

Abstract
In Italy, over the last decade, the spread of vaccine hesitancy has caused a steep decrease in vaccination coverage rates, both at the national and regional level. In this study, we pool and critically analyze childhood immunization coverage rates (2011-2018) in Lombardy, Italy’s most populated region, and compare them to national trends. Overall, childhood vaccination coverage in Lombardy is slightly higher the Italian national average. In 2017, the law on mandatory vaccinations came into force, acting as a powerful tool for coverage increase.
Keywords: immunization, vaccines, vaccination coverage, law, obligation, Italy, Lombardy
Introduction
Over the last decade, vaccine hesitancy(1) has imposed itself in Italy as a new, alarming phenomenon(2-4), causing a decline of immunization coverage rates. Vaccine coverage for critical pathogens dropped below the World Health Organization (WHO)-recommended herd immunity threshold(5, 6).
In July 2017, after a previous Governmental Decree-Law (n.73, June 2017)(7), the Italian Parliament approved law No. 119(8), extending free mandatory vaccinations.
The schedule currently includes a total of ten mandatory (poliomyelitis, diphtheria-tetanus-pertussis DTP, measles, mumps, rubella-varicella- MMR-v, Hepatitis B, Haemophilus influenzae type b) and five recommended vaccines (Human Papilloma Virus- HPV, Rotavirus, Pneumococcus, Meningococcal B, Meningococcal ACW135Y).
The law imposed fines on families who refused to comply and gave the basis for turning away unvaccinated children from nurseries and primary schools.
For the first time in Italian legislation, law No. 119 has taken a life-course approach to immunization, to tackle the epidemiological priorities of the National Vaccine Prevention Plan (2017-2019)(9).
The path towards a nationwide Italian immunization registry is still long. A possible roadmap has been devised by D’Ancona et al. (10), while other authors offer a complete overview of Italy’s vaccination data reporting system (11, 12).
A recent national survey elaborates on the detrimental health impact of the Italian economic crisis(13).
The current study addresses unmet research needs. Indeed, to the best of our knowledge, no single paper has performed a complete report and assessment of vaccine coverage trends in Lombardy from 2011 onwards.
A broad literature scan on PubMed and Embase just offered one relevant paper on the subject, featuring Lombardy coverage data for measles and rubella (14).
A second source is the “Regional Vaccine Prevention Plan” (15), a document issued by Lombardy Regional Council in response to the Italian National Plan (9). As a piece of grey literature meant to inform policymakers, it describes regional and Italian-level vaccination coverage data (2000-2016) using graphs only.
Aim of this study is to monitor regional-level coverage data for childhood vaccinations in Lombardy and to assess the overall impact of the post-2017 legislative framework on regional immunization coverage rates.
The analysis was focused on the ten compulsory vaccinations, with a separate discussion of two representative recommended ones. Immunizations against HPV and Rotavirus were deliberately excluded, as the former is often administered in adolescence, and the latter is too recent to allow a meaningful retrospective analysis.
Methods
We collected, analyzed and critically interpreted Lombardy regional-level coverage rates for childhood immunizations (2011-2018) and compared them to Italian national averages.
We reported data for 24-months old children, as this cohort seemed more representative of recent epidemiological trends.
Data on childhood immunizations were retrieved from the Italian Ministry of Health (MoH) yearly reports(16).
Coverages for 2011-2012 were grouped per vaccine (e.g. M-MMR-MMR-v/DT-DTP). All subsequent data (2013-2018) were collected per single antigen.
Immunization coverage rates were expressed as the proportion of immunized subjects by resident target population, in percentage.
Results
Mandatory vaccines
MMR-v quadrivalent vaccine coverage showed an encouraging starting point in 2011 in Lombardy (94,6%), while the Italian data was not as favourable (90,1%). Considering measles as the most critical antigen for this group of immunizations, a constant fall in coverage rates can be noticed after 2011, with lowest coverages below 90%.
Afterwards, rates started an increasing path, which still lasts. In 2018, measles vaccine coverage in Lombardy is still slightly below 2011 (94,16%), while Italy had a better crude improvement (+7,93%; Lombardy +4,67%), but since the starting point was lower, is still lagging. (Figure 1, Tables 1 and 2)
Figure 1.
