

Abstract
SUMMARY: We present a case report of a patient on long-term dialysis who underwent percutaneous vertebroplasty to treat a painful intrabody vertebral cleft and who subsequently experienced a refracture of the posterior portion of the same vertebral body, resulting in anterior displacement of the cement through the anterior cortex. The case raises the question whether, in some patients, the marrow space should be filled with cement in addition to the cleft.
Vertebroplasty has become widespread in the treatment of vertebral compression fractures refractory to medical therapy and has success rates as high as 90% in some studies. Complications from this procedure, while rare, have been described and include bleeding, infection, cement embolism, and various other complications from cement extravasation. Patients with a vertebral cleft, containing either air or fluid, comprise a subset of patients in which vertebroplasty, with filling of the cleft, is typically very effective, and there have been reported cases of height restoration following this type of procedure. This is a report of refracture of the same vertebral body following filling of a large cleft during vertebroplasty in an end-stage renal patient; the case questions whether filling the cleft alone is adequate in some patients.
Case Report
A 75-year-old diabetic woman, who had been on dialysis for >20 years, presented with a 3-month history of severe back pain, unresponsive to bed rest, analgesics, and bracing. Sequential plain films showed severe diffuse osteopenia and a compression fracture at L3 that had progressed from 20% height loss at initial presentation to 60% height loss over a short period of time (Fig 1). Physical examination demonstrated marked tenderness upon palpation of the posterior spinous process of L3, and vertebroplasty was ordered, because of her rapidly progressing fracture. Vertebroplasty was performed by using an 11-gauge needle via a unipedicular approach, and it was immediately noted that the cement was filling a large cavity within the L3 vertebral body.
Fig 1.
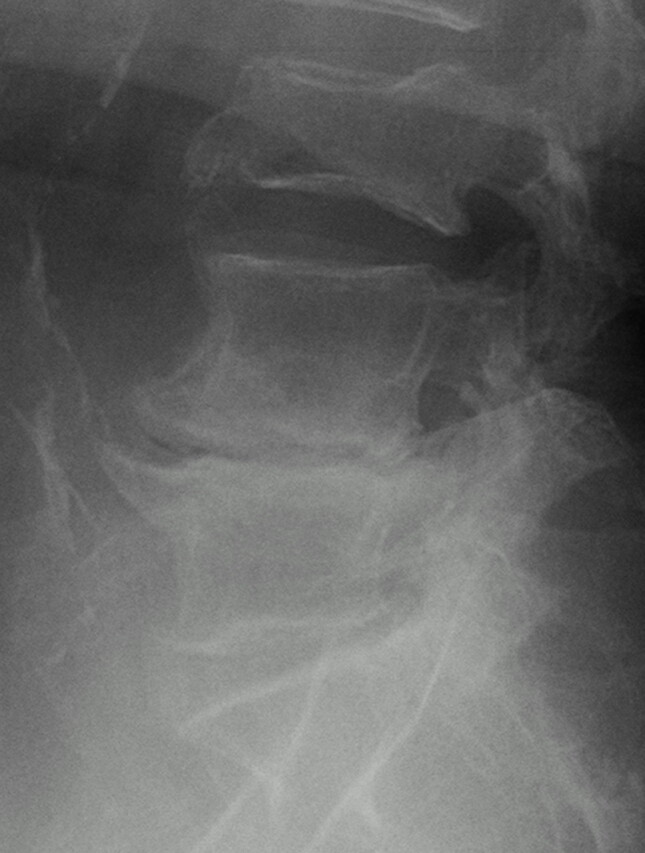
Lateral radiograph of the lumbar spine before initial vertebroplasty reveals compression of the L3 vertebral body with little anterior wall bowing.
Cement was injected until a pressure end point was reached and was no longer filling the cavity, at which point the procedure was terminated. Although she experienced some mild relief at first, the patient continued to have pain in the same area. MR imaging was performed and demonstrated incomplete filling of the cavity around the existing cement and some marrow edema at the L3 level, with no other explanation for the patient’s pain. A second procedure was performed from the opposite side, with resultant filling of the additional cavity (Fig 2), and repeat MR imaging 2 weeks later demonstrated good filling of the cavity with no significant residual edema. The patient continued to have some back pain until approximately 1 month after the second procedure, when she experienced a sudden, severe onset of unrelenting back pain more severe than any previous episodes. Repeat conventional radiographs at that time demonstrated that the patient had compressed the posterior 25% of the L3 vertebral body, and the cement bolus within the vertebral body had been displaced anteriorly approximately 1 cm into the retroperitoneal space (Fig 3). At this point, the patient refused any more therapy, elected to stop dialysis treatment, and died soon thereafter.
