

Abstract
Background and aim of the work:
In response to the alarming reduction of vaccination coverage rates, Italian Ministry of Health approved the law number 119/2017, which has extended the number of mandatory vaccinations, for school attendance, from four to ten. The present study aims to evaluate accesses to the vaccination services of the Palermo Local Health Unit (LHU) and the variation of the vaccination coverage rates for hexavalent and measles, mumps, rubella and varicella (MMRV) vaccines, after the implementation of the law 119/2017.
Methods:
An extent of opening hours and an involvement of other health-care professionals in the vaccination services of the Palermo LHU have been adopted to manage the excess of accesses after the introduction of 119/2017 law and to limit the discomfort of general population. Vaccination accesses and coverage rates were calculated from the electronic immunization registers.
Results:
An overall increase of about 15% of single vaccination accesses was observed in the three semester after the introduction of the law in the LHU of Palermo. A peak of 35,516 accesses was observed during the second semester of 2017 (+ 30% compared to the same semesters of 2016 and 2018). From 2016 to 2018, coverage rates for full hexavalent cycle and first dose of MMRV, at 24 and 36 months, and for full MMRV cycle and fourth dose of diphtheria, tetanus, pertussis, poliomyelitis (DTPa+IPV), among 6 years old children, showed considerable increases.
Conclusions:
Law 199/2017 demonstrated a high efficacy in increase vaccination coverage rates also in Sicily. The synergy established between the LHU and the University of Palermo allowed an excellent management of the accesses to vaccination services, making it possible to respond to the public health needs of the general population.
Keywords: vaccination coverage, immunization programs, vaccination policies, mandatory vaccination, National Immunization Plan
Introduction
Vaccination is the most effective and efficient preventive measure for the control, elimination or eradication of several infectious diseases (1).
The Italian National Immunization Plan (NIP) 2017-2019 identified, within the National Health System, vaccines that are offered actively and free of charge to at risk populations (2). Despite this, similarly to other European countries, Italian health-care professionals had to face the re-emerging phenomenon of the vaccine hesitancy, that contributed to alarming decreasing trends in childhood vaccination coverage (3). Recently, the general positive attitude of the population to vaccination has been undermined by “fake” news easily spread on the internet and social media, reports on suspected side effects after vaccination, increase of anti-vaccination movements actions (4 - 6).
The decrease of vaccination coverage rates led to a resurgence of vaccine preventable diseases. In particular, a significant increase of measles cases recorded in Italy from 1 January 2017 to 31 December 2018 was observed, with 7,854 cases notified by Italian Ministry of Health (7).
Of note, Sicilian Health Department reported 1,111 cases of measles in 2018 (44% of the total Italian cases), making Sicily the administrative Italian region with the highest incidence (222 cases per million inhabitants) (8).
In response to the alarming reduction of vaccination coverage rates, Italian Ministry of Health approved in July 2017 the law number 119, which has extended the number of mandatory vaccinations, for school attendance, from four to ten (9).
In particular, vaccination against poliomyelitis, diphtheria, tetanus, pertussis, hepatitis B, Haemophilus influenzae type B disease, measles, mumps, rubella and varicella (chicken-pox) became compulsory for kindergarten attendance (9).
For children and adolescents attending primary and secondary schools (6-16 years), monetary fines for families of unvaccinated children were imposed (9).
In order to further improve vaccination adherence among school-age children and other at-risk categories, the Sicilian Health Department has issued two directives, mainly focused on health-care professionals and staff, in order to make uniform both the vaccination offer and the application of the law n.119/2017 (10, 11).
After the adoption of the law, a significant raise of catch-up appointments and accesses to vaccination services were observed for mandatory but also for recommended vaccination (such as meningococcal and pneumococcal vaccination) (12). Several extraordinary measures have been therefore adopted by the LHU of Palermo, to manage the accesses to vaccination services and to limit the discomfort of general population and the increase in the workload of healthcare workers (HCWs) (10).