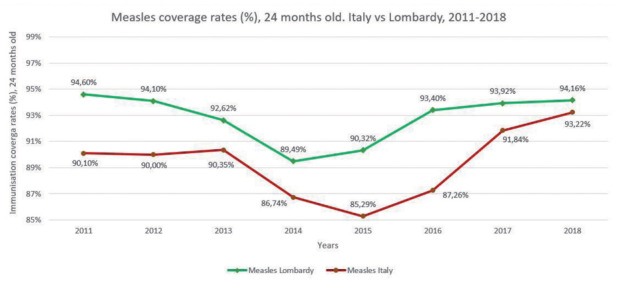
Immunization coverage rates (%) for measles. Twenty-four months old children, Lombardy vs Italy (2011-2018).
Table 1.
Immunization coverage rates (%), per vaccine (2011-2012), per antigen (2013-2018). Lombardy and Italy. Twenty-four months old children.
| Antigen/vaccine | Years | ||||||||
| 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | ||
| MMR-MMRV° | L | 93,9 | 94,0 | n/a | |||||
| I | 89,9 | 89,2 | |||||||
| M-MMR-MMRV° | L | 94,6 | 94,1 | ||||||
| I | 90,1 | 90,0 | |||||||
| Measles° | L | n/a 90,3 |
92,6 | 89,5 | 90,3 | 93,4 | 93,9 | 94,2 | |
| I | 86,7 | 85,3 | 97,3 | 91,8 | 93,2 | ||||
| Mumps° | L | n/a 90,3 |
92,6 | 89,4 | 90,2 | 93,3 | 93,8 | 94,1 | |
| I | 86,7 | 85,2 | 87,2 | 91,8 | 93,2 | ||||
| Rubella° | L | n/a 90,3 |
92,6 | 89,4 | 90,2 | 93,3 | 93,9 | 94,1 | |
| I | 86,7 | 85,2 | 87,2 | 91,8 | 93,2 | ||||
| Chickenpox/Varicella° | L | n/a 33,2 |
0,00 | - | 0,83 | - | 1,85 | 73,0 | |
| I | 36,6 | 30,7 | 46,0 | 45,6 | 74,2 | ||||
| DTP° | L | 96,9 | 96,5 | n/a | |||||
| I | 95,8 | 96,0 | |||||||
| DT-DTP° | L | 97,1 | 96,7 | ||||||
| I | 96,3 | 96,2 | |||||||
| Diphteria° | L | n/a 95,7 |
95,9 | 95,0 | 93,4 | 94,2 | 95,0 | 95,2 | |
| I | 94,7 | 93,3 | 93,6 | 94,6 | 95,1 | ||||
| Tetanus° | L | n/a 95,8 |
95,9 | 95,1 | 93,6 | 94,4 | 95,2 | 95,3 | |
| I | 94,8 | 93,6 | 93,7 | 94,7 | 95,1 | ||||
| Pertussis° | L | n/a 95,7 |
95,8 | 94,8 | 93,4 | 94,2 | 95,0 | 95,2 | |
| I | 94,6 | 93,3 | 93,5 | 94,6 | 95,1 | ||||
| Polio° | L | 97,0 | 96,7 | 95,9 | 95,0 | 93,5 | 92,8 | 94,9 | 95,3 |
| I | 96,1 | 96,1 | 95,7 | 94,7 | 93,4 | 93,3 | 94,6 | 95,1 | |
| Hep B° | L | 96,2 | 96,5 | 95,8 | 94,9 | 93,2 | 91,8 | 94,6 | 95,1 |
| I | 96,0 | 96,0 | 95,6 | 94,6 | 93,2 | 93,0 | 94,4 | 94,9 | |
| Hib° | L | 95,9 | 95,2 | 95,2 | 94,3 | 92,9 | 92,9 | 94,3 | 95,0 |
| I | 95,6 | 94,8 | 94,9 | 94,3 | 93,0 | 93,0 | 94,3 | 94,3 | |
| Pneumo* | L | - 86,9 |
83,7 | 79,4 | 86,8 | 85,7 | 92,5 | 92,8 | |
| I | 87,5 | 88,7 | 88,3 | 90,9 | 91,9 | ||||
| Men C* | L | - 77,0 |
69,1 | 79,4 | 85,8 | 88,2 | 92,2 | 92,4 | |
| I | 73,9 | 76,6 | 80,7 | 82,6 | 84,9 | ||||
Table 2.
