

Abstract
Introduction
To explore whether Skog's theory of collectivity of drinking cultures is valid across groups with different socioeconomic position (SEP).
Methods
Individual‐level information on alcohol consumption and SEP for the years 2004–2014 were retrieved from the Monitoring Project; a nationally representative monthly alcohol use survey. The analytical sample consisted of 162 369 respondents aged 25–79 years. SEP was measured by education level. Alcohol use was measured by yearly volume of consumption and frequency of heavy episodic drinking (HED). Respondents were divided into six SEP‐groups based on their education level and sex. Mean yearly volume consumption and prevalence of monthly HED was calculated for each group and graphically plotted against the overall mean volume of consumption.
Results
The yearly changes in overall mean consumption during the study period reflected a collective shift in drinking across groups with basic, intermediate and high education. There were also indications that changes in overall mean consumption reflected collective shifts in the prevalence of HED across the SEP‐groups. Moreover, while the magnitude of the associations for both average volume and HED differed somewhat in strength across the SEP‐groups, they were clearly in the same, positive, direction.
Discussion and Conclusions
Our findings add support for including a socioeconomic dimension to Skog's theory of collectivity of drinking cultures. Future studies should replicate our analyses on cases and periods with more tangible changes in the price and availability of alcohol.
Keywords: average volume of alcohol consumption, heavy episodic drinking, socioeconomic position, collectivity, Sweden
Introduction
A large body of research has documented a positive association between total alcohol consumption and related harm at the population level [1]. This observation forms a cornerstone of alcohol epidemiology, and acts as the main motivation for general population approaches that aim to prevent alcohol‐related harm by reducing the total consumption [2, 3, 4, 5]. Such approaches mainly involve policy measures targeting the price and availability of alcohol [6].
The key theory for understanding the mechanism underlying the population‐level association between alcohol and harm is provided by Skog's theory of the collectivity of drinking cultures and focuses on how alcohol consumption tends to shift within populations [7]. According to Skog, individual drinking behaviour is heavily affected by mechanisms of social interaction, both through direct personal interaction and in the form of more indirect social control. This social process aggregates up to a complex pattern of interdependencies between individual members of a group, or even an entire society, so that it displays a strong collectivity in its drinking behaviour. More specifically, Skog predicts that changes in overall mean consumption tend to occur as collective shifts across drinkers at all levels of the consumption distribution, including heavy drinkers [8]. As a result, changes in overall mean alcohol consumption tend to be positively associated with changes in alcohol‐related harm, and for this reason, alcohol policy measures that reduce mean alcohol consumption will also tend to lower the prevalence of alcohol‐related harm [3].
Skog's own empirical research was based on survey‐derived consumption data from cross‐sectional samples of different populations, and did not actually assess temporal changes within populations. However, the theory has more recently been tested on temporal data within countries, and received strong empirical support for adult populations [7, 9] as well as for youth [10, 11, 12].
Still, few studies have tested if changes in mean consumption tend to occur as collective shifts also across subgroups of the population, for instance, across different socioeconomic strata—which is the focus of the present study. This question is highly relevant from a policy perspective, considering the increasing evidence of an alcohol harm paradox, that is, the observation that groups with low socioeconomic position (SEP) experience a disproportionally large share of alcohol‐related harm, although they tend to drink less, or at least not more, than other social strata [13, 14, 15, 16]. Moreover, a recent study applying auto‐regressive integrated moving average time series modelling to Swedish data for the period 1990–2017, found that a 1 L increase in per capita consumption was associated with a larger increase in the number of alcohol‐related deaths among low than among highly educated groups [17]. A possible explanation of this finding is that there has been a differential development in SEP‐specific alcohol consumption trajectories, with increases in per capita consumption disproportionally allocated to low SEP‐groups, which would imply an exception from the pattern of collectivity.
According to Skog [18], exceptions from the pattern of collectivity are plausible under some circumstances. First, the network effect underlying the synchronisation of drinking may be constrained by social and cultural boundaries between population subgroups, resulting in more or less diverging drinking trajectories across social strata. Second, Skog noted that consumption is influenced by numerous structural factors, for example, real income and alcohol prices/taxation, and that changes in these factors may have a differential impact on the alcohol consumption across SEP‐groups. In line with this, some studies have found diverging trajectories of consumption and/or related harm across SEP‐groups following changes in the economic availability of alcohol [19, 20, 21, 22]. One such case is Finland, where a 33% reduction of alcohol excise taxes in 2004 resulted in increased alcohol‐related mortality mainly among less privileged groups (unemployed and early‐age pensioners) [19]. However, other findings are more inconclusive. For instance, one study tested the hypothesis that the increased affordability of alcohol in Sweden that followed from the EU membership in 1995 would be associated with an increase in SEP‐differences in alcohol‐related mortality [23]. Findings suggested that this was the case for women but not for men. Furthermore, a more recent and systematic study from Germany [24] explored possible explanations for diverging trends in alcohol consumption and related harm by testing for polarisation in drinking within and across SEP‐groups. Although the rate of change tended to be larger among higher consumption levels, all SEP‐groups showed a general decrease in consumption during the study period. Still, to our knowledge, no study has applied Skog's analytical approach to directly test whether changes in mean consumption tend to reflect collective shifts also across SEP‐groups.
