

Abstract
Recent studies argue that major crises can have long‐lasting effects on individual behavior. While most studies focused on natural disasters, we explore the consequences of the global pandemic caused by a lethal influenza virus in 1918–19: the so‐called “Spanish Flu.” This was by far the worst pandemic of modern history, causing up to 100 million deaths worldwide. Using information about attitudes of respondents to the General Social Survey, we find evidence that experiencing the pandemic likely had permanent consequences in terms of individuals' social trust. Our findings suggest that lower social trust was passed on to the descendants of the survivors of the Spanish Flu who migrated to the United States. As trust is a crucial factor for long‐term economic development, our research offers a new angle from which to assess current health threats.
Keywords: epidemic, generalized trust, mortality crisis, pandemic, Spanish flu
1. INTRODUCTION
A century ago, an influenza‐A virus caused the greatest pandemic in human history, the “Spanish Flu.” It infected about a third of the world population and caused an estimated 50–100 million victims (Johnson & Mueller, 2002; Taubenberger & Morens, 2006). The long‐term effects of the Spanish Flu went well beyond the immediate demographic losses that it caused. Much research has been conducted into its consequences for the health of survivors, even when experienced in‐utero (Almond, 2006; Bengtsson & Helgertz, 2015; Myrskylä, Mehta, & Chang, 2013). Fewer studies exist on the way in which experiencing the Spanish Flu‐shaped individual behavior and human societies at large (Almond, 2006; Bengtsson & Helgertz, 2015; Carillo & Jappelli, 2020; Cohn, 2018; Galletta & Giommoni, 2020; Guimbeau, Menon, & Musacchio, 2019; Karlsson, Nilsson, & Pichler, 2014; Lin & Liu, 2014). Yet a growing literature argues that the second‐worst pandemic in human history, the Black Death, had long‐term economic, social and cultural consequences, shaping behavior well into the 20th century (Alfani, 2020; Alfani & Murphy, 2017; Jedwab, Johnson, & Koyama, 2016; Richardson & McBride, 2009; Voitgländer & Voth, 2012). Here we show that similarly to the Black Death, also the Spanish Flu had long‐lasting social consequences, leading to a decline in social trust. This would result from having experienced the social disruption and generalized mistrust characterizing the pandemic period.
Uncovering the broader societal impact of an historical pandemic, such as the Spanish flu, is obviously challenging. In the case of attitudes and social trust, which we study here, no direct survey measures exist. Instead we exploit information about the descendants of those who experienced the historical event (Algan & Cahuc, 2010). This method leverages on the fact that cultural traits and attitudes are inherited across generations, passing on from parents to children (Dohmen, Falk, Huffman, & Sunde, 2012). We use the General Social Survey (GSS), which is a representative survey of the US population. Social trust is derived from those respondents who were direct descendants of migrants to the United States, and by using this information, we are able to provide an estimate of social trust for each country of origin before and after the spread of the Spanish Flu. Importantly, the derived measure of trust from the GSS is exogenous to socioeconomic differences between countries at that time. For each country of origin, we compare the estimated levels of social trust for the two periods, and we analyze how the possible difference in trust depends on the pandemic mortality rate by adopting a difference‐in‐difference (DiD) approach.
The results of our analysis suggest a negative and significant effect of the Spanish Flu on trust. An increase in influenza mortality of one death per thousand resulted in a 1.4 percentage points decrease in trust. This result is robust to an extensive set of tests, including a falsification test, different samples and variable definitions, different functional specifications and different control strategies. We also provide evidence on the possible mechanism underlying the change in trust, namely the neutrality of the home country in world war I (WWI). A narrower resonance of the war within neutral countries, together with the specific lack of war censorship on media, might have led their respective citizens to internalize the extent and severity of the pandemic, and thus altered their social interactions accordingly. 1 Consistently with this hypothesis, we do find a stronger reduction in social trust for the descendants of people migrating from countries heavily hit by the epidemic and that remained neutral during the war.
Trust is an important determinant of long‐run economic development (Tabellini, 2010), and recent literature has shown its reactivity to natural disasters such as earthquakes or floods (Carlin, Love, & Zechmeister, 2014; Skidmore & Toya, 2014). By bringing attention to major epidemics, our study also provides useful insights into how more recent events, such as the HIV pandemic or the recent Ebola epidemic of 2013–2016 as well as the one which started in 2018 and is currently ongoing, might have lasting consequences on the societies affected (Hayden, 2014; Young, 2005), possibly compromising their economic performances for years to come. However, we also argue that the effects of a specific pandemic or epidemic cannot be easily generalized, as they depend on its characteristics both in terms of infection rates and chances of survival, as well as on the cultural and social‐economic context in which it took place. This conclusion is in line with the recent literature on the consequences of large‐scale plagues in European history (Alfani & Percoco, 2019). Finally, the fact that the impact of the Spanish Flu on trust in neutral countries is different from belligerent ones, illustrates how the portrayal of a pandemic by the media plays an important role in affecting societies. The possible lesson from history is that, during large‐scale pandemic crises, including the current one caused by COVID‐19, availability of open, accurate and reliable information might contribute to contain persistent damage to social capital. This, however, remains an hypothesis that it would be unfeasible to formally test in this study.
In the next section, we provide an overview of the Spanish Flu and its main impact on society. Section 2 describes the data employed in the analysis while Section 3 the methodology applied to carry it out. In Section 4, we report our main findings as well as an extended set of robustness tests. Finally, Section 5 concludes, and highlights the relevance of our findings for the current crisis caused by COVID‐19.
2. THE INFLUENZA PANDEMIC AND ITS IMPACT ON SOCIETY
The first wave of the Spanish Flu pandemic started in spring 1918 and spread rapidly across the world. Earlier scholarship placed its origin in the United Stated, where the influenza was first identified in March 1918, however this is now doubted (Crosby, 1976; Taubenberger & Morens, 2006). The pandemic was caused by an influenza H1N1 virus, whose entire genome has been sequenced (Taubenberger et al., 2005; Tumpey et al., 2005). All influenza, A pandemics since 1918, have been caused by descendants of the Spanish Flu virus (Taubenberger & Morens, 2006) and vaccines developed to protect against the 2009 H1N1 virus would also work against the original Spanish Influenza virus (Medina et al., 2010). While this offers some reassurance about the health threats associated to H1N1, it is also one of the two factors explaining why the Spanish Flu continues to be the object of considerable interdisciplinary attention. The other is its exceptional severity, especially during the second wave (September–November 1918) and the third (early 1919). The third wave, which involved fewer countries, was probably exacerbated by the end of WWI, with soldiers returning home and the resuming of commerce (Crosby, 1976; Taubenberger & Morens, 2006). However, looking at the average mortality rates associated with the influenza pandemic showed in Figure 1, there is no considerable differences across neutral and belligerent countries.
FIGURE 1.
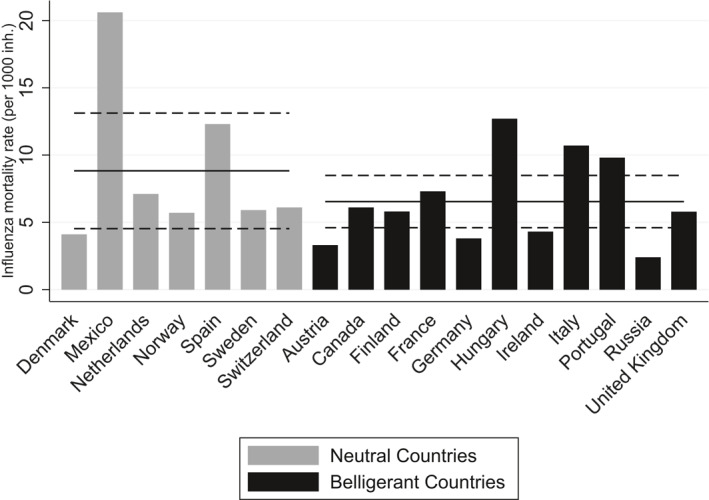
Spanish Flu mortality by participation to World War I. The figure shows the influenza mortality rates for the sample countries employed in the analysis, divided by their participation in World War I. Horizontal lines represent the mean death rate for each group while the dashed horizontal lines show the 95% confidence intervals
The exceptionally high mortality is the combined result of the extremely high infectiousness of the disease and of a case‐fatality rate of >2.5%, which is high compared to the <0.1% characterizing other influenza pandemics (Taubenberger & Morens, 2006). Overall, this resulted in at least 50, and possibly as much as 100 million victims globally (Johnson & Mueller, 2002; Taubenberger & Morens, 2006). These grim statistics place the Spanish Flu at the top of the ranking of the worst pandemics in human history, at least looking at the number of deaths (Alfani & Murphy, 2017). Another striking characteristic of the Spanish Flu was that most of its victims were young adults. This is different from the standard influenza outbreaks that tend to affect the very young and older strata of the population, thereby leading to the well‐known U‐shaped relationship between age and flu mortality. The Spanish flu in contrast, killed disproportionately young adults aged 15–34. The resulting relationship between age and deaths is W‐shaped (Mamelund, 2011), and very similar across genders, as shown in Figure 2.
