage (defined as administration of at least 1 dose of RV5 or RV1) in a subgroup of children with continuous enrollment in 1 insurance plan from birth through at least 3 months of age. The criterion of continuous enrollment ensured that nearly all vaccinations administered were captured. Children from 13 states with universal vaccination programs that included rotavirus vaccine at any time during the assessment period or where rotavirus vaccine inclusion in the universal vaccination program could not be ascertained (Alaska, Idaho, Massachusetts, Maine, North Dakota, New Hampshire, New Mexico, Oregon, Rhode Island, Vermont, Washington, Wisconsin, and Wyoming) were excluded from the coverage assessment because vaccinations in these states were not likely to have been billed to third-party payers and thus would probably not be recorded in this database. According to the National Immunization Survey (NIS) in 2010, the median (range) of rotavirus vaccine coverage rates among children 19–35 months old in these 13 states was 53% (42–77) compared with 59% (44–82) in states without universal rotavirus vaccination. 9 Within the coverage cohort, we identified enrollees who received RV5 and RV1 by using the Current Procedural Terminology codes 90680 and 90681, respectively.
Coverage on December 31 of each study year was assessed on the basis of age group and region. To validate results, we compared coverage with at least 1 dose of diphtheria-tetanus-acellular pertussis vaccine (DTaP) by 3 months of age in the MarketScan database with DTaP coverage reported by the NIS, considered the US standard for vaccine coverage.9
Trends in Diarrhea-Associated Health Care Utilization
We assessed trends in diarrhea-associated health care utilization rates for enrollees <5 years of age who were seen in inpatient, emergency department, and outpatient settings. Data from all states, including those with universal vaccination programs, were included in the analysis of trends. We used the number of days each child was enrolled per calendar month and year of the study as the follow-up time in calculating utilization rates per 10 000 person-years of follow-up.
We examined temporal trends of the diarrhea-associated health care utilization rate during the entire study period. Furthermore, we compared rotavirus-coded hospitalization and diarrhea-associated health care utilization rates during each of the postvaccine years 2007–2011 (July – June) with the annual mean rates during the 5-year prevaccine baseline period from July 2001–June 2006, according to age group and census region. The numbers of emergency department or outpatient visits for diarrhea with the rotavirus-specific code were too few to analyze.
Examination of Direct Benefits of RV5 and RV1 in Contemporary Use
To examine direct vaccine benefits from RV5 and RV1, we compared rates of rotavirus-coded hospitalization and diarrhea-associated health care utilization among vaccinated versus age-eligible, unvaccinated children. Because rates of rotavirus disease were low in the 2010 rotavirus season, we restricted our analyses to outcomes during the 2011 rotavirus season (ie, from July 2010 to June 2011). Children who were both age-eligible to receive at least 1 RV5 or RV1 dose before the 2011 rotavirus season (ie, those who were 3–23 months of age by July 1, 2010) and who were continuously enrolled in the same insurance plan from birth through June 30, 2011, were included in the analysis. Children who were either from states with universal vaccination programs or had received mixed vaccine schedules with both RV1 and RV5 doses were excluded. Rate ratios and 95% confidence intervals associated with RV1 or RV5 administration were adjusted for birth quarter by means of Poisson regression for hospitalizations and binomial regression for emergency department and outpatient visits. The adjusted estimates were subtracted from 1 to obtain adjusted rate reductions.
Duration of RV5 Protection
To assess the duration of protection provided by RV5, we compared rates of rotavirus-coded hospitalizations among vaccinated versus unvaccinated children, by age group (3–11 months, 12–23 months, 24–35 months, 36–47 months, and 48–59 months). We included all children who were age-eligible to receive RV5 (ie, age less than the first dose upper limit of 14 weeks and 6 days when RV5 was licensed on February 3, 2006) and who were continuously enrolled in their insurance plan for the entire time period captured within each age group. Rate ratios and 95% confidence intervals associated with RV5 administration were adjusted for birth quarter by means of Poisson regression; the adjusted estimates were subtracted from 1 to obtain adjusted rate reductions.
