

Abstract
BACKGROUND AND PURPOSE: Congenital causes of hearing loss in children commonly are encountered, and imaging aids in diagnosis as well as presurgical evaluation. Atresia of the oval window not associated with atresia of the external auditory canal (EAC) is a rare cause of congenital hearing loss in children. We present the clinical and imaging findings in children with isolated oval-window atresia.
METHODS: Atresia of the oval window was defined as the absence of the structure with the presence of a bony plate superimposed between the vestibule and middle ear. The bony plate is within the expected region of the oval window. Using a computerized database, nine patients with isolated oval-window atresia were found. All had been evaluated with high-resolution computed tomography (HRCT) and all had medical records available for review, including audiogram results. Imaging studies were interpreted by the consensus of two pediatric neuroradiologists.
RESULTS: Atresia of the oval window was documented in all cases using HRCT criteria. The most common anomalies associated with oval-window atresia were inferomedial malposition of the facial nerve (n = 8), malformed incus (n = 6), and displaced stapes (n = 2). Four patients had symmetric bilateral involvement. Hearing tests were not specific, because conductive, sensorineural, and mixed patterns were found.
CONCLUSION: Anomalies of the oval window should be sought in all patients with congenital hearing loss. Associated findings, such as facial nerve aberrancy and ossicular anomalies, are important in both diagnosis and surgical planning.
Hearing loss is the most common sensory disturbance in children. Congenital etiologies are found frequently and can be the result of various anomalies ranging from atresia of the external auditory canal (EAC) to enlargement of the vestibular aqueduct (1). At our institution, children with congenital hearing loss of unknown etiology are referred more often for CT rather than MR imaging because of the ability of CT scanning to evaluate the ossicles and osseous labyrinth. Atresia of the EAC is clinically obvious. These patients are referred for high-resolution computed tomography (HRCT) to evaluate the ossicles, the position of the facial nerve, and the thickness of the atretic bony plate prior to potential surgical repair. Oval-window atresia is known to occur with atresia of the EAC (2). Nevertheless, atresia of the oval window may be overlooked when the EAC is formed normally and a potentially correctable cause of congenital hearing loss may be missed. The imaging findings of isolated atresia of the oval window have received little attention in the literature (3–5). We report the clinical presentation and HRCT findings in children with oval-window atresia not associated with anomalies of the EAC.
Methods
Using a computer database, nine patients with isolated oval-window atresia were found between June 1993 and June 1997. The database is comprehensive and includes all patients who underwent neuroimaging in our department. Age range of patients at initial CT scanning was 2 to 13 years (mean, 5.6 years). Five patients were male, and four were female. All had been referred for evaluation of congenital hearing loss. Medical records were reviewed, with specific attention to audiogram results and type of hearing loss (ie, conductive, mixed, or sensorineural).
All patients were imaged by using HRCT in the axial and coronal planes. One-mm collimation, bone algorithm, and targeted magnified reconstruction were used. Two neuroradiologists evaluated the images by consensus. The diagnosis of oval-window atresia was confirmed in all cases by demonstrating a well-defined bony plate in the expected region of the oval window between the middle ear cavity and the vestibule. The distance between the superior and inferior margins of the oval window was narrowed, which was visualized best on the coronal images. In addition to the bony atresia of the oval window, we documented position of the facial nerve canal, any ossicular anomalies, anomalies of the bony labyrinth, and the patency of the EAC. Surgical confirmation was not present. In our institution, this entity previously was thought to be inoperable owing to potential complications and limitations in technology. Also, children with unilateral hearing loss were not examined because of normal hearing within the contralateral ear.