Specifically, an extent of vaccination services’ opening hours (on late afternoon and on Saturday) was accompanied by an involvement of other health-care professionals working in the continuity care services, such as general practitioners (GPs) and family pediatricians (FPs) trainees (11).
Moreover, a collaboration between the LHU of Palermo and the Hygiene and Preventive Medicine post-graduate medical school of the University of Palermo was launched, with a direct contribution of medical residents in the activities of vaccination services.
The aim of the study was to evaluate the accesses to the vaccination services of the Palermo Local Health Unit, during the three semesters before and after the implementation of the national law 119/2017, with a particular focus on the variation of the vaccination coverage rates for hexavalent (diphtheria, tetanus, pertussis, poliomyelitis, hepatitis b, Haemophilus influenza type b) and MMRV (measles, mumps, rubella and varicella) vaccines.
Material and Methods
Sicily is the fourth most populous Italian administrative Region, with 4,999,891 inhabitants (13). The Region is divided into 9 Local Health Units (LHUs), one for each Province: Agrigento, Caltanissetta, Catania, Enna, Messina, Palermo, Ragusa, Siracusa and Trapani. In particular, the Province of Palermo, accounting for 1,252,588 inhabitants resident in 82 municipalities including three minor islands, is the most populous (13). The Local health Unit of Palermo consists of 10 Sanitary District and 65 vaccination services.
The Territorial Unit of Public Health, Epidemiology and Preventive Medicine of the Local Health Unit of Palermo, throughout electronic immunization registers available in every vaccination service, collected data on vaccination coverage rates, included in the Regional vaccination schedule.
Data collected by single Sicilian LHUs were annually recorded into a digital Regional immunization registry and, within February 28th of the following year were checked, verified and sent by the Regional Health Department in aggregate form to the Ministry of Health, to estimate the national vaccination coverage (14).
A descriptive analysis of the accesses to vaccination services in the three semesters before (from 1st of January 2016 to 30th of June 2017) and after (from 1st of July 2017 to of 31st December 2018) the implementation of the law 119/2017, and the corresponding percentage increase, were performed.
Moreover, vaccination coverage rates over the last three years (2016, 2017, 2018) were analyzed using crude rates at 24 and 36 months (for full vaccination cycle of hexavalent and first dose of MMRV) and at 6 years of age (for fourth dose of diphtheria, tetanus, pertussis, poliomyelitis - DTPa + IPV - and full vaccination cycle of MMRV).
All data were collected in a database using software EpiInfo 3.5.1 (Epi Info™, CDC, Atlanta) and were analyzed using statistical software package STATA v14.2 (StataCorp LP, College Station, TX, USA).
Results
In table 1, the total number of accesses to vaccination services of the Palermo LHU, in the three semesters before and after the introduction of law 119/2017, are showed. In particular, before the introduction of the law from the 1st of January 2016 to the 30th of June 2017, 76,165 accesses were registered, while from the 1st of July 2017 to the 31st of December 2018 an overall increase of about 15% of single vaccination accesses (n=89,442) was observed.
Table 1.
Accesses to vaccination services of the Palermo LHU, in the three semesters before and after the introduction of the law 119/2017
| Before law 119/2017 introduction (from 1st of July 2017 to 31st of December 2018) | After law 119/2017 introduction (from 1st of January 2016 to 30th of June 2017) | Overall single accesses percentage change (%) | ||||
| Observation period | Number of single accesses | Overall single accesses | Observation period | Number of single accesses | Overall single accesses | |
| 1st semester 2016 | 23,591 | 76,165 | 2nd semester 2017 | 35,516 | 89,442 | +14.8 |
| 2nd semester 2016 | 24,833 | 1st semester 2018 | 29,578 | |||
| 1st semester 2017 | 27,741 | 2nd semester 2018 | 24,348 | |||
In particular, a peak of 35,516 single accesses to the vaccination services was observed during the second semester of 2017 (+ 30% compared to the same semesters of 2016 and 2018). Also during the first semester of 2018 an increase of accesses was observed (n=29,578) in comparison with first semesters of 2016 (n=23,591; +20%) and of 2017 (n=27,741; +7%).
