

Abstract
BACKGROUND AND PURPOSE: Distally located cerebral aneurysms are difficult to treat with preservation of the parent vessel. We report the angiographic results and clinical outcome for 27 patients with peripheral cerebral aneurysms.
METHODS: From January 2000 to June 2005, 27 patients, 13 female and 14 male, presented to our institution with peripheral intracranial aneurysms and were treated endovascularly. None of these aneurysms were mycotic in origin. The age of our patients ranged from 23 to 76 years with a mean age of 53. Twenty of the 27 patients had subarachnoid and/or intracerebral hemorrhage upon presentation. In 5 patients, the aneurysm was an incidental finding. One patient with a fusiform P2 aneurysm presented with cranial nerve III palsy, and another patient with P4 aneurysm had visual disturbances. Locations of the aneurysms were as follows: posterior cerebral artery in 9 patients, superior cerebellar artery in 5 patients, anterior inferior cerebellar artery in 1 patient, posterior inferior cerebellar artery in 5 patients, middle cerebral artery (MCA) in 5 patients, and anterior cerebral artery in 2 patients.
RESULTS: Seven patients were treated with selective embolization with Guglielmi detachable coils (GDCs). Nineteen patients with fusiform aneurysms underwent parent artery occlusion (PAO). Fifteen PAOs were performed with coils and 4 with glue. One patient with a MCA aneurysm was found at the time of planned embolization to have spontaneously thrombosed the aneurysm and the distal branch of the MCA, 1 day after the initial diagnostic angiogram. Five patients (5/18 or 27.7%) who underwent PAO developed neurologic deficits. Two patients (2/18 or 11.1%) had permanent neurologic deficits (a visual field defect).
CONCLUSION: Our results support that distally located aneurysms can be treated with endovascular PAO in the cases in which selective occlusion of the aneurysmal sac with GDC or surgical clipping cannot be achieved.
The approach to the treatment of distally located aneurysms is difficult and significantly different from that for aneurysms located more proximally. The introduction of endovascular methods has added an attractive minimally invasive therapeutic approach, sparing the patient some of the hazards associated with craniotomy and open surgical clipping. On occasion, the configuration of these aneurysms may not be amenable to selective coil embolization and parent artery occlusion is the preferred treatment. The aim of our study was to report our results in 27 patients with distally located aneurysms who underwent endovascular treatment.
Patients and Techniques
From January 2000 to June 2005, 27 patients, 13 female and 14 male, presented to our institution with peripheral intracranial aneurysms (Table 1). Twenty-six were treated endovascularly. The age of our patients ranged from 23 to 76 years, with a mean age of 53. Locations of the aneurysms were as follows: posterior cerebral artery (PCA) in 9 patients, superior cerebellar artery (SCA) in 5 patients, anterior inferior cerebellar artery (AICA) in one patient, posterior inferior cerebellar artery (PICA) in 5 patients, middle cerebral artery (MCA) in 5 patients, and anterior cerebral artery (ACA) distal to pericallosal-callosomarginal artery in 2 patients.
Table 1:
Summary of clinical and angiographic data
| Case | Age/Sex | Presentation | Aneurysm | Treatment | Clinical Outcome/Follow-Up Imaging Findings |
|---|---|---|---|---|---|
| 1 | 43/M | Incidental | SCA | PAO | Ataxia that resolved within 1 month post-op. CT/MRI: cerebellar infarct |
| 2 | 51/M | SAH (I) | SCA | PAO | Excellent |
| 3 | 40/F | SAH (II) | SCA | PAO | Excellent |
| 4 | 54/M | SAH (II) | SCA | PAO | Ataxia that resolved within 3 weeks CT/MRI: cerebellar infarct |
| 5 | 73/F | SAH(II) | SCA | PAO | Excellent |
| 6 | 68/F | SAH (III) | PICA | Selective | Excellent |
| 7 | 67/F | SAH (III) | PICA | PAO* | Excellent |
| 8 | 66/F | SAH (II) | PICA | PAO* | Excellent |
| 9 | 64/F | SAH (II) | PICA | PAO | Excellent |
| 10 | 64/F | SAH (II) | PICA | PAO | Excellent |
| 11 | 63/M | SAH (II) | AICA | Selective | Excellent |
| 12 | 57/M | SAH (II) | PCA | PAO | Hemiparesis/CT: Thalamic infarct |
| 13 | 40/M | Incidental | PCA | Selective | Excellent |
| 14 | 38/F | Incidental | PCA | Selective | Excellent |
