

Abstract
Some individuals diagnosed with intellectual and developmental disabilities engage in automatically reinforced self-injurious behavior (SIB). For these individuals, identifying effective treatments may be difficult due to the nature of the reinforcement contingency. The purpose of this study was to review the literature on the treatment of automatically reinforced SIB to determine commonalities in procedures that produced effective and ineffective treatment outcomes, as well as historical trends in the treatment of this class of SIB. Results of this review indicated that there were many high-quality studies on this topic, but also a wide range in the quality of studies. As for effective treatments, noncontingent reinforcement (the most common treatment component) was found to be more effective when informed by a competing stimulus assessment rather than a preference assessment. Suggestions to improve the quality of the published record and areas in which additional research is needed are discussed.
Keywords: automatic reinforcement, treatment, self-injury
Many individuals with intellectual and developmental disabilities (IDD) engage in self-injurious behavior (SIB; Baghdadli, Pascal, Grisi, & Aussilloux, 2003; Bodfish, Symons, Parker, & Lewis, 2000; Soke et al., 2016). The nature of SIB as a severe problem behavior is unique because SIB produces wounds to one’s own person (Tate & Baroff, 1966). In addition, specific topographies and forms of SIB are one of the defining features of a number of behavioral phenotypes, such as Smith-Magenis, Lesch–Nyhan, and Prader-Willi syndromes (Didden, Korzilius, & Curfs, 2007; Elsea & Girirajan, 2008; Hustyi, Hammond, Rezvani, & Hall, 2013, Lee, Berkowitz, & Choi, 2002; Nyhan, 1976; Poisson et al., 2015; Symons, Butler, Sanders, Feurer, & Thompson, 1999; Thompson & Caruso, 2002). For example, in a study by Symons et al. (1999), 81% of their sample of individuals with Prader-Willi syndrome engaged in a specific form of SIB (skin picking) and often in the same body locations.
Functional analysis (FA; Iwata, Dorsey, Slifer, Bauman, & Richman, 1982/1994) research indicates that SIB was maintained by automatic reinforcement (henceforth referred to as automatically reinforced SIB) in approximately a quarter of cases. For example, Iwata, Pace, Dorsey, et al. (1994) found that SIB of individuals hospitalized for treatment was automatically reinforced in 25.7% of cases. Similarly, multiple reviews of FAs of SIB in the published record have found a similar prevalence of automatically reinforced SIB (Beavers, Iwata, and Lerman, 2013; Hanley, Iwata, & McCord, 2003; Kahng, Iwata, & Lewin, 2002b). Iwata, Pace, Dorsey, et al. identified two patterns of behavior observed in an FA that were indicative of an automatic function. The first of these patterns was SIB occurring more frequently in the alone condition of the FA relative to other conditions (i.e., when there are no materials, demands, or people present). The second pattern was SIB occurring across all conditions of the FA, including the control condition. Both of these response patterns indicate that SIB occurs independent of social consequences, suggesting that there is a direct relation between SIB and reinforcement that is not mediated by another person (Vaughan & Michael, 1982; Vollmer, 1994).
Differences Between Automatically and Socially Reinforced SIB
Applied behavior analytic research suggests some differences in the clinical presentation and treatment of automatically and socially reinforced SIB. When the results of an FA indicate a socially mediated function, the nature of the reinforcement contingency is also indicated (social positive, social negative reinforcement, or both) by increased rates of behavior as compared to the control condition. Although the rate of responding in a specific condition (e.g., the attention condition) may be affected by subtle aspects of how the reinforcer is delivered (e.g., Piazza et al., 1999), the general class of the reinforcer (e.g., social positive reinforcement) can be identified. This is not the case when the result of an FA suggests SIB is automatically reinforced.
Automatically reinforced SIB has been hypothetically linked to a number of controlling variables, including access to positive reinforcement (e.g., sensory stimulation or production of opioids) and negative reinforcement (e.g., pain attenuation). However, for a given individual, it is unclear whether their automatically reinforced behavior is a function of positive or negative reinforcement, or perhaps both. For this reason, the conclusion of automatic reinforcement is merely a useful hypothetical construct that sets the stage for additional analysis to identify the sources of that reinforcement (Kennedy, 1994). Thus with an automatic function, the class of the reinforcer remains unknown (Iwata, Dorsey, et al., 1982/1994; Kennedy & Thompson, 2000; Thompson, Symons, Delaney, & England, 1995).
Research suggests that treatment of automatically reinforced SIB may be more difficult than socially reinforced SIB because of the uncertainty in specific variables maintaining automatically reinforced SIB. Iwata, Pace, Dorsey, et al. (1994) summarized the FA outcomes for 152 individuals who engaged in SIB and treatment for 121 of these individuals. They reported some differences in the effectiveness of reinforcement-based treatments (noncontingent reinforcement and differential reinforcement) for SIB maintained by automatic reinforcement and social reinforcement. Both differential reinforcement and noncontingent reinforcement treatments were successful in more than 90% of applications for socially reinforced SIB, whereas these treatments were effective in approximately 65% of applications for automatically reinforced SIB (see Figure 6 in Iwata, Pace, Dorsey, et al., 1994). These apparent differences in treatment outcomes suggest that automatically reinforced SIB may be more resistant to treatment than socially reinforced SIB.
Hagopian, Rooker, and Zarcone (2015) conducted a consecutive case series of 38 clinical cases to describe a model for subtyping automatically reinforced SIB based on the pattern of responding in the FA. Automatically reinforced SIB was categorized as Subtype 1 if it occurred at a higher level in the no-interaction conditions (i.e., alone or ignore) relative to the control condition. It was categorized as Subtype 2 if it occurred at a comparable level across the no- interaction and control condition. A third subtype (Subtype 3) was characterized by the presence of self-restraint. Hagopian et al. (2015) found that Subtype 2 SIB was highly resistant to the least restrictive treatment (i.e., reinforcement alone) relative to socially reinforced SIB; whereas, Subtype 1 SIB was responsive to treatment at similar levels to SIB maintained by social reinforcement.
Hagopian, Rooker, Zarcone, Bonner, and Arevalo (2017) conducted a review of published research on automatically reinforced SIB to further examine SIB subtypes. They found similar differential treatment outcomes based on Subtypes 1 and 2. The findings of Hagopian et al. (2015) and Hagopian et al. (2017) in combination with Iwata, Pace, Dorsey, et al. (1994) add support to the notion that at least some forms of automatically reinforced SIB (Subtype 2) may be more resistant to treatment than socially reinforced SIB.
Differences Between Automatically Reinforced SIB and Other Behavior
Any behavior maintained by automatic reinforcement is reinforced by stimulation produced by the response itself. However, it can be argued that the stimulation produced by SIB is fundamentally different than that produced by other types of behaviors maintained by automatic reinforcement because one of the sensory consequences of SIB should be pain. For example, some evidence suggests that individuals with IDD who engage in SIB have increased sensitivity to tactile stimulation. Symons, Byiers, Raspa, Bishop, & Bailey (2010) examined the facial expressions of individuals undergoing a test of sensory evoked pain (light touch, deep pressure, pin prick, warm, and cold stimuli) in 44 adults with IDD. Of these individuals, 29 engaged in SIB, and those individuals were more facially expressive during these tests, suggesting that individuals with IDD who engage in SIB may be more sensitive to tactile stimulation. Courtemanche, Schroeder, Sheldon, Sherman, and Fowler (2012) evaluated the temporal correlation between indices of distress (thought to be correlates of painful experience) and SIB for four individuals using a lag sequential analysis. For two individuals, the authors found that distress was highly likely subsequent to SIB suggesting that distress related to pain may be related to SIB. Thus, SIB may be unique from other behaviors maintained by automatic reinforcement because both appetitive (the reinforcer) and aversive (painful stimulation) consequences may be present, although additional research is needed on this topic.
Current Knowledge of Treatment for Automatically Reinforced SIB
Current knowledge about behavioral treatment of automatically reinforced SIB is informed by a number of sources. These include: (a) individual studies in the behavior analytic literature (e.g., Tiger, Fisher, & Bouxsein, 2009); (b) review studies describing published datasets on the treatment of SIB, but not specifically automatically reinforced SIB (e.g., Kahng, Iwata, & Lewin, 2002a); and (c) review studies of the treatment of automatically reinforced problem behavior (e.g., pica, stereotypies), but not specifically SIB (e.g., LeBlanc, Patel, & Carr, 2000).
Individual studies, which use single-case experimental designs to determine the effects of behavioral treatments on the occurrence of SIB for a single or handful of individuals, comprise the majority of the research on the behavioral treatments of SIB in general, and automatically reinforced SIB in particular (Kahng, Iwata, & Lewin, 2002b). For example, Ringdahl, Vollmer, Marcus, and Roane (1997) examined the predictive validity of competing stimulus assessments (CSA) for the treatment of automatically reinforced SIB. Procedurally, a CSA concurrently measures stimulus interaction or engagement and problem behavior, as compared to the control condition where no stimulus is present (Piazza, Fisher, Hanley, Hilker, & Derby, 1996). Ringdahl et al. used CSAs to identify items to be included in a differential reinforcement of alternative behavior (DRA), a differential reinforcement of other behavior (DRO), or a noncontingent reinforcement (NCR) treatment (i.e., environmental enrichment). The authors found that the CSA correctly predicted the effectiveness of NCR to treat SIB for all three participants.
Individual studies such as that of Ringdahl et al. (1997) provide strong support for effective treatments of automatically reinforced SIB; however, individual studies are not without their weaknesses. These studies are commonly conducted with only a few individuals and, when detailing clinical care, the application of assessment and treatment procedures is (appropriately) driven by the needs of the patient. Thus, literature reviews often summarize the research in a particular area to highlight commonalities across these studies.
Two relevant literature reviews were conducted by Kahng et al. (2002a) and LeBlanc et al. (2000). Kahng et al. reviewed 35 years of published research on the behavioral treatment of SIB that was maintained by social and/or automatic reinforcement. The authors detailed the effectiveness of several behavioral treatments and reported on the relative effectiveness of these treatments over time. Specifically, the authors found that SIB was reduced by a mean of 83.7% across all published behavioral treatments. Whereas Kahng et al. focused on the treatment of SIB regardless of function, Leblanc et al. focused specifically on the effectiveness of treatments for problem behaviors maintained by automatic reinforcement (e.g., pica, SIB, stereotypies) but did not focus exclusively on SIB (i.e., less than 50% of the individuals’ data reviewed in that study engaged in SIB). In their analysis, the authors noted that CSAs have advanced our understanding of treatment for automatically reinforced behavior.
In both of these reviews, the authors did not focus solely on automatically reinforced SIB. Kahng et al. (2002a) may not have been able to conduct this analysis because the function of SIB was likely unknown for more than half their sample (particularly for articles reviewed before 1982). This type of analysis would have been outside the scope of Leblanc et al. (2000), but as a result the study did not examine how the unique properties of SIB may have differentially affected treatment outcomes for this behavior. Thus, although these articles and other review papers on SIB (e.g., Favell, McGimsey, & Schell, 1982; Matson & LuVullo, 2008) and behaviors maintained by automatic reinforcement (e.g., Lanovaz, & Sladeczek, 2012) are very informative in demonstrating the effectiveness of behavioral treatments, they are less informative about the treatment of automatically reinforced SIB in particular. In addition, more than a decade has passed since these reviews were conducted, and additional summary of more recent studies has not been conducted, particularly in light of additional evidence suggesting the differential effectiveness of treatment for socially maintained SIB versus automatic SIB (Hagopian et al., 2017).
Hagopian et al. (2017) provides a review of the literature on the treatment of automatically maintained SIB. However, because the focus of the Hagopian et al. study was to subtype FAs and determine the effectiveness of treatment across subtypes, the authors excluded from their review a large portion of the published literature on the treatment of automatically reinforced SIB. This resulted in limited information on the breadth of research on the treatment of automatically reinforced SIB. For example, the data of 27 individuals, the majority of whose data was published in this century, were excluded from their study (see Hagopian et al., supplemental table). Further, the number of excluded datasets suggested that there might be issues with the quality of research published on the topic. Thus, the purpose of this study was to critically review studies published over the last 34 years on the treatment of automatically reinforced SIB. Analyses were performed to identify trends and commonalities in procedures that produced effective and ineffective treatment outcomes. In addition, we evaluated the methodological quality of the studies, summarized current knowledge, and identified directions for future research.