In figure 1 and 2 coverage rates from 2016 to 2018 for full hexavalent vaccination cycle and for the first dose of MMRV observed in the LHU of Palermo, were reported by the birth cohorts at 24 and 36 months.
Figure 1.
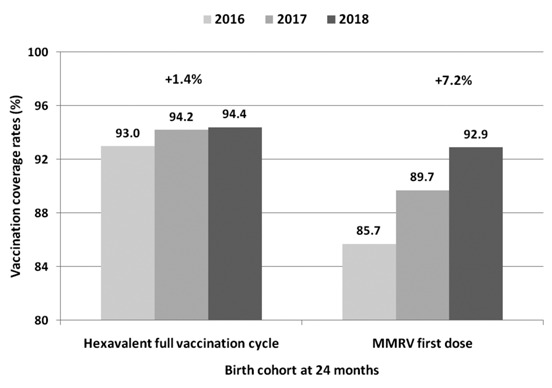
Vaccination coverage rates for hexavalent full vaccination cycle and first dose of MMRV, among 24 months children of the Palermo LHU.
Figure 2.
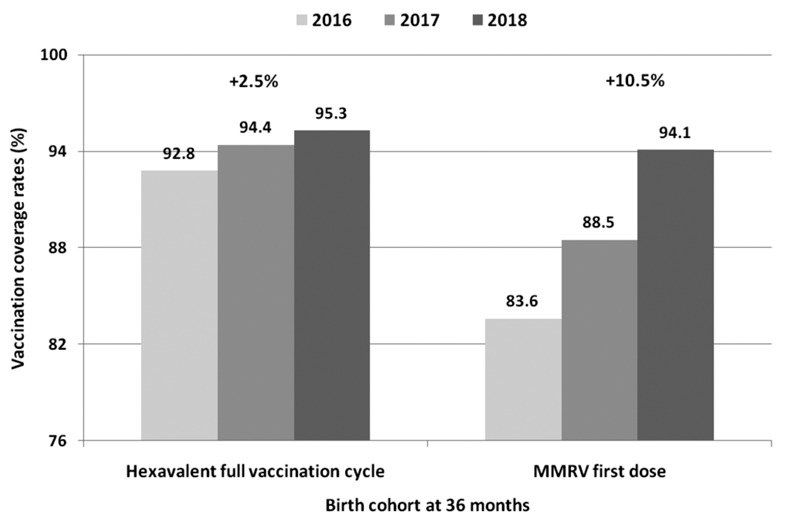
Vaccination coverage rates for hexavalent full vaccination cycle and first dose of MMRV, from 2016 to 2018, among 36 months children of the Palermo LHU.
Full cycle hexavalent coverage rates showed an increase of 1.4% and 2.5% at 24 and 36 months respectively, from 2016 to 2018. Moreover, in the same period, a 7.2% and a 10.5% increase of adherence to first dose of MMRV were observed at 24 and 36 months, respectively.
Finally, as reported in figure 3, vaccination coverage rates for full vaccination cycle of MMRV in the Palermo LHU, among 6 years old children, showed an increase from 61% to 89.7% (+28.7%) from 2016 to 2018.
Figure 3.