| 15 | 23/F | SAH (II) | PCA | PAO | Excellent |
| 16 | 53/F | SAH (II) | PCA | Selective | Excellent |
| 17 | 23/M | Headache, visual disturbances | PCA | PAO | Excellent |
| 18 | 49/M | Diplopia | PCA | PAO | Homonymous hemianopsia, hemiparesis improved; diplopia goneCT, MRI: occipital, thalamic infarct |
| 19 | 54/F | Incidental | PCA | PAO | Visual field defect/occipital Infarct |
| 20 | 76/M | SAH (III) | PCA | PAO | Excellent |
| 21 | 23/M | SAH (III) | MCA | PAO | Hemiparesis (due to hematoma) resolved |
| 22 | 44/M | SAH (III) | MCA | PAO | Excellent/CT: small infarct/not relevant to the procedure (angiospasm) |
| 23 | 38/M | Incidental | MCA | PAO | Excellent |
| 24 | 72/M | Hematoma | MCA | PAO | Excellent |
| 25 | 67/F | SAH (III) | MCA | Spontaneous thrombosis | Excellent |
| 26 | 53/F | SAH (IV) | ACA | PAO | Dead (sepsis) |
| 27 | 64/M | SAH (III) | ACA | PAO | Excellent |
Note:—M indicates male; F, female; SCA, superior cerebellar artery; PAO, parent artery occlusion; SAH, subarachnoid hemorrhage; PICA, posterior inferior cerebellar artery; AICA, anterior inferior cerebellar artery; PCA, posterior cerebral artery; MCA, middle cerebral artery; ACA, anterior cerebral artery;
, delayed parent artery occlusion.
Twenty of the 27 patients presented with subarachnoid and/or intracerebral hemorrhage as the result of rupture of the peripheral aneurysm. According to the Hunt and Hess scale, 1 patient’s condition was grade I, 10 patients were grade II, 8 were grade III, and 1 patient was grade IV. In 5 patients, the aneurysm was an incidental finding. One patient with a fusiform P2 aneurysm presented with cranial nerve III palsy, and 1 patient with a distal PCA aneurysm presented with visual disturbances.
Four patients had multiple aneurysms. Two of these had a ruptured PICA aneurysm upon presentation and a second symmetric unruptured aneurysm in the opposite PICA. We treated the ruptured PICA aneurysm with selective coil embolization and the second mirror aneurysm in the opposite PICA was left untreated because the patients refused further treatment. A third patient with 2 aneurysms had surgical clipping of the ruptured MCA aneurysm elsewhere and was sent to us for embolization of the second asymptomatic PCA (P2 segment) aneurysm. This was treated successfully with selective coil embolization. The fourth patient with 2 aneurysms had a ruptured distal MCA aneurysm that underwent successful embolization with parent artery occlusion (PAO) and a second unruptured vertebrobasilar artery aneurysm that underwent selective coil embolization later.
All patients underwent CT angiography (CTA) and digital substraction angiography (DSA) and therapeutic options, surgical or endovascular, were discussed. Both studies are routinely performed on all patients with cerebral aneurysms in our institution. CTA is usually the first examination and has an important role as an adjunct to DSA because it is noninvasive and can provide useful information about the morphology of the aneurysm and its relation to adjacent vessels thus assisting in treatment planning.
All patients underwent endovascular treatment under general anesthesia after giving informed consent. A baseline CTA was obtained to herald baseline anticoagulation. Heparin (12,500 IU/L) was administered in the flushing solutions. Bolus infusions of heparin were not administered; thus, any anticoagulation that may have occurred from the flush solutions was not reversed at the end of the procedure.
Seven patients were treated with selective embolization with Guglielmi detachable coils (GDCs; Boston Scientific, Natick, Mass). Two of these patients (7 and 8) with PICA aneurysms were treated with selective coil embolization. A control angiogram 6 months after treatment showed thrombosis of the parent vessel. The parent vessel was patent in the immediate postprocedural angiogram, thus had late thrombus formation.
Nineteen patients with fusiform (4) and saccular aneurysms with incorporated origins of the distal branches (15) underwent parent artery occlusion (PAO). Three patients, 2 with distally located MCA aneurysms and 1 with P2 aneurysm underwent balloon test occlusion. All parent vessel test occlusions included angiographic assessment of collateral blood flow as well as clinical monitoring.
