

Abstract
Background
University students with depression and anxiety do not easily receive or seek treatment; therefore, internet-based interventions have been suggested to be a promising way to improve treatment accessibility and availability. However, it has not been examined whether a guided, culturally adapted, transdiagnostic, internet-based intervention is effective for treating symptoms of depression, anxiety, or both among university students in Indonesia.
Objective
This study aims to investigate the feasibility (acceptability and satisfaction, usability, and uptake) of a guided, culturally adapted, transdiagnostic, internet-based intervention among university students with symptoms of depression, anxiety, or both in Indonesia.
Methods
Students from Universitas Gadjah Mada, Yogyakarta, Indonesia, were screened for symptoms of depression, anxiety, or both, and filled online informed consent, demographic questionnaires, and a quality of life measure at pretreatment assessment (T0). Subsequently, the participants started the intervention. Seven weeks after T0, the primary outcomes of this feasibility study were analyzed at posttreatment assessment (T1) using the 8-item Client Satisfaction Questionnaire (CSQ-8) and the System Usability Scale (SUS). Mean and SDs for the CSQ-8 and SUS were calculated to examine feasibility. Within-group secondary outcomes (depression, anxiety, and quality of life) were inspected for outliers and normal distribution. Paired-sample t tests were used to investigate differences between time points of secondary outcomes. A mixed-method approach of quantitative and qualitative analyses was adopted. Both the primary and secondary outcomes were additionally explored with an individual semistructured interview and synthesized descriptively.
Results
A total of 50 participants completed the intervention. We found a moderate to high level of satisfaction and acceptability, a slightly below-average level of desirable usability (≥70), and an adherence rate of 52% which was higher than expected given the novelty of the intervention. Results for the secondary outcomes indicated a decrease in depression and anxiety. For depression, the overall mean difference between the 2 time points for depression was 3.92 (95% CI 2.75-5.1; Hedges g 1.15; P<.001). For anxiety, the overall mean difference between the 2 time points was 3.34 (95% CI 2.06-4.61; Hedges g 1.02; P<.001). Further, a moderate effect in improving quality of life was found (g=0.50). Overall, participants were positive about the online intervention and ECoaches (online guidance), and they found the intervention to be culturally appropriate.
Conclusions
A culturally adapted, transdiagnostic, internet-based intervention appears to be acceptable and feasible for reducing symptoms of depression, anxiety, or both, and increasing quality of life in university students in Indonesia. Future studies should include a randomized controlled trial to assess the effectiveness of such interventions as they may supplement existing counseling services in universities, reduce the treatment costs, and maximize treatment accessibility in low-resourced settings.
International Registered Report Identifier (IRRID)
RR2-10.1016/j.invent.2018.11.002
Keywords: anxiety, cultural adaptation, depression, guided, internet-based intervention, transdiagnostic, university students
Introduction
University students may experience common mental health disorders such as depression and anxiety [1-3]. Epidemiological studies [4] have shown that depression and anxiety are prevalent in college students (31%). This percentage is significantly larger when compared with nonstudents (21.4%) in the same age group [5]. The prevalence of anxiety and depression among university students may be influenced by the complexity of the transition from late adolescence to young adulthood [6]. This common mental health risk has been associated with academic demands [7], social adjustment [8], and financial challenges that students may face [9]. Depression and anxiety can be effectively treated with either pharmacotherapy or psychotherapy [10]. This is in line with the biopsychosocial approach suggested by the World Health Organization (WHO) for managing common mental disorders. The biopsychosocial approach promotes a thorough understanding that mental health issues are an outcome of biological, psychological, and social factors [11]. Effective treatment is imperative as it may prevent a series of negative cascades, such as poor academic adjustment, study dropout, and chronicity [12,13]. Many universities have counseling services that play an important role in improving mental health care by providing effective, accessible, and confidential ways to detect, prevent, and treat common mental disorders in students. The effectiveness of university counseling services for students with high levels of distress has been reported [14]. However, most university students do not receive or seek treatment at counseling services for their psychological problems [6] due to stigma, lack of time, lack of motivation, or they have a preference for a self-management approach [15]. In addition, the low university mental health service availability and high underutilization are very common in non-Western countries [16,17]. In Indonesia, university counseling services are unevenly distributed across universities, as they are mostly dependent on the presence and service of faculties of psychology in the universities.
Therefore, novel therapeutic delivery formats for university students with depression and anxiety may be a feasible way to improve treatment accessibility. Digital technologies offer an excellent opportunity for improving treatment availability and accessibility, especially in low- and middle-income countries, given the widespread acceptance of internet and mobile phone use among university students. Studies on interventions delivered via the internet have shown promising outcomes for students in Western countries due to their anonymity, accessibility, and adaptability to student needs [18,19]. Another known characteristic of internet-based interventions is that they can also be delivered with some form of human guidance (eg, by an ECoach) or can be purely self-guided [20]. Guided internet-based interventions were reported to be more effective compared to self-guided interventions, possibly because participants receive feedback and motivation, and this encourages them to proceed with the sessions and understand the content of the intervention better [21].
For Indonesian university students, internet-based interventions may have a high level of feasibility for a number of reasons. First, internet use is widespread among Indonesian university students (74.23% use the internet), compared to the general Indonesian population, with 94% of them using the internet on their mobile phones [22]. Second, guided internet-based interventions may be more attractive than face-to-face treatment in and outside the university, as the latter involves a high cost that might not be affordable for Indonesian students. Thus, internet-based interventions may be more favorable because they include minimal asynchronous support at a much lower cost than face-to-face interventions. Besides, such interventions can be accessed anywhere [20,23], at any time, and are thus more flexible for students who have very demanding daily schedules at the university.
Third, online interventions can reduce the fear of being exposed to others because students can access the online interventions anonymously [23]. By contrast, students may not utilize internet interventions for a number of reasons including time constraints due to their study duties, lack of nonverbal communication with the ECoach, and the high demand of self-discipline associated with self-help interventions [24]. Fourth, in Indonesia, internet-based interventions for depression and anxiety are currently not available for either university students or for the general population. The first randomized control trial on internet-based behavioral activation for adult depression in Indonesia [25,26] showed promising results with lower symptoms at posttest assessment in favor of the intervention with minimum support by a lay counselor who did not have professional education and qualifications in mental health care. However, the intervention was tested in the general population, and thus, it remains unclear whether these interventions are also effective in university students with elevated symptoms of depression and anxiety. Additionally, given that depression and anxiety are highly comorbid conditions [27,28], a transdiagnostic approach could be beneficial as it targets both symptoms of depression and anxiety simultaneously. Findings on transdiagnostic interventions for university students in Western countries with common mental disorders have been encouraging. More specifically, such interventions have shown to reduce symptoms of common mental disorders with moderate to large effect sizes in the range of 0.42-0.80 for outcomes such as depression and anxiety [23,29-31].
To the best of our knowledge, it has not yet been examined whether guided, culturally adapted, transdiagnostic, internet-based interventions are feasible in treating symptoms of depression or anxiety or both among university students in non-Western countries, such as Indonesia. Therefore, in this pilot study, we aimed to investigate the feasibility (defined as acceptability, satisfaction, usability, and uptake) of a guided, culturally adapted, transdiagnostic internet-based intervention among university students with symptoms of depression, anxiety, or both in Indonesia. This paper reports the results of stage 3 from a theory-based cultural adaption framework, namely, preliminary adaptation test [32]. The first 2 stages of the framework, namely, information gathering and preliminary adaptation design, are reported in the protocol paper of this study [33].