Against this background, the present study aims to perform a more comprehensive test of whether Skog's notion of collectivity of drinking is also valid across SEP‐groups. To this aim, we will apply Skog's analytical approach on data from a unique, annually repeated national Swedish cross‐sectional alcohol use survey, and assess whether yearly changes in the mean consumption of alcohol between 2004 and 2014 have occurred as collective shifts across educational groups. Moreover, because SEP‐differences in heavy episodic drinking (HED) tend to account for a larger proportion of the social gradient in alcohol‐related mortality and morbidity than does the average volume of consumption [25], we also test whether changes in per capita consumption are echoed in collective shifts in the prevalence of HED across educational groups.
It should be noted that Skog's theory makes predictions about marginal distributions, not about individual‐level changes in drinking. Thus, the finding that an increase in total consumption by, say 10%, reflects an increase by about 10% in all consumption groups, from light to heavy drinkers, does not imply that every individual drinker has increased his/her drinking by 10%. Some may have increased more, some less (or even decreased) [see Ref. 18]. The degree of divergency in the pattern underlying these collective movements is of interest in itself, but it is not the issue that our study addresses. Our methodological approach is thus the same as that which has been applied in other tests of Skog's theory of collectivity [7, 10]. The novelty of our study is that we test whether the theory of collectivity is valid not only across consumption groups (light to heavy drinkers), but also across SEP‐groups.
Methods
Individual‐level data on alcohol consumption and SEP were retrieved from a database collected within the Monitoring Project; an ongoing monthly telephone survey including questions about self‐reported drinking habits and purchases of unrecorded alcohol (e.g. travellers' imports and smuggling). A nationally representative sample of the general Swedish population aged 16–80 years is randomly drawn on a monthly basis. Interviews are then conducted until 1500 respondents have been interviewed each month, resulting in a repeated cross‐sectional sample of approximately 18 000 respondents per year. Respondents who appear more than once in the sample during a year (which occurs 2–4 times per year) are excluded. The monthly non‐response rate ranges between 40% and 60%, and has tended to increase over time [26]. The analytical sample for the present study included the years 2004–2014 and respondents aged 25–79 years, who provided complete information on education and alcohol use, amounting to 162 369 individuals.
Ethical considerations
The study was approved by the regional ethics committee in Stockholm (Dnr 2018/2018–2031/5).
Measures
Socioeconomic position
We used self‐reported education as indicator of SEP. Education, together with occupation and income, is one of the main dimensions for classifying SEP in epidemiological studies. Education has the advantage of being more stable within individuals over time, and is less likely to be affected by reversed causation than are occupation and income, that is, that a person's occupation and/or income may be negatively affected by his/her misuse of alcohol. The education measure was categorised into three groups: (i) basic education (9 years or less); (ii) intermediate education (upper secondary school education, 10–12 years); and (iii) high education (college or university education, 13+ years).
Average volume of alcohol consumption
This was measured by a beverage‐specific quantity and frequency scale. This scale combines questions on how often spirits, wine, beer and cider have been consumed during the past 30 days, with the typical amount consumed per occasion. The frequency questions were the same for all beverage types: ‘How often have you consumed spirits/wine/beer during the past 30 days?’. The response alternatives were ‘never’, ‘about once’, ‘about 2–3 times’, ‘4–5 times a week’ and ‘more or less every day’. The response alternatives for the quantity questions were specific to each beverage and customised to correspond to the standard containers in which each beverage is sold. The answers were then summarised into a measure of overall drinking during the past 30 days, and converted into yearly volume of consumption in litres of 100% alcohol. HED was measured by a question on how often the respondent, on one occasion, had consumed alcohol equivalent to at least a whole bottle of wine, four cans (50 cl) of strong beer (5.5% alcohol by volume), six cans of medium‐strength beer (3.5% alcohol by volume) or 25 cl spirits. The responses were coded into a dichotomous variable taking the value 1 for those reporting HED once a month or more often, and 0 otherwise.