Fifteen PAOs were performed with GDCs and 4 with glue. We find glue to be efficient for very distally located aneurysms in small arteries, where occlusion of parent vessel at the level of the aneurysmal neck was decided. A 50% mixture of glue was used in all cases. Slow injection of the glue allows filling of the aneurysm without distal migration or reflux into the parent vessel. Antithrombotic medication (heparin, low-molecular-weight heparin, aspirin, or clopidogrel) was not given postoperatively.
All patients who underwent selective coil embolization of the aneurysm had follow-up angiogram 6–12 months later. All patients who underwent PAO had CT scans 48 hours, 3 months, and 1 year after treatment and follow-up angiograms 6 months after the procedure. Five patients also had follow-up MR images.
In 1 patient with an MCA aneurysm, spontaneous thrombosis of the aneurysm and the distal branch of the MCA were seen at the time of planned embolization 1 day after the diagnostic angiogram. Further follow-up angiograms 15 days, 3 months, and 6 months later were stable.
Results
Immediate Angiographic Results
Selective Coil Embolization.
Seven patients (3 PCA aneurysms, 3 PICA aneurysms, and 1 AICA aneurysm) were treated with selective coil embolization of the aneurysmal sac. Complete occlusion was achieved in 5 patients, and neck remnant was evident in 2 patients. In 2 of these patients treated with selective coil embolization, follow-up angiogram 6 months after treatment showed occlusion of the parent artery that was not evident in the immediate postprocedural angiogram. Thus there was late thrombus formation. Both patients with late thrombosis of the parent artery remained asymptomatic.
Parent Artery Occlusion.
Nineteen patients (6 PCA, 4 MCA, 5 SCA, 2 ACA, and 2 PICA aneurysms) underwent PAO. Angiograms obtained immediately after treatment showed occlusion of the aneurysm and retrograde filling of the vessel. One patient had spontaneous thrombosis of the aneurysm and the distal branch of the MCA.
Procedural Complications
One complication related to the procedure occurred. One 44-year-old male patient (patient 22) with an MCA aneurysm developed severe spasm of the MCA during parent vessel occlusion test immediately after the first inflation of the balloon just proximal to the aneurysmal neck. The patient developed transient hemiparesis. The spasm resolved with the administration of papaverine intra-arterially, and the symptoms resolved completely within a few minutes. After resolution of symptoms, the balloon test occlusion was repeated successfully without further complication, and retrograde filling of the branch distal to the aneurysm was demonstrated. In the same sitting, the patient underwent PAO.
Immediate Clinical Outcome
Selective Coil Embolization.
No patient who underwent selective coil embolization developed neurologic deficits related to the procedure.
Parent Artery Occlusion.
Five patients who underwent PAO developed neurologic deficits after treatment. Two patients (1 and 4) with SCA aneurysms developed ataxia, and the CT scan performed 48 hours after the procedure showed a cerebellar infarct. Three patients with distally located PCA aneurysm (12, 18, and 19) developed neurologic deficits 72 hours (patient 12) and 24 hours (18 and 19) after treatment. Patient 12 developed mild right-sided hemiparesis, and CT scan showed a small thalamic infarct. Patient 18 developed right-sided hemiparesis and homonymous hemianopsia. The CT scan revealed an occipital and a thalamic infarct. Patient 19 developed a visual field defect, and a small occipital infarct was detected on follow-up CT.
Clinical Follow-Up
The clinical follow-up ranged from 3 to 61 months. One patient with grade IV (Hunt and Hess) subarachnoid hemorrhage died 10 days later from sepsis. All other patients had good neurologic recovery. Only 2 patients with P2 aneurysm (18 and 19) had a permanent neurologic deficit (visual field defect).
Imaging Follow-Up
Selective Coil Embolization.
All patients who underwent selective coil embolization of the aneurysm had a follow-up angiogram 6–12 months after the operation. There was no recanalization of the embolized aneurysm on any of the follow-up studies. Control angiogram 6 months after treatment for the 2 patients with neck remnants in postprocedural angiography showed that the degree of occlusion remained unchanged.
In 2 patients (7 and 8) with PICA aneurysm, treated initially with selective embolization of the aneurysm, control angiogram 6 months after treatment showed thrombosis of the parent vessel. This was not evident in the immediate postprocedural angiogram because of late thrombus formation. The distal part of the thrombosed vessel filled retrogradely. The patients remained asymptomatic and CT scans were normal.
