

Abstract
Suicide is a leading cause of death among youth globally. In this critical interpretive synthesis, we examined literature on resiliency factors and suicidality. Systematic searches identified 474 articles, 37 of which were included. Results revealed internal (positive self‐appraisal, zest for life, personal traits, and coping skills) and external factors (social support system and inclusive environments) contribute to resilience among youth, with age, sex and gender, and Indigenous identity as important intersecting considerations. Findings validated fostering resilience as primary suicide prevention among youth, with little explanation for how these factors may work to protect youth from suicidality. Continued research in this area requires a focus on how to promote resilience at the community and systems levels.
Suicide is the second leading cause of death among youth globally and in Canada, and is a major cause of preventable death for all ages (Gallagher & Miller, 2018; Navaneelan, 2012; World Health Organization [WHO], 2019). Suicide deaths among youth are trending upwards, with a disconcerting number of children younger than 13 years of age dying by suicide each year (Gallagher & Miller, 2018; Navaneelan, 2012; Statistics Canada, 2012). Suicide‐related statistics, often under‐reported and inconsistent across jurisdictions, limit both national and international comparisons and access to high quality, current data to inform policies and interventions (Canadian Council of Child & Youth Advocates [CCCYA], 2019; Little, Roche, Chow, Schenck, & Byam, 2016).
Studying suicide and its risk factors is further complicated by the challenges of retrospective research on the trajectories leading to suicide, particularly for youth who have died by suicide without previously recorded or identified risks or warning signs. A greater focus on supporting resiliency (i.e., the ability to recover from challenges faced in everyday life) as a population‐level youth suicide intervention is promising (Caldwell, 2008; Flouri, 2005; Malone et al., 2000). Responsive research in this field must address intersecting social factors for a better understanding of resilience, and its role in suicide prevention. The purpose of this paper is to report on the findings from a systematic literature review to elucidate the role of resiliency in youth suicide prevention.
A recent review by Gallagher and Miller (2018) looked at interactions between protective factors and risk factors related to suicide outcomes to inform a proposed ecological model of resilience to suicidal outcomes in youth. Based on their findings, the authors called for suicide prevention efforts for youth to move beyond risk reduction to include the promotion of resilience for youth through the incorporation of multi‐domain, multi‐level suicide prevention programs (Gallagher & Miller, 2018). Risk factor research often strips context and the dynamics of human experiences and social conditions to produce individual‐level, static, and unitary variables (White, 2016). Yet, multiple intersectionalities are known to influence rates of suicide among youth, including sex, gender, social inclusion, and Indigenous identity. When referring to Indigenous identity in this paper, the authors have not identified a specific group of Indigenous peoples and respectfully use the term Indigenous to acknowledge Indigenous peoples’ international legal rights under the UN Declaration of Rights of Indigenous Peoples.
Deaths due to suicide are twice as common among male adolescents as among females, and LGBTQ youth face increased risk of suicide (Gallagher & Miller, 2018; Little et al., 2016; Soor et al., 2012; Veale, Watson, Peter, & Saewyc, 2017). Suicide rates for First Nation youth in Canada are five to seven times higher than non‐Indigenous youth, and Inuit youth have the highest suicide rates in the world (Government of Canada, 2019). These intersecting influences, in turn, interact with person‐level factors to shape differences in resilience and protective factors among youth and emerging adults (Heisel & Flett, 2008; Johnson, Gooding, Wood, & Tarrier, 2010; Roy, Sarchiapone, & Carli, 2007). Given these differences in risk profiles and the urgency of prevention research, there is a need to better understand resilience in the context of suicide prevention across a spectrum of social positionalities and risk profiles to inform population‐level interventions to promote youth resilience to suicide.
Resilience is understood as the ability to recover from challenges faced in everyday life (Wesley‐Esquimaux, 2009) through adaptation (Kirmayer, Dandeneau, Marshall, Phillips, & Williamson, 2012). Sometimes described as a measurement of hardiness (Kirmayer et al., 2012), it involves dynamic protective processes that help people navigate adversity across the lifespan (Ungar, 2011). Resilience theory focuses on strengths rather than deficits and on understanding healthy development in spite of risk exposures (Fergus & Zimmerman, 2005). Rather than a static trait or quality, it can vary with context, population, risk, protective factor, and the potential outcome(s) of the relevant risk exposure (Fergus & Zimmerman, 2005).
Resilience is theorized as a multitude of complex relationships and interactions between protective factors, risk factors, and outcomes (O’Leary, 1998; Zimmerman, Bingenheimer, & Notaro, 2002). It involves both positive internal factors, referred to as assets (such as competence, self‐efficacy, and coping skills) and external factors, referred to as resources (such as support, mentorship, and promotion) that foster positive development (Fergus & Zimmerman, 2005; Kirmayer et al., 2012). Importantly, while positive youth development in response to exposure to a risk is considered a resilient outcome, the process of overcoming the risk is resilience (Benson, Scales, & Syvertsen, 2011; Fergus & Zimmerman, 2005). Resilience therefore functions in many ways to enable prevention, including to (1) decrease risk and chain reactions that can follow risk; (2) develop and maintain self‐efficacy and self‐identity; and (3) enhance opportunities for change, increased success, and decreased risk exposures (O’Leary, 1998; Ungar, 2011).
Despite decades of extensive research exploring youth suicidal behavior and risk profiles for specific at‐risk youth populations, there remains a dearth of research evidence related to the experiences of youth who died by suicide yet showed no previous identifiable risks or warning signs. Given the scope and scale of youth suicide in Canada, there is an urgent need to understand how to engage in primary suicide prevention and foster resilience for all youth, regardless of risk profile. In response to this need, the Community‐Led Actions for Resilience Important Throughout Youth Project (CLARITY), based in Kelowna, British Columbia, Canada, was mobilized as a community‐driven program of research focused on primary suicide prevention. CLARITY aims to create evidence‐informed, community‐based actions to promote resilience among youth. The CLARITY advisory group guides the initiative through collaborative leadership, contributing at each stage of the research process, and includes people with lived experience, researchers, local community organizations that support youth mental health, representatives from the local police and health services, health professionals serving youth, and school district administrators.
Through process of consensus, the CLARITY advisory group looked to the literature to identify what is currently known about promoting resilience among youth to prevent suicide, then based on their expertise and needs helped delineate the research question (i.e., what, if any, identified factors are associated with resiliency and youth suicide prevention, and in what ways?) and set parameters for the literature search strategy. In alignment with these objectives, this systematic literature review was conducted to inform how best to support the research program (designed and implemented with leadership from an existing, local youth advisory group) and to provide guidance on next steps. Upon completion of the review, the research team will begin the next phase, which is to validate and extend this review’s findings through deliberative dialogues with local youth—to center and privilege their voices and perspectives on the topic. Data collected through these dialogues will clarify future directions for appropriately and sustainably moving forward. During this phase, youth representation will be added to the CLARITY advisory group.
A theoretical framework and integrative approach was identified as most appropriate to engage this systematic literature review and represent evidence‐informed results. Critical interpretive synthesis is a systematic approach to reviewing literature that applies qualitative analysis to a systematically selected body of literature, where the body of literature becomes the data set for analysis (Dixon‐Woods, Agarwal, Jones, Young, & Sutton, 2005). In addition to resiliency theory, this critical interpretive synthesis was informed by an integration of a health equity approach and intersectionality (Table 1). According to Whitehead and Dahlgren (2006), “equity in health implies that ideally everyone could attain their full health potential and that no one should be disadvantaged from achieving this potential because of their social position or other socially determined circumstance” (p. 5). Using a health equity approach draws critically reflective attention to systems‐level drivers of inequity and the equity implications of any initiative (Pauly, Shahram, van Roode, Strosher, & MacDonald, 2018; Plamondon & Bisung, 2019). Intersectionality extends this approach further by explicitly drawing attention to the ways human beings are shaped by the interaction of different social locations in the context of connected systems and structures of power (Hankivsky, 2014).
Table 1.