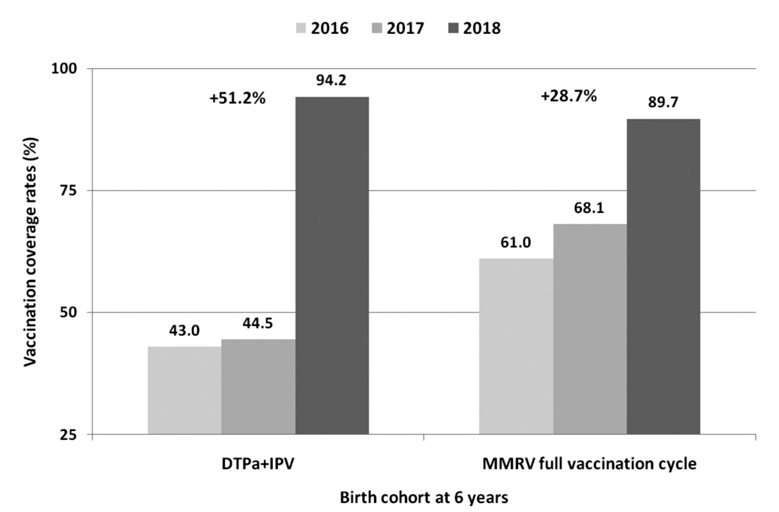
Vaccination coverage rates for fourth dose of DTPa+IPV and full vaccination cycle of MMRV, from 2016 to 2018, among 6 years old children of the Palermo LHU.
Moreover, in the same time interval, a considerable increase of vaccination coverage rates for the 4th dose of DTPa+IPV at 6 years of age was observed (from 43% to 94.2%; +51.2%).
Discussion
In Italy, all vaccinations recommended in the National Immunization Plan are actively and freely offered to general population and are usually administered by vaccination services (2).
Moreover, all these vaccines is considered part of the so-called “minimum level of healthcare services” that the Italian regional public health authorities must provide to citizens free of charge (2).
Nevertheless, the debate about vaccine efficacy and safety, occurred in the last decade at national and international levels, caused a reduction of vaccination coverage rates and a consequent reemergence of outbreaks due to vaccine preventable diseases (8, 15, 16).
For all these reasons, the Italian Ministry of Health, after expressing concerns about increasing numbers of parents refusing to vaccinate their children, introduced the law 119 for compulsory vaccination of all children against ten vaccine-preventable diseases in case of kindergarten attendance (17).
Similarly to Italy, also France and other non-European Countries recently opted for mandatory childhood vaccination (18, 19).
On the other hand, Greece Ministry of Health, in the same period (end of May 2017), proposed that all parents could choose if vaccinated their children, moving from a paternalist to a more free approach to infant vaccination (20).
The law 119/2017 showed a rapid increase of vaccination coverage not only for mandatory vaccines, but also for those recommended among Italian children (21).
Also in the LHU of Palermo, an increase of more than 13 thousands single access to vaccination services was observed during the three semesters after the implementation of the law 119/2017, with a peak in the second semester of 2017, concomitantly with the beginning of the first school year (in September 2017) with a vaccination mandate for attendance of school age children.
To manage the excess of workload of each vaccination services of the Palermo LHU, an organizational effort involving Academic and Territorial Public Health Authorities was carried out.
The extension of the opening days (on saturday morning) and hours (on the late afternoon) has made it possible to better support the increase of vaccination accesses reducing waiting times for general population.
Because of the increase activity of vaccination centers, vaccination coverage rates at 24 months, 36 months and at 6 years of age, for all the vaccines involved in the law 119/2017, have risen.
A greater increase was observed for MMRV vaccination coverage rates in any birth cohort analyzed, similarly to what observed in Emilia-Romagna Region (22).
Before the introduction of the law 119, the MMRV vaccination was affected by a considerable coverage rates reduction from 2012 to 2017 (16).
In particular, in Italy coverage rates have been decreasing since 15 March 2012, in correspondence with the Rimini Court judgment that supported, extensively sustained by mass media, the possible association between vaccine and autism (23).
The Rimini sentence was overturned only three years later by the Bologna Appeal Court, allowing to no-vax movements and their correlated web and social media pages to increase mistrust and fear into general population during this period (24, 25).
