

Abstract
SUMMARY: We present a 75-year-old man who, for 2 weeks, had progressive pain in both of his thighs when standing straight. MR imaging showed a sequestrated disk fragment, which had a signal intensity similar to that of a herniated disk with a rim enhancement in the posterior epidural space and a ruptured outermost annulus of the intervertebral disk at L2–3. Awareness of these MR imaging findings can help in the diagnosis of posterior epidural disk migration.
Disk fragment migration is generally contained in the anterior epidural space, which is well-defined and delimited by the posterior longitudinal ligament and by lateral membranes attached to it.1 Posterior epidural migration of a sequestrated disk fragment to the posterior epidural space is rare. Previously reported cases were of middle-aged adults who presented with radiculopathy of relatively short duration.2–4 In this report, we present the indications for diagnosing posterior epidural migration of a sequestrated disk fragment on MR imaging.
Case Report
A 75-year-old man had progressive pain over his thighs bilaterally when standing. This pain could be relieved by changing his position, especially by bending at the waist. No urinary incontinence was noted. Physical examination revealed full muscle power and intact sensation of the lower extremities. Laboratory tests revealed no abnormal findings.
MR imaging of the lumbar spine showed a right posterior epidural mass lesion, measuring 2.7 × 1.6 × 1.0 cm, at L2–3. The lesion exhibited an isointense signal intensity relative to the intervertebral disk on both T1- and T2-weighted images and had a rim enhancement on gadolinium-enhanced T1-weighted images. A disrupted outermost annulus of the adjacent disk and a tractlike enhancement leading to the right posterior epidural space were noted (Fig 1A–E). Our preoperative diagnosis was a posterior epidural migration of a sequestrated lumbar disk fragment.
Fig 1.
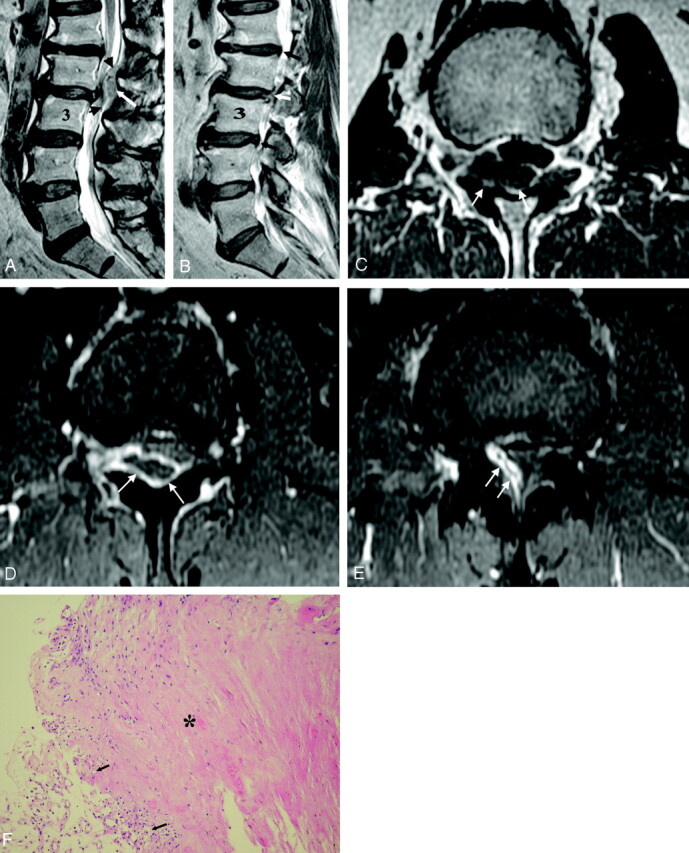
A 75-year-old man with a posterior epidural disk migration.
A, Sagittal T2-weighted (TR/TE, 4000/119.8) fast spin-echo MR image of the lumbar spine at the midline plane reveals a mass lesion (arrow) with isointensity relative to the intervertebral disk at the posterior epidural space at the L2–3 level, compressing the dura (arrowheads).