FIGURE 2.

Age‐Specific excess mortality rates. The figure shows the median excess mortality rates by sex and age group, based on data for 13 countries, namely Australia, Denmark, England, Finland, France, Italy, Netherlands, New Zealand, Norway, Spain, Sweden, Switzerland, and the United States America (Source: Murray, Lopez, Chin, Feehan, & Hill, 2006)
Explaining differences in trust has attracted considerable interest. This is in part driven by the fact that social trust matters for a whole range of societal outcomes—including economic prosperity. Additionally, this interest comes from the observation that social trust appears rather stable over time, though with significant differences across countries. Consequently, it is important to identify the cultural roots of social trust. Some have focused on climate variation, arguing that in agricultural societies, unfavorable weather conditions may have encouraged cooperation, and therefore created differences in trust over time (Buggle & Durante, 2017). Others have emphasized historical developments (Guiso, Sapienza, & Zingales, 2016), such as the slave trade and colonial medicine in Africa (Lowes & Montero, 2018; Nunn & Wantchekon, 2011), the establishment of Leaper colonies in Colombia (Ramos‐Toro, 2019), or mass‐surveillance in East‐Germany (Lichter, Loeffler, & Siegloch, 2015), that might have generated long‐standing distrust in those societies exposed to them. Another strand of literature has focused on the potential role of natural disasters in affecting social trust (Calo‐Blanco, Kovářík, Mengel, & Romero, 2017; Carlin et al., 2014; Uslaner & yamamura, 2016), a literature related to our current study.
This literature does not make clear‐cut predictions for how a natural disaster may alter social trust. On the one hand, a natural disaster could increase trust as citizens get together through rebuilding efforts. But in so far as a natural disaster brings about economic destitution and poverty, individuals may be forced to fend for themselves rather than engaging in healthy cooperation, which may in turn lower social trust.
A similar issue applies for pandemics. It seems natural to hypothesize that a highly contagious disease would reduce social contacts from fear of contracting the disease. People would naturally avoid social interaction with those they do not know and perhaps avoid large gatherings, and over time, the social trust will decline. For the Spanish Flu, measures of public health, and the general encouragement from the authorities and the media to avoid inter‐personal contacts, created a profound climate of suspicion and mistrust (Cohn, 2018). However, social distancing alone would probably have had limited consequences. It was high mortality and the concentration of deaths among young adults that increased the ability of the pandemic to disrupt the social tissue. Indeed, historical accounts of the Spanish Flu show that panic was so widespread that the red cross in rural Kentucky reported “people starving to death not from lack of food but because the [healthy] were panic stricken and would not go near the sick” (Barry, 2005). Different locations attempted to combat the pandemic with a variety of methods. Quarantines, closing schools, bars, churches and other gathering places and compulsory gauze masks were implemented, though most of these actions turned ineffective in containing the disease (Crosby, 1976; Johnson, 2012). In other words, the fear of contracting a lethal influenza dramatically altered social interactions (Phillps & Killingray, 2003). Some scientists worried that “If the epidemic continues its mathematical rate of acceleration, civilization could easily disappear from the face of the earth within a matter of a few more weeks” (Collier, 1974). However, comparatively speaking, the Spanish Flu was not merely as lethal as other epidemics, such as the Ebola. An important aspect of the Spanish Flu was instead its sheer magnitude. The world struggled to cope as vaccines were not developed and none of the suggested cures were effective (Crosby, 1976; Taubenberger & Morens, 2006). Across Europe and the United States, civilian hospitals were severely understaffed, in part because doctors and nurses were involved in the war efforts, but also because of the very large number of people contracting the disease. The case of the Spanish Flu is consequently a textbook case of utter failure of health care institutions both in containing the spread of an epidemic and in providing effective care. Observing the failure of institutions and society to cope with the crisis (a failure whose most visible result was the widespread mortality) is what, we believe, led to significant and persistent consequences on individual's social trust—a point which, as discussed in the conclusion, might have some relevance for the current crisis caused by COVID‐19.
Other pandemics may have different impact. The case‐fatality rate from contracting Ebola is way higher than the Spanish Flu, for instance. But its extent, in terms of infections rates and overall mortality, has been dramatically lower so far, and the areas where one may contract Ebola are typically very small. Individuals will know instantly about an outbreak as they observe fellow villagers dying from the disease. But given the (relatively) small scale, it is not at all sure that an Ebola epidemic would have a big impact on social trust. In fact, a recent study found evidence that effective public intervention to contain Ebola outbreaks might have actually increased trust in government authorities (Flückiger, Ludwig, & SinaÖnder, 2019). The same study, however, did not find a strong effect on social trust. In contrast to the Ebola outbreaks, the number of people who were infected by the Spanish Flu—but survived—was orders of magnitude greater and those survivors (and their relations) might have experienced the deepest changes in their attitudes. Indeed, the survivors were those who had been faced more directly with the collapse of traditional networks of social support as well as with the inability of public institutions to provide adequate care and relief.
3. DATA: INHERITED TRUST AND SPANISH FLU MORTALITY
The data employed in this work are mostly obtained from the GSS. The GSS is a repeated cross‐sectional survey held in the United States and nationally representative of the US population of adults (18 + ) speaking either English or Spanish. 2 The questionnaire is provided face‐to‐face with an in‐person interview by National Opinion Research Center at the University of Chicago, and the response rate is generally above 70%. The survey was conducted every year from 1972 to 1994 (except in 1979, 1981, and 1992). Since 1994, it has been conducted each two years. It contains a standard core of demographic, behavioral, and attitudinal questions that are repeated in each wave of the survey. This gives access to a vast pool of respondents providing the information required for our analysis. In particular, we use the waves from 1978 to 2018.
The main variable of interest that can be obtained from the GSS is generalized trust. This variable comes from the question “Generally speaking, would you say that most people can be trusted or that you can't be too careful in dealing with people?“. First formulated by Almond and Verba (1963), the question is extensively used in the literature to measure generalized trust on the basis of surveys (Algan & Cahuc, 2014). We code generalized trust as a dummy variable that takes value 1 (high trust) for the people that answered “Can Trust” and 0 (low trust) for those who answered either “Cannot Trust” or “Depends”. 3
Survey respondents were also asked about their country of ethnic origin and a series of questions regarding their migration history: whether they were born in the United States or not, whether their mother and father were born in the United States and the number of grandparents born outside the country. Using this information, we group respondents on the basis of their country of ethnic origin and categorize them in three waves of immigration: second‐generation Americans (i.e., people born in the United States with at least one parent and all the grandparents born abroad), third‐generation Americans (i.e., people with at least two immigrant grandparents and both parents born in the United States) and fourth‐generation Americans (i.e., people with more than two grandparents born in the United States and both parents born in the United States). We exploit different waves of immigration to measure the inter‐generational path of social capital transmission by people migrated before and after the spread of the Spanish flu (i.e., 1918), following the methodology introduced by Algan and Cahuc (2010) and Tabellini (2008).
We measure the severity of the Spanish flu using the data on flu mortality, expressed in deaths per thousand inhabitants, collected by Johnson and Mueller (2002). This is the most comprehensive published study in terms of countries coverage, and it presents estimates for flu mortality, pooling together the results of multiple studies on single countries. Specifically, the countries for which the estimates of Spanish flu death rates are available that are included in our analysis are Austria, Canada, Denmark, Finland, France, Germany, Hungary, Ireland, Italy, Mexico, the Netherlands, Norway, Portugal, Russia, Spain, Sweden, Switzerland, and the United Kingdom. 4 Note that we focus on mortality and not on other epidemiological variables, like morbidity, as a measure of the severity of the Spanish Flu for two reasons: first, because estimates of mortality rates are available for more countries and are of better quality compared to morbidity rates, and secondly, because for the general population it was experiencing a sharp increase in the number of deaths and the failure of institutions to prevent it that can reasonably be expected to have had the stronger consequences on psychology and behavior.
4. METHODOLOGY
4.1. Estimation of inherited trust in the home countries
In order to obtain estimates for the level of trust in each country before and after the spread of the Spanish flu, we follow the method proposed by Algan and Cahuc (2010) and Tabellini (2008). Algan and Cahuc (2010) leverage on the evolution of trust of descendants of the US migrants to detect historical changes in the level of trust in the home country. The starting point is that a part of social attitudes, including trust, is shaped by the contemporary environment and society while another is due to beliefs and norms inherited from earlier generations (Dohmen et al., 2012). By estimating the latter part using the GSS survey, they obtain a proxy for the level of generalized trust that was present in the countries of origin at the time of the ancestors' migration to the United States. Since the date of departure of the respondents' ancestors is not directly available from the survey, the authors infer it from the year of birth of the person interviewed and whether he is second‐, third‐ or fourth‐generation American. Assuming a 25‐year gap between generations, Algan and Cahuc (2010) hypothesize that the respondent's ancestor moved to the United States before the date Y if (I) the respondent is a second‐generation American born before Y or (II) the respondent is a third‐generation American born before Y+25 or (III)the respondent is a fourth‐generation American born before Y+50. Algan and Cahuc (2010) also assume that the respondent's ancestor moved to the United States after the date Y if (I) the respondent is a second‐generation American born after Y or (II) the respondent is a third‐generation American born after Y+25 or (III) the respondent is a fourth‐generation American born after Y+50. Having created these two groups, for each of them Algan and Cahuc (2010) regress the individual levels of trust on a set of variables, including dummies for each country of origin. Thus, the levels of trust for a specific country of origin before and after date Y are captured by the coefficients of the fixed effect for that country in each of the two regressions.