METHOD
Article Search, Inclusion/Exclusion, and Coding of Articles
Studies were identified for inclusion by conducting a comprehensive search of Google Scholar, Pubmed, and Web of Science for articles published between 1982–2015 that contained the following terms: “self-injur* AND automatic reinforcement”, “SIB AND automatic reinforcement”, “self-injur* AND sensory”, “SIB AND sensory”, “self-injur* AND nonsocial”, “SIB AND nonsocial”, “self-injur* AND undifferentiated”, “SIB AND undifferentiated”, “self-restrain* AND self-injur*”, and “self-restrain* AND SIB.” We used 1982 as a search parameter because the purpose of the study was related to a particular function of SIB and a conclusive demonstration of the function of SIB was unlikely to be published prior to the Iwata, Dorsey, et al. (1994/1982) publication.
In order to try to capture all of the possible treatments attempted for automatically reinforced SIB, we applied inclusion criteria that were as broad as possible, while still ensuring the behavior being treated was thought to be automatically reinforced SIB. Thus, all articles that met the following criteria were included: (a) the article contained original research (i.e., not a review of previously published data), (b) the targeted behavior met the definition of SIB (i.e., was injurious) and was measured independently from other behaviors (i.e., the targeted problem behavior did not contain SIB and another non-self-injurious behavior), (c) SIB was reported or suggested by the authors to be maintained by automatic reinforcement (or an analogous term, such as sensory stimulation or self-stimulatory), (d) a behavioral treatment of SIB was reported, and (e) individualized treatment data were depicted in session-by-session format. In addition, all studies with individuals with SIB maintained by automatic reinforcement that Hagopian et al. (2017) had identified were included, as long as treatment data were available. Data sets were excluded if the authors concluded that SIB was maintained by social reinforcement, a behavioral treatment of SIB was not conducted, the specific type of behavioral treatment (e.g., NCR) was not indicated, or individual data on the behavioral treatment were not presented. We defined a behavioral treatment as any treatment that manipulated the external environment in an effort to reduce automatically reinforced SIB. Studies targeting hand-mouthing were excluded, as published research indicates this behavior may sometimes be injurious but is sometimes considered noninjurious (i.e., a stereotypy). For example, Roscoe, Iwata, and Zhou (2013) found that at least 20% of individuals in their study had no evidence of injury related to hand-mouthing and did not wear equipment or restraint that limited the damage produced by this behavior. In addition, a number of published reports directly state this behavior is stereotypic or proto-SIB rather than SIB (e.g., Rapp & Vollmer, 2005; Richman & Lindauer, 2005). Thus, to avoid including behaviors in this review that may be noninjurious, we chose to be conservative and exclude any studies on hand mouthing. Among those articles that met our inclusion criteria, a demonstration of experimental control in the FA or treatment was not required; however, we scored these articles on the degree to which experimental control was demonstrated (see below).
After identifying articles for inclusion, a 15-item Research Article Rating Scale (RARS) was developed to judge the quality of each article based on distinct relevant features (see Supporting Material for a copy of the RARS). The RARS was composed of five subscales: (a) the description of the participant, setting, and dependent variables; (b) measurement of the dependent variable, and interobserver agreement; (c) the presence of an FA, the length of this FA, and the inclusion of test and control conditions in the FA; (d) the degree of baseline stability (based on visual analysis), completeness/quality of experimental design, and degree of level change between phases; and (e) description of the baseline and treatment conditions, as well as experimenter control of the independent variable (during introduction and withdrawal). Each of the subscales contained three questions and each question had equal weight toward the final RARS score. For each question scorers assigned a value of full credit (1 point) for complete information, partial-credit (0.5 points) for limited or incomplete information, or no credit (zero points) for no information being provided. By totaling the number of points earned and dividing by the total number of possible points (15 points), each article received a score, and each subscale was worth a maximum of 20% of the total possible score. To ensure scoring of articles was accurate, the second and third authors were trained to score the articles using five quasirandomly selected articles. The raters then coded each article and interrater agreement was calculated using exact agreement for each item on the datasheet, and the level of agreement was determined for each article. Interrater agreement was assessed for 30.6% of articles and the mean exact agreement score across these articles was 95% (range 87.5% – 100%).
Descriptive data.
For each participant in a study, data were extracted and retained on the individual’s demographic information, response topography, the treatment setting, and treatment type. For demographic information, we retained the individual’s gender, age, level of intellectual disability, autism spectrum disorder diagnosis, and any identified genetic or medical conditions. For SIB topography, similar to Hagopian et al. (2015), we classified each specific form with respect to the area of the body to which SIB targeted. That is, SIB targeting the body (e.g., leg slapping) was recorded as body-directed, SIB targeting the head (e.g., head banging) was recorded as head-directed, SIB targeting the skin (e.g., scratching) was recorded as skin-directed, and SIB targeting the mouth or lips (e.g., tongue-biting) was recorded as mouth-directed. In one case (Barry from Ringdahl et al., 1997), two different response topographies were assessed and scored separately. For treatment settings, we identified if interventions were conducted in an outpatient day program, inpatient hospital, school, vocational setting, residential setting, or community setting; or as unknown, if the location could not be identified. For treatment types, we categorized them with respect to the components embedded within the intervention as follows: type of differential and/or noncontingent reinforcement (e.g., DRA, DRO, NCR), antecedent manipulations (e.g., the use of wrist weights as a means to increase the response effort associated with SIB), protective equipment (e.g., a helmet), blocking (e.g., a therapist using any part of their own body to physically block or interfere with the occurrence of SIB), punishment (e.g., contingent hands down for 30 s), mechanical restraint (e.g., devices used to limit the movement of extremities or prevent the occurrence of SIB, such as arm splints), and finally, multiple components if reinforcement and two of the components listed previously were present. Throughout, the term “additional component” refers only to the nonreinforcement-based procedures described above. Individual treatments were distinguished from each other by changes in fundamental components of treatment (e.g., changing from noncontingent to contingent reinforcement) or the addition of new treatment components (e.g., adding blocking to reinforcement). For example, if a single participant experienced a reinforcement treatment in an ABAB design, this would count as one implementation of reinforcement treatment; whereas if both reinforcement and reinforcement with an additional component (e.g., punishment) were experienced (e.g., ABACAC), two treatment implementations would have been included in the analysis.
For all treatments utilizing reinforcement, the specific type of reinforcement (e.g., NCR, DRO, DRA) was identified. For NCR (because this was the most common treatment), we also identified how items were identified for inclusion in treatment. Specifically, we identified if a preference assessment (Fisher et al., 1992; Pace, Ivancic, Edwards, Iwata, & Page 1985) or a CSA (Piazza et al., 1996) was used to identify the item(s) included during NCR. The primary difference between these procedures was the collection of data on the occurrence of SIB during periods in which a stimulus was present. Similarly, all additional procedures were reviewed in detail to determine the types of additional components used.
Treatment effectiveness data.
For all data sets included in the analysis, data point values were extracted using GetData Graph Digitizer (version 2.26; www.getdata-graph-digitizer.com). This computer software allows digital conversion of graphed data points into actual values. This program has been used in prior behavior-analytic (Bowman-Perrot, Burke, Zaini, Zhang, & Vannest, 2015; Hagopian et al., 2017; Levy et al., 2017) and medical research (Ma et al., 2015; Prieto, Vazquez, & Murado, 2014; Zhou et al., 2015).
To extract published data point values, the portable document format of the published graph was converted to a picture file and uploaded to the GetData program. The axes parameters were provided to the program based on the graph and the value of individual data points was determined by selecting them using a point and click method with the mouse. Once these data were obtained, we examined the procedures of each individual study to identify both the session duration and measurement type. For frequency and percentage of interval data collection, we rounded the GetData obtained value to the closet possible value given the session duration and method of data collection. For example, if the session duration was 10 min and data were presented as responses per minute (RPM), an obtained GetData value was rounded to the nearest 10th decimal place (e.g., 2.31 RPM was rounded to 2.3 RPM). If the authors did not specify the length of the session or the interval size, the unaltered GetData value was used.
After we extracted the data values for each graph using GetData, we calculated the mean occurrence (rate, percentage of intervals, or percentage of session) of SIB in baseline and treatment conditions using the last five data points in each of these conditions. For cases in which a given condition contained fewer than five data points, all data points in that phase were used. We then calculated the percent reduction in SIB during the final implementation of a given treatment condition compared to the initial baseline condition to determine the effectiveness of the intervention (mean baseline occurrence of SIB minus mean treatment occurrence of SIB divided by mean baseline occurrence of SIB multiplied by 100). Effective treatments were defined as those that produced at least an 80% reduction of target responding.
RESULTS
Results of the review identified 49 published research articles that met the inclusions criteria, detailing the treatment of 69 individuals (1.4 individuals on average per study). Table 1 shows the demographic information for these individuals. Slightly more than half of the individuals were younger than 18 years of age. A diagnosis of autism was reported for approximately one third of individuals. The majority of individuals had either profound or severe intellectual disability (62.3%). Additional genetic or medical conditions were reported for 39.1% of individuals, with the presence of some genetic or natal syndrome (n = 14) and sensory deficits (n = 8) being the most common conditions. Across the 69 individuals, 90 categories of SIB were reported (1.3 categories on average per individual), with individuals most commonly engaging in head-directed (68.1%) and/or skin-directed SIB (44.9%).
Table 1.
Participant Characteristics (n = 69)
| Participant Variable | Number of Participants | Percent of Participants |
|---|---|---|
| Age | ||
| Children (3 to 12 years) | 30 | 43.5 |
| Adolescents (13 to 18 years) | 10 | 14.5 |
| Adults (>18 years) | 29 | 42.0 |
| Autism | ||
| Yes | 21 | 30.4 |
| No/not reported | 48 | 69.6 |
| Level of Intellectual | ||
| Disability (n = 69) | ||
| None | 2 | 2.9 |
| Mild/Borderline | 1 | 1.4 |
| Moderate | 7 | 10.1 |
| Severe | 11 | 15.9 |
| Profound | 32 | 46.4 |
| Unspecified | 8 | 11.6 |
| Intellectual Disability not reported | 8 | 11.6 |
| Genetic/Medical Conditions (n = 27) | ||
| Sensory deficit | 8 | 11.6 |
| Cerebral palsy | 5 | 7.2 |
| Down syndrome | 3 | 4.3 |
| Other genetic or natal syndromes | 6 | 8.7 |
| Disorders | 5 | 7.2 |
| Hydro/microcephalus | 3 | 4.3 |
| Response Category | ||
| Head-directed | 47 | 68.1 |
| Body-directed | 9 | 13.0 |
| Skin-directed | 31 | 44.9 |
| Mouth -directed | 3 | 4.3 |
Quality Analysis of the Published Record
The quality of each article was assessed to demonstrate the relative strength (or lack thereof) of literature in this area, and to identify aspects of the published record that could be improved. The quality of each article was determined using the RARS (see Supporting Information), and the mean overall article score for all papers reviewed was 86.2% (range 53% to 100%). Table 2 shows the results across all RARS subscales.
Table 2.
Summary of All RARS Scores
| Number of articles with a perfect score | Percent of articles with perfect scores | Mean Score | Range | |
|---|---|---|---|---|
| Participants and Setting | 28 | 57.1% | 17.1 | 13.3 – 20 |
| Dependent Variables and Agreement | 36 | 73.5% | 18.2 | 13.3 – 20 |
| Functional Analysis | 24 | 49.0% | 14.3 | 0 – 20 |
| Experimental Control | 32 | 65.3% | 17.5 | 10 – 20 |
| Treatment Description | 43 | 87.8% | 19.2 | 6.7 – 20 |
In general, scores were lowest for the description of and presence of experimental control in the FA. Figure 1 provides additional detail on these data. The top panel shows the percentage of points obtained in each subscale and total percentage of points for each article. These data suggest that articles lost the most percentage points for the FA and for experimental control during treatment. Additionally, the majority of the articles scored were of a high quality (scored >80%); however, 11 articles (22.4% of the sample) scored less than 80%. In the bottom panel, the percentage of available points scored for each RARS question across all articles is shown. For example, all 49 articles provided complete information on first RARS question. These data indicated that in the minority of studies, which were not scored as high quality, the missing information in these articles tended to be related to the similar aspects. This included an incomplete description of the setting, IOA reported at less than the conventional standard or not at all, not conducting and presenting FA data, and a failure to produce a change in level (which is required to demonstrate experimental control).