Results
The EAC was widely patent in all the patients without elongation of the scutum. Oval-window atresia was clearly shown in all patients and was associated with specific anomalies of the incus, stapes, and facial nerve. The incus was highly visible on all scans. A malformed or absent lenticular process was documented in six patients (67%). The stapes was difficult to visualize in six patients and clearly was malpositioned in two patients. Axial images revealed the stapes to be directed posterior and attached to the pyramidal eminence (Fig 1 and 2). The tympanic portion of the facial nerve had an aberrant position in eight patients (90%). Usually, the tympanic segment was displaced inferior to the expected region of the absent oval window (n = 5). In two patients, the tympanic portion of the facial nerve was displaced below the atretic oval window just lateral to the cochlear prominence (Fig 3). The descending portion of the facial nerve was located normally in all patients. The epitympanic recess, mesotympanum, and hypotympanum otherwise were formed normally and the tympanic membranes were normal. There were no anomalies of the osseous labyrinth. Four of nine patients had bilateral involvement, which was symmetrical. The children with unilateral involvement had a clearly defined patent oval window on the unaffected side.
fig 1.
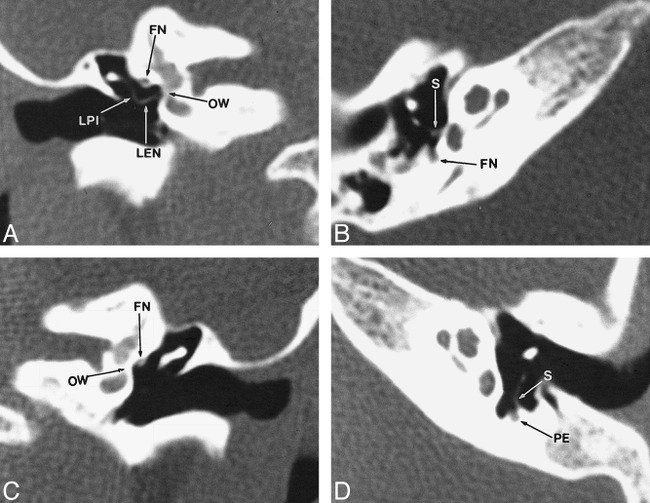
Case 5: A 4-year-old male patient with left sensorineural hearing loss.
A and B, Coronal (A) and axial (B) HRCT images through right temporal bone show no abnormality. Lenticular process (LEN) is well formed and joins long process of incus (LPI) at 90° angle. oval window (OW) is patent. stapes (S) and facial nerve (FN) are appropriately positioned.
C and D, Coronal (C) and axial (D) HRCT images through left temporal bone. Left oval window (OW) is absent with facial nerve (FN) present within expected location of structure. Lenticular process of incus is not well developed and crura of stapes (S) are oriented toward pyramidal eminence (PE).
fig 2.
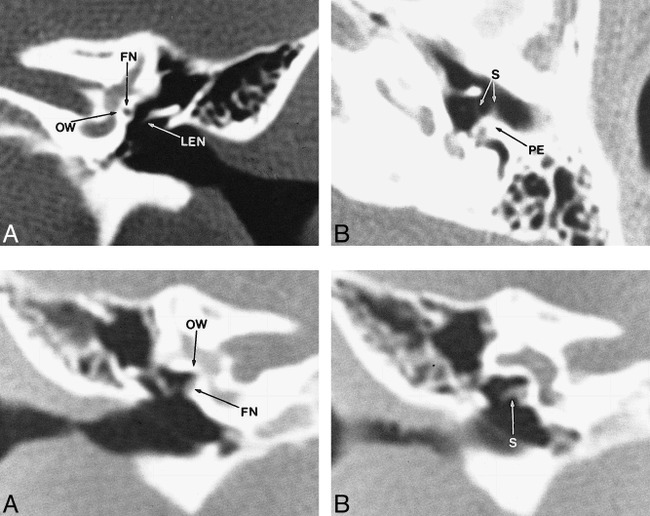
Case 6: A 3-year-old male patient with left conductive hearing loss.
A and B, Coronal (A) and axial (B) HRCT images of left temporal bone. Left oval window (OW) is absent with facial nerve (FN) displaced into region. Lenticular process of incus (LEN) is absent and crura of stapes (S) are oriented toward pyramidal eminence (PE).
fig 3. Case 1: A 2-year-old female patient with left sensorineural hearing loss.