Indirect Benefits From Rotavirus Vaccination
To examine indirect benefits of the vaccine (ie, protection of unvaccinated persons because vaccinated persons did not contract and transmit infection), we compared rates of rotavirus-coded hospitalization and diarrhea-associated health care utilization among age-eligible, unvaccinated children <2 years of age from July to June in each study year with prevaccine rates. Rates were standardized by birth quarter to allow comparison across age groups. The relative rate reductions and 95% confidence intervals were calculated with the use of standardized morbidity ratios, with prevaccine rates as the baseline data.10
Estimation of National Reductions in Hospitalization Rates and Costs
By extrapolating observed diarrhea-associated rates of hospitalizations, emergency department and outpatient visits in children <5 years of age from July 2007 through June 2011 to the 2009 US population, we estimated the national burden of diarrhea-associated health care utilization after the introduction of the rotavirus vaccines. We then determined the median total payments for diarrhea-associated hospitalizations and converted them to 2009 constant dollars on the basis of the Bureau of Labor Statistics Consumer Price Index for medical care.11 For both the US population census and the Consumer Price Index constant dollars, estimates were based on data from 2009 as that represents the midpoint of our study period (ie, 2007–2011). Median payments were multiplied by the number of diarrhea-associated events to estimate national payments. Baseline costs were derived according to prevaccine rates from 2001 through 2006. The estimated reduction in diarrhea-associated health care utilization costs was calculated as the difference between national payments before and after the introduction of the rotavirus vaccines.
RESULTS
Rotavirus Vaccine Coverage
In a cohort of >406 000 children <5 years of age from 37 states, 58% had received at least 1 dose of RV5, and 5% had received at least 1 dose of RV1 by December 31, 2010 (Table 1). Following a rapid uptake of rotavirus vaccine after RV5 licensure, the proportion of rotavirus vaccine (either RV5 or RV1) recipients in children <1 year old continued to increase from 64% on December 31, 2007, to 78% on Deceber 31, 2010. In the same cohort, the proportion of children who had received at least 1 DTaP dose by 3 months of age was 89%, compared with 88% according to the NIS.9
TABLE 1.
Annual Rates of Rotavirus-Coded and Diarrhea-Associated Health Care Utilization Among Children <5 Years of Age Before and After Rotavirus-Vaccine Introduction, According to Age Group and Health Care Setting
| Age Group | Rotavirus-Coded Hospitalizations | Diarrhea-Associated Hospitalizations | Diarrhea-Associated ED Visits | Diarrhea-Associated Outpatient Visits | Coverage | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Rate, n/10 000 PY | Rate Reduction (95% CI), % |
Rate, n/10 000 PY | Rate Reduction (95% CI), % |
Rate, n/10 000 PY | Rate Reduction (95% CI),% |
Rate, n/10 000 PY | Rate Reduction (95% CI),% |
RV5a,% | RV1b, % | |
| <1 y | ||||||||||
| 2001–06c | 16 | ref | 65 | ref | 212 | ref | 1713 | ref | NA | NA |
| 2007–2008 | 3 | 81 (77 to 84) | 50 | 24 (20 to 27) | 204 | 4 (1 to 6) | 1608 | 6 (5 to 7) | 64 | NA |
| 2008–2009 | 4 | 78 (74 to 81) | 45 | 30 (27 to 34) | 185 | 13 (11 to 15) | 1499 | 13 (12 to 13) | 73 | NA |
| 2009–2010 | 1 | 95 (93 to 96) | 34 | 47 (45 to 50) | 131 | 38 (37 to 40) | 1196 | 30 (30 to 31) | 64 | 12 |
