

Abstract
Summary: Developmental venous anomalies (DVAs) are common variants of cerebral venous drainage that are typically incidental findings on contrast-enhanced MR imaging studies. We present four cases of asymptomatic DVAs that demonstrate increased cerebral blood flow, cerebral blood volume, mean transit time, and time to peak on perfusion MR images. Our study indicates that alterations in perfusion MR imaging parameters can be seen with uncomplicated DVAs and do not necessarily imply a more ominous underlying etiologic factor, such as hypervascular tumor or stroke.
Developmental venous anomalies (DVAs), formerly known as venous angiomas, are congenital variants of cerebral venous drainage that are frequently identified in contrast-enhanced MR imaging brain studies. In general, these anomalies are incidentally found and of no consequence to the patient. The brain surrounding the DVA is nearly always normal, and histologically the anomaly is limited to the venous structures, without involvement of capillaries or arteries. Perfusion MR imaging is capable of noninvasively characterizing the hemodynamic features of DVAs both at the site of these anomalies and in the surrounding tissues and thus may provide further insight into their physiological significance. In this report, we present unusual perfusion MR imaging findings in four patients with DVAs.
Case Reports
Case 1
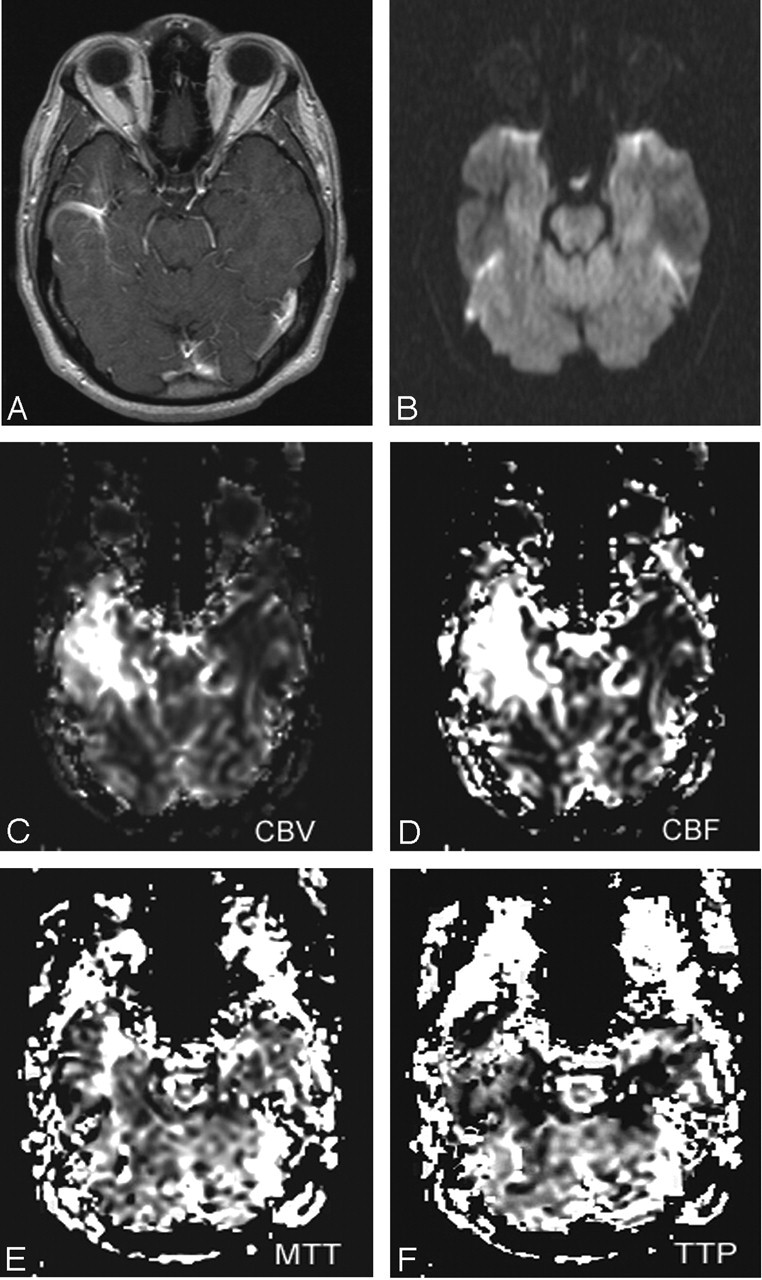
A 44-year-old female patient with a history of anxiety disorder presented with several hours of left facial weakness following an episode suggestive of a panic attack. Her medical history was significant for smoking and hypertension. No neurologic deficits were present on physical examination. MR imaging of the brain was performed to evaluate for stroke. No acute infarctions were seen on diffusion-weighted (DW) images. T1-weighted, postcontrast images demonstrated a left frontal lobe DVA with a large central vein draining into the superior sagittal sinus. Perfusion sequences demonstrated elevations in cerebral blood flow (CBF), cerebral blood volume (CBV), mean transit time (MTT), and time-to-peak (TTP) within the DVA and in the surrounding parenchyma (Fig 1; Table). The remainder of the MR imaging examination was unremarkable. The patient was admitted for overnight observation. Her symptoms resolved by the following morning, and she was discharged.