Figure 1.
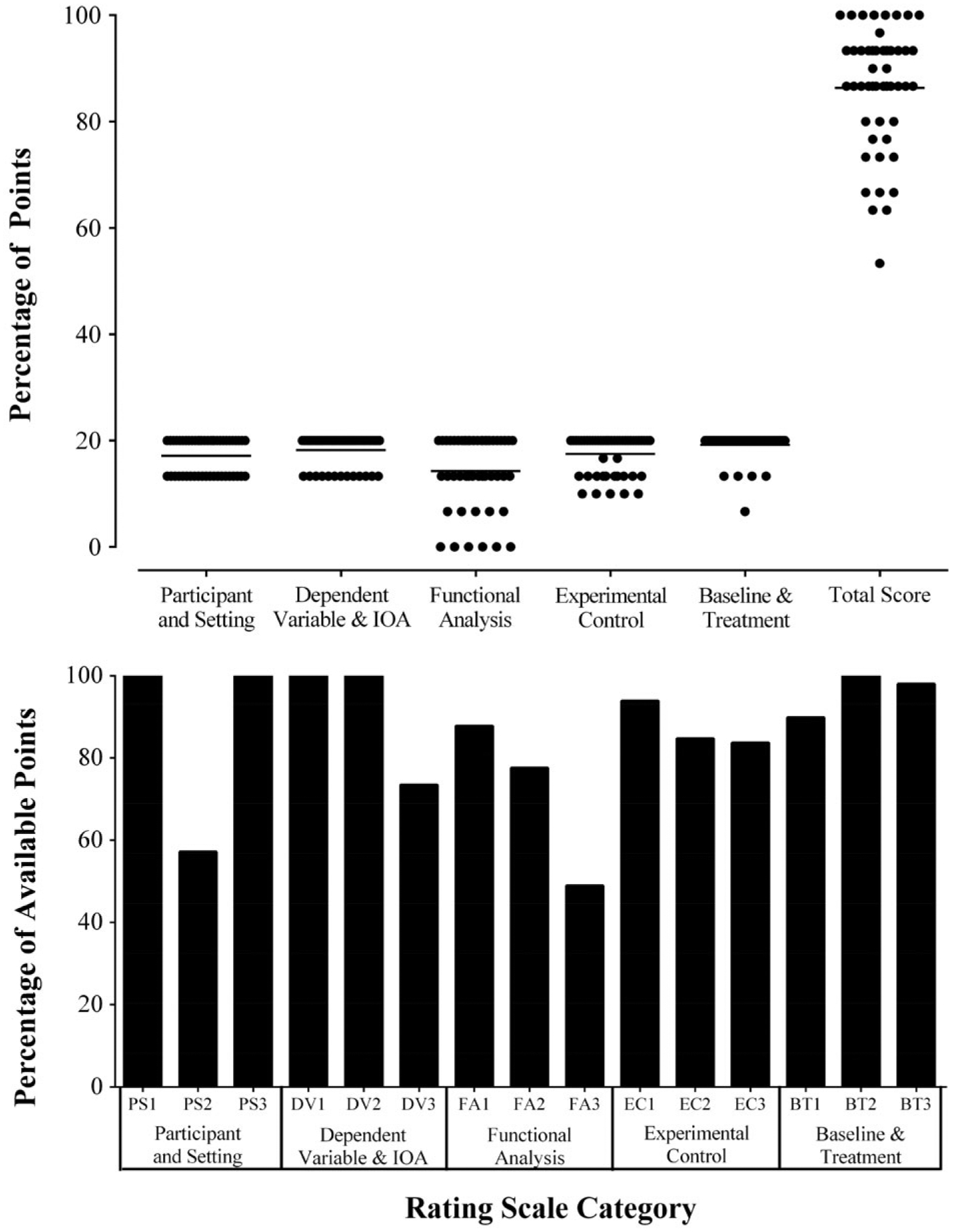
Results of the Research Article Rating Scale (RARS) analysis.. The top panel shows the percentage of points obtained in each subscale and total percentage of pointsfor each article. The bottom panel shows the percentage of available points obtained across all articles for each question on the RARS. See the RARS for the specific questions in each subscale.
Because experimental control was directly related to the purpose of the study (i.e., examining the effectiveness of treatment), additional analyses were conducted on articles relating to three aspects of the experimental control subscale. Specifically, we compared results of studies: (a) determined to have scored perfectly (20%) or not (< 20%) in this subsection; (b) determined to have a complete (e.g., ABAB), partial (e.g., ABA or BAB), or incomplete (e.g., AB) experimental design; and (c) determined to have produced a strong (i.e., ~ 80%) reduction based on visual analysis, rates were similar across baselines, and less than 25% of data points in baseline and treatment were overlapping), moderate (i.e., ~50% – 80% reduction based on visual analysis, or baseline rates were not recaptured in second baseline, or 25% – 50% of data points were overlapping) and weak (i.e., < ~50% reduction based on visual analysis) level change.
When comparing studies that scored perfectly (32) on the experimental control subsection to those that didn’t (17), we noted no difference in the distributions of treatment types employed. In addition, although the mean percent reduction (82.7%) across treatments was greater for those articles having a perfect score in comparison to those scoring less than 20% (55.2%), approximately 60% of treatments in articles scoring less than 20% were effective (producing an 80% reduction in SIB from baseline) and there was no significant difference in the percent reduction as determined by a Mann–Whitney test of statistical significance (p = .44; U = 1730). Thus, there appeared to be no relation between overall score on the experimental control subscale for an article and treatment effectiveness.
When comparing studies that used a complete (40), partial (3), or incomplete (6) design, similar to the prior results, there was no difference in the distribution of treatment types in these articles. The mean percent reduction across treatments was greatest in those studies scored as having a partial design (80.3%), followed by those scored as having an incomplete design (78.1%), and by those scored as having a complete design (66.3%) although all were relatively similar. Across these design groups, a similar proportion of treatments produced an 80% reduction in SIB from baseline (range 66.3% – 77.8%). There was no significant difference between groups when compared using a Kruskal-Wallis test of statistical significance (p = .06, H = 5.6). Thus, there appeared to be no relation between overall design and treatment effectiveness.
When comparing articles scored as having a strong (37), moderate (8), or weak (4) level change, we noted no difference in the distributions of treatment types employed in these studies. Mean percent reduction was greatest for those treatments from articles scored as having a strong level change (82.8%), followed by articles scored as having moderate level change (78.4%) and finally, articles scored as having a weak level change (−9.5%). Additionally, a difference was found across groups comparing treatment percent reduction using a Kruskal-Wallis test of statistical significance (p < 0.0001. H = 21.12). Specifically, differences were found between the percent reduction of treatments in the strong and weak level change groups and the strong and moderate level change groups. This finding was expected, as level change is directly related to treatment effectiveness. That is, a weak change in level is the definition of ineffective treatment.
In addition to these analyses, comparisons were conducted based on treatment types (described below) relating to the experimental control subscale when sufficient numbers for comparison were available; however, none of these comparisons produced differences suggesting that treatment outcomes differed based on score or experimental design. Based on this information, all of the treatment data we identified were retained for continued analysis. This was because: (a) a high proportion of treatments were effective despite coming from studies that scored less than 20% on the experimental control subscale or had a partial or incomplete design and (b) when a difference was obtained based on a quality measure of experimental design, it was related to the lack of a treatment effect and identifying when treatments were ineffective was part of the purpose of the study.
Types and outcomes of treatments of automatically reinforced SIB.
For the 69 participants, 71 designs were used to evaluate 123 attempted treatments (1.8 treatments per individual on average). For one individual, a different experimental design was used to evaluate two different behaviors and for another individual two independent designs were used to assess treatment for one behavior. Across studies, a complete (e.g., ABAB) or partial reversal (e.g., ABA) was used to evaluate treatment in 55% of cases, a multielement or multiple baseline was used in 24% of cases, a combined design (e.g., reversal plus multielement) was used in 12% of cases, and a single baseline and exposure (i.e., AB) was used in 8% of these cases. In addition, for 62 of the 69 participants (90%), authors provided information on the setting in which treatments were assessed. Assessments and treatments were conducted in outpatient clinics for 20 individuals, inpatient programs for 19 individuals, schools for 14 individuals, residential care facilities for 7 individuals, in the community for 1 individual, and in a vocational setting for 1 individual.
Table 3 shows the number of times each type of treatment was attempted. The first column provides information on the number of reinforcement procedures used alone. The following columns show the number of times each additional procedure was used. The first row provides information on the number of times procedures were used without reinforcement. The following rows provide information on the type and number of reinforcement procedures used. Of the treatments evaluated, 57 (46.3%) used reinforcement alone (i.e., with no other component), 52 (42.3%) used reinforcement plus some other component, and 14 (11.4%) did not include a reinforcement component. Of the reinforcement treatment components evaluated, NCR was evaluated 75 times (either alone or in combination with an additional procedure), differential reinforcement procedures were evaluated 27 times (alone or in combination with an additional procedure), and combined reinforcement treatments (e.g., DRA with DRO) were evaluated 7 times. In addition, punishment was the most commonly added procedure, and in fact, was used without reinforcement on six occasions. Given the difficulty in treating automatically reinforced SIB, it is not surprising that additional procedures had to be combined with reinforcement. However, it was somewhat surprising that in 14 applications a treatment with no reinforcement component at all was attempted.
Table 3.
Attempted Treatments for Automatically Reinforced SIB
| Reinforcement | None | Antecedent | Protective Equipment |
Blocking | Punishment | Restraint | Multiple Components | |
|---|---|---|---|---|---|---|---|---|
| None | n/a | 4 | 3 | 1 | 6 | 0 | 0 | 14 |
| DRA | 3 | 2 | 0 | 3 | 0 | 1 | 0 | 9 |
| DRO | 10 | 0 | 0 | 1 | 7 | 0 | 0 | 18 |
| DRA/DRO | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 3 |
| NCR | 37 | 7 | 3 | 6 | 17 | 1 | 4 | 75 |
| DRA/NCR | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 3 |
| DRA/DRO/NCR | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| Total | 57 | 13 | 6 | 11 | 30 | 2 | 4 | 123 |
Note. The columns depict the components of treatment and the rows depict the type of reinforcement used. DRA = differential reinforcement of alternative behavior; DRO = differential reinforcement of other behavior; NCR = noncontingent reinforcement; Antecedent = antecedent other than NCR.
Table 4 shows how often these treatments were successful (producing an 80% reduction in SIB from baseline) as well as the average percent reduction (in parentheses). Similar to Table 3, Table 4 shows reinforcement-based treatments with no additional components (reinforcement alone) in the first column, reinforcement with additional treatment components in subsequent columns, and treatments without reinforcement across the first row, and the type of reinforcement procedure in subsequent rows. For the 69 individuals, 85.5% had at least one successful treatment (defined as reducing target behavior by at least 80% compared to a baseline). Of the 123 treatments, 85 effective treatments were identified (69.1%) and the mean percent reduction was 69.3%. Considering each reinforcement procedure, including with and without additional components, NCR treatments were the most commonly used and effective (74.7% applications were successful and a mean percent reduction of 80.2% was found). DRA and DRO by themselves were not found to be effective, but in combination an 89% reduction was achieved. Interestingly, DRA and DRO were combined with fewer additional procedures, but when they were, these treatments were mostly successful.
Table 4.