| 2010–2011 | 2 | 88 (85 to 90) | 36 | 45 (43 to 48) | 140 | 34 (32 to 36) | 1211 | 29 (29 to 30) | 68 | 10 |
| 1 y | ||||||||||
| 2001–06c | 33 | ref | 96 | ref | 324 | ref | 2376 | ref | NA | NA |
| 2007–2008 | 9 | 72 (69 to 76) | 56 | 41 (38 to 44) | 282 | 13 (11 to 15) | 2264 | 5 (4 to 5) | 23 | NA |
| 2008–2009 | 9 | 74 (71 to 77) | 60 | 38 (35 to 41) | 298 | 8 (6 to 10) | 2355 | 1 (0 to 2) | 64 | NA |
| 2009–2010 | 1 | 96 (95 to 97) | 35 | 64 (62 to 66) | 197 | 39 (37 to 41) | 1825 | 23 (23 to 24) | 72 | 1 |
| 2010–2011 | 4 | 87 (85 to 89) | 39 | 59 (57 to 61) | 220 | 32 (30 to 34) | 1933 | 19 (18 to 19) | 64 | 12 |
| 2–4 y | ||||||||||
| 2001–06c | 8 | ref | 32 | ref | 130 | ref | 871 | ref | NA | NA |
| 2007–2008 | 2 | 72 (67 to 76) | 21 | 34 (31 to 37) | 119 | 9 (7 to 11) | 871 | 0 (−1 to 1) | 0 | NA |
| 2008–2009 | 6 | 26 (19 to 32) | 29 | 9 (5 to 13) | 155 | −19 (−21 to −17) | 984 | −13 (−14 to −20) | 8 | NA |
| 2009–2010 | 1 | 89 (87 to 91) | 17 | 49 (46 to 51) | 105 | 19 (18 to 21) | 794 | 9 (8 to 9) | 29 | 0 |
| 2010–2011 | 3 | 63 (59 to 67) | 20 | 37 (35 to 40) | 124 | 5 (3 to 7) | 865 | 1 (0 to 1) | 53 | 0 |
| <5 y | ||||||||||
| 2001–06c | 14 | ref | 52 | ref | 185 | ref | 1348 | ref | NA | NA |
| 2007–2008 | 4 | 75 (72 to 77) | 35 | 33 (32 to 35) | 169 | 9 (7 to 10) | 1303 | 3 (3 to 4) | 17 | NA |
| 2008–2009 | 6 | 60 (58 to 63) | 39 | 25 (23 to 27) | 188 | −2 (−3 to 0) | 1360 | −1 (−1 to 0) | 32 | NA |
| 2009–2010 | 1 | 94 (93 to 95) | 24 | 54 (52 to 55) | 128 | 31 (30 to 32) | 1078 | 20 (20 to 20) | 45 | 3 |
| 2010–2011 | 3 | 80 (78 to 81) | 27 | 47 (46 to 49) | 145 | 22 (21 to 23) | 1139 | 16 (15 to 16) | 58 | 5 |
CI, confidence interval; ED, emergency department; NA, not applicable; PY, person-year; ref, reference group.
Coverage was defined as receipt of at least 1 dose of RV5 by December 31, 2007; December 31, 2008; December 31, 2009; or December 31, 2010, in children who had been in the database since birth and for at least 3 mo continuously. Coverage for children <1 y of age was restricted to those who were eligible for vaccination (ie, aged those 3–11 mo).
Coverage was defined as receipt of at least 1 dose of RV1 by December 31, 2009, or December 31, 2010, in children with the same criteria as defined for RV5 coverage. Because RV1 was not introduced until April 2008, coverage of RV1 begins with the first full season starting in 2009.
For 2001–2006, the average annual rate for the time period is shown.
Trends in Diarrhea-Associated Health Care Utilization
During 2001-2011, a total of 53 964 hospitalizations, 242 818 emergency department visits, and 1 846 488 outpatient visits associated with diarrhea were recorded among children <5 years of age. No secular trend in diarrhea-associated health care utilization was seen in prevaccine years from 2001 through 2006 (Fig 1). In each of the prevaccine years, monthly diarrhea-associated health care utilization rates peaked in February–March in all settings, similar to the seasonal pattern of rotavirus-coded hospitalizations. During each postvaccine year from 2007 through 2011, this seasonal peak was blunted compared with prevaccine years. Seasonal peaks during the 2008–2009 and 2010–2011 seasons were somewhat higher compared with seasonal peaks during the 2007–2008 and 2009–2010 seasons (Fig 1, Table 1, and Supplementary Tables 6 and 7).
Figure 1.
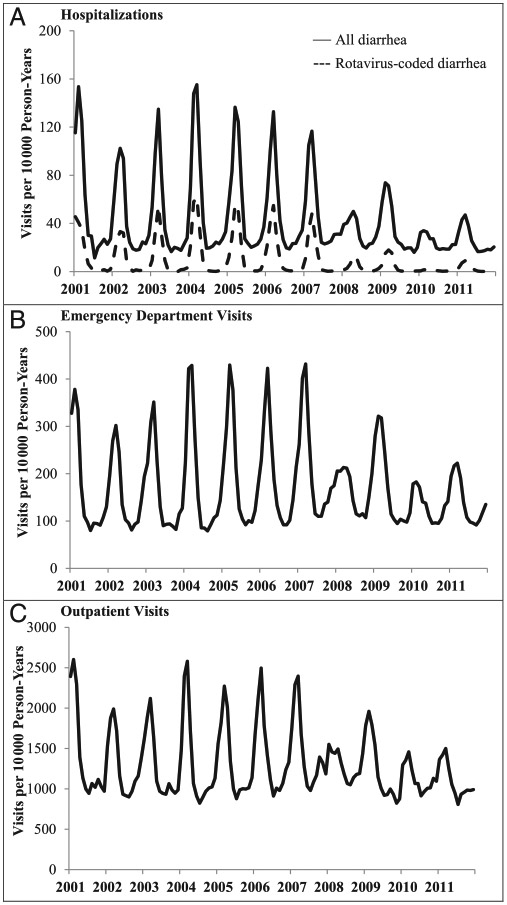
Diarrhea-associated health care utilization rates among children <5 years of age, 2001–2011.
