

Abstract
Background and aim:
Important public health improvements have been achieved over the past decades, but new challenges are emerging and progress cannot be taken for granted. Urban settlements host most of the global population, but they are also sources of several threats. The aim of the paper is to investigate the role of architects and planners in contributing to overcome these critical health challenges and propose strategic actions for collaboration with the public health workforce.
Methods:
Taking global trends and public health challenges as starting point, a scoping literature review has been conducted to illustrate the possible synergies that architecture and public health workforce should exploit to support population health improvement and tackle key public health challenges.
Results:
The built environment affects climate change and public health through the use of resources, site location, and green spaces. In architecture curricula, limited space is devoted to health and vice versa. There is an urgent need for recognition of the benefits of collaboration and cross-fertilisation between public health and planning workforce from local to global levels.
Conclusion:
Public health is evolving from a bio-medical to a socio-anthropological approach and architects/planners have fundamental roles; further collaboration, research and training are needed.
Keywords: public health, urban health, workforce collaboration, climate change, noncommunicable diseases, evidence based design, urbanization, multidisciplinary, architects role
Introduction
Public health transformations and challenges
In recent years, important public health improvements have been achieved thanks to technological, social and economic evolution, but this progress cannot be taken for granted. The risk that this success can be reversed is real. In the era of increasing urbanization, globalization, digitalization, ageing population, rise of non-communicable diseases and climate changes, the nature and scale of public health challenges is rapidly evolving, and significant transformations are both necessary and urgent (1-4).
Globally, the average life expectancy at birth increased by 5.5 years between 2000 and 2016 reporting the fastest increase since the 1960s (5). Overall, it is expected to increase by 4.4 years between 2016 and 2040 and by 7.8 years for males and 7.2 years for females if more progresses are made. Nevertheless, if less progress is made, life expectancy could even decrease by 0.4 years for males and stagnate for females (6). Additionally, latest CDC data show that the U.S. life expectancy has declined over the past few years and this troubling trend is largely driven by deaths from drug overdose and suicide (7).
According to the latest Bloomberg Global Health Index, good health is still not achievable for all the countries and there are tremendous differences between the top 10 and the lowest ones (8). If a key component of achieving universal health coverage is ensuring that all populations have access to quality health care those data appears as fairly critical. Indeed, despite substantial gains since 2000, many low and middle Socio-demographic Index (SDI, a summary measure of overall development) countries, face considerable challenges unless intense policy action and investments focus on advancing access to and quality of health care across key health services, especially Non-Communicable Diseases (NCD) (9). NCDs, such as diabetes, cancer and heart diseases, are responsible for over 70% of global deaths. The associated principal risk factors, that also exacerbate mental health issues are: tobacco use, physical inactivity, harmful use of alcohol, unhealthy diets and air pollution (5).
Emergent conceptual frameworks place a substantial focus on the built and urban environment not least because of the contribution that healthy urban design can make to the prevention and reduction of the burden of disease associated with these elements..
For example it is recognized that two sets of risk factors related to obesity such as food quality and physical activity are strictly linked to built environment characteristics in terms of physical access to local supermarkets, groceries, fast food restaurants, or convenience stores, area walkability, greenness, blue water, land use mix, and access to recreational facilities (10).
Another important topic to consider is the risks related to air pollution and the impact this has on stroke, heart disease, lung cancer prevalence, and both chronic and acute respiratory diseases, including asthma. Healthy design intervention along with sustainable policies at the urban and building level (such as supporting cleaner transport, energy-efficient homes, power generation, industry and better waste management) would reduce key sources of outdoor air pollution (11).
Finally, recent studies highlighted that good accessibility to public transport and densely built urban texture could contribute to reduce mental health risks such as depression, especially for fragile citizens (12); at the same time, poor environmental conditions and building features that include ventilation, lighting, temperature, indoor microbial, chemical and pest exposures are likely to have negative impacts (13) .
Transformations in cities and society and their impact on public health
Cities significantly contributed to increase health conditions and are also deeply linked to the aforementioned NCDs risk factors. In fact, at the beginning of 20th century only 10% of people inhabited urban settlements while in 2015 more than half (54%) of the world population lived in urban area and this figure is projected to 60% in 2030 and 66% in 2050. The United Nations estimates that more than 90% of future urban population growth will be in developing countries (14,15). Cities constitute centers of concentration of wealth, productive capability and creativity. They are best placed to satisfy population needs because basic services can be produced at a higher quality and at lower per-capita costs, and because in cities people can best organize for their rights (16). At the same time, cities are the platform of several issues that in the recent history contributed to challenging the living conditions of dweller and workers. For example, the industrial revolution radically transformed our cities and society. Whilst significantly supporting economic growth, it also gave rise to several environmental and health problems which were new at that epoch. As stated by Szreter, “The world’s first industrial revolution seemed to be having anything but obvious health benefits for the majority of the population” (17). Today leap changes in civilizations spearheaded by technology breakthroughs and economic growth do not always automatically result in improved health, at least not for all persons from all backgrounds in society, and particularly if they harm the earth and the environment. Another example is that urban sprawl and the segregation of workplaces from housing, when incorporated with the increasing affordability of motor vehicles and the prioritization by policy makers and planners of mobility over accessibility, have led to an over reliance on the private motor vehicle increasing sedentary, pollution and other relevant NCDs risk factors (18,19). At the same time global challenges for 21st century cities emerged related to a fast-growing urban population. Foremost amongst these include, the need for expansion of affordable housing, upgrading of water and sanitation infrastructure, provision of critical services to increasing numbers of migrants to the city and meeting of the growing demand for a reliable energy supply while mitigate greenhouse gas emissions. Cities with clean air, energy-efficient infrastructure, and widely accessible green spaces can attract more investment and businesses, create more jobs, and offer more opportunity to people from all walks of life. These issues cannot be tackled by Public Health professionals alone but there is a need for a multidisciplinary approach, stressing the social responsibility of practitioners that are directly involved into the urban planning process.