B, Right parasagittal T2-weighted image shows a disrupted outermost annulus fibrosus (white arrow) of the intervertebral disk at L2–3. By comparison, the intact outermost annulus fibrosus (black arrows) is shown as a delicate dark line along the margin of the disk at adjacent L1–2 and L3–4 levels.
C, Axial T1-weighted (TR/TE, 600/10.42) fast spin-echo MR image obtained at the level of the migrating disk fragment shows an irregularly shaped mass lesion (arrows), with an isointense signal intensity relative to the intervertebral disk at the right posterior epidural space, which is contrasted by high-signal-intensity epidural fat.
D, Axial gadolinium-enhanced T1-weighted (TR/TE, 466.7/10.22) MR image with fat saturation at the disk fragment level shows a rim enhancement of the epidural disk material (arrows).
E, The same pulse sequence MR image obtained at a higher level than that in D at the intervertebral disk shows a tractlike enhancement (arrows) from the site behind the ruptured annulus fibrosus to the right posterior epidural space, indicating the route of disk migration.
F, Photomicrograph of the surgical specimen shows increased vasculature (arrows) and focal mild lymphocytic infiltration at the edge of the degenerated fibrocartilage (asterisk) (H&E, original magnification ×100).
Three days later, the patient underwent total laminectomy at L2 and diskectomy at L2–3. At surgery, a right paramedian ruptured disk compressing the swollen L3 nerve root was seen. The ruptured fragment was recognized along the right lateral recess to the posterior epidural space. Histopathologic findings of the surgical specimen revealed degenerated fibrocartilage and increased vascularity and lymphocytes at the edge of the disk materials (Fig 1F).
The postoperative course was smooth and the patient’s symptom was relieved.
Discussion
Disk sequestration can be defined as a herniated disk with perforation of the fibrous ring (or outermost annulus fibrosus) and posterior longitudinal ligament with migration of the disk fragment to the epidural space.2 The most common path of disk fragment migration is a posterior and posterolateral direction to the anterior epidural space, which is delimited by the attachment of the posterior longitudinal ligament and its associated “midline septum” and “lateral membranes.”1,4,5 Therefore, disk fragment migration usually occurs cranial, caudal, or lateral but seldom posterior to the anterior epidural space. Migration of a sequestrated disk fragment in this manner has been reported only rarely.2–4 Most of the reported cases have involved the lumbar region, and a few cases with cauda equina syndrome have been described.2–4
Myelography typically can show a complete block of the contrast medium at the level of disk herniation or sequestration, but it is unable to characterize the nature of the compression.6,7 Findings of CT or CT myelography are inconclusive because of its limitation in recognizing the extradural migrated fragment as a mass compressing the dural sac; therefore, a differential diagnosis may include primary or metastatic tumors, synovial cyst, dural abscess, or hematoma.3
MR imaging, especially with gadolinium administration, appears to be the method of choice for diagnosis. Sequestrated fragments usually show low signal intensity on T1-weighted images, and 80% of cases exhibit high signal intensity on T2-weighted images relative to the degenerated disk of origin.8 The high signal intensity on T2-weighted images can be explained as either the herniated material still having a higher water content than an intact disk or a reparative process leading to a transient water gain.8 The remaining 20% had isointense signal intensity relative to the degenerated disk on T2-weighted images8; a similar finding was also noted in our patient. Most of the disk fragments show peripheral contrast enhancement attributed to an inflammatory response with granulation tissue and newly formed vessels around the sequestrated tissue,9,10 as shown in the present report.