Overall, reductions in rotavirus-coded hospitalization rates correlated with vaccine coverage across age groups, but the magnitude of reductions tended to exceed the vaccine coverage in each age group and year (Table 1). In particular, during the 2007–2008 and 2009–2010 rotavirus seasons, substantial reductions in rotavirus-coded hospitalization rates were seen in older age groups with lower vaccine coverage. In 2009–2010, the rotavirus season that had the greatest reduction of any of the 4 postvaccine seasons, annual rates of rotavirus-coded hospitalizations among children <5 years of age declined by 94% compared with prevaccine rates, from 14 hospitalizations per 10 000 person-years during 2001–2006 to 1 per 10 000 person-years in 2009–2010.
Among children <5 years of age, the annual rates of diarrhea-associated hospitalization, emergency department visits, and outpatient visits were significantly lower during each of the 4 postvaccine seasons from 2007 through 2011, except for rates of emergency department and outpatient visits during the 2008–2009 season (Table 1). The most substantial rate reductions were noted among 1-year-olds. In 2009–2010, which had the greatest reductions of all the postvaccine years, annual rates of diarrhea-associated hospitalizations, emergency department visits, and outpatient visits declined by 54%, 31%, and 20%, respectively, compared with 2001–2006 (Table 1). During the peak rotavirus months from January through June, declines in rates of diarrhea-associated health care utilization exceeded annual declines in all age groups and in each postvaccine year, consistent with an impact of vaccination (Supplementary Table 6). Declines in diarrhea-associated hospitalization rates were seen in each geographic region during each of the 4 postvaccine years (Supplementary Table 7); rates of diarrhea-associated emergency department and outpatient visits declined significantly in all regions during 2009–2011.
Examination of Direct Benefits of RV5 and RV1 in Contemporary Use
During 2010–2011, children who received RV5 and those who received RV1 had 92% and 96% fewer rotavirus-coded hospitalizations, respectively, compared with age-eligible unvaccinated children (test of interaction, P = .48; Table 2). Rate reduction in diarrhea-associated hospitalizations was 55% for children who received RV5 and 53% for those who received RV1. Diarrhea-associated hospitalization rate reductions were similar across regions, except for children who received RV1 in the West, where no effect was apparent and the number of children receiving RV1 was low, resulting in high variability for that estimate. Diarrhea-associated emergency department visit rates were reduced by 31% in RV5 recipients and by 33% in RV1 recipients, compared with unvaccinated children (Table 2). Rates of outpatient visits for diarrhea among vaccinated and unvaccinated children were similar.
TABLE 2.