Percentage of Effective Treatments and Mean Percentage Reduction for All Treatments
| Reinforcement | None | Antecedent | Protective Equipment | Blocking | Punishment | Restraint | Multiple Components | |
|---|---|---|---|---|---|---|---|---|
| None | n/a | 75 (82.5) | 33.3 (75.2) | 0 (73) | 66.7 (68.9) | -- | -- | 57.1 (74.9) |
| DRA | 0 (−4.4) | 100 (89.4) | -- | 66.7 (82.2) | -- | 100 (100) | -- | 55.6 (56.9) |
| DRO | 30 (−35) | -- | -- | 100 (96.4) | 100 (95.8) | -- | -- | 61.1 (23.2) |
| DRA/DRO | 66.7 (89) | -- | -- | -- | -- | -- | -- | 66.7 (89) |
| NCR | 75.7(74.2) | 71.4 (88.7) | 100 (97.8) | 66.7 (76.3) | 70.6 (85.9) | 100 (97.3) | 75 (86.4) | 74.7 (80.2) |
| DRA/NCR | 66.7 (81.4) | -- | -- | -- | -- | -- | -- | 66.7 (81.4) |
| DRA/DRO/NCR | 100 (100) | -- | -- | -- | -- | -- | -- | 100 (100) |
| Total | 63.2 (52.5) | 76.9 (86.9) | 66.7 (86.5) | 63.6 (79.4) | 63.6 (84.8) | 100 (98.6) | 75 (86.4) | 69.1 (69.3) |
Note. The columns depict the components of treatment and the rows depict the type of reinforcement used. DRA = differential reinforcement of alternative behavior; DRO = differential reinforcement of other behavior; NCR = noncontingent reinforcement.
Across the 57 reinforcement-alone treatments, 36 effective treatments were identified (63.2%), and the mean percent reduction was 52.5%. For each type of reinforcement treatment: NCR was effective in 28 applications, and the mean percent reduction was 74.2%; DRO was effective in 3 applications, and the mean percent reduction was −35% (that is, target behavior actually increased on average, as a result of the other seven failed attempts); DRA combined with DRO was effective in 2 applications, and the mean percent reduction was 89%; DRA combined with NCR was effective in 2 applications, and the mean percent reduction was 81.4%; DRA combined with DRO and NCR was effective in 1 application, and the mean percent reduction was 100%; and DRA was never effective (0%), the mean percent reduction was −4.4%.
Across the 52 treatments that used reinforcement with an additional component, 41 effective treatments were identified (78.9%), and the mean percent reduction was 87.8%. When comparing all of the additional components that were combined with reinforcement, punishment was the most frequently used additional component, with 19 of 24 applications (79.2%) effective, and a mean percent reduction of 88.8%. Additional components that appeared to be effective were the use of restraints (98.6% mean percent reduction), protective equipment (97.8% mean percent reduction); antecedents (88.9% mean percent reduction), blocking (80.1% mean percent reduction), and multiple components (86.4% mean percent reduction).
For the reinforcement components used with these additional procedures: the use of NCR was effective in 28 of 38 applications (73.7%), with a mean percent reduction of 86.2%; DRO was effective in 8 of 8 applications (100%), with a mean percent reduction of 95.8%, and DRA was effective in 5 of 6 applications (83.3%), with a mean percent reduction of 87.6%. Of the 14 treatments without reinforcement: punishment was effective in four applications (66.7%) with a mean percent reduction of 68.9%; the use of an antecedent component other than NCR was effective in three applications (75%), with a mean percent reduction of 82.5%; protective equipment was effective in a single application (33.3%), with a mean percent reduction of 75.2%; and blocking did not quite meet the criteria for effectiveness during the single application it was attempted; there was a 73% percent reduction.
Regarding treatment effectiveness, results of the current analysis indicate that a successful treatment of automatically reinforced SIB was developed for most individuals (59 out of 69). Of the 123 treatments of automatically reinforced SIB evaluated, 69.1% of treatments attempted reduced SIB by 80% from baseline (a very similar finding to Iwata, Pace, Dorsey, et al., 1994), and the mean percent reduction across all treatments was 69.3%; however, diverse outcomes were observed across specific treatments. For example, given an equal number of applications, DRA alone never produced an 80% reduction in SIB, with a mean percent reduction of −4.4%; whereas, NCR with protective equipment produced an 80% reduction in SIB in 100% of applications with a mean percent reduction of 97.8%. These results should be tempered by the potential for publication bias, which has been noted with some behavior analytic procedures (Sham & Smith, 2014). However, the behavior analytic research also suggests that some behavioral treatments (e.g., NCR) may have similar effectiveness in the published record and when used clinically (Phillips, Iannaccone, Rooker, & Hagopian, 2017).
Historical trends in the treatment of automatically reinforced SIB.
Figure 2 shows the number of procedures attempted and successful when reinforcement alone was implemented (top panel), reinforcement plus other components (middle panel), and treatments without reinforcement (bottom panel) presented cumulatively across the 34-year period analyzed in this study. A dramatic increase in the number of reinforcement and reinforcement plus other components was observed starting in 1996 and continuing to 2009, after which, reinforcement alone treatments were much more likely to be published than reinforcement plus other component treatments. Comparing the past decade (2006 – 2015) and the decade before (1996 – 2005), both reinforcement alone and reinforcement with other components have become more effective over time. For reinforcement alone, treatment was effective in 15 of 25 applications (60%) during the 1996 – 2005 decade; whereas, this treatment was effective in 15 of 21 applications (71.4%) during the next decade. For reinforcement with additional components, treatment was effective in 24 of 31 applications (77.4%) during the 1996 – 2005 period; whereas, these treatments were effective in 5 of 6 applications (83.3%) during 2006 – 2015 period. Similar analysis was not conducted for treatments without reinforcement, because so few applications were conducted during the same period.
Figure 2.
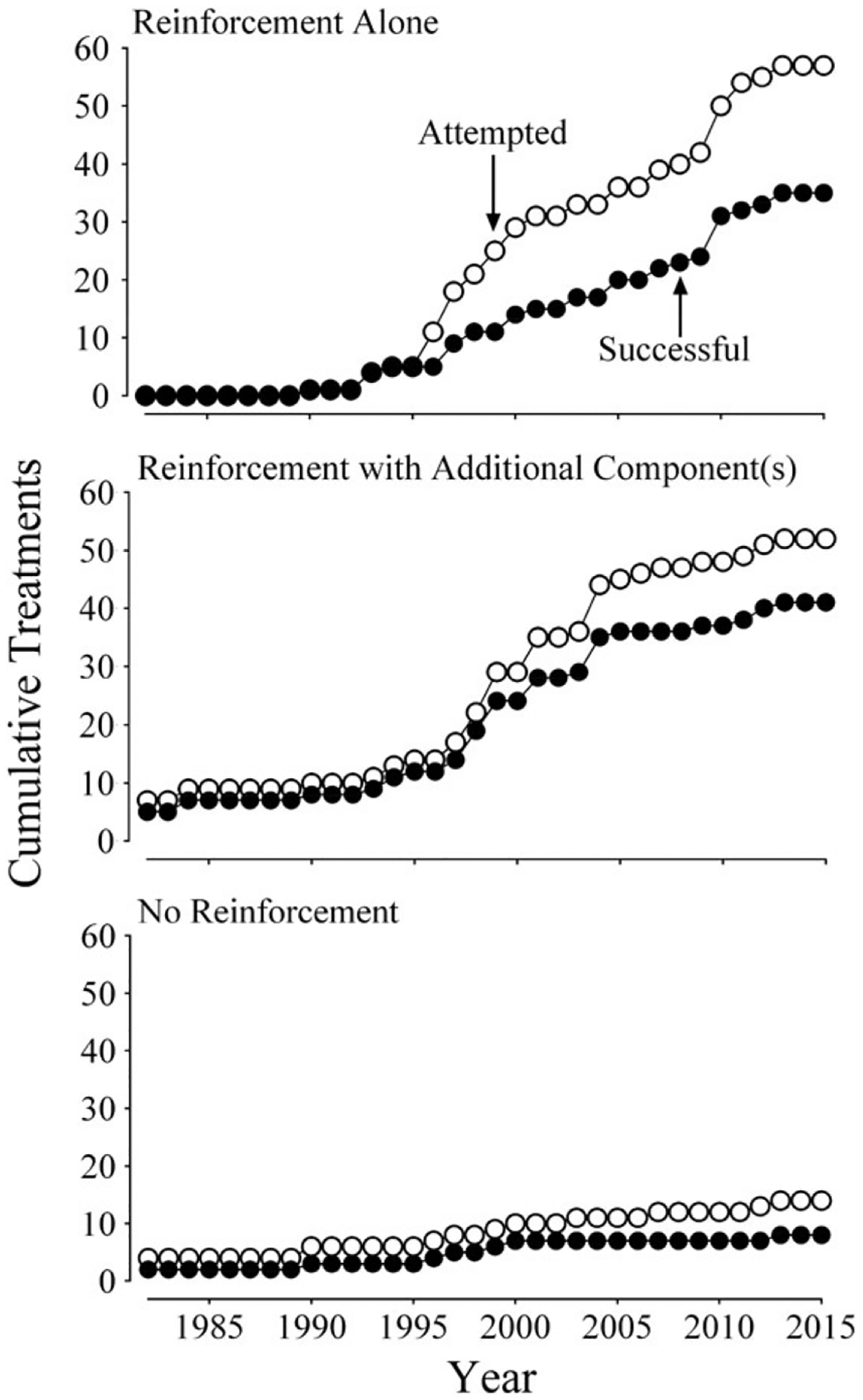
Cumulative use and effectiveness of reinforcement (top panel), reinforcement plus additional components (middle panel), and no reinforcement (bottom panel) treatments since 1982.
Figure 3 shows the data from table 2 across the 34-year period in 5-year bins. Between 1996 and 2005, a large increase in the number of treatments using punishment and antecedent (other than NCR) components was observed. The most common form of punishment was response cost (33.3%), followed closely by a hands-down procedure (21.2%) and overcorrection (12.1%). No other punishment procedure was conducted more than twice. Since 2005, there has been a slight increase in the use of less restrictive components (antecedents, blocking, and equipment) and a large decrease in the use of more restrictive procedures (punishment, restraint, and multiple components). Comparing data from the past decade (2006 – 2015) and the decade before (1996 – 2005) indicates a substantial decrease in the use of punishment. In the past decade (2006 – 2015), of the 15 articles reviewed only one application of punishment was attempted (proportion of studies = 0.07); in the decade before, of the 23 articles reviewed 16 applications of punishment were attempted (proportion of studies = 0.7). This translates to a 90% reduction in the use of punishment across the two decades.
Figure 3.
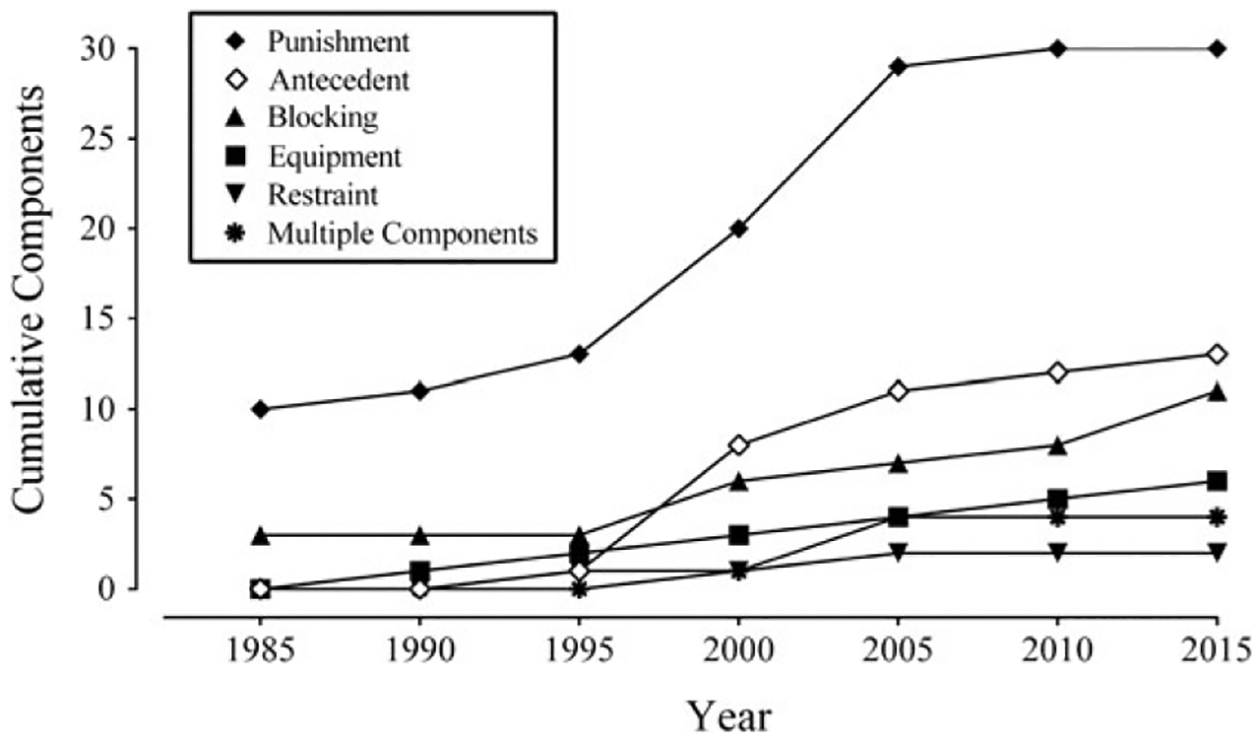
Cumulative use of nonreinforcement components since 1982 based on the studies used for this review.