Starting from the Health in All policies and the humble recognition that health system alone can only make a limited contribution to health improvements, a more holistic intervention can support the creation of policies such as the Economy of Wellbeing, putting people and their wellbeing at the center of decision-making processes (20,21). This can improve productivity, foster gender equality and increase social protection toward a sustainable long-term economic growth (22).
In the climate change era, socially responsible urban planners need to recognize and assume a role in improving the living conditions of city dwellers, recognizing that urban development is deeply linked to politics, economics, management and health (16,23).
In March 2019 the European chapter of the International Academy for Design & Health organized the 1st European Sysmposium in “Salutogenic Hospital Design and Urban Health - Global Perspectives and Local Identities in Healthcare Architecture”, as a first attempt to set up this dialogue at the international level boosting what already achieved by national associations both in health and planning field (i.e. SIti, Italian society of Public Health and CNETO, Italian Center for Healthcare Architecture) patronaging different events and multidisciplinary working groups, in line with the innovation addressed by the European Public Health Association (EUPHA). The symposium value was to bring in the keynote session high level political representatives and decision makers (Minister of Health, Regional and Municipal healthcare authorities) along with international experts in the field of Public Health, Planning and Architecture (24).
Research Objective
Therefore, starting from this exemplary event and the challenges addressed, the aim of the paper is to investigate the relationship between public health and architecture and understand the benefits that such synergy can provide to populations and urban health.
Methods
The 2019 International Academy for Design & Health 1st European Symposium “Salutogenic Hospital Design & Urban Health – Global Perspectives and Local Identities in Healthcare Architecture” offered the platform for bringing together different expertise from the public health and the built environment field and to understand the common challenges that the two disciplines are facing. In the same year World Health Organization (WHO) started its new 5-year strategic plan focusing on universal health coverage, health emergencies and promoting better health and wellbeing. Reaching these goals would include targeting the 17 Sustainable Development Goals as well and therefore will require addressing the threats to health from a variety of angles (25). A multidisciplinary approach is therefore mandated. As stressed by WHO, issues including climate change and NCDs, are not exclusively the public health workforce responsibility, but several professional fields are involved. Specifically, in recent years there is a growing awareness on the role of architects and urban planners around those issues and researchers are starting to ask themselves “What can urban planners do to promote the health and wellbeing of people in their cities and regions?” (26).
Therefore, the paper is developed as a scoping review, with the aim of deepening the understanding of the relationship between public health and urban/architectural planning. In particular, specific research questions are explicitly addressed hereafter:
Are there example of existing relationships between public health and architecture? Is the scientific literature addressing this topic? Which are the challenges? Are there areas or challenges for future improvement?
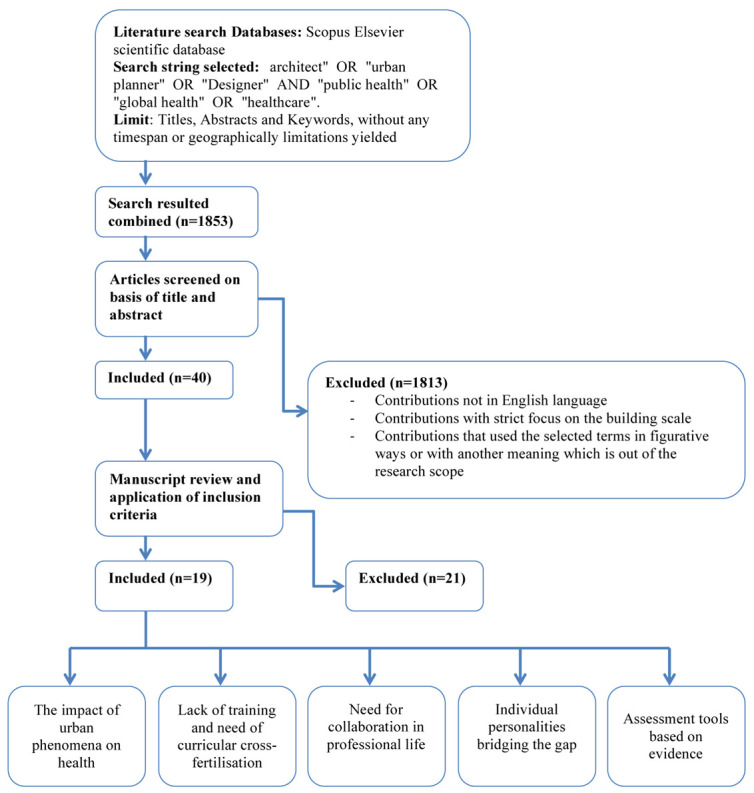
In order to address the research question, a literature review was conducted in the Scopus Elsevier scientific database. This database was preferentially selected because it involves most of the technical and social science disciplines that might include a substantial component of the contributions related to architecture, urban planning and engineering along with public health, health management and health policies researches. After some preliminary searches based on the keywords that emerged during the 2019 International Academy for Design & Health 1st European Symposium “Salutogenic Hospital Design & Urban Health – Global Perspectives and Local Identities in Healthcare Architecture”, the search string selected was the following:
“architect” OR “urban planner” OR “designer” AND “public health” OR “global health” OR “healthcare”.