Rates and Rate Reductions of Diarrhea-Associated Health Care Utilization Among Children Who Received at Least 1 Dose of RV5 or RV1 Versus Unvaccinated Children by Region During July 1, 2010–June 30, 2011a
| Region | Health Care Utilization Rate, n/ 10 000 PY |
Rate Reduction (95% CI)b, % | |||
|---|---|---|---|---|---|
| RV5 | RV1 | Unvaccinated | RV5 | RV1 | |
| Rotavirus-coded hospitalizations | |||||
| All | 1 | 0.4 | 18 | 92 (87 to 96) | 96 (74 to 100) |
| Northeast | 0 | 0 | 8 | NA | NA |
| Midwest | 1 | 2 | 27 | 96 (87 to 98) | 90 (24 to 99) |
| South | 2 | 0 | 17 | 88 (75 to 94) | NA |
| West | 0.3 | 0 | 13 | 96 (65 to 99) | NA |
| Diarrhea-associated hospitalizations | |||||
| All | 27 | 30 | 62 | 55 (46 to 62) | 53 (36 to 66) |
| Northeast | 26 | 20 | 62 | 56 (32 to 71) | 61 (11 to 82) |
| Midwest | 23 | 27 | 68 | 64 (52 to 74) | 56 (16 to 77) |
| South | 31 | 26 | 62 | 51 (36 to 62) | 60 (35 to 76) |
| West | 25 | 75 | 45 | 41 (3 to 64) | −22 (−168 to 45) |
| Diarrhea-associated ED visits | |||||
| All | 159 | 155 | 231 | 31 (25 to 36) | 33 (22 to 42) |
| Northeast | 152 | 120 | 225 | 30 (15 to 43) | 51 (27 to 67) |
| Midwest | 145 | 170 | 224 | 35 (25 to 43) | 12 (−13 to 32) |
| South | 166 | 171 | 244 | 32 (24 to 40) | 34 (19 to 46) |
| West | 166 | 87 | 211 | 17 (−3 to 34) | 53 (19 to 73) |
| Diarrhea-associated outpatient visits | |||||
| All | 1416 | 1396 | 1402 | −2 (−5 to 1) | −0.1 (−5 to 4) |
| Northeast | 1347 | 1242 | 1445 | 6 (−1 to 12) | 13 (2 to 23) |
| Midwest | 1232 | 1284 | 1182 | −7 (−13 to −1) | −10 (−21 to 0.4) |
| South | 1556 | 1500 | 1566 | 0.5 (−4 to 5) | 4 (−3 to 10) |
| West | 1392 | 1369 | 1363 | −3 (−12 to 4) | −0.2 (−16 to 14) |
CI, confidence interval; ED, emergency department; NA, not applicable; PY, person-year.
Children who were aged 3 to 23 mo at the start of the study period, July 1, 2010, and were continuously enrolled in their insurance plan from birth through the end of the study period, June 30, 2011. Vaccination status was determined by the presence or absence of a current procedural terminology code for receipt of at least 1 dose of RV5 or RV1 (eg, children who received at least 1 vaccine dose were considered vaccinated). Rates were adjusted for quarter of birth. Children who were either from states with universal vaccination programs or who had received mixed vaccine schedules with both RV1 and RV5 doses were excluded.
Rotavirus-coded diarrhea hospitalization rate reductions for among RV5 recipients in the Northeast and RV1 recipients in the Northeast, South, and West were not reported owing to small numbers of events.
Duration of RV5 Protection
Among those vaccinated with RV5 compared with age-eligible unvaccinated children, rotavirus-coded hospitalization rates were 87% lower among children 3 to 11 months of age, 87% lower among those 12 to 23 months of age, 86% among those 24 to 35 months of age, and 81% lower among those 48 to 59 months of age (Table 3). Because of low rates of rotavirus-coded hospitalization rates among vaccinated children 36 to 47 months of age, rate reductions could not be assessed for this age group.
TABLE 3.
Duration of Protection and Reduction in Rates of Rotavirus-Coded Hospitalization Among Children Who Received at Least 1 Dose of RV5 Versus Unvaccinated Children, According to Agea
| Age (mo)b | Rotavirus-Coded Diarrhea | ||
|---|---|---|---|
| Hospitalization Rate, n/10 000 PY |
Rate Reduction (95% CI), % | ||
| Vax + | Vax − | ||
| 3–11 | 1 | 8 | 87 (85–90) |
| 12–23 | 1 | 19 | 87 (84–89) |
| 24–35 | 2 | 11 | 86 (83–89) |
| 36–47 | 0 | 5 | NA |
| 48–59 | 1 | 5 | 81 (75–86) |
NA, not applicable; PY, person-year; Vax +, vaccinated; Vax −, unvaccinated.
Children who were age-eligible for the RV5 vaccine as of February 3, 2006, when RV5 was first recommended (ie, age less than the first-dose upper limit of 14 wk and 6 d when RV5 was licensed on February 3, 2006) and who were continuously enrolled in their insurance plan for at least 3 mo). Vaccination status was determined by the presence or absence of a current procedural terminology code for receipt of at least 1 dose of RV5. Children who were either from states with universal vaccination programs or had received mixed vaccine schedules with both RV1 and RV5 doses were excluded.
Age at hospitalization for a diarrhea-associated event.
Indirect Benefits From Rotavirus Vaccination
Overall, reductions of 50%, 77%, and 25% in rates of rotavirus-coded hospitalizations were observed among age-eligible, unvaccinated children during the years 2007–2008, 2009–2010, and 2010–2011, respectively, compared with prevaccine rates (Table 4). Reductions were not seen during the 2008–2009 season. Reductions in emergency department and outpatient visits were also observed among unvaccinated children, mostly during 2009–2011 (Supplementary Table 8)
TABLE 4.
