

Abstract
BACKGROUND AND PURPOSE:
Children with sickle cell disease have low hematocrit and elevated CBF, the latter of which can be assessed with arterial spin-labeling MR imaging. Quantitative CBF values are obtained by using an estimation of the longitudinal relaxation time of blood (T1blood). Because T1blood depends on hematocrit in healthy individuals, we investigated the importance of measuring T1blood in vivo with MR imaging versus calculating it from hematocrit or assuming an adult fixed value recommended by the literature, hypothesizing that measured T1blood would be the most suited for CBF quantification in children with sickle cell disease.
MATERIALS AND METHODS:
Four approaches for T1blood estimation were investigated in 39 patients with sickle cell disease and subsequently used in the CBF quantification from arterial spin-labeling MR imaging. First, we used 1650 ms as recommended by the literature (T1blood-fixed); second, T1blood calculated from hematocrit measured in patients (T1blood-hematocrit); third, T1blood measured in vivo with a Look-Locker MR imaging sequence (T1blood-measured); and finally, a mean value from T1blood measured in this study in children with sickle cell disease (T1blood–sickle cell disease). Quantitative flow measurements acquired with phase-contrast MR imaging served as reference values for CBF.
RESULTS:
T1blood-measured (1818 ± 107 ms) was higher than the literature recommended value of 1650 ms, was significantly lower than T1blood-hematocrit (2058 ± 123 ms, P < .001), and, most interesting, did not correlate with hematocrit measurements. Use of either T1blood-measured or T1blood–sickle cell disease provided the best agreement on CBF between arterial-spin labeling and phase-contrast MR imaging reference values.
CONCLUSIONS:
This work advocates the use of patient-specific measured T1blood or a standardized value (1818 ms) in the quantification of CBF from arterial spin-labeling in children with SCD.
Sickle cell disease (SCD) is associated with a considerable risk of stroke,1 which is reduced by blood transfusion therapy2 and identified by screening blood flow velocities in intracranial arteries with transcranial Doppler.3 Additionally, microvascular tissue perfusion, or CBF, is also increased in patients with SCD4,5; which is related to low hematocrit (Hct).6,7 CBF measurements are instrumental in understanding the pathophysiology of impaired perfusion in the occurrence of silent cerebral infarcts in SCD.4,8,9 Noninvasive CBF measurements can be performed with arterial spin-labeling (ASL) and a quantification model to calculate physiological CBF values. The wide range of CBF values reported in the literature in SCD1,4,9 emphasizes the need for either more accurate estimates or direct measurements of the often-assumed parameters required for CBF quantification models.
The longitudinal relaxation time of the blood (T1blood) parameter accounts for the decay of the ASL signal with time, and inaccurate estimates of T1blood could result in over- or underestimation of CBF.10–12 For healthy adults, with a stable Hct, a fixed T1blood value of 1650 ms is recommended for CBF quantification from pseudocontinuous ASL (pCASL) at 3T.13,14 T1blood is inversely correlated with Hct,10,13,15–19 and a linear relationship has been proposed in the literature permitting the calculation of T1blood from measured Hct values.12,13,16 While Hct ranges from 38% to 45% in healthy children,20 it is as low as 18%–30% in children with SCD.21 Hence, if measured Hct values are available, T1blood can be derived accordingly. However, recent studies suggest that T1blood may additionally differ in children with SCD.12,22,23
Owing to recent developments in MR imaging, direct measurements of the inversion recovery of T1blood are now possible by combining a global inversion pulse and a subsequent section-selective Look-Locker readout in the sagittal sinus.16,17 Patient-specific, in vivo T1blood measurements are noninvasive, robust, and fast, making them preferable to calculating T1blood from blood samples. Our first hypothesis was that in vivo–measured T1blood would be higher in children with SCD than the adult reference value of 1650 ms due to anemia. We also considered that conformational changes inherent to sickle red blood cells may produce additional unforeseen changes in T1blood.12 We investigated the importance of measuring patient-specific differences in T1blood for the accuracy of ASL quantification in patients with SCD. We hypothesized that patient-specific T1blood values acquired in vivo would improve CBF quantification in SCD compared with CBF quantification with T1blood calculated from Hct or T1blood-fixed at 1650 ms.
The aim of this study was to determine which of the following 4 T1blood derivatives would provide the best CBF quantification compared with quantitative reference CBF values measured with 2D phase-contrast MR imaging (PC-MRI): 1) literature-recommended adult T1blood of 1650 ms,14 2) T1blood calculated from Hct, 3) in vivo–measured T1blood, or 4) a fixed average SCD value from the mean T1blood measured in vivo in this study.