This combination searched in Titles, Abstracts and Keywords, without any timespan or geographically limitations yielded 1853 results.
The results were screened and several contributions were excluded because they were out of the research scope. In particular the main exclusion criteria were:
contributions not in English language. Some papers seemed to tackle the issue in a precise manner but they were available only in original language (i.e. Portuguese) and therefore they have been excluded because of their limited audience and local scope.
contributions with strict focus on the building scale. Some papers had a specific focus on the role of architects and planner in the design or management of building assets, especially hospital facilities. This area is very specific therefore only contributions with explicit reference to health have been considered
contributions that used the selected terms in figurative ways or with another meaning which is out of the research scope (i.e. architecture used as a metaphor for articulated public health governance characteristics).
After title and abstract screening, 40 full text papers were read and out of these 19 were selected, analysed and further discussed according to the following 5 thematic areas:
The impact of urban phenomena on health
Lack of training and need of curricular cross-fertilisation
Need for collaboration in professional life
Individual personalities bridging the gap
Assessment tools based on evidence, such as: Strategic Environmental Assessment (SEA), Sustainability Assessment (SE) or Health Impact Assessment (HIA).
The full Prisma flow diagram is described in Figure 1 while the complete list of papers is highlighted in Annex 1.
Figure 1.
WHO regions of origin: distribution of subjects per year of study
ANNEX 1.
Table of Literature included
| Authors, year | Authors | Year | Title | Journal | type | place | author field | journal field | Urban phenomena impacts on health | Lack of training and need of curricula contamination | Need for collaboration in professional life Need for collaboration in professional life | Individual personalities bridging the gap | Assessment tools based on evidence (SEA / SE / HIA / EBD) |
| Dubé, 2000 | Dubé, P. | 2000 | Urban health: An urban planning perspective | Reviews on Environmental Health | study | Canada | policy | health | x | ||||
| De La Barra, 2000 | De La Barra, X. | 2000 | Fear of epidemics: The engine of urban planning | Planning Practice and Research | study | Chle | policy | design | x | ||||
| Barton, 2005 | Barton, H. | 2005 | A health map for urban planners: Towards a conceptual model for healthy, sustainable settlements | Built Environment | review | UK | design | design | x | x | x | ||
| Kochtitzky et al, 2006 | Kochtitzky, C.S., Frumkin, H., Rodriguez, R., Dannenberg, A.L., Rayman, J., Rose, K., Gillig, R., Kanter, T. | 2006 | Urban planning and public health at CDC | MMWR. Morbidity and mortality weekly report | review | USA | health+ policy | health | x | x | |||
| Galea et al, 2006 | Galea, S., Freudenberg, N., Vlahov, D. | 2006 | Cities and the Health of the Public | A framework for the study of urban health | study | USA | health | health | x | ||||
| Gorman et al, 2007 | Gorman, N., Lackney, J.A., Rollings, K., Huang, T.T.-K. | 2007 | Designer schools: The role of school space and architecture in obesity prevention | Obesity | review | USA | health+ design | health | x | x | |||
| Younger et al, 2008 | Younger, M., Morrow-Almeida, H.R., Vindigni, S.M., Dannenberg, A.L. | 2008 | The Built Environment, Climate Change, and Health. Opportunities for Co-Benefits | American Journal of Preventive Medicine | review | USA | health | health | x | x | x | ||
| Plkington et al, 2008 | Pilkington, P., Grant, M, Orme, J. | 2008 | Promoting integration of the health and built environment agendas through a workforce development initiative | Journal of the Royal Institute of Public Health | study | USA | design | design | x | x | x | ||
| Verderber, 2012 | Verderber, S. | 2012 | Sprawling cities and our endangered public health | Sprawling Cities and Our Endangered Public Health | study | USA | design | design | x | ||||
| Seidel et al, 2012 | Seidel, A.D., Kim, J.T., Tanaka, I.B.R. | 2012 | Architects, urban design, health, and the built environment | Journal of Architectural and Planning Research | review | USA | design | design | x | x | x | ||
| Ganske, 2012 | Ganske, I. | 2012 | A different angle: Physician and architect | Physicians' Pathways to Non-Traditional Careers and Leadership Opportunities | study | USA | health | health | x | x | x | ||
| Burton et al, 2015 | Burton, A., Bambrick, H., Friel, S. | 2015 | If you don't know how can you plan? Considering the health impacts of climate change in urban planning in Australia | Urban Climate | study | Australia | health | design | x | x | |||
| Exner, 2015 | Exner, M. | 2015 | Edwin Chadwick and the public health act 1848: Principal architect of sanitary reform | Routledge Handbook of Water and Health | review | UK | health | health | x | x | |||
| Capolongo et al, 2016 | Capolongo, S., Lemaire, N., Oppio, A., Buffoli, M., Le Gall, A.R. | 2016 | Action planning for healthy cities: The role of multi-criteria analysis, developed in Italy and France, for assessing health performances in land-use plans and urban development projects | Epidemiologia e Prevenzione | study | Italy+ France | design | health | x | x | x | ||
| Dannenberg & Burpee, 2018 | Dannenberg, A.L., Burpee, H. | 2018 | Architecture for Health Is Not Just for Healthcare Architects | Health Environments Research and Design Journal | comment | USA | health+ design | design | x | x | x | ||
| Anderson, 2019 | Anderson, D.C. | 2019 | Bricks and Morals—Hospital Buildings, Do No Harm | Journal of General Internal Medicine | comment | USA | health+ design | health | x | x | x | ||
| Carmichael et al, 2019 | Carmichael, L., Townshend, T.G., Fischer, T.B., Lock, K., Petrokofsky, C., Sheppard, A., Sweeting, D., Ogilvie, F. | 2019 | Urban planning as an enabler of urban health: Challenges and good practice in England following the 2012 planning and public health reforms | Land Use Policy | study | UK+ South Africa | health+ design+ policy | design | x | x | x | ||
| Marsh et al, 2020 | Marsh, R., Pilkington, P., Rice, L. | 2020 | A guide to architecture for the public health workforce(Article) | Public Health | study | UK | health+ design | health | x | x | x | ||