Percentage increase in immunization coverage rates. Minimal 2011-2017 coverage vs 2018 coverage (%). Lombardy and Italy.
| Vaccine | Lombardy/Italy | Minimal coverage (year) | 2018 coverage | Increase# |
| Measles-containing vaccines | L | 89,5 (2014) | 94,1 | +4,7% |
| I | 85,3 (2015) | 93,2 | +7,9% | |
| Polio-containing vaccines | L | 92,8 (2016) | 95,3 | +2,5% |
| I | 93,3 (2016) | 95,1 | +1,8% | |
| Pneumococcal Conjugate | L | 79,4 (2014) | 92,8 | +13,4% |
| I | 86,9 (2013) | 91,9 | +4,9% | |
| Meningococcal C Conjugate | L | 69,1 (2013) | 92,4 | +23,3% |
| I | 73,9 (2014) | 84,9 | +11,0% |
Notes to tables: L = Lombardy region; I = Italy; DTP = Diphtheria-Tetanus-Pertussis; Hep B = Hepatitis B; Hib = Haemophilus influenzae type b; Pneumo = Pneumococcal Conjugate; Men C = Meningococcal C Conjugate; MMR-v = measles, mumps, rubella, chickenpox; Polio = poliomyelitis; ° = mandatory under Law No. 119/2017; * = Recommended under Law No. 119/2017; n/a = not applicable (different data collection); - = missing data; # = 2018 coverage minus minimal coverage.
Data paucity about the newly-introduced varicella vaccination impedes formulation of any substantial trend analysis. Nevertheless, 2018 coverage is <75% (Table 1).
As for diphtheria-tetanus-pertussis (DTP) vaccine, 2011 data were optimal both in Lombardy (97,1%) and Italy (96,3%). In the following years, rates have declined, though always stably above 90%, with lowest values in 2015 and excellent recovery after 2017 (>95% in 2018, Table 1). Nevertheless, 2011 levels are yet to be reached.
Hepatitis B (Hep B) and Haemophilus influenzae type b (Hib) experienced a similar trend (Table 1). Of note, in 2018, Italy had average rates slightly below 95% for both antigens, while Lombardy is slightly above the threshold.
Recommended vaccines:
Data availability is restricted to 2013 - 2018.
Anti-pneumococcal vaccine coverage has been fluctuating in the course of the observation period, the lower point being 2013 (Table 1).
In Lombardy, meningococcal C vaccination coverage has been continuously rising from 2013 to 2018.
Representative antigens:
We report immunization coverage rates for Measles (Figure 1) and Poliomyelitis (Figure 2) as vicarious antigens for the quadrivalent (MMR-v) and the hexavalent (IPV-DTP-HepB-Hib) vaccinations, respectively.
Figure 2.
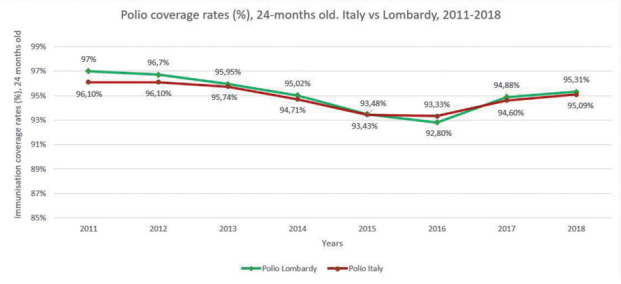
Immunization coverage rates (%) for poliomyelitis. Twenty-four months old children, Lombardy vs Italy (2011-2018).
Both in Lombardy and Italy, a sharp decrease took place in coverages for measles immunization, especially in 2014-2015.
For polio, vaccination uptake in Lombardy and Italy are almost identical, with 2018 data both above 95%. A seroprevalence study of poliomyelitis in a vulnerable Northern Italy cohort is described by Veronesi et al. (17).
Altogether, Lombardy and Italy experienced a mildly comforting rise in measles and polio coverage. In Lombardy alone, an improvement can be seen in pneumococcal and meningococcal C.
Table 2 illustrates all increments across the study period.
Conclusions
Lombardy is Italy’s most prosperous and most populated region and displays a peculiar healthcare organization (18, 19). Overall, childhood vaccination coverage in Lombardy is slightly higher than the Italian national average.
Lowest coverage was seen in 2014-2015, roughly the same time of vaccine hesitancy’s maximal spread. Hesitancy is an international phenomenon, massively fuelled in Italy by a mixture of ideological fervour, mass media clamour, and pseudoscientific popular culture(20, 21).