Materials and Methods
Experiments were performed according to principles of the Declaration of Helsinki, and the study was approved by the local institutional review board at the Academic Medical Center, Amsterdam, the Netherlands.
Patients
Eligible children were approached prospectively from 2 outpatient clinics as described previously.24 Informed consent was obtained from parents or guardians and children older than 12 years of age. Inclusion criteria were HbSS or HbSβ0 genotypes and 8–17 years of age. Exclusion criteria were a history of stroke, stenosis of the intracranial arteries and velocity of >155 cm/s on transcranial Doppler imaging, current chronic blood transfusion therapy, bone marrow transplant, MR imaging contraindications, and major concomitant health problems. Patients were in a steady-state of SCD, without evidence of infection or sickle cell crisis up to 1 month before participation.
Hematocrit
Venous blood samples were drawn from an antecubital vein on the day of the MR imaging assessment and processed according to standard procedures in the hospital laboratory. Hct values were used to calculate T1blood-Hct values.
MR Imaging Acquisition
Thirty-two children underwent 3T imaging on an Intera scanner (Philips Healthcare, Best, the Netherlands) with an 8-channel head coil, and due to a scanner upgrade, the remaining 8 children were scanned at 3T on an Ingenia (Philips Healthcare) with a 15-channel head coil. The protocol included 3D-TOF MRA, 2D T2-weighted, T1blood, 2D pseudocontinuous ASL, and 2D phase-contrast sequences.
The T1blood acquisition section was planned perpendicular to the posterior sagittal sinus16 and comprised a multi time-point inversion recovery experiment. This technique uses a global inversion pulse followed by a series of 95° section-selective readout pulses, which are intended to saturate the tissue surrounding the sinus. Assuming complete replenishment of inverted blood between 2 consecutive pulses, a high contrast is achieved between tissue and blood, allowing the detection of the inversion recovery of blood. A nonselective adiabatic 180° inversion pulse (hyperbolic secant pulse, B1 value/duration of the pulse = 13.5 mT/13 ms) preceded a single section Look-Locker EPI readout (flip angle, 95°; voxel size, 1.5 × 1.5 mm; matrix, 240 × 240 mm; section thickness, 2 mm; TE/TR, 15/10,000 ms; TI1, 200 ms; ΔTI, 150 ms; 60 readouts; 6 signal averages; scan duration, 1 minute 20 seconds).
A gradient-echo single-shot EPI pCASL sequence was used to acquire perfusion-weighted images (75 subtracted label-control pairs; resolution, 3 × 3 × 7 mm; FOV, 240 × 240 mm; 17 continuous axial sections; TE/TR, 17/4000 ms; flip angle, 90°; labeling duration, 1650 ms; postlabeling delay, 1525 ms; background suppression, 1680 and 2830 ms after a prelabeling saturation pulse; scan duration, 10 minutes 7 seconds).
Quantitative flow measurements were obtained with a nontriggered 2D single-section PC-MRI acquisition in the internal carotid and vertebral arteries. Imaging parameters were the following: FOV, 230 × 230 mm; voxel size, 0.45 × 0.45 mm; TR/TE, 15/5 ms; flip angle, 15°; maximum velocity-encoding, 140 cm/s; section thickness, 4 mm; scan duration, 1 minute.
Data Postprocessing
T1blood.
Blood-filled voxels within the sagittal sinus were selected on the basis of the highest signal intensity. Voxel values were subsequently averaged, and the data were fitted to a 3-parameter model (Nealder-Mead method; MathWorks, Natick, Massachusetts), with the parameters M0, Offset, and T1blood,17 and solved for T1blood:
 |
where M models the T1 recovery from the data, nTI is the readout number, abs denotes the absolute values, M0 is the net magnetization, “Offset” accounts for imperfect inversion, TI1 is 200 ms, and ΔTI is the sampling interval (150 ms). The sum of squared errors of the final (optimal) iteration after solving the Nealder-Mead function indicated how well the data fitted the model and served as a quality check.
Cerebral Blood Flow.
Raw pCASL data were processed as described previously25 by using a processing pipeline for the registration and quantification of the data. A 2-compartment quantification model was used, as published in detail previously9,26 (except that the equilibrium magnetization of arterial blood was derived from the M0 of CSF multiplied by the blood-water partition coefficient,27 and labeling efficiency was 0.7). The T1blood parameter was adjusted for each CBF quantification as follows: first, adult fixed T1blood of 1650 ms taken from literature13; second, patient-specific Hct-calculated T1blood values16; third, patient-specific in vivo–measured T1blood values; and finally an average T1blood value obtained from the mean of in vivo T1blood measurements in our patients with SCD. T1blood-Hct was calculated per patient according to the relationship proposed by Varela et al16 derived from venous blood in neonates:
PC-MRI.