| Rice, 2020 | Rice, L. | 2020 | The nature and extent of healthy architecture: the current state of progress | Archnet-IJAR | review | UK | design | design | x | x | x |
Results
Descriptive analysis of the papers reviewed
Amongst the papers reviewed, the majority are primary studies (58%), 6 (32%) literature reviews and two commentaries/ editorials. Both in the primary studies as well as in the reviews, authors attempted to identify a problem or issue and propose possible frameworks to deepen the topic understanding or the systematization and conceptual elaboration. This is itself denotes a high level of novelty of the research field. Research was mostly developed in USA (47%) and UK (32%) -if considering also a case of collaboration with South Africa institution). Canada, Chile and Australia Italy and France contributed one paper each. No studies from Asian countries were found.
The topic is very recent, indeed the oldest papers included have been published in year 2000 while the newest are from year 2020.
The author affiliations are related to three main fields typically; policy, design (built environment) and health. Only two group of authors (11%) can be related to the policy-making field, 5 (26%) to the architectural, built environment and urban design field and 6 (32%) to the public health and medical field. The remaining 32% (6 out of 19) papers have been written by co-authors that are coming from a combination of these different fields, showing a good level of collaboration.
The authors published slightly more in public health-related journals (58%) versus a 42% of the articles that are from built environment related platform. An interesting fact is that in two cases design-related authors published in health-related journals and vice-versa.
In general terms, it is noted that in the last 20 years the topic of relationship between design and health emerged, first from a policymaker point of view and then in the architectural and public health field, with a growing interest in cross-fertilisation and multidisciplinarity.
The impact of urban phenomena on health
Worldwide, the urban population has grown rapidly from 751 million in 1950 to 4.2 billion in 2018 and projections show that global trends could add another 2.5 billion by 2050 resulting in almost 70% of the total population (15). Therefore, seeking to improve public health globally requires an improved awareness of how urban life affects health and well-being (27) .
Sanitary engineering interventions importantly changed the profile of many diseases such as the case of Cholera outbreaks, where the water depuration and the improvement of sewer systems in urban areas are fundamental actions to prevent and reduce the diffusion of the bacteria (28). Indeed today several forms of engineering expertise are applied to basic public health problems, such as improving water, sanitation, and hygiene (WASH) conditions in low and middle income countries (29).
Since the mid-1990s, the European Sustainable Cities and Towns Campaign with the participation of the WHO-Healthy Cities has explored the relationship between health and planning. SDG 11 in particular aims to make cities and human settlements inclusive, safe, resilient and sustainable. Other SDGs and many of the 169 SDG targets relate closely to urban design and health planning dimension with specific regard to housing, transportation, water management, air quality, etc. (30,31). As stated by several researchers, built environment can contribute to climate change, influence transportation and affect health through the use of resources, materials, site location, availability of green space (32-35). Urban planning and public health share also common missions and perspectives. Both aim to improve human well-being, emphasize needs assessment and service delivery, manage complex social systems, focus at the population level, and rely on community-based participatory methods (36).
Urban environment, indeed, affects all aspect of life and health and therefore architects and planner play an important role in determining health and wellbeing (27,35).
Lack of training, need for curricular cross-fertilisation and collaboration in professional life
Nevertheless, despite health being considered in several relevant documents, (i.e. EU policies, UN and WHO reports) it does not appear to be part of the architectural profession or education at European and international level (35). Marsh et al recently showed that the Royal Society of Public Health reported that professionals related to environment (including architects and planners) are considered between the largest employment group of professionals that have impact in the wider public health realm (13%), the ones that should be most interested but the least involved into the public health agenda (1%) (4). Scholars highlighted that the profession charged with planning the urban environment currently lacks a conceptual framework for integrating health into spatial planning decision- making (32). As already mentioned, since 1992 Rio “Earth summit” and the introduction of SDGs, the official view of urban planning has shifted from a simply physical or aesthetic constructs, or manifestations of economic forces, toward providers of sustainable and healthy human habitat and ecosystems (30,32). Nevertheless, as recently pointed out by Rice, there are no requirements that stipulate that health expertise should be mandatory in the institution and agencies that have the power to mandate the scope of architectural profession, training education practice or knowledge. The current situation is that the design of built environment is undertaken by professional figures that lack sufficient exposure on health throughout their education (35,4). Despite exceptional situations in top European universities, among which is important to mention Politecnico di Milano “Design & Health Lab” and Chalmers University of Technology “Center for Healthcare Architecture”, health is rarely considered and never systematically incorporated into the architecture and planning curricula. By becoming knowledgeable about the growing body of research on health and the built environment, architects can become a positive force in the development of healthy urban centers (37,38).
