

Understanding hidradenitis suppurativa clinical epidemiology and management facilitates early diagnosis and treatment, thereby reducing morbidity with the potential to favorably alter disease trajectory.
Abstract
Hidradenitis suppurativa is a chronic immune-mediated inflammatory skin disease with a prevalence of 0.1–1%, characterized by nodules and abscesses in the axillae, groin, and inframammary areas, sometimes developing into tunnels (or fistulas) and scars. Because hidradenitis suppurativa is more common in women and in those aged 18–40 years, obstetrician–gynecologists (ob-gyns) have the opportunity to diagnose, educate, initiate treatment, and coordinate care with ancillary health care professionals. The recently published North American treatment guidelines, along with management information for patients with hidradenitis suppurativa who are pregnant or breastfeeding, are summarized. By diagnosing and optimizing hidradenitis suppurativa treatment early in the disease course, ob-gyns can reduce morbidity, with the potential to favorably alter disease trajectory.
Obstetrician–gynecologists (ob-gyns) often serve as the primary medical contact for female patients with hidradenitis suppurativa. The first North American clinical management guidelines from the U.S. and Canadian Hidradenitis Suppurativa Foundations (NAHS guidelines hereafter) have been recently published,1,2 which creates an opportunity to summarize these guidelines and other recent related literature for ob-gyns.
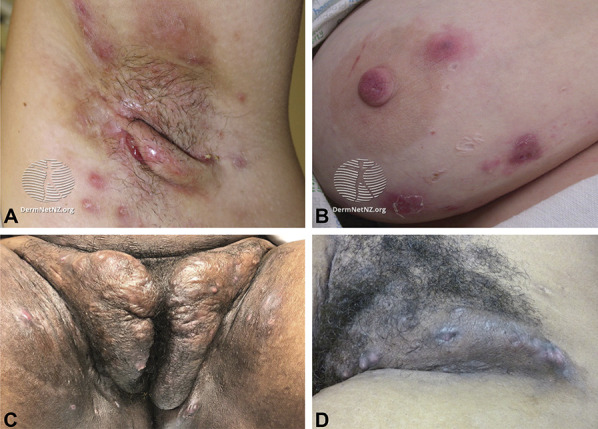
Morbidity and mortality in hidradenitis suppurativa cannot be overstated: pain and malodorous drainage torment patients, and the condition is independently associated with increased mortality after adjusting for other comorbidities.3 Early intervention requires establishing the diagnosis soon after initial symptoms, but evidence suggests that current efforts are insufficient. The average time from symptom onset to diagnosis is 10 years, with 65% of patients having six or more physician visits before diagnosis.4 This delay, coupled with multiple misdiagnoses, fragmented care, and inappropriate treatments contributes to disease progression and morbidity. Acute lesions are painful inflammatory nodules (solid, raised, round-oval lesions without puncta associated with redness and tenderness) and abscesses (fluctuant, exquisitely tender lesions that can drain purulent fluid), typically in axillary, inframammary, and inguinal areas (Fig. 1). More than half of patients experience disease flares at least weekly.4 Over time, hypertrophic scars or tunneling sinus tracts may develop that drain purulent, malodorous fluid and limit range of motion. Almost 15% report disease-related disability.4 Approximately 5% of patients with hidradenitis suppurativa report that ob-gyns were the physicians who correctly diagnosed their disease, positioning ob-gyns to help shorten diagnostic delay.4
Fig. 1. Hidradenitis suppurativa involving left axilla, with multiple inflammatory nodules and a sinus tract in the axillary vault (A), right breast, with multiple abscesses and atrophic scars (B), groin (C–D), chronic changes of hyperpigmentation and hypertrophic scarring, with persistent inflammatory activity. Figures 1A and 1B are reprinted from DermNet AZ. Accessed December 3, 2020. https://dermnetnz.org/topics/hidradenitis-suppurativa-images/?stage=Live. These images are reprinted under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 (New Zealand) license, available at https://creativecommons.org/licenses/by-nc-nd/3.0/nz/legalcode. No changes were made from the original. Figures 1C and 1D are courtesy of Christopher J. Sayed, MD. Used with permission.
Sayed. Hidradenitis Suppurativa Management Update. Obstet Gynecol 2021.
Diagnosis is based on the clinical criteria of 1) typical inflammatory lesions: abscesses, nodules, and tunnels (openings at the skin surface, sometimes draining malodorous fluid), 2) in intertriginous locations (eg, axilla, inframammary areas, crural folds), with 3) history of recurrence.1 Disease progression can be staged using the Hurley classification system: stage I connotes the absence of tunnels or scarring, stage II connotes the presence of tunnels or scarring interspersed among areas of normal skin, stage III connotes diffuse tunnels or scarring replacing all, or nearly all, normal skin in an entire anatomic region.1 Female and male patients with hidradenitis suppurativa have a similar likelihood of axillary involvement, with females more commonly having disease activity in mammary, intermammary, and inguinofemoral regions, and males more commonly having sequelae in perianal, perineal, and buttock regions5; it is unknown whether the frequency of misdiagnosis differs for men and women. Principal diseases in the differential diagnosis include inflamed epidermal inclusion cyst (or epidermoid cyst), nodulocystic acne, and furuncle (or carbuncle) (Fig. 2 and Table 1). Furuncles and inflamed epidermal inclusion cysts typically have a punctum, are not predominantly localized in intertriginous areas, and with inflamed cysts there is typically a chronic history of a noninflamed cyst present before onset of inflammation. Nodulocystic acne typically is localized to the face and torso, and acne lesions do not typically form tunnels.
Fig. 2. Differential diagnosis for hidradenitis suppurativa includes: epidermal inclusion cyst, which typically has a central punctum lacking in hidradenitis suppurativa (A), nodulocystic acne, with its different distribution (B), and furuncle, with an acute course and central pustule (C). Figure 2A is reprinted from DermNetNZ. Lam M. Epidermoid cyst. Accessed December 3, 2020. https://dermnetnz.org/topics/epidermoid-cyst/. Figure 2B is reprinted from DermNet NZ. Acne affecting the back images. Accessed December 3, 2020. https://www.dermnetnz.org/topics/acne-affecting-the-back-images/. Figures 2A and 2B are reprinted under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 (New Zealand) license, available at https://creativecommons.org/licenses/by-nc-nd/3.0/nz/legalcode. No changes were made from the original. Figure 2C is reprinted with permission from the Department of Dermatology at the Waikato District Health Board.

Sayed. Hidradenitis Suppurativa Management Update. Obstet Gynecol 2021.
Table 1.
Differential Diagnosis for Hidradenitis Suppurativa

Hidradenitis suppurativa is hypothesized to be an inflammatory, not infectious, disease of the hair follicle. Follicular hyperkeratosis, with subsequent rupture of the hair follicle and spillage of contents into the dermis, provokes intense inflammation associated with upregulation of multiple pro-inflammatory cytokines. Though dysbiosis and colonization with biofilm-forming bacteria occurs, its role in disease pathogenesis is unclear.6
EPIDEMIOLOGY AND COMORBIDITIES
The most comprehensive prevalence estimates in the United States and United Kingdom range from 0.1% to 1%.1,7,8 Most patients are aged 18–40 years. The standardized point prevalence in U.S. women is approximately 2.4-fold higher than in men7 and 3-fold higher among Black patients than White patients.7 Increased body mass index (BMI, calculated as weight in kilograms divided by height in meters squared) is positively associated with presence and severity of hidradenitis suppurativa,5,9 and smoking tobacco is a risk factor.10
As a chronic inflammatory disease, hidradenitis suppurativa exemplifies the link between integumentary and comorbid systemic disease through shared inflammatory pathways. Patients have double the comorbidity burden compared with the general population,11 and hidradenitis suppurativa has independent associations with several individual comorbid diseases (Table 2). Polycystic ovarian syndrome (PCOS) prevalence among women with hidradenitis suppurativa is 9.0%, approximately twice the independent odds for patients who do not have hidradenitis suppurativa,12 yet there is no evidence of biochemical hyperandrogenism in women with hidradenitis suppurativa compared with matched controls.13
Table 2.
Comorbid Conditions Associated With Hidradenitis Suppurativa

The most frequent, and perhaps most severe, comorbidities in hidradenitis suppurativa are psychiatric. Depression prevalence is estimated to be as high as 43%.4,14,15 Suicidal ideation or attempt has been reported in 12% of patients,4 who tragically demonstrate increased rates of completed suicide,16 particularly among women.17 The devastating effect of physical pain presumably leads to the greater reported risk for substance use disorder (4% prevalence).18 Patients with hidradenitis suppurativa were observed to have a 53% greater risk of chronic opioid use compared with controls in adjusted analyses.19
MANAGEMENT
Treatment plans must address both acute control of symptoms such as pain and drainage as well as management of chronic problems such as tunneling, disfigurement and progression. In patients with active inflammation, pharmacologic treatment is first line for all levels of disease activity. Excision is typically reserved for disease inadequately responsive to pharmacologic intervention, or for localized disease.
LIFESTYLE MODIFICATIONS
Lifestyle modifications such as smoking cessation, weight loss, or modifications in shaving or antiperspirants20 are not supported by high-quality evidence and can be considered medical and surgical treatment adjuncts. It is unclear whether changes in smoking status influence hidradenitis suppurativa severity, treatment response, or disease duration5,21–25 (though smoking cessation is encouraged to improve overall health26).