Fig 2.
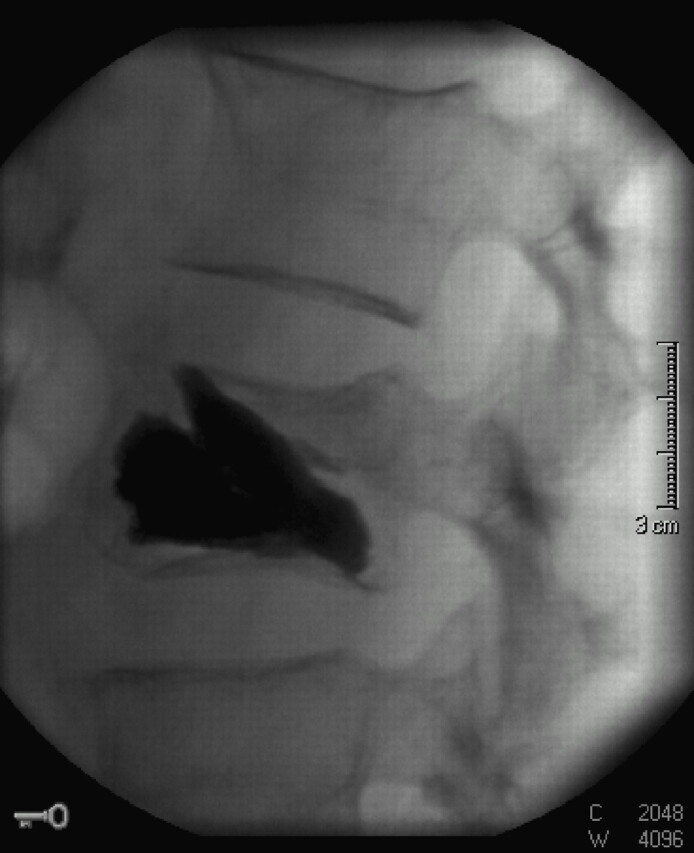
Lateral view of the L3 vertebral body at the conclusion of vertebroplasty demonstrates cement extending throughout the anterior and middle portions of the vertebral body, filling a large cleft. The presence of the cleft is confirmed by the solid appearance and sharp outer borders of the cement bolus.
Fig 3.
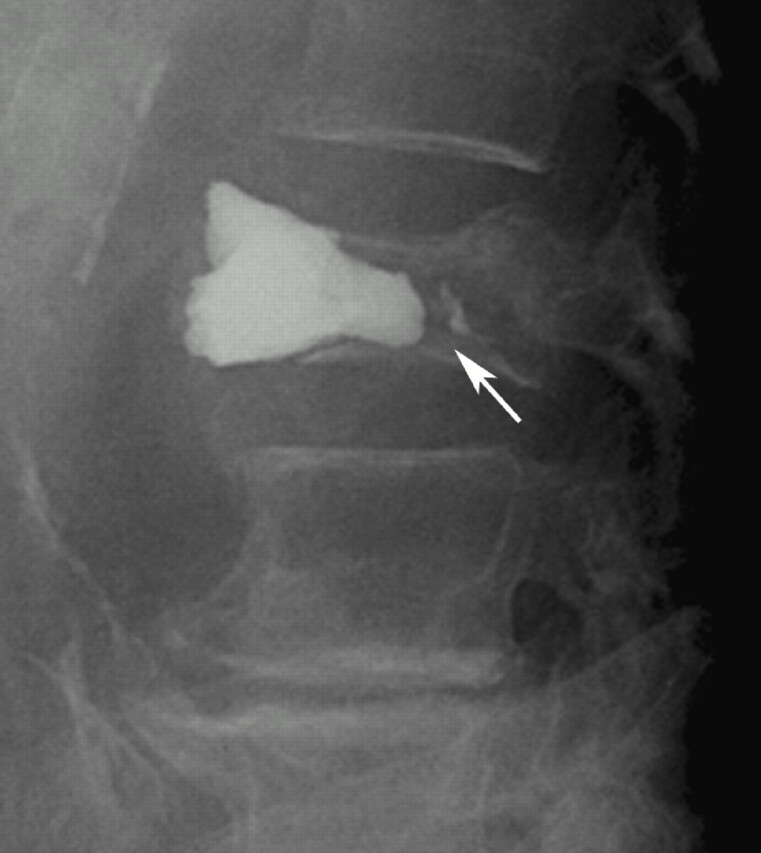
Lateral radiograph of the lumbar spine following a severe acute exacerbation of the patient’s back pain revels that the posterior portion of the vertebral body has collapsed further since the prior MR imaging, with 1 cm of anterior displacement of the intravertebral cement, which now projects well past the anterior spinal line. Note the reduced attenuation in the inferior L3 vertebral body corresponding to where the cement was initially located as well as a small amount of cement remaining in the original location (arrow).