On the other hand, tumors usually enhance uniformly on gadolinium MR images. Synovial cysts have a characteristic MR imaging signal intensity, and they are related to the facet joint. An epidural abscess could present as a mass with hypointensity on T1-weighted imaging, hyperintensity on T2-weighted imaging, and rim enhancement; however, the lack of associated change in the disk and adjacent endplates and the lack of clinical findings of infection suggest another diagnosis.11 Hematoma usually has isointensity or hyperintensity on T1-weighted imaging, no enhancement, and an associated trauma history.2,3
Three cases of posterior epidural disk migration at the L2–3 level have been reported.3,4 Other levels of this condition involving T7–8 and L3–4 also have been described previously.2,3 Most of the migrations have occurred on the left side. In previously reported cases,2–4 the disk fragments measured up to 2.5 cm, and most gave low signal intensity on T1-weighted images and moderately high signal intensity on T2-weighted images and had a rim contrast enhancement on gadolinium-enhanced images. One report revealed that the lesion displayed low signal intensity on T2-weighted and T1-weighted images and showed rim enhancement after administration of gadolinium,4 similar to the MR imaging signal intensity noted in our case.
In our patient, rim enhancement of the migrating free fragment was also noted. In addition, a tractlike structure with enhancement from the site of the ruptured disk to the posterior epidural space was identified, suggesting the route of the sequestrated disk migration. The contrast rim enhancement can be attributed to the increased vascularized epidural tissue wrapping the disk contents,4,9,10 as documented in our histopathologic findings (Fig 1F).
Most of the previously reported cases with posterior epidural disk migration presented with a relatively short duration of symptoms of radiculopathy and muscle power deficit of the affected limb in a middle-aged individual.2–4 Our patient, however, was older and had a longer duration of milder symptoms. Prompt surgery is the treatment of choice for best recovery.
References
- 1.Schellinger D, Manz HJ, Vidic B, et al. Disc fragment migration. Radiology 1990;175:831−36 [DOI] [PubMed] [Google Scholar]
- 2.Dosoglu M, Is M, Gezen F, et al. Posterior epidural migration of a lumbar disc fragment causing cauda equina syndrome: case report and review of the relevant literature. Eur Spine J 2001;10:348−51 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Neugroschl C, Kehrli P, Gigaud M, et al. Posterior extradural migration of extruded thoracic and lumbar disc fragments: role of MRI. Neuroradiol 1999;41:630−35 [DOI] [PubMed] [Google Scholar]
- 4.Bonaroti EA, Welch WC. Posterior epidural migration of an extruded lumbar disc fragment causing cauda equina syndrome: clinical and magnetic resonance imaging evaluation. Spine 1998;23:378−81 [DOI] [PubMed] [Google Scholar]
- 5.Sarlieve P, Delabrousse E, Clair C, et al. Intradural disc herniation with cranial migration of an excluded fragment. Clin Imaging 2004;28:170−72 [DOI] [PubMed] [Google Scholar]
- 6.Branam BR, Stambough JL. Atypical lumbar disc herniation: a case report. Spine J 2002;2:224−26 [DOI] [PubMed] [Google Scholar]
- 7.Lutz JD, Smith RR, Jones HM. CT myelography of a fragment of a lumbar disk sequestrated posterior to the thecal sac. AJNR Am J Neuroradiol 1990;11:610−11 [PMC free article] [PubMed] [Google Scholar]
- 8.Masaryk TJ, Ross JS, Modic MT, et al. High-resolution MR imaging of sequestered lumbar intervertebral disks. AJNR Am J Neuroradiol 1988;9:351–58 [DOI] [PubMed] [Google Scholar]
- 9.Hwang GJ, Suh JS, Na JB, et al. Contrast enhancement pattern and frequency of previously unoperated lumbar discs on MRI. J Magn Reson Imaging 1997;7:575−78 [DOI] [PubMed] [Google Scholar]
- 10.Wasserstrom R, Mamourian AC, Black JF, et al. Intradural lumbar disk fragment with ring enhancement on MR. AJNR Am J Neuroradiol 1993;14:401−04 [PMC free article] [PubMed] [Google Scholar]
- 11.Sandhu FS, Dillon WP. Spinal epidural abscess: evaluation with contrast-enhanced MR imaging. AJNR Am J Neuroradiol 1991;12:1087−93 [PMC free article] [PubMed] [Google Scholar]