Inconsistent and limited evidence supports an association between increasing BMI and worsening hidradenitis suppurativa severity.5,27 Despite limited evidence and possible confounding variables (Rayner CR. Pathogenesis, clinical features and management of hidradenitis suppurativa [letter]. Ann R Coll Surg Engl 1997;79:309.),28–31 screening for and treating obesity (BMI 30 or higher) is encouraged.32 Though insufficient evidence exists, benefits from avoiding dairy33 and brewer's yeast (Saccharomyces cerevisiae)34 have been described.
Case reports and a survey study suggest that tight-fitting clothing or other sources of rubbing contribute to hidradenitis suppurativa flares.35–39 Whether personal care practices such as hair removal (eg, shaving) and use of deodorant or antiperspirant exacerbates this condition22 is unclear because research is limited by recall bias.40,41
Patients with hidradenitis suppurativa often show high interest in complementary and alternative medical therapy,42 but it should be considered adjunctive owing to limited evidence. An uncontrolled prospective study of zinc gluconate at 90 mg daily in 22 patients was associated with a 36% rate of clinical remission.43,44 An uncontrolled prospective study of vitamin D supplementation in 14 patients noted that all had evidence of vitamin D deficiency (serum 25-hydroxyvitamin D3 levels less than 30 ng/mL) at baseline, with serum levels negatively correlated with disease severity, and that supplementation tailored to patients' measured vitamin D level was associated with a 51% reduction in inflammatory nodule count.45 Insufficient evidence exists to generally recommend use of zinc or vitamin D.
PHARMACOLOGIC THERAPY
Topical therapy is appropriate for most patients with hidradenitis suppurativa. Based on expert opinion, the NAHS guidelines support the use of chlorhexidine, benzoyl peroxide, or zinc pyrithione antimicrobial washes; topical retinoid therapy is not recommended.2 Clindamycin 1% solution twice daily is recommended, based on placebo- and active-controlled trials,46,47 and concomitant use of benzoyl peroxide is suggested to reduce development of antibiotic resistance.2 For acute flares, intralesional triamcinolone 10 mg/mL (0.2–2.0 mL) may rapidly reduce pain and inflammation.48,49
The four recommended classes of systemic therapy include antibiotics, hormonal therapy, oral retinoids, and immunosuppressants, though comparative studies are lacking, with detailed dosing and duration information recently reviewed.50 The NAHS guidelines do not include a treatment algorithm flow diagram to tier these classes.
The NAHS guidelines make five specific recommendations for systemic antibiotics: 1) tetracyclines; 2) clindamycin combined with rifampin51–54; 3) moxifloxacin, metronidazole, and rifampin in combination; 4) dapsone; and 5) IV ertapenem, with tetracyclines and clindamycin plus rifampin receiving top-line recommendations (Table 3). Efficacy of clindamycin monotherapy (150 mg four times daily) has also been described55 as an alternative to combination therapy. Chronic therapy with clindamycin and rifampin in combination is not recommended in the NAHS guidelines, presumably because of the paucity of long-term safety data, though a critical appraisal of the literature suggests that long-term treatment may not substantially increase risks over short-term treatment.56 Because hidradenitis suppurativa is an inflammatory disease, it is unclear whether antibiotics' efficacy is due to antiinflammatory effects or disruption of host–microbiome interactions that fuel inflammation. Recurrence of disease activity frequently follows therapy interruption or discontinuation. Bacterial culture should not be routinely performed (unless secondary soft tissue infection is suspected) and does not typically guide antibiotic selection.1
Table 3.
Medical Management of Hidradenitis Suppurativa

Hormonal effect in hidradenitis suppurativa is suggested by typical disease onset around or after puberty, exacerbation during pregnancy for some patients (Fig. 3), association with PCOS, and worsening with menstrual cycles.12,57,58 The mechanism by which hormones affect the disease is unclear (there is no evidence for significant differences between hidradenitis suppurativa and control patients in mean basal levels of estrogen and other sex hormones),59 yet clinical evidence suggests that combination oral contraceptives, spironolactone, and finasteride can be effective (Table 3). Both ethinyl estradiol with norgestrel and ethinyl estradiol with cyproterone acetate resulted in similar improvement, with 50% (12/24) of patients improving or clearing completely.60 Progestin-only contraceptives should be used cautiously; a case series suggests these may sometimes trigger hidradenitis suppurativa.61 Spironolactone or finasteride should be considered as monotherapy in women with mild-to-moderate symptoms or as adjunctive agents for more severe disease. Patients reporting hidradenitis suppurativa flares around menses or with features of PCOS may more likely benefit.62,63 Metformin, 500 mg 2–3 times daily, was associated with significant improvement in a 24-week uncontrolled, prospective study. Most patients (22/25) were women with features of PCOS.64
Fig. 3. Woman with hidradenitis suppurativa on the vulva, groin, and upper inner thighs, whose hidradenitis suppurativa flared during pregnancy. Given the large disease burden and location of her hidradenitis suppurativa, the patient had discussions with her ob-gyn and ultimately had a cesarean delivery. Image courtesy of Jennifer L. Hsiao, MD. Used with permission.

Sayed. Hidradenitis Suppurativa Management Update. Obstet Gynecol 2021.
Oral retinoids are typically either ineffective in hidradenitis suppurativa, or have efficacy limited mostly to milder cases.65–67 Expert opinion suggests acitretin is superior to isotretinoin, but comparative evidence is lacking. Oral retinoids should be prescribed by those familiar with side effects, including teratogenicity, and laboratory monitoring, and mostly considered if nodulocystic acne is concomitant.
Broad immunomodulators such as methotrexate, azathioprine, and cyclosporine have shown limited efficacy in scarce published data and generally are not recommended.68–72 Prednisone can be effective at a dose of 10 mg daily as an adjunct to other therapies, though the benefits of prolonged use should be balanced against the risks of hyperglycemia, osteoporosis, and immunosuppression.73 Prednisone or prednisolone pulses (0.5–0.7 mg/kg/d tapered over several weeks) can be used as rescue therapy for flares or to bridge between long-term therapies.74
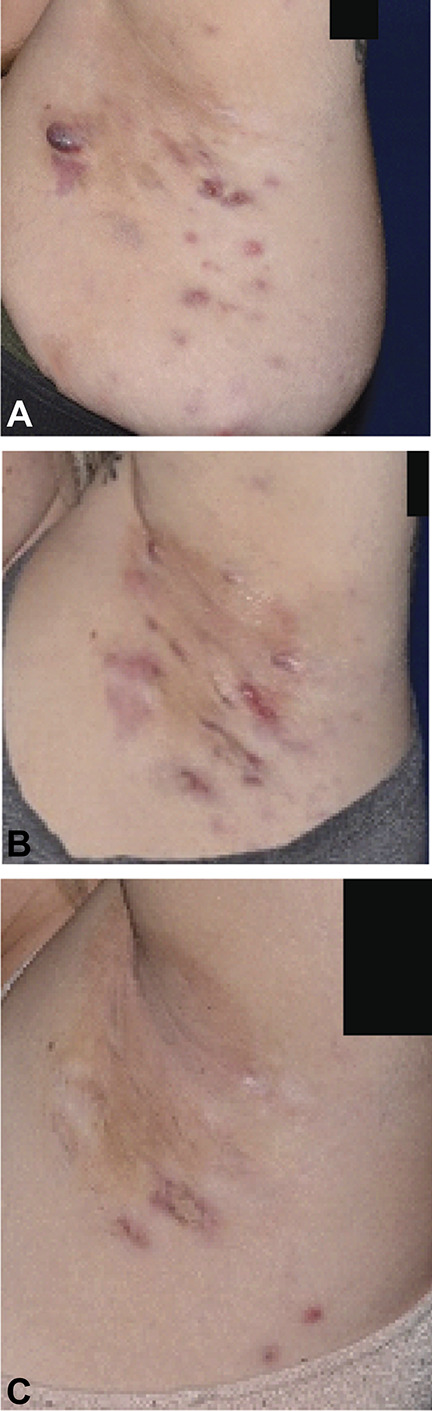
The cornerstone of therapy for moderate-to-severe hidradenitis suppurativa is immunomodulation targeting tumor necrosis factor (TNF). Adalimumab 40 mg weekly is approved by the U.S. Food and Drug Administration for treating moderate-to-severe hidradenitis suppurativa in patients aged 12 and older (dosing is 40 mg every other week for adolescents weighing less than 132 pounds) (Fig. 4).75 Two parallel double-blind placebo controlled phase 3 trials (PIONEER 1 and PIONEER 2) evaluated a primary end point of hidradenitis suppurativa clinical response at 12 weeks. Hidradenitis suppurativa clinical responses for adalimumab compared with placebo were 42% and 26%, respectively (P=.003), in PIONEER 1 and 59% and 28%, respectively (P<.001), in PIONEER 2.76 Infliximab has been investigated in smaller studies and has shown potential.77,78 Low-level evidence suggests efficacy for other TNF inhibitors and inhibitors of interleukin (IL)-12, IL-23, IL-17, and IL-1 as next-line therapies. Biologic therapies are best prescribed by practitioners familiar with their adverse effect profile.
Fig. 4. Hidradenitis suppurativa patient before and during treatment with adalimumab. Baseline (A), week 12 (B), and week 52 (C). Images courtesy of Martin M. Okun, MD, PhD. Used with permission.
Sayed. Hidradenitis Suppurativa Management Update. Obstet Gynecol 2021.
SURGICAL THERAPY
Incision and drainage can be performed with local anesthesia. New-onset (ie, acute) abscesses are more likely to heal with incision and drainage than lesions that have recurred at a site where a previous lesion had been present (ie, chronic), though substantial short-term pain relief is provided for acute and chronic lesions.79–82 Wound packing does not improve outcomes so is best avoided given the associated pain and morbidity.83 Instead of a blade, using a 4–6-mm punch tool for incision with secondary intention healing allows for drainage in the subsequent days and may prevent short-term recurrences.