This approach provides two main advantages in the estimation of country‐level trust. First and foremost, it allows us to calculate inherited trust starting from a measure of present trust that is exogenous to socioeconomic differences between countries at the time of the pandemic. Furthermore, we can rely on a single survey and on questions that are consistent across the waves, granting the comparability of the variables both between countries and between periods.
As in Algan and Cahuc (2010) we run two separate regressions: one to estimate trust up to 1918 and the other to estimate trust after 1918. Furthermore, as in Algan and Cahuc (2010), we assume a 25‐year gap between generations. Specifically, in the sample used to estimate inherited trust before 1918 we include (I) all the second‐generation respondents that were born in 1918 or earlier (II) all the third‐generation respondents that were born by 1918 + 25 (i.e., 1943), and (III) all the fourth‐generation Americans that were born by 1918 + 50 (i.e., 1968). As for trust after 1918, we sample (I) all the second‐generation respondents that were born after 1918, (II) the third‐generation respondents born after 1918 + 25 (i.e., 1943), and (III) all the fourth‐generation Americans born after 1918 + 50 (i.e., 1968).
Differently from Algan and Cahuc (2010), we are interested in the variation of inherited trust around a precise date, 1918, and this requires higher accuracy in the identification of the respondents whose ancestors migrated before or after such date. Taking for example second‐generation Americans, since we infer the date of migration of their parents from their year of birth, including in the post‐1918 sample also people born immediately after such date (i.e., 1919, 1920, etc.) might lead to consider as migrated after the spread of the epidemic also some individuals whose parents actually migrated before that date. Such risk of misclassification of the period in which individuals' parents migrated is decreasing in the time distance L between their birth date and the date of the outbreak of the Spanish flu (1918). Thus, to address this possible issue we run two sets of robustness tests. In the first one, we allow for the existence of a lag between the time of migration and having a child in the country of arrival, and we test the robustness of our baseline results to the use of different lengths for such lag. In the second one, we run a set of “donut” regressions by directly removing individuals arriving in the United States in a year close to the cutoff. The results of both sets of tests are not significantly different with respect to the main specification.
Concerning the empirical specification adopted in the baseline analysis, we estimate inherited trust in both periods by Ordinary Least Squares (OLS) and using the following equation:
| (1) |
where i identifies the individual and c the country of ethnic origin. We exclude from the estimation all those countries which are present within only the pre‐1918 sample or only the post‐1918 one, and those for which there are less than 25 observations in one of the two periods, in order to guarantee a minimum level of representation within each sample (see Section Sensitivity Tests). We are interested in estimating the coefficients β c, that is the coefficients of the country‐of‐origins fixed effects. Each of these coefficients should capture the average level of trust transmitted to their descendants by people that moved from one of the sample countries of origins to the United States with respect to the reference country of origin, that is Austria. Given the dichotomous nature of the dependent variable each coefficient represents the variation in the predicted probability of trusting others (i.e., Trusti = 1) for a given country of origin with respect to Austrian Americans. The vector X i includes all the controls used in the regression, namely age, age squared, gender, education, income, religion, employment status, number of immigrant grandparents and whether he is second‐, third‐ or fourth‐generation American. Standard errors are adjusted for heteroskedasticity and clustered at country‐of‐origins level to account for serial correlation.
Appendix A provides a detailed list of all the variables employed in the estimation of inherited trust together with their description, while Table 1 shows the summary statistics for all of them. Table 2, instead, provides the estimated value of inherited trust (i.e., the predicted probability of trusting the others) for each country of origin, separately for the pre and post‐1918 samples.
TABLE 1.
Estimating inherited trust: Summary statistics
| Mean | Std. Dev. | Min | Max | |
|---|---|---|---|---|
| Pre‐1918 | ||||
| Trust | 0.48 | 0.50 | 0 | 1 |
| Income class | 10.61 | 2.38 | 1 | 12 |
| Age | 51.40 | 16.92 | 18 | 89 |
| Education | 13.41 | 2.90 | 0 | 20 |
| Male | 0.46 | 0.50 | 0 | 1 |
| Protestant | 0.66 | 0.47 | 0 | 1 |
| Catholic | 0.21 | 0.41 | 0 | 1 |
| Employed | 0.60 | 0.49 | 0 | 1 |
| Unemployed | 0.02 | 0.15 | 0 | 1 |
| Immigrant grandparents | 0.55 | 1.14 | 0 | 4 |
| Second‐generation | 0.03 | 0.16 | 0 | 1 |
| Third‐generation | 0.12 | 0.32 | 0 | 1 |
| Fourth‐generation | 0.86 | 0.35 | 0 | 1 |
| Post‐1918 | ||||
| Trust | 0.39 | 0.49 | 0 | 1 |
| Income class | 10.97 | 2.18 | 1 | 12 |
| Age | 37.42 | 13.99 | 18 | 89 |
| Education | 13.94 | 2.57 | 0 | 20 |
| Male | 0.48 | 0.50 | 0 | 1 |
| Protestant | 0.38 | 0.49 | 0 | 1 |
| Catholic | 0.35 | 0.48 | 0 | 1 |
| Employed | 0.73 | 0.45 | 0 | 1 |
| Unemployed | 0.04 | 0.19 | 0 | 1 |
| Immigrant grandparents | 1.83 | 1.64 | 0 | 4 |
| Second‐generation | 0.18 | 0.38 | 0 | 1 |
| Third‐generation | 0.40 | 0.49 | 0 | 1 |
| Fourth‐generation | 0.42 | 0.49 | 0 | 1 |
Note: The table displays the summary statistics for the variables used in the estimation of inherited trust.
TABLE 2.
Estimates of inherited trust
| Country | Pre‐1918 | se | Post‐1918 | se |
|---|---|---|---|---|
| Austria | 0.541*** | (0.013) | 0.406*** | (0.006) |
| Canada | 0.486*** | (0.006) | 0.493*** | (0.003) |
| Denmark | 0.477*** | (0.005) | 0.550*** | (0.010) |
| Finland | 0.509*** | (0.009) | 0.450*** | (0.009) |
| France | 0.483*** | (0.002) | 0.361*** | (0.003) |
| Germany | 0.481*** | (0.001) | 0.403*** | (0.002) |
| Hungary | 0.498*** | (0.009) | 0.415*** | (0.007) |
| Ireland | 0.469*** | (0.002) | 0.413*** | (0.004) |
| Italy | 0.428*** | (0.010) | 0.338*** | (0.007) |
| Mexico | 0.470*** | (0.009) | 0.283*** | (0.008) |
| Netherlands | 0.449*** | (0.003) | 0.432*** | (0.004) |
| Norway | 0.562*** | (0.006) | 0.422*** | (0.010) |
| Portugal | 0.384*** | (0.009) | 0.336*** | (0.004) |
| Russia | 0.386*** | (0.018) | 0.420*** | (0.012) |
| Spain | 0.385*** | (0.006) | 0.388*** | (0.002) |
| Sweden | 0.453*** | (0.006) | 0.444*** | (0.006) |
| Switzerland | 0.471*** | (0.003) | 0.515*** | (0.004) |
| United Kingdom | 0.504*** | (0.003) | 0.442*** | (0.005) |
| Observations | 10,107 | 4901 |
Dependent variable: Trust. Each coefficient represents the predicted probability of trusting the others in one of the country of origin included in the estimation samples for the pre‐1918 and post‐1918 periods. The predicted probability are calculated using the estimates of Equation (1) for both periods.
The pre‐ and post‐1918 sample of the GSS are not the same in terms of size. This is in part due to the large immigration waves to the US before 1918. 5 The use of a time varying control for changes in migration flows from each country of origins to the US, as described in Section 3.2, as well as the inclusion of the interaction between the post‐1918 dummy and the value of change in migration flows before 1918 as a robustness test in Section 4.1, should rule out any concern related that these samples differ in size. Another reason behind the difference in size between the two samples comes from the way we reconstruct the time of arrival in the United States of the GSS respondents' ancestors, and in particular to the fact that we consider a lower bound in the time window for defining each generation before and after 1918, but not an upper bound. 6 Given that, in Section 4.1, we explicitly test the robustness of the main results to the use of a 25‐years‐long period for defining each generation before and after 1918, thus with both an upper and a lower bound. The main results remain unaffected.