Definition of Key Terms
| Health equity approach | According to Whitehead and Dahlgren (2006), “equity in health implies that ideally everyone could attain their full health potential and that no one should be disadvantaged from achieving this potential because of their social position or other socially determined circumstance” (p. 5). Using a health equity approach invites consideration of the social, economic, and environmental conditions that generate differences in health outcomes among populations, with critically reflective attention to systems‐level drivers of inequity and the equity implications of any initiative (Pauly et al., 2018; Plamondon & Bisung, 2019). Understanding these conditions requires engaging in dialogue with diverse groups of people at systems levels (Pauly et al., 2018) and using critically reflective considerations about equity implications of any initiative (Plamondon & Bisung, 2019). |
| Intersectionality | Directs attention to the ways human beings are shaped by the interaction of different social locations in the context of connected systems and structures of power (Hankivsky, 2014). |
| Resilience Theory | Focuses on strengths rather than deficits and on understanding healthy development in spite of risk exposures (Fergus & Zimmerman, 2005). Rather than a static trait or quality, it can vary with context, population, risk, protective factor and the potential outcome(s) of the risk exposure (Fergus & Zimmerman, 2005). |
Method
Using critical interpretive synthesis methodology (Dixon‐Woods et al., 2005), we formulated an iterative process to (1) familiarize ourselves with the literature; (2) develop and refine inclusion and exclusion criteria; (3) select relevant studies to review; and (4) qualitatively analyze the theme‐selected studies. Guided by PRISMA guidelines (Moher, Liberati, Tetzlaff, & Altman, 2009), the review began with the large body of literature identified through a preliminary search. After a general reading of the kinds of articles retrieved, SS and MS refined our search strategy (Table 2) with an intention to access the broadest range of eligible articles over the previous decade related to resilience factors and youth suicide.
Table 2.
Search Strategy
| Databases | Terms | Inclusion | Exclusion |
|---|---|---|---|
|
Academic Search Complete Academic Search Premier CINAHL Complete ERIC MEDLINE PsycARTICLES PsycINFO PsycExtra Social Work Abstracts Google Scholar |
Resilien * OR Prevent * OR Protect * AND Suicid * AND youth OR young OR young adult OR children OR adolescents OR teens OR early years OR infant/baby OR toddler OR development OR Perinatal OR prenatal OR maternal OR pregnan * AND Australia OR Canada OR England OR Ireland OR New Zealand OR Scotland OR United Kingdom OR United States OR Wales |
Resilience OR Protective OR Preventive factors AND Peer‐reviewed journal AND Range: 2008–2018 AND Age range 0–25 years OR have analyzed age groups within age range 0–25 years AND English language |
Locations/countries not listed in search terms OR Homicide associated with suicide OR Literature review OR Gray literature |
Boolean search mode words are searched exactly as they are typed. Use the asterisk wildcard character (*) to include alternative forms of words, plurals, etc.
Selection Criteria
Our selection criteria focused on identifying articles that had been published from 2008 to 2018 had a specific focus on youth (i.e., included youth 25 and younger as a distinct population of focus), and included a focus on resilience, prevention and or protective factors related to suicide. We limited our search to English language articles from Australia, Canada, England, Ireland, New Zealand, Scotland, United Kingdom, and the United States. The limitations set were designed to encompass the experiences of populations or groups of peoples (identified and or defined by their shared social, economic, demographic, geographic, and or other levels of stratification) with resilience and suicidality, including Indigenous perspectives on resilience. Although there is great diversity and variation among Indigenous peoples in and within these countries, on account of historic and contemporary colonization practices, as well as imposed misclassifications, many Indigenous people in these countries share a common experience of the loss of land, language, and socio‐cultural resources (Shahram et al., 2017). While Indigenous peoples have demonstrated exceptional resilience in the face of systemic racism, discrimination and social exclusion, many populations or groups face similar population health experiences and outcomes on account of these shared contexts (Shahram et al., 2017).
Data Extraction and Analysis
The process of identifying articles for inclusion began with screening of titles and abstracts by SS and MS followed by review of full text articles (SS and MS). As screening progressed, inclusion and exclusion criteria were refined, and the final criteria as detailed in Figure 1 were applied to guide the selection of articles for inclusion. (SS, MS, SB‐D, and KP) engaged in third and fourth readings of selected articles focused on extracting descriptive data (study and population characteristics; presence of sex and or gender analysis; focus on Indigenous populations). SS, MS, SB‐D, and KP, through iterative content (Schreier, 2014) and constant comparative analysis (Glaser, 2008; Mays, Pope, & Popay, 2005), then explained, interpreted and grouped resiliency factors associated with suicidality (including suicidal ideation, attempts and death by suicide) under two overarching themes of assets and resources, in keeping with resiliency theory terminology (Fergus & Zimmerman, 2005). Given the variability in definitions and outcome measurements, and the authors’ goal to inform population‐level primary prevention efforts, we purposefully left this term, suicidality, as broad as possible to capture all potential resiliency factors related to suicide risk among youth. The initial extraction was informed by the CLARITY advisory team’s identified needs for understanding the literature. Preliminary findings were reviewed by all authors (SS, MS, SB‐D, MF, TK, and KP), who separately categorized the findings and then came back together to discuss and validate the main resiliency factors identified. This analysis was then shared with the CLARITY advisory team for further feedback and input before being finalized.
Figure 1.
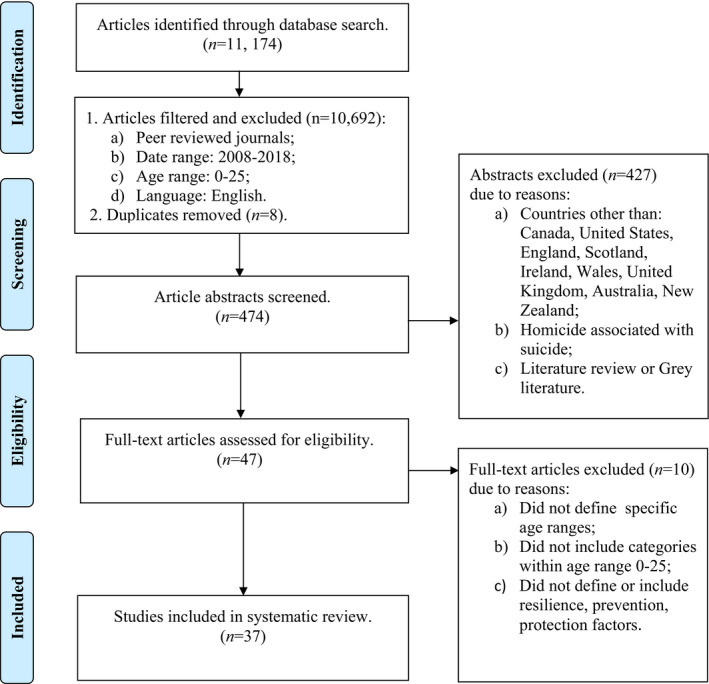
PRISMA 2009 flow diagram. From: Moher et al. (2009). For more information, visit www.prisma‐statement.org
Results
Our preliminary search identified 11,174 articles for initial screening, of which 474 full‐text articles were selected for in‐depth screening against inclusion and exclusion criteria (Figure 1). Thirty‐seven articles were included in the sample, including 27 primary research studies and 10 secondary data analyses. The majority of these studies (n = 33) used validated measures and scales to gather data and were conducted in the United States (n = 22); sample sizes ranged from nine to over 150,000 participants. Two studies were mixed‐methods, and two studies were qualitative. Twenty‐six studies included some type of sex and or gender analysis and eight studies included Indigenous youth as a discrete population. Data collection related to sex, gender, and sexual orientation was inconsistent among the studies, with sex and gender often being described as the same and sometimes conflated with sexual orientation. Details of each study are summarized in Table 3.
Table 3.