The internal carotid and vertebral arteries were segmented manually from phase difference images by using ITK-SNAP (http://www.itksnap.org) to obtain total flow (milliliters per minute). Total flow was then divided by brain mass (gram), which was calculated from the product of the volume (estimated from segmented anatomic images in SPM8; http://www.fil.ion.ucl.ac.uk/spm/software/spm12) and an assumed brain density of 1.05 g/L,28 to obtain PC-MRI CBF in milliliters/100 g/min,29 which served as the reference value for CBF.22,29
Statistical Analysis
A Pearson correlation was performed between T1blood-measured and Hct. Repeated-measures ANOVA was used to test the statistical significance of the differences among the 5 CBF quantification methods: 1) CBF (T1blood-fixed at 1650 ms), 2) CBF (T1blood-Hct), 3) CBF (T1blood-measured in vivo, 4) CBF (T1blood-SCD fixed at the average measured value), and 5) PC-MRI reference CBF. Paired t tests were used to test the statistical significance of individual group differences post hoc. Agreement between PC-MRI and the 4 ASL methods was investigated with linear regression and Bland-Altman analyses in Matlab (MathWorks, Natick, Massachusetts). Linear regression analysis was performed to show agreement between PC-MRI and the 4 CBF quantification methods from ASL. Bland-Altman analysis was performed to indicate the bias corresponding to over- or underestimation of the ASL CBF method compared with the PC-MRI method. The limits of agreement (dotted lines) indicate the 95% confidence intervals.
Results
Demographic and clinical characteristics are summarized in Table 1. One patient's T1blood scan was discarded due to poor image quality, so the mean CBF values from pCASL are based on 39 datasets. For PC-MRI, only 33 datasets were of sufficient quality to quantify reference CBF.
Table 1:
Demographic and clinical characteristics
| Demographic or Clinical Parameter | Mean and SD |
|---|---|
| Total No. | 39 |
| Females (No. and % of total) | 16 (41%) |
| Males (No. and % of total) | 23 (59%) |
| Age (yr) | 12 ± 2 |
| Hematocrit (%) | 23 ± 3 |
| Hemoglobin (g/d/L)a | 8.4 ± 1.1 |
| Hemoglobin F (%)b | 10 ± 6 |
| Hemoglobin A2 (%)c | 4.8 ± 1 |
| Hemoglobin S (%) | 84 ± 5 |
| Mean corpuscular volume (mL)d | 82 ± 10 |
| Mean corpuscular hemoglobin concentration (mmol/L)e | 21 ± 0.6 |
Normal range reference values: Hb = 10–16.
HbF < 1%.
HbA2 = 2–3.
MCV = 75–95.
MCHC = 19.0–22.5.
Measured T1blood
The mean Hct was 23% ± 3% for 39 children. The mean T1blood-measured value was 1818 ± 107 ms, which was significantly lower than mean T1blood-Hct values (2045 ± 69 ms; paired t test, P < .001) but higher compared to the fixed adult value of 1650 ms. T1blood-measured was not significantly different between scanners (t test, P = .94). Figure 1A shows a representative inversion recovery curve from 1 patient as a function of the sum of least-squares fit. The sum of squared errors from fitting the T1blood-measured values to the model is shown in On-line Fig 1. T1blood-measured values did not correlate with Hct values measured from blood samples (r = 0.02, P = .89; Fig 1B) or with age (r = 0.03, P = .85) and did not differ significantly between males and females (t test, P = .37).
Fig 1.

A, Representative inversion recovery of the venous T1blood signal acquired in the sagittal sinus in a child with sickle cell disease. B, In vivo–measured T1blood values are significantly lower than Hct-derived T1blood values. T1blood-measured does not correlate with patient hematocrit (mean Hct, 23% ± 3%) (Pearson r = 0.02, P = .89; n = 39).