4.2. Inherited trust and Spanish Flu
In order to evaluate how inherited trust varied due to the spread of an epidemic, we compare its evolution before and after the outbreak of the Spanish flu. Thus, the estimates of inherited trust for each country of origin for the pre‐1918 and post‐1918 periods obtained as explained in Section Estimation of Inherited Trust are now used as the dependent variable.
To isolate the effect of the Spanish flu on inherited trust we adopt the following empirical approach:
| (2) |
where c identifies one of the 18 countries of origin and t the period of migration (i.e., pre‐ or post‐1918). The dependent variable, inherited trust is the predicted probability of trusting the others for each country as given in Table 2. The coefficient of interest here is β 2, that captures the effect of the treatment: mortality in the home country interacted with post 1918, a dummy that takes value 1 for the post‐1918 observations and 0 for those before 1918. It broadly measures the variation in the level of inherited trust of people whose ancestors emigrated to the United States after the outbreak of the Spanish flu from countries highly affected by the pandemic with respect to those whose ancestors came from less affected countries.
The equation includes X c,t which collects the country of origin‐level controls. We focus on five main variables that could affect both the level of trust of people emigrating from a specific country and their propensity to migrate from that country. Among these factors, which we collected for the pre‐ and post‐1918 periods, we take into consideration the GDP per capita, the population density, primary school enrollment, a general index for the quality of the home country institutions (Polity‐IV score) and the rate of change in migration flows from the home country to the United States. Moreover, we also include the interaction between post 1918 and a dummy, neutral, which is equal to one if the country of origins remained neutral during WWI, and 0 otherwise. Given the time overlap between the spread of the epidemic and the end of WWI, the inclusion of such interacting term is aimed at controlling for different kinds of heterogeneity in the post 1918 period for neutral and belligerent countries, respectively. In fact, the literature have found that experiencing a war may either lower or foster the level of trust among individuals (Bauer et al., 2016), thus controlling for the participation of the countries to WWI becomes crucial in our setting in order to avoid a possible bias in our estimates due to this alternative source of long‐lasting change in trust that is contemporaneous to the outbreak of the Spanish flu. 7 Lastly, country of origin fixed effects are captured by δ c, 8 while standard errors are adjusted for heteroskedasticity.
The validity of the DiDapproach just described relies on the assumption that countries heavily hit by the flu are on parallel trends of generalized trust with respect to those less affected in the pre‐1918 period. We test is this is indeed the case by also running an event study approach. In particular, we adapt the Algan and Cahuc's procedure described in Section 3.1 to estimate the level of trust for two different periods before 1918 (i.e., 1891–1900 and 1901–1910), and for one after (i.e., 1926–1935) 9 We estimate the following regression equation:
| (3) |
where Period 1t is a dummy indicating if the observation is related to the 1891–1900 period, and Period 3t if it instead refers to the 1926‐1935 period. To assess the validity of our DiD approach, interest lies in consistently estimating β 3 and β 4, which represent the differential change in the level of trust for the two periods, between countries more affected by the flu and those less affected, with respect to the last period before the epidemic, that is, our reference period that is 1901–1910. In other words, if our DiD is valid, we should expect the former to be not significant, while the latter to be negative and significant. The set of control variables X c,t is the same as included in Equation (2), with the only difference that now they are calculated for three different periods. As before, δ c controls for country of origins fixed effect and the standard error are robust to heteroschedasticity.
Appendix A provides a detailed list of all variables employed in the estimation of the effect of the pandemic on inherited trust together with their description, while Table 3 reports the summary statistics for all of them.
TABLE 3.
Spanish flu and trust: Summary statistics
| Mean | Std. Dev. | Min | Max | |
|---|---|---|---|---|
| Inherited trust | 0.44 | 0.06 | 0.28 | 0.56 |
| Flu death rate (deaths per 1000 inh.) | 7.4 | 4.4 | 2.4 | 20.6 |
| Polity‐IV | 3.8 | 6.0 | ‐6.6 | 10 |
| Population density (inh. per km2) | 70 | 62 | 1 | 217 |
| GDP per capita | 10,783 | 8923 | 1608 | 31,856 |
| Primary school enrolment (%) | 59 | 23 | 16 | 95 |
| Change in migration flows to US | 0.39 | 0.93 | −0.95 | 3.26 |
Note: The table displays the summary statistics for the variables used in the estimation of the relationship between inherited trust and Spanish flu mortality.
5. THE IMPACT OF THE SPANISH FLU ON SOCIAL TRUST
The main results of our analysis are presented in Table 4. In column (1) we run Equation (2) without any control, in column (2) we add the time‐varying controls, while in column (3) we also include the interaction between Post 1918 and Neutral. Instead, column (4) investigates how the neutrality of the home country in WWI eventually channeled the impact of the epidemic on trust by including a triple interaction between Flu Mortality, Post 1918, and the dummy Neutral.
TABLE 4.
The effect of Spanish flu on inherited trust: DiD estimates
| (1) | (2) | (3) | (4) | |
|---|---|---|---|---|
| Post1918 | −0.000 (0.032) | 0.031 (0.102) | 0.140 (0.101) | 0.158 (0.101) |
| Flu mortality × Post1918 | −0.007** (0.003) | −0.009** (0.004) | −0.014*** (0.004) | −0.009*** (0.003) |
| Flu Mortality × Post 1918 × Neutral | −0.013*** (0.004) | |||
| Country FE | YES | YES | YES | YES |
| Controls | NO | YES | YES | YES |
| Neutral × Post 1918 FE | NO | NO | YES | YES |
| Observations | 36 | 36 | 36 | 36 |
| Number of countries | 18 | 18 | 18 | 18 |
| R 2 | 0.486 | 0.568 | 0.666 | 0.723 |
Dependent variable: Inherited Trust. FluMortality is the country‐level death rate for Spanish flu (i.e., deaths per thousand inh.). Post1918 is a dummy taking the value 1 for the observations after 1918 and 0 otherwise. Columns (2), (3), and (4) include time‐varying controls. The controls are: GDP per capita (PPP), population density, primary school enrollment (%), Polity‐IV index and the change in migration flows to the US. Columns (3) and (4) also includes the interaction between the dummy Post1918 and the dummy Neutral, which is equal to 1 if the country of origins remained neutral during WWI and 0 otherwise. Standard errors are robust to heteroschedasticity.
*, **, *** indicate statistical significance at 10%, 5%, and 1% level, respectively.
As columns (1)–(3) show, we find a negative and significant effect of the Spanish Flu on trust, suggesting that large‐scale epidemics can indeed have a negative impact on the latter. According to the most complete estimates (i.e., column [3]), an increase in influenza mortality of 1 death per thousand resulted in a 1.4 percentage points decrease in trust, while a 1 standard deviation increase in mortality (i.e., an increase of 4.4 deaths per thousands) decreased our measure of trust by 6.6 percentage points, corresponding approximately to a 1 standard deviation in trust.
The results showed in column (4) provide suggestive evidence on the possible mechanism through which the main effect took place: the impact of the pandemic on trust was significantly more negative in countries that remained neutral during WWI. In fact, an increase in influenza mortality of 1 death per thousand in neutral countries resulted in a 2.2 percentage points decrease in trust. This evidence is strongly consistent with the idea that the narrower resonance of the war within these countries, and in particular the specific lack of war censorship on media, allowed citizens to fully perceive the extent and severity of the pandemic, and thus alter their social interactions in a stronger way.
Figure 3 gives a graphical representation of the main results obtained from running the event study specification with all the controls described in Equation (3), that is the estimates for the coefficient β 3 and β 4. 10 In line with our expectation, the estimation of the coefficient for the period 1891–1900 is not significant, signaling that the parallel trend assumption does hold, whereas the coefficient for the post‐flu period 1926–1935 is still negative and strongly significant. 11 This ultimately provides further support for the validity of our baseline approach.
FIGURE 3.