Rotavirus-Coded Hospitalization Rates and Rate Reductions by Season, Among Unvaccinated Children After RV5 or RV1 Introductiona
| Study Period | Hospitalization Rate, n/10 000 PY | Rate Reduction (95% CI), % | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| All | Northeast | Midwest | South | West | All | Northeast | Midwest | South | West | |
| 2001–2006b | 24 | 16 | 25 | 31 | 13 | ref | ref | ref | ref | ref |
| 2007–2008 | 12 | 4 | 12 | 11 | 19 | 50 (36 to 62) | 76 (−13 to 95) | 52 (24 to 70) | 66 (50 to 78) | −53 (−166 to 12) |
| 2008–2009 | 23 | 12 | 29 | 25 | 7 | 2 (−17 to 18) | 24 (−86 to 69) | −16 (−52 to 12) | 19 (−4 to 37) | 41 (−40 to 76) |
| 2009–2010 | 5 | 7 | 3 | 7 | 5 | 77 (65 to 85) | 57 (−43 to 87) | 89 (69 to 96) | 76 (58 to 86) | 59 (−33 to 87) |
| 2010–2011 | 18 | 8 | 27 | 17 | 13 | 25 (4 to 41) | 50 (−23 to 79) | −7 (−52 to 25) | 46 (20 to 64) | 1 (−120 to 55) |
CI, confidence interval; PY, person-year; ref, reference group.
Data for each postvaccine study period were averaged among unvaccinated children who were age-eligible for the vaccine: those aged 3–17 mo by July 1, 2007, and those aged 3–23 mo by July 1, 2008; July 1, 2009; and July 1, 2010. Age groups were standardized by birth quarter. Rate reductions for diarrhea-associated emergency department and outpatient visits are provided in SupplementaryInformation Table 8. Children who were from states with universal vaccination programs were excluded.
Average annual hospitalization rate for 2001–2006 among children under 2 y of age during the July–June study period.
Estimated National Reduction in Health Care Utilization and Associated Costs
We estimated that nationally, 176 587 hospitalizations, 242 335 emergency department visits and 1 116 869 outpatient visits for diarrhea were averted among children <5 years of age during July 1, 2007–June 30, 2011. By applying this reduction to the median payment for a diarrhea-associated hospitalization in the MarketScan database in 2009, we estimated that health care utilization costs were reduced by $924 million for the 4-year period (Table 5).
TABLE 5.
Estimated Reductions in the Number and Cost of Diarrhea-Associated Health Care Utilization Among Children <5 Years of Age, After the Introduction of Rotavirus Vaccine in the United States, 2007–2011a
| Year | No. of Hospitalizations | Reduction | No. of ED Visits | Reduction | No. of Outpatient Visits | Reduction |
|---|---|---|---|---|---|---|
| No. of events | ||||||
| 2001–2006 | 110 688 | ref | 394 619 | ref | 2 871 726 | ref |
| 2007–2008 | 73 778 | 36 890 | 360 218 | 34 401 | 2 775 196 | 96 530 |
| 2008–2009 | 82 703 | 27 965 | 401 237 | NAb | 2 896 199 | NAb |
| 2009–2010 | 51 410 | 59 258 | 272 768 | 121 851 | 2 296 955 | 574 771 |
| 2010–2011 | 58 195 | 52 473 | 308 536 | 86 083 | 2 426 159 | 445 568 |
| Total 2007–2011 | NA | 176 587 | NA | 242 335 | NA | 1 116 869 |
| Cost ($) | ||||||
| 2001–2006 (annual average) | 473 770 195 | ref | 137 327 317 | ref | 212 507 733 | |
| 2007–2008 | 315 842 541 | 157 927 653 | 125 355 743 | 11 971 574 | 205 364 510 | 7 143 223 |
| 2008–2009 | 354 051 300 | 1 19 718 894 | 139 630 312 | NAb | 214 318 757 | NAb |
| 2009–2010 | 220 086 757 | 253 683 438 | 94 923 144 | 42 404 173 | 169 974 663 | 42 533 070 |
| 2010–2011 | 249 132 453 | 224 637 742 | 107 370 586 | 29 956 731 | 179 535 738 | 32 971 995 |
| Total 2007–2011 | NA | 755 967 727 | NA | 84 332 478 | NA | 82 648 288 |
ED, emergency department; NA, not applicable; ref, reference group.