In 2017, the law on mandatory vaccinations came into force, acting as a powerful tool for coverage increase – as the data show. Policy evaluation of the law’s implementation efforts goes beyond this article’s scope and can be retrieved in a recent Eurosurveillance paper(22).
The main antigen-specific findings of this study concerned the rising coverage trends of meningococcal C and pneumococcal conjugate vaccine in Lombardy (Table 2).
A recent small number of invasive meningococcal disease outbreaks in Centre-Northern Italy, which claimed conspicuous media attention(23), could be a partial explanation of the former finding. At the same time, we have no substantial hypothesis for the latter.
Different disease risk perceptions could play a role in the coverage disparity between MMR and the hexavalent vaccine (3, 24).
Exploring Lombardy’s response to the national legislation could enable clinicians to gain a better understanding of the local epidemiological context. Furthermore, it could guide policymakers to develop tailored vaccination strategies.
Both regional and national immunization strategies should aim at reaching and maintaining optimal targets (≥ 95%) for all the vaccines included in the National Vaccine Prevention Plan 2017-2019 in all future newborn cohorts (25, 26). Conveying useful and persuasive information about vaccines is a shared duty of all healthcare personnel, and the entire scientific world (27, 28).
Stronger actions are urgently needed to fight vaccine hesitancy – a costly, and entirely avoidable, public health threat.
Conflict of interest:
Each author declares that he or she has no commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangement etc.) that might pose a conflict of interest in connection with the submitted article
References
- 1.MacDonald NE. Vaccine hesitancy: Definition, scope and determinants. Vaccine. 2015;33(34):4161. doi: 10.1016/j.vaccine.2015.04.036. [DOI] [PubMed] [Google Scholar]
- 2.Gualano MR, Bert F, Voglino G, et al. Attitudes towards compulsory vaccination in Italy: Results from the NAVIDAD multicentre study. Vaccine. 2018;36(23):3368–74. doi: 10.1016/j.vaccine.2018.04.029. [DOI] [PubMed] [Google Scholar]
- 3.Giambi C, Fabiani M, D’Ancona F, et al. Parental vaccine hesitancy in Italy - Results from a national survey. Vaccine. 2018;36(6):779–87. doi: 10.1016/j.vaccine.2017.12.074. [DOI] [PubMed] [Google Scholar]
- 4.Vaccine hesitancy: a generation at risk. Lancet Child & Adolescent Health. 2019;3(5):281. doi: 10.1016/S2352-4642(19)30092-6. [DOI] [PubMed] [Google Scholar]
- 5.Fine P, Eames K, Heymann DL. “Herd immunity”: a rough guide. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America. 2011;52(7):911–6. doi: 10.1093/cid/cir007. [DOI] [PubMed] [Google Scholar]
- 6.World Health Organization. Global measles and rubella strategic plan: 2012-2020. 2012 [Google Scholar]
- 7.Decreto-Legge 7 giugno 2017, n.73, “Disposizioni urgenti in materia di prevenzione vaccinale” [Google Scholar]
- 8.Legge 31 luglio 2017, n. 119. “Conversione in legge, con modificazioni, del decreto-legge 7 giugno 2017, n. 73, recante disposizioni urgenti in materia di prevenzione vaccinale.” [Google Scholar]
- 9.Ministero della Salute. Piano nazionale prevenzione vaccinale 2017–2019. [Available from: http://www . salute. gov. it/imgs/C_17_pubblicazioni_2571_allegato. pdf.] [Google Scholar]
- 10.D’Ancona F, Gianfredi V, Riccardo F, et al. Immunisation Registries at regional level in Italy and the roadmap for a future Italian National Registry. Ann Ig. 2018;30(2):77–85. doi: 10.7416/ai.2018.2199. [DOI] [PubMed] [Google Scholar]
- 11.Signorelli C, Odone A, Cella P, et al. Childhood vaccine coverage in Italy after the new law on mandatory immunization. Annali di igiene: medicina preventiva e di comunita. 2018;30(4 Supple 1):1–10. doi: 10.7416/ai.2018.2227. [DOI] [PubMed] [Google Scholar]