Methods
Participants
Participants were recruited via our study website [34], which was disseminated on posters, social media platforms, and business cards containing brief information about the study. As we described in our protocol [33], there is no golden standard for calculating the sample size of a pilot study [35]. For our study, we performed a post hoc power calculation to describe statistically the power of our chosen sample (n=50 participants). Further details can be found in our study protocol [33]. Participants were eligible if they (1) were students at Universitas Gadjah Mada Yogyakarta with access to broadband internet, (2) were 18 years of age or older, (3) could speak and read Bahasa Indonesia fluently, and (4) experienced mild to moderate depression, anxiety, or both (9-item Patient Health Questionnaire [PHQ-9] score >4, 7-item Generalized Anxiety Disorder [GAD-7] score >4, or both). Exclusion criteria were (1) moderately severe depression, anxiety, or both (PHQ-9 score >14, GAD-7 score >14, or both) and (2) currently receiving psychological treatment for depression, anxiety, or both.
Procedures
Students who were interested in participating in the pilot study filled in their demographic details on the digital registration form on our study website. Subsequently, the students received an email with a link, which directed them to the pretreatment assessment (T0) consisting of the study’s screening questionnaires: the Indonesian version of the PHQ-9 [36,37] and the GAD-7 scale [36,37]. After completing the PHQ-9 and GAD-7 at the screening, participants were asked to provide an informed consent for using their responses to these questionnaires in our analyses (retrospectively). For pragmatic reasons, these eligibility screening scores were also used as a baseline assessment for included participants. Subsequently, an information sheet was provided to them through an emailed link containing an explanation of the study and an online informed consent form that needed to be signed before being able to participate. Those who consented to participate received additional questions about their demographics and quality of life using the Indonesian version of the Euro Quality of Life 5 Dimension-5 Level Scale (EQ5D5L) [38]. The EQ5D5L was used because performance and changes in mental health are captured through one of its dimensions (depression/anxiety) and it is a widely used generic quality of life scale that is also usable for health economic calculations. After completing these additional questionnaires, participants were assigned online to an ECoach (a trained Clinical Psychology Master’s student from the Faculty of Psychology at Universitas Gadjah Mada or a licensed Psychologist) and were given secure login details. Subsequently, the I-AiMentalWELLness (Saya menuju mental sehat) online intervention was activated for them through Mind District [39], an eHealth platform providing digital therapy.
The posttreatment assessment (T1) was given 7 weeks after the pretreatment assessment (T0) and consisted of the primary outcomes of this feasibility study, namely, participants’ reported acceptability and satisfaction, usability, and uptake.
Further details about the procedures of this pilot study can be found in our protocol paper [33]. Ethical approval was obtained from the Medical and Health Research Committee of the Medical Faculty in Universitas Gadjah Mada/DR Sardjito General Hospital (reference number: KE/FK/0098/EC/2018).
Measures
Primary Outcomes
The participants’ reported acceptability and satisfaction, as well as the usability and uptake of the I-AiMentalWELLness (Saya menuju mental sehat) intervention were the primary outcomes of this feasibility study. Acceptability and satisfaction were measured using the Indonesian version of the 8-item Client Satisfaction Questionnaire (CSQ-8) [40]. Moreover, we used the Indonesian version of the System Usability Scale (SUS) [41] as a usability outcome. While the psychometric properties for the Indonesian version of the CSQ-8 and the SUS are currently not available, both had good psychometric properties in studies conducted in Western countries (CSQ-8 and SUS Cronbach =.93 and .90, respectively) [42-44]. The internal consistency for CSQ-8 and SUS in this study was good with Cronbach α=.87 and .83, respectively. Moreover, the CSQ-8 has been adapted to internet-based interventions (CSQ-I) and has demonstrated overall good psychometric properties in 2 studies [45].
In the study protocol, we reported that intervention uptake would be measured by participants’ adherence to the intervention. Adherence was defined as the number of log-ons, time spent on site, and number of sessions attempted. However, due to the technical limitations of the platform used, we could not measure adherence using the numbers of log-ons and time spent online as we originally intended to do [33]. Thus, in this paper, we have described adherence as the number of participants who completed the sessions in the online intervention divided by the number of participants who started the intervention [46]. We also calculated the initial uptake rates by dividing the number of participants who responded to the invitation link from the number of participants who initially expressed interest in participating in the study. We did so to give an overall impression about how many students remained interested in doing the intervention when they had the option to do so.
Secondary Outcomes
Secondary outcome measures included depression, anxiety, and quality of life, which were measured using PHQ-9, GAD-7, and EQ5D5L, respectively. The psychometric properties for the Indonesian version of PHQ-9 and GAD-7 are currently not available. Nonetheless, both PHQ-9 and GAD-7 have demonstrated good psychometric properties in studies conducted in Western countries. The PHQ-9 had high internal consistency (α=.89) and a reliability value of 0.84 [47]. Meanwhile, GAD-7 indicated good internal consistency (α=.92) and test–retest reliability of 0.83 [48]. The internal consistency for PHQ-9 was on the edge of being satisfactory (Cronbach α=.70) and that for GAD-7 was good (Cronbach α=.83). The test–retest reliability of the Indonesian version of EQ5D5L was assessed with sequential measurements using the weighted kappa. Results indicated fair agreements of 0.35, 0.30, 0.37, and 0.39 for the dimensions of mobility, self-care, usual activities, and anxiety/depression, respectively [49]. Meanwhile, the intraclass correlation coefficient for Visual Analog Scale was reported as 0.32, indicating a moderate value [49].
Semistructured Interviews
Both the primary and secondary outcomes of this feasibility study were explored additionally with an individual semistructured interview to obtain a broader perspective and realistic understanding of acceptability, satisfaction, and usability concerning the culturally adapted online intervention for our student population. The semistructured interviews were conducted after participants completed the interventions, by videoconferences between the first author (MR) in The Netherlands and 10 participants in Indonesia. We took account of heterogeneous factors by ensuring equal representation of age, gender, educational, and ethnic background to gain a better understanding of the primary outcome. The demographic characteristics of the participants included in the semistructured interview are reported in Table 1.
Table 1.
Demographic characteristic of participants included in the semistructured interview (N=10).
| Characteristics | Value | ||
| Age (years), mean (SD); range | 24.5 (6.73); 19-41 | ||
| Gender, n (%) |
|
|
|
|
|
Female | 6 (60) | |
|
|
Male | 4 (40) | |
| Ethnicity, n (%) |
|
|
|
|
|
Java | 8 (80) | |
|
|
Other | 2 (20) | |
| Level of education, n (%) |
|
|
|
|
|
Bachelor | 6 (60) | |
|
|
Doctorate | 1 (10) | |
|
|
Master | 3 (30) | |
| Study program, n (%) |
|
|
|
|
|
Psychology | 3 (30) | |
|
|
Medical | 2 (20) | |
|
|
Other | 5 (50) | |
The interview questions were modified from the study of Devi et al [50] to fit the purpose of this study (Multimedia Appendix 1). The participants’ responses were audio-recorded, and additional note taking was also performed during data collection by the first author and 1 team member (local supervisor) in Indonesia. The interview time range was approximately 30 minutes and was conducted in Bahasa Indonesia.