Cerebral Blood Flow
Four CBF quantification methods were compared with PC-MRI CBF, the results of which are summarized in Table 2. Linear regression analyses between PC-MRI and pCASL CBF are shown in the left panel of Fig 2 and reveal slopes significantly different from zero for all CBF quantifications except for the T1blood-Hct CBF quantification. The Bland-Altman plots in the right panel of Fig 2 show the bias and limits of agreement for the mean and the difference between the measurements. T1blood-fixed overestimated CBF and T1blood-Hct underestimated CBF, while the individual in vivo T1blood-measured values and mean T1blood-SCD value provided the best agreement with PC-MRI values, both on an absolute level, revealed by no significant difference between PC-MRI and CBF in the repeated-measures ANOVA analysis (Table 2), but also on a one-to-one basis, as demonstrated in the linear regression plots (Fig 2). A representative example of CBF maps quantified with T1blood-measured from 2 patients is shown in Fig 3.
Table 2:
T1blood values and corresponding CBF values quantified from ASLa
| T1blood | Method (Value) | ASL-CBF (mL/100 g/min) | P Value |
|---|---|---|---|
| T1blood-fixed | Literature (1650 ms) | 114 ± 13 | <.05 |
| T1blood-Hct | Calculated from patient's hematocrit (variable) | 95 ± 10 | <.05 |
| T1blood- measured | Measured with MR in vivo in patients with SCD (variable) | 106 ± 14 | NS |
| T1blood-SCD | Mean of T1blood-measured (1818 ms) | 105 ± 12 | NS |
Note:—NS indicates not significant.
Repeated-measures ANOVA was performed to test the significance (P in the final column) of differences between CBF from ASL and reference CBF obtained from phase-contrast MRI flow measurements.
Fig 2.
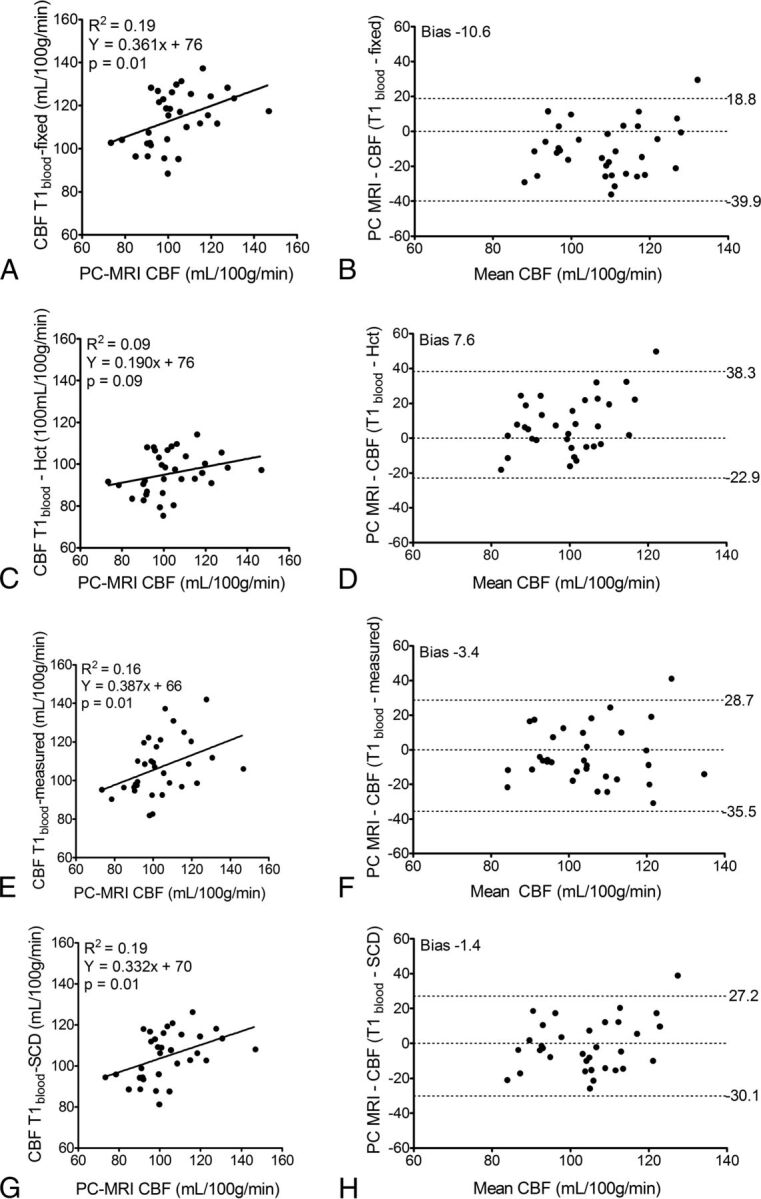
Linear regression and Bland-Altman plots between CBF values measured with PC-MRI and ASL, which was quantified by using 4 different T1blood values: a fixed literature value of 1650 ms (CBF T1blood-fixed) (A and B); T1blood calculated from hematocrit (CBF T1blood-Hct), T1 = 0.5*Hct+0.37 (C and D)16; in vivo–measured T1blood (CBF T1blood-measured) (E and F); and a fixed SCD value obtained from the mean of the in vivo–measured T1blood (CBF T1blood-SCD) (G and H). The left panel shows linear regressions (solid line), and the right panel shows the mean on the x-axis versus the difference on the y-axis between pCASL and PC-MRI CBF with limits of agreement (dotted lines above and below) (n = 33).