Parent Artery Occlusion.
All patients who underwent PAO had CT scans 48 hours, 3 months, and 1 year after treatment and follow-up angiograms 6 months after treatment. Five patients had follow-up MR images also.
Two of these patients with a peripheral SCA aneurysm and 3 with a PCA aneurysm developed infarcts after PAO that were detected on follow-up CT and/or MR images. On follow-up angiograms, occlusion of the parent artery remained stable, and none of the aneurysms refilled by a retrograde or leptomeningeal collateral supply.
Discussion
Cerebral aneurysms located distally are rare.1 Distal aneurysms represent approximately 7%–9% of anterior cerebral artery aneurysms, 2%–7% of MCA aneurysms, and 5% of PCA aneurysms.2 Aneurysms of the cerebellar arteries are also rare. PICA aneurysms are the most frequent among these (<1%), and most are located at the origin of the PICA. Distally located PICA aneurysms represent less than a fifth of PICA aneurysms.3 At our institution, 27 patients with peripheral aneurysms not related to arteriovenous malformations and nonmycotic in origin were included in our study.
Distally located aneurysms can be difficult to treat with embolization techniques that spare the parent artery. In these cases, PAO has been suggested as an alternative treatment. In our series, selective embolization of the aneurysmal sac was successfully performed in 7 patients. In general, the main limitation of selective embolization is the morphology of the aneurysm and the size of the aneurysmal neck in relation to the diameter of the parent vessel. In these cases, endovascular parent vessel occlusion has been suggested as an alternative treatment.4 This technique has been frequently reported in the literature for treatment of aneurysms of the cavernous or paraclinoid internal carotid artery and for aneurysms involving the vertebrobasilar junction.4 Parent vessel occlusion for the treatment of distally located aneurysms has been reported less frequently. Cloft et al5 reported 2 cases with peripheral ruptured cerebral aneurysms, 1 PCA and 1 AICA, that were treated endovascularly with parent vessel occlusion with short GDCs. Eckard et al4 reported 9 patients with peripheral aneurysms. All patients were treated endovascularly with PAO using microcoils after test injection with amobarbital. Peripheral vessel occlusion for mycotic aneurysms has also been reported previously. Khayata et al6 reported on 3 patients with mycotic aneurysms. Two of these aneurysms were treated with parent vessel occlusion and the third by placing a detachable balloon within the aneurysm.
In our group of patients, PAO was planned after detailed evaluation of the aneurysm and its relations to the parent artery and the distal branches rendered selective occlusion of the sac predictively impossible. The evaluation included CTA, DSA, and selective angiograms. Fusiform aneurysms, saccular aneurysms that incorporate the origins of distal branches, and wide-necked aneurysms arising from small diameter distal branches were treated by PAO. The aim of embolization in these cases is to occlude the aneurysm and the parent artery in front of the aneurysmal neck. The proximal portion of the vessel, as well as the perforating arteries arising from these arterial segments, remains patent, and the distal segments fill retrogradely from the pial collateral circulation.
The potential risk of this technique is ischemia in the parent vessel territory. Many authors supported the idea that the endovascular approach allows functional investigation of the artery and its distal territory before occlusion and suggested amobarbital test or balloon test occlusion in cooperative patients with close neurologic monitoring before PAO. Eckard et al4 monitored the neurologic statuses in 8 of 9 patients before final placement of coils and PAO by using an amobarbital injection. They concluded that amobarbital testing is overly predictive of deficits owing to its deep penetration into all of the peripheral vessels, and when the vessel is actually occluded, collaterals may partially bypass the occlusion. They suggested performing the amobarbital testing to get an idea of the deficit the patient might expect when the artery was occluded. Hallacq et al7 performed balloon test occlusion in 5 of 9 patients who underwent parent artery occlusion for P2 segment aneurysms. In our 19 patients who underwent PAO, we performed balloon test occlusion in 2 patients with distally located MCA aneurysms and in 1 with a P2 fusiform aneurysm. In 1 patient (patient 18) with a P2 aneurysm, balloon test occlusion revealed poor collateral supply, but PAO was performed because the patient declined any surgical intervention, including bypass surgery. The patient had significant neurologic deficits after PAO (visual field defect and mild right-sided hemiparesis, which improved 1 month after treatment). We believe that this test is useful to assess the leptomeningeal collateral supply but should not be critical for treatment planning because it may give false-positive or false-negative results and because, in many cases, the treatment remains the same even if the test is not tolerated. The lack of adequate information in the literature about the clinical consequences of PAO in the treatment of distal aneurysms led us to use balloon test occlusion in preparation for PAO in our early cases, but we no longer use it routinely.