The secondary outcomes were further explored to understand (1) each participant’s evaluation of his/her ECoach, and (2) the cultural appropriateness of the adapted internet-based intervention. These interview questions were modified [51] to fit the purpose of the study. The interview questions can be found in Multimedia Appendix 1.
The I-AiMentalWELLness Intervention
This intervention targets common cognitive and behavioral processes of both anxiety and depression across all sessions; therefore, it is considered a transdiagnostic intervention. Moreover, this intervention was based on cognitive behavioral therapy principles [51,52]. It was originally developed for the general population in Germany and Switzerland [53] and then adapted to meet the needs of domestic and international university students in The Netherlands [54,55]. For the purpose of this study, the current version was culturally adapted from English to Bahasa Indonesia for the student population based on the heuristic theoretical framework [32] which entails (1) information gathering, (2) preliminary adaptation design, (3) preliminary testing, (4) adaptation refinement, and (5) cultural adaptation trial. As reported in the study protocol [33], the first and second phase involved end users (students) as part of the developmental process of the current intervention. Further, the cultural adaptation process concerned all elements of the intervention including language, images, testimonials, and other examples that might not be applicable to the Indonesian culture. Core components of the intervention (eg, behavioral activation, problem solving, cognitive restructuring) remained unchanged. More specifically, after the focus group discussions, we omitted all parts related to unmarried cohabitation, sexual activities, and terms related to alcoholic beverages due to the majority of university students being Muslim. These topics are considered inappropriate in the Islamic religion. We have also changed all parts related to medication such as antidepressants and sleep medication, winter-related sports, and membership in sports and music school. These culturally adapted changes did not influence the main therapeutic components of the internet-based cognitive behavioral therapy intervention (eg, cognitive restructuring) but they solely reflected the local context. An image of one of the sessions in the I-AiMentalWELLness (Saya menuju mental sehat) intervention is provided in Multimedia Appendix 2.
The online intervention consisted of 7 sessions and an additional booster session, which took place 4 weeks after the seventh session of the intervention was completed. The purpose of the booster session was to refresh the memory of the participants about what they learned in the previous 7 sessions of the intervention. It aimed at reinforcing the progress that has been made throughout the interventions and to prepare in case the participants encounter a new episode of, for example, depressive mood. The transdiagnostic approach for anxiety or depression is found particularly in sessions 5 and 6. For further detailed description of the intervention’s content, the reader is referred to Table 2.
Table 2.
The content of the intervention.
| Module | Content description |
| Session 1: Identifying my needs | Goal setting and behavioral activation |
| Session 2: Taking action | Problem solving |
| Session 3: Worth knowing | Psychoeducation on depression and anxiety |
| Session 4: Thoughts pattern | Cognitive restructuring |
| Session 5: Dealing with challenges | Solve problems concerning depressive symptoms or exposure to anxiety-provoking situations |
| Session 6: In daily practice | Solve problems concerning depressive symptoms or exposure to anxiety-provoking situations |
| Session 7: Future plan | Planning for the future |
| Session 8: Strong going forward | Booster session |
| OMa 1: Sleep | Information related to sleep or how to sleep better |
| OM 2: Perfectionism | Identify high standards and understanding the vicious cycle of perfectionism |
| OM 3: Gratitude and appreciating good things | Express gratitude and appreciate goodness in life |
| OM 4: Self-worth | Understanding low self-worth and how to increase it |
| OM 5: Relaxation | Progressive muscle relaxation |
| OM 6: Acceptance | Learning to accept unfulfilled needs |
| OM 7: What is brooding and when is it excessive? | Information on rumination and learning how to overcome it |
aOM: optional modules.
Each session consisted of text, exercises, testimonials, and audio recordings with a duration of approximately 60 minutes to complete. A monetary incentive of Indonesian Rupiah (IDR) 125.000 (equivalent to €7/US $8.5) was given to participants who completed sessions 1-4 and another IDR 125.000 (equivalent to €7/US $8.5) was given to participants who completed sessions 5-8. This monetary incentive was meant to compensate the prepaid cards that participants used to access internet via their mobile phones. Participants were only allowed to complete a maximum of 2 sessions per week to have enough time to integrate the skills acquired from the intervention into their daily life. After the completion of each session, participants received individualized asynchronous feedback from their ECoach through the messaging system of the platform. According to our protocol, each ECoach was advised to spend a maximum of 30 minutes to give feedback per participant at the end of each session. The feedback was brief and of motivational nature to encourage participants to continue with the intervention. Participants were able to move to the next session only after reading the feedback of their ECoach. Furthermore, participants were allowed to contact their ECoach whenever they wanted via the messaging system in the platform. In such case, the ECoaches were advised to respond within 48 hours. When the feedback had been read by the participant, subsequently, the ECoach unlocked the next intervention session. The feedback was of a motivational nature, meaning it consisted of positive reinforcement and encouragement, which reflected on participants’ responses to the online exercises and homework assignments.
Statistical and Descriptive Analysis of Qualitative Data
Quantitative analyses were conducted using the IBM SPSS version 25. Because the primary outcomes regarding acceptability, satisfaction, and usability were only assessed after completion of the interventions, these were analyzed only at posttreatment assessment. We calculated means and SD for the CSQ-8 and SUS to display feasibility. Descriptive statistics were used to summarize (1) participants’ demographic information (age, gender, employment, ethnicity, marital status, study program, and level of education) and (2) participants’ uptake.
For the quantitative analyses of within-group secondary outcomes, data were inspected for outliers and normal distribution. In order to investigate differences between pre- and post-assessment of secondary outcomes, paired-sample t tests were used. To investigate baseline differences between completers and dropouts, an independent sample t test or a Mann–Whitney U test was used. Effect sizes were measured using Hedges g, and interpreted as small=0.2, medium=0.5, and high effect=0.8 [56].
In the protocol, we suggested performing thematic analysis according to the guidelines [57] to analyze the transcripts of the interviews with the participants. However, the data were not suitable for this approach because the participants did not elaborate in depth on the questions asked. Thus, we did not analyze the results of the interview but instead we descriptively synthesized the qualitative data for both primary (acceptability, satisfaction, and usability regarding the internet-based intervention) and secondary outcomes (ECoach evaluation and cultural appropriateness of the adapted internet-based intervention).
Results
Participants
Of the 240 participants who expressed an interest in participating in the study, 118 did not further respond to the invitation link to participate in the screening (initial uptake=50.8%, 122/240). Of those (n=122) screened for eligibility using the PHQ-9 and GAD-7, 96 were eligible to participate in this study and 26 were excluded after obtaining scores indicating moderately severe to severe or no depression or anxiety. Participants with severe depression or anxiety (n=11) were referred to student counseling services, while those who scored below the mild threshold for depression and anxiety (n=15) were excluded and thanked for their participation and interest in our study. The remaining 96 participants were subsequently invited to provide online informed consent, and they completed the additional quality of life measurement (EQ5D5L) and started the first session (intervention uptake=40.0%, 96/240). Fifty participants completed all 7 sessions and the posttreatment assessment. Almost all participants retained at postassessment also followed the booster session (n=46) 4 weeks after the seventh session.