A and B, Coronal (A) and axial (B) HRCT images of right temporal bone. Oval window (OW) is absent. Inferior to oval window is displaced facial nerve (FN). Dysmorphic stapes (S) is attached to aberrant facial nerve. Both temporal bones were symmetrically abnormal.
A pediatric otolaryngologist performed hearing tests, with audiograms obtained from all children. The classical finding of a mixed pattern of hearing loss usually found, with pathology at the level of the oval window, was encountered in only two patients. The remainder of patients presented with conductive (n = 4) or sensorineural (n = 3) hearing loss. One patient with bilateral anomalies had left sensorineural hearing loss whereas hearing on the right was normal.
Discussion
Isolated oval-window atresia is considered a minor anomaly of the middle ear. Patients typically present with conductive or mixed hearing loss and a history consistent with congenital hearing loss (6). Sensorineural hearing loss, which was found in three patients in our series, has not been reported, to our knowledge, in patients with oval-window atresia; however, inner-ear anomalies have been reported in the pathology literature in association with oval-window atresia (7). The finding of sensorineural hearing loss is important, especially when examining this cohort of patients with MR imaging, because the oval window and associated structures will not be evaluated adequately. MR imaging, however, may be complementary and reveal subtle dysplasias of the membranous labyrinth or hypoplasia of the vestibulocochlear nerve not seen by HRCT (8). Bilateral oval-window atresia was associated with left sensorineural hearing loss in one patient (Fig 3). The absence of hearing loss on the right is difficult to explain. Surgical confirmation was not performed owing to the presence of unilateral hearing loss.
Isolated oval atresia has been reported infrequently in the literature (9–14). Most reported cases are of surgical findings and have limited or no correlation with HRCT. Two cases of oval-window atresia with an aberrant facial nerve have been missed by HRCT, but found at surgery (5). HRCT was found to be diagnostic by using imaging criteria in our series of patients. The bony plate present within the oval window was visualized easily on coronal images in all patients. Surgical exploration in cases of oval-window atresia has shown the stapes to be uniformly dysplastic or absent (3). In our group of patients, the stapes was not seen well in most (n = 6) and actually displaced in two cases. The inability to visualize the stapes may relate to absence or severe dysplasia of the structure. We found evaluation of the incus to be most useful owing to the relative ease of identification on coronal images. The lenticular process of the incus was absent or inferiorly malpositioned in six cases. The tympanic segment of the facial nerve was visualized in all patients and was positioned abnormally in eight.
The embryology of oval-window atresia is related directly to the development of second branchial arch structures and, most importantly, the facial nerve. The lenticular process of the incus, stapes suprastructure, and facial nerve all develop from the second branchial arch. The oval window is actually derived from the optic capsule, but will not form without the stimulus of contact by the stapes. Two theories have been developed to explain oval-window atresia. The first links the abnormal formation of the oval window to the development and subsequent position of the facial nerve. The tympanic and descending segments of the facial nerve become visible at 5 to 6 weeks. The facial nerve becomes displaced anteriorly and inferiorly, and lies between the stapes blastema and oval window. This position prevents the normal migration of the stapes and thus prevents induction of the oval window (15). The second theory links underdevelopment of the first arch and subsequent compensatory anterior shifting of the second arch structures to explain oval-window atresia (16). Both theories incorporate the normal development of the facial nerve as a requirement for formation of a patent oval window. In our series, the former theory seems more plausible because of the lack of first arch anomalies as well as the facial nerve being displaced more inferiorly rather than anteriorly. In children with major anomalies of the middle ear and oval-window atresia, the facial nerve seems to be displaced anteriorly and is associated by definition with anomalies of the first arch. These findings make the latter theory more applicable in this group of patients.
Surgery is an option in this group of patients, but variable results have been reported. Sterkers and Sterkers (13) reported long-term correction of conductive hearing loss in six of eight cases. The oval window was bypassed and a fenestra drilled above the expected region of the oval window with placement of a piston. Lambert (4) reported a series of patients treated with vestibulotomy and prosthesis placement. Initial improvement in hearing was eventually lost in a majority of patients. Attempted surgical intervention with the possibility of injury to the facial nerve remains controversial in this group of patients. Surgical results potentially could be affected by coexisting occult malformations of the inner ear.