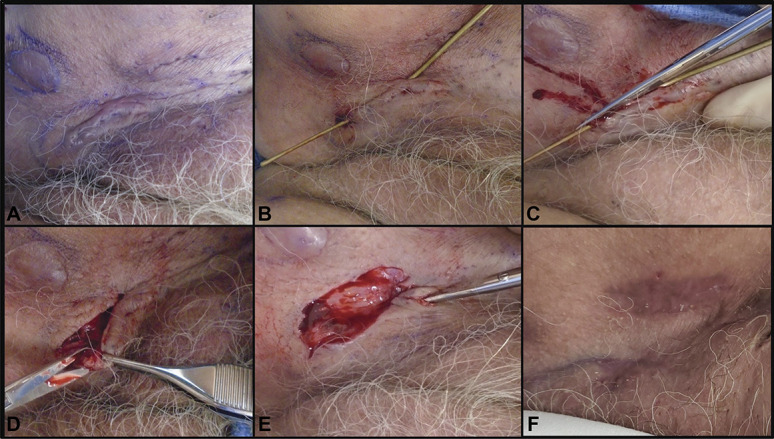
Other surgical options include deroofing, excision, or laser therapy. Deroofing involves probing chronic tunnels and sinuses, removing overlying skin, and beveling wound edges with scissor, blade, electrosurgical tools, or ablative lasers to create a broad-based wound that heals by secondary intention (Fig. 5),80,84–86 with detailed explanations and videos recently published.50 Deroofing may be used for recurrent nodules, abscesses, or interconnected sinuses, and typically leaves a relatively superficial (dermal or subcutaneous) wound.
Fig. 5. Deroofing procedure for a female, age 71 years, with long-standing hidradenitis suppurativa. A. Cutaneous tunnel of inguinal region with multiple dilated follicular openings. B. Double-ended fistula probe entering and exiting two dilated openings. Iris scissors opening the tunnel at the level of the probe (C), excising the loose tissue edge from the roof of the tunnel (D), and probing and opening a small extension at the superior tip of the deroofed wound (E). A thick layer of petrolatum is applied before application of nonstick bandaging. F. Follow-up at postoperative week 21 with absence of inflammatory nodules, abscesses, or tunnels. Images courtesy of Christopher J. Sayed, MD. Used with permission.
Sayed. Hidradenitis Suppurativa Management Update. Obstet Gynecol 2021.
Excisions may be local (specific lesion) or wide, depending on disease extent, typically limited to superficial subcutis but may extend if deeper involvement is encountered intraoperatively. Healing by secondary intention or immediate or delayed closure using grafts, flaps, or skin substitutes have been described.1 Smaller, stepwise excisions are less morbid than wider procedures, and may allow for gradual improvement without prolonged school, work, or lifestyle disruptions. More extensive excision provides more dramatic improvement in a single procedure.87,88 Excision recurrence rates were similar to deroofings in one series (approximately 25%),79 whereas, in others, the recurrence rates of wide excision using traditional or carbon dioxide laser excision were less than 5%.81,89 Risk factors for recurrence include younger age, multiple surgical sites, and perianal, vulvar, and inframammary sites. Although 95% of patients in one survey still reported disease-specific life restrictions postoperatively, 80% were satisfied or very satisfied after surgery.90
Follicular destruction with neodymium:yttrium-aluminum-garnet or alexandrite lasers, or diodes and intense pulsed light reduces disease activity, and is likely particularly important in early disease.91–101 Multiple sessions are required, but risks are low with high potential for improvement. Carbon dioxide laser requires specialized equipment and training and may lead to prolonged healing, but outcomes of excision, marsupialization, and vaporization are typically excellent.
The NAHS guidelines recommend continuing medical therapy, including biologics perioperatively because theoretical effects on wound healing from medication is less likely than the risk of perioperative disease flares that complicate recovery (Benjamin L, Cohen PF, SV Kane, Herfarth HH, Palekar N, Farraye FA, et al. 415a—Anti-tumor necrosis factor therapy is not associated with post-operative infection: results from prospective cohort of ulcerative colitis and Crohn's disease patients undergoing surgery to identify risk factors for postoperative infection I (Puccini) [abstract]. Gastroenterology 2019;156:S-80.).102,103
PAIN MANAGEMENT
Uncontrolled pain is a major cause of morbidity among individuals living with hidradenitis suppurativa. Many pain-management guidelines distinguish between nociceptive and neuropathic pain for treatment selection.104–107 Pain has been found to be both nociceptive (a direct consequence of disease activity, described as “throbbing,” “aching,” and “gnawing”) and neuropathic (dysfunction in central or peripheral nervous system, described as “burning,” “stabbing,” “stinging,” or like an electric shock)108,109 and both are exacerbated by comorbid anxiety and depression.109 Owing to this complexity, multimodal therapy is essential.
The NAHS guidelines suggest that pain treatment begins with improved disease control,1 but current therapies are sometimes inadequate,110 in which case pharmacologic and nonpharmacologic symptomatic treatments are indicated. Acute hidradenitis suppurativa flares may be treated with topical or systemic analgesics including acetaminophen, nonsteroidal antiinflammatory drugs, and limited courses of immediate release opioids (lowest dose and shortest possible duration, typically less than 2 weeks and fewer than 20 pills).111,112 The same pharmacologic classes can be employed for management of chronic nociceptive pain when topical therapies are insufficient (Table 4). A multidisciplinary approach including physical therapy, wound care, and mental or behavioral health often yields the best outcomes for chronic pain.113 A pain specialist can help explore further options such as anticonvulsants, chronic opioids, implantable devices, and nerve blocks. In our experience, referral is appropriate when a patient: 1) has had at least two failed pharmacologic pain treatments, 2) has medically refractory hidradenitis suppurativa and debilitating pain deemed unlikely to improve despite maximal medical therapy, 3) is already using chronic opioids, or 4) is at high risk for substance use disorder.
Table 4.
Pharmacologic Analgesia for Chronic Pain in Hidradenitis Suppurativa

DRESSINGS
Hidradenitis suppurativa wounds may be a consequence of disease or surgery, and require meticulous medical and surgical management. Drainage from tunnels and ulcers is an important concern for patients, so absorptive dressings that meet the dynamic needs of the wound or tunnel should be selected. Superabsorbent (eg, gelling polymers and fibers), absorbent (eg, abdominal pads), or calcium alginates and foams, in order of decreasing absorbency, can be used.114 Gentle adhesive borders reduce irritation and pain during dressing changes. Cost remains a significant barrier (silver-impregnated 4×4-inch foam sheets retail for approximately $10 per sheet). Wound colonization and biofilms may be mitigated with antiseptic washes such as chlorhexidine and its derivatives or silver-based dressings (in exudative wounds). For postsurgical wound management, negative pressure wound therapy (NPWT) with delayed reconstruction for large axillary wounds may be useful.115,116
SPECIAL POPULATIONS: PEDIATRICS AND PREGNANT
Pediatrics
Pediatric hidradenitis suppurativa is especially devastating because it strikes during the most formative years of children's emotional development. As with adults, pediatric patients bear a higher risk of metabolic syndrome, PCOS and psychiatric comorbidities. The NAHS guidelines recommend evaluating patients with hidradenitis suppurativa younger than 11 years for precocious puberty. Medical and surgical treatment options for pediatric and adult patients are similar. For acute flares antibiotics can be used, but in our practice, we limit treatment duration to 6 months, and avoid tetracyclines in children younger than 9 years. In 2018, adalimumab was approved by the U.S. Food and Drug Administration for adolescents aged 12 years and older with moderate-to-severe symptoms.
Pregnancy
Information on hidradenitis suppurativa and pregnancy is limited. Two European patient survey studies found an improvement during pregnancy in 20–30.2% and worsening in 8–16.7%,58,117 and 62% flared during pregnancy in a U.S.-based retrospective chart review.118 More than 10% of these patients continued smoking cigarettes and marijuana, highlighting the importance of cessation counseling. Gestational diabetes, gestational hypertension, and preeclampsia were more common in this cohort compared with the general U.S. population, so screening is warranted; no statistically significant differences were found for miscarriage, stillbirth, cesarean delivery, and perinatal mortality.119
Hidradenitis suppurativa treatment during pregnancy is challenging, and co-management with dermatology is recommended. Topical agents such as benzoyl peroxide wash and clindamycin lotion, gel, or solution are safe. Acetaminophen is the analgesic of choice, and oral antibiotic options include clindamycin, rifampin, metronidazole,120 and in the author's experience, cephalexin and some penicillin derivatives such as amoxicillin with clavulanate. For severe disease, a course of intravenous ertapenem may also be considered. Other systemic therapies to consider include metformin and zinc gluconate. In our practice, for the appropriately selected patient with active disease uncontrolled with other therapies, benefits of TNF antagonist therapy (such as adalimumab or infliximab) are considered to outweigh risks, particularly during the 1st and 2nd trimesters, with a recalibration of the risk-benefit analysis necessary during 3rd trimester because of increased placental transfer of monoclonal antibodies during this time.121 Neonates born to mothers who are continually treated with biologic agents should avoid live vaccinations (eg, rotavirus) for 6 months.122 Certolizumab is a pegylated TNF antagonist that does not cross the placental barrier, but there is a paucity of data regarding its use in hidradenitis suppurativa,123,124 and insurance coverage may be a barrier.