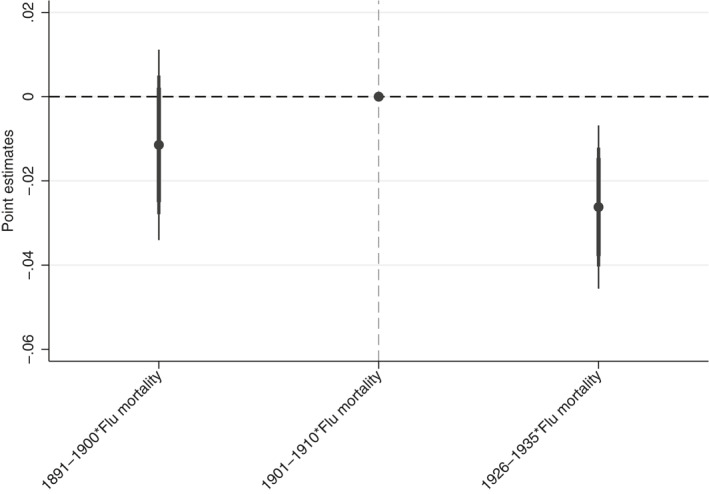
The Effect of Spanish Flu on inherited trust: Event study. The figure shows the point estimates and the confidence intervals at 90% (i.e., least‐wide spikes), at 95% (i.e., medium‐wide spikes) and at 99% (i.e., widest spikes) for the coefficients β 3 and β 4 showed in Equation (3). The dependent variable is generalized trust. Among the time‐varying controls included in the regression there are: GDP per capita (PPP), population density, primary school enrollment (%), Polity‐IV index, the change in migration flows to the United States, countries of origins fixed effect and the interaction between the dummy Post 1918 and the dummy Neutral, which is equal to 1 if the country of origins remained neutral during WWI and 0 otherwise. Standard errors are robust to heteroschedasticity
5.1. Robustness checks
In Table 5, we present the results of several tests to assess the robustness of the baseline results presented in column (3) of Table 4, which, as already said, we consider the most complete specification of our baseline regression model.
TABLE 5.
Robustness tests
| (1). | (2) | (3) | (4) | (5) | (6) | |
|---|---|---|---|---|---|---|
| Coeff. | Std. Err. | R 2 | F.S. obs. | S.S. obs. | Countries | |
| Panel (a): Different samples | ||||||
| 1) No minimum num. of respondents | −0.014*** | (0.003) | 0.540 | 15,579 | 38 | 19 |
| 2) Minimum 50 respondents | −0.016*** | (0.004) | 0.776 | 14,933 | 24 | 12 |
| 3) Bounded age intervals | −0.011** | (0.005) | 0.432 | 11,351 | 36 | 18 |
| 4) Excluding Mexico | −0.009** | (0.004) | 0.603 | 14,909 | 34 | 17 |
| Panel (b): Functional specification | ||||||
| 5) One step estimation | −0.015*** | (0.003) | 0.067 | ‐ | 15,536 | 18 |
| 6) Logit | −0.014*** | (0.004) | 0.671 | 15,536 | 36 | 18 |
| 7) Ordered logit | −0.014*** | (0.004) | 0.671 | 15,536 | 36 | 18 |
| Panel (c): Arrival in the US | ||||||
| 8) Lag = 5 | −0.013*** | (0.004) | 0.676 | 14,354 | 36 | 18 |
| 9) Lag = 10 | −0.014*** | (0.004) | 0.735 | 13,273 | 36 | 18 |
| 10) Lag = 15 | −0.014*** | (0.004) | 0.911 | 12,382 | 36 | 18 |
| 11) donut = ± 5 | −0.015*** | (0.005) | 0.638 | 12,985 | 36 | 18 |
| 12) donut = ± 10 | −0.017*** | (0.005) | 0.684 | 10,383 | 36 | 18 |
| 13) donut = ± 15 | −0.019*** | (0.005) | 0.877 | 7846 | 36 | 18 |
| 14) 20 Years generations | −0.015** | (0.005) | 0.552 | 15.536 | 36 | 18 |
| 15) 30 Years generations | −0.009** | (0.003) | 0.620 | 15.536 | 36 | 18 |
| Panel (d): Discrete measures | ||||||
| 16) Top 40% | −0.095* | (0.048) | 0.578 | 15,536 | 36 | 18 |
| 17) Top 10% | −0.262*** | (0.062) | 0.673 | 15,536 | 36 | 18 |
| Panel (e): Different control strategies | ||||||
| 18) Excluding population density | −0.014*** | (0.004) | 0.660 | 15,536 | 36 | 18 |
| 19) WWI deaths*Post1918 | −0.013*** | (0.003) | 0.699 | 15,536 | 32 | 16 |
| 20) WWII*Post1918 | −0.014*** | (0.004) | 0.749 | 15,536 | 36 | 18 |
| 21) Education*Post1918 | −0.014*** | (0.003) | 0.687 | 15,536 | 36 | 18 |
| 22) GDP*Post1918 | −0.010** | (0.004) | 0.618 | 15,536 | 36 | 18 |
| 23) Polity‐IV*Post1918 | −0.012** | (0.005) | 0.619 | 15,536 | 36 | 18 |
| 24) population density*Post 1918 | −0.014*** | (0.004) | 0.662 | 15,536 | 36 | 18 |
| 25) Migration*Post 1918 | −0.014*** | (0.004) | 0.659 | 15,536 | 36 | 18 |
| 26) All interactions | −0.009* | (0.005) | 0.633 | 15,536 | 36 | 18 |
| Panel (f): Std. Errors correction | ||||||
| 27) Small sample correction | −0.014*** | (0.004) | 0.650 | 15,536 | 36 | 18 |
| Panel (g): Falsification tests | ||||||
| 28) Trust in military | −0.004 | (0.003) | 0.407 | 22,820 | 36 | 18 |
| Panel (h): Additional outcomes | ||||||
| 29) Trust in federal govt. | −0.003 | (0.002) | 0.433 | 22,793 | 36 | 18 |
| 30) Trust in medicine | −0.006** | (0.003) | 0.693 | 22,915 | 36 | 18 |
Dependent variable: Inherited Trust. Coefficients showed in column (1) refers to the interaction term between FluMortality and Post1918 showed in Equation (2), while column (2) reports the standard errors of such coefficients. Column (3) reports the R 2, whereas columns (4)‐(6) the number of observations in the first step of the estimation procedure, those in the second one and the total number of countries included i each specifications, respectively. In row (1), we do not set a minimum number of GSS respondents for a country to be included in the sample, thus adding Japan. In row (2), we set a minimum of 50 GSS respondents. In row (3), we set bounded age interval to defining the generations before and after 1918. In row (4), we exclude Mexico from the sample countries. In row (5), we use a one‐step procedure for the estimation, while in row 6) and 7) we use as estimation model a logit and an order logit respectively. In rows (8), (9), and (10), we test different lags L to separate the pre‐1918 and post‐1918 GSS respondents groups. In rows (11), (12), and (13), we remove individuals at different distance from the cutoff of 1918. In rows (14) and (15), we define generations as being of 20 and 30 years respectively. In panel (d), we adopt discrete measures of flu mortality: in row (16), FluMortality is coded as 1 if a country belongs to the top 40% of the flu mortality distribution, while in row (17), if it belongs to the top 10%. In row (18), we exclude population density as a control, in row 19) we add the interaction between the number of WWI fatalities and the dummy Post1918 as further control, while in row (20), we add the interaction between participation to WWII and the dummy Post 1918. In rows (21)–(25), we separately include the value of each control before 1918 interacted with Post 1918, and jointly in row (26). In row (27), we adjust standard errors for small sample size. In row (28), we use as dependent variable Trust in the army. In row (29), we use as dependent variable Trust in the federal government, while in row 30) trust in medicine. If not diversely specified, the controls are GDP per capita (PPP), population density, primary school enrollment (%), Polity‐IV, migration to US and the interaction between the dummy Post1918 and the dummy Neutral, which is equal to 1 if the country of origins remained neutral during WWI and 0 otherwise. Standard errors are heteroskedastic‐robust.
*, ** ***indicate statistical significance at 10%, 5%, and 1% level, respectively.
In Panel (a), we test different ways of constructing the sample for estimating inherited trust in the pre‐ and post‐1918 periods, as well as the exclusion of Mexico from the analysis. Specifically, in row (1), we remove the minimum threshold of 25 respondents in each period, which essentially means adding also Japan to the sample of countries of origins taken into account. Instead, in row (2), we increase this threshold to 50 respondents. On the one hand, this implies an increase in the degree of representativeness of our estimates of inherited trust, but on the other hand it leads to a narrower sample of countries of origins. 12 In row (3), we consider 25‐year‐long periods for defining each generation before and after 1918, thus with both an upper and a lower bound. As pointed out in Section 3.1, this test is aimed at reducing any enedogeneity related to differences in size between the pre‐ and post‐1918 samples. In row (4), we exclude Mexico from our estimation since it represents an outlier both in terms of deaths due to the epidemic and size of the migration flow toward the United States.
Next, in Panel (b), we test an alternative functional forms for Equation (1). In row (5), we implement a one‐step procedure, thus estimating an individual‐level regression on GSS respondents that include individual controls, country‐fixed effects, time‐varying country characteristics, and the dummy Post 1918 to measure if the respondent's ancestors migrated before or after the epidemics. As in the baseline model, we interact Post 1918 with Spanish flu mortality in the home country to assess the impact of the epidemics on generalized trust. In particular, this test helps us to address any possible concern related to the precision of the second step‐coefficients of our procedure eventually connected to the fact that the values of dependent variable for this step are not directly observed but instead estimated through the first‐step. In row (6), we take into consideration the dichotomous nature of the dependent variable in Equation (1) and we estimate this latter by using a nonlinear regression model in the place of OLS, that is a Logit regression model. Next, while in the baseline we code trust as 1 for “Most people can be trusted” and 0 for “Cannot be too careful” or “Depends”, in row (7), we estimate trust using an ordered logit model, thus separating the respondents that answered “Depends” from those that answered “Cannot be too careful”.