Statistical analysis
The respondents were stratified into six groups (for convenience, they are hereafter denoted as SEP‐groups), based on their educational level and sex (that is, men with basic education, men with intermediate education, men with high education, women with basic education, women with intermediate education and women with high education). The six SEP‐groups differ from each other with respect to age; for instance, men with basic education are on average 11 years older than men with high education. As age is related to drinking, these age differences need to be adjusted for. In order to account for possible confounding by age, we first estimated a regression model with alcohol consumption as outcome, and age and SEP (categorical variable) as input. Next, we used the post‐estimation procedure Margins in Stata v.15 to obtain the age‐adjusted mean consumption in each SEP‐group. The same procedure was applied to obtain the age‐adjusted prevalence of monthly HED [see 27 for a description of the Margins command].
In our assessment of the collectivity of drinking hypothesis, we first depicted the consumption trajectories for each SEP‐group. Next, we followed the procedure applied by Skog, that is, for each year the consumption of each SEP‐group was logged and plotted against the overall mean logged consumption the corresponding year [8]. However, where Skog plotted the logged mean consumption for different consumption quintiles, we instead plotted: (i) the logged mean consumption; and (ii) prevalence of HED for each of the SEP‐groups. Lastly, we used linear regression (ordinary least‐squares regression) to estimate the following model separately for each of the six SEP‐groups:
where C it is the age‐adjusted mean consumption in SEP‐group i at year t, and C t is the overall mean consumption at year t. The parameter of interest is e i, that is, the elasticity that expresses the percentage change in mean consumption in SEP‐group i, given a 1% change in the overall mean consumption. The collectivity of drinking hypothesis predicts that the elasticity is positive for each SEP‐group.
Results
Tables 1 and 2 provide descriptive information on the number of individuals and group proportions for each of the SEP‐groups. During the study period, the distribution of the population across the educational groups changed. For both sexes, high education has become more common, whereas the group with basic education, which was already the smallest in 2004, shrank further from approximately 20% to 12%.
Table 1.
Descriptive information on the number of individuals, group proportions, age‐adjusted mean yearly volume of consumption and prevalence of monthly heavy episodic drinking for groups with basic, intermediate and high education: Men, aged 25–79 years
| Education | Basic | Intermediate | High | Total | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Year | n | % | Mean volume | % HED | n | % | Mean volume | % HED | n | % | Mean volume | % HED | n |
| 2004 | 1428 | 19.1 | 5.66 | 48.1 | 3533 | 47.4 | 6.24 | 47.5 | 2467 | 33.1 | 6.88 | 44.4 | 7460 |
| 2005 | 1431 | 19.2 | 5.26 | 45.2 | 3429 | 46.1 | 5.93 | 46.9 | 2563 | 34.4 | 6.62 | 43.4 | 7446 |
| 2006 | 1475 | 19.8 | 5.47 | 44.4 | 3446 | 46.3 | 6.14 | 47.1 | 2494 | 33.5 | 6.80 | 42.9 | 7441 |
| 2007 | 1276 | 17.3 | 5.22 | 45.9 | 3444 | 46.6 | 5.93 | 46.4 | 2638 | 35.7 | 6.32 | 41.2 | 7386 |
| 2008 | 1244 | 16.9 | 5.34 | 43.4 | 3443 | 46.8 | 6.33 | 43.4 | 2642 | 35.9 | 6.67 | 38.0 | 7351 |
| 2009 | 1204 | 16.3 | 4.79 | 40.8 | 3398 | 45.9 | 5.95 | 41.4 | 2780 | 37.6 | 6.32 | 37.1 | 7401 |
| 2010 | 1123 | 15.3 | 4.63 | 42.2 | 3448 | 46.9 | 5.41 | 41.8 | 2767 | 37.7 | 5.93 | 38.2 | 7349 |
| 2011 | 1127 | 15.2 | 4.56 | 40.9 | 3315 | 44.8 | 5.30 | 42.0 | 2940 | 39.7 | 5.81 | 35.5 | 7400 |
| 2012 | 1037 | 14.1 | 4.91 | 47.9 | 3317 | 45.1 | 5.74 | 45.6 | 2969 | 40.4 | 6.28 | 38.1 | 7349 |
| 2013 | 1051 | 14.1 | 4.65 | 42.1 | 3384 | 45.3 | 5.75 | 43.1 | 2997 | 40.1 | 6.17 | 37.7 | 7468 |
| 2014 | 903 | 13.5 | 4.01 | 41.1 | 3032 | 45.5 | 4.90 | 41.6 | 2669 | 40.0 | 5.15 | 34.6 | 6670 |
HED, heavy episodic drinking.
Table 2.