Although few safety data exist for procedures for hidradenitis suppurativa during pregnancy, intralesional triamcinolone and laser-based follicular destruction are likely safe. Excision with local anesthesia after the first trimester is also reasonable for recalcitrant areas.120 Treatment with cryoinsufflation has been reported during pregnancy, but vagal reactions may occur.125
Although expert consensus does not exist regarding how anogenital disease should affect delivery methods, author experience and survey data suggest it sometimes leads to recommendation for cesarean delivery, at times with specific use of high transverse or midline vertical incision to avoid involved areas (Fig. 3). These decisions should rely on open communication and shared decision-making between ob-gyns and patients.
Hidradenitis suppurativa may interfere with breast feeding. Of 134 infants born to affected mothers, about a quarter were bottle-fed, and maternal breast hidradenitis suppurativa was significantly associated with not breastfeeding.119 Painful axillary lesions making it difficult to lift the infant also interfere with breastfeeding, so proactive management during pregnancy and early counseling is important for supporting mothers planning to breastfeed.20 Clindamycin and rifampin are compatible with breastfeeding.120 Cephalexin, amoxicillin with clavulanate, and ertapenem are also compatible, though may cause infant diarrhea. Metformin has minimal excretion in breast milk without significant effect on infants.126,127 Adalimumab and infliximab appear to be safe during lactation though more data are needed.120,128
CONCLUSIONS
Successful management of hidradenitis suppurativa is challenging and at times requires comprehensive care from a coordinated team of health care professionals, including dermatologists, general or plastic surgeons, experts in pain management and wound care, and gastroenterologists or rheumatologists. Patients most often seek care with primary care physicians, including ob-gyns, and only one in five Americans with hidradenitis suppurativa have an established relationship with a dermatologist.129 Ob-gyns are uniquely poised to be front-line physicians for diagnosing and treating women with hidradenitis suppurativa, including partnering with dermatologists to significantly improve their care.
CME FOR THE CLINICAL EXPERT SERIES
Learning Objectives for “Clinical Epidemiology and Management of Hidradenitis Suppurativa”
After completing this learning experience, the involved learner should be able to:
Discuss the pathophysiology of hidradenitis suppurativa
List other diagnoses that should be considered for patients presenting with symptoms of hidradenitis suppurativa
Implement an effective management strategy for patients with this condition
Instructions for Obtaining AMA PRA Category 1 Credits™
Continuing Medical Education credit is provided through joint providership with The American College of Obstetricians and Gynecologists.
Obstetrics & Gynecology includes CME-certified content that is designed to meet the educational needs of its readers. This article is certified for 2 AMA PRA Category 1 Credits.™ This activity is available for credit through April 30, 2024.
Accreditation Statement
ACCME Accreditation
The American College of Obstetricians and Gynecologists is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians.
AMA PRA Category 1 Credit(s)™
The American College of Obstetricians and Gynecologists designates this journal-based CME activity for a maximum of 2 AMA PRA Category 1 Credits.™ Physicians should claim only the credit commensurate with the extent of their participation in the activity.
College Cognate Credit(s)
The American College of Obstetricians and Gynecologists designates this journal-based CME activity for a maximum of 2 Category 1 College Cognate Credits. The College has a reciprocity agreement with the AMA that allows AMA PRA Category 1 Credits™ to be equivalent to College Cognate Credits.
Disclosure of Faculty and Planning Committee Industry Relationships
In accordance with the College policy, all faculty and planning committee members have signed a conflict of interest statement in which they have disclosed any financial interests or other relationships with industry relative to article topics. Such disclosures allow the participant to evaluate better the objectivity of the information presented in the articles.
How to Earn CME Credit
To earn CME credit, you must read the article in Obstetrics & Gynecology and complete the quiz, answering at least 70 percent of the questions correctly. For more information on this CME educational offering, visit the Lippincott CMEConnection portal at https://cme.lww.com/browse/sources/196 to register and to complete the CME activity online. ACOG Fellows will receive 50% off by using coupon code, ONG50.
Hardware/software requirements are a desktop or laptop computer (Mac or PC) and an Internet browser. This activity is available for credit through April 30, 2024. To receive proper credits for this activity, each participant will need to make sure that the information on their profile for the CME platform (where this activity is located) is updated with 1) their date of birth (month and day only) and 2) their ACOG ID. In addition, participants should select that they are board-certified in obstetrics and gynecology.
The privacy policies for the Obstetrics & Gynecology website and the Lippincott CMEConnection portal are available at http://www.greenjournal.org and https://cme.lww.com/browse/sources/196, respectively.
Contact Information
Questions related to transcripts may be directed to educationcme@acog.org. For other queries, please contact the Obstetrics & Gynecology Editorial Office, 202-314-2317 or obgyn@greenjournal.org. For queries related to the CME test online, please contact ceconnection@wolterskluwer.com or 1-800-787-8985.
Footnotes
Financial Disclosure Christopher J. Sayed, MD, has been a speaker for AbbVie and Novartis, an advisor for UCB and AbbVie, and an investigator for InflaRx, UCB, Novartis, AbbVie, Chemocentryx, Incyte and GSK. Martin M. Okun, MD, PhD, has been a speaker for AbbVie and a consultant for AbbVie, Azora Therapeutics, Boehringer Ingelheim, Gilead, Glaxo Smith Kline, Incyte, Innovaderm, InflaRx, Genentech, Pfizer, Regeneron, and Seattle Genetics. The other author did not report any potential conflicts of interest.
Each author has confirmed compliance with the journal's requirements for authorship.
The authors thank the other members of the Hidradenitis Suppurativa Foundation Women's Health Subcommittee: Amit Garg, MD, Iltefat Hamzavi, MD, FAAD, Joslyn S. Kirby, MD, MS, Hadar Lev-Tov, MD, MAS, and Lauren A.V. Orenstein, MD, for assistance with manuscript drafting, review, and feedback.
Peer reviews are available at http://links.lww.com/AOG/C233.
Contributor Information
Christopher J. Sayed, Email: christopher_sayed@med.unc.edu.
Jennifer L. Hsiao, Email: jennhsiao@gmail.com.
Figure.

No available caption
REFERENCES
- 1.Alikhan A, Sayed C, Alavi A, Alhusayen R, Brassard A, Burkhart C, et al. North American clinical management guidelines for hidradenitis suppurativa: a publication from the United States and Canadian hidradenitis suppurativa Foundations. Part I: diagnosis, evaluation, and the use of complementary and procedural management. J Am Acad Dermatol 2019;81:76–90. doi: 10.1016/j.jaad.2019.02.067 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Alikhan A, Sayed C, Alavi A, Alhusayen R, Brassard A, Burkhart C, et al. North American clinical management guidelines for hidradenitis suppurativa: a publication from the United States and Canadian Hidradenitis Suppurativa Foundations: part II: topical, intralesional, and systemic medical management. J Am Acad Dermatol 2019;81:91–101. doi: 10.1016/j.jaad.2019.02.068 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Reddy S, Strunk A, Garg A. All-cause mortality among patients with hidradenitis suppurativa: a population-based cohort study in the United States. J Am Acad Dermatol 2019;81:937–42. doi: 10.1016/j.jaad.2019.06.016 [DOI] [PubMed] [Google Scholar]
- 4.Garg A, Neuren E, Cha D, Kirby JS, Ingram JR, Jemec GBE, et al. Evaluating patients' unmet needs in hidradenitis suppurativa: results from the global survey of impact and healthcare needs (VOICE) project. J Am Acad Dermatol 2020;82:366–76. doi: 10.1016/j.jaad.2019.06.1301 [DOI] [PubMed] [Google Scholar]