Fig 3.

Axial brain sections showing CBF from 2 representative examples of 2 fourteen-year-old boys with SCD. The upper row shows a patient with low CBF and the lower row shows a patient with high CBF.
Discussion
We demonstrate that in vivo–measured venous T1blood values in children with SCD were higher than the literature-recommended 1650 ms, were not significantly correlated with measured Hct, and were lower than the Hct-derived values for T1blood. CBF quantified with in vivo–measured T1blood provided better agreement with PC-MRI reference measurements than CBF quantified with fixed adult T1blood and Hct-derived T1blood.
T1blood and Hematocrit
Previous literature suggests that healthy children 6–18 years of age (assuming a stable Hct of 40%–45%) have T1blood values between 1680 and 1880 ms.18 In this study, in patients with a much lower Hct than healthy children, we measured T1blood values closer to the upper range of the literature-reported T1blood values.18 Yet, our T1blood values were lower than expected, considering the low Hct values obtained from our patients' blood samples. It is unlikely that we underestimated T1blood due to sequence-related limitations because the Look-Locker T1 technique has previously provided robust results in the same ROI.16,17,27
Reports of T1blood values ranging from 1500 to 2100 ms follow a linear relationship with Hct between 23% and 50%.13,16,18 It is possible that we did not have sufficient precision to detect this inverse relationship in our dataset or that the range of Hct values was too narrow in our patients (17%–32%). Abnormalities in SCD blood, other than low Hct, may account for the incongruity between T1blood and Hct measured here. While we did not measure blood rheology, abnormalities such as decreased red blood cell deformability, increased aggregation, and increased viscosity have been demonstrated consistently.21,30–34 Furthermore, red blood cells in SCD exhibit different membrane properties and viscosity, which may have reduced T1blood due to shrinkage of cells and therefore lower water content.35
CBF Quantification
Our CBF results fall within the large range of reported values in children with SCD (∼70–150 mL/100 g/min).1,4,9,36,37 The necessary reliance on a quantification model for obtaining physiologically meaningful CBF values means that the method is sensitive to the assumptions of the model used, which could differ between healthy adults and children with SCD. The fact that measured T1blood ameliorates the CBF quantification but Hct-calculated T1blood does not opposes the use of Hct-corrected CBF quantification in SCD and, instead, advocates the use of measured T1blood. T1blood measurements are advantageous over Hct-calculated T1blood because they are faster (1 minute 20 seconds) and less invasive. In the absence of T1blood measurements, we propose using a mean value of 1818 ms, as measured in this study in children with SCD, which would suffice in improving the absolute agreement with PC-MRI for CBF quantification from ASL.
Limitations
This study should be considered in light of the technical limitations of the T1blood measurement and the potentially inaccurate reference flow measurements from PCMR.
Whereas T1blood measurements were acquired in venous blood, the quantification model requires arterial estimates. However, because we compared venous T1blood measurements with T1blood values derived from venous Hct, the potential mismatch would have been similar for both methods. Moreover, we demonstrate that the measured venous T1blood, used to quantify CBF, improved the agreement with independently acquired flow measurements in arterial vessels with PC-MRI, which shows that although the arterial measurement may be better, the venous measurement is sufficient.
PC-MRI as a surrogate for CBF could be critiqued for CBF overestimation due to partial volume effects38 and inaccurate brain density estimates or underestimated flow due to noncardiac-triggered acquisition. Still, recent literature suggests that errors in flow values associated with nontriggered 2D PC-MRI are <3% compared with triggered acquisitions.29,39 Despite these limitations, a recent study has shown high agreement (intraclass correlation coefficient, 0.73) between PC-MRI and pCASL,40 emphasizing that PC-MRI is currently the best noninvasive reference for pCASL CBF.
Conclusions
Inaccurate T1blood estimates can be a major confounder for quantitative perfusion assessment from ASL. Patient-specific, in vivo–measured T1blood measurements provided more accurate CBF values than T1blood derived from Hct values. To avoid overestimation of CBF in SCD, we recommend the use of a fixed value of 1818 ms (T1blood-SCD) for CBF quantification from ASL in SCD if measured T1blood values are not available.