Individual personalities bridging the gap and assessment tools based on evidence
Since 1854 Jon Snow’s study of public water pump in London to fight cholera, toward 1960s Jane Jacobs’s call for safe, walkable and non-segregating American cities, relevant personalities have overcome the disciplinary threshold between public health and urban studies (36,39). But it is now time for a call to systematic action for all the professionals and researchers, professional bodies and institutions to closely work together to face the biggest challenges for public health at global level.
Some methodologies and assessment tools, such as Strategic Environmental Assessment (SEA) and Sustainability Assessment (SA) encourage holistic, systematic projects and plans appraisal, but deeper frameworks are necessary (32,40,41). Examples of Health Impact Assessment (HIA) tools are also encouraged by the WHO and some examples are emerging (30, 42). Tools and methodologies are important in order to support the decision makers. Difficulties in basing decisions on evidence can be related to language, exploitability of data, relevancy, not willingness of listen the academic results or, not direct link of health benefits with return on investments (30). Therefore, public health evidence must be translated into actionable healthy planning principles ensuring an Evidence-Based Design process of planning at different scales, providing empirical data on design elements. While architecture itself does not necessarily provide a cure, good design can also act as a preventive tool and enhance the overall quality of life (43-45). As per the introduction of green and sustainable requirements into European laws, regulation and recommendation, there is the urgent need of identify also healthy requirements to be translated into rigorous and concrete policy interventions (46-48).
Discussion
The need for collaboration between the two fields
There is a renewed and growing recognition of the link between public health and built environment because many of the most important advancements in public health have come thanks to improvement and innovation in the built environment. Moreover, recent rising public health issues such as obesity and non-communicable diseases stressed the attention on the lifestyle and on how built environment can impact that. Unfortunately, the specialists in public health have not worked alongside built environment colleagues and the same happened with other way around. Therefore, the need for a workforce development initiative through shared learning and reflection between the two professional sectors and agendas emerges (37).
On one hand, by focusing on the health-promoting aspects of design, architects have the opportunity to contribute to find solutions to major societal challenges, to lead change, to improve the quality of life for everyone, and to grow the demand for their services (49). In the ideal world, architects and their clients will begin to consider the health-promoting aspects of design as routine and desirable as they now consider sustainable elements of design understanding that many features of sustainable design offer co-benefits of promoting health (50). To reach that stage, architecture students and health science students need to be taught consistently about the health impacts of design elements in an Evidence Based Design perspective (4,35,51).
On the other hand, among the different non-traditional careers and leadership opportunities that medical doctors have, an emerging field is the relationship between health and built environment. As highlighted by Ganske, clearly emerge the need of cross-fertilisation between the two field both in education and in practice. This shared learning approach could open up valuable and multidisciplinary career possibilities strengthening the characteristics of public health as interdisciplinary and multi-professional field (52,53).
Joint collaboration between the two field and a higher degree of contamination should be promoted and improved. Working across sectors to incorporate a health promotion approach in the design and evaluation of built environment components may mitigate climate change, promote adaptation, and eventually improve public health (34,54). Furthermore, the engagement of professional bodies, institutions and government for significantly incorporating and better integrating health in the built environment and urban agenda is fundamental. Leadership capabilities emerged to be very important in this negotiation, in order to building bridges, enforcing the decision-making role and empowering the next generations (55). Appropriate governance is also important in terms of policies, structures, funding and services that are able to leverage and address resources in a proper way. Finally, it is important to exploit the power of contemporary communication and dissemination toward politicians, clinicians and technicians but, as well, to the general public with a wise use of new media and a narrative aligned to people’s real concerns.
Both evidence and experience should support large scale decisions to solve complex problems and communicate the solutions to the wider public in order to truly implement the SDGs.
Conclusion
Recent trends in contemporary society engender new challenges for public health, including climate change, ageing population and non-communicable diseases. To face those complex issues a novel and multidisciplinary approach is required and public health workforce should be enriched and contaminated by other disciplines.
The appraisal of the literature in the area highlighted also important gaps and relevant future research agenda in terms of analysis, advocacy and actions. New strategies must be taken in the different fields of research, teaching and practice in order to improve the synergies and achieve global objectives.
The literature review conducted highlights in several ways that the built environment in which we live is a significant determinant of health. Therefore, architecture and planning should be finally considered as an instrument for creating healthy communities and contribute to tackling the emerging public health challenges at local and global level. Public health is the result of various socio-economic, cultural and environmental factors and therefore should move from a bio-medical to a socio-anthropological model. Contamination between planning and health in the spheres of education, research, dissemination and governance is highly recommended for future developments.
Limitations
The search has been conducted only in Scopus Elsevier database and only scientific articles have been reviewed therefore some relevant journals from the architectural field who are not traditionally indexed in those databases might have been excluded.