- 5.Canoui-Poitrine F, Revuz JE, Wolkenstein P, Viallette C, Gabison G, Pouget F, et al. Clinical characteristics of a series of 302 French patients with hidradenitis suppurativa, with an analysis of factors associated with disease severity. J Am Acad Dermatol 2009;61:51–7. doi: 10.1016/j.jaad.2009.02.013 [DOI] [PubMed] [Google Scholar]
- 6.Vossen ARJV, van der Zee HH, Prens EP. Hidradenitis suppurativa: a systematic review integrating inflammatory pathways into a cohesive pathogenic model. Front Immunol 2018;9:2965. doi: 10.3389/fimmu.2018.02965 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Garg A, Kirby JS, Lavian J, Lin G, Strunk A. Sex- and age-adjusted population analysis of prevalence estimates for hidradenitis suppurativa in the United States. JAMA Dermatol 2017;153:760–4. doi: 10.1001/jamadermatol.2017.0201 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ingram JR, Jenkins-Jones S, Knipe DW, Morgan CLI, Cannings-John R, Piguet V. Population-based Clinical Practice Research Datalink study using algorithm modelling to identify the true burden of hidradenitis suppurativa. Br J Dermatol 2018;178:917–24. doi: 10.1111/bjd.16101 [DOI] [PubMed] [Google Scholar]
- 9.Revuz JE, Canoui-Poitrine F, Wolkenstein P, Viallette C, Gabison G, Pouget F, et al. Prevalence and factors associated with hidradenitis suppurativa: results from two case-control studies. J Am Acad Dermatol 2008;59:596–601. doi: 10.1016/j.jaad.2008.06.020 [DOI] [PubMed] [Google Scholar]
- 10.Garg A, Papagermanos V, Midura M, Strunk A. Incidence of hidradenitis suppurativa among tobacco smokers: a population-based retrospective analysis in the U.S.A. Br J Dermatol 2018;178:709–14. doi: 10.1111/bjd.15939 [DOI] [PubMed] [Google Scholar]
- 11.Reddy S, Strunk A, Garg A. Comparative overall comorbidity burden among patients with hidradenitis suppurativa. JAMA Dermatol 2019;155:797–802. doi: 10.1001/jamadermatol.2019.0164 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Garg A, Neuren E, Strunk A. Hidradenitis suppurativa is associated with polycystic ovary syndrome: a population-based analysis in the United States. J Invest Dermatol 2018;138:1288–92. doi: 10.1016/j.jid.2018.01.009 [DOI] [PubMed] [Google Scholar]
- 13.Barth JH, Layton AM, Cunliffe WJ. Endocrine factors in pre- and postmenopausal women with hidradenitis suppurativa. Br J Dermatol 1996;134:1057–9. [PubMed] [Google Scholar]
- 14.Matusiak L, Bieniek A, Szepietowski JC. Psychophysical aspects of hidradenitis suppurativa. Acta Derm Venereol 2010;90:264–8. doi: 10.2340/00015555-0866 [DOI] [PubMed] [Google Scholar]
- 15.Onderdijk AJ, van der Zee HH, Esmann S, Lophaven S, Dufour DN, Jemec GB, et al. Depression in patients with hidradenitis suppurativa. J Eur Acad Dermatol Venereol 2013;27:473–8. doi: 10.1111/j.1468-3083.2012.04468.x [DOI] [PubMed] [Google Scholar]
- 16.Thorlacius L, Cohen AD, Gislason GH, Jemec GBE, Egeberg A. Increased suicide risk in patients with hidradenitis suppurativa. J Invest Dermatol 2018;138:52–7. doi: 10.1016/j.jid.2017.09.008 [DOI] [PubMed] [Google Scholar]
- 17.Tiri H, Huilaja L, Jokelainen J, Timonen M, Tasanen K. Women with hidradenitis suppurativa have an elevated risk of suicide. J Invest Dermatol 2018;138:2672–4. doi: 10.1016/j.jid.2018.06.171 [DOI] [PubMed] [Google Scholar]
- 18.Garg A, Papagermanos V, Midura M, Strunk A, Merson J. Opioid, alcohol, and cannabis misuse among patients with hidradenitis suppurativa: a population-based analysis in the United States. J Am Acad Dermatol 2018;79:495–500.e1. doi: 10.1016/j.jaad.2018.02.053 [DOI] [PubMed] [Google Scholar]
- 19.Reddy S, Orenstein LAV, Strunk A, Garg A. Incidence of long-term opioid use among opioid-naive patients with hidradenitis suppurativa in the United States. JAMA Dermatol 2019;155:1284–90. doi: 10.1001/jamadermatol.2019.2610 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Collier E, Shi VY, Parvataneni RK, Lowes MA, Hsiao JL. Special considerations for women with hidradenitis suppurativa. Int J Womens Dermato 2020;6:85–8. doi: 10.1016/j.ijwd.2020.02.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sartorius K, Emtestam L, Jemec GB, Lapins J. Objective scoring of hidradenitis suppurativa reflecting the role of tobacco smoking and obesity. Br J Dermatol 2009;161:831–9. doi: 10.1111/j.1365-2133.2009.09198.x [DOI] [PubMed] [Google Scholar]
- 22.Zouboulis CC, Bechara FG, Fritz K, Kurzen H, Liakou AI, Marsch WC, et al. S1 guideline for the treatment of hidradenitis suppurativa/acne inversa * (number ICD-10 L73.2) [in German]. J Dtsch Dermatol Ges 2012;10(suppl 5):S1–31. doi: 10.1111/j.1610-0387.2012.08006.x [DOI] [PubMed] [Google Scholar]
- 23.Schrader AM, Deckers IE, van der Zee HH, Boer J, Prens EP. Hidradenitis suppurativa: a retrospective study of 846 Dutch patients to identify factors associated with disease severity. J Am Acad Dermatol 2014;71:460–7. doi: 10.1016/j.jaad.2014.04.001 [DOI] [PubMed] [Google Scholar]
- 24.Denny G, Anadkat MJ. The effect of smoking and age on the response to first-line therapy of hidradenitis suppurativa: An institutional retrospective cohort study. J Am Acad Dermatol 2017;76:54–9. doi: 10.1016/j.jaad.2016.07.041 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Simonart T. Hidradenitis suppurativa and smoking. J Am Acad Dermatol 2010;62:149–50. doi: 10.1016/j.jaad.2009.08.001 [DOI] [PubMed] [Google Scholar]
- 26.Patnode CD, Henderson JT, Thompson JH, Senger CA, Fortmann SP, Whitlock EP. behavioral counseling and pharmacotherapy interventions for tobacco cessation in adults, including pregnant women: a review of reviews for the U.S. Preventive Services Task Force. Ann Intern Med 2015;163:608–21. doi: 10.7326/m15-0171 [DOI] [PubMed] [Google Scholar]
- 27.Vazquez BG, Alikhan A, Weaver AL, Wetter DA, Davis MD. Incidence of hidradenitis suppurativa and associated factors: a population-based study of Olmsted County, Minnesota. J Invest Dermatol 2013;133:97–103. doi: 10.1038/jid.2012.255 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Boer J. Resolution of hidradenitis suppurativa after weight loss by dietary measures, especially on frictional locations. J Eur Acad Dermatol Venereol 2016;30:895–6. doi: 10.1111/jdv.13059 [DOI] [PubMed] [Google Scholar]
- 29.Thomas CL, Gordon KD, Mortimer PS. Rapid resolution of hidradenitis suppurativa after bariatric surgical intervention. Clin Exp Dermatol 2014;39:315–8. doi: 10.1111/ced.12269 [DOI] [PubMed] [Google Scholar]
- 30.Scheinfeld N. Hidradenitis suppurativa: a practical review of possible medical treatments based on over 350 hidradenitis patients. Dermatol Online J 2013;19:1. [PubMed] [Google Scholar]
- 31.Kromann CB, Ibler KS, Kristiansen VB, Jemec GB. The influence of body weight on the prevalence and severity of hidradenitis suppurativa. Acta Derm Venereol 2014;94:553–7. doi: 10.2340/00015555-1800 [DOI] [PubMed] [Google Scholar]
- 32.LeBlanc E, O'Connor E, Whitlock EP, Patnode C, Kapka T. Screening for and management of obesity and overweight in adults. Report no.: 11-05159-EF-1. Agency for Healthcare Research and Quality (US); 2011. [PubMed] [Google Scholar]
- 33.Danby FW. Diet in the prevention of hidradenitis suppurativa (acne inversa). J Am Acad Dermatol 2015;73(5 Suppl 1):S52–4. doi: 10.1016/j.jaad.2015.07.042 [DOI] [PubMed] [Google Scholar]
- 34.Cannistrà C, Finocchi V, Trivisonno A, Tambasco D. New perspectives in the treatment of hidradenitis suppurativa: surgery and brewer's yeast-exclusion diet. Surgery 2013;154:1126–30. doi: 10.1016/j.surg.2013.04.018 [DOI] [PubMed] [Google Scholar]
- 35.Boer J, Mihajlovic D. Boils at frictional locations in a patient with hidradenitis suppurativa. Acta Dermatovenerol Croat 2016;24:303–4. [PubMed] [Google Scholar]
- 36.Dufour DN, Bryld LE, Jemec GB. Hidradenitis suppurativa complicating naevus comedonicus: the possible influence of mechanical stress on the development of hidradenitis suppurativa. Dermatology (Basel, Switzerland) 2010;220:323–5. doi: 10.1159/000287261 [DOI] [PubMed] [Google Scholar]
- 37.Bettoli V, Toni G, Ricci M, Zauli S, Virgili A. Hidradenitis suppurativa-acne inversa-like lesions complicating naevus comedonicus: second case supporting the mechanical stress as a triggering factor. G Ital Dermatol Venereol 2016;151:306–7. [PubMed] [Google Scholar]
- 38.de Winter K, van der Zee HH, Prens EP. Is mechanical stress an important pathogenic factor in hidradenitis suppurativa? Exp Dermatol 2012;21:176–7. doi: 10.1111/j.1600-0625.2012.01443.x [DOI] [PubMed] [Google Scholar]