Supplementary Material
Acknowledgments
The authors thank the participants and the medical and technical staff who helped with recruitment, scanning, and blood measurements.
ABBREVIATIONS:
- ASL
arterial spin-labeling
- Hct
hematocrit
- pCASL
pseudocontinuous ASL
- PC-MRI
phase-contrast MR imaging
- SCD
sickle cell disease
- T1blood
longitudinal relaxation time of blood
Footnotes
Disclosures: Lena Václavů—RELATED: Grant: Fonds NutsOhra (grant from Dutch Sickle Cell Research Foundation).* Dennis F.R. Heijtel—UNRELATED: Employment: Philips Healthcare (currently employed). Matthias J.P. van Osch—UNRELATED: Employment: Philips Healthcare; Patents (planned, pending or issued): joint patent with Philips Healthcare* and a joint patent with the Florey Institute of Neuroscience and Mental Health (Melbourne, Australia) and Lund University (Sweden),* both pending; Other: research support by Philips Healthcare.* Charles B.L.M. Majoie—UNRELATED: Payment for Lectures (including service on Speakers Bureaus): Stryker.* John C. Wood—UNRELATED: Consultancy: BioMed Informatics, ApoPharma, Isis Pharmaceuticals, Pfizer, Celgene, WorldCare Clinical; Grants/Grants Pending: National Institutes of Health (1U01HL117718–01 from the National Heart, Lung, and Blood Institute),* National Institutes of Health National Institute of Diabetes and Digestive and Kidney Diseases (1R01DK097115–01A1)*; Payment for Development of Educational Presentations: American Society of Hematology; Other: Philips Healthcare,* Comments: Work-in-Kind—Philips provided technical expertise, pulse sequences, and engineering staff and we have tested new MRI techniques, product feedback, and academic productivity (abstracts and papers). *Money paid to the institution.
Patients were recruited and scanned by V.v.d.L., H.J.M.M.M., and D.F.R.H.; the study was designed by K.J.F. and A.J.N. The data were analyzed by L.V. and H.J.M.M.M, and the final manuscript was drafted, reviewed, and edited by all authors.
This work was funded by the Dutch NutsOhra Foundation, Amsterdam, the Netherlands (grant 1303-055).
Paper previously presented, in part, at: Annual Meeting of the International Society for Magnetic Resonance in Medicine Benelux, January 16, 2015; Ghent, Belgium.
References
- 1. Helton KJ, Adams RJ, Kesler KL, et al. ; SWiTCH Investigators. Magnetic resonance imaging/angiography and transcranial Doppler velocities in sickle cell anemia: results from the SWiTCH trial. Blood 2014;124:891–98 10.1182/blood-2013-12-545186 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Adams RJ, McKie VC, Hsu L, et al. Prevention of a first stroke by transfusions in children with sickle cell anemia and abnormal results on transcranial Doppler ultrasonography. N Engl J Med 1998;339:5–11 10.1056/NEJM199807023390102 [DOI] [PubMed] [Google Scholar]
- 3. Arkuszewski M, Krejza J, Chen R, et al. Sickle cell disease: reference values and interhemispheric differences of nonimaging transcranial Doppler blood flow parameters. AJNR Am J Neuroradiol 2011;32:1444–50 10.3174/ajnr.A2529 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Oguz K, Golay X, Pizzini FB, et al. Sickle cell disease: continuous arterial spin-labeling perfusion MR imaging in children. Radiology 2003;227:567–74 10.1148/radiol.2272020903 [DOI] [PubMed] [Google Scholar]
- 5. Arkuszewski M, Krejza J, Chen R, et al. Sickle cell anemia: reference values of cerebral blood flow determined by continuous arterial spin labeling MRI. Neuroradiol J 2013;26:191–200 10.1177/197140091302600209 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Prohovnik I, Hurlet-Jensen A, Adams R, et al. Hemodynamic etiology of elevated flow velocity and stroke in sickle-cell disease. J Cereb Blood Flow Metab 2009;29:803–10 10.1038/jcbfm.2009.6 [DOI] [PubMed] [Google Scholar]
- 7. Doepp F, Kebelmann-Betzing C, Kivi A, et al. Stenosis or hyperperfusion in sickle cell disease: ultrasound assessment of cerebral blood flow volume. Ultrasound Med Biol 2012;38:1333–38 10.1016/j.ultrasmedbio.2012.04.003 [DOI] [PubMed] [Google Scholar]