Descriptive information on the number of individuals, group proportions, age‐adjusted mean yearly volume of consumption and prevalence of monthly heavy episodic drinking for groups with basic, intermediate and high education: Women, aged 25–79 years
| Education | Basic | Intermediate | High | Total | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Year | n | % | Mean volume | % HED | n | % | Mean volume | % HED | n | % | Mean volume | % HED | n |
| 2004 | 1529 | 20.0 | 1.92 | 22.4 | 3219 | 42.1 | 2.49 | 21.8 | 2859 | 37.4 | 3.31 | 18.6 | 7644 |
| 2005 | 1551 | 20.1 | 1.88 | 20.6 | 3179 | 41.2 | 2.55 | 21.9 | 2939 | 38.1 | 3.24 | 19.4 | 7710 |
| 2006 | 1521 | 19.9 | 1.99 | 21.2 | 3007 | 39.4 | 2.66 | 23.1 | 3075 | 40.3 | 3.32 | 20.1 | 7625 |
| 2007 | 1363 | 17.8 | 1.90 | 19.6 | 3029 | 39.6 | 2.61 | 19.9 | 3229 | 42.2 | 3.00 | 16.6 | 7654 |
| 2008 | 1295 | 17.0 | 1.82 | 19.6 | 3016 | 39.6 | 2.80 | 19.6 | 3270 | 42.9 | 3.15 | 16.2 | 7618 |
| 2009 | 1193 | 15.9 | 1.66 | 19.4 | 2955 | 39.5 | 2.82 | 19.8 | 3308 | 44.2 | 3.19 | 17.0 | 7489 |
| 2010 | 1178 | 15.8 | 1.68 | 20.1 | 2920 | 39.1 | 2.47 | 19.9 | 3351 | 44.8 | 2.98 | 17.5 | 7477 |
| 2011 | 1041 | 13.8 | 1.66 | 19.3 | 2831 | 37.6 | 2.40 | 20.1 | 3629 | 48.2 | 2.90 | 15.9 | 7535 |
| 2012 | 943 | 12.8 | 1.61 | 22.2 | 2715 | 36.9 | 2.44 | 20.6 | 3674 | 49.9 | 2.98 | 15.8 | 7361 |
| 2013 | 958 | 12.6 | 1.42 | 20.5 | 2656 | 35.1 | 2.51 | 21.5 | 3921 | 51.8 | 2.93 | 16.1 | 7576 |
| 2014 | 767 | 11.4 | 1.55 | 18.6 | 2342 | 34.9 | 2.44 | 18.9 | 3543 | 52.7 | 2.69 | 14.6 | 6719 |
HED, heavy episodic drinking.
Education‐specific trends in mean alcohol consumption
Tables 1 and 2 reveal a marked positive gradient across the SEP‐groups in mean yearly volume of consumption. That is, for both sexes, the high‐educated group drinks more than those with intermediate education, while the lowest consumption is recorded for those with basic education. The mean ratio between the consumption in the group with high and the group with basic education is 1.4 for men and 1.8 for women.
The time trends in the mean yearly volume of consumption are presented in Figure 1. As can be seen, there has been a gradual, continuous decline in the overall mean consumption, from 4.5 L in 2004 to 3.7 L in 2014; that is, a decrease by 18% (or 0.8 L). The decrease in consumption is reflected in all SEP‐groups, although to a varying degree. The largest decreases, ranging between approximately 1.3 and 1.7 L (22 and 29%), are found for the three male educational groups. The decline in consumption has been somewhat smaller among women, with the largest decrease (0.6 L, or 19%) among women with high educational level, and the lowest (0.1 L, or 2%) among women with intermediate educational level.
Figure 1.
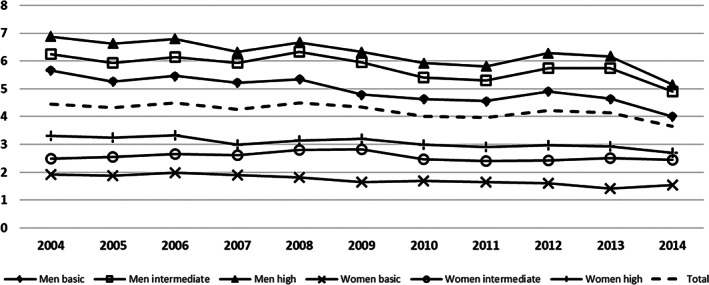
Trends in age‐adjusted yearly mean alcohol consumption (in litres of 100% alcohol) for the total population and by socioeconomic position groups, aged 25–79 years, 2004–2014.
The prevalence of HED shows a reversed, negative, gradient across the SEP‐groups, for both sexes (Tables 1 and 2), with the lowest prevalence found for the highly educated groups and the highest prevalence among the groups with intermediate and basic education. Similar to the trends in mean volume of consumption, the trends in prevalence of HED show a gradual decline across all SEP‐groups (Figure 2), with decreases ranging between 3 percentage points, (among women with intermediate educational level) and 10 percentage points (among men with high educational level).
Figure 2.