- 12.Signorelli C, Odone A, Cella P, et al. Infant immunization coverage in Italy (2000-2016) Annali dell’Istituto superiore di sanita. 2017;53(3):231–7. doi: 10.4415/ANN_17_03_09. [DOI] [PubMed] [Google Scholar]
- 13.Odone A, Landriscina T, Amerio A, et al. The impact of the current economic crisis on mental health in Italy: evidence from two representative national surveys. The European Journal of Public Health. 2018;28(3):490–5. doi: 10.1093/eurpub/ckx220. [DOI] [PubMed] [Google Scholar]
- 14.Amendola A, Bubba L, Piralla A, et al. Surveillance and vaccination coverage of measles and rubella in Northern Italy. Human vaccines & immunotherapeutics. 2015;11(1):206. doi: 10.4161/hv.35865. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Giunta Regionale Lombardia, Deliberazione n° X/7629 Determinazione in ordine alle vaccinazioni dell’età infantile e dell’adulto in Regione Lombardia: aggiornamenti alla luce del Piano Nazionale Prevenzione Vaccinale 2017-2019 [Google Scholar]
- 16.Ministero della Salute. Vaccinazioni dell’età pediatrica e dell’adolescente - Coperture vaccinali. [Available from: http://www.salute.gov.it/portale/documentazione/p6_2_8_3_1.jsp?lingua=italiano&id=20 .] [Google Scholar]
- 17.Veronesi L, Affanni P, Verrotti di Pianella C, et al. Immunity status against poliomyelitis in childbearing women in a province of northern Italy. A cross-sectional analysis. Ann Ig. 2013;25(5):427–33. doi: 10.7416/ai.2013.1944. [DOI] [PubMed] [Google Scholar]
- 18.European C. Statistical Office of the European U. Eurostat regional yearbook: 2019 edition. 2019. [Available from: http://publications.europa.eu/publication/manifestation_identifier/PUB_KSHA19001ENN . [Google Scholar]
- 19.Ferre F, de Belvis AG, Valerio L, et al. Italy: health system review. Health systems in transition. 2014;16(4):1–168. [PubMed] [Google Scholar]
- 20.Petrelli F, Contratti CM, Tanzi E, et al. Vaccine hesitancy, a public health problem. Ann Ig. 2018;30(2):86–103. doi: 10.7416/ai.2018.2200. [DOI] [PubMed] [Google Scholar]
- 21.Odone A, Signorelli C. When vaccine hesitancy makes headlines. Vaccine. 2017;35(9):1209–10. doi: 10.1016/j.vaccine.2015.11.051. [DOI] [PubMed] [Google Scholar]
- 22.D’Ancona F, D’Amario C, Maraglino F, et al. The law on compulsory vaccination in Italy: an update 2 years after the introduction. Euro surveillance: bulletin Europeen sur les maladies transmissibles = European communicable disease bulletin. 2019;24(26) doi: 10.2807/1560-7917.ES.2019.24.26.1900371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Covolo L, Croce E, Moneda M, et al. Meningococcal disease in Italy: public concern, media coverage and policy change. BMC public health. 2019;19(1):1061. doi: 10.1186/s12889-019-7426-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Allan N, Harden J. Parental decision-making in uptake of the MMR vaccination: a systematic review of qualitative literature. Journal of public health. 2015;37(4):678–87. doi: 10.1093/pubmed/fdu075. [DOI] [PubMed] [Google Scholar]
- 25.Signorelli C, Odone A, Ricciardi W, et al. The social responsibility of public health: Italy’s lesson on vaccine hesitancy. Eur J Public Health. 2019;29(6):1003–4. doi: 10.1093/eurpub/ckz135. [DOI] [PubMed] [Google Scholar]
- 26.Burioni R, Odone A, Signorelli C. Lessons from Italy’s policy shift on immunization. Nature. 2018;555(7694):30. doi: 10.1038/d41586-018-02267-9. [DOI] [PubMed] [Google Scholar]
- 27.Biasio LR, Corsello G, Costantino C, et al. Communication about vaccination: A shared responsibility. Hum Vaccin Immunother. 2016;12(11):2984–7. doi: 10.1080/21645515.2016.1198456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rossi D, Bizzarro A, Affanni P, et al. The educational background of the Top Managers of the Italian Health Authorities: Results of a study on eight Regions. Acta Biomedica. 2019;90(9S):87–91. doi: 10.23750/abm.v90i9-S.8731. [DOI] [PMC free article] [PubMed] [Google Scholar]