

Abstract
Aerodigestive tract fish bones are common and often utilize significant hospital resources. Some pharyngeal fish bones can be retrieved with basic equipment thus clinicians should exhaust all simple techniques including that described in this paper.
Keywords: fish bone, Foreign body, hypopharynx, laryngoscope
Aerodigestive tract fish bones are common and often utilize significant hospital resources. Some pharyngeal fish bones can be retrieved with basic equipment thus clinicians should exhaust all simple techniques including that described in this paper.

1. INTRODUCTION
Aerodigestive fish bones are particularly problematic, there are those that lie within the oropharynx and upper hypopharynx that may be reached with simple tools and manoeuvres. We have describe a more tolerable alternative to a traditional method which utilizes a laryngoscope.
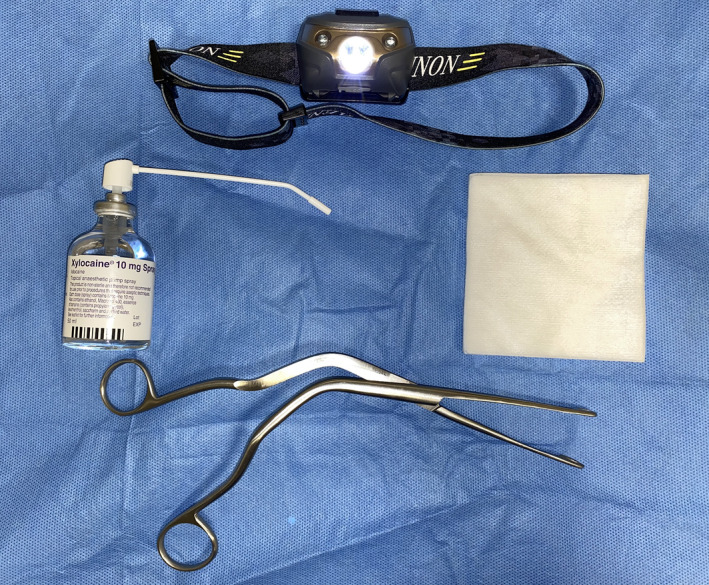
Aerodigestive tract foreign bodies are a relatively common in otolaryngology and most doctors will likely encounter this in their junior years in the emergency department (ED) or on an otolaryngology rotation. Among foreign bodies, fish bones are particularly problematic and can be embedded in soft tissue anywhere from the oral cavity to the esophagus. A significant amount of these lie within the oral cavity and can be remove very easily and there are those that lie in the esophagus and recesses of the hypopharynx that justify the need for more invasive measures such as pharyngoscopy or esophagoscopy. There are also those that lie in between, and initial attempt at retrieval may be achieved with simple tools (Figure 1) and maneuvers postponing the need for complex procedures, general anesthesia, valuable human resources, theatre space, time, and equipment.
FIGURE 1.
Fish bone in base of tongue seen on flexible nasoendoscopy
This article describes a simple alternative technique to remove a foreign body from the upper aerodigestive tract but beyond the oral cavity and oropharynx thus forgoing the need for pharyngoscopy and general anesthesia and the associated resources.
2. CASE DESCRIPTION
A 37‐year‐old female was seen in the emergency department after being referred to ENT for a throat pain after eating fish. The patient gave a four‐hour history of having had fish when she started having sticking right sided throat pain made worse by swallowing. Patient gave no history of drooling, coughing, shortness of breath, chest pain nor fever. On examination, the patient was in mild painful distress. Examination of the oral cavity and visible oropharynx was normal, no significant neck tenderness on palpation, no crepitus. A review of a lateral soft tissue neck X‐ray ordered by ED staff was negative for fish bone. However, on flexible nasoendoscopy (FNE), a fish bone was noted to be imbedded in right tongue base (Figure 2).
FIGURE 2.
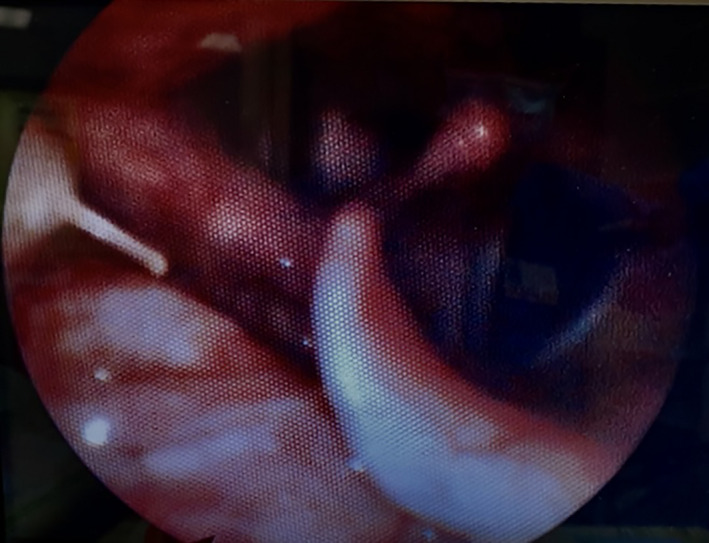
Fish bone in base of tongue seen on flexible nasoendoscopy
Generous application topical local anesthetic solution a sprayed to the back of the mouth for the patient to gargle for 30 to 60 seconds. The patient was made to lie supine in the sniffing morning air position. The clinician sits at the head of the couch with the patient at a comfortable height. Attempts to remove the fish bone with the aid of a curved Magill laryngoscope to displace the tongue for attempt at visualizing the fish bone were unsuccessful. This was poorly tolerated due to a strong gag reflex. Instead, the patient was asked to stick the tongue out and a sterile gauze was wrapped around the middle third of the tongue which was then held and gentle upward and caudal traction was applied (Figure 3). With the aid of a headlight, direct vision of the oropharynx and upper aspect of the hypopharynx was visualized and a pair of Magill forceps was used to retrieve foreign body (Figure 4). The patient was discharged directly from the emergency department with advice.
FIGURE 3.