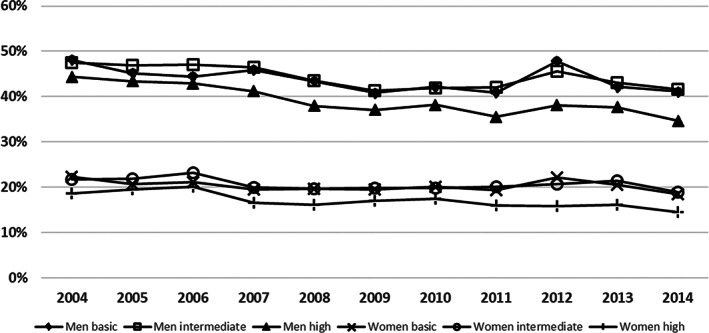
Trends in age‐adjusted prevalence of monthly heavy episodic drinking by socioeconomic position groups aged 25–79 years, 2004–2014.
Tests of collectivity of drinking
Figure 3 plots the logged yearly mean volume of consumption for each SEP‐group against the logged overall mean consumption for the corresponding year. As can be seen, the figure reveals a pattern of positive relationships that accords well with the synchronisation in drinking predicted from the collectivity hypothesis. This result is further strengthened by the estimates from the ordinary least‐squares regressions (Table 3), which reveal that the associations are significant for all groups, except for women with intermediate education (P = 0.081). Moreover, the magnitude of the association varies across the groups, and is strongest among the group with basic education for both sexes. The estimates imply that a 1% increase in overall mean consumption is associated with an approximately 0.6–1% increase in mean consumption among the three educational groups for men and a 0.64–1.4% increase among women.
Figure 3.
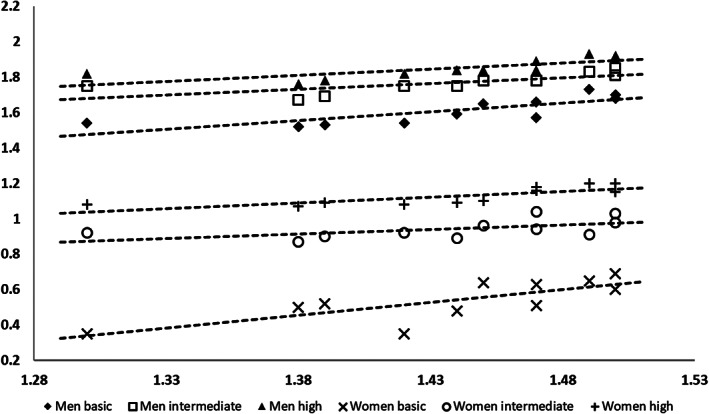
Age‐adjusted mean (logged) volume of alcohol consumption in six socioeconomic position groups aged 25–79 years (y‐axis), plotted against the overall (logged) mean alcohol consumption (x‐axis). Based on annual data 2004–2014.
Table 3.
Ordinary least‐squares regression models of the association (expressed as elasticity) between overall mean consumption (input variable) and mean consumption/prevalence of monthly heavy episodic drinking (outcome variables) in each of the SEP‐groups: Women and men aged 25–79 years
| SEP‐group | Mean volume | Prevalence HED | ||||
|---|---|---|---|---|---|---|
| B | SE | P | B | SE | P | |
| Men basic | 0.97 | 0.25 | 0.004 | 0.23 | 0.12 | 0.090 |
| Men intermediate | 0.64 | 0.20 | 0.010 | 0.25 | 0.10 | 0.038 |
| Men high | 0.67 | 0.02 | 0.006 | 0.37 | 0.12 | 0.014 |
| Women basic | 1.40 | 0.40 | 0.007 | 0.11 | 0.05 | 0.084 |
| Women intermediate | 0.47 | 0.24 | 0.081 | 0.12 | 0.06 | 0.062 |
| Women high | 0.64 | 0.17 | 0.005 | 0.18 | 0.07 | 0.027 |
HED, heavy episodic drinking; SEP, socioeconomic position.
Similar to our main analyses, increasing overall consumption is associated with a positive and collective displacement also in the prevalence of HED across all SEP‐groups (Figure 4). However, Table 3 reveals a reversed pattern in the magnitude of the associations for both sexes, with the highest estimates found for the highly educated groups, whereas the estimates for the groups with basic education are somewhat lower, and only marginally significant (P‐value for men = 0.090 and for women 0.084).
Figure 4.