We reviewed the results from the most recent series according to the location of the aneurysms and therefore divided the peripheral aneurysms into 4 groups: cerebellar, PCA, MCA, and ACA aneurysms.
Lubicz et al3 reported 3 peripheral cerebellar aneurysms that were treated with PAO, 2 PICA and 1 AICA, with excellent clinical outcome. Cognard et al2 reported treatment of a distal SCA aneurysm with PAO by glue injection. The patient developed left-sided hemiparesis that resolved within 3 days. Zager et al8 reported 4 patients with distal AICA aneurysms. One patient underwent coil embolization of the distal AICA and the aneurysm, without neurologic deficit. Eckard et al4 reported 4 distal cerebellar aneurysms: 1 SCA, 2 PICAs, and one AICA. All patients were treated with PAO, and postprocedural course was uneventful. Chapoulka et al1 described 2 cases of peripheral SCA aneurysms that were treated successfully with PAO. The first patient developed a right cerebellar hemisphere infarction and the second patient developed ataxia though serial CT scan showed no evidence of cerebellar infarction (Table 2). Our group included 11 patients with peripheral cerebellar aneurysms. Five SCA and 2 PICA aneurysms were treated with PAO. Two patients with SCA aneurysms (2/5) developed mild cerebellar symptoms, and CT scans showed cerebellar infarcts. Two other patients (7 and 8) with PICA aneurysm underwent selective embolization of the aneurysm. Control angiogram 6 months after treatment showed occlusion of the parent vessel that was not evident in the immediate postprocedural angiogram because of delayed propagation of thrombus. The distal part of the vessel filled retrogradely. These patients remained asymptomatic and CT scans were normal (Table 2).
Table 2:
Reported complications in patients with peripheral cerebellar aneurysms treated with parent artery occlusion
| Series | PICA | AICA | SCA | Complications |
|---|---|---|---|---|
| Lubicz et al3 | 2 | 1 | AICA: VIIth nerve palsy (persisted) | |
| Cognard et al2 | 1 | Slight left-side hemiparesis (resolved) | ||
| Zager et al8 | 1 | |||
| Eckard et al4 | 2 | 1 | 1 | SCA, mild dysmetria (resolved); AICA, decreased hearing (persisted) |
| Cloft et al5 | 1 | |||
| Chapoulka et al1 | 2 | 1 pt, mild cerebellar dysfunction | ||
| Present study | 4 | 1 | 5 | 2 pts, SCA, ataxia (resolved) |
Note:—PICA indicates posterior inferior cerebellar artery; AICA, anterior inferior cerebellar artery; SCA indicates superior cerebellar artery; pt, patient; pts, patients.
Aneurysms of the PCA mostly arise from P2-related sites and are more likely to be fusiform or giant compared with other cerebral aneurysms. Arat et al9 reported 8 patients with large-giant or fusiform distal PCA aneurysms who were treated with PAO. Three patients (3/8) developed infarcts, 1 occipital and 2 thalamic, that were detected in postprocedure imaging. Only 1 of these 8 patients developed symptoms (homonymous hemianopsia) that did not resolve. Hallacq et al7 reported the result of endovascular treatment of 10 patients with P2 segment aneurysms. Nine of them were treated with PAO at the level of the aneurysmal neck, and all tolerated the procedure well. Test occlusion was performed in 5 patients, and the anatomy of leptomeningeal collateral supply was evaluated. The authors concluded that acute parent artery occlusion appears to be safe in the treatment of P2 segment aneurysms, whatever the location of the occlusion. Ciceri et al10 presented their experience in the endovascular treatment of PCA aneurysms. Six patients with distal PCA aneurysms were treated with PAO. Two of them developed permanent neurologic deficit because of PAO (homonymous hemianopsia in both patients and contralateral hemiparesis in 1). The authors suggested that the low incidence of visual field defect complicating PAO is related to the rich anastomotic collaterals that exist between the PCA and other arteries. Our series includes 9 patients with distal PCA aneurysms; 6 were treated with PAO and 3 with selective obliteration of the aneurysmal sac. Three patients developed infarcts: 1 patient thalamic, 1 patient occipital, and 1 patient occipital and thalamic infarcts. Two of them (2/6) had residual neurologic symptoms (a visual field defect). The incidence of permanent neurologic deficit (visual field defect) in our group of patients with distal PCA aneurysms treated with PAO (2/6 or 33%) was similar to that reported by Ciceri et al10 (2/6 or 33%). We agree with their conclusion that it is impossible to be certain whether a PAO will be tolerated. The anastomotic collaterals that exist between PCA territory and that of other arteries cannot be adequately evaluated before a planned artery occlusion (Table 3).