Following, in Panel (c), we show the results of a set of tests aimed at better differentiating the respondents whose ancestors migrated before the flu epidemic from those whose ancestors migrated after that. As explained in Section 3.1, we do that by two batteries of tests. In the first set of tests, we introduce a lag L for selecting the respondents to include in the post‐1918 sample according to their birth date. In details, the post‐1918 sample will include now (I) all the second‐generation respondents that were born after 1918+L, (II) the third‐generation respondents born after 1943+L, and (III) all the fourth‐generation Americans born after 1968+L. As pointed out in Section 3.1, this is a departure from Algan and Cahuc (2010), and it is due to the fact that differently from them, we are interested in the variation of inherited trust around a precise date, 1918, thus requiring higher accuracy in the identification of the respondents whose ancestors migrated before or after such date. Taking for example second‐generation Americans, since we infer the date of migration of their parents from their year of birth, including in the post‐1918 sample also people born immediately after such date (i.e., 1919, 1920, etc..) might lead to consider as migrated after the spread of the epidemic also some individuals whose parents actually migrated before that date. Indeed, it is fair to assume the existence of a lag between the time of migration and having a child in the country of arrival, for instance related to the adaptation to the new context. Such risk of mis‐classification of the period in which individuals' parents migrated is decreasing in the time distance L between their birth date and the date of the outbreak of the Spanish flu (1918). Allowing for greater values of L would mean that we are allowing for a wider adaptation period, thus we are more likely to include only people whose parents did migrate after 1918 and then they had the child. On the contrary, very high values of L might lead us to consider in the post‐1918 sample many individuals whose parents did not really experience the epidemic in their home country because they were too young at that time or still not born. In row (8), L is equal to 5 years, it is equal to 10 years in row (9), while it is equal to 15 in row (10). As for the second kind of test, and similarly to the approach proposed in Barreca, Guldi, Lindo, and Waddell (2011), we run a set of “donut” regressions by simply removing individuals close to the 1918 cutoff. Specifically, we implement separately three regressions that in turn exclude individuals whose ancestors arrived in the US within 5 (row [11]), 10 (row [12]), and 15 (row [13]) years before or after 1918. As additional tests regarding the definition of ancestors' arrival, we also present the coefficients obtained by separately using two different lengths for the gap between generations, which are 20‐ and 30‐years (rows [14] and [15]). 13
In Panel (d), we present alternative discrete measures for the Spanish flu mortality in each county. Indeed, the method used to calculate the death rates employed in the main analysis varies from study to study, on the basis of the data available for each country. Such heterogeneity in how the death rates are calculated for each country could undermine the reliability of the comparison based on the continuous measure, mainly due to the difficulty of measuring marginal differences in such rates across countries. Moreover, in terms of size of the effect, the continuous measure captures the effect of the Spanish flu on trust only at the average level of the former, while it says nothing on the existence of possible non linearities in the relationship between the two variables. For this reasons, we repeat the analysis using two discrete measures of Spanish flu mortality related to its general distribution across all the countries included in our sample. In row (14), countries are assigned to the high flu mortality group if they belong to top 40% of the flu mortality distribution and 0 otherwise. In row (15), countries are assigned to the high flu mortality group if they belong to the top 10% of the flu mortality distribution and 0 otherwise. These measures, given their non‐parametric nature, should make the analysis of differences across countries both more reliable and more insightful than the use of a continuous measure of the impact of the Spanish flu.
In Panel (e), we test different control strategies for our baseline regression. In row (16), we do not include population density as a control in the regression, since population density after 1918 was potentially affected by the Spanish flu epidemic. In row (17)–(18), we allow the dummy Post 1918 to vary differently with respect to the country's deaths due to WWI, and its participation to WWII, respectively. We do so by including the interaction of Post 1918 separately with the number of WWI deaths at the country level as compiled by Barro, Ursua, and Weng (2020) 14 , and with a dummy taking value 1 if a country participated in WWII and 0 otherwise. Similarly, in rows (19)–(24). we include as controls a set of interactions between the dummy Post 1918 and the pre‐1918 value of the controls present in the baseline regression, first separately and then all taken together. The aim of this set of tests is to control for other possible major shocks experienced by some countries in the post‐1918 period by allowing the post‐1918 fixed effect to vary across different levels of each control variable. 15
Given the reduced number of observations for estimating Equation (2), in row (25) of Panel (f), we allow for small‐sample correction of the standard errors. In row (26) of Panel (g), we run a falsification test for the baseline specification by analyzing another social attitude that, while correlated with generalized trust, is unlikely to be significantly altered by the Spanish flu pandemic, that is, trust in the army.
All the tests presented through Panels (a)–(f) show that the coefficient of interest remains significantly negative, whereas the falsification test presented in Panel (g) is not statistically different from zero. These results ultimately confirm the robustness of the main findings: social trust appears to have decreased in countries that were hit the hardest by the pandemic.
In Panel (h), we extend our analysis and we show the effect of the Spanish flu on other two outcomes potentially related to our main analysis on generalized trust, which are trust in federal government (row [27]) and medicine (row [28]). 16 On the one hand, we do not find any significant effect on the former. This is a quite interesting result, especially in the light of the work by Flückiger et al. (2019) on the Ebola outbreak in Africa. In fact, while for Ebola there is no effect on social trust but a positive one on trust in government, just the opposite seems to be true for the Spanish flu. This eventually reflects how different features of the two diseases led to different impacts on individual attitudes. On the other hand, we also observe a negative and significant effect of the Spanish flu on the general level of trust in medicine, which is in line with our argument that the pandemic was an utter failure of health care institutions, and that such failure could have helped to catalyze the negative impact of the epidemic on peoples' level of generalized trust.
Lastly, it is worth reflecting on the fact that in principle, our estimates might be explained by the existence of negative selection on high‐trust migrants from each country of origins, which is positively correlated with the intensity of Spanish flu in the country, rather than by the effect of epidemics on trust. In fact, it is possible that people with a higher level of trust had higher mortality from the flu, and so they migrated less. Here the argument would be that high trust individuals would have a lower reduction in their social interactions, and consequently increase their probability of becoming infected and dying. Unfortunately, the complete absence of cross‐countries data about social trust among migrants to the United States for the periods considered in our analysis makes any kind of empirical test of such hypothesis simply unfeasible in our framework. Nonetheless, the literature on the role of trust in mediating the probability of infection during an epidemic seems to point toward to the opposite dynamics (Barrios, Benmelech, Hochberg, Sapienza, & Zingales, 2020; Chuang, Huang, Tseng, Yen, & Yang, 2015; Rönnerstrand, 2013). In particular, the higher the level of social trust, the more people will comply with the policy recommendation to avoid contagion, thus decreasing their likelihood to get infected. This would mean that if a selection on high‐trust of migrants induced by the flu does exist, it would be a positive one ultimately generating an attenuation bias in our estimates.
6. CONCLUSIONS
Our analyses suggest that experiencing the Spanish Flu and the associated condition of social disruption and generalized mistrust had permanent consequences on individual behavior in terms of lower social trust. These mutated individual social traits were inherited by descendants, at least to some significant degree. Our results are in line with recent studies showing how large‐scale crises affect individual behavior in a lasting way. This literature, however, has focused on natural disasters, and not on epidemics or pandemics. Moreover, disasters of different kinds also produce different consequences for trust (Albrecht, 2017; Skidmore & Toya, 2014). In other words, not all natural disasters would necessarily reduce social trust. Among those that do, however, earthquakes and floods feature prominently (Carlin et al., 2014; Skidmore & Toya, 2014). Our finding suggests that major pandemics should be added to this list of trust‐reducing catastrophes. Although we are unable to undertake similar studies for pre‐Spanish Flu pandemics, one can hypothesize that processes of this kind might also have been triggered by other major mortality crises of the past, which would include the medieval Black Death and the severe Cholera pandemics of the nineteenth century. Our findings are fully in line with recent research on the lasting consequences of some of these episodes, consequences that can be felt for several centuries (Alfani, 2020; Alfani & Murphy, 2017; Jedwab et al., 2016, 2019; Koyama & Johnson, 2019; Richardson & McBride, 2009; Voitgländer & Voth, 2012). Although our evidence involves a much shorter time period and we do not claim that the effects of the Spanish Flu will be felt centuries from now, our key result has important implications for our understanding of socioeconomic development of today's societies. Given the enduring differential in health levels across world regions, and considering the fact that the most recent major epidemics have mostly involved relatively poor countries, one may argue that any forecasting of their future performance should account for the lasting damage to social trust, which has elsewhere been shown to have pivotal impact on the quality of institutions (Knack, 2002) and economic success (Algan & Cahuc, 2010). This feature might be relevant for the African sub‐Saharan countries which have been affected by Ebola in recent years. Indeed, during the 2013–16 Ebola epidemic episodes of social mistrust were reported, involving not only those infected but also the survivors who carried a heavy social stigma several months after they had recovered from the disease (Hayden, 2014; O'Grada, 2016; Reardon, 2015). The trauma suffered caused lingering clinical mental health conditions to the survivors (Reardon, 2015), but the consequences of Ebola and of other severe epidemics and pandemics—both future and past—might be more subtle, last longer, and in the end be more harmful to society as a whole than what can be detected clinically.