Study Characteristics
| Study | Location | Population | Sample | Study Objective(s) |
|---|---|---|---|---|
| Armstrong and Manion (2015) | Canada | Students, 13–19 years old, attending from 3 urban/2 rural schools | 813 | Highlight differing patterns of risk factors and protective factors. |
| Blalock et al. (2015) | United States | Undergrad students, mean age 20 years old | 209 | Examine if grit buffered the relationship between negative life events and suicidal ideation. |
| Borowsky et al. (2013) | United States | Students in grades 6, 9, 12 | 130,908 | Identify risk and protective factors associated with thinking about or attempting suicide among youth involved in verbal and social bullying. |
| Brennan et al. (2017) | United States | Individuals, aged 19 + years old, who self‐identify differently than their biological sex | 83 | Use gender minority stress model to investigate role of gender‐related stressors and resilience factors on mental health outcomes (depression, anxiety, and suicidality). |
| Bureau et al. (2012) | Canada | High school and college students, mean age 16 years old | 326 | Examine (a) self‐determination as a protective factor against negative life events on suicide ideation; (b) if highly self‐determined adolescents’ negative life events have weaker impact on hopelessness and suicide ideation than for non‐self‐determined adolescents. |
| Burke et al. (2016) | United States | Adolescents, 12–13 years old, and their mother | 324 | Examine the impact of cognitive vulnerabilities, as well as protective factors, for suicide ideation among adolescents over 2 years during their transition to mid‐adolescence. |
| Cha and Knock (2009) | United States | Individuals, 12–19 years old, with recent history of suicidal ideation or attempts or no history | 54 | Determine whether emotional intelligence decreases likelihood of suicidal ideation and attempts among those at risk. |
| Collins et al. (2016) | Australia |
Undergraduate students mean age 19 years old |
Study 1: 92 Study 2: 52 |
Examine a potential role for resilience within framework of interpersonal theory. |
| Collinshaw et al. (2016) | United Kingdom | parents with depression and their child, aged 9–17 years old |
331 families |
Identify protective factors that predict sustained good mental health in adolescents with a parent who has depression and to test whether these contribute beyond what is explained by parent illness severity. |
| Cwik et al. (2015) | United States | WMAT Reservation residents, aged 10–19 years old | 71 | Seek (a) knowledge from Apache adolescents who attempted suicide about potential risk and protective factors; and (b) data to develop suicide prevention and intervention strategies. |
| Eisenberg et al. (2017) | United States | Students in grades 5, 8, 9, 11 | 81,885 | Determine prevalence of transgender/gender nonconforming adolescents (TGNC) identity among youth and how does prevalence differ across demographic characteristics. |
| Foster et al. (2017) | United States | At risk youth, 12–15 years old, urban pediatric ED or urgent care clinic | 224 | Understand whether/to what extent specific types of connectedness are beneficial for youth characterized by two specific categories of risk factor (a) social challenges; and/or (b) residence in an underserved urban community with high rates of unemployment, poverty, and crime. |
| Fraser et al. (2015) | Canada | Inuit youth, 15–24 years old | 305 | Assess the prevalence of suicide ideation and attempts among Inuit youth, 10 years after two previous studies completed with population; explore potential risk and protective factors for suicide attempts as a function of gender. |
| Galligan et al. (2010) | United States | Undergraduate male students, 18–24 years old | 394 | Examine effects of gender role conflict on resilience, especially as linked to suicidal propensity, in adolescent and emerging adult males. |
| Harrison et al. (2014) | Australia | Undergraduate students, mean age 20 years old | 408 | Examine whether the d/sIAT (death/suicide implicit association test) reflects an individual's desire to die or a diminished desire to live and whether the predictive utility of implicit cognition is mediated by life‐oriented beliefs. |
| Hatzenbuehler (2011) | United States | Students in grade 11 | 31,582 | Examine environmental correlates of suicide attempts among LGB youth. Social environment measurement included (a) proportion of same‐sex couples; (b) Democrats; (c) schools with gay‐straight alliances; (d) schools with anti‐bullying policies specific to LGB students; and (e) schools with anti‐discrimination policies that included sexual orientation. |
| Hopkins et al. (2014) | Australia | Australian Aboriginal youth, 12–17 years old | 1,021: Male 510 Female 511 | Identify factors that uniquely protect psychosocial development within high and low family‐risk exposed youth. |
| Johnson et al. (2010) | United Kingdom | Undergraduate students, mean age 19 years old |
78: Male 13 Female 65 |
Explore whether positive self‐appraisals buffered individuals from suicidality in the face of stressful life events. |
| Kelley et al. (2018) | United States | Residents of American Indian reservation (Montana), 15–24 years old |
100: Male 33 Female 67 |
Highlight efforts of American Indian community to prevent suicide using public health approach framework. |
| Kidd and Shahar (2008) | Canada/United States | Homeless youth, 12–24 years old | 208 | Examine the protective role of self‐esteem, social involvement, and secure attachment among homeless youth. |
| Kleiman et al. (2013) | United States | College students, mean age 20 years old | 209 | Examine if gratitude and grit as factors synergistically confer resiliency to suicide by increasing meaning in life. |
| Kleiman and Beaver (2013) | United States | Undergraduate students, mean age 21 years old |
Base 670 f/up 585 |
Assess meaning in life as a prospective predictor of suicidal ideation and a retrospective predictor of suicide attempt status. |
| Kleiman et al. (2012) | United States | Undergraduate students, mean age 20 years old | 209 | Determine if enhancing attributional style would buffer the relationship between depressive symptoms and suicidal ideation. |
| Lamis and Lester (2013) | United States | Undergraduate students, mean age 19 years old | 994 | Compare the correlates and predictors of suicidal ideation for men and women at a southwestern university. |
| Lester (2017) | United States | Students in grade 9–12 |
152,858 SI 138,690 SA |
Study whether participation in sports has a protective impact on suicidal behavior (SI = suicide ideation; SA = attempted suicide) in students across 1991–2011. |
| Matel‐Anderson and Bekhet (2016) | United States | Caucasian psychiatric nurses | 9 | Explore resilience in adolescents who survived a suicide attempt from perspective of nurses. |
| Murphy (2014) | United States | Students in grades 8, 10, 12 | 10,672 | Identify dissimilarities in predictors of suicide ideation across the rural/urban threshold, assuming ideation is one of the most important predictors of suicide. |
| Mustanski and Liu (2013) | United States | LGBT youth, 16–20 years old | 248 | Examine general and lesbian, gay, bisexual and transgender (LGBT) specific risk and protective factors for suicide attempts in ethnically diverse sample. |
| Nagra et al. (2016) | United Kingdom/Australia | Individuals, 16 + years old (mean age 22–24 years old) reported self‐harm | 323 | Extend the empirical evidence of potential psychological risk and protective factors of suicidality in a population with history of self‐harm. |
| Peter and Taylor (2014) | Canada | University students (6% LGBTQ), mean age 20 years old | 1,200 | Examine suicidal behavior between LGBTQ and non LGBTQ university students to investigate risk and protective factors in prediction of suicidality. |
| Philip et al. (2016) | United States | Yup'ik Alaska Native youth, 12–19 years old | 57 | Describe the youth social networks of rural Yup'ik Alaska Native community in order to evaluate the extent to which network statistics are predictive of protective factors. |
| Taliaferro and Muehlenkamp (2014) | United States | Students in grade 9 and 12 | 70,772 | Address gaps in epidemiological research on suicidality among adolescents using a population‐based sample of high school students. |
| Taliaferro and Muehlenkamp (2017) | United States | Students in grades 5, 8, 9, 11 | 77, 758 | Investigate differences in prevalence of repetitive nonsuicidal self‐injury (NSSI), suicidal ideation and suicide attempt among youth identified as bisexual, gay, lesbian, questioning. |
| Teevale et al. (2016) | New Zealand | Pacific New Zealand students, 12–17 years old | 1,445 | Address key gaps in literature and focus on a particular youth group with previously recorded high risk of suicidal behavior. |
| Veale, Peter, et al. (2017) | Canada | Youth Trans, genderqueer, or with gender and body not matched, 14–25 years old | 923 | Examine impact of stressors and protective factors on mental health of transgender adolescents and young adults. |
| Whitaker et al. (2016) | United States | Students in grade 9, 11 identifying as lesbian, gay or bisexual | 356 | Understand whether school‐based protective factors are associated with decreased suicidal ideation for LGB adolescents. |
| Woodford et al. (2018) | United States | College students LBGQ/trans, 18 + years old | 778 | Advance knowledge of the risk and protective factors related to LGBTQ students' mental health. |
All the studies reviewed in this critical interpretive synthesis supported the role of resilience in reducing risk of suicidality. Resilience themes are grouped as either assets (derived from within the individual) or resources (derived from the individual’s interaction with their external environment). Six of the reviewed studies included both assets and resources related to resilience. Table 4 describes categories under each theme with wording extracted from the studies, while Table 5 summarizes which studies had findings related to each category. Considerations related to the interactions between these themes, as well as to sex and gender and to Indigenous‐specific resiliency factors, are also reviewed following the description of each theme.