In general, among European parents, several factors such as misleading knowledge, beliefs and perceptions on MMRV vaccine and a limited knowledge of HCWs on this vaccination were significantly associated with lower vaccination uptake rates (26, 27).
The involvement of general practitioner, pediatricians trainees and of medical residents in Preventive Medicine in the strategies adopted to manage the emergency, could lead to a more conscious and proactive adherence to immunization campaigns of future health-care professionals, in order to contrast the phenomenon of vaccine hesitancy (28).
Furthermore, the implementation or the strengthening of National and Regional immunization registries should be ensured in order to allow an updated monitoring of vaccination coverage and to quickly organize vaccination strategies tailored to areas or at risk groups.
Specifically, among children of 6 years of age, low vaccination coverage rates were observed for the fourth dose of DTPa + IPV (below 45%) and for the full MMRV cycle (below 70%).
After the introduction of the 119/2017 law, probably supported by the introduction of monetary fines for families of unvaccinated children at primary school, a considerable increase of vaccination coverage for these two vaccination booster was observed.
In future, although the Italian law on mandatory vaccination demonstrated high efficacy, tailored communicative strategies should be promoted by Public Health Authorities, in order to educate general population in a more conscious adherence to vaccinations (29 - 31).
Preventive Medicine issues suffering for ineffective communication or influential interactions with health care providers (32). In Italy other 5 vaccines were strongly recommended and freely offer to general population under 18 years old and, without a strong physician’s recommendation that represent a major significant predictor for vaccination adherence, these vaccinations may not reach the minimum level of coverage rates requested by National Immunization Plan (2, 30). This topic could play a role in a lower adherence to vaccinations in particular among the more vulnerable segments of the population, such as Sicilian population with low socio-economic level and particular cultural characteristics (27, 33).
In conclusion, law 199/2017 demonstrated a high efficacy in increase vaccination coverage rates also in Sicily. The synergy established between the LHU and the University of Palermo allowed an adequate management of the accesses to vaccination services, making it possible to respond effectively to the public health needs of the general population.
Conflict of interest:
Each author declares that he or she has no commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangement etc.) that might pose a conflict of interest in connection with the submitted article
References
- 1.World Health Organization. Regional Office for Europe. European Region Vaccine Action Plan 2015-2020. Available online: http://www.euro.who.int/__data/assets/pdf_file/0007/255679/WHO_EVAP_UK_v30_WEBx.pdf?ua=1. (last accessed on 07 January 2020) [Google Scholar]
- 2.Ministry of Health. National Vaccination Plan 2017-2019. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2571_allegato.pdf. (last accessed on 07 January 2020) [Google Scholar]
- 3.Signorelli C, Odone A, Cella P, et al. Infant immunization coverage in Italy (2000-2016) Ann Ist Super Sanita. 2017;53(3):231–237. doi: 10.4415/ANN_17_03_09. [DOI] [PubMed] [Google Scholar]
- 4.Stahl JP, Cohen R, Denis F, et al. The impact of the web and social networks on vaccination. New challenges and opportunities offered to fight against vaccine hesitancy. Med Mal Infect. 2016;46(3):117–22. doi: 10.1016/j.medmal.2016.02.002. [DOI] [PubMed] [Google Scholar]