Our findings are also relevant for the ongoing debate about the economic consequences of COVID‐19. A general point to make, is that based on the experience of the Spanish Flu, we should consider the possibility that beyond immediate and relatively easy to measure effects on national economies, other, more elusive effects of the pandemic might be equally relevant and should be properly taken into account. A particularly important point is that if, during the Spanish Flu, the failure of government institutions and national health care services to contain the crisis led civil societies to experience a serious breakdown due to the climate of generalized suspicion (a situation further exacerbated by mistakes in communication, also due to war censorship) and this increased the persistent damage to social capital, then governments facing COVID‐19 today might have an additional reason to opt for strong policies of pandemic containment. While these are undoubtedly costly in the short run, it might be that they will contribute to minimize some economic costs to be paid in the long run.
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest.
Supporting information
Supporting information S1
ACKNOWLEDGMENT
We are grateful to Gianmarco Daniele, Noel Johnson, Federico Masera and the participants at Giornate di Studio sulla Popolazione (Popdays) 2019 for the useful comments. We gratefully acknowledge financial support from the European Research Council with grant no. 694145.
ENDNOTES
In fact, as described by Honigsbaum (2013), p. 184, in belligerent countries, “propaganda discourses encouraged the cultivation of stoicism at the expense of other emotional scripts”, which might have gone a long way toward reducing the impact of the pandemic on individual behavior and on public memory (Crosby, 1976).
The 1972–1974 surveys used modified probability designs while for the remaining waves a full‐probability sample design has been adopted.
In a robustness test included in Section 4, we also consider the three categories separately.
There are three other countries for which this information is available, that is Japan, India and the Philippines. Concerning Japan, it is excluded from the baseline due to its very limited representation within the final samples used to run our main analysis. However, among the sensitivity tests, we re‐run the regression including this country and the results are almost unaffected. Regarding India and the Philippines, they are excluded because of missing values in the control variables. It is also worth mentioning that an estimation of the Spanish flu mortality is also available for Brazil from a specific administrative source and it has been employed in Guimbeau et al. (2019), but such estimation cannot be used in our study since it regards only a specific region within the country (i.e., the state of São Paulo), thus not comparable with those at the country level provided in Johnson and Mueller (2002).
In fact, our estimation samples contain mostly European countries, and the arrival of people from these countries before the Spanish flu mostly happened during two specific periods: (i) the first part of the 19th Century and (ii) between 1880 and 1920.
This mechanically implies a higher number of individuals available to estimate the pre‐1918 level of trust than for the one for post‐1918, simply because there is a longer time window for arriving in the US and having descendants.
This interaction also helps us to address potential concerns related to any kind of trend in the reported number of deaths for Spanish flu linked to WWI.
It is worth to notice that among the many potentially observable and unobservable confounders, which the inclusion of country of origin‐fixed effects eventually controlled for, there is the possible existence of country‐specific measurement error in the numbers of reported deaths for Spanish flu, as for example the one linked to the participation of the country to WWI. In fact, it is fair to assume this error to be fixed at the country of origins level, at least in the one year and half during which the epidemic spread, and so captured by the country of origin‐fixed effects.
The estimates for the three periods are presented in Appendix B. Given the possibility of misclassification around the cutoff described in Section 3.1, we exclude from this specification the period between 1911 and 1925. Furthermore, it is worth to notice that, given the lower and upper limits imposed on the time window for each period, the number of individuals available for estimating the level of trust in the first stage of our procedure is strongly reduced with respect to the DiD specification. For this reason, we prefer to maintain the event study only as a complementary approach to the DiD implemented in the baseline.
This specification is directly comparable with the estimates presented in column (3) of Table 4.
We run the event study approach using the most complete specification, that is the one including time‐varying controls, country of origins fixed effects and the interaction between the period dummies and the status of the country during WWI. For sake of brevity and clarity we omit the regression tables with the coefficients of the first and second stage of our procedure. Instead they are reported in Appendix B.
Specifically, using the threshold of 50 respondents we are left only with Canada, the United Kingdom, France, Germany, Ireland, Italy, Mexico, Netherlands, Norway, Russia, Spain, and Sweden.
Note that using a shorter or a longer definition does not have much sense in our specific framework, since we are interested in estimating inherited trust around a specific date (i.e., 1918). A significantly shorter definition for the generational gap would magnify the concerns related to the differentiation between respondents whose ancestors migrated before the flu epidemic and those whose ancestors migrated afterward, which we try to partially address in rows (8)–(13) of Table 5. For example, with 10‐years generations we would consider as third‐generation Americans all the individuals born after 1929, thus likely also including many respondents whose ancestors actually emigrated before the onset of the pandemic. Similarly, a longer definition would also increase the likelihood to mis‐classified the arrival individuals' ancestor with respect to 1918, but just in the opposite direction. Indeed, a significantly longer generational gap, as for example one of 50 years, would imply to consider the ancestors of third‐generation Americans born up to 1968 to have migrated to the United States before 1918, a rather questionable assumption.
Data are unavailable for Finland and Ireland.
In particular, the test presented in row (24) allow for the possibility of changes in the US migration policy both between countries and periods.
These measures, as the one employed in row (26), are calculated with the same methodology employed in the main analysis, but using different GSS survey questions.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
REFERENCES
- Albrecht, F. (2017). Natural hazard events and social capital: the social impact of natural disasters. Disasters, 42(2), 336–360. 10.1111/disa.12246 [DOI] [PubMed] [Google Scholar]
- Alfani, G. (2020). Pandemics and asymmetric shocks: Evidence from the history of plague in europe and the mediterranean. Technical report, CAGE Working Paper No. 478. [Google Scholar]
- Alfani, G. , & Murphy, T. (2017). Plague and lethal epidemics in the pre‐industrial world. Journal of Economic History, 77(1), 314–343. [Google Scholar]
- Alfani, G. , & Percoco, M. (2019). Plague and long‐term development: The lasting effects of the 1629–30 epidemic on the Italian cities. Economic History Review, 72(4), 1175–1201. [Google Scholar]
- Algan Y., & Cahuc P. (2010). Inherited Trust and Growth. American Economic Review, 100(5), 2060–2092. http://org/10.1257/aer.100.5.2060 [Google Scholar]
- Algan, Y. , & Cahuc, P. (2014). Trust, growth and well‐being: New evidence and policy implications. North Holland, Netherlands: Handbook of Economic Growth. [Google Scholar]
- Almond, D. (2006). Is the 1918 influenza pandemic over? Long‐term effects of in utero influenza exposure in the post‐1940 U.S. Population. Journal of Political Economy, 114(4), 672–712. [Google Scholar]
- Almond, G. , & Verba, S. (1963). The civic culture: Political attitudes and democracy in five nations. Sage Publications, Inc. [Google Scholar]
- Barreca, A. I. , Guldi, M. , Lindo, J. M. , & Waddell, G. R. (2011). Saving babies? Revisiting the effect of very low birth weight classification*. The Quarterly Journal of Economics, 126(4), 2117–2123. [DOI] [PubMed] [Google Scholar]
- Barrios, J. M. , Benmelech, E. , Hochberg, Y. V. , Sapienza, P. , & Zingales, L. (2020). Civic capital and social distancing during the covid‐19 pandemic. Working Paper 27320. Cambridge, MA: National Bureau of Economic Research. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barro, J. , Ursua, J. , & Weng, J. (2020). The coronavirus and the great influenza epidemic lessons from the “Spanish flu” for the coronavirus's potential effects on mortality and economic activity. Technical report, CESifo Working Paper No. 8166. [Google Scholar]