Numbers of hospital care utilization visits were derived by applying average rates of hospitalizations, emergency department visits, and outpatient visits for July 2001–June 2006, July 2007–June 2008, July 2008–June 2009, July 2009–June 2010, and July 2010–June 2011 to the 2009 US Census population estimate for children under 5 y of age. The 2009 estimates were selected as are the midpoints between years 2007–2011. Treatment costs were calculated by multiplying the numbers of health care utilization visits by the inflation-adjusted median payment per visit during the July 2008–June 2009 period ($4281, $348, and $74 for hospitalizations, ED visits, and outpatient visits, respectively).
During 2008–2009 season there was an increase of 6618 emergency department visits and 24 473 outpatient visits with an estimated cost of $2 302 995 and $1 811 025, respectively. These increases were not included in the calculated totals.
DISCUSSION
We observed declines in rates of diarrhea-associated hospitalizations, emergency department visits, and outpatient visits in US children <5 years of age over four successive rotavirus seasons following implementation of rotavirus vaccination, with greater declines in later years when greater vaccine coverage had been achieved and during months of the year with peak rotavirus activity. Both RV5 and RV1 were highly effective in preventing rotavirus-coded hospitalizations and also prevented diarrhea-associated hospitalizations and emergency department visits; both vaccines conferred similar protection. The protection from RV5 vaccination against rotavirus-coded hospitalizations was sustained at a high level through four years of life, with no indication of waning immunity. The reduction in rotavirus-coded hospitalization rates among unvaccinated children in postvaccine years compared with prevaccine years indicates indirect benefits from vaccination; the magnitude of indirect benefit varied over the study years. Overall, during 2007–2011, we estimated that rotavirus vaccination reduced diarrhea health care utilization by ~1.5 million visits and associated costs by $924 million in the United States.
Reductions in rotavirus and all-cause diarrhea-associated hospitalizations in US children during the 2007–2008 and 2008–2009 rotavirus seasons have been well documented.5-7,12-14 Our results demonstrate that these declines were sustained and were greater in the subsequent rotavirus seasons in 2009–2010 and 2010–2011. Furthermore, a biennial pattern in the incidence of severe rotavirus disease emerged in postvaccine years, with low incidence in 2007–2008 and 2009–2010 and greater incidence in adjacent years. In addition, we documented significant declines in the 2009–2010 and 2010–2011 rotavirus seasons in rates of emergency department and outpatient visits for diarrhea; these ambulatory outcomes have not been well evaluated in postlicensure US evaluations and were not significantly reduced in our previous evaluation of MarketScan data for 2007–2008 and 2008–2009 rotavirus seasons.5 Both increasing vaccine coverage and indirect protection among older and unvaccinated children may have contributed to the declines in emergency department and outpatient visits observed during 2009–2011.9 By the end of 2010, rotavirus vaccine coverage had reached 63% of children <5 years of age and 78% in children <1 years of age; however, rotavirus vaccination rates were still ~10% lower than DTaP vaccination rates in this age group.9
Our study has some limitations. First, information on ethnic group, race, and socioeconomic status is not included in MarketScan data and uninsured and Medicaid populations are not represented; these gaps may affect generalizability of our findings to some extent. Specifically, our comparison of MarketScan coverage results with NIS coverage estimates among publicly insured or uninsured population should be interpreted with caution. Second, rotavirus testing and coding are not consistently performed across all health care settings; thus, we were not able to examine the effect of vaccination specifically against rotavirus-coded emergency department and outpatient visits. Third, although we adjusted for age-related variation in the risk of rotavirus disease and changes in vaccine coverage over time by controlling for quarter of birth, we may have not accounted for all potential confounders. Finally, although we estimated reduction in health care costs from diarrhea following vaccine implementation, a full analysis of the cost-effectiveness of vaccination requires consideration of other factors, particularly the cost of the vaccine program and indirect cost savings from prevention of lost productivity.
CONCLUSIONS
In summary, our findings demonstrate the substantial and sustained decline in diarrhea-associated health care utilization and related costs in US children after rotavirus vaccine implementation. Both rotavirus vaccines showed comparable effectiveness and long-term protection was documented for RV5. Indirect benefits from vaccination were observed and have amplified the overall impact of the vaccination program.