Table 4.
Themes: Protective Factors Potentially Contribute to Resilience Against Suicidality
| Theme | Category | Subcategory (factors as defined by literature) |
|---|---|---|
| Assets for Resilience | Positive self‐appraisal |
|
| Zest for Life |
|
|
| Coping Skills |
|
|
| Theme | Category |
Subcategory (factors as defined by literature) |
| Resources for Resilience | Social Support System |
|
| Inclusive Environments |
|
Assets for Resilience: defined internal sources from within an individual. Resources for Resilience: defined as external sources influencing an individual’s interactions with their environment.
Gender Identity specific.
Indigenous overlap.
Gender Identity overlap.
Indigenous specific.
Table 5.
Resilience Themes and Categories Identified Across Studies
| Study | Resilience themes | ||||
|---|---|---|---|---|---|
| Assets | Resources | ||||
| Positive self‐appraisal | Zest for life | Coping skills | Social support network | Inclusive environments | |
| Armstrong and Manion (2015) | √ | √ | |||
| Blalock et al. (2015) | √ | ||||
| Borowsky et al. (2013) | √ | √ | √ | √ | |
| Brennan et al. (2017) | √ | √ | |||
| Bureau et al. (2012) | √ | ||||
| Burke et al. (2016) | √ | ||||
| Cha and Knock (2009) | √ | ||||
| Collins et al. (2016) | √ | ||||
| Collinshaw et al. (2016) | √ | √ | |||
| Cwik et al. (2015) | √ | √ | √ | ||
| Eisenberg et al. (2017) | √ | √ | √ | ||
| Foster et al. (2017) | √ | ||||
| Fraser et al. (2015) | √ | √ | |||
| Galligan et al. (2010) | √ | √ | √ | √ | √ |
| Harrison et al. (2014) | √ | ||||
| Hatzenbuehler (2011) | √ | ||||
| Hopkins et al. (2014) | √ | √ | √ | ||
| Johnson et al. (2010) | √ | √ | √ | ||
| Kelley et al. (2018) | √ | √ | |||
| Kidd and Shahar (2008) | √ | ||||
| Kleiman et al. (2013) | √ | ||||
| Kleiman and Beaver (2013) | √ | √ | |||
| Kleiman et al. (2012) | √ | ||||
| Lamis and Lester (2013) | √ | √ | |||
| Lester (2017) | √ | ||||
| Matel‐Anderson and Bekhet (2016) | √ | √ | √ | ||
| Murphy (2014) | √ | ||||
| Mustanski and Liu (2013) | √ | ||||
| Nagra et al. (2016) | √ | ||||
| Peter and Taylor (2014) | √ | √ | √ | ||
| Philip et al. (2016) | √ | √ | |||
| Taliaferro and Muehlenkamp, 2014 | √ | √ | √ | ||
| Taliaferro and Muehlenkamp, 2017 | √ | √ | |||
| Teevale et al. (2016) | √ | √ | √ | ||
| Veale, Peter, et al. (2017) | √ | ||||
| Whitaker et al. (2016) | √ | √ | |||
| Woodford et al. (2018) | √ | √ | |||
Assets for Resilience
Thirty‐one of the included studies (84%) reported on assets for resilience (Table 5). Three subthemes emerged related to this internal construct: positive self‐appraisal, zest for life, and coping skills.
Positive self‐appraisal
Positive self‐appraisal was the most frequently identified asset. Twenty studies identified the belief in one’s ability to conceptualize and succeed in situations or tasks and having a strong sense of self (including internal assets and agency, high self‐esteem, and a sense of self‐determination and or cultural identity) as protective against suicidality (Table 5). For example, Kidd and Shahar (2008) found high self‐esteem was associated with perceived resilience against loneliness, feeling trapped, suicidal ideation, subjective health status, and substance abuse behavior among homeless youth. Self‐esteem appeared to buffer the impact of fearful attachment on loneliness, and youth identified self‐resources of efficacy, resourcefulness, intelligence, personal strength, and wariness of others (in the context of living in unstable and unsafe social environments) as important for their resilience.
Some of the studies described protective factors related to self‐efficacy and suicide. These factors include (1) participating in a traditional lifestyle or traditional activities (for Indigenous youth) (Cwik et al., 2015; Fraser, Geoffroy, Chachamovich, & Kirmayer, 2015; Kelley, Restad, & Killsback, 2018; Philip, Ford, Henry, Rasmus, & Allen, 2016); (2) demonstrating communal mastery (i.e., seeing oneself as able to achieve goals by virtue of being attached to others) (Philip et al., 2016); (3) positive self‐appraisals in the face of stressful life events (Johnson et al., 2010) or a sense of pride (Brennan et al., 2017); (4) a high sense of self‐determination (Bureau, Genevieve, Vallerand, Rousseau, & Otis, 2012); and (5) participating in physical activity and sports (Borowsky, Taliaferro, & McMorris, 2013; Collinshaw et al., 2016; Lester, 2017; Taliaferro & Muehlenkamp, 2014). Bureau et al. (2012) found, among French‐speaking high school and college students (N = 682) exposed to negative life events and or experiencing feelings of hopelessness, those with high perceived self‐determination (i.e., people who experience a sense of freedom to do what is interesting, personally important, and vitalizing) appear to have decreased suicide ideation. Finally, in a study with self‐identified LGBTQ college students (N = 776), Woodford et al. (2018) found higher scores on a brief resilience scale (i.e., higher belief in one’s ability to bounce back after adversity) were significantly associated with decreased adjusted odds of reporting suicide attempts.
Zest for life
Twelve studies reported some form of positive engagement with life as a protective factor. Collins, Best, Stritzke, and Page (2016) defined zest for life as “a will to live that manifests as a sense of engagement with and positive outlook on life” (p.705). Studies operationalized this construct as young people (1) having an interest or positive engagement in life (Collins et al., 2016; Harrison, Stritzke, Fay, Ellison, & Hudaib, 2014; Lamis & Lester, 2013; Peter & Taylor, 2014); (2) searching for meaning in life (Johnson et al., 2010; Kleiman, Adams, Kashdan, & Riskind, 2013; Kleiman & Beaver, 2013; Lamis & Lester, 2013; Peter & Taylor, 2014); (3) having reasons for living (Peter & Taylor, 2014); (4) having an enhanced attribution style (EAS) (Kleiman, Miller, & Riskind, 2012); (5) manifesting an internalized motivational drive for achievement (Galligan, Barnett, Brennan, & Israel, 2010); (6) exhibiting a level of grit (Blalock, Young, & Kleiman, 2015; Harrison et al., 2014; Kleiman et al., 2013); (7) practicing mindfulness and gratitude (Collins et al., 2016; Harrison et al., 2014; Kleiman et al., 2013; Kleiman & Beaver, 2013); and (8) engaging in future planning (Matel‐Anderson & Bekhet, 2016). Collins et al. (2016) argued that this will to live must be overcome before a person can act on their desire for death. They found that among undergraduate students (N = 92), individual differences in zest for life moderated the predicted effects of elevated burdensomeness and diminished belongingness on impaired persistence.
Harrison et al. (2014) similarly found having strong survival beliefs was an asset as determined by a subscale of the Reasons for Living Inventory. The subscale items included agreement with life‐oriented belief statements like “I have a desire to live,” and “I care about myself enough to live” (p. 834). Such beliefs mediated the relationship between the Death Suicide Implicit Association Test (ds IAT) and six suicide risk factors among undergraduates (N = 408). Having a belief in some type of meaning in life (i.e., a sense of a broader purpose) decreased lifetime odds of suicide attempts among undergraduate students, while believing in or searching for the meaning in life were both associated with decreased suicidal ideation over time (Kleiman & Beaver, 2013, p. 937). Searching for the meaning in life was also found to mediate the relationship between psychological theory variables (i.e., perceived burdensomeness and thwarted belonging) and suicidal ideation among undergraduate students (Kleiman & Beaver, 2013).