Discussion
Vertebroplasty has become a mainstay in the treatment of osteoporotic fractures, with the first large series in this population appearing in 1997.1 Since then, there have been numerous retrospective and prospective reports in the literature regarding the efficacy and safety of this procedure.2–4 There have been complications, however, as there are in most interventional procedures, including additional fractures of the transverse process or pedicle, bleeding, infection, cement extravasation, and embolization.2, 5
The presence of a vertebral cleft represents a situation that has been well-suited to vertebroplasty, as filling the cleft with cement usually relieves pain6 and has even been reported to increase vertebral body height in some patients.7 The descriptions of the technique in the literature consist of filling of the cleft alone, with no recommendation to also fill marrow space. In our case, filling of the cleft was inadequate to treat the patient, as a refracture at the same level resulted in extrusion of the cement bolus anteriorly approximately 1 month after the procedure. To the best of our knowledge, this complication has been described only once before in the literature,8 and that patient was successfully treated with surgical stabilization. Although it is true that many levels that have undergone vertebroplasties will show some additional collapse on follow-up examinations without associated pain, the risk of symptomatic refracture has not been one commonly associated with vertebroplasty. When filling a vertebral cleft in an osteoporotic patient, it seems reasonable to assume that there is additional risk of refracture of that level, because of the strength of the cement compared with the weakness of the surrounding bone.
In this patient, the presence of long-standing renal failure and dialysis-associated osteonecrosis was the likely etiology of her vertebral cavity. Unfortunately, the marrow does not seem to have been strong enough to support the large volume of cement injected into the vertebral body, with postprocedure posterior vertebral fracture causing anterior cement extrusion. Although this is a rarely seen complication that has only been described twice, it does raise the question whether in certain patients, such as those on dialysis or with secondary drug-induced osteoporosis, and who have vertebral clefts, the marrow space should also be bolstered with cement, to prevent further collapse.
References
- 1.Jensen ME, Evans AJ, Mathis JM, et al. Percutaneous polymethylmethacrylate vertebroplasty in the treatment of osteoporotic vertebral body compression fractures: technical aspects. AJNR Am J Neuroradiol 1997;18:1897–1904 [PMC free article] [PubMed] [Google Scholar]
- 2.Evans AJ, Jensen ME, Kip KE, et al. Vertebral compression fractures: pain reduction and improvement in functional mobility after percutaneous polymethylmethacrylate vertebroplasty: retrospective report of 245 cases. Radiology 2003;226:366–72 [DOI] [PubMed] [Google Scholar]
- 3.Zoarski GH, Snow P, Olan WJ, et al. Percutaneous vertebroplasty for osteoporotic compression fractures: quantitative prospective evaluation of long term outcomes. J Vasc Interv Radiol 2002;13:139–48 [DOI] [PubMed] [Google Scholar]
- 4.Barr JD, Barr MS, Lemley TJ, et al. Percutaneous vertebroplasty for pain relief and spinal stabilization. Spine 2000;15:923–28 [DOI] [PubMed] [Google Scholar]
- 5.Laredo JD, Hamze B. Complications of percutaneous vertebroplasty and their prevention. Skeletal Radiol 2004;33:493–505 [DOI] [PubMed] [Google Scholar]
- 6.Lane JI, Maus TP, Wald JT, et al. Intravertebral clefts opacified during vertebroplasty: pathogenesis, technical implications, and prognostic significance. AJNR Am J Neuroradiol 2002;23:1642–46 [PMC free article] [PubMed] [Google Scholar]
- 7.Teng MM, Wei CJ, Wei LC, et al. Kyphosis and height restoration effects of percutaneous vertebroplasty. AJNR Am J Neuroradiol 2003;24:1893–1900 [PMC free article] [PubMed] [Google Scholar]
- 8.Tsai TT, Chen WJ, Lai PL, et al. Polymethylmethacrylate cement dislodgment following percutaneous vertebroplasty: a case report. Spine 2003;28:E457–60 [DOI] [PubMed] [Google Scholar]