Because NCR was commonly evaluated (making up more than half of the sample), additional analyses regarding this treatment were conducted. As previously mentioned, each NCR article was coded on the procedure used (e.g., CSA) to determine the item included in NCR. Across all 75 NCR treatments, we could not determine how an item came to be included in NCR in 10 implementations. For the remaining 65 implementations, the item was selected based on CSAs in 33 implementations (44% of NCR treatments), based on a preference assessment in 25 implementations (33.3% of NCR treatments), and based on anecdotal observation or report in 7 implementations (9.3% of NCR treatments).
Figure 4 shows the historical use of preference and competition procedures to identify the item included in NCR-alone (top panel) and in NCR plus additional components (bottom panel) over 5-year periods since 1990. Neither preference nor competition procedures were identified as being used for NCR prior to 1990. For NCR-alone treatments, trends indicate that preference assessments and CSAs were used approximately the same amount for the first decade (1990 – 2000). However, since 2000, CSAs were much more likely when used for NCR-alone (top panel). The use of CSAs for NCR with an additional component also increased, but only slightly between 2010 and 2015 (bottom panel).
Figure 4.
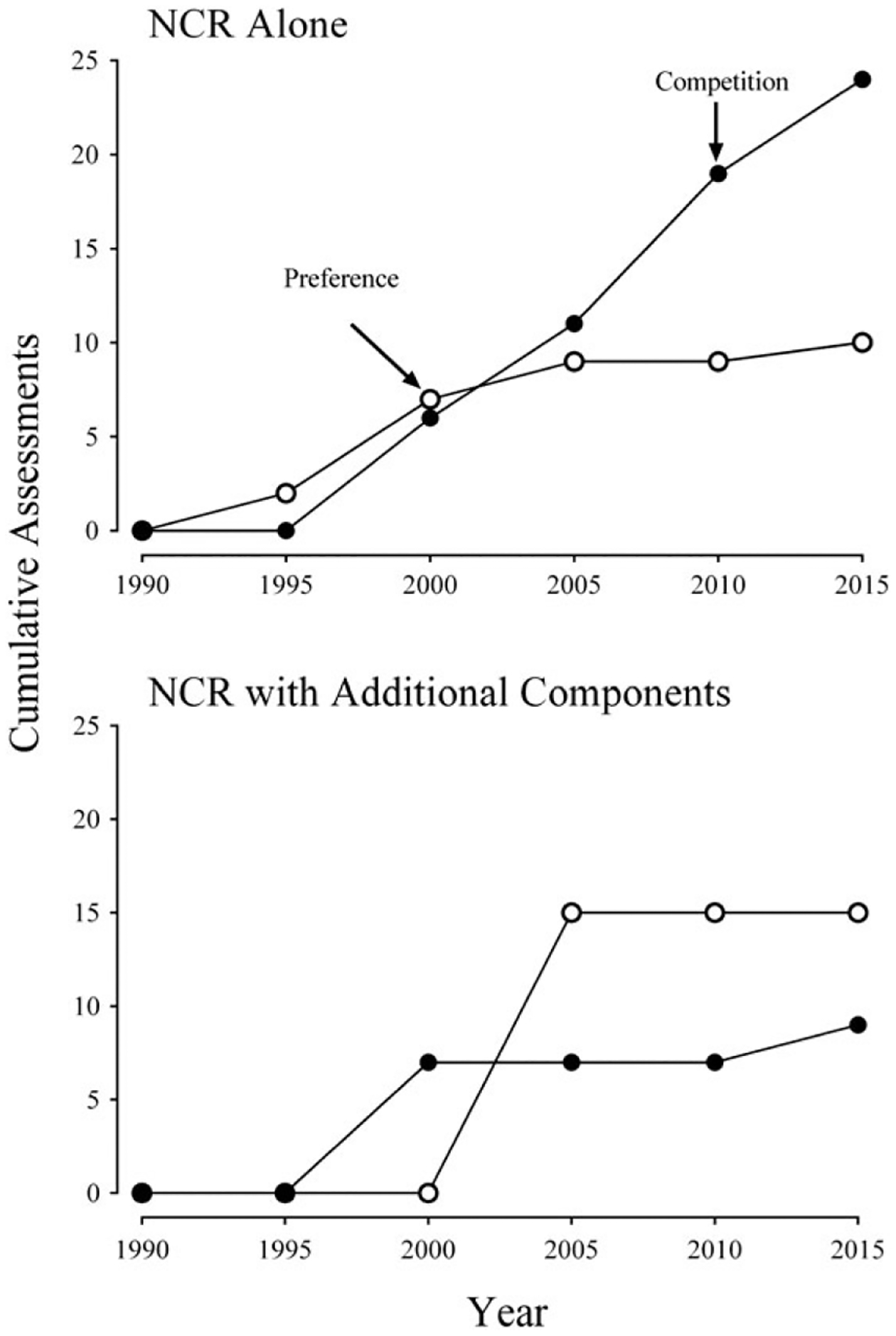
Cumulative competition and preference procedures used to identify items included in NCR-alone (top panel) and NCR with additonal components (bottom panel) treatments.
Figure 5 shows the number and effectiveness of NCR-alone and NCR plus other components treatments based on the type of procedure used to select the item included in NCR. NCR alone was attempted 10 times based on a preference assessment, and was effective 6 times (60%); whereas, this treatment was attempted 24 times based on a CSA procedure, and was effective 19 times (79.2%). NCR with an additional component was attempted 15 times based on a preference assessment, and was effective 11 times (73.3%); whereas, this treatment was attempted 9 times based on a CSA procedure and was effective 7 times (77.8%). Across all NCR treatments, when a preassessment was used to identify the item(s) included in NCR, this treatment was attempted 25 times based on preference, and effective 17 times (68%); whereas, this treatment was attempted 33 times based on competition and found to be effective 26 times (78.8%).
Figure 5.
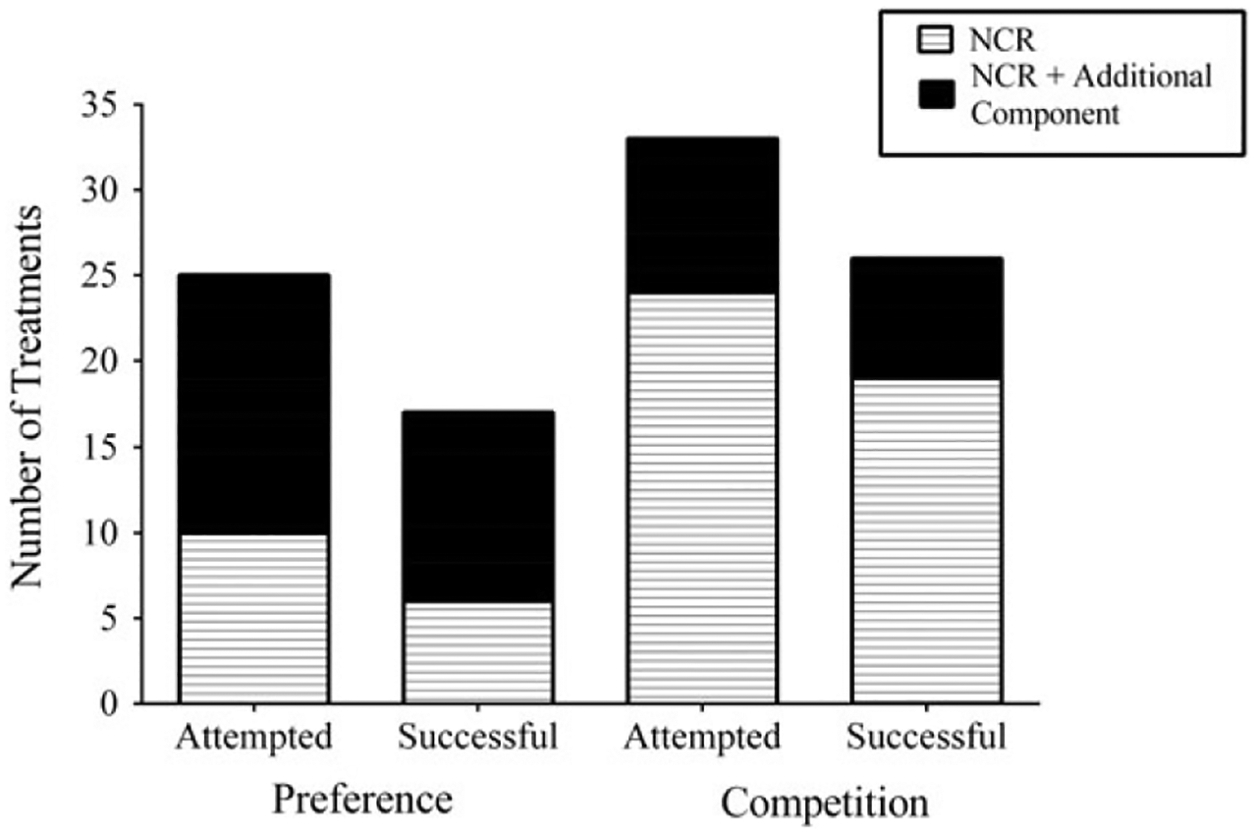
Frequency of attempted and successful NCR treatments using preference and competition procedures.
DISCUSSION
Hagopian et al. (2017) reviewed the treatment of automatically reinforced SIB for 20 individuals with 38 treatments, with the focus on determining how subtypes of automatically reinforced SIB responded to similar treatments. Expanding the inclusion and exclusion criteria from the Hagopian et al. study, we identified an additional 49 individuals who engaged in automatically reinforced SIB and an additional 85 treatments for this behavior.
Results of our analysis indicated that the majority of articles published on automatically reinforced SIB were of a high quality. Several studies identified as “low quality” (e.g., having a poor design) did in fact report highly successful treatment outcomes (e.g., Stokes & Luiselli, 2008). Thus, we felt this justified the inclusion of these studies. Using our scoring procedure, approximately 73% of articles scored above an 80% regarding the quality of their description, as well as their design. However, when analyzing these scores, the lowest proportion was awarded for the FA description and data, as well as the treatment data subscales.
Eighty-eight percent of articles reported conducting an FA. Of those articles that conducted an FA, the description of the FA was detailed enough to determine an appropriate test (e.g., alone) and control (e.g., play) condition. However, far fewer details were provided regarding the length of FAs (i.e., the number of series of the FA conducted to determine an automatic function). Indeed, across all 49 studies, the majority of studies did not provide evidence that an FA of sufficient length (three series) was used to determine behavior maintained by automatic reinforcement; six studies did not conduct an FA, three studies provided evidence that less than three series had been conducted (based on an FA graph), and 22 studies provided no detail (did not have an FA graph). Given that it may have taken several years for FA methodology to become disseminated to the research and clinical communities, it is not surprising that some researchers may not have conducted an FA. However, the practice in publication of simply reporting that an FA was conducted and that behavior was determined to be automatic (rather than presenting description and data depiction of the FA to the reader) has reduced the quality of literature when comparing FA results to treatment results, particularly for automatically reinforced SIB (Hagopian et al., 2017). These results suggest that it may be unclear at present the types of data that would be relevant for future retrospective or meta-analysis, thus it would be in the best interest of the community to provide more detailed information in publication when procedures are conducted, rather than referring to a common procedure and a brief statement of its outcomes.