A total of 46 participants discontinued the intervention during sessions 1-4. On the Minddistrict platform, the ECoaches were able to view their participants’ platform, enabling them to notice inactivity such as unread feedback or no further progress on a session. If such inactivity was observed, the ECoach made further attempts to contact the participants through email and text messages (eg, SMS text messages or WhatsApp). If the ECoach received no response from inactive participants, they were considered to have discontinued the intervention. In the end, the participants who discontinued (n=46) were not contacted again for the posttreatment assessment because all previous attempts at communication had failed. Last, 50 participants dropped out from the intervention (sessions 1-7 and booster session 8) and 46 participants dropped out from the study. The flow chart of study participants is presented in Figure 1.
Figure 1.
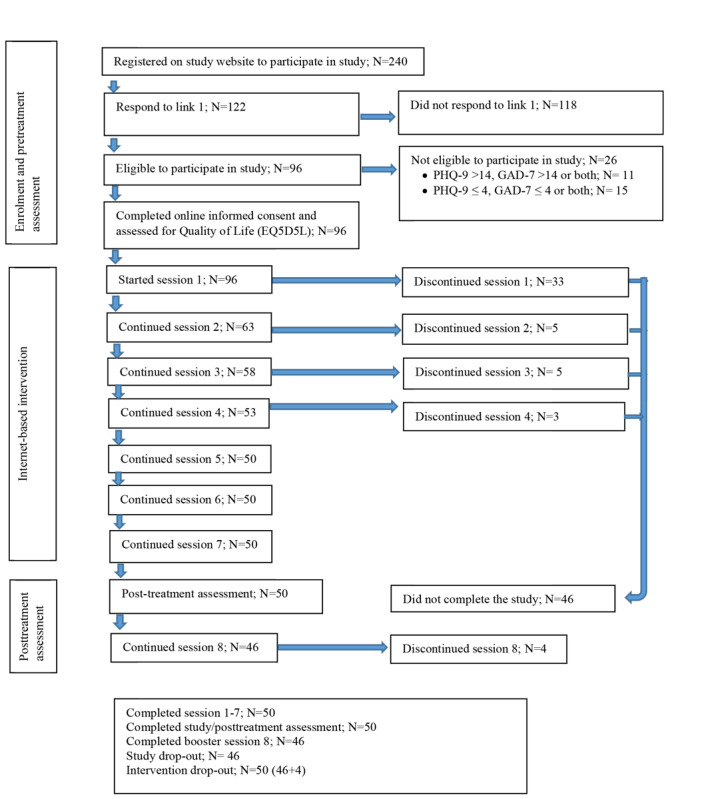
The flowchart of study participants.
The demographic characteristics of the participants and baseline differences between completers and dropouts are presented in Table 3. There were no significant differences in baseline assessment between completers and dropouts (see also Table 3).
Table 3.
Participants’ characteristics and baseline differences between completers and dropouts.
| Characteristics | Completers (N=50) | Dropout (N=46) | t (df)/ꭓ2 (df) | P value | 95% CI | ||||||
| Age (years), mean (SD) | 22 (3.74) | 22 (5.0) | 0.11 (94)a | .91 |
|
||||||
| Gender, n (%) |
|
|
0.003 (1)b | .96 |
|
||||||
|
|
Female | 40 (80) | 37 (80) |
|
|
|
|||||
|
|
Male | 10 (20) | 9 (20) |
|
|
|
|||||
| Ethnicity, n (%) |
|
|
0.85 (1)b | .36 |
|
||||||
|
|
Java | 44 (88) | 43 (93) |
|
|
|
|||||
|
|
Other | 6 (12) | 3 (7) |
|
|
|
|||||
| Marital status, n (%) |
|
|
1.62 (2)b | .44 |
|
||||||
|
|
Divorced | 1 (2) | 0 (0) |
|
|
|
|||||
|
|
Married | 3 (6) | 5 (11) |
|
|
|
|||||
|
|
Single | 46 (92) | 41 (89) |
|
|
|
|||||
| Occupational status, n (%) |
|
|
0.53 (1)b | .47 |
|
||||||
|
|
Employed | 7 (14) | 9 (20) |
|
|
|
|||||
|
|
Unemployed | 43 (86) | 37 (80) |
|
|
|
|||||
| Level of education, n (%) |
|
|
0.50 (2)b | .78 |
|
||||||
|
|
Bachelor | 40 (80) | 35 (76) |
|
|
|
|||||
|
|
Doctorate | 1 (2) | 2 (4) |
|
|
|
|||||
|
|
Master | 9 (18) | 9 (20) |
|
|
|
|||||
| Study program, n (%) |
|
|
2.68 (1)b | .10 |
|
||||||
|
|
Psychology | 21 (42) | 12 (26) |
|
|
|
|||||
|
|
Other | 29 (58) | 34 (74) |
|
|
|
|||||
| PHQ-9c, mean (SD) | 9.46 (3.59) | 9.33 (3.41) | 0.00 (94)a | .99 | –0.06 to 0.06 | ||||||
| GAD-7d, mean (SD) | 7.54 (3.8) | 7.37 (3.46) | –0.22 (94)a | .82 | –1.65 to 1.30 | ||||||
| EQ5D5Le, mean (SD) | 0.83 (0.10) | 0.86 (0.12) | 916.5f | .08 |
|
||||||
aIndependent sample t test.
bChi-square test.
cPHQ-9: 9-item Patient Health Questionnaire.
dGAD-7: 7-item Generalized Anxiety Disorder.
eEQ5D5L: Euro Quality of Life 5 Dimension-5 Level Scale.
fMann–Whitney U test.
Primary Outcomes
The participants who completed the intervention (N=50) had a mean score of 25.8 (SD 3.40) on CSQ-8, indicating moderate to high level of satisfaction and acceptability regarding the online intervention. They had a mean score of 65.1 (SD 13.37) on SUS, indicating a slightly below average of the desirable usability of 70 or more [58]. Of the 96 participants who started, only 50 completed the intervention sessions, resulting in a 52% adherence rate.
Secondary Outcomes
There was a significant decrease in the PHQ-9 and GAD-7 scores. For depression, the overall mean differences in PHQ-9 between the 2 time points was 3.92 (95% CI 2.75-5.1; Hedges g 1.15; P<.001). For anxiety, the overall mean differences between the 2 time points in GAD-7 was 3.34 (95% CI 2.06-4.61; Hedges g 1.02; P<.001), as reported in Table 4. Regarding the EQ5D5L scores, there appeared to be an outlier. However, excluding this outlier did not affect the results, therefore the participant was not excluded from the analysis. At posttreatment assessment, there was a significant increase (P=.008) in the EQ5D5L scores, indicating improved quality of life (Table 4).
Table 4.
Pretreatment and posttreatment assessment for PHQ-9, GAD-7, and EQ5D5L.
| Variable | T0, mean (SD) | T1, mean (SD) | t (df)/Z | P value | Effect size (g) | 95% CI |
| PHQ-9a | 9.46 (3.59) | 5.54 (3.21) | 6.75 (49)b | <.001 | 1.15 | 2.75-5.1 |
| GAD-7c | 7.54 (3.8) | 4.2 (2.65) | –4.22d | <.001 | 1.02 | 2.06-4.61 |
| EQ5D5Le | 0.83 (0.10) | 0.88 (0.10) | –2.66d | .008 | 0.50 |
|
aPHQ-9: 9-item Patient Health Questionnaire.
bPaired sample test.
cGAD-7: 7-item Generalized Anxiety Disorder.
dWilcoxon signed-rank test.
eEQ5D5L: Euro Quality of Life 5 Dimension-5 Level Scale.