- 8. Helton KJ, Glass JO, Reddick WE, et al. Comparing segmented ASL perfusion of vascular territories using manual versus semiautomated techniques in children with sickle cell anemia. J Magn Reson Imaging 2015;41:439–46 10.1002/jmri.24559 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Gevers S, Nederveen AJ, Fijnvandraat K, et al. Arterial spin labeling measurement of cerebral perfusion in children with sickle cell disease. J Magn Reson Imaging 2012;35:779–87 10.1002/jmri.23505 [DOI] [PubMed] [Google Scholar]
- 10. Varela M, Petersen ET, Golay X, et al. Cerebral blood flow measurements in infants using look-locker arterial spin labeling. J Magn Reson Imaging 2015;41:1591–600 10.1002/jmri.24716 [DOI] [PubMed] [Google Scholar]
- 11. Wu WC, St Lawrence KS, Licht DJ, et al. Quantification issues in arterial spin labeling perfusion magnetic resonance imaging. Top Magn Reson Imaging 2010;21:65–73 10.1097/RMR.0b013e31821e570a [DOI] [PubMed] [Google Scholar]
- 12. Hales PW, Kirkham FJ, Clark CA. A general model to calculate the spin-lattice (T1) relaxation time of blood, accounting for haematocrit, oxygen saturation and magnetic field strength. J Cereb Blood Flow Metab 2016;36:370–74 10.1177/0271678X15605856 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Lu H, Clingman C, Golay X, et al. Determining the longitudinal relaxation time (T1) of blood at 3.0 Tesla. Magn Reson Med 2004;52:679–82 10.1002/mrm.20178 [DOI] [PubMed] [Google Scholar]
- 14. Alsop DC, Detre JA, Golay X, et al. Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: a consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn Reson Med 2015;73:102–16 10.1002/mrm.25197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. De Vis JB, Hendrikse J, Groenendaal F, et al. Impact of neonate haematocrit variability on the longitudinal relaxation time of blood: implications for arterial spin labelling MRI. Neuroimage Clin 2014;4:517–25 10.1016/j.nicl.2014.03.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Varela M, Hajnal JV, Petersen ET, et al. A method for rapid in vivo measurement of blood T1. NMR Biomed 2011;24:80–88 10.1002/nbm.1559 [DOI] [PubMed] [Google Scholar]
- 17. Zhang X, Petersen ET, Ghariq E, et al. In vivo blood T(1) measurements at 1.5 T, 3 T, and 7 T. Magn Reson Med 2013;70:1082–86 10.1002/mrm.24550 [DOI] [PubMed] [Google Scholar]
- 18. Wu WC, Jain V, Li C, et al. In vivo venous blood T1 measurement using inversion recovery true-FISP in children and adults. Magn Reson Med 2010;64:1140–47 10.1002/mrm.22484 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Shimada K, Nagasaka T, Shidahara M, et al. In vivo measurement of longitudinal relaxation time of human blood by inversion-recovery fast gradient-echo MR imaging at 3T. Magn Reson Imaging Sci 2012;11:265–71 10.2463/mrms.11.265 [DOI] [PubMed] [Google Scholar]
- 20. Hollowell J, van Assendelft O, Gunter E, et al. Hematological and iron-related analytes: reference data for persons aged 1 year and over: United States, 1988–94. Vital Health Stat 11 2005;247:1–156 [PubMed] [Google Scholar]
- 21. Tripette J, Alexy T, Hardy-Dessources M, et al. Red blood cell aggregation, aggregate strength and oxygen transport potential of blood are abnormal in both homozygous sickle cell anemia and sickle-hemoglobin C disease. Haematologica 2009;94:1060–65 10.3324/haematol.2008.005371 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Jain V, Duda J, Avants B, et al. Longitudinal reproducibility and accuracy of pseudo-continuous arterial spin-labeled perfusion MR imaging in typically developing children. Radiology 2012;263:527–36 10.1148/radiol.12111509 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Hales PW, Kawadler JM, Aylett SE, et al. Arterial spin labeling characterization of cerebral perfusion during normal maturation from late childhood into adulthood: normal “reference range” values and their use in clinical studies. J Cereb Blood Flow Metab 2014;34:776–84 10.1038/jcbfm.2014.17 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. van der Land V, Hijmans CT, de Ruiter M, et al. Volume of white matter hyperintensities is an independent predictor of intelligence quotient and processing speed in children with sickle cell disease. Br J Haematol 2015;168:553–56 10.1111/bjh.13179 [DOI] [PubMed] [Google Scholar]