- 5.Costantino C, Restivo V, Ventura G, et al. Increased Vaccination Coverage among Adolescents and Young Adults in the District of Palermo as a Result of a Public Health Strategy to Counteract an ‘Epidemic Panic’. Int J Environ Res Public Health. 2018;15(5) doi: 10.3390/ijerph15051014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Signorelli C, Odone A, Conversano M, et al. Deaths after Fluad flu vaccine and the epidemic of panic in Italy. BMJ. 2015;350:h116. doi: 10.1136/bmj.h116. [DOI] [PubMed] [Google Scholar]
- 7.Andrianou XD, Del Manso M, Bella A, et al. Spatiotemporal distribution and determinants of measles incidence during a large outbreak, Italy, September 2016 to July 2018. Euro Surveill. 2019;24(17) doi: 10.2807/1560-7917.ES.2019.24.17.1800679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Epicentro - Istituto Superiore di Sanità. Morbillo&Rosolia News Gennaio. 2019 Available online: https://www.epicentro.iss.it/morbillo/bollettino/RM_News_2018_48%20def.pdf. (last accessed on 07 January 2020) [Google Scholar]
- 9. Legge 31 luglio 2017, n. 119. Conversione in legge, con modificazioni, del decreto-legge 7 giugno 2017, n. 73, recante disposizioni urgenti in materia di prevenzione vaccinale. (17G00132). GU Serie Generale n. 182 del 05-08-2017. Available online: http://www.gazzettaufficiale.it/eli/id/2017/08/5/17G00132/sg. (last accessed on 07 January 2020) [Google Scholar]
- 10.Assessorato della Salute-Regione Sicilia. Disposizioni Operative Emergenza Morbillo. Direttiva Protocollo del Servizio 4 n. 29454 del 12.04.2018. Available online: https://www.vaccinarsinsicilia.org/assets/uploads/files/nota-assessorato-morbillo.pdf. (last accessed on 07 January 2020) [Google Scholar]
- 11.Assessorato della Salute-Regione Sicilia. Disposizioni Operative Vaccini per l’anno scolastico 2018-2019. Protocollo del Servizio 4 n. 6542 del 05.09.2018. Available online: https://www.usr.sicilia.it/attachments/article/2295/Nota%20prot.%20n.%2065482%20del%205%20settembre%202018.pdf. (last accessed on 07 January 2020) [Google Scholar]
- 12.Signorelli C, Odone A, Cella P, et al. Childhood vaccine coverage in Italy after the new law on mandatory immunization. Ann Ig. 2018;30 (Suppl. 1):1–10. doi: 10.7416/ai.2018.2227. [DOI] [PubMed] [Google Scholar]
- 13. DemoIstat. Available online: http://demo.istat.it/pop2019/index.html. (last accessed on 07 January 2020) [Google Scholar]
- 14.D’Ancona F, Gianfredi V, Riccardo F, et al. Immunisation Registries at regional level in Italy and the roadmap for a future Italian National Registry. Ann Ig. 2018;30(2):77–85. doi: 10.7416/ai.2018.2199. [DOI] [PubMed] [Google Scholar]
- 15.Gowda C, Dempsey AF. The rise (and fall?) of parental vaccine hesitancy. Hum Vaccin Immunother. 2013;9(8):1755–1762. doi: 10.4161/hv.25085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bonanni P, Ferro A, Guerra R, et al. Vaccine coverage in Italy and assess-ment of the 2012-2014 National Immunization Prevention Plan. Epidemiol Prev. 2015;39(4 Suppl 1):146–158. [PubMed] [Google Scholar]
- 17.Signorelli C, Iannazzo S, Odone A. The imperative of vaccination put into practice. Lancet Infect Dis. 2018 Jan;18(1):26–27. doi: 10.1016/S1473-3099(17)30696-5. [DOI] [PubMed] [Google Scholar]
- 18.Ward JK, Colgrove J, Verger P. Why France is making eight new vaccines mandatory. Vaccine. 2018;36(14):1801–1803. doi: 10.1016/j.vaccine.2018.02.095. [DOI] [PubMed] [Google Scholar]
- 19.MacDonald NE, Harmon S, Dube E, et al. Mandatory infant & childhood immunization: Rationales, issues and knowledge gaps. Vaccine. 2018;36(39):5811–5818. doi: 10.1016/j.vaccine.2018.08.042. [DOI] [PubMed] [Google Scholar]