For treatment data, only the minority of studies used a design that would not allow for a demonstration of experimental control. Much more commonly, a failure in level change was observed while using an appropriate single subject design, thus not allowing for the demonstration of experimental control. This finding should be tempered by the known resistance of automatically reinforced SIB to treatment (e.g., Berg et al., 2016; Hagopian et al., 2017). However, given the heterogeneity of treatments attempted (21 treatment types reported in this study), additional efforts should be made to use strong experimental designs in future studies.
Although the number of applications varied across different treatment types, a number of findings are relevant for the clinical care of individuals who engage in automatically reinforced SIB. With the exception of DRA with DRO and NCR, which was attempted only once, NCR was the most effective reinforcement-alone treatment. When NCR was combined with an additional component, the effectiveness of this intervention improved for five out of six of these components. Although NCR was the most effective reinforcement-alone treatment, both DRA and DRO were more significantly improved than NCR when other components were added. In fact, DRA and DRO with additional components were both more effective than NCR alone, and when all three reinforcement procedures included additional components, the mean percent reduction was greater than 80% for all treatments. Although this finding is likely related to a ceiling effect (i.e., NCR alone was already mostly effective, so there was little room for improvement), these results suggest that similar effectiveness may be obtained across reinforcement procedures when additional components are included, and that particular components may complement each other in treatment packages.
These results also suggested some differences in the effectiveness of components used to treat automatically reinforced SIB. As might be expected, the most restrictive treatment (restraint) was highly effective regardless of the type of reinforcement treatment used. Unexpectedly, punishment (another component usually considered very restrictive) when added to reinforcement alone was not as effective as one of the less restrictive components (antecedent intervention), and was equally effective to another of the less restrictive components (blocking). Research on the use of an antecedent intervention (other than NCR) in the treatment of automatically reinforced SIB may be a good area for future investigation. These interventions are less intrusive but appear highly effective; however, evaluations of antecedent components other than NCR are rare in the literature.
Our analysis of the types of assessments used to identify items for NCR and the subsequent effectiveness of NCR is similar to findings by Groskreutz, Groskreutz, and Higbee (2011). In this study, the authors prospectively examined the effectiveness of NCR as a treatment for one individual’s vocal stereotypy using items derived from either a preference assessment or CSA. The authors found that using the items identified from the CSA produced a more effective treatment. Although our study analyzed the effectiveness of NCR across individuals based on how items were identified in a retrospective manner, and Groskreutz et al. examined stereotypy in a prospective manner, the results are similar and suggest that CSAs should be used to identify items to use in NCR treatments. Interestingly, data from Figure 4 suggests that clinicians and researchers who published studies on the use of NCR for automatically reinforced SIB have already adopted the use of CSAs as the preferred means to identify items for NCR.
The method and results of the current analysis were most comparable to the method and finding in Kahng et al. (2002a), who reviewed published articles on behavioral treatments of SIB (maintained by any function) over a 35-year period. Our study overlapped with Kahng et al. (2002a) in that both included studies with automatically reinforced SIB between 1982–2000. Similar to the Kahng et al. study, we found the use of punishment had decreased over time (90% reduction in the past decade). In the place of punishment, we found that reinforcement alone had become more effective in the past decade (an 11% increase in effectiveness over the decade prior) and that there was a minor increase in the use of less restrictive additional components. The improvement of treatments using reinforcement alone may be related to the increased use of competition procedures to identify items for NCR over the same time period. However, in comparison to Kahng et al., across the entire 34-year period, we found that reinforcement was, on the whole, less effective. Kahng et al. found that the use of reinforcement alone produced a mean percent reduction in SIB of 73.2% across all years included their study. In the current study, reinforcement alone was less effective, producing only a 52.5% mean percent reduction in SIB. It is unlikely that reinforcement procedures have become less effective since the publication of Kahng et al., thus the difference is likely related to the fact that we only included automatically reinforced SIB in the review.
There are several potential reasons why SIB may be more resistant to reinforcement alone as a treatment in our review. First, evidence from the current study suggests that consequence-based reinforcement interventions (i.e., DRA and DRO) are much less effective for automatically reinforced SIB (effective in only 5 of 16 consequence-only-based interventions) than NCR (effective in 28 of 37 antecedent-only-based interventions). It may be that for consequence-based interventions to be effective, the individual must either engage in other behavior and/or refrain from engaging in SIB to obtain reinforcement. Thus, individuals who engage in a high rate of automatically reinforced SIB may never contact the consequence-based reinforcement contingency, due to response competition, decreasing the effectiveness of these interventions. Second, as discussed above, using an item from a preference assessment in NCR may make NCR more likely to fail in the treatment of automatically reinforced SIB, thus it is possible that our sample had more preference assessments than Kahng et al. (2002b). However, Kahng et al. likely had a similar distribution of preference assessments and CSAs (if not more preference assessments) used to identify items for NCR as the current study (given the time period in which the studies Kahng et al. reviewed were conducted) and still found reinforcement more effective. In addition, in our study, there were seven cases where a CSA was conducted and NCR was still found to be ineffective. Finally, there is evidence that some forms of automatically reinforced SIB are more resistant to treatment. For example, Hagopian et al. (2015) and Hagopian et al. (2017) demonstrated that subtypes of automatically reinforced SIB may respond differently to reinforcement alone as a treatment. Furthermore, a subset of the individuals in the current study was demonstrated to have subtype 2 SIB (see Hagopian et al., 2017). Unfortunately, in the current study, the majority of individuals could not be subtyped due to the lack of published FAs. However, it is likely that on average reinforcement alone was less effective in the current study because overall treatment effectiveness was reduced by the presence of subtypes of automatically reinforced SIB associated with treatment resistance.
Several weaknesses in this study should be noted. First, because this was a retrospective study of published research, the data are limited. For example, it is highly likely that the degree to which the individual interacts with items in NCR determines its effectiveness (through response competition); however, these data could not be obtained from the studies we reviewed. Second, the inclusion criteria were intentionally broad, and studies were included without a conclusive demonstration that SIB was maintained by automatic reinforcement (aside from the authors’ statement). Although this may introduce some doubt into the current findings, in the majority of cases the authors either presented an FA or noted that an FA was conducted. Third, although we evaluated the completeness of articles, the degree to which procedures were implemented in exactly the same way across studies was impossible to determine, as these publications often did not present integrity data. Despite this, in most cases, coders reported they could replicate the basic components of the treatment (e.g., how often reinforcement was programmed). Fourth, there was no uniform progression of treatments across studies. Thus, the degree to which a given treatment may or may not have been effective for an individual is unknowable and limits the type of analyses that can be conducted. Finally, not all treatments were implemented as part of clinical care. That is, some studies were not focused necessarily on the most effective treatment for automatically reinforced SIB through an application of the least to most intrusive treatments. Thus, more intrusive treatments may have been attempted with individuals who could have been successfully treated with less intrusive treatments (e.g., Lerman, Iwata, Shore, & DeLeon, 1997). Alternatively, unpublished clinical treatments may have been attempted prior to the published data we evaluated. In which case, information on the effectiveness or ineffectiveness of treatments may exist and have informed the experimenters prior to their study. Both of these possibilities may artificially inflate or deflate the degree to which additional treatment components were required to successfully treat automatically reinforced SIB.
Kahng et al. (2002a) indicated a decrease in the use of punishment in the treatment of SIB in published studies across time, suggesting that reinforcement alone as a treatment had become more effective for SIB. Results of the current study demonstrated this was true for automatically reinforced SIB, but to a lesser extent. Thus, future research should examine means to make reinforcement alone a more effective treatment for automatically reinforced SIB, and particularly for treatment-resistant automatically reinforced SIB (e.g., subtype 2). For the subset of individuals who engage in this treatment-resistant SIB, research on making alternative activities more attractive, training leisure skills, and making NCR more durable for extended use is needed. In addition, research might examine how additional components influence item interaction in assessment and treatment. Similarly, research is needed on the least intrusive and most effective forms of additional components to complement reinforcement treatments (e.g., response effort manipulations). Finally, further research is needed to examine individual, behavioral, and procedural reasons why reinforcement alone fails as a treatment. The current analysis identified NCR based on preference as one reason NCR might be ineffective; however, in the current study, this is only a subset of the ineffective reinforcement-alone treatments.
For the clinical treatment of automatically reinforced SIB, this review provides several distinct recommendations. Importantly, NCR is the most thoroughly studied treatment option and when using a reinforcement procedure alone, NCR has been used successfully most often. Further, the effectiveness of NCR can be improved by using items in the treatment that are determined to compete with SIB in a pretreatment assessment (i.e., CSA). However, NCR alone cannot be relied on to be effective in every case of automatically reinforced SIB. Thus, in some cases additional treatment components will be necessary. When this is the case, punishment has been used most often. However, our results suggest that a number of less intrusive procedures (e.g., antecedents other than NCR, blocking, and protective equipment) have been equally effective and may in fact produce a greater percent reduction in automatically reinforced SIB. Thus, the prudent course when faced with automatically reinforced SIB would be to first use empirical means to determine competing stimuli, evaluate those stimuli through NCR, and then add additional, less restrictive components, relying on punishment and restraint for only the most treatment-resistant cases.
Supplementary Material
Acknowledgments
Manuscript preparation was supported by Grant R01 HD076653 from the Eunice K. Shriver National Institute of Child Health and Human Development (NICHD). The contents are solely the responsibility of the authors and do not necessarily represent the official views of NICHD.
The authors wish to thank Louis P. Hagopian and Clare J. Liddon for their comments on earlier versions of this manuscript.
Footnotes
SUPPORTING INFORMATION
Additional Supporting Information may be found in the online version of this article at the publisher’s website.
Contributor Information
Griffin W. Rooker, JOHNS HOPKINS UNIVERSITY SCHOOL OF MEDICINE AND THE KENNEDY KRIEGER INSTITUTE
Andrew C. Bonner, UNIVERSITY OF FLORIDA
Christopher M. Dillon, THE KENNEDY KRIEGER INSTITUTE AND UNIVERSITY OF MARYLAND, BALTIMORE COUNTY
Jennifer R. Zarcone, JOHNS HOPKINS UNIVERSITY SCHOOL OF MEDICINE AND THE KENNEDY KRIEGER INSTITUTE
REFERENCES
Studies marked with an asterisk include data summarized in this review.