Descriptive Analysis of the Qualitative Data
Overall, participants (n=9) reported to be satisfied when using the online intervention. It was reported to be informative, challenging, and triggered them to further recognize the symptoms of depression and anxiety as a student. The optional module was rated as being the most enjoyable part of the intervention as it provided many personal insights. The recorded relaxation was also in favor as it delivered a calm feeling. Participants further acknowledged the online intervention to be more practical than face-to-face interventions as it overcame geographical and stigma barriers. Only one participant reported being confused for not receiving an immediate response to questions that might arise when working through the sessions.
Good user experience with the intervention was reported, indicating clarity in the instructions and workflow in a session. However, difficulties were also reported as 1 participant felt unfamiliar with reading online content, whereas 2 others had problems with the stability of the internet connection when working on the intervention in a remote area.
Regarding the semistructured interviews, 6 out of 10 participants responded positively on being supported through the internet by an ECoach as they received sufficient support, encouragement, reminders, and had their work progress monitored. Nonetheless, 4 out of 10 participants were less positive about having an ECoach because of the unavailability of synchronous feedback and having difficulty with writing what is on their mind. Moreover, they reported that the likelihood of being misinterpreted was high because of absent nonverbal communication signals. Finally, feedback was written in a generic manner and did not always cover specific tasks, as these participants would have expected the feedback to be more elaborative.
As much as 7 out of 10 participants indicated that the overall content of the intervention was culturally appropriate and relevant to university students in Indonesia. Nonetheless, 3 out of 10 participants indicated that some case examples of the intervention were less relevant to the Indonesian context. For instance, it is uncommon for Indonesian university students to have a part-time job during bachelor studies or to be enrolled in a sport and music academy.
Some talk about working. Not all students work, especially bachelor students.
There were some story examples that seem less relevant to the Indonesian culture, such as joining a music or a sport club.
Discussion
Principal Findings
This study has demonstrated promising outcomes for the feasibility of an internet-based intervention for university students in Indonesia, as indicated by participants’ reported acceptability, satisfaction, usability, and uptake regarding the intervention. In addition, a decrease in symptoms of depression and anxiety, and improved quality of life were reported.
Participants reported to have a moderate to a high level of satisfaction and acceptability regarding the online intervention. Results from the interviews also indicated that participants were satisfied with the online intervention as a new approach that acknowledged personal development, and overcame stigma and geographical barriers. The usability/functionality of the internet-based intervention as it applies to the end users was also assessed. One component of usability explained [41] is learnability, which assesses first-time experiences with a new system for end users. A transdiagnostic approach is characterized by a focus on common characteristics that may underpin a number of different psychological disorders such as in case of depression and anxiety disorders. Advantages of such a treatment approach include treating simultaneously these underlying common factors in case of comorbid symptoms [59]. In light of our positive findings regarding the reduction in anxiety and depressive symptoms, the transdiagnostic approach appears promising in the given context. Further research is needed to investigate the effectiveness of such approach in a randomized control trial. However, a transdiagnostic approach delivered online to treat symptoms of depression and anxiety under a single protocol is relatively new. The findings for the mean usability rate for the internet intervention are slightly below average (65.1) for the desired usability ≥70 [58] which is not surprising. Thus, further development and continued improvement are needed to provide individually tailored transdiagnostic intervention, such as by minimizing the use of formal language in the intervention.
With respect to the secondary outcomes of this study, we found a significant decrease (P<.001) in symptoms of depression and anxiety at the posttreatment assessment, and a significant increase (P=.008) in quality of life. Online interventions may offer a promising treatment solution, given the high prevalence of common mental disorders among university students and the under-resourced counseling services [1,2,10]. Many studies have indicated the effectiveness of an online intervention to treat depression and anxiety among university students [10,19]. Understanding quality of life among university students is also important, as it contributes to their physical, psychological, social, and environmental well-being [60]. As the quality of life encompasses various dimensions closely related to the life of a university student, it is important that symptoms of depression and anxiety are treated properly.
It must be noted, of course, that our study did not have a control group. Therefore, the improvements might be attributed to other factors than the intervention, such as spontaneous recovery or regression toward mean.
All participants of this feasibility study were guided by an ECoach who monitored their progress throughout the intervention. The likelihood of completion rate may be associated with therapeutic guidance [42,58,60]. However, we have not tested this hypothesis, and this remains to be confirmed by future studies in low-resource settings.
The secondary outcome of this intervention was further supported by the interview results, which indicated participants’ overall positive response to being treated through the internet by an ECoach, the extent of support received, the average time with regard to receiving feedback, and how comprehensively the feedback was delivered.
A randomized controlled trial will follow this promising feasibility study to further investigate the effectiveness of the existing internet-based intervention to treat depression and anxiety for students within university setting in Indonesia. This is a necessary step before this intervention is made publicly available in Indonesia.
Strengths and Limitations
To the best of our knowledge, this study was one of the first to investigate the feasibility of a guided culturally adapted internet-based intervention to treat symptoms of depression, anxiety, or both among university students in Indonesia. Originally, in the study protocol, we defined appropriate uptake as an adherence rate of 35% due to the novelty of the intervention in Indonesia. However, participants’ adherence rates reached 52% (50/96), which is higher than expected and underlines the feasibility of online interventions for Indonesian university students. It should be noted that we provided monetary incentives to participants who completed the sessions. Thus, it is possible that these incentives have enhanced participation rates. Nevertheless, the amount of incentives was very small and thus it is unlikely that participants completed the study only because of this reason. This feasibility study also has several limitations that must be taken into account. First, the majority of the participants were female, bachelor students, Javanese, and were studying psychology. Future research could benefit from investigating more diverse groups from other faculties and universities to improve the generalizability of these preliminary findings. Second, 46 participants could not be invited to undergo the posttreatment assessment, because they could not be contacted by the ECoach by any means. The research team were unable to locate these participants and thus it limits the understanding of reasons for dropout. Third, data regarding participants’ uptake (log-on time, time spent on site, and number of sessions attempted) of the online intervention could not be provided in this study as participants had previously been instructed to record the time that they spent online. They did so to avoid confusion because Minddistrict (a Dutch company) displayed the Central European time zone. However, this self-reported approach was considered subjective. Other attempts were made by contacting the platform provider to obtain the participants’ recorded time of log-ons but such information was not monitored by the platform. Fourth, the findings regarding the secondary outcome within 2 different time points need to be interpreted with caution as this study was a small pre–post assessment and not a randomized controlled trial. Fifth, another limitation of our study is that our qualitative data were limited in depth, and thus not well suited to thematic analysis. This might have been the result of the way we phrased these questions. In particular, some questions may have been formulated in a too closed manner, thereby preventing the respondents from giving more elaborate answers and convey possible nuances that qualitative research requires. However, the aim of this part of our study was to enrich our quantitative findings. Thus, future qualitative research in this field should aim at more open-ended formulated questions if the aim is to gain in-depth insights into the topic.