Fig 1.

Coronal T1-weighted postcontrast image (TR/TE, 635/17) (A), axial DW image (TR/TE, 4300/122; b = 1000) (B), and axial GE CBV (C), CBF (D), MTT (E), and TTP (F) maps of the brain in a patient with an uncomplicated DVA (case 1). The postcontrast image demonstrates a DVA in the left frontal lobe. DW image demonstrates flow void in the central draining vein of the DVA, but no restriction of diffusion. Perfusion maps show increased signal intensity within the DVA and in the surrounding parenchyma on CBV, CBF, MTT, and TTP maps.
MR imaging perfusion measurements in four DVAs
| Case 1 | Case 2 | Case 3 | Case 4 | Mean | |
|---|---|---|---|---|---|
| Age/Sex | 44/F | 31/F | 35/M | 60/M | |
| draining vein diameter (mm) | 3.80 | 1.00 | 5.50 | 2.60 | |
| CBF ratio* | 3.51 | 4.89 | 15.80 | 1.31 | 6.38 |
| CBV ratio | 4.27 | 4.22 | 8.47 | 3.39 | 5.09 |
| MTT ratio | 1.84 | 1.37 | 1.22 | 1.64 | 1.52 |
| TTP ratio | 1.11 | 1.05 | 1.07 | 1.08 | 1.08 |
A ratio was computed for each parameter by drawing a region of interest around the area of signal abnormality associated with the DVA (ROIDVA) and a region of interest around a similar area of uninvolved contralateral brain (ROIcontra). The ratio was computed by dividing the mean signal intensity of ROIDVA by the mean signal intensity of ROIcontra.
Case 2
A 31-year-old female patient presented with a 5-minute episode of lightheadedness, palpitations, and mild headache. This was followed by a sensation of leaning to the left while walking. Her blood pressure and pulse were within normal limits, and she was not orthostatic. Physical examination was remarkable only for slightly decreased strength in her left arm and leg and a mildly ataxic gait. Noncontrast cranial CT findings were normal. Cranial MR imaging showed no restriction of diffusion. On T1-weighted, postcontrast images, a small DVA was present in the subcortical region of the left posterior parietal lobe. A 1-mm enhancing vessel extended from this area to the left lateral ventricle. Perfusion sequences demonstrated elevations in CBF, CBV, MTT, and TTP in this region (Table). An MR venogram was normal, and no other abnormalities were identified on the MR imaging study. The patient was admitted for overnight observation and discharged the next morning following resolution of her symptoms.
Case 3
A 35-year-old male patient, who had a left frontal lobe ganglioglioma resected 3 years previously, presented for routine imaging follow-up. His only reported symptoms were chronic, occasional, mild auras that did not interfere with daily activities. Cranial MR imaging revealed stable postsurgical and postradiation changes in the left frontal lobe with no tumor recurrence. No restriction of diffusion was identified on DW images. On T1-weighted postcontrast images, a 5.5-mm-diameter, curvilinear, enhancing vessel compatible with a DVA was seen in the right temporal lobe. This DVA was stable when compared with multiple prior cranial MR imaging examinations over an 8-year period. Perfusion sequences demonstrated marked increases in CBF and CBV and mild increases in MTT and TTP in the right temporal lobe within and surrounding the DVA (Fig 2, Table). In light of the stability of his imaging findings and clinical symptoms, no further clinical interventions were undertaken at that time. The patient was scheduled for routine imaging follow-up.
Fig 2.
Axial T1-weighted postcontrast image (TR/TE, 635/17) (A), axial DW image (TR/TE, 4300/122; b = 1000) (B), and axial gradient echo CBV (C), CBF (D), MTT (E), and TTP (F) maps of the brain in a patient with an uncomplicated DVA (case 3). The postcontrast image demonstrates a DVA in the right temporal lobe. DW image demonstrates flow void in the draining vein of the DVA, but no restriction of diffusion. Perfusion maps show marked elevations in CBF and CBV and milder elevations in MTT and TTP within the DVA and in the surrounding parenchyma.