- Baghdadli A, Pascal C, Grisi S, & Aussilloux C (2003). Risk factors for self-injurious behaviours among 222 young children with autistic disorders. Journal of Intellectual Disability Research, 47, 622–627. 10.1046/j.1365-2788.2003.00507.x [DOI] [PubMed] [Google Scholar]
- *.Banda DR, McAfee JK, & Hart SL (2012). Decreasing self-injurious behavior and fading self-restraint in a student with autism and Tourette syndrome. Behavioral Interventions, 27, 164–174. 10.1002/bin.1344 [DOI] [Google Scholar]
- Beavers GA, Iwata BA, & Lerman DC (2013). Thirty years of research on the functional analysis of problem behavior. Journal of Applied Behavior Analysis, 46, 1–21. 10.1002/jaba.30 [DOI] [PubMed] [Google Scholar]
- Berg WK, Wacker DP, Ringdahl JE, Stricker J, Vinquist K, Salil Kumar Dutt A, … & Mews J (2016). An integrated model for guiding the selection of treatment components for problem behavior maintained by automatic reinforcement. Journal of Applied Behavior Analysis, 49, 617–638. 10.1002/jaba.303 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bodfish JW, Symons FJ, Parker DE, & Lewis MH (2000). Varieties of repetitive behavior in autism: Comparisons to mental retardation. Journal of Autism and Developmental Disorders, 30, 237–243. 10.1023/A:1005596502855 [DOI] [PubMed] [Google Scholar]
- Bowman-Perrott L, Burke MD, Zaini S, Zhang N, & Vannest K (2015). Promoting positive behavior using the good behavior game a meta-analysis of single-case research. Journal of Positive Behavior Interventions. 18, 180–190. 10.1177/1098300715592355 [DOI] [Google Scholar]
- *.Cavalari RN, DuBard M, & Luiselli JK (2013). Simplified habit reversal and treatment fading for chronic skin picking in an adolescent with autism. Clinical Case Studies, 13, 190–198 10.1177/1534650113510348 [DOI] [Google Scholar]
- Courtemanche A, Schroeder S, Sheldon J, Sherman J, & Fowler A (2012). Observing signs of pain in relation to self-injurious behaviour among individuals with intellectual and developmental disabilities. Journal of Intellectual Disability Research, 56, 501–515. Accessed at: https://onlinelibrary.wiley.com/doi/10.1111/j.1365-2788.2011.01492.x/full [DOI] [PubMed] [Google Scholar]
- *.Cowdery GE, Iwata BA, & Pace GM (1990). Effects and side effects of DRO as treatment for self-injurious behavior. Journal of Applied Behavior Analysis, 23, 497–506. 10.1901/jaba.1990.23-497 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Davis TN, Dacus S, Strickland E, Machalicek W, & Coviello L (2013). Reduction of automatically maintained self-injurious behavior utilizing noncontingent matched stimuli. Developmental Neurorehabilitation, 16, 166–171. 10.3109/17518423.2013.766819 [DOI] [PubMed] [Google Scholar]
- *.DeLeon IG, Anders BM, Rodriguez-Catter V, & Neidert PL (2000). The effects of noncontingent access to single- versus multiple-stimulus sets on self-injurious behavior. Journal of Applied Behavior Analysis, 33, 623–626. 10.1901/jaba.2000.33-623 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Demanche J, & Chok JT (2013). The use of wrist weights and vibratory stimulation to treat self-injurious behavior. Journal of Developmental and Physical Disabilities, 25, 79–90. 10.1007/s10882-012-9304-2 [DOI] [Google Scholar]
- Didden R, Korzilius H, & Curfs LM (2007). Skin-picking in individuals with Prader-Willi syndrome: Prevalence, functional assessment, and its comorbidity with compulsive and self-injurious behaviours. Journal of Applied Research in Intellectual Disabilities, 20, 409–419. 10.1111/j.1468-3148.2007.00388.x [DOI] [Google Scholar]
- *.Dozier CL, Vollmer TR, Borrero JC, Borrero CS, Rapp JT, Bourret J, & Gutierrez A (2007). Assessment of preference for behavioral treatment versus baseline conditions. Behavioral Interventions, 22, 245–261. 10.1002/bin.241 [DOI] [Google Scholar]
- Elsea SH, & Girirajan S (2008). Smith–Magenis syndrome. European Journal of Human Genetics, 16, 412–421. 10.1038/sj.ejhg.5202009 [DOI] [PubMed] [Google Scholar]
- *.Favell JE, McGimsey JF, & Schell RM (1982). Treatment of self-injury by providing alternate sensory activities. Analysis and Intervention in Developmental Disabilities, 2, 83–104. 10.1016/0270-4684(82)90007-6 [DOI] [Google Scholar]
- Fisher W, Piazza CC, Bowman LG, Hagopian LP, Owens JC, & Slevin I (1992). A comparison of two approaches for identifying reinforcers for persons with severe and profound disabilities. Journal of Applied Behavior Analysis, 25, 491–498. 10.1901/jaba.1992.25-491 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Groskreutz MP, Groskreutz NC, & Higbee TS (2011). Response competition and stimulus preference in the treatment of automatically reinforced behavior: A comparison. Journal of Applied Behavior Analysis, 44, 211–215. 10.1901/jaba.2011.44-211 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Hagopian LP, Paclawskyj TR, & Kuhn SC (2005). The use of conditional probability analysis to identify a response chain leading to the occurrence of eye poking. Research in Developmental Disabilities, 26, 393–397. 10.1016/j.ridd.2003.09.002 [DOI] [PubMed] [Google Scholar]
- Hagopian LP, Rooker GW, & Zarcone JR (2015). Delineating subtypes of self-injurious behavior maintained by automatic reinforcement. Journal of Applied Behavior Analysis, 48, 523–543. 10.1002/jaba.236 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hagopian LP, Rooker WG, Zarcone JR, Bonner AC, & Arevalo AR, (2017). Further analysis of subtypes of automatically reinforced SIB: A replication and quantitative analysis of published datasets. Journal of Applied Behavior Analysis, 50, 48–66. 10.1002/jaba.368 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hanley GP, Iwata BA, & McCord BE (2003). Functional analysis of problem behavior: A review. Journal of Applied Behavior Analysis, 36, 147–185. 10.1901/jaba.2003.36-147 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Hanley GP, Piazza CC, Keeney KM, Blakeley-Smith AB, & Worsdell AS (1998). Effects of wrist weights on self-injurious and adaptive behaviors. Journal of Applied Behavior Analysis, 31, 307–310. 10.1901/jaba.1998.31-307 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Healey JJ, Ahearn WH, Graff RB, & Libby ME (2001). Extended analysis and treatment of self-injurious behavior. Behavioral Interventions, 16, 181–195. 10.1002/bin.91 [DOI] [Google Scholar]
- *.Higgins WJ, Falcomata TS, Roane HS, & Thomas KM (2012). Effects of body positioning on automatically reinforced self-injurious behavior exhibited by a child with Duane syndrome and Goldenhar syndrome. Journal of Developmental and Physical Disabilities, 24, 135–144. 10.1007/s10882-011-9262-0 [DOI] [Google Scholar]
- Hustyi KM, Hammond JL, Rezvani AB, & Hall SS (2013). An analysis of the topography, severity, potential sources of reinforcement, and treatments utilized for skin picking in Prader–Willi syndrome. Research in Developmental Disabilities, 34, 2890–2899. 10.1016/j.ridd.2013.06.014 [DOI] [PubMed] [Google Scholar]
- Iwata BA, Dorsey MF, Slifer KJ, Bauman KE, & Richman GS (1994). Toward a functional analysis of self-injury. Journal of Applied Behavior Analysis, 27, 197–209. (Reprinted from Analysis and Intervention in Developmental Disabilities, 2, 3–20, 1982) 10.1901/jaba.1994.27-197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Iwata BA, Pace GM, Cowdery GE, & Miltenberger RG (1994). What makes extinction work: An analysis of procedural form and function. Journal of Applied Behavior Analysis, 27, 131–144. 10.1901/jaba.1994.27-131 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iwata BA, Pace GM, Dorsey MF, Zarcone JR, Vollmer TR, Smith RG, … Willis KD (1994). The functions of self-injurious behavior: An experimental-epidemiological analysis. Journal of Applied Behavior Analysis, 27, 215–240. 10.1901/jaba.1994.27-215 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Jennett H, Jann K, & Hagopian LP (2011). Evaluation of response blocking and re-presentation in a competing stimulus assessment. Journal of Applied Behavior Analysis, 44, 925–929. 10.1901/jaba.2011.44-925 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Kahng S, Abt KA, & Wilder DA (2001). Treatment of self-injury correlated with mechanical restraints. Behavioral Interventions, 16, 105–110. 10.1002/bin.86 [DOI] [Google Scholar]
- Kahng S, Iwata BA, & Lewin AB (2002a). Behavioral treatment of self-injury, 1964 to 2000. American Journal on Mental Retardation, 107, 212–221. [DOI] [PubMed] [Google Scholar]
- Kahng S, Iwata BA, & Lewin AB (2002b). The impact of functional assessment on the treatment of self-injurious behavior. In Schroeder S, Oster-Granite ML, & Thompson T (Eds.), Self-injurious behavior: Gene-brain-behavior relationships (pp. 119–131). Washington, DC: American Psychological Association. [Google Scholar]
- Kennedy CH (1994). Automatic reinforcement: Oxymoron or hypothetical construct? Journal of Behavioral Education, 4, 387–395. 10.1007/BF01539540 [DOI] [Google Scholar]
- *.Kennedy CH, & Souza G (1995). Functional analysis and treatment of eye poking. Journal of Applied Behavior Analysis, 28, 27–37. 10.1901/jaba.1995.28-27 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kennedy CH, & Thompson T (2000). Health conditions contributing to problem behavior among people with mental retardation and developmental disabilities. In Wehmeyer M & Patten J (Eds.), Mental retardation in the 21st century (pp. 211–231). Austin, TX: Pro-Ed. [Google Scholar]
- *.Kern L, Bailin D, & Mauk JE (2003). Effects of a topical anesthetic on non-socially maintained self-injurious behavior. Developmental Medicine & Child Neurology, 45, 769–771. 10.1017/S0012162203001427 [DOI] [PubMed] [Google Scholar]
- *.Kuhn DE, DeLeon IG, Fisher WW, & Wilke AE (1999). Clarifying an ambiguous functional analysis with matched and mismatched extinction procedures. Journal of Applied Behavior Analysis, 32, 99–102. 10.1901/jaba.1999.32-99 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Ladd MV, Luiselli JK, & Baker L (2009). Continuous access to competing stimulation as intervention for self-injurious skin picking in a child with autism. Child & Family Behavior Therapy, 31, 54–60. 10.1080/07317100802701400 [DOI] [Google Scholar]
- *.Lane KL, Thompson A, Reske CL, Gable LM, & Barton-Arwood S (2006). Reducing skin picking via competing activities. Journal of Applied Behavior Analysis, 39, 459–462. 10.1901/jaba.2006.62-05 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Lang R, Didden R, Sigafoos J, Rispoli M, Regester A, & Lancioni GE (2009). Treatment of chronic skin-picking in an adolescent with Asperger syndrome and borderline intellectual disability. Clinical Case Studies, 8, 317–325. 10.1177/1534650109341841 [DOI] [Google Scholar]
- Lanovaz MJ, & Sladeczek IE (2012). Vocal stereotypy in individuals with autism spectrum disorders a review of behavioral interventions. Behavior Modification, 36, 146–164. 10.1177/0145445511427192 [DOI] [PubMed] [Google Scholar]
- LeBlanc LA, Patel MR, & Carr JE (2000). Recent advances in the assessment of aberrant behavior maintained by automatic reinforcement in individuals with developmental disabilities. Journal of Behavior Therapy and Experimental Psychiatry, 31, 137–154. 10.1016/S0005-7916(00)00017-3 [DOI] [PubMed] [Google Scholar]
- Lee JH, Berkowitz RJ, & Choi BJ (2002). Oral self-mutilation in the Lesch-Nyhan syndrome. Journal of Dentistry for Children, 69, 66–69. Accessed at: https://www.ingentaconnect.com/content/aapd/jodc/2002/00000069/00000001/art00014#expand/collapse [PubMed] [Google Scholar]
- *.Lerman DC, Iwata BA, Shore BA, & DeLeon IG (1997). Effects of intermittent punishment on self-injurious behavior: An evaluation of schedule thinning. Journal of Applied Behavior Analysis, 30, 187–201. 10.1901/jaba.1997.30-187 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levy A, DeLeon IG, Martinez CK, Fernandez N, Gage NA, Sigurdsson SO, & Frank-Crawford M (2017). A quantitative review of over-justification effects in persons with intellectual and developmental disabilities. Journal of Applied Behavior Analysis. 50, 206–221. 10.1002/jaba.359 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Lindberg JS, Iwata BA, & Kahng S (1999). On the relation between object manipulation and stereotypic self-injurious behavior. Journal of Applied Behavior Analysis, 32, 51–62. 10.1901/jaba.1999.32-51 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Lindberg JS, Iwata BA, Roscoe EM, Worsdell AS, & Hanley GP (2003). Treatment efficacy of noncontingent reinforcement during brief and extended application. Journal of Applied Behavior Analysis, 36, 1–19. 10.1901/jaba.2003.36-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Linscheid TR, Iwata BA, Ricketts RW, Williams DE, & Griffin JC (1990). Clinical evaluation of the self-injurious behavior inhibiting system (SIBIS). Journal of Applied Behavior Analysis, 23, 53–78. 10.1901/jaba.1990.23-53 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Long ES, Hagopian LP, DeLeon IG, Marhefka JM, & Resau D (2005). Competing stimuli in the treatment of multiply controlled problem behavior during hygiene routines. Research in Developmental Disabilities, 26, 57–69. 10.1016/j.ridd.2003.01.001 [DOI] [PubMed] [Google Scholar]