Table 3:
Reported complications in patients with peripheral PCA aneurysms treated with parent artery occlusion
| PCA | Complications | |
|---|---|---|
| Arat et al9 | 8 | 1 pt: hemianopsia—occipital infarct1 pt: transient hemiparesis—thalamic infarct |
| Hallacq et al7 | 9 | None |
| Ekcard et al4 | 3 | 1 pt: visual field cut |
| Cloft et al5 | 1 | None |
| Ciceri et al10 | 6 | 1 pt: hemianopsia & hemiparesis1 pt: hemianopsia |
| Present study | 6 | 1 pt: transient hemiparesis—thalamic infarct1 pt: transient hemiparesis & hemianopsia—thalamic & occipital infarct1 pt: hemianopsia—occipital infarct |
Note:—PCA indicates posterior cerebral artery; pt, patient.
For peripheral MCA and ACA aneurysms, PAO is considered a safe alternative treatment. We treated 4 patients with peripheral MCA aneurysms and 2 with peripheral ACA aneurysms. All 6 patients’ posttreatment courses were uneventful. Similar results were reported by Eckard et al (1 MCA and 1 ACA aneurysm) and Khayata et al (with 2 MCA mycotic aneurysms) who treated these aneurysms with PAO.
To avoid any infarction from proximal occlusion of the parent vessel, some authors advocate aneurysmal excision with end-to-end anastomosis of the parent artery, or bypass surgery. However, the morbidity and mortality of reconstructive surgical treatment is considerable in these aneurysms (36%),9 whereas the ischemic complications from PAO are acceptable and, with neurologic recovery over time, ultimately of limited clinical significance. Thus, PAO should be considered a therapeutic option for distal cerebral aneurysms because it is relatively safe and effective and carries acceptable morbidity and mortality.
Fig 1.

Patient 5: subarachnoid hemorrhage (Hunt and Hess grade II) in a 73-year-old female patient.
A and B, Left vertebral artery angiogram (lateral and anteroposterior views) shows distal aneurysm of the left superior cerebellar artery.
C, Intra-aneurysmal contrast injection shows opacification of the aneurysm and the distal branch.
D and E, After intra-aneurysmal glue injection left vertebral angiogram (lateral and anteroposterior views) shows complete obliteration of the aneurysm.
Fig 2.

Patient 17: 23-year-old male patient with visual disturbances.
A and B, Left vertebral lateral and anteroposterior angiogram shows a distal aneurysm of the right PCA.
C, Selective opacification of the aneurysm and the distal branch.
D and E, After intra-aneurysmal injection of glue, left vertebral artery angiogram (lateral and AP view) shows complete occlusion of the aneurysm.
F, Lateral angiogram of the right ICA shows retrograde filling of the part of the PCA distal to the occluded aneurysm.
Fig 3.