Conclusion
Internet-based interventions appear to be acceptable and feasible for reducing symptoms of anxiety and depression and improving quality of life among university students in Indonesia. Future studies should further investigate the (cost-) effectiveness of such interventions as they may be used to supplement existing counseling services in universities, reduce the treatment costs, and maximize treatment accessibility in low-resourced settings.
Acknowledgments
This work was supported by the Indonesia Endowment Fund for Education (Lembaga Pengelola Dana Pendidikan), Ministry of Finance, Republic of Indonesia which provided a PhD scholarship and research funding for the first author (MR). The first author wishes to thank the research assistants Aril, Achi, Icha, Erna, Rara, Olaff, Isti, Deksi, Nana, Dila, Berta, and the study participants of the I-AiMentalWELLness intervention.
Abbreviations
- CSQ 8
Client Satisfaction Questionnaire-8
- EQ5D5L
Euro Quality of Life 5 Dimension-5 Level Scale
- GAD 7
Generalized Anxiety Disorder-7
- IDR
Indonesian Rupiah
- PHQ 9
Patient Health Questionnaire-9
- SUS
System Usability Scale
Appendix
Semi-structured interview questions.
Screenshot example of intervention session 3 in Bahasa Indonesia.
{kind=link}
Footnotes
Authors' Contributions: HR contributed to the design of the study. MR drafted the manuscript under the supervision of EK and MS. All authors contributed to revising the manuscript. All authors read and approved the final manuscript.
Conflicts of Interest: DE has served as a consultant to/on the scientific advisory boards of Sanofi, Novartis, Minddistrict, Lantern, Schoen Kliniken, Ideamed and German health insurance companies (BARMER, Techniker Krankenkasse) and a number of federal chambers for psychotherapy. He is also stakeholder of the Institute for health training online (formerly GET.ON/ now HelloBetter), which aims to implement scientific findings related to digital health interventions into routine care. The remaining authors declare no conflict of interest.
References
- 1.Lun KW, Chan C, Ip PK, Ma SY, Tsai W, Wong C, Wong CH, Wong T, Yan D. Depression and anxiety among university students in Hong Kong. Hong Kong Med J. 2018 Sep 24;24(5):466–472. doi: 10.12809/hkmj176915. [DOI] [PubMed] [Google Scholar]
- 2.Fawzy M, Hamed SA. Prevalence of psychological stress, depression and anxiety among medical students in Egypt. Psychiatry Res. 2017 Sep;255:186–194. doi: 10.1016/j.psychres.2017.05.027. [DOI] [PubMed] [Google Scholar]
- 3.Said D, Kypri K, Bowman J. Risk factors for mental disorder among university students in Australia: findings from a web-based cross-sectional survey. Soc Psychiatry Psychiatr Epidemiol. 2013 Jun;48(6):935–44. doi: 10.1007/s00127-012-0574-x. [DOI] [PubMed] [Google Scholar]
- 4.Auerbach RP, Mortier P, Bruffaerts R, Alonso J, Benjet C, Cuijpers P, Demyttenaere K, Ebert DD, Green JG, Hasking P, Murray E, Nock MK, Pinder-Amaker S, Sampson NA, Stein DJ, Vilagut G, Zaslavsky AM, Kessler RC, WHO WMH-ICS Collaborators WHO World Mental Health Surveys International College Student Project: Prevalence and distribution of mental disorders. J Abnorm Psychol. 2018 Oct;127(7):623–638. doi: 10.1037/abn0000362. http://europepmc.org/abstract/MED/30211576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Auerbach RP, Alonso J, Axinn WG, Cuijpers P, Ebert DD, Green JG, Hwang I, Kessler RC, Liu H, Mortier P, Nock MK, Pinder-Amaker S, Sampson NA, Aguilar-Gaxiola S, Al-Hamzawi A, Andrade LH, Benjet C, Caldas-de-Almeida JM, Demyttenaere K, Florescu S, de GG, Gureje O, Haro JM, Karam EG, Kiejna A, Kovess-Masfety V, Lee S, McGrath JJ, O'Neill S, Pennell B, Scott K, Ten HM, Torres Y, Zaslavsky AM, Zarkov Z, Bruffaerts R. Mental disorders among college students in the World Health Organization World Mental Health Surveys. Psychol Med. 2016 Oct;46(14):2955–2970. doi: 10.1017/S0033291716001665. http://europepmc.org/abstract/MED/27484622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Pedrelli P, Nyer M, Yeung A, Zulauf C, Wilens T. College Students: Mental Health Problems and Treatment Considerations. Acad Psychiatry. 2015 Oct 21;39(5):503–11. doi: 10.1007/s40596-014-0205-9. http://europepmc.org/abstract/MED/25142250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Nam SK, Chu HJ, Lee MK, Lee JH, Kim N, Lee SM. A meta-analysis of gender differences in attitudes toward seeking professional psychological help. J Am Coll Health. 2010;59(2):110–116. doi: 10.1080/07448481.2010.483714. [DOI] [PubMed] [Google Scholar]
- 8.Perry C, Lausch DW, Weatherford J, Goeken R, Almendares M. International students' perceptions of university life. College Student Journal. 2017;51(2):279–290. [Google Scholar]
- 9.ul Haq MA, Dar IS, Aslam M, Mahmood QK. Psychometric study of depression, anxiety and stress among university students. J Public Health. 2017 Oct 24;26(2):211–217. doi: 10.1007/s10389-017-0856-6. [DOI] [Google Scholar]
- 10.Cuijpers P, Sijbrandij M, Koole SL, Andersson G, Beekman AT, Reynolds CF. The efficacy of psychotherapy and pharmacotherapy in treating depressive and anxiety disorders: a meta-analysis of direct comparisons. World Psychiatry. 2013 Jun;12(2):137–48. doi: 10.1002/wps.20038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Babalola E, Noel P, White R. The biopsychosocial approach and global mental health: Synergies and opportunities. Indian J Soc Psychiatry. 2017;33(4):291. doi: 10.4103/ijsp.ijsp_13_17. [DOI] [Google Scholar]
- 12.Cuijpers P, Auerbach RP, Benjet C, Bruffaerts R, Ebert D, Karyotaki E, Kessler RC. The World Health Organization World Mental Health International College Student initiative: An overview. Int J Methods Psychiatr Res. 2019 Jan 06;28(2):e1761. doi: 10.1002/mpr.1761. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bolinski F, Boumparis N, Kleiboer A, Cuijpers P, Ebert D, Riper H. The effect of e-mental health interventions on academic performance in university and college students: A meta-analysis of randomized controlled trials. Internet Interventions. 2020 Apr;20:100321. doi: 10.1016/j.invent.2020.100321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Murray AL, McKenzie K, Murray KR, Richelieu M. An analysis of the effectiveness of university counselling services. British Journal of Guidance & Counselling. 2015 Jun 12;44(1):130–139. doi: 10.1080/03069885.2015.1043621. [DOI] [Google Scholar]
- 15.Yorgason JB, Linville D, Zitzman B. Mental Health Among College Students: Do Those Who Need Services Know About and Use Them? Journal of American College Health. 2010 Aug 06;57(2):173–182. doi: 10.3200/jach.57.2.173-182. [DOI] [PubMed] [Google Scholar]