Equipment used to retrieve fish bone; headlight, gauze, topical lidocaine, Magill forceps
FIGURE 4.

Fish bone removed from pharynx
3. DISCUSSION
This paper has described an alternative minimally invasive approach to retrieving a foreign body within the lower aspect of the oropharynx and upper hypopharynx. In 10%‐20% of cases of fish bones and other foreign bodies in the hypopharynx and esophagus are challenging to retrieve and require general anesthesia and pharyngoscopy or rigid esophagoscopy. 1 However, for those fish bones in reachable places in the aerodigestive tract, attempts should be made to remove them before moving to more invasive measures.
In this case, our patient had a fish bone imbedded to the right of the tongue base just at the level of the epiglottis. This was initially missed on X‐ray which is not uncommon but was picked up on FNE. 2 Despite application of topical local anesthesia, initial attempts using a laryngoscope as described in the literature 3 , 4 failed because the patient had poor tolerance of a metal instrument passed into the vallecula due to a functional gag reflex. 5 The novel technique described in this paper was successful due to the lack of instrumentation of the oropharynx of a conscious patient. Instead, the tongue was displaced with anterior and caudal traction negating the need for an instrument which thus eliminated stimulating the gag reflex. This allowed for a thorough look without thrashing from the patient and a more controlled attempt at grasping and removing the fish bone. It should be noted that when applying traction, this should be gentle and the middle third of the tongue should be held as traction at the tip is restricted by the frenulum and produces pain. This was relatively challenging and the writer would recommend having an assistant or having the patient themselves hold their tongue. As a result of this technique, this patient had removal of a fish bone from the pharynx without the need for operating theatre.
4. CONCLUSION
A fish bone was found imbedded in a reachable region of the upper hypopharynx and be removed with the simple technique described in this paper. This technique was superior to another which utilizes a laryngoscope as it was vastly more tolerable especially in the presence of locally anesthetized pharynx. This afforded the clinician more time and an increased the chance of success and thus negated the need for unnecessary pharyngoscopy and general anesthesia.
CONFLICT OF INTEREST
None declared.
AUTHOR CONTRIBUTIONS
KB is the corresponding author and sole contributor to the concept, implementation and to the writing of the manuscript.
ACKNOWLEDGMENTS
All works described in this paper was done at the Royal London Hospital and were conducted solely by the author. Published with written consent of the patient.
Brown KM. A tolerable alternative for removal of a fish bone to the pharynx: A case report. Clin Case Rep. 2021;9:1598–1600. 10.1002/ccr3.3841
Funding information
There were financial incentives or funding organizations associated with this paper.
DATA AVAILABILITY STATEMENT
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
REFERENCES
- 1. Cianci P, Tartaglia N, Altamura A, et al. Cervical esophagotomy for foreign body extraction: a case report and extensive literature review of the last 20 years. Am J Case Rep. 2018;19:400‐405. 10.12659/AJCR.908373 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Sanei‐Moghaddam A, Sanei‐Moghaddam A, Kahrobaei S. Lateral Soft Tissue X‐ray for Patients with Suspected Fishbone in Oropharynx, A thing in the past. Iran J Otorhinolaryngol. 2015;27(83):459‐462. [PMC free article] [PubMed] [Google Scholar]
- 3. Nathan B, Premachandran S, Hashemi K. Removal of fish bones from the throat. Emerg Med J. 1995;12(4):303‐303. 10.1136/emj.12.4.303 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Sakaida H, Chiyonobu K, Ishinaga H, Takeuchi K. Use of a rigid curved laryngoscope for removal of a fish bone in the hypopharynx. Case Rep Otolaryngol. 2016;2016:1‐3. 10.1155/2016/9689521 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Svecova N, Ward M. Nebulised local anaesthesia technique for fish bone removal. Ann R Coll Surg Engl. 2014;96(4):321‐321. 10.1308/rcsann.2014.96.4.321 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.