- 39.von der Werth JM, Williams HC. The natural history of hidradenitis suppurativa. J Eur Acad Dermatol Venereol 2000;14:389–92. doi: 10.1046/j.1468-3083.2000.00087.x [DOI] [PubMed] [Google Scholar]
- 40.Edlich RF, Silloway KA, Rodeheaver GT, Cooper PH. Epidemiology, pathology, and treatment of axillary hidradenitis suppurativa. J Emerg Med 1986;4:369–78. doi: 10.1016/0736-4679(86)90214-3 [DOI] [PubMed] [Google Scholar]
- 41.Morgan WP, Leicester G. The role of depilation and deodorants in hidradenitis suppurativa. Arch Dermatol 1982;118:101–2. [PubMed] [Google Scholar]
- 42.Kearney N, Byrne N, Kirby B, Hughes R. Complementary and alternative medicine use in hidradenitis suppurativa. Br J Dermatol 2019;182:484–5. doi: 10.1111/bjd.18426 [DOI] [PubMed] [Google Scholar]
- 43.Brocard A, Knol AC, Khammari A, Dreno B. Hidradenitis suppurativa and zinc: a new therapeutic approach. A pilot study. Dermatology 2007;214:325–7. doi: 10.1159/000100883 [DOI] [PubMed] [Google Scholar]
- 44.Hessam S, Sand M, Meier NM, Gambichler T, Scholl L, Bechara FG. Combination of oral zinc gluconate and topical triclosan: an anti-inflammatory treatment modality for initial hidradenitis suppurativa. J Dermatol Sci 2016;84:197–202. doi: 10.1016/j.jdermsci.2016.08.010 [DOI] [PubMed] [Google Scholar]
- 45.Guillet A, Brocard A, Bach Ngohou K, Graveline N, Leloup AG, Ali D, et al. Verneuil's disease, innate immunity and vitamin D: a pilot study. J Eur Acad Dermatol Venereol 2015;29:1347–53. doi: 10.1111/jdv.12857 [DOI] [PubMed] [Google Scholar]
- 46.Clemmensen OJ. Topical treatment of hidradenitis suppurativa with clindamycin. Int J Dermatol 1983;22:325–8. doi: 10.1111/j.1365-4362.1983.tb02150.x [DOI] [PubMed] [Google Scholar]
- 47.Jemec GB, Wendelboe P. Topical clindamycin versus systemic tetracycline in the treatment of hidradenitis suppurativa. J Am Acad Dermatol 1998;39:971–4. doi: 10.1016/s0190-9622(98)70272-5 [DOI] [PubMed] [Google Scholar]
- 48.Riis PT, Boer J, Prens EP, Saunte DM, Deckers IE, Emtestam L, et al. Intralesional triamcinolone for flares of hidradenitis suppurativa (HS): a case series. J Am Acad Dermatol 2016;75:1151–5. doi: 10.1016/j.jaad.2016.06.049 [DOI] [PubMed] [Google Scholar]
- 49.Zouboulis CC, Tzellos T, Kyrgidis A, Jemec GBE, Bechara FG, Giamarellos-Bourboulis EJ, et al. Development and validation of the International Hidradenitis Suppurativa Severity Score System (IHS4), a novel dynamic scoring system to assess HS severity. Br J Dermatol 2017;177:1401–9. doi: 10.1111/bjd.15748 [DOI] [PubMed] [Google Scholar]
- 50.Orenstein LAV, Nguyen TV, Damiani G, Sayed C, Jemec GBE, Hamzavi I. Medical and surgical management of hidradenitis suppurativa: a review of international treatment guidelines and implementation in general dermatology practice. Dermatology 2020;236:393–412. doi: 10.1159/000507323 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Bettoli V, Zauli S, Borghi A, Toni G, Minghetti S, Ricci M, et al. Oral clindamycin and rifampicin in the treatment of hidradenitis suppurativa-acne inversa: a prospective study on 23 patients. J Eur Acad Dermatol Venereol 2014;28:125–6. doi: 10.1111/jdv.12127 [DOI] [PubMed] [Google Scholar]
- 52.Gener G, Canoui-Poitrine F, Revuz JE, Faye O, Poli F, Gabison G, et al. Combination therapy with clindamycin and rifampicin for hidradenitis suppurativa: a series of 116 consecutive patients. Dermatology 2009;219:148–54. doi: 10.1159/000228334 [DOI] [PubMed] [Google Scholar]
- 53.van der Zee HH, Boer J, Prens EP, Jemec GB. The effect of combined treatment with oral clindamycin and oral rifampicin in patients with hidradenitis suppurativa. Dermatology 2009;219:143–7. doi: 10.1159/000228337 [DOI] [PubMed] [Google Scholar]
- 54.Mendonça CO, Griffiths CE. Clindamycin and rifampicin combination therapy for hidradenitis suppurativa. Br J Dermatol 2006;154:977–8. doi: 10.1111/j.1365-2133.2006.07155.x [DOI] [PubMed] [Google Scholar]
- 55.Caposiena Caro RD, Cannizzaro MV, Botti E, Di Raimondo C, Di Matteo E, Gaziano R, et al. Clindamycin versus clindamycin plus rifampicin in hidradenitis suppurativa treatment: Clinical and ultrasound observations. J Am Acad Dermatol 2019;80:1314–21. doi: 10.1016/j.jaad.2018.11.035 [DOI] [PubMed] [Google Scholar]
- 56.Albrecht J, Baine PA, Ladizinski B, Jemec GB, Bigby M. Long-term clinical safety of clindamycin and rifampicin combination for the treatment of hidradenitis suppurativa. A Critically Appraised Topic. Br J Dermatol 2019;180:749–55. doi: 10.1111/bjd.17265 [DOI] [PubMed] [Google Scholar]
- 57.Riis PT, Ring HC, Themstrup L, Jemec GB. The role of androgens and estrogens in hidradenitis suppurativa—a systematic review. Acta Dermatovenerol Croat 2016;24:239–49. [PubMed] [Google Scholar]
- 58.Vossen AR, van Straalen KR, Prens EP, van der Zee HH. Menses and pregnancy affect symptoms in hidradenitis suppurativa: a cross-sectional study. J Am Acad Dermatol 2017;76:155–6. doi: 10.1016/j.jaad.2016.07.024 [DOI] [PubMed] [Google Scholar]
- 59.Harrison BJ, Kumar S, Read GF, Edwards CA, Scanlon MF, Hughes LE. Hidradenitis suppurativa: evidence for an endocrine abnormality. Br J Surg 1985;72:1002–4. doi: 10.1002/bjs.1800721223 [DOI] [PubMed] [Google Scholar]
- 60.Mortimer PS, Dawber RP, Gales MA, Moore RA. A double-blind controlled cross-over trial of cyproterone acetate in females with hidradenitis suppurativa. Br J Dermatol 1986;115:263–8. doi: 10.1111/j.1365-2133.1986.tb05740.x [DOI] [PubMed] [Google Scholar]
- 61.Stellon AJ, Wakeling M. Hidradenitis suppurativa associated with use of oral contraceptives. BMJ 1989;298:28–9. doi: 10.1136/bmj.298.6665.28 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Khandalavala BN, Do MV. Finasteride in hidradenitis suppurativa: a “male” therapy for a predominantly "female" disease. J Clin Aesthet Dermatol 2016;9:44–50. [PMC free article] [PubMed] [Google Scholar]
- 63.Kraft JN, Searles GE. Hidradenitis suppurativa in 64 female patients: retrospective study comparing oral antibiotics and antiandrogen therapy. J Cutan Med Surg 2007;11:125–31. doi: 10.2310/7750.2007.00019 [DOI] [PubMed] [Google Scholar]
- 64.Verdolini R, Clayton N, Smith A, Alwash N, Mannello B. Metformin for the treatment of hidradenitis suppurativa: a little help along the way. J Eur Acad Dermatol Venereol 2013;27:1101–8. doi: 10.1111/j.1468-3083.2012.04668.x [DOI] [PubMed] [Google Scholar]
- 65.Boer J, Nazary M. Long-term results of acitretin therapy for hidradenitis suppurativa. Is acne inversa also a misnomer?. Br J Dermatol 2011;164:170–5. doi: 10.1111/j.1365-2133.2010.10071.x [DOI] [PubMed] [Google Scholar]
- 66.Huang CM, Kirchhof MG. A new perspective on isotretinoin treatment of hidradenitis suppurativa: a retrospective chart review of patient outcomes. Dermatology 2017;233:120–5. doi: 10.1159/000477207 [DOI] [PubMed] [Google Scholar]
- 67.Nazary M, van der Zee HH, Prens EP, Folkerts G, Boer J. Pathogenesis and pharmacotherapy of Hidradenitis suppurativa. Eur J Pharmacol 2011;672:1–8. doi: 10.1016/j.ejphar.2011.08.047 [DOI] [PubMed] [Google Scholar]
- 68.Anderson MD, Zauli S, Bettoli V, Boer J, Jemec GB. Cyclosporine treatment of severe Hidradenitis suppurativa—a case series. J Dermatolog Treat 2016;27:247–50. doi: 10.3109/09546634.2015.1088128 [DOI] [PubMed] [Google Scholar]
- 69.Bianchi L, Hansel K, Stingeni L. Recalcitrant severe hidradenitis suppurativa successfully treated with cyclosporine A. J Am Acad Dermatol 2012;67:e278–9. doi: 10.1016/j.jaad.2012.06.011 [DOI] [PubMed] [Google Scholar]
- 70.Buckley DA, Rogers S. Cyclosporin-responsive hidradenitis suppurativa. J R Soc Med 1995;88:289–90P. [PMC free article] [PubMed] [Google Scholar]
- 71.Jemec GBE. Methotrexate is of limited value in the treatment of hidradenitis suppurativa. Clin Exp Dermatol 2002;27:528–9. doi: 10.1046/j.1365-2230.2002.11125.x [DOI] [PubMed] [Google Scholar]
- 72.Nazary M, Prens EP, Boer J. Azathioprine lacks efficacy in hidradenitis suppurativa: a retrospective study of nine patients. Br J Dermatol 2016;174:639–41. doi: 10.1111/bjd.14086 [DOI] [PubMed] [Google Scholar]
- 73.Wong D, Walsh S, Alhusayen R. Low-dose systemic corticosteroid treatment for recalcitrant hidradenitis suppurativa. J Am Acad Dermatol 2016;75:1059–62. doi: 10.1016/j.jaad.2016.06.001 [DOI] [PubMed] [Google Scholar]
- 74.Zouboulis CC, Desai N, Emtestam L, Hunger RE, Ioannides D, Juhász I, et al. European S1 guideline for the treatment of hidradenitis suppurativa/acne inversa. J Eur Acad Dermatol Venereol 2015;29:619–44. doi: 10.1111/jdv.12966 [DOI] [PubMed] [Google Scholar]
- 75.HUMIRA® [Package insert]. North Chicago, IL. AbbVie, Inc.; 2020.