Acknowledgements
The authors certify that the submitted manuscript is an original article. Moreover, the authors would like to acknowledge that an extract has been presented at the International Academy for Design & Health 1st European Symposium “Salutogenic Hospital Design & Urban Health – Global Perspectives and Local Identities in Healthcare Architecture”.
Conflict of interest:
Each author declares that he or she has no commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangement etc.) that might pose a conflict of interest in connection with the submitted article
References
- 1.Azzopardi-Muscat N. Twenty years observation of health systems and policies: what has the European observatory meant for public health? European Journal of Public Health. 2018;28(5):787–788. doi: 10.1093/eurpub/cky124. https://doi.org/10.1093/eurpub/cky124 . [DOI] [PubMed] [Google Scholar]
- 2.Capolongo S, Rebecchi A, Dettori M, Appolloni L, Azara A, Buffoli M, Capasso L, Casuccio A, Oliveri Conti G, D’Amico A, et al. Healthy Design and Urban Planning Strategies, Actions, and Policy to Achieve Salutogenic Cities. Int. J. Environ. Res. Public Health. 2018;15:2698. doi: 10.3390/ijerph15122698. doi: 10.3390/ijerph15122698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Capolongo S, Rebecchi A, Brambilla A. E-collection – Urban design and health. European Journal of Public Health. 2019 Available on: https://academic.oup.com/eurpub/pages/urban_design_and_health. / [Last accessed: 2020, January 10] [Google Scholar]
- 4.Marsh R, Pilkington P, Rice L. A guide to architecture for the public health workforce. Public Health. 2020;178:120–123. doi: 10.1016/j.puhe.2019.09.013. [DOI] [PubMed] [Google Scholar]
- 5.Geneva: World Health Organization; 2018. World health statistics 2018: monitoring health for the SDGs, sustainable development goals. Licence: CC BY-NC-SA 3.0 IGO. Available online https://www.who.int/gho/publications/world_health_statistics/2018/EN_WHS2018_TOC.pdf?ua=1. [Last accessed: 2020, January 10] [Google Scholar]
- 6.Foreman KJ, Marquez N, Dolgert A, et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016–40 for 195 countries and territories using data from the Global Burden of Disease Study 2016. The Lancet. 2018;392:2052–90. doi: 10.1016/S0140-6736(18)31694-5. doi: 10.1016/S0140-6736(18)31694-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.CDC Director’s Media Statement on U.S. Life Expectancy Media Statement For Immediate Release: Thursday, November 29, 2018 Centers for Disease Control and Prevention. Available online https://www.cdc.gov/media/releases/2018/s1129-US-life-expectancy.html. [Last accessed: 2020, January 10] [Google Scholar]
- 8.Bloomberg Global Health Index. 2019 Available online https://www.bloomberg.com/news/articles/2019-02-24/spain-tops-italy-as-world-s-healthiest-nation-while-u-s-slips?utm_source=url_link. [Last accessed: 2020, January 10] [Google Scholar]
- 9.Fullman N, Yearwood J, Abay SM, Abbafati C, et al. Measuring performance on the Healthcare Access and Quality Index for 195 countries and territories and selected subnational locations: A systematic analysis from the Global Burden of Disease Study 2016. TheLancet. 2018;391(10136):2236–2271. doi: 10.1016/S0140-6736(18)30994-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Drewnowski A, Buszkiewicz J, Aggarwal A, Rose C, Gupta S, Bradshaw A. Obesity and the Built Environment: A Reappraisal. Obesity. 2020;28(1):22–30. doi: 10.1002/oby.22672. doi: 10.1002/oby.22672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Neira M. WHO Health must be the number one priority for urban planners. 21 March 2018 Available online https://www.who.int/news-room/commentaries/detail/health-must-be-the-number-one-priority-for-urban-planners. [Last accessed: 2020, January 10] [Google Scholar]
- 12.Melis G, Gelormino E, Marra G, Ferracin E, Costa G. The Effects of the Urban Built Environment on Mental Health: A Cohort Study in a Large Northern Italian City. Int. J. Environ. Res. Public Health. 2015;12:14898–14915. doi: 10.3390/ijerph121114898. doi: 10.3390/ijerph121114898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hoisington AJ, Stearns-Yoder KA, Schuldt SJ, Beemer CJ, Maestre JP, Kinney KA, Postolache TT, Lowry CA, Brenner LA. Ten questions concerning the built environment and mental health. Building and Environment. 2019;155:58–69. doi: 10.1016/j.buildenv.2019.03.036. [Google Scholar]
- 14.Talukder S, Capon A, Nath D, Kolb A, Jahan S, Boufford J. Urban health in the post-2015 agenda. Lancet. 2015;385(9970):769. doi: 10.1016/S0140-6736(15)60428-7. doi.org/10.1016/S0140-6736(15)60428-7 [Last accessed: 2020, January 10] [DOI] [PubMed] [Google Scholar]
- 15.New York: United Nations; United Nations, Department of Economic and Social Affairs, Population Division (2019). World Urbanization Prospects: The 2018 Revision (ST/ESA/SER.A/420) Available online https://population.un.org/wup/Publications/Files/WUP2018-Report.pdf . [Google Scholar]