- 20.Kennedy J, Michailidou D. Divergent policy responses to increasing vaccine scepticism in southern Europe. Lancet Infect Dis. 2017;17(9):900. doi: 10.1016/S1473-3099(17)30456-5. [DOI] [PubMed] [Google Scholar]
- 21.D’Ancona F, D’Amario C, Maraglino F, et al. The law on compulsory vaccination in Italy: an update by 2 years after the introduction. Euro Surveill. 2019;24(26) doi: 10.2807/1560-7917.ES.2019.24.26.1900371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Gori D, Ialonardi M, Odone A, et al. Vaccine Hesitancy and Mandatory Immunizations in Emilia-Romagna Region: the case of MMR vaccine. Acta Biomed. 2019;90(3):394–397. doi: 10.23750/abm.v90i3.8865. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Il Fatto Quotidiano. Il tribunale di Rimini: “Il vaccino del morbillo causa l’autismo”. Insorge la comunità medica. Available online: https://www.ilfattoquotidiano.it/2012/04/16/tribunale-rimini-vaccino-morbillo-causa-lautismo-insorge-comunita-medica/204717. / (last accessed on 07 January 2020) [Google Scholar]
- 24.La Repubblica. Autismo, i giudici assolvono il vaccino. Available online: https://www.repubblica.it/salute/medicina/2015/03/01/news/autismo_i_giudici_assolvono_il_vaccino-108441541. / (last accessed on 07 January 2020) [Google Scholar]
- 25.Hwang J, Shah DV. Health Information Sources, Perceived Vaccination Benefits, and Maintenance of Childhood Vaccination Schedules. Health Commun. 2019;34(11):1279–1288. doi: 10.1080/10410236.2018.1481707. [DOI] [PubMed] [Google Scholar]
- 26.Brown KF, Kroll J, Hudson M, et al. Factors underlying parental decisions about combination childhood vaccinations including MMR: a systematic review. Vaccine. 2010;28(26):4235–4248. doi: 10.1016/j.vaccine.2010.04.052. [DOI] [PubMed] [Google Scholar]
- 27.Tabacchi G, Costantino C, Napoli G, et al. Determinants of European parents’ decision on the vaccination of their children against measles, mumps and rubella: A systematic review and meta-analysis. Hum Vaccin Immunother. 2016;12(7):1909–1923. doi: 10.1080/21645515.2016.1151990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Costantino C, Amodio E, Vitale F, et al. Attitudes, behaviours and perceptions of Italian General Practitioner trainees towards influenza vaccination in Western Sicily (Italy) Ital J Public Health. 2012;9:33–39. [Google Scholar]
- 29.Biasio LR, Corsello G, Costantino C, et al. Communication about vaccination: A shared responsibility. Hum Vaccin Immunother. 2016;12(11):2984–2987. doi: 10.1080/21645515.2016.1198456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hwang J, Shah DV. Health Information Sources, Perceived Vaccination Benefits, and Maintenance of Childhood Vaccination Schedules. Health Commun. 2019;34(11):1279–1288. doi: 10.1080/10410236.2018.1481707. [DOI] [PubMed] [Google Scholar]
- 31.Hickler B, Guirguis S, Obregon R. Vaccine Special Issue on Vaccine Hesitancy. Vaccine. 2015;33(34):4155–6. doi: 10.1016/j.vaccine.2015.04.034. [DOI] [PubMed] [Google Scholar]
- 32.Restivo V, Costantino C, Marras A, et al. Pap Testing in a High-Income Country with Suboptimal Compliance Levels: A Survey on Acceptance Factors among Sicilian Women. Int J Environ Res Public Health. 2018;15(9) doi: 10.3390/ijerph15091804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Costantino C, Mazzucco W, Marotta C, et al. Methodological issues in a cross-sectional survey on cervical cancer screening using telephone interviews in Sicily (Italy): a SWOT analysis. J Int Med Res. 2019;47(10):5174–5184. doi: 10.1177/0300060519860950. [DOI] [PMC free article] [PubMed] [Google Scholar]