- 76.Kimball AB, Okun MM, Williams DA, Gottlieb AB, Papp KA, Zouboulis CC, et al. Two phase 3 trials of adalimumab for hidradenitis suppurativa. N Engl J Med 2016;375:422–34. doi: 10.1056/NEJMoa1504370 [DOI] [PubMed] [Google Scholar]
- 77.Moriarty B, Jiyad Z, Creamer D. Four-weekly infliximab in the treatment of severe hidradenitis suppurativa. Br J Dermatol 2014;170:986–7. doi: 10.1111/bjd.12713 [DOI] [PubMed] [Google Scholar]
- 78.Oskardmay AN, Miles JA, Sayed CJ. Determining the optimal dose of infliximab for treatment of hidradenitis suppurativa. J Am Acad Dermatol 2019;81:702–8. doi: 10.1016/j.jaad.2019.05.022 [DOI] [PubMed] [Google Scholar]
- 79.Kohorst JJ, Baum CL, Otley CC, Roenigk RK, Schenck LA, Pemberton JH, et al. Surgical management of hidradenitis suppurativa: outcomes of 590 consecutive patients. Dermatol Surg 2016;42:1030–40. doi: 10.1097/DSS.0000000000000806 [DOI] [PubMed] [Google Scholar]
- 80.Mehdizadeh A, Hazen PG, Bechara FG, Zwingerman N, Moazenzadeh M, Bashash M, et al. Recurrence of hidradenitis suppurativa after surgical management: a systematic review and meta-analysis. Meta-analysis review. J Am Acad Dermatol 2015;73(5 suppl 1):S70–7. doi: 10.1016/j.jaad.2015.07.044 [DOI] [PubMed] [Google Scholar]
- 81.Ritz JP, Runkel N, Haier J, Buhr HJ. Extent of surgery and recurrence rate of hidradenitis suppurativa. Int J Colorectal Dis 1998;13:164–8. doi: 10.1007/s003840050159 [DOI] [PubMed] [Google Scholar]
- 82.Kohorst JJ, Baum CL, Otley CC, Roenigk RK, Pemberton JH, Dozois EJ, et al. Patient satisfaction and quality of life following surgery for hidradenitis suppurativa. Dermatol Surg 2017;43:125–33. doi: 10.1097/DSS.0000000000000942 [DOI] [PubMed] [Google Scholar]
- 83.O'Malley GF, Dominici P, Giraldo P, Aguilera E, Verma M, Lares C, et al. Routine packing of simple cutaneous abscesses is painful and probably unnecessary. Acad Emerg Med 2009;16:470–3. doi: 10.1111/j.1553-2712.2009.00409.x [DOI] [PubMed] [Google Scholar]
- 84.van der Zee HH, Prens EP, Boer J. Deroofing: a tissue-saving surgical technique for the treatment of mild to moderate hidradenitis suppurativa lesions. J Am Acad Dermatol 2010;63:475–80. doi: 10.1016/j.jaad.2009.12.018 [DOI] [PubMed] [Google Scholar]
- 85.Lin CH, Chang KP, Huang SH. deroofing: an effective method for treating chronic diffuse hidradenitis suppurativa. Case reports letter. Dermatol 2016;42:273–5. doi: 10.1097/DSS.0000000000000609 [DOI] [PubMed] [Google Scholar]
- 86.van Hattem S, Spoo JR, Horvath B, Jonkman MF, Leeman FW. Surgical treatment of sinuses by deroofing in hidradenitis suppurativa. Dermatol Surg 2012;38:494–7. doi: 10.1111/j.1524-4725.2011.02255.x [DOI] [PubMed] [Google Scholar]
- 87.Miedema J, Sayed C. Staged excision in the outpatient setting for the treatment of axillary hidradenitis suppurativa. Case reports letter. Dermatol 2016;42:267–9. doi: 10.1097/DSS.0000000000000620 [DOI] [PubMed] [Google Scholar]
- 88.Tchernev G, Temelkova I. Hidradenitis suppurativa (Hurley I/II): serial excisions with primary wound closure under local anesthesia as most adequate treatment approach. Open Access Maced J Med Sci 2019;7:400–2. doi: 10.3889/oamjms.2019.148 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Silverberg B, Smoot CE, Landa SJ, Parsons RW. Hidradenitis suppurativa: patient satisfaction with wound healing by secondary intention. Plast Reconstr Surg 1987;79:555–9. [PubMed] [Google Scholar]
- 90.Kofler L, Schweinzer K, Heister M, Kohler M, Breuninger H, Häfner HM. Surgical treatment of hidradenitis suppurativa: an analysis of postoperative outcome, cosmetic results and quality of life in 255 patients. J Eur Acad Dermatol Venereol 2018;32:1570–4. doi: 10.1111/jdv.14892 [DOI] [PubMed] [Google Scholar]
- 91.Tierney E, Mahmoud BH, Hexsel C, Ozog D, Hamzavi I. Randomized control trial for the treatment of hidradenitis suppurativa with a neodymium-doped yttrium aluminium garnet laser. Dermatol Surg 2009;35:1188–98. doi: 10.1111/j.1524-4725.2009.01214.x [DOI] [PubMed] [Google Scholar]
- 92.Xu LY, Wright DR, Mahmoud BH, Ozog DM, Mehregan DA, Hamzavi IH. Histopathologic study of hidradenitis suppurativa following long-pulsed 1064-nm Nd:YAG laser treatment. Randomized Controlled Trial Research Support, Non-U.S. Gov't. Arch Dermatol 2011;147:21–8. doi: 10.1001/archdermatol.2010.245 [DOI] [PubMed] [Google Scholar]
- 93.Jain V, Jain A. Use of lasers for the management of refractory cases of hidradenitis suppurativa and pilonidal sinus. J Cutan Aesthet Surg 2012;5:190–2. doi: 10.4103/0974-2077.101377 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.John H, Manoloudakis N, Stephen Sinclair J. A systematic review of the use of lasers for the treatment of hidradenitis suppurativa. J Plast Reconstr Aesthet Surg. 2016;69:1374–81. doi: 10.1016/j.bjps.2016.05.029 [DOI] [PubMed] [Google Scholar]
- 95.Zerbinati N, D'Este E, Ini L, et al. Clinical and histological changes in Hidradenitis suppurativa following 1064 nm nd:YAG intralesional laser treatment. J Biol Regul Homeost Agents 2017;31(2 suppl 2):131–40. [PubMed] [Google Scholar]
- 96.Downs A. Smoothbeam laser treatment may help improve hidradenitis suppurativa but not Hailey-Hailey disease. J Cosmet Laser Ther 2004;6:163–4. doi: 10.1080/14764170410003002 [DOI] [PubMed] [Google Scholar]
- 97.Sehgal VN, Verma P, Sawant S, Paul M. Contemporary surgical treatment of hidradenitis suppurativa (HS) with a focus on the use of the diode hair laser in a case. Case reports review. J Cosmet Laser Ther 2011;13:180–90. doi: 10.3109/14764172.2011.594066 [DOI] [PubMed] [Google Scholar]
- 98.Fabbrocini G, Franca K, Lotti T, Marasca C, Annunziata MC, Cacciapuoti S, et al. Intralesional diode laser 1064 nm for the treatment of hidradenitis suppurativa: a report of twenty patients. Open Access Maced J Med Sci 2018;6:31–4. doi: 10.3889/oamjms.2018.045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Highton L, Chan WY, Khwaja N, Laitung JK. Treatment of hidradenitis suppurativa with intense pulsed light: a prospective study. Plast Reconstr Surg 2011;128:459–66. doi: 10.1097/PRS.0b013e31821e6fb5 [DOI] [PubMed] [Google Scholar]
- 100.Piccolo D, Di Marcantonio D, Crisman G, Cannarozzo G, Sannino M, Chiricozzi A, et al. Unconventional use of intense pulsed light. Biomed Res Int 2014;2014:618206. doi: 10.1155/2014/618206 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Saunte DM, Lapins J. Lasers and intense pulsed light hidradenitis suppurativa. Dermatol Clin 2016;34:111–9. doi: 10.1016/j.det.2015.08.001 [DOI] [PubMed] [Google Scholar]
- 102.Adamina M, Bonovas S, Raine T, Spinelli A, Warusavitarne J, Armuzzi A, et al. ECCO guidelines on therapeutics in Crohn's disease: surgical treatment. J Crohns Colitis 2020;14:155–168. doi: 10.1093/ecco-jcc/jjz187 [DOI] [PubMed] [Google Scholar]
- 103.Xu Y, Yang L, An P, Zhou B, Liu G. Meta-analysis: the influence of preoperative infliximab use on postoperative complications of Crohn's disease. Inflamm Bowel Dis 2019;25:261–9. doi: 10.1093/ibd/izy246 [DOI] [PubMed] [Google Scholar]
- 104.Jongen JL, Hans G, Benzon HT, Huygen F, Hartrick CT. Neuropathic pain and pharmacological treatment. Pain Pract 2014;14:283–95. doi: 10.1111/papr.12085 [DOI] [PubMed] [Google Scholar]
- 105.Dworkin RH, O'Connor AB, Audette J, Baron R, Gourlay GK, Haanpää ML, et al. Recommendations for the pharmacological management of neuropathic pain: an overview and literature update. Mayo Clin Proc 2010;85(3 Suppl):S3–14. doi: 10.4065/mcp.2009.0649 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Chou R, Fanciullo GJ, Fine PG, Adler JA, Ballantyne JC, Davies P, et al. Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain. J Pain 2009;10:113–30. doi: 10.1016/j.jpain.2008.10.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Bruce RD, Merlin J, Lum PJ, Ahmed E, Alexander C, Corbett AH, et al. 2017 HIVMA of IDSA clinical practice guideline for the management of chronic pain in patients living with HIV. Clin Infect Dis 2017;65:e1–37. doi: 10.1093/cid/cix636 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Nielsen RM, Lindsø Andersen P, Sigsgaard V, Theut Riis P, Jemec GB. Pain perception in patients with hidradenitis suppurativa. Br J Dermatol 2020;182:166–74. doi: 10.1111/bjd.17935 [DOI] [PubMed] [Google Scholar]