Case 4
A 60-year-old HIV-positive male patient presented with unsteady gait and altered mental status. He had a history of hypertension, hypercholesterolemia, and newly diagnosed lung masses with hilar adenopathy. The patient had a known cavernous angioma in the right caudate nucleus. An MR imaging examination of the brain was performed, and DW imaging showed no restriction of diffusion. A 1.2-cm rounded heterogeneous lesion in the head of the right caudate nucleus was seen, consistent with the patient’s known cavernous angioma. Lateral to this lesion on T1-weighted, postcontrast images was a DVA with a 2.6-mm draining vein. Perfusion sequences revealed markedly increased signal intensity in the vicinity of the DVA on CBF and CBV maps and mildly increased signal intensity on MTT and TTP maps (Table). No other cranial MR imaging abnormalities were identified. Lumbar puncture and blood cultures revealed no infectious pathogens. During his 5-day hospital stay, his mental status improved, and his gait remained mildly ataxic. He was discharged on antiretroviral therapy with a presumed diagnosis of HIV encephalopathy. He showed no progression of symptoms at his 2-month follow-up.
Discussion
Although DVAs were thought to be rare before the advent of CT and MR imaging, they are now considered the most common anomalies of the intracranial vasculature (1). Embryologically, an in utero arrest in venous development is believed to occur after arterial development is nearly complete, resulting in the retention of primitive medullary veins that feed into a single, large draining vein (1, 2). Histopathologic studies of these anomalies have found large numbers of closely aggregated, distended, thin-walled veins similar to the vessels of arteriovenous malformations, but without abnormal arteries (3, 4). Although several authors have reported that the brain parenchyma separating these abnormal vascular channels is normal (5, 6), others have described gliosis, neuronal degeneration, and demyelination (7). DVAs are typically benign, asymptomatic and uncomplicated; however, they can rarely be a cause of hemorrhage, seizure, or ischemia, particularly if they are associated with other vascular malformations (5, 7–9).
DVAs have a characteristic appearance on imaging studies. On noncontrast T2-weighted MR images, signal intensity void is seen in the draining vein. Variable degrees of T2 and T1 prolongation may be present in the adjacent parenchyma. This is thought to be due to the increased blood pool throughout the DVA (10). At both contrast-enhanced MR imaging and conventional angiography, a series of small deep parenchymal veins converge toward a larger collecting vein that follows a transhemispheric course before draining into a normal deep or superficial vein. At angiography, a DVA typically opacifies at the same time as the normal veins, although DVAs in the frontal lobes may opacify earlier with an associated capillary blush (2, 5).
The DVAs in our study were associated with varying degrees of elevation in CBV, MTT, and TTP (Table). The marked elevations in CBV measurements are consistent with prior histologic studies of DVAs demonstrating an increase in both the number and the caliber of their vessels. The increases in MTT and TTP may be due to abnormalities of their drainage. Truwit (1) reported that a focal stenosis of the draining vein may be seen at the point where it penetrates the dura to enter the dural sinus, leading to delayed filling and emptying of a DVA. If venous pressure in the territory drained by the DVA progressively increases, regional ischemia may ensue, resulting in focal neurologic deficits, seizure, or hemorrhage (5).
In contrast to prior imaging studies reporting decreased CBF in association with DVAs, CBF values in our four patients were 1.3–15.8 times greater in DVAs than in uninvolved, contralateral parenchyma (Table). By using xenon-enhanced CT scanning, Uchida et al (11) found that CBF values were significantly reduced in two large DVAs and unchanged in a small DVA and postulated that the larger anomalies resulted in the development of regional ischemia. In a brain perfusion SPECT study using I-123 IMP, Matsuda et al (7) demonstrated an area of focally decreased CBF immediately adjacent to a DVA in a patient with simple partial seizures. Although this area correlated with the electroencephalographic seizure focus, the interictal timing of this imaging study may have contributed to the decreased CBF to that region.
Increased CBF, as seen in our patients, may be related to the gradient-echo (GE) technique used in perfusion sequences. Several studies have shown that GE perfusion sequences are more sensitive than spin-echo (SE) sequences to flow in large caliber vessels (12–14). Although contrast-to-noise ratios are greater in GE sequences than in SE sequences, the greater susceptibility effect created in and around larger vessels with GE sequences can lead to overestimation of both CBF and CBV in these regions (12, 15). The relative elevations in CBF in the current study may therefore reflect blood products in the more numerous and dilated venous channels that are histologically characteristic of DVAs, rather than true elevations in tissue-level capillary perfusion. Of the many patients with DVAs evaluated in our institution with similar perfusion studies, however, only the four described here have shown increased parameters. Donahue et al (13) demonstrated increased signal intensity on GE CBV maps and normal signal intensity on SE CBV maps in a single DVA. The effects of this DVA on CBF, MTT, and TTP were not reported. Whereas DVAs are typically thought to be anomalies of venous drainage with normal arterial anatomy, Wendling et al (6) visualized abnormally enlarged perforating arterial branches filling the periphery of two of three DVAs at magnification angiography. This suggests that some of the apparent increases in CBF surrounding the DVAs in our study may also have a physiological basis. Future studies directly comparing the perfusion MR imaging characteristics of DVAs by using GE, SE, and arterial spin-labeling techniques may provide further insight into these findings, and we propose that two types of DVAs may exist—a group with normal perfusion and one with increased perfusion. The clinical implications of increased arterial perfusion in DVAs remain uncertain.