- Ma G, Wang Q, Lv C, Qiang F, Hua Q, Chu H, … & Gong W (2015). The prognostic significance of HOTAIR for predicting clinical outcome in patients with digestive system tumors. Journal of cancer research and clinical oncology, 141, 2139–2145. 10.1007/s00432-015-1980-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Magnusson AF, & Gould DD (2007). Reduction of automatically-maintained self-injury using contingent equipment removal. Behavioral Interventions, 22, 57–68. 10.1002/bin.231 [DOI] [Google Scholar]
- *.Mason SA, & Iwata BA (1990). Artifactual effects of sensory-integrative therapy on self-injurious behavior. Journal of Applied Behavior Analysis, 23, 361. 10.1901/jaba.1990.23-361 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Matson JL, & LoVullo SV (2008). A review of behavioral treatments for self-injurious behaviors of persons with autism spectrum disorders. Behavior Modification, 32, 61–76. 10.1177/0145445507304581 [DOI] [PubMed] [Google Scholar]
- Morrison H, Roscoe EM, & Atwell A (2011). An evaluation of antecedent exercise on behavior maintained by automatic reinforcement using a three-component multiple schedule. Journal of Applied Behavior Analysis, 44, 523–541. 10.1901/jaba.2011.44-523 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nyhan WL (1976). Behavior in the Lesch-Nyhan syndrome. Journal of Autism and Childhood Schizophrenia, 6, 235–252. 10.1007/BF01543464 [DOI] [PubMed] [Google Scholar]
- *.O’Reilly MF (1996). Assessment and treatment of episodic self-injury: A case study. Research in Developmental Disabilities, 17, 349–361. 10.1016/0891-4222(96)00018-2 [DOI] [PubMed] [Google Scholar]
- *.O’Reilly MF, Murray N, Lancioni GE, Sigafoos J, & Lacey C (2003). Functional analysis and intervention to reduce self-injurious and agitated behavior when removing protective equipment for brief time periods. Behavior Modification, 27, 538–559. 10.1177/0145445503255573 [DOI] [PubMed] [Google Scholar]
- Pace GM, Ivancic MT, Edwards GL, Iwata BA, & Page TJ (1985). Assessment of stimulus preference and reinforcer value with profoundly retarded individuals. Journal of Applied Behavior Analysis, 18, 249–255. 10.1901/jaba.1985.18-249 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Patel MR, Carr JE, Kim C, Robles A, & Eastridge D (2000). Functional analysis of aberrant behavior maintained by automatic reinforcement: Assessments of specific sensory reinforcers. Research in Developmental Disabilities, 21, 393–407. 10.1016/S0891-4222(00)00051-2 [DOI] [PubMed] [Google Scholar]
- Phillips CL, Iannaccone JA, Rooker GW, & Hagopian LP (2017). Noncontingent reinforcement for the treatment of severe problem behavior: An analysis of 27 consecutive applications. Journal of Applied Behavior Analysis, 2, 357–376. 10.1002/jaba.376 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piazza CC, Bowman LG, Contrucci SA, Delia MD, Adelinis JD, & Goh HL (1999). An evaluation of the properties of attention as reinforcement for destructive and appropriate behavior. Journal of Applied Behavior Analysis, 32, 437–449. 10.1901/jaba.1999.32-437 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Piazza CC, Fisher WW, Hanley GP, Hilker K, & Derby KM (1996). A preliminary procedure for predicting the positive and negative effects of reinforcement-based procedures. Journal of Applied Behavior Analysis, 29, 137–152. 10.1901/jaba.1996.29-137 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Poisson A, Nicolas A, Cochat P, Sanlaville D, Rigard C, de Leersnyder H, … & Demily C (2015). Behavioral disturbance and treatment strategies in Smith-Magenis syndrome. Orphanet Journal of Rare Diseases, 10, 111. 10.1186/s13023-015-0330-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prieto MA, Vázquez JA, & Murado MA (2014). A new mathematical model to quantify and characterize the response to pro-and anti-oxidants of the copper-induced oxidation of LDL assay. A tool for examination of potential preventive compounds and clinical risk prediction. Food Research International, 66, 501–513. 10.1016/j.foodres.2014.07.046 [DOI] [Google Scholar]
- Rapp JT, & Vollmer TR (2005). Stereotypy I: A review of behavioral assessment and treatment. Research in Developmental Disabilities, 26, 527–547. 10.1016/j.ridd.2004.11.005 [DOI] [PubMed] [Google Scholar]
- Richman DM, & Lindauer SE (2005). Longitudinal assessment of stereotypic, proto-injurious, and self-injurious behavior exhibited by young children with developmental delays. American Journal on Mental Retardation, 110, 439–450. 10.1352/0895-8017(2005)110[439:LAOSPA]2.0.CO;2 [DOI] [PubMed] [Google Scholar]
- *.Richman DM, Wacker DP, Asmus JM, & Casey SD (1998). Functional analysis and extinction of different behavior problems exhibited by the same individual. Journal of Applied Behavior Analysis, 31, 475–478. 10.1901/jaba.1998.31-475 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Ringdahl JE, Vollmer TR, Marcus BA, & Roane HS (1997). An analogue evaluation of environmental enrichment: The role of stimulus preference. Journal of Applied Behavior Analysis, 30, 203–216. 10.1901/jaba.1997.30-203 [DOI] [Google Scholar]
- *.Rosales R, Worsdell A, & Trahan M (2010). Comparison of methods for varying item presentation during noncontingent reinforcement. Research in Autism Spectrum Disorders, 4, 367–376. 10.1016/j.rasd.2009.10.004 [DOI] [Google Scholar]
- *.Roscoe EM, Iwata BA, & Goh HL (1998). A comparison of noncontingent reinforcement and sensory extinction as treatments for self-injurious behavior. Journal of Applied Behavior Analysis, 31, 635–646. 10.1901/jaba.1998.31-635 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roscoe EM, Iwata BA, & Zhou L (2013). Assessment and treatment of chronic hand mouthing. Journal of Applied Behavior Analysis, 46, 181–198. 10.1002/jaba.14 [DOI] [PubMed] [Google Scholar]
- Sham E, & Smith T (2014). Publication bias in studies of an applied behavior-analytic intervention: An initial analysis. Journal of Applied Behavior Analysis, 47, 663–678. 10.1002/jaba.146 [DOI] [PubMed] [Google Scholar]
- *.Shore BA, Iwata BA, DeLeon IG, Kahng S, & Smith RG (1997). An analysis of reinforcer substitutability using object manipulation and self-injury as competing responses. Journal of Applied Behavior Analysis, 30, 21–41. 10.1901/jaba.1997.30-21 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Slifer KJ, Iwata BA, & Dorsey MF (1984). Reduction of eye gouging using a response interruption procedure. Journal of Behavior Therapy and Experimental Psychiatry, 15, 369–375. 10.1016/0005-7916(84)90104-6 [DOI] [PubMed] [Google Scholar]
- *.Smith RG, Iwata BA, Vollmer TR, & Zarcone JR (1993). Experimental analysis and treatment of multiply controlled self-injury. Journal of Applied Behavior Analysis, 26, 183–196. 10.1901/jaba.1993.26-183 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Soke GN, Rosenberg SA, Hamman RF, Fingerlin T, Robinson C, Carpenter L, … & DiGuiseppi C (2016). Brief report: Prevalence of self-injurious behaviors among children with Autism Spectrum Disorder—A population-based study. Journal of Autism and Developmental Disorders, 46, 3607–3614. 10.1007/s10803-016-2879-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Stokes JV, & Luiselli JK (2008). Applied behavior analysis assessment and intervention for health: Threatening self-injury (rectal picking) in an adult with Prader-Willi syndrome. Clinical Case Studies, 8, 38–47. 10.1177/1534650108327011 [DOI] [Google Scholar]
- Symons FJ, Butler MG, Sanders MD, Feurer ID, & Thompson T (1999). Self-injurious behavior and Prader-Willi syndrome: behavioral forms and body locations. American Journal on Mental Retardation, 104, 260–269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Symons FJ, Byiers BJ, Raspa M, Bishop E, & Bailey DB (2010). Self-injurious behavior and fragile X syndrome: Findings from the national fragile X survey. American Journal of Intellectual and Developmental Disabilities, 115, 473–481. 10.1352/1944-7558-115.6.473 [DOI] [PubMed] [Google Scholar]
- Tate BG, & Baroff GS (1966). Aversive control of self-injurious behavior in a psychotic boy. Behaviour Research and Therapy, 4, 281–287. 10.1016/0005-7967(66)90024-6 [DOI] [PubMed] [Google Scholar]
- *.Thompson RH, Iwata BA, Conners J, & Roscoe EM (1999). Effects of reinforcement for alternative behavior during punishment of self-injury. Journal of Applied Behavior Analysis, 32, 317–328. 10.1901/jaba.1999.32-317 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thompson T, & Caruso M (2002). Self-injury: Knowing what we’re looking for. In Schroeder SR, Oster-Granite ML, & Thompson T (Eds.), Self-injurious Behavior: Gene-brain-behavior relationships (pp. 3–21). Washington, DC: American Psychological Association. [Google Scholar]
- Thompson T, Symons F, Delaney D, & England C (1995). Self-injurious behavior as endogenous neurochemical self-administration. Developmental Disabilities Research Reviews, 1, 137–148. Accessed at: https://onlinelibrary.wiley.com/doi/10.1002/mrdd.1410010210/full [Google Scholar]
- *.Tiger JH, Fisher WW, & Bouxsein KJ (2009). Therapist- and self-monitored DRO contingencies as a treatment for the self-injurious skin picking of a young man with Asperger syndrome. Journal of Applied Behavior Analysis, 42, 315–319. 10.1901/jaba.2009.42-315 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Toole LM, DeLeon IG, Kahng S, Ruffin GE, Pletcher CA, & Bowman LG (2004). Reevaluation of constant versus varied punishers using empirically derived consequences. Research in Developmental Disabilities, 25, 577–586. 10.1016/j.ridd.2004.03.005 [DOI] [PubMed] [Google Scholar]
- *.Van Camp CM, Lerman DC, Kelley ME, Roane HS, Contrucci SA, & Vorndran CM (2000). Further analysis of idiosyncratic antecedent influences during the assessment and treatment of problem behavior. Journal of Applied Behavior Analysis, 33, 207–221. 10.1901/jaba.2000.33-207 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Van Camp CM, Vollmer TR, & Daniel D (2001). A systematic evaluation of stimulus preference, response effort, and stimulus control in the treatment of automatically reinforced self-injury. Behavior Therapy, 32, 603–613. 10.1016/S0005-7894(01)80037-X [DOI] [Google Scholar]
- *.Van Houten R (1993). The use of wrist weights to reduce self-injury maintained by sensory reinforcement. Journal of Applied Behavior Analysis, 26, 197–203. 10.1901/jaba.1993.26-197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vaughan ME, & Michael JL (1982). Automatic reinforcement: An important but ignored concept. Behaviorism, 10, 217–227. Accessed at: http://www.jstor.org/tc/accept?origin=/stable/pdf/27759007.pdf [Google Scholar]
- Vollmer TR (1994). The concept of automatic reinforcement: Implications for behavioral research in developmental disabilities. Research in Developmental Disabilities, 15, 187–207. 10.1016/0891-4222(94)90011-6 [DOI] [PubMed] [Google Scholar]
- *.Vollmer TR, Marcus BA, & LeBlanc L (1994). Treatment of self-injury and hand mouthing following inconclusive functional analyses. Journal of Applied Behavior Analysis, 27, 331–344. 10.1901/jaba.1994.27-331 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Wesolowski MD, & Zawlocki RJ (1982). The differential effects of procedures to eliminate an injurious self-stimulatory behavior (digito-ocular sign) in blind retarded twins. Behavior Therapy, 13, 334–345. 10.1016/S0005-7894(82)80042-7 [DOI] [Google Scholar]
- Zhou Q, Chen A, Song H, Tao J, Yang H, & Zuo M (2015). Prognostic value of cancer stem cell marker CD133 in ovarian cancer: a meta-analysis. International Journal of Clinical & Experimental Medicine, 8, 3080–3088. Accessed at: http://pubmedcentralcanada.ca/pmcc/articles/PMC4443030/ [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.