Supplementary Material
WHAT’S KNOWN ON THIS SUBJECT:
Since the introduction of rotavirus vaccines, diarrhea-associated health care utilization among US children has decreased substantially. Moreover, indirect benefits from rotavirus vaccination have been observed in unvaccinated children and in adults.
WHAT THIS STUDY ADDS:
With increasing rotavirus vaccine coverage during 2009–2011, we observed continued reductions in diarrhea-associated health care utilization and cost. Both rotavirus vaccines conferred high protection against rotavirus hospitalizations; pentavalent rotavirus vaccine provided durable protection through the fourth year of life.
Acknowledgments
FUNDING: No external funding.
ABBREVIATIONS
- DTaP
diphtheria-tetanus-acellular pertussis vaccine
- NIS
National Immunization Survey
- RV1
monovalent rotavirus vaccine
- RV5
pentavalent rotavirus vaccine
Footnotes
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
Reprints
Information about ordering reprints can be found online: http://www.aappublications.org/site/misc/reprints.xhtml
REFERENCES
- 1.Parashar UD, Alexander JP, Glass RI; Advisory Committee on Immunization Practices, Centers for Disease Control and Prevention. Prevention of rotavirus gastroenteritis among infants and children. Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2006;55(RR-12):1–13 [PubMed] [Google Scholar]
- 2.Cortese MM, Parashar UD; Centers for Disease Control and Prevention. Prevention of rotavirus gastroenteritis among infants and children: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2009;58(RR-2):1–25 [PubMed] [Google Scholar]
- 3.Malek MA, Curns AT, Holman RC, et al. Diarrhea- and rotavirus-associated hospitalizations among children less than 5 years of age: United States, 1997 and 2000. Pediatrics. 2006;117(6):1887–1892 [DOI] [PubMed] [Google Scholar]
- 4.Payne DC, Staat MA, Edwards KM, et al. Active, population-based surveillance for severe rotavirus gastroenteritis in children in the United States. Pediatrics. 2008;122(6):1235–1243 [DOI] [PubMed] [Google Scholar]
- 5.Cortes JE, Curns AT, Tate JE, et al. Rotavirus vaccine and health care utilization for diarrhea in U.S. children. N Engl J Med. 2011; 365(12):1108–1117 [DOI] [PubMed] [Google Scholar]
- 6.Curns AT, Steiner CA, Barrett M, Hunter K, Wilson E, Parashar UD. Reduction in acute gastroenteritis hospitalizations among US children after introduction of rotavirus vaccine: analysis of hospital discharge data from 18 US states. J Infect Dis. 2010;201 (11):1617–1624 [DOI] [PubMed] [Google Scholar]
- 7.Lopman BA, Curns AT, Yen C, Parashar UD. Infant rotavirus vaccination may provide indirect protection to older children and adults in the United States. J Infect Dis. 2011;204(7):980–986 [DOI] [PubMed] [Google Scholar]
- 8.Truven Health MarketScan Commercial Claims and Encounters Database. Ann Arbor, MI: Thomson Rueters; 2011 [Google Scholar]
- 9.Estimated vaccination coverage with individual vaccines by 3 months of age. National Immunization Survey. 2012. Available at: www.cdc.gov/vaccines/stats-surv/nis/data/tables_2011.htm#age. Accessed June 3, 2013, 2013 [Google Scholar]
- 10.Rothman KJ, Greenland S, eds. Modern Epidemiology. 2nd ed. Philadelphia, PA: Lippincott-Raven; 1998 [Google Scholar]
- 11.Consumer Price Index. Available at: https://www.bls.gov/data. Accessed June 3, 2013
- 12.Chang HG, Smith PF, Tserenpuntsag B, Markey K, Parashar U, Morse DL. Reduction in hospitalizations for diarrhea and rotavirus infections in New York state following introduction of rotavirus vaccine. Vaccine. 2010;28(3):754–758 [DOI] [PubMed] [Google Scholar]
- 13.Tate JE, Mutuc JD, Panozzo CA, et al. Sustained decline in rotavirus detections in the United States following the introduction of rotavirus vaccine in 2006. Pediatr Infect Dis J. 2011;30(suppl 1):S30–S34 [DOI] [PubMed] [Google Scholar]
- 14.Yen C, Tate JE, Wenk JD, Harris JM II, Parashar UD. Diarrhea-associated hospitalizations among US children over 2 rotavirus seasons after vaccine introduction. Pediatrics. 2011;127(1). Available at: www.pediatrics.org/cgi/content/full/127/1/e9 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.