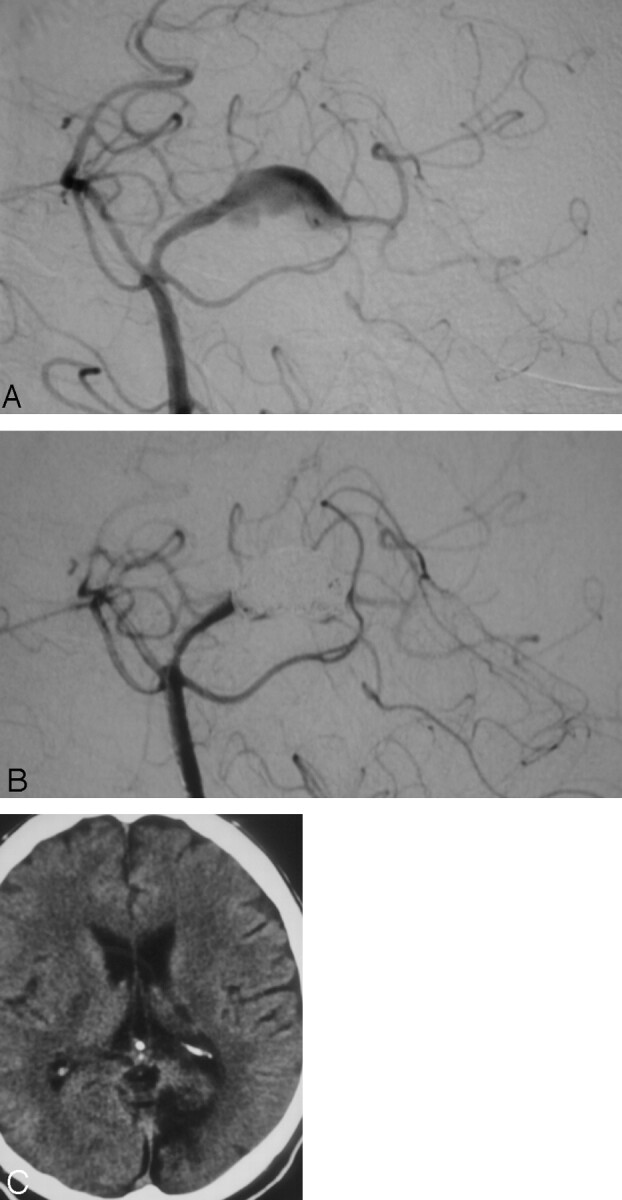
Patient 18: 49-year-old male patient with cranial nerve III nerve palsy.
A and B, Left vertebral oblique views before and after coil embolization.
C, Noncontrast CT scan 2 months after embolization shows a left occipital and left thalamic infarct.
References
- 1.Chapoulka J, Putman C, Awad I. Endovascular therapeutic approach to peripheral aneurysms of the superior cerebellar artery. AJNR Am J Neuroradiol 1996;17:1338–42 [PMC free article] [PubMed] [Google Scholar]
- 2.Cognard C, Weill A, Tovi M, et al. Treatment of distal aneurysms of the cerebellar arteries by intraaneurysmal injection of glue. AJNR Am J Neuroradiol 1999;20:780–84 [PMC free article] [PubMed] [Google Scholar]
- 3.Lubicz B, Leclerc X, Gauvrit J, et al. Endovascular treatment of peripheral cerebellar artery aneurysms. AJNR Am J Neuroradiol 2003;24:1208–13 [PMC free article] [PubMed] [Google Scholar]
- 4.Eckard D, O’Boynick P, McPherson C, et al. Coil occlusion of the parent artery for the treatment of symptomatic peripheral intracranial aneurysms. AJNR Am J Neuroradiol 2000;21:137–42 [PMC free article] [PubMed] [Google Scholar]
- 5.Cloft H, Kallmes D, Jensen M, et al. Endovascular treatment of ruptured peripheral cerebral aneurysms: parent artery occlusion with short Guglielmi detachable coils. AJNR Am J Neuroradiol 1999;20:308–10 [PMC free article] [PubMed] [Google Scholar]
- 6.Khayata M, Aymard A, Casasco A, et al. Selective endovascular techniques in the treatment of cerebral mycotic aneurysms. J Neurosurg 1993;78:661–65 [DOI] [PubMed] [Google Scholar]
- 7.Hallacq P, Piotin M, Moret J. Endovascular occlusion of the posterior cerebral artery for the treatment of P2 segment aneurysms: retrospective review of 10-year series. AJNR Am J Neuroradiol 2002;23:1128–36 [PMC free article] [PubMed] [Google Scholar]
- 8.Zager E, Shaver E, Hurst R, et al. Distal anterior inferior cerebellar artery aneurysms. Report of four cases. J Neurosurg 2002;97:692–96 [DOI] [PubMed] [Google Scholar]
- 9.Arat A, Islak C, Saatci I, et al. Endovascular parent artery occlusion in large-giant or fusiform distal posterior cerebral artery aneurysms. Neuroradiology 2002;44:700–05 [DOI] [PubMed] [Google Scholar]
- 10.Ciceri E, Klucznik R, Grossman R, et al. Aneurysms of the posterior cerebral artery: Classification and endovascular treatment. AJNR Am J Neuroradiol 2001;22:27–34 [PMC free article] [PubMed] [Google Scholar]