- 109.Huilaja L, Hirvonen MJ, Lipitsä T, Vihervaara A, Harvima R, Sintonen H, et al. Patients with hidradenitis suppurativa may suffer from neuropathic pain: a Finnish multicenter study. J Am Acad Dermatol 2019;82:1232–4. doi: 10.1016/j.jaad.2019.11.016 [DOI] [PubMed] [Google Scholar]
- 110.Kimball AB, Sundaram M, Shields AL, Hudgens S, Okun M, Foley C, et al. Adalimumab alleviates skin pain in patients with moderate-to-severe hidradenitis suppurativa: Secondary efficacy results from the PIONEER I and PIONEER II randomized controlled trials. J Am Acad Dermatol 2018;79:1141–3. doi: 10.1016/j.jaad.2018.05.015 [DOI] [PubMed] [Google Scholar]
- 111.Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, et al. Development of the AGREE II, part 2: assessment of validity of items and tools to support application. CMAJ 2010;182:E472–8. doi: 10.1503/cmaj.091716 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Hegmann KT, Weiss MS, Bowden K, Branco F, DuBrueler K, Els C, et al. ACOEM practice guidelines: opioids for treatment of acute, subacute, chronic, and postoperative pain. J Occup Environ Med 2014;56:e143–59. doi: 10.1097/JOM.0000000000000352 [DOI] [PubMed] [Google Scholar]
- 113.Kamper SJ, Apeldoorn AT, Chiarotto A, Smeets RJ, Ostelo RW, Guzman J, et al. Multidisciplinary biopsychosocial rehabilitation for chronic low back pain: Cochrane systematic review and meta-analysis. BMJ 2015;350:h444. doi: 10.1136/bmj.h444 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Alavi A, Sibbald RG, Kirsner RS. Optimal hidradenitis suppurativa topical treatment and wound care management: a revised algorithm. J Dermatolog Treat 2018;29:383–4. doi: 10.1080/09546634.2017.1385719 [DOI] [PubMed] [Google Scholar]
- 115.Gonzaga TA, Endorf FW, Mohr WJ, Ahrenholz DH. Novel surgical approach for axillary hidradenitis suppurativa using a bilayer dermal regeneration template: a retrospective case study. J Burn Care Res 2013;34:51–7. doi: 10.1097/BCR.0b013e31826a7be7 [DOI] [PubMed] [Google Scholar]
- 116.Pearce FB, Richardson KA. Negative pressure wound therapy, staged excision and definitive closure with split-thickness skin graft for axillary hidradenitis suppurativa: a retrospective study. J Wound Care 2017;26(suppl 1):S36–42. doi: 10.12968/jowc.2017.26.Sup1.S36 [DOI] [PubMed] [Google Scholar]
- 117.Kromann CB, Deckers IE, Esmann S, Boer J, Prens EP, Jemec GB. Risk factors, clinical course and long-term prognosis in hidradenitis suppurativa: a cross-sectional study. Br J Dermatol 2014;171:819–24. doi: 10.1111/bjd.13090 [DOI] [PubMed] [Google Scholar]
- 118.Lyons AB, Peacock A, McKenzie SA, Jacobsen G, Naik HB, Shi VY, et al. Evaluation of hidradenitis suppurativa disease course during pregnancy and postpartum. JAMA Dermatol 2020;156:681–5. doi: 10.1001/jamadermatol.2020.0777 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Lyons AB, Peacock A, McKenzie SA, Jacobsen G, Naik HB, Shi VY, et al. Retrospective cohort study of pregnancy outcomes in hidradenitis suppurativa. Br J Dermatol 2020;183:945–7. doi: 10.1111/bjd.19155 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Perng P, Zampella JG, Okoye GA. Management of hidradenitis suppurativa in pregnancy. J Am Acad Dermatol 2017;76:979–89. doi: 10.1016/j.jaad.2016.10.032 [DOI] [PubMed] [Google Scholar]
- 121.Androulakis I, Zavos C, Christopoulos P, Mastorakos G, Gazouli M. Safety of anti-tumor necrosis factor therapy during pregnancy in patients with inflammatory bowel disease. World J Gastroenterol 2015;21:13205–11. doi: 10.3748/wjg.v21.i47.13205 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Smith CH, Yiu ZZN, Bale T, Burden AD, Coates LC, Edwards W, et al. British Association of Dermatologists guidelines for biologic therapy for psoriasis 2020: a rapid update. Br J Dermatol 2020;83:628–37. doi: 10.1111/bjd.19039 [DOI] [PubMed] [Google Scholar]
- 123.Savage KT, Flood KS, Porter ML, Kimball AB. TNF-α inhibitors in the treatment of hidradenitis suppurativa. Ther Adv Chronic Dis 2019;10:2040622319851640. doi: 10.1177/2040622319851640 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Naik HB, McGinness A, Shinkai K. Concurrent anticytokine biologics for the management of severe hidradenitis suppurativa: are they safe and effective? Cutis 2018;101:163;164;176. [PubMed] [Google Scholar]
- 125.Pagliarello C, Fabrizi G, Feliciani C, Di Nuzzo S. Cryoinsufflation for Hurley stage II hidradenitis suppurativa: a useful treatment option when systemic therapies should be avoided. JAMA Dermatol 2014;150:765–6. doi: 10.1001/jamadermatol.2014.430 [DOI] [PubMed] [Google Scholar]
- 126.Hale T, Kristensen J, Hackett L, Kohan R, Ilett K. Transfer of metformin into human milk. Adv Exp Med Biol 2004;554:435–6. doi: 10.1007/978-1-4757-4242-8_58 [DOI] [PubMed] [Google Scholar]
- 127.Briggs GG, Ambrose PJ, Nageotte MP, Padilla G, Wan S. Excretion of metformin into breast milk and the effect on nursing infants. Obstet Gynecol 2005;105:1437–41. doi: 10.1097/01.AOG.0000163249.65810.5b [DOI] [PubMed] [Google Scholar]
- 128.Menter A, Strober BE, Kaplan DH, Kivelevitch D, Prater EF, Stoff B, et al. Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with biologics. J Am Acad Dermatol 2019;80:1029–72. doi: 10.1016/j.jaad.2018.11.057 [DOI] [PubMed] [Google Scholar]
- 129.Garg A, Lavian J, Strunk A. Low utilization of the dermatology ambulatory encounter among patients with hidradenitis suppurativa: a population-based retrospective cohort analysis in the USA. Dermatology 2017;233:396–8. doi: 10.1159/000480379 [DOI] [PubMed] [Google Scholar]
- 130.Wertenteil S, Strunk A, Garg A. Overall and subgroup prevalence of acne vulgaris among patients with hidradenitis suppurativa. J Am Acad Dermatol 2019;80:e131–2. doi: 10.1016/j.jaad.2018.11.022 [DOI] [PubMed] [Google Scholar]
- 131.Tannenbaum R, Strunk A, Garg A. Overall and subgroup prevalence of pyoderma gangrenosum among patients with hidradenitis suppurativa: a population-based analysis in the United States. J Am Acad Dermatol 2019;80:1533–7. doi: 10.1016/j.jaad.2019.02.004 [DOI] [PubMed] [Google Scholar]
- 132.Garg A, Birabaharan M, Strunk A. Prevalence of type 2 diabetes mellitus among patients with hidradenitis suppurativa in the United States. J Am Acad Dermatol 2018;79:71–6. doi: 10.1016/j.jaad.2018.01.014 [DOI] [PubMed] [Google Scholar]
- 133.Tzellos T, Zouboulis CC, Gulliver W, Cohen AD, Wolkenstein P, Jemec GB. Cardiovascular disease risk factors in patients with hidradenitis suppurativa: a systematic review and meta-analysis of observational studies. Br J Dermatol 2015;173:1142–55. doi: 10.1111/bjd.14024 [DOI] [PubMed] [Google Scholar]
- 134.Reddy S, Strunk A, Jemec GBE, Garg A. Incidence of myocardial infarction and cerebrovascular accident in patients with hidradenitis suppurativa. JAMA Dermatol 2020;156:65–71. doi: 10.1001/jamadermatol.2019.3412 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Garg A, Hundal J, Strunk A. Overall and subgroup prevalence of Crohn disease among patients with hidradenitis suppurativa: a population-based analysis in the United States. JAMA Dermatol 2018;154:814–8. doi: 10.1001/jamadermatol.2018.0878 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Shavit E, Dreiher J, Freud T, Halevy S, Vinker S, Cohen AD. Psychiatric comorbidities in 3207 patients with hidradenitis suppurativa. J Eur Acad Dermatol Venereol 2015;29:371–6. doi: 10.1111/jdv.12567 [DOI] [PubMed] [Google Scholar]
- 137.Wertenteil S, Strunk A, Garg A. Incidence of obstructive sleep apnoea in patients with hidradenitis suppurativa: a retrospective population-based cohort analysis. Br J Dermatol 2018;179:1398–9. doi: 10.1111/bjd.16931 [DOI] [PubMed] [Google Scholar]
- 138.Tannenbaum R, Strunk A, Garg A. Association between hidradenitis suppurativa and lymphoma. JAMA Dermatol 2019;155:624–5. doi: 10.1001/jamadermatol.2018.5230 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Burmester G, Lanas A, Biasucci L, Hermann M, Lohmander S, Olivieri I, et al. The appropriate use of non-steroidal anti-inflammatory drugs in rheumatic disease: opinions of a multidisciplinary European expert panel. Ann Rheum Dis 2011;70:818–22. doi: 10.1136/ard.2010.128660 [DOI] [PMC free article] [PubMed] [Google Scholar]