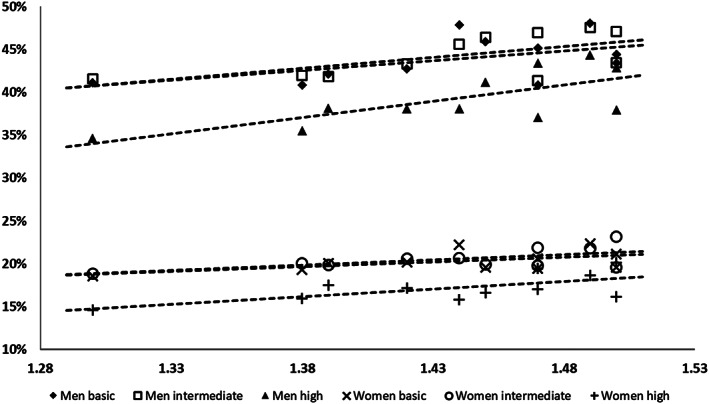
Age‐adjusted prevalence of monthly heavy episodic drinking in six socioeconomic position groups aged 25–79 years (y‐axis), plotted against the logged overall mean consumption (x‐axis). Based on annual data 2004–2014.
Discussion
This is the first study that applies Skog's approach to test whether changes in overall mean alcohol consumption tend to reflect collective shifts in drinking across different socioeconomic strata. Our findings suggest that Skog's notion of collectivity of drinking indeed is applicable across SEP‐groups. That is, during the period 2004 to 2014, yearly changes in overall mean consumption in Sweden are echoed in collective shifts in drinking across groups with basic, intermediate and high educational level. There were also indications that changes in overall mean consumption reflected collective shifts in the prevalence of HED across educational groups, although some groups did not quite conform to the expected pattern (men and women with basic education, and women with intermediate education). Moreover, while the magnitude of the associations for both average volume and HED differed somewhat in strength across the educational groups, they were clearly in the same, positive, direction. Our findings thus correspond to the notion of soft, rather than hard collectivity, as discussed by Holmes et al. [28].
The observed collective changes in drinking indicate that factors influencing consumption during the study period have had a similar effect across educational groups. According to Skog's theory, this could reflect an absence of strong social and cultural boundaries between educational groups in relation to drinking behaviour. However, while the study period saw gradually increased affordability of alcohol in Sweden [29, 30], no substantial alcohol policy initiative focusing on price and availability was undertaken. To further our understanding of under what circumstances the notion of collectivity of drinking applies across SEP‐groups, future studies should replicate our analyses on cases and study periods with more tangible changes in alcohol policy.
Moreover, our results do not support the hypothesis that the differential association between per capita consumption and alcohol‐related mortality across educational groups in Sweden, as reported in a recent study [17], may be explained by differences in consumption trajectories. Rather, our findings of a collectivity in drinking across educational groups suggest an explanation where a mechanism assumed to underlie the alcohol harm paradox—differential vulnerability—aggregate up to the population level. Recent studies have found that the alcohol harm paradox can largely be attributed to a differential vulnerability to the harmful effects of alcohol, so the same levels and patterns of drinking are associated with a higher risk of alcohol‐related harm in lower, compared to higher SEP‐groups [31, 32, 33]. When such differential vulnerability exists, changes in exposure that occur collectively, as found in the present study, will have a larger impact on the harm rates in more vulnerable groups, which in our case tend to be the more disadvantaged parts of the population [34]. Moreover, a recent systematic review concluded that up to 30% of the social gradient in alcohol‐related morbidity and mortality may be explained by a differential exposure to hazardous patterns of drinking across SEP‐groups [25]. In line with this, our finding of a negative social gradient in prevalence of monthly HED suggests that the differential effect of per capita consumption on alcohol‐related mortality, may in part be attributed to a higher prevalence of hazardous drinking patterns in low SEP‐groups.
Taken together, the results presented in this study and in Norström and Landberg [17] add a socioeconomic dimension to the evidence of a population‐level association between alcohol and related harm. That is, changes in per capita consumption tend to reflect collective shifts in drinking across SEP‐groups, which, together with differential vulnerability, may contribute to a social gradient in the association between per‐capita consumption and rates of alcohol‐related harm. These findings have important policy implications; given that changes in per capita alcohol consumption tend to have a larger impact on related harm among the more disadvantaged part of the population, policy measures that effectively regulate the total consumption of alcohol across different SEP‐groups will not only have the potential of decreasing rates of alcohol‐related harm, but may also reduce the social gradient of this outcome.
Strengths and limitations
Our analyses are based on a large nationally representative sample that has been collected monthly, using the same survey methodology, over a long period of time. This has provided us with a unique opportunity to analyse trends in drinking across SEP‐groups, minimising the risk that the results are artefacts of methodological changes. Moreover, as the recall period for the applied quantity and frequency scale only is 30 days, distorting memory effects are assumed to be smaller in our study than in studies using longer recall periods, for example, 12 months [35]. Still, some limitations of the study should be noted. The increasing non‐response rates may have affected the inclusion of heavy drinkers, which would lead to an overestimation of the temporal decrease in consumption. However, the coverage rate of the self‐reported volume of consumption, when compared to the estimated per capita alcohol consumption, has remained stable, at approximately 45% of the estimated per capita consumption [36], suggesting that this is not a significant problem in the present study. Lastly, marginalised heavy drinkers, for example, the institutionalised and the homeless, are probably over‐represented among the non‐responders, which limits the generalisability of our results.