- 16.Roberts T, Miguel Esponda G, Krupchanka D, Shidhaye R, Patel V, Rathod S. Factors associated with health service utilisation for common mental disorders: a systematic review. BMC Psychiatry. 2018 Aug 22;18(1) doi: 10.1186/s12888-018-1837-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lukito Setiawan J. Willingness to seek counselling, and factors that facilitate and inhibit the seeking of counselling in Indonesian undergraduate students. British Journal of Guidance & Counselling. 2006 Aug;34(3):403–419. doi: 10.1080/03069880600769654. [DOI] [Google Scholar]
- 18.Davies EB, Morriss R, Glazebrook C. Computer-delivered and web-based interventions to improve depression, anxiety, and psychological well-being of university students: a systematic review and meta-analysis. J Med Internet Res. 2014 May 16;16(5):e130. doi: 10.2196/jmir.3142. http://www.jmir.org/2014/5/e130/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Harrer M, Adam SH, Fleischmann RJ, Baumeister H, Auerbach R, Bruffaerts R, Cuijpers P, Kessler RC, Berking M, Lehr D, Ebert DD. Effectiveness of an Internet- and App-Based Intervention for College Students With Elevated Stress: Randomized Controlled Trial. J Med Internet Res. 2018 Apr 23;20(4):e136. doi: 10.2196/jmir.9293. https://www.jmir.org/2018/4/e136/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Andersson G, Titov N. Advantages and limitations of Internet-based interventions for common mental disorders. World Psychiatry. 2014 Feb;13(1):4–11. doi: 10.1002/wps.20083. doi: 10.1002/wps.20083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Richards D, Murphy T, Viganó N, Timulak L, Doherty G, Sharry J, Hayes C. Acceptability, satisfaction and perceived efficacy of “Space from Depression” an internet-delivered treatment for depression. Internet Interventions. 2016 Sep;5:12–22. doi: 10.1016/j.invent.2016.06.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Asosiasi Penyelenggara Jasa Internet-Indonesia. 2017. [2018-11-14]. https:///www.apjii.or.id/
- 23.Ebert DD, Zarski A, Christensen H, Stikkelbroek Y, Cuijpers P, Berking M, Riper H. Internet and computer-based cognitive behavioral therapy for anxiety and depression in youth: a meta-analysis of randomized controlled outcome trials. PLoS One. 2015 Mar;10(3):e0119895. doi: 10.1371/journal.pone.0119895. http://dx.plos.org/10.1371/journal.pone.0119895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Wallin EEK, Mattsson S, Olsson EMG. The Preference for Internet-Based Psychological Interventions by Individuals Without Past or Current Use of Mental Health Treatment Delivered Online: A Survey Study With Mixed-Methods Analysis. JMIR Ment Health. 2016;3(2):e25. doi: 10.2196/mental.5324. http://mental.jmir.org/2016/2/e25/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Arjadi R, Nauta MH, Bockting CLH. Acceptability of internet-based interventions for depression in Indonesia. Internet Interventions. 2018;13:8–15. doi: 10.1016/j.invent.2018.04.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Arjadi R, Nauta MH, Scholte WF, Hollon SD, Chowdhary N, Suryani AO, Uiterwaal CSPM, Bockting CLH. Internet-based behavioural activation with lay counsellor support versus online minimal psychoeducation without support for treatment of depression: a randomised controlled trial in Indonesia. The Lancet Psychiatry. 2018 Sep;5(9):707–716. doi: 10.1016/s2215-0366(18)30223-2. [DOI] [PubMed] [Google Scholar]
- 27.Wu Z, Fang Y. Comorbidity of depressive and anxiety disorders: challenges in diagnosis and assessment. Shanghai Arch Psychiatry. 2014 Aug;26(4):227–31. doi: 10.3969/j.issn.1002-0829.2014.04.006. http://europepmc.org/abstract/MED/25317009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Garber J, Weersing VR. Comorbidity of Anxiety and Depression in Youth: Implications for Treatment and Prevention. Clin Psychol (New York) 2010 Dec;17(4):293–306. doi: 10.1111/j.1468-2850.2010.01221.x. http://europepmc.org/abstract/MED/21499544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Musiat P, Conrod P, Treasure J, Tylee A, Williams C, Schmidt U. Targeted prevention of common mental health disorders in university students: randomised controlled trial of a transdiagnostic trait-focused web-based intervention. PLoS One. 2014 Apr;9(4):e93621. doi: 10.1371/journal.pone.0093621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Mullin A, Dear BF, Karin E, Wootton BM, Staples LG, Johnston L, Gandy M, Fogliati V, Titov N. The UniWellbeing course: A randomised controlled trial of a transdiagnostic internet-delivered cognitive behavioural therapy (CBT) programme for university students with symptoms of anxiety and depression. Internet Interventions. 2015 May;2(2):128–136. doi: 10.1016/j.invent.2015.02.002. http://www.sciencedirect.com/science/article/pii/S2214782915000068. [DOI] [Google Scholar]
- 31.Day V, McGrath PJ, Wojtowicz M. Internet-based guided self-help for university students with anxiety, depression and stress: A randomized controlled clinical trial. Behaviour Research and Therapy. 2013 Jul;51(7):344–351. doi: 10.1016/J.BRAT.2013.03.003. [DOI] [PubMed] [Google Scholar]
- 32.Barrera M, Castro FG, Strycker LA, Toobert DJ. Cultural adaptations of behavioral health interventions: a progress report. J Consult Clin Psychol. 2013 Apr;81(2):196–205. doi: 10.1037/a0027085. http://europepmc.org/abstract/MED/22289132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Rahmadiana M, Karyotaki E, Passchier J, Cuijpers P, van Ballegooijen W, Wimbarti S, Riper H. Guided internet-based transdiagnostic intervention for Indonesian university students with symptoms of anxiety and depression: A pilot study protocol. Internet Interventions. 2019 Mar;15:28–34. doi: 10.1016/j.invent.2018.11.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.I-AiMentalWELLness. 2017. [2017-12-21]. https://i-aimentalwellness.com.
- 35.Hertzog MA. Considerations in determining sample size for pilot studies. Res. Nurs. Health. 2008 Apr;31(2):180–191. doi: 10.1002/nur.20247. [DOI] [PubMed] [Google Scholar]
- 36.Smarr KL, Keefer AL. Measures of depression and depressive symptoms: Beck Depression Inventory-II (BDI-II), Center for Epidemiologic Studies Depression Scale (CES-D), Geriatric Depression Scale (GDS), Hospital Anxiety and Depression Scale (HADS), and Patient Health Questionna. Arthritis Care Res. 2011 Nov 07;63(S11):S454–S466. doi: 10.1002/acr.20556. [DOI] [PubMed] [Google Scholar]
- 37.Patient Health Questionnaire (PHQ) Screener. 2018. [2018-01-09]. https://www.phqscreeners.com.