In our four patients, the DVAs and their associated elevations in perfusion MR imaging parameters were in regions of the brain that were likely unrelated to the patients’ clinical symptoms. Perfusion MR imaging sequences are commonly performed in the evaluation of known or suspected brain tumor, trauma, or stroke, and the number of potential additional applications is growing. In light of the high prevalence of DVAs in the general population and the increasing incorporation of perfusion sequences in cranial MR imaging protocols, DVA-associated perfusion abnormalities will likely be detected with increasing frequency in the imaging workup for other suspected brain disease, particularly if GE sequences are used. Our study indicates that alterations in perfusion MR imaging parameters can be seen with uncomplicated, asymptomatic DVAs and do not necessarily imply a more ominous underlying factor, such as the presence of hypervascular tumor or stroke.
References
- 1.Truwit CL. Venous angioma of the brain: history, significance, and imaging findings. AJR Am J Roentgenol 1992;159:1299–1307 [DOI] [PubMed] [Google Scholar]
- 2.Saito Y, Kobayashi N. Cerebral venous angiomas: clinical evaluation and possible etiology. Radiology 1981;139:87–94 [DOI] [PubMed] [Google Scholar]
- 3.Abe M, Hagihara N, Tabuchi K, et al. Histologically classified venous angiomas of the brain: a controversy. Neurol Med Chir (Tokyo) 2003;43:1–10 [DOI] [PubMed] [Google Scholar]
- 4.McCormick WF. The pathology of vascular (“arteriovenous”) malformations. J Neurosurg 1966;24:807–816 [DOI] [PubMed] [Google Scholar]
- 5.Lasjaunias P, Burrows P, Planet C. Developmental venous anomalies (DVA): the so-called venous angioma. Neurosurg Rev 1986;9:233–242 [DOI] [PubMed] [Google Scholar]
- 6.Wendling LR, Moore JS, Kieffer SA, et al. Intracerebral venous angioma. Radiology 1976;119:141–147 [DOI] [PubMed] [Google Scholar]
- 7.Matsuda H, Terada T, Katoh M, et al. Brain perfusion SPECT in a patient with a subtle venous angioma. Clin Nucl Med 1994;19:785–788 [DOI] [PubMed] [Google Scholar]
- 8.Huber G, Henkes H, Hermes M, et al. Regional association of developmental venous anomalies with angiographically occult vascular malformations. Eur Radiol 1996;6:30–37 [DOI] [PubMed] [Google Scholar]
- 9.Rothfus WE, Albright AL, Casey KF, et al. Cerebellar venous angioma: “benign” entity? AJNR Am J Neuroradiol 1984;5:61–66 [PMC free article] [PubMed] [Google Scholar]
- 10.Augustyn GT, Scott JA, Olson E, et al. Cerebral venous angiomas: MR imaging. Radiology 1985;156:391–395 [DOI] [PubMed] [Google Scholar]
- 11.Uchida K, Tamura K, Takayama H, et al. Xenon-enhanced CT CBF measurements in intracranial vascular malformations. No Shinkei Geka 1989;17:239–246 [PubMed] [Google Scholar]
- 12.Speck O, Chang L, DeSilva NM, Ernst T. Perfusion MRI of the human brain with dynamic susceptibility contrast: gradient-echo versus spin-echo techniques. J Magn Reson Imaging 2000;12:381–387 [DOI] [PubMed] [Google Scholar]
- 13.Donahue KM, Krouwer HG, Rand SD, et al. Utility of simultaneously acquired gradient-echo and spin-echo cerebral blood volume and morphology maps in brain tumor patients. Magn Reson Med 2000;43:845–853 [DOI] [PubMed] [Google Scholar]
- 14.Grandin CB. Assessment of brain perfusion with MRI: methodology and application to acute stroke. Neuroradiology 2003;45:755–766 [DOI] [PubMed] [Google Scholar]
- 15.Carroll TJ, Haughton VM, Rowley HA, Cordes D. Confounding effect of large vessels on MR perfusion images analyzed with independent component analysis. AJNR Am J Neuroradiol 2002;23:1007–1012 [PMC free article] [PubMed] [Google Scholar]