Conclusions
The findings from this study, based on Swedish data for the period 2004–2014, suggest that changes in overall consumption are echoed as collective shifts in drinking across SEP‐groups with basic, intermediate and high educational level. Our findings thus provide support for including a socioeconomic dimension to Skog's theory of collectivity of drinking cultures.
Conflict of interests
The authors have no conflicts of interest.
Acknowledgements
This study was funded by the Swedish Research Council for Health, Working Life and Welfare (Forte) [dnr: 2017‐01769] and Systembolagets Research Council (Systembolagets Alkoholforskningsråd) [FO2017‐0084].
Jonas Landberg PhD, Associate Professor and Senior Lecturer, Björn Trolldal PhD, Researcher, Thor Norström PhD, Professor Emeritus.
References
- 1. Norström T, Ramstedt M. Mortality and population drinking: a review of the literature. Drug Alcohol Rev 2005;24:537–47. [DOI] [PubMed] [Google Scholar]
- 2. Bruun K, Edwards G, Lumio M et al. Alcohol control policies in public health perspective. Helsinki: Finnish Foundation for Alcohol Studies, 1975. [Google Scholar]
- 3. Edwards G, Anderson P, Babor T et al. Alcohol policy and the public good. Oxford: Oxford University Press, 1994. [Google Scholar]
- 4. Room R, Babor T, Rehm J. Alcohol and public health. Lancet 2005;365:519–30. [DOI] [PubMed] [Google Scholar]
- 5. Anderson P, Chisholm D, Fuhr DC. Effectiveness and cost‐effectiveness of policies and programmes to reduce the harm caused by alcohol. Lancet 2009;373:2234–46. [DOI] [PubMed] [Google Scholar]
- 6. Babor T, Caetano R, Casswell S et al. Alcohol: no ordinary commodity: research and public policy, 2nd edn. Oxford: Oxford University Press, 2010. [Google Scholar]
- 7. Rossow I, Mäkelä P, Kerr W. The collectivity of changes in alcohol consumption revisited. Addiction 2014;109:1447–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Skog O‐J. The collectivity of drinking cultures: a theory of the distribution of alcohol consumption. Br J Addict 1985;80:83–99. [DOI] [PubMed] [Google Scholar]
- 9. Raninen J, Leifman H, Ramstedt M. Who is not drinking less in Sweden? An analysis of the decline in consumption for the period 2004–2011. Alcohol Alcohol 2013;48:592–7. [DOI] [PubMed] [Google Scholar]
- 10. Norström T, Svensson J. The declining trend in Swedish youth drinking: collectivity or polarization? Addiction 2014;109:1437–46. [DOI] [PubMed] [Google Scholar]
- 11. Raninen J, Livingston M, Leifman H. Declining trends in alcohol consumption among Swedish youth—does the theory of collectivity of drinking cultures apply? Alcohol Alcohol 2014;49:681–6. [DOI] [PubMed] [Google Scholar]
- 12. Brunborg GS, Bye EK, Rossow I. Collectivity of drinking behavior among adolescents: an analysis of the Norwegian ESPAD data 1995‐2011. Nord Stud Alcohol Drugs 2014;31:389–400. [Google Scholar]
- 13. Schmidt L et al. Alcohol: equity and social determinants. Geneva: World Health Organization, 2009. [Google Scholar]
- 14. Mackenbach JP, Kulhánová I, Bopp M et al. Inequalities in alcohol‐related mortality in 17 European countries: a retrospective analysis of mortality registers. PLoS Med 2015;12:e1001909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Probst C, Roerecke M, Behrendt S, Rehm J. Socioeconomic differences in alcohol‐attributable mortality compared with all‐cause mortality: a systematic review and meta‐analysis. Int J Epidemiol 2014;43:1314–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Jones L, Bates G, McCoy E, Bellis MA. Relationship between alcohol‐attributable disease and socioeconomic status, and the role of alcohol consumption in this relationship: a systematic review and meta‐analysis. BMC Public Health 2015;15:400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Norström T, Landberg J. The link between per capita alcohol consumption and alcohol‐related harm in educational groups. Drug Alcohol Rev 2020;39:656–63. [DOI] [PubMed] [Google Scholar]
- 18. Skog O‐J. Commentary on Gmel & Rehm's interpretation of the theory of collectivity of drinking culture. Drug Alcohol Rev 2001;20:325–31. [Google Scholar]