- 38.Purba FD, Hunfeld JAM, Iskandarsyah A, Fitriana TS, Sadarjoen SS, Ramos-Goñi JM, Passchier J, Busschbach JJV. The Indonesian EQ-5D-5L Value Set. PharmacoEconomics. 2017 Jul 10;35(11):1153–1165. doi: 10.1007/s40273-017-0538-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Minddistrict. 2017. [2017-08-24]. https://www.minddistrict.com/
- 40.Utoyo DB, Lubis DU, Jaya ES, Arjadi R, Hanum L, Astri K, Putri MDD. Preliminary study on the effectiveness of short group cognitive behavioral therapy (GCBT) on Indonesian older adults. PLoS One. 2013;8(2):e57198. doi: 10.1371/journal.pone.0057198. https://dx.plos.org/10.1371/journal.pone.0057198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Sharfina Z, Santoso HB. An Indonesian adaptation of the System Usability Scale (SUS). 2016 International Conference on Advanced Computer Science and Information Systems, ICACSIS 2016; 15-16 October 2016; Malang, Indonesia. Malang, Indonesia: Institute of Electrical and Electronics Engineers Inc; 2016. pp. 145–148. [DOI] [Google Scholar]
- 42.Larsen DL, Attkisson C, Hargreaves WA, Nguyen TD. Assessment of client/patient satisfaction: Development of a general scale. Evaluation and Program Planning. 1979 Jan;2(3):197–207. doi: 10.1016/0149-7189(79)90094-6. [DOI] [PubMed] [Google Scholar]
- 43.Attkisson C, Zwick R. The client satisfaction questionnaire. Evaluation and Program Planning. 1982 Jan;5(3):233–237. doi: 10.1016/0149-7189(82)90074-X. [DOI] [PubMed] [Google Scholar]
- 44.Lewis JR, Brown J, Mayes DK. Psychometric Evaluation of the EMO and the SUS in the Context of a Large-Sample Unmoderated Usability Study. International Journal of Human-Computer Interaction. 2015 Jun 25;31(8):545–553. doi: 10.1080/10447318.2015.1064665. [DOI] [Google Scholar]
- 45.Boß L, Lehr D, Reis D, Vis C, Riper H, Berking M, Ebert DD. Reliability and Validity of Assessing User Satisfaction With Web-Based Health Interventions. J Med Internet Res. 2016 Aug 31;18(8):e234. doi: 10.2196/jmir.5952. http://www.jmir.org/2016/8/e234/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.van BW, Cuijpers P, van SA, Karyotaki E, Andersson G, Smit JH, Riper H. Adherence to Internet-based and face-to-face cognitive behavioural therapy for depression: a meta-analysis. PLoS One. 2014 Jul;9(7):e100674. doi: 10.1371/journal.pone.0100674. http://dx.plos.org/10.1371/journal.pone.0100674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Kroenke K, Spitzer RL, Williams JBW. The PHQ-9. J Gen Intern Med. 2001 Sep;16(9):606–613. doi: 10.1046/j.1525-1497.2001.016009606.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006 May 22;166(10):1092–7. doi: 10.1001/archinte.166.10.1092. [DOI] [PubMed] [Google Scholar]
- 49.Arifin B, Purba FD, Herman H, Adam JMF, Atthobari J, Schuiling-Veninga CCM, Krabbe PFM, Postma MJ. Comparing the EQ-5D-3 L and EQ-5D-5 L: studying measurement and scores in Indonesian type 2 diabetes mellitus patients. Health Qual Life Outcomes. 2020 Feb 7;18(1) doi: 10.1186/s12955-020-1282-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Devi R, Carpenter C, Powell J, Singh S. Exploring the experience of using a web-based cardiac rehabilitation programme in a primary care angina population: a qualitative study. International Journal of Therapy and Rehabilitation. 2014 Sep 02;21(9):434–440. doi: 10.12968/ijtr.2014.21.9.434. [DOI] [Google Scholar]
- 51.Knaevelsrud C, Maercker A. Internet-based treatment for PTSD reduces distress and facilitates the development of a strong therapeutic alliance: a randomized controlled clinical trial. BMC Psychiatry. 2007 Apr 19;7(13):13–10. doi: 10.1186/1471-244X-7-13. https://bmcpsychiatry.biomedcentral.com/articles/10.1186/1471-244X-7-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Johnston L, Titov N, Andrews G, Dear BF, Spence J. Comorbidity and internet-delivered transdiagnostic cognitive behavioural therapy for anxiety disorders. Cogn Behav Ther. 2013;42(3):180–192. doi: 10.1080/16506073.2012.753108. [DOI] [PubMed] [Google Scholar]
- 53.Weisel KK, Zarski A, Berger T, Krieger T, Schaub MP, Moser CT, Berking M, Dey M, Botella C, Baños R, Herrero R, Etchemendy E, Riper H, Cuijpers P, Bolinski F, Kleiboer A, Görlich D, Beecham J, Jacobi C, Ebert DD. Efficacy and cost-effectiveness of guided and unguided internet- and mobile-based indicated transdiagnostic prevention of depression and anxiety (ICare Prevent): A three-armed randomized controlled trial in four European countries. Internet Interventions. 2018 Apr; doi: 10.1016/j.invent.2018.04.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Bolinski F, Kleiboer A, Karyotaki E, Bosmans JE, Zarski A, Weisel KK, Ebert DD, Jacobi C, Cuijpers P, Riper H. Effectiveness of a transdiagnostic individually tailored Internet-based and mobile-supported intervention for the indicated prevention of depression and anxiety (ICare Prevent) in Dutch college students: study protocol for a randomised controlled trial. Trials. 2018 Mar 20;19(1):118. doi: 10.1186/s13063-018-2477-y. https://trialsjournal.biomedcentral.com/articles/10.1186/s13063-018-2477-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Karyotaki E, Klein AM, Riper H, Wit LD, Krijnen L, Bol E, Bolinski F, Burger S, Ebert DD, Auerbach RP, Kessler RC, Bruffaerts R, Batelaan N, van der Heijde CM, Vonk P, Kleiboer A, Wiers RW, Cuijpers P. Examining the effectiveness of a web-based intervention for symptoms of depression and anxiety in college students: study protocol of a randomised controlled trial. BMJ Open. 2019 May 14;9(5):e028739. doi: 10.1136/bmjopen-2018-028739. https://bmjopen.bmj.com/lookup/pmidlookup?view=long&pmid=31092668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Cohen J. Statistical power analysis for the behavioral sciences, 2nd ed. New York, NY: Lawrence Erlbaum Associates; 1988. [Google Scholar]
- 57.Maguire M, Delahunt B. Doing a Thematic Analysis: A Practical, Step-by-Step Guide for Learning and Teaching Scholars. All Ireland Journal of Teaching and Learning in Higher Education (AISHE-J) 2017;8(3):3351–33514. http://ojs.aishe.org/index.php/aishe-j/article/view/335/553. [Google Scholar]
- 58.Bangor A, Kortum PT, Miller JT. An Empirical Evaluation of the System Usability Scale. International Journal of Human-Computer Interaction. 2008 Jul 30;24(6):574–594. doi: 10.1080/10447310802205776. [DOI] [Google Scholar]
- 59.Bitsika V, Sharpley CF. Comorbidity of anxiety-depression among Australian university students: implications for student counsellors. British Journal of Guidance & Counselling. 2012 Aug;40(4):385–394. doi: 10.1080/03069885.2012.701271. [DOI] [Google Scholar]
- 60.Al Naggar RA, Osman MT, Musa R. Quality of Life among University Students in a Single Malaysian Institute. Pensee Journal. 2013;75(10) [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Semi-structured interview questions.
Screenshot example of intervention session 3 in Bahasa Indonesia.