Conclusion
Anomalies of the oval window should be sought in all patients presenting with congenital hearing loss. The type of congenital hearing deficit is variable and should not influence the radiologic diagnosis. This entity is overlooked easily using CT scanning unless meticulous axial and coronal images, in particular, are obtained. Associated findings, such as facial nerve and stapedial malposition, are important factors in surgical planning. Anomalies of the lenticular process of the incus are found commonly among patients with oval-window atresia and can serve as an indicator of pathology at the level of the oval window.
Footnotes
Presented at the annual meeting of the American Society of Neuroradiology, Philadelphia, May 1998.
Address reprint requests to Timothy N. Booth, MD, Children's Medical Center of Dallas, Department of Radiology, 1935 Motor Street, Dallas, TX 75235.
References
- 1.Fisher NA, Curtin HD. Radiology of congenital hearing loss. Otolaryngol Clin NA 1994; 27:511-531 [PubMed] [Google Scholar]
- 2.Jahrsdoefer RA. Transposition of the facial nerve in congenital aural atresia. Am J Otol 1995;16:290-294 [PubMed] [Google Scholar]
- 3.Kerman HK, Kimmelman CP. Congenital anomalies limited to the middle ear. Otolaryngol Head Neck Surg 1992;106:285-287 [DOI] [PubMed] [Google Scholar]
- 4.Lambert PR. Congenital absence of the oval window. Laryngoscope 1990;100:37-40 [DOI] [PubMed] [Google Scholar]
- 5.Huang TS. Anomalously coursing facial nerves above and below the oval window: Three case reports. Otolaryngol Head Neck Surg 1997;116:438-441 [DOI] [PubMed] [Google Scholar]
- 6.Jahrsdoefer RA. The facial nerve in congenital middle ear malformations. Laryngoscope 1981;111:1217-1225 [DOI] [PubMed] [Google Scholar]
- 7.Harada T, Black OF, Sando I, et al. Temporal bone histopathologic findings in congenital anomalies of the oval window. Otolaryngol Head Neck Surg 1980;88:275-287 [DOI] [PubMed] [Google Scholar]
- 8.Casselman JW, Offeciers FE, Govaerts PJ, et al. Aplasia and hypoplasia of the vestibulocochlear nerve: diagnosis with MR imaging. Radiology 1997;220:773-781 [DOI] [PubMed] [Google Scholar]
- 9.Pou JN. Symposium: Congenital anomalies of the middle ear. III. Congenital anomalies of the middle ear. Larynoscope 1976;86:251-254 [DOI] [PubMed] [Google Scholar]
- 10.Hough JD. Malformations and anatomic variation seen in the middle ear during the operation for mobilization of the stapes. Laryngoscope 1958;65:1337-1360 [DOI] [PubMed] [Google Scholar]
- 11.Jahrsdoefer RA. Congenital malformations of the ear, analysis of 94 operations. Ann Otol 1980;89:348-352 [DOI] [PubMed] [Google Scholar]
- 12.Al-Shihabi BS. Abnormalities of the facial nerve and middle ear. J Laryngol Otol 1984; 98:391-393 [DOI] [PubMed] [Google Scholar]
- 13.Sterkers JM, Sterkers O. Surgical management of congenital absence of the oval window with malposition of the facial nerve. Adv Otorhinolatungol 1988;1988:33-37 [DOI] [PubMed] [Google Scholar]
- 14.Tabor JR. Absence of the oval window. Arch Otolaryngol 1961;74:515-521 [DOI] [PubMed] [Google Scholar]
- 15.Jahrsdoefer RA. Embryology of the facial nerve. Am J Otol 1988;9:423-426 [PubMed] [Google Scholar]
- 16.Gerhardt IU, Otto HD. The intratemporal course of the facial nerve and its influence of the development of the ossicular chain. Acta Otolaryngol 1981;91:567-573 [DOI] [PubMed] [Google Scholar]