- 19. Herttua K, Makela P, Martikainen P. Changes in alcohol‐related mortality and its socioeconomic differences after a large reduction in alcohol prices: a natural experiment based on register data. Am J Epidemiol 2008;168:1110–8 discussion 1126‐31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Helakorpi S, Makela P, Uutela A. Alcohol consumption before and after a significant reduction of alcohol prices in 2004 in Finland: were the effects different across population subgroups? Alcohol Alcohol 2010;45:286–92. [DOI] [PubMed] [Google Scholar]
- 21. Norström T, Romelsjö A. Social class, drinking and alcohol‐related mortality. J Subst Abuse 1998;10:385–95. [DOI] [PubMed] [Google Scholar]
- 22. Crombie IK, Precious E. Changes in the social class gradient of cirrhosis mortality in England and Wales across the 20th century. Alcohol Alcohol 2011;46:80–2. [DOI] [PubMed] [Google Scholar]
- 23. Budhiraja M, Landberg J. Socioeconomic disparities in alcohol‐related mortality in Sweden, 1991–2006: a register‐based follow‐up study. Alcohol Alcohol 2016;51:307–14. [DOI] [PubMed] [Google Scholar]
- 24. Gomes de Matos E, Kraus L, Pabst A, Piontek D. Does a change over all equal a change in all? Testing for polarized alcohol use within and across socio‐economic groups in Germany. Alcohol Alcohol 2015;50:700–7. [DOI] [PubMed] [Google Scholar]
- 25. Probst C, Kilian C, Sanchez S, Lange S, Rehm J. The role of alcohol use and drinking patterns in socioeconomic inequalities in mortality: a systematic review. Lancet Public Health 2020;5:E324–32. [DOI] [PubMed] [Google Scholar]
- 26. Trolldal B, Leifman H. Hur mycket dricker svensken? Registrerad och oregistrerad alkoholkonsumtion 2001–2014 [How much does the Swede drink? Registered and unregistered alcohol consumption 2001–2014]. Stockholm: Centralförbundet för alkohol‐ och narkotikaupplysning, Rapport nr 152, 2015. [Google Scholar]
- 27. Williams R. Using Stata's margins command to estimate and interpret adjusted predictions and marginal effects. Stata J 2012;12:308–31. [Google Scholar]
- 28. Holmes J, Ally AK, Meier PS, Pryce R. The collectivity of British alcohol consumption trends across different temporal processes: a quantile age–period–cohort analysis. Addiction 2019;114:1970–80. [DOI] [PubMed] [Google Scholar]
- 29. Herttua K, Östergren O, Lundberg O, Martikainen P. Influence of affordability of alcohol on educational disparities in alcohol‐related mortality in Finland and Sweden: a time series analysis. J Epidemiol Community Health 2017;71:1168–76. [DOI] [PubMed] [Google Scholar]
- 30. Ramstedt M. Change and stability? Trends in alcohol consumption, harms and policy: Sweden 1990–2010. Nord Stud Alcohol Drugs 2010;27:409–24. [Google Scholar]
- 31. Katikireddi SV, Whitley E, Lewsey J, Gray L, Leyland AH. Socioeconomic status as an effect modifier of alcohol consumption and harm: analysis of linked cohort data. Lancet Public Health 2017;2:e267–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Christensen HN, Diderichsen F, Hvidtfeldt UA et al. Joint effect of alcohol consumption and educational level on alcohol‐related medical events. Epidemiology 2017;28:872–9. [DOI] [PubMed] [Google Scholar]
- 33. Thern E, Landberg J. Understanding the differential effect of alcohol consumption on the relation between socio‐economic position and alcohol‐related health problems: results from the Stockholm public health cohort. Addiction 2020. [Epub ahead of print]. 10.1111/add.15213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Diderichsen F, Hallqvist J, Whitehead M. Differential vulnerability and susceptibility: how to make use of recent development in our understanding of mediation and interaction to tackle health inequalities. Int J Epidemiol 2018;48:268–74. [DOI] [PubMed] [Google Scholar]
- 35. Stockwell T, Donath S, Cooper‐Stanbury M, Chikritzhs T, Catalano P, Mateo C. Under‐reporting of alcohol consumption in household surveys: a comparison of quantity–frequency, graduated–frequency and recent recall. Addiction 2004;99:1024–33. [DOI] [PubMed] [Google Scholar]
- 36. Raninen J. Ingen dricker som Svensson: om svenska befolkningens dryckesvanor [Nobody drinks like Svensson: about the drinking habits of the Swedish population]. Stockholm: Centralförbundet för alkokhol‐och narkotikaupplysning, Rapport nr 153, 2015. [Google Scholar]