- 16.De La Barra X. Fear of epidemics: The engine of urban planning. Planning Practice and Research. 2000;15(1-2):7–16. [Google Scholar]
- 17.Szreter S. The population health approach in historical perspective, Public Health: Then and Now. American Journal of Public Health. 2003;93(3) doi: 10.2105/ajph.93.3.421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Verderber S. Routledge; 2012. Sprawling Cities and Our Endangered Public Health. ISBN: 978-0-415-66532-2. [Google Scholar]
- 19.Burton A, Bambrick H, Friel S. If you don’t know how can you plan? Considering the health impacts of climate change in urban planning in Australia. Urban Climate. 2015;12:104–118. [Google Scholar]
- 20.Council of the European Union. Council Conclusions on Health in All Policies (HiAP) 2006 Available online https://ec.europa.eu/health/ph_projects/2005/action1/docs/2005_1_18_frep_a8_en.pdf. [Last accessed: 2020, January 10] [Google Scholar]
- 21.Llena-Nozal A, Martin N, Murtin F. The economy of well-being: Creating opportunities for people’s well-being and economic growth. OECD Statistics Working Papers. 2019/02, OECD Publishing, Paris, https://doi.org/10.1787/498e9bc7-en . [Google Scholar]
- 22.Council of the European Union. The Economy of Wellbeing Council Conclusions. 24 October 2019 13432/19. Available online https://data.consilium.europa.eu/doc/document/ST-13432-2019-INIT/en/pdf. [Last accessed: 2020, January 10] [Google Scholar]
- 23.Prior JH, Connon ILC, McIntyre E, Adams J, Capon A, Kent J, Rissel C, Thomas LE, Thompson SM, Westcott H. Built environment interventions for human and planetary health: integrating health in climate change adaptation and mitigation. Public Health Res Pract. 2018;28(4) doi: 10.17061/phrp2841831. [DOI] [PubMed] [Google Scholar]
- 24.Quotidiano Sanità. Grillo sui nuovi ospedali: “Già stanziati 6,6 mld ma ne servono 32 per riqualificarli tutti”. Available at: https://www.quotidianosanita.it/governo-e-parlamento/articolo.php?articolo_id=72550. [Last accessed: 2020, January 10] [Google Scholar]
- 25.World Health Organization. The Thirteenth General Programme of Work, 2019–2023. Available at: https://apps.who.int/iris/bitstream/handle/10665/324775/WHO-PRP-18.1-eng.pdf. [Last accessed: 2020, January 10] [Google Scholar]
- 26.Dubé P. Urban health: An urban planning perspective. Reviews on Environmental Health. 2000;15(1-2):249–265. doi: 10.1515/reveh.2000.15.1-2.249. [DOI] [PubMed] [Google Scholar]
- 27.Galea S, Freudenberg N, Vlahov D. A framework for the study of urban health. In Cities and the Health of the Public. Vanderbilt University Press; 2006. pp. 3–18. [Google Scholar]
- 28.Global Task Force on Cholera Control. Ending Cholera—A Global Roadmap to 2030. 2019 Available online https://www.who.int/cholera/publications/global-roadmap.pdf?ua=1. [Last accessed: 2020, January 10] [Google Scholar]
- 29.Gelting RL, Chapra SC, Nevin PE, Harvey DE, Gute DM. “Back to the Future”: Time for a Renaissance of Public Health Engineering. Int. J. Environ. Res. Public Health. 2019;16:387. doi: 10.3390/ijerph16030387. doi:10.3390/ijerph16030387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Carmichael L, Townshend TG, Fischer TB, Lock K, Petrokofsky C, Sheppard A, Sweeting D, Ogilvie F. Urban planning as an enabler of urban health: Challenges and good practice in England following the 2012 planning and public health reforms. Land Use Policy. 2019;84:154–162. [Google Scholar]
- 31.United Nations. Transforming our world: the 2030 agenda for sustainable development A/RES/70/1. 2015 Available online https://sustainabledevelopment.un.org/content/documents/21252030%20Agenda%20for%20Sustainable%20Development%20web.pdf. [Last accessed: 2020, January 10] [Google Scholar]
- 32.Barton H. A health map for urban planners: Towards a conceptual model for healthy, sustainable settlements. Built Environment. 2005;31(4):339–355. [Google Scholar]
- 33.Muessig A. “How do we design healthy cities for people?”. 2017 Available online http://gehlpeople.com/blog/how-do-we-design-healthy-cities-for-people. / [Last accessed: 2020, January 10] [Google Scholar]
- 34.Younger M, Morrow-Almeida HR, Vindigni SM, Dannenberg AL. The Built Environment, Climate Change, and Health. Opportunities for Co-Benefits. American Journal of Preventive Medicine. 2008;35(5):517–526. doi: 10.1016/j.amepre.2008.08.017. [DOI] [PubMed] [Google Scholar]
- 35.Rice L. The nature and extent of healthy architecture: the current state of progress. Archnet-IJAR. 2019;13(2):244–259. [Google Scholar]
- 36.Kochtitzky CS, Frumkin H, Rodriguez R, Dannenberg AL, Rayman J, Rose K, Gillig R, Kanter T. Urban planning and public health at CDC. MMWR. Morbidity and mortality weekly report. 2006;55(2):34–38. [PubMed] [Google Scholar]