- Barry, J. M. (2005). 1918 revisited: Lessons and suggestions for further inquiry. In: Knobler, K. , Mack, A. , & Mahmoud, A. (Eds)., The Threat of Pandemic Influenza: Are We Ready? Workshop Summary. Washington, DC: National Academies Press. [PubMed] [Google Scholar]
- Bauer, M. , Blattman, C. , Chytilová, J. , Henrich, J. , Miguel, E. , & Mitts, T. (2016). Can war foster cooperation? Journal of Economic Perspectives, 30(3), 249–274. [Google Scholar]
- Bengtsson, T. , & Helgertz, J. (2015). The long lasting influenza: The impact of fetal stress during the 1918 influenza pandemic on socioeconomic attainment and health in Sweden 1968‐2012. IZA Discussion Paper (9327). 672–712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buggle, J. , & Durante, R. (2017). Climate risk, cooperation, and the co‐evolution of culture and institutions Discussion Paper No. DP12380. [Google Scholar]
- Calo‐Blanco, A. , Kovářík, J. , Mengel, F. , & Romero, J. G. (2017). Natural disasters and indicators of social cohesion. PloS One, 12(6).e0176885. 10.1371/journal.pone.0176885 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carillo, M. , & Jappelli, T. (2020). Pandemics and local economic growth: Evidence from the great influenza in Italy. Technical report, CEPR Discussion Paper No. DP14849. [Google Scholar]
- Carlin, R. , Love, G. , & Zechmeister, E. (2014). Trust shaken: Earthquake damage, state capacity, and interpersonal trust in comparative perspective. Comparative Politics, 46(4), 419–437. [Google Scholar]
- Chuang, Y.‐C. , Huang, Y.‐L. , Tseng, K.‐C. , Yen, C.‐H. , & Yang, L.‐h. (2015). Social capital and health‐protective behavior intentions in an influenza pandemic. PloS One, 10(4). 10.1371/journal.pone.0122970 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohn, S. (2018). Epidemics. Hate and compassion from the plague of Athens to AIDS. Oxford University Press. [Google Scholar]
- Collier, R. (1974). The plague of the Spanish lady: The influenza pandemic of 1918‐1919. New York, NY: Atheneum. [Google Scholar]
- Crosby, W. (1976). America's forgotten pandemic: The influenza of 1918. Cambridge University Press. [Google Scholar]
- Dohmen, T. , Falk, A. , Huffman, D. , & Sunde, U. (2012). The intergenerational transmission of risk and trust attitudes. The Review of Economic Studies, 79(2), 645–677. [Google Scholar]
- Flückiger, M. , Ludwig, M. , & Sina Önder, A. (2019). Ebola and state legitimacy. The Economic Journal, 129(621), 2064–2089. [Google Scholar]
- Galletta, S. , & Giommoni, T. (2020). The effect of the 1918 influenza pandemic on income inequality: Evidence from Italy. Covid Economics Vetted and Real‐Time Papers (33). [Google Scholar]
- Guimbeau, A. , Menon, N. , & Musacchio, A. (2019). The Brazilian bombshell? The long‐term impact of the 1918 influenza pandemic the south American way. Retrieved from 10.2139/ssrn.3381800 [DOI] [Google Scholar]
- Guiso, L. , Sapienza, P. , & Zingales, L. (2016). Long‐term persistence. Journal of the European Economic Association, 14(6), 1401–1436. [Google Scholar]
- Hayden, E. (2014, December). Ebola survivors fight prejudice. Nature (News). [Google Scholar]
- Honigsbaum, M. (2013). Regulating the 1918–19 pandemic: Flu, stoicism and the northcliffe press. Medical History, 57(2), 165–185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jedwab, R. , Johnson, N. D. , & Koyama, M. (2016). Bones, bacteria and break points: The heterogeneous spatial effects of the black death and long‐run growth. GMU Working Paper in Economics, 16–30. [Google Scholar]
- Jedwab, R. , Johnson, N. D. , & Koyama, M. (2019). Negative shocks and mass persecutions: Evidence from the black death. Journal of Economic Growth. [Google Scholar]
- Johnson, N. (2012). Measuring a pandemic: Mortality, demography and geography. Popolazione e storia, 4(2). [Google Scholar]
- Johnson, N. , & Mueller, J. (2002). Updating the accounts: Global mortality of the 1918‐1920 ‘Spanish’ influenza pandemic. Bullettin of the History of Medicine, 76, 105–115. [DOI] [PubMed] [Google Scholar]
- Karlsson, M. , Nilsson, T. , & Pichler, S. (2014). The impact of the 1918 Spanish flu epidemic on economic performance in Sweden: An investigation into the consequences of an extraordinary mortality shock. Journal of Health Economics, 36, 1–19. [DOI] [PubMed] [Google Scholar]
- Knack, S. (2002). Social capital and the quality of government: Evidence from the states. American Journal of Political Science, 46(4), 772–785. [Google Scholar]
- Koyama, M. , & Johnson, N. (2019). Persecution & toleration: The long road to religious freedom. Cambridge University Press. [Google Scholar]
- Lichter, A. , Loeffler, M. , & Siegloch, S. (2015). The economic costs of mass surveillance: Insights from Stasi spying in East Germany. Technical report IZA Discussion Papers. [Google Scholar]
- Lin, M.‐J. , & Liu, E. M. (2014). Does in utero exposure to illness matter? The 1918 influenza epidemic in taiwan as a natural experiment. Journal of Health Economics, 37, 152–163. [DOI] [PubMed] [Google Scholar]
- Lowes, S. R. , & Montero, E. (2018). The legacy of colonial medicine in central Africa. CEPR discussion papers 12772. [Google Scholar]
- Mamelund, S. (2011). Geography may explain adult mortality from the 1918–20 influenza pandemic. Epidemics, 3(1), 46–60. [DOI] [PubMed] [Google Scholar]
- Medina, R. , Manicassamy, B. , Stertz, S. , Seibert, C. , Hai, R. , Belshe, R. , … García‐Sastre, A. (2010). Pandemic 2009 H1N1 vaccine protects against 1918 Spanish influenza virus. Nature Communications, 1(28). 10.1038/ncomms1026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murray, C. J. , Lopez, A. D. , Chin, B. , Feehan, D. , & Hill, K. H. (2006). Estimation of potential global pandemic influenza mortality on the basis of vital registry data from the 1918–20 pandemic: A quantitative analysis. The Lancet, 368(9554), 2211–2218. [DOI] [PubMed] [Google Scholar]
- Myrskylä, M. , Mehta, N. , & Chang, V. (2013). Early life exposure to the 1918 influenza pandemic and old‐age Mortality by cause of death. American Journal of Public Health, 103(7), 83–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nunn, N. , & Wantchekon, L. (2011). The slave trade and the origins of Mistrust in Africa. American Economic Review, 101(7), 3221–3252. [Google Scholar]
- O'Grada, C. (2016). On plague in a time of Ebola. School of Economics Working Papers 201529. Dublin, Ireland: University College Dublin. [Google Scholar]
- Phillps, H. , & Killingray, K. (2003). The Spanish influenza Pandemic of 1918‐1919: New perspectives. 2 park square. Milton Park, Abingdon, Oxon, UK: Routledge. [Google Scholar]
- Ramos‐Toro, D. (2019). Social exclusion and social preferences: Evidence from Colombia's leper colony. [Google Scholar]
- Reardon, S. (2015). Ebola's mental‐health wounds linger in Africa: Health‐care workers struggle to help people who have been traumatized by the epidemic. Nature, 519(7541), 13–15. [DOI] [PubMed] [Google Scholar]
- Richardson, G. , & McBride, M. (2009). Religion, longevity, and cooperation: The case of the craft guild. Journal of Economic Behavior & Organization, 71(2), 172–186. [Google Scholar]
- Rönnerstrand, B. (2013). Social capital and immunisation against the 2009 a (h1n1) pandemic in Sweden. Scandinavian Journal of Public Health, 41(8), 853–859. [DOI] [PubMed] [Google Scholar]
- Skidmore, M. , & Toya, H. (2014). Do natural disasters enhance societal trust?. Kyklos, 67, 255–279. [Google Scholar]
- Tabellini, G. (2008). Institutions and culture. Journal of the European Economic Association, 6(2–3), 255–294. [Google Scholar]
- Tabellini, G. (2010). Culture and institutions: Economic development in the regions of europe. Journal of the European Economic Association, 8(4), 677–716. [Google Scholar]
- Taubenberger, J. , & Morens, D. (2006). 1918 influenza: The mother of all pandemics. Emerging Infectious Diseases, 12(1), 15–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taubenberger, J. K. , Reid, A. H. , Lourens, R. M. , Wang, R. , Jin, G. , & Fanning, T. G. (2005). Characterization of the 1918 influenza virus polymerase genes. Nature, 437(7060), 889. [DOI] [PubMed] [Google Scholar]
- Tumpey, T. M. , Basler, C. F. , Aguilar, P. V. , Zeng, H. , Solórzano, A. , Swayne, D. E. , … García‐Sastre, A. (2005). Characterization of the reconstructed 1918 Spanish influenza pandemic virus. Science, 310(5745), 77–80. [DOI] [PubMed] [Google Scholar]
- Uslaner, E. , & yamamura, E. (2016). Disaster and political trust: The Japan tsunami and earthquake of 2011. Technical report, MPRA Paper No. 70527. [Google Scholar]
- Voitgländer, N. , & Voth, H. (2012). Persecution perpetuated: The Medieval origins of anti‐semitic violence in Nazi Germany. Quarterly Journal of Economics, 127(3), 1339–1392. [Google Scholar]
- Young, A. (2005). The gift of the dying: The tragedy of aids and the welfare of future african generations. The Quarterly Journal of Economics, 120(2), 423–466. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting information S1
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.