- 25. Mutsaerts HJ, van Osch MJ, Zelaya FO, et al. Multi-vendor reliability of arterial spin labeling perfusion MRI using a near-identical sequence: implications for multi-center studies. Neuroimage 2015;113:143–52 10.1016/j.neuroimage.2015.03.043 [DOI] [PubMed] [Google Scholar]
- 26. Gevers S, Heijtel D, Ferns SP, et al. Cerebral perfusion long term after therapeutic occlusion of the internal carotid artery in patients who tolerated angiographic balloon test occlusion. AJNR Am J Neuroradiol 2012;33:329–35 10.3174/ajnr.A2776 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Heijtel DF, Mutsaerts HJ, Bakker E, et al. Accuracy and precision of pseudo-continuous arterial spin labeling perfusion during baseline and hypercapnia: a head-to-head comparison with 15O H2O positron emission tomography. Neuroimage 2014;92:182–92 10.1016/j.neuroimage.2014.02.011 [DOI] [PubMed] [Google Scholar]
- 28. Herscovitch P, Raichle ME. What is the correct value for the brain–blood partition coefficient for water? J Cereb Blood Flow Metab 1985;5:65–69 10.1038/jcbfm.1985.9 [DOI] [PubMed] [Google Scholar]
- 29. Aslan S, Xu F, Wang PL, et al. Estimation of labeling efficiency in pseudocontinuous arterial spin labeling. Magn Reson Med 2010;63:765–71 10.1002/mrm.22245 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Vent-Schmidt J, Waltz X, Romana M, et al. Blood thixotropy in patients with sickle cell anaemia: role of haematocrit and red blood cell rheological properties. PLoS One 2014;9:e114412 10.1371/journal.pone.0114412 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Connes P, Coates TD. Autonomic nervous system dysfunction: implication in sickle cell disease. C R Biol 2013;336:142–47 10.1016/j.crvi.2012.09.003 [DOI] [PubMed] [Google Scholar]
- 32. Brandão MM, Fontes A, Barjas-Castro ML, et al. Optical tweezers for measuring red blood cell elasticity: application to the study of drug response in sickle cell disease. Eur J Haematol 2003;70:207–11 10.1034/j.1600-0609.2003.00027.x [DOI] [PubMed] [Google Scholar]
- 33. Hebbel RP, Yamada O, Moldow CF, et al. Abnormal adherence of sickle erythrocytes to cultured vascular endothelium: possible mechanism for microvascular occlusion in sickle cell disease. J Clin Invest 1980;65:154–60 10.1172/JCI109646 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Prengler M, Pavlakis SG, Prohovnik I, et al. Sickle cell disease: the neurological complications. Ann Neurol 2002;51:543–52 10.1002/ana.10192 [DOI] [PubMed] [Google Scholar]
- 35. Kiihne S, Bryant RG. Protein-bound water molecule counting by resolution of (1)H spin-lattice relaxation mechanisms. Biophys J 2000;78:2163–69 10.1016/S0006-3495(00)76763-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Strouse JJ, Cox CS, Melhem ER, et al. Inverse correlation between cerebral blood flow measured by continuous arterial spin-labeling (CASL) MRI and neurocognitive function in children with sickle cell anemia (SCA). Blood 2006;108:379–81 10.1182/blood-2005-10-4029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. van den Tweel XW, Nederveen AJ, Majoie CB, et al. Cerebral blood flow measurement in children with sickle cell disease using continuous arterial spin labeling at 3.0-Tesla MRI. Stroke 2009;40:795–800 10.1161/STROKEAHA.108.523308 [DOI] [PubMed] [Google Scholar]
- 38. Lotz J, Meier C, Leppert A, et al. Measurement with imaging: basic facts and implementation. Radiographics 2002;22:651–71 10.1148/radiographics.22.3.g02ma11651 [DOI] [PubMed] [Google Scholar]
- 39. Spilt A, Box FM, van der Geest RJ, et al. Reproducibility of total cerebral blood flow measurements using phase contrast magnetic resonance imaging. J Magn Reson Imaging 2002;16:1–5 10.1002/jmri.10133 [DOI] [PubMed] [Google Scholar]
- 40. Ambarki K, Wahlin A, Zarrinkoob L, et al. Accuracy of parenchymal cerebral blood flow measurements using pseudocontinuous arterial spin-labeling in healthy volunteers. AJNR Am J Neuroradiol 2015;36:1816–21 10.3174/ajnr.A4367 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.