- 37.Pilkington P, Grant M, Orme J. Promoting integration of the health and built environment agendas through a workforce development initiative. Public Health. 2008;122:545–551. doi: 10.1016/j.puhe.2008.03.004. [DOI] [PubMed] [Google Scholar]
- 38.Seidel AD, Kim JT, Tanaka IBR. Architects, urban design, health, and the built environment. Journal of Architectural and Planning Research. 2012;29(3):241–268. [Google Scholar]
- 39.Exner M. Edwin Chadwick and the public health act 1848: Principal architect of sanitary reform in Routledge Handbook of Water and Health. 2015:699–706. [Google Scholar]
- 40.Gorman N, Lackney JA, Rollings K, Huang TT. Designer schools: The role of school space and architecture in obesity prevention. Obesity. 2007;15(11):2521–2530. doi: 10.1038/oby.2007.300. [DOI] [PubMed] [Google Scholar]
- 41.Capolongo S, Lemaire N, Oppio A, Buffoli M, Le Gall AR. Action planning for healthy cities: The role of multi-criteria analysis, developed in Italy and France, for assessing health performances in land-use plans and urban development projects. Epidemiologia e Prevenzione. 2016;40(3-4):257–264. doi: 10.19191/EP16.3-4.P257.093. [DOI] [PubMed] [Google Scholar]
- 42.Brambilla A, Buffoli M, Capolongo S. Measuring hospital qualities. A preliminary investigation on Health Impact Assessment possibilities for evaluating complex buildings. Acta bio-medica: Atenei Parmensis. 2019;90(9S):54–63. doi: 10.23750/abm.v90i9-S.8713. doi: 10.23750/abm.v90i9-S.8713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Anderson DC. Bricks and Morals—Hospital Buildings, Do No Harm. Journal of General Internal Medicine. 2019;34(2):312–316. doi: 10.1007/s11606-018-4707-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Brambilla A, Rebecchi A, Capolongo S. Evidence Based Hospital Design. A literature review of the recent publications about the EBD impact of built environment on hospital occupants’ and organizational outcomes. Ann Ig. 2019;31(2) doi: 10.7416/ai.2019.2269. DOI: 10.7416/ai.2019.2269. [DOI] [PubMed] [Google Scholar]
- 45.Capolongo S, Buffoli M, Brambilla A, Rebecchi A. Healthy Urban Planning & Design Strategies to improve urban quality and attractiveness of places. TECHNE. 2020;19 in press. [Google Scholar]
- 46.European Council meeting 12th December 2019 Conclusion EUCO 29/19. Available onlin: https://www.consilium.europa.eu/media/41783/12-euco-final-conclusions-it.pdf. [Last accessed: 2020, January 10] [Google Scholar]
- 47.Implementation framework for phase VII (2019–2024) of the WHO European Healthy Cities Network: goals, requirements and strategic approaches final. Available online: http://www.euro.who.int/__data/assets/pdf_file/0020/400277/04-FINAL-Phase-VII-implementation-framework_ENG.PDF?ua=1. [Last accessed: 2020, January 10] [Google Scholar]
- 48.Gola M, Signorelli C, Buffoli M, Rebecchi A, Capolongo S. Local health rules and building regulations: a survey on local hygiene and building regulations in italian municiples. Ann. Istituto superiore di sanità. 2017;53(3):223–230. doi: 10.4415/ANN_17_03_08. doi: 10.4415/ANN_17_03_08. [DOI] [PubMed] [Google Scholar]
- 49.Miedema E, Lindahl G, Elf M. Conceptualizing Health Promotion in Relation to Outpatient Healthcare Building Design: A Scoping Review. HERD. 2019 doi: 10.1177/1937586718796651. doi: 10.1177/1937586718796651. [DOI] [PubMed] [Google Scholar]
- 50.Brambilla A, Capolongo S. Healthy and sustainable hospital evaluation-A review of POE tools for hospital assessment in an evidence-based design framework. Buildings. 2019;9(4) doi:10.3390/buildings9040076. [Google Scholar]
- 51.Dannenberg AL, Burpee H. Architecture for Health Is Not Just for Healthcare Architects (Editorial) Health Environments Research and Design Journal. 2018;11(2):8–12. doi: 10.1177/1937586718772955. [DOI] [PubMed] [Google Scholar]
- 52.Kuhlmann E, Batenburg R, Wismar M, et al. A call for action to establish a research agenda for building a future health workforce in Europe. Health Res Policy Sys. 2018 doi: 10.1186/s12961-018-0333-x. doi:10.1186/s12961-018-0333-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Ganske I. A different angle: Physician and architect in Urman RD, Ehrenfeld JM (Eds.) Physicians’ Pathways to Non-Traditional Careers and Leadership Opportunities. 2012 263-271 ISBN: 978-1-4614-0550-4. [Google Scholar]
- 54.Capolongo S, Buffoli M, Mosca EI, Galeone D, D’Elia R, Rebecchi A. Public Health Aspects’ Assessment Tool for Urban Projects, According to the Urban Health Approach in Della Torre S et al. (eds.), Regeneration of the Built Environmentfrom a Circular Economy Perspective, Research for Development. 2020:325–335. doi: 10.1007/978-3-030-33256-3_30325. [Google Scholar]
- 55.Dell’Ovo M, Oppio A. Bringing the Value-Focused Thinking approach to urban development and design processes: the case od Foz do Tua area in Portugal. Valori e Valutazioni. 2019;23:91–106. ISSUN 2036-2404. [Google Scholar]