An EAS (i.e., individuals that give global and stable attributions to positive events) was reported as a protective factor against suicide among undergraduate students (N = 209; Kleiman et al., 2012). Enhanced attribution style in people with higher depressive symptoms was associated with less suicide ideation when compared to individuals with comparable depressive symptoms without EAS. By neutralizing negative bias toward negative information (in turn increasing attention on positive thoughts), authors hypothesized EAS may buffer the relationship between depressive symptoms and suicidal ideation. Collins et al. (2016) described mindfulness as a protective factor for suicide risk through its contribution to supporting a person to display less reactivity when faced with adversity. Blalock et al. (2015) found a person’s level of grit (defined as “a psychological strength involving perseverance through adversity to reach long‐term goals”) buffered the relationship between negative life events and suicidal ideation (p. 781).
Coping skills
Finally, 10 studies endorsed coping skills as a protective factor. This construct was operationalized as (1) the ability to communicate stressful thoughts and express feelings (Cwik et al., 2015; Galligan et al., 2010; Johnson et al., 2010; Matel‐Anderson & Bekhet, 2016); (2) the ability to identify positive ways of coping with stressful life events (Peter & Taylor, 2014); (3) the confidence in their ability to solve problems (Burke et al., 2016; Nagra, Lin, & Upthegrove, 2016); (4) the strategies to bounce back (Woodford et al., 2018); and (e) a well‐developed level of emotional intelligence (Cha & Nock, 2009; Johnson et al., 2010).
Nagra et al. (2016) examined 323 youth (aged 22–24) to understand potential associations between self‐harm, forgiveness and attachments in suicidality. Higher levels of dismissing attachment relationships were associated with suicidality, and higher levels of self‐forgiveness, emotion coping and support‐seeking were protective against suicidality. Woodford et al. (2018) report that psychological resilience, defined as personalized coping strategies and ability to bounce back, was associated with increased resiliency in gender and sexual minority students.
Cha and Knock (2009) also identified emotional intelligence (EI), defined as a multidimensional construct that includes two abilities identified as strategic EI—“to understand and manage emotions,” and experiential EI—“to perceive emotions and use them to facilitate thought” (p. 423), as a protective factor against suicidal behavior among 12–19 year olds recruited from local psychiatric clinics and the community (N = 54). Lower EI was associated with suicidality, while high EI was not associated with suicidality, and mid‐levels of emotional intelligence provided some association with less suicidality. Further analyses indicated most of the protective effects of EI were associated with strategic EI rather than experiential EI. Burke et al. (2016) found responding to depression symptoms with distraction and problem‐solving enhanced a person’s resilience associated with decreased suicide ideation among family dyads of 12–13 year old adolescents and their primary female caregiver. In many of these studies of coping skills the researchers also named the relationship between individual coping skills and environments supportive of fostering them.
Resources for Resilience
Twenty‐two (59%) of the included studies reported on resources for resilience (Table 5). Two major subthemes emerged related to this external construct: social support systems and inclusive environments.
Social support systems
Having a strong and broad social support system was reported as a protective factor to suicidality. Social support systems (including considerations around being part of a social network) and the types of social support received from those linkages are described. Important social networks were identified as family, friends, community, and school connectedness (Borowsky et al., 2013; Brennan et al., 2017; Collinshaw et al., 2016; Eisenberg et al., 2017; Foster et al., 2017; Fraser et al., 2015; Hopkins, Zubrick, & Taylor, 2014; Lamis & Lester, 2013; Murphy, 2014; Mustanski & Liu, 2013; Philip et al., 2016; Taliaferro & Muehlenkamp, 2014, 2017; Teevale et al., 2016; Veale, Peter, Travers, & Saewyc, 2017; Whitaker, Shapiro, & Shields, 2016), and access to holistic systems of care (Kelley et al., 2018). Types of social supports included practical and emotional support (Armstrong & Manion, 2015; Galligan et al., 2010; Kleiman & Beaver, 2013) from these social networks.
Family connectedness was frequently identified as a protective factor for mental health, while school connectedness was identified as a protective factor for extreme stress and or despair among transgendered adolescents (Veale, Peter, et al., 2017). A perception of having caring friends was found to be predictive and protective of suicide attempts in the past year (Veale, Peter, et al., 2017). Similarly, parent connectedness, and or connectedness to other adults and caring friends reduced the likelihood of suicide attempts among high school students (Taliaferro & Muehlenkamp, 2014). Connectedness to parents and school was associated with lower levels of suicidal ideation, social anxiety, and sexual activity and lower parent‐reported conduct problems among youth experiencing social challenges (e.g., bullying) (Foster et al., 2017). Community connectedness was associated with lower social anxiety as an associated risk factor for suicidality (Foster et al., 2017). Similarly, Collinshaw et al. (2016) found social support system factors were associated with good mental health for youth when they have at least one caregiver parent that positively expressed emotion, co‐parent support, and good quality social relationships.
When comparing adolescents from urban and rural communities, Murphy (2014) found that while “the ability to discuss personal problems with parents,” “enjoying spending time with parents,” and “having good friends who displayed positive attributes” were associated with decreased suicide ideation among urban youth, these resources were not significant for rural youth (pp. 180–183). In a large study of Western Australian Aboriginal youth, researchers identified the protective role of prosocial friendships because they promote “adaptive functioning” (Hopkins et al., 2014, p. 5). In this study, such friendships were correlated with resilience notably even for youth with high‐risk home environments.
Inclusive Environments
Inclusive environments and safety in social environments (e.g., feeling safe within schools, neighborhoods, communities) were reported as protective factors in eight studies (Borowsky et al., 2013; Eisenberg et al., 2017; Galligan et al., 2010; Hatzenbuehler, 2011; Hopkins et al., 2014; Taliaferro & Muehlenkamp, 2014, 2017; Whitaker et al., 2016). Two studies found that feeling safe at school and in one’s neighborhood was a protective factor against suicidal ideation both among LGB youth (Whitaker et al., 2016) and among youth involved in verbal and social bullying (Borowsky et al., 2013). Five of these studies explored resilience or prevention of suicidality among nonheteronormative youth (Eisenberg et al., 2017; Galligan et al., 2010; Hatzenbuehler, 2011; Taliaferro & Muehlenkamp, 2017; Whitaker et al., 2016). Three studies identified freedom from discrimination as important contributors to resilience, with one focused on freedom from racism (Galligan et al., 2010), and two focused on freedom from discrimination related to heteronormativity (Hatzenbuehler, 2011; Hopkins et al., 2014).
Other interesting examples of structural drivers of safer social settings were highlighted in the following two studies. In a large cross‐sectional study (N = 33,714), Hatzenbuehler (2011) used a five‐item index to explore relationships between suicidality, risk, and what was hypothesized to be a socially protective environment. This social climate index included the (1) “proportion of same‐sex couples in the county”; (2) “ proportion of Democrats living in the county”; (3) “proportion of schools with gay‐straight alliances”; (4) “proportion of schools with anti‐bullying policies specific to LGB students”; and (5) “proportion of schools with anti‐discrimination policies that included sexual orientation” (Hatzenbuehler, 2011, p.897). Their findings suggest that, even after adjusting for individual risk factors, a positive social climate was significantly associated with fewer suicide attempts.
In another study, involving Western Australian Aboriginal youth and their parents, Hopkins et al. (2014) reported reduced resilience among youth who lived in neighborhoods with higher socio‐economic indices. Although these findings may seem counterintuitive, the researchers commented that Aboriginal families living in higher income Australian neighborhoods would be in the vast minority and may therefore have more frequent encounters with racism and discrimination, whereas living in environments where youth fit in might support resilience. Both studies point to the ways in which policy environments, social climate, and prevention of discriminatory attitudes and acts can play a role in fostering resilience.
Intersectionalities of Interest
Age and life transitions
Suicidality in preadolescent children under 13 years is a growing concern. Westefeld et al. (2010) report the need for a call to action for targeted suicide prevention for preadolescents, with continued support as they move through life transitions into later adolescence and young adulthood. In this review, however, only 11 studies included 12 year olds in their participant population age range, while three studies included children as young as 10 years old and one included children as young as nine years old. The majority of studies (n = 24) included 13 to 18 years old as participants and 17 studies included young adults aged 19 to 25 years old.
Sex and Gender Considerations
Although 27 studies provided some information regarding the sex and gender demographics of their study samples, only 11 studies included analysis of sex and gender differences in study outcomes. Most of these studies used data that distinguished between sex, gender, and gender identity. Eisenberg et al. (2017) compared four protective factors (i.e., internal assets, family connectedness, student–teacher relationships, and feeling safe in community) between transgender and gender nonconforming (TGNC; i.e., people who have a gender identity that is not fully aligned with their sex assigned at birth) youth and cis‐gendered youth (i.e., people whose sex assigned at birth is aligned with their gender identity) (p. 524). Cis‐gendered youth reported higher ratings for all four factors compared to TGNC youth. Birth‐assigned females reported significantly higher emotional distress and bullying experiences than males. In all studies focused on sexual and or gender minority youth, there was increased suicide risk among these youth compared to others, often with access to fewer protective factors.
Among Inuit youth, Fraser et al. (2015) reported suicidal thoughts and attempts were both higher for females than males, and although no protective factors were identified for males, participating in hunting activities was protective for females. Although hunting activities were traditionally male dominated, the roles have been changing alongside social changes, and the authors speculate that participation in hunting may be indicative of affirmation of Inuit identity and values related to land‐based activities and or high levels of integration into family structures for young women.
When examining gender differences in suicidal ideation among college students, Lamis and Lester (2013) found having a reason for living was protective for both men and women. Men reported both lower depressive symptoms and reasons for living, suggesting although they may be at decreased risk, they also have fewer protective factors to protect against risk. Interestingly, this study also found increased family support was associated with a higher risk of suicidal ideation among men, contradicting previous research findings that identify social support as protective. The researchers hypothesize there may be some engendered dimension to this finding whereby the support is also linked to fears of disappointing parents that could increase suicidal ideation. Similarly, Lester (2017) found that although participating in sports was good for overall youth mental health, for ethnic minority girls, it was a significant risk factor for suicidal behavior. The researchers speculate this may be related to acculturation stress and or having families that may not view athletic activities as appropriate for their female daughters. Taliaferro and Muehlenkamp (2014) found neighborhood safety was a protective factor among males, while academic achievement had a large protective effect for females in terms of suicidal behavior.
Indigenous Youth
Nine studies reported on protective factors for Indigenous groups (Cwik et al., 2015; Eisenberg et al., 2017; Fraser et al., 2015; Hopkins et al., 2014; Kelley et al., 2018; Lester, 2017; Philip et al., 2016; Taliaferro & Muehlenkamp, 2017; Teevale et al., 2016). Five of these studies focused solely on Indigenous‐specific resiliency and protective factors among American Indian, Inuit, Yup’ik Alaska Native and Pacific Islander youth, respectively (Cwik et al., 2015; Fraser et al., 2015; Kelley et al., 2018; Philip et al., 2016; Teevale et al., 2016). These factors were primarily family‐ and community‐level resiliency considerations, with a strong focus on culture and connection, including (1) safety (very close community, freedom from racism); (2) social support (holistic system of care, connection to Elders, connection to adults, connections to parents, friend, family, community); (3) self‐efficacy (traditional lifestyle and activities, communal mastery, sports participation and physical activity); (4) self‐identity (proud to be [Indigenous], religious [beliefs, faith, spirituality], cultural identity, wanting to be a role model); and (5) zest for life (life satisfaction).
Discussion
Our findings validate the importance of fostering resilience as an important part of primary suicide prevention among youth, aligning with others’ descriptions of resilience as dynamic, including both assets, or positive internal factors (e.g., competence, self‐efficacy, coping skills), and resources, or external factors in the social environment (e.g., social support, mentorship, social networks) (Fergus & Zimmerman, 2005). Our findings also reveal important gaps in research related to understanding and promoting population‐level resilience to youth suicide as a primary prevention strategy. In particular, with a preponderance of research focused on individual‐level protective factors and little information examining the interactions between resiliency factors in conjunction with attention to context and intersectionality, this review provides limited applicability for informing systems‐level interventions to support resilience among youth. We discuss the findings within this context below, followed by considerations for integrating Indigenous knowledge systems to support this work in the future as well as acknowledging the limitations of both the research in this area and of this review.
Despite the focus of our review, as depicted by our results, most of the research in this area has reported primarily on individual‐level resilience factors, with less attention to broader sources of resilience. An important and consistent barrier to upstream prevention is the dominance of bio‐behavioral (Clarke, Mamo, Fosket, Fishman, & Shim, 2010; Hanson, 2017) and reductionist assumptions (Jayasinghe, 2011; Rogers et al., 2013) in the health sciences. In the context of preventing suicidality, these tendencies can entrench a deep focus on individuals rather than on the contexts and social constructs in which they are situated. Extending our consideration of suicidality to include family, community, cultural constructs across peoples, understandings of the impact of childhood experiences, and life trajectories (British Columbia Coroners Service [BCCS], 2019; Thompson, Kingree, & Lamis, 2019; Ungar, 2011, 2018; White, 2014, 2016, 2017; White & Mushquash, 2016; Zuckerman & Pedersen, n.d.) could lead to more comprehensive and meaningful interventions.
Many studies of youth suicide prevention have produced individual‐level intervention strategies, yet population‐level youth suicide rates continue to rise. When considering the findings from this study, and for example, recent attention on how access to one caring adult can shift youth suicide risk (Aubrey, 2019), it is important to understand not only how to promote these individual‐level supports for youth, but also how to intervene at the systems level to create the conditions within which these promising supports are equitably and sustainably available to all youth. However, in keeping with other major criticisms of resiliency research (Ungar, 2011, 2018), our review revealed little explanation for how resources and assets for resiliency interact, and the findings were limited by an over‐reliance on individual‐level resilience factors, often to the exclusion of broader contextual or environmental factors that are likely more relevant to experiences of resilience to suicidality.
Future research that includes resilience indicators at the community‐ and structural‐levels, in combination with longitudinal, multifactorial, and qualitative approaches, will be paramount to contextualizing, and understanding the interactions between resilience factors (Little et al., 2016). Similarly, the cross‐sectional nature of most of the identified studies limited insights into how resiliency factors shift across time, contexts, and life transitions. Longitudinal research that is attentive to the complexity of resiliency processes through incorporating contextually and temporally specific designs to explore resilience‐related outcomes can provide deeper understandings of how resilience factors may buffer suicidality risk throughout development and life transitions (Gallagher & Miller, 2018; Johnson et al., 2010; Ungar, 2011).
Although trauma‐informed practice is suggested in response to the impact of adverse childhood experiences (ACEs) on youth suicide risk (Thompson et al., 2019; Zuckerman & Pedersen, n.d.), preventing exposure to ACEs in the first place through structures, policies, and environments that facilitate the development of resilient youth is less clear. The youngest participants included in our review were 10 years of age, with the majority of studies focusing on youth who were young adolescents or older. Amid growing concern for suicide risk among preadolescent children (Westefeld et al., 2010) and growing acknowledgement of the importance of supporting perinatal mental health for the long‐term wellness of children and families (Shahram et al., 2017), research that engages a life course perspective grounded in social ecological understandings of resilience is paramount to elucidating better understandings of the nature of resilience‐promoting processes. Such insights can inform development of more comprehensive community‐ and systems‐level interventions to promote facilitative environments that provide children and youth with the opportunity to thrive (Ungar, 2011).
Our findings also suggest that fostering resilience requires attentiveness to the intersections between the internal and external drivers of resiliency, positioning individuals in the context of ecosystems or communities in order to achieve true primary prevention goals.
Primary prevention draws attention to upstream determinants of health outcomes. Life trajectories are shaped by social and structural determinants of health, including policy environments and the distribution of power and resources in society (Commission on Social Determinants of Health [CSDH], 2008; Marmot, Allen, Bell, Bloomer, Goldblatt, & Consortium for the European Review of Social Determinants of Health and the Health Divide, 2012). Studies reviewed here illuminate the intersectionality of social climate and safety (Galligan et al., 2010; Hatzenbuehler, 2011; Hopkins et al., 2014) with social locations of youth and their resilience to suicidality. These findings demonstrate a need for deep attentiveness to how to cultivate supportive and accepting social climate within families, schools, and communities through connectedness, and social political inclusivity through policy and environments. Examining multivariate interrelations between different risk and protective factors for suicidal behavior, from individual‐level to systems‐level factors, could provide further understanding of resilience (Kumar et al., 2012; Mustanski & Liu, 2013; Ungar, 2011, 2018; Wyatt, Ung, Park, Kwon, & Trinh‐Shevrin, 2015).
Indigenous communities have done much thinking and work on community‐level resilience to suicidality (Chandler, Lalonde, Sokol, & Hallett, 2003; Kirmayer et al., 2012; Marcellus & Shahram, 2017) and life course perspectives related to mental wellness for children and youth (Shahram et al., 2017). Indeed, as demonstrated by this review, the majority of considerations around environmental‐ and community‐level resilience factors were from Indigenous‐specific research; there is a wealth of opportunity to learn from and with Indigenous knowledge systems and approaches to preventing youth suicide. However, as also demonstrated in this review, much of resiliency research to date has ignored the contribution of cultural relativity to resilience and is often assessed primarily from the standpoint of the dominant cultural reference group, limiting our understandings of resilience as a process that reflects the influence of culture (Ungar, 2011). These shortcomings are further compounded by the field’s relative silence on incorporating analyses of power as it relates to resilience (Ungar, 2018), as well as a lack of attention, credit and validity being afforded to culturally distinct strategies to promote resilience (Shahram, Horsethief, Pauly, Kent, & Pierre, 2020; Ungar, 2011). Decolonizing research processes, spaces and systems is a necessary consideration for supporting the meaningful inclusion of Indigenous knowledge systems and approaches to promoting resiliency to suicide for all youth (Shahram et al., 2020).
It is important to recognize that people exist within synergistic environments. While vitally important for at‐risk youth, for youth who do not reveal or reach out for help regarding their suicidal inclinations, individual‐focused prevention strategies likely will remain rather ineffective. Positive and or negative outcomes can arise from the context of these environments and a person’s interaction within. For example, Hole et al. (2015) describe Indigenous peoples’ experience as a consequence of structural privileging associated with the biomedical approach. The value and importance of culture in health and healing and cultural safety has not been traditionally supported in biomedicine, despite more recent shifts. “By engaging young people as knowledgeable collaborators and by paying attention to broader socio‐political and cultural contexts in understanding sources of suffering, a more flexible approach to youth suicide prevention research and practice is envisioned” (White, 2014, p. 104). Indeed, a major focus of the Canadian Council of Child and Youth Advocates’ call to action for the development of a national strategy for youth suicide was the foundational importance of including young people in developing the solutions at every stage of the process, with particular attention to inclusion of Indigenous peoples and communities (CCCYA, 2019).
These considerations, coupled with the understanding that resiliency is supported by supportive societies and communities, point to the need for more ecological perspectives related to resilience that include community as a starting point (Ungar, 2011, 2018). Future research to promote resilience to suicide among youth should engage with what Ungar (2018) refers to as systemic resilience, whereby the complexity of resilience processes is embraced in an effort to design interventions that can promote youth resilience from a systems perspective, rather than through biomedical, individually focused risk reduction interventions. Further exploration of how developmental assets and other positive youth development theories align with resiliency theory related to primary prevention of youth suicide is also warranted (Benson et al., 2011; Lerner, Phelps, Forman, & Bowers, 2009).
This body of literature also presented some particular limitations that warrant consideration. One such limitation regards the age of youth involved in research. Despite evidence that suicide risk can present as young as 10 years old (BCCS, 2019; Statistics Canada, 2012) and evidence that building resilience is a life‐long process that spans life transitions and developmental stages (Johnson et al., 2010), less than a third of studies included children younger than 13 (Borowsky et al., 2013; Burke et al., 2016; Cha & Nock, 2009; Collinshaw et al., 2016; Cwik et al., 2015; Eisenberg et al., 2017; Foster et al., 2017; Hopkins et al., 2014; Philip et al., 2016; Taliaferro & Muehlenkamp, 2017; Teevale et al., 2016) and none included considerations around perinatal mental health. Another limitation was the consistent use of binary sex and gender indicators and or the conflation of sex and gender. This limitation points to a clear need for further sex and gender considerations, particularly given emerging evidence of suicide rates among sex‐ and gender‐diverse youth.
Limitations
Our search was limited to articles published between 2008 and 2018 in peer‐reviewed journals in a handful of countries, and in English only. While this was determined to be important to our purposes to maintain some consistency related to the social and cultural contexts of the youth included in the studies, it is likely that other sources of research on this topic could be informative. Importantly, our review’s inclusion of the term suicide may have excluded relevant resilience research that focused on youth resiliency more generally and may have also included more structural resiliency factors. Still, the dearth of attention to these factors in suicide‐related research warrants attention.
Another limitation of this review is that we did not assess study quality or strength. However, the purpose and strength of a critical interpretive synthesis versus meta‐analysis is to synthesize and critically reflect on diverse forms of evidence, rather than to be inherently reproducible in process or product (Dixon‐Woods, 2006). Lastly, a lack of consistency between definitions across studies, including indicators, age groupings, and suicide outcomes of interest, is an inherent challenge for accurately extrapolating and categorizing the review’s findings. This issue has been well documented and developing consistency across measures and indicators is a frequent focus of current suicide research strategies.
Conclusions
Studies included in this review identified a range of factors that are correlated with resilience while providing little explanation for how these factors may work to protect youth from suicidality and or how different protective factors may be interrelated or dependent. Preventing youth suicide requires approaches that are multidimensional, adaptable, context‐specific, and culturally appropriate (White, 2014, 2016; White & Mushquash, 2016). Further research is needed to explore youth perspectives on these factors, particularly in how they believe community can play a role in creating meaningful supports. Doing so requires broadly representative research approaches that engage, include and center the perspectives of youth through participatory action research designs that emphasize ecological understandings of resilience, incorporating context, culture, environment, familial and community connections, and structural determinants of health.
This work will require shifting away from individual‐level resilience factors to explore, assess, and promote resilience at the community and systems levels while also explicitly attending to power considerations and opportunities to learn from other culture‐specific approaches (i.e., Indigenous approaches to wellness). Resilience is a dynamic and multi‐leveled process, and understanding how to promote resilience to suicide among youth will require embracing complexity to broaden targeted interventions across the life course and beyond the individual‐level to include systems‐level interventions.
The Blenk Family Fund was established together with the KGH Foundation to strengthen the network of mental health support and services available to young people and families in our community—supporting research, prevention, and care surrounding youth mental health.
References
- Armstrong, L. L. , & Manion, I. G. (2015). Predictors of rural and urban youth suicidal ideation by gender: A case for targeted approaches to prevention. Vulnerable Children and Youth Studies, 10(3), 206–219. 10.1080/17450128.2015.1046535 [DOI] [Google Scholar]
- Aubrey, A. J. (2019, September 11). For kids who face trauma, good neighbors or teachers can save their longterm health. Retrieved from https://news.byu.edu/children‐who‐face‐adversity‐have‐better‐long‐term‐health‐if‐they‐have‐enough‐positive‐childhood‐experiences‐too.
- Benson, P. L. , Scales, P. C. , & Syvertsen, A. K. (2011). The contribution of the developmental assets framework to positive youth development theory and practice. Advances in Child Development and Behavior, 41, 197–230. 10.1016/b978-0-12-386492-5.00008-7 [DOI] [PubMed] [Google Scholar]
- Blalock, D. V. , Young, K. C. , & Kleiman, E. M. (2015). Stability amidst turmoil: Grit buffers the effects of negative life events on suicidal ideation. Psychiatry Research, 228, 781–784. 10.1016/j.psychres.2015.04.041 [DOI] [PubMed] [Google Scholar]
- Borowsky, I. W. , Taliaferro, L. A. , & McMorris, B. J. (2013). Suicidal thinking and behavior among youth involved in verbal and social bullying: Risk and protective factors. Journal of Adolescent Health, 53(Supp. 1), S4–S12. 10.1016/j.jadohealth.2012.10.280 [DOI] [PubMed] [Google Scholar]
- Brennan, S. L. , Irwin, J. , Drincic, A. , Amoura, J. N. , Randall, A. , & Smith‐Sallans, M. (2017). Relationship among gender‐related stress, resilience factors, and mental health in a Midwestern US transgender and gender nonconforming population. International Journal of Transgenderism, 18, 433–445. 10.1080/15532739.2017.1365034 [DOI] [Google Scholar]
- British Columbia Coroners Service (2019). Supporting youth and health professionals: A report on youth suicides. Retrieved from https://www2.gov.bc.ca/assets/gov/birth‐adoption‐death‐marriage‐and‐divorce/deaths/coroners‐service/child‐death‐review‐unit/reports‐publications/youth_suicide_drp_report_2018.pdf [Google Scholar]
- Bureau, J. S. , Genevieve, M. , Vallerand, R. J. , Rousseau, F. L. , & Otis, J. (2012). Self determination: A buffer against suicide ideation. Suicide and Life‐Threatening Behavior, 42(4), 377–393. 10.1111/j.1943-278X.2012.00097.x [DOI] [PubMed] [Google Scholar]
- Burke, T. A. , Connolly, S. L. , Hamilton, J. L. , Stange, J. P. , Abramson, L. Y. , & Alloy, L. B. (2016). Cognitive risk and protective factors for suicidal ideation: A two year longitudinal study in adolescence. Journal of Abnormal Child Psychology, 44, 1145–1160. 10.1007/s10802-015-0104-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caldwell, D. (2008). The suicide prevention continuum. Pimatisiwin, 6(2), 145–153. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2936581/ [PMC free article] [PubMed] [Google Scholar]
- Canadian Council of Child and Youth Advocates (2019). A national paper on youth suicide. Retrieved from http://www.cccya.ca/Images/english/pdf/CCCYA%20National%20Suicide%20Paper%20Final%20September%2025%202019.pdf [Google Scholar]
- Cha, C. , & Nock, M. (2009). Emotional intelligence is a protective factor for suicidal behavior. Journal of the American Academy of Child and Adolescent Psychiatry, 48, 422–430. 10.1097/CHI.0b013e3181984f44 [DOI] [PubMed] [Google Scholar]
- Chandler, M. J. , Lalonde, C. E. , Sokol, B. W. , & Hallett, D. (2003). Personal persistence, identity development, and suicide: A study of Native and non‐Native North American adolescents. Monographs of the Society for Research in Child Development, 68(2), i‐130. 10.1111/1540-5834.00246 [DOI] [PubMed] [Google Scholar]
- Clarke, A. , Mamo, L. , Fosket, J. R. , Fishman, J. R. , & Shim, J. K. (2010). Biomedicalization: Technoscientific transformations of health, illness, and US biomedicine. In Clarke A.E., Mamo L., Fosket J.R., Fishman J.R., & Shim J.K. (Eds.), Biomedicalization: Technoscience, health, and illness in the US (pp. 47–87). Durham, NC: Duke University Press. [Google Scholar]
- Collins, K. R. L. , Best, I. , Stritzke, W. G. K. , & Page, A. C. (2016). Mindfulness and zest for life buffer the negative effects of experimentally‐induced perceived burdensomeness and thwarted belongingness: Implications for theories of suicide. Journal of Abnormal Psychology, 125, 704–714. 10.1037/abn0000167 [DOI] [PubMed] [Google Scholar]
- Collinshaw, S. , Hammerton, G. , Mahedy, L. , Sellers, R. , Owen, M.J. , Craddock, N. , … Thapar, A. (2016). Mental health resilience in the adolescent offspring of parents with depression: A prospective longitudinal study. Lancet Psychiatry, 3, 49–57. 10.1016/S2215-0366(15)00358-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Commission on Social Determinants of Health (2008). Closing the gap in a generation: Health equity through action on the social determinants of health: Commission on Social Determinants of Health final report. Retrieved from World Health Organization website: https://www.who.int/social_determinants/final_report/csdh_finalreport_2008.pdf. [Google Scholar]
- Cwik, M. , Barlow, A. , Tingey, L. , Goklish, N. , Larzelere‐Hinton, F. , Craig, M. , & Walkup, J. T. (2015). Exploring risk and protective factors with a community sample of American Indian adolescents who attempted suicide. Archives of Suicide Research, 19(2), 172–189. 10.1080/13811118.2015.1004472 [DOI] [PubMed] [Google Scholar]
- Dixon‐Woods, M. (2006, October). Critical interpretive synthesis: What it is and why it is needed [PowerPoint slides]. Oral presentation at the Come to the Craic. Abstracts of the 14th Cochrane Colloquium, Dublin, UK. Retrieved from https://abstracts.cochrane.org/2006‐dublin/critical‐interpretive‐synthesis‐what‐it‐and‐why‐it‐needed [Google Scholar]
- Dixon‐Woods, M. , Agarwal, S. , Jones, D. , Young, B. , & Sutton, A. (2005). Synthesising qualitative and quantitative evidence: A review of possible methods. Journal of Health Services Research & Policy, 10(1), 45–53. 10.1177/135581960501000110 [DOI] [PubMed] [Google Scholar]
- Eisenberg, M. E. , Gower, A. L. , McMorris, B. J. , Rider, N. G. , Shea, G. , & Coleman, E. (2017). Risk and protective factors in the lives of transgender/gender nonconforming adolescents. Journal of Adolescent Health, 61, 521–526. 10.1016/j.jadohealth.2017.04.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fergus, S. , & Zimmerman, M. A. (2005). Adolescent resilience: A framework for understanding healthy development in the face of risk. Annual Review of Public Health, 26, 399–419. 10.1146/annurev.publhealth.26.021304.144357 [DOI] [PubMed] [Google Scholar]
- Flouri, E. (2005). Psychological and sociological aspects of parenting and their relation to suicidal behavior. Archives of Suicide Research, 9(4), 373–383. 10.1080/13811110500182463 [DOI] [PubMed] [Google Scholar]
- Foster, C. E. , Horwitz, A. , Thomas, A. , Opperman, K. , Gipson, P. , Burnside, A. , … King, C. A. (2017). Connectedness to family, school, peers, and community in socially vulnerable adolescents. Children and Youth Services Review, 81, 321–331. 10.1016/j.childyouth.2017.08.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fraser, S. L. , Geoffroy, D. , Chachamovich, E. , & Kirmayer, L. J. (2015). Changing rates of suicide ideation and attempts among Inuit youth: A gender‐based analysis of risk and protective factors. Suicide and Life‐Threatening Behavior, 45(2), 141–156. 10.1111/sltb.12122 [DOI] [PubMed] [Google Scholar]
- Gallagher, M. L. , & Miller, A. B. (2018). Suicidal thoughts and behavior in children and adolescents: An ecological model of resilience. Adolescent Research Review, 3(2), 123–154. 10.1007/s40894-017-0066-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galligan, S. B. , Barnett, R. V. , Brennan, M. A. , & Israel, G. D. (2010). Understanding the link between gender role conflict, resilience, and propensity for suicide in adolescent and emerging adult males. International Journal of Men’s Health, 9(3), 201–210. 10.3149/jmh.0903.201 [DOI] [Google Scholar]
- Glaser, B. G. (2008). The constant comparative method of qualitative analysis. Grounded Theory Review: an International Journal, 7(3), 1–13. Retrieved from http://groundedtheoryreview.com/2008/11/29/the‐constant‐comparative‐method‐of‐qualitative‐analysis‐1/. [Google Scholar]
- Government of Canada (2019, July 22). Suicide in Canada. Retrieved August 26, 2019 from https://www.canada.ca/en/public‐health/services/suicide‐prevention/suicide‐canada.html.
- Hankivsky, O. (2014). Intersectionality 101. Vancouver, BC: The Institute for Intersectionality Research & Policy, Simon Fraser University. Retrieved from http://vawforum‐cwr.ca/sites/default/files/attachments/intersectionallity_101.pdf. [Google Scholar]
- Hanson, L. (2017). From reflexivity to collectivity: Challenging the benevolence narrative in global health. Canadian Medical Education Journal, 8(2), e1–e3. 10.36834/cmej.42021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harrison, D. P. , Stritzke, W. G. K. , Fay, N. , Ellison, M. T. , & Hudaib, A. R. (2014). Probing the implicit suicidal mind: Does the death/suicide implicit association test reveal a desire to die, or a diminished desire to live? Psychological Assessment, 26, 831–840. 10.1037/pas0000001 [DOI] [PubMed] [Google Scholar]
- Hatzenbuehler, M. L. (2011). The social environment and suicide attempts in lesbian, gay, and bisexual youth. Pediatrics, 127, 896–903. 10.1542/peds.2010-3020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heisel, M. J. , & Flett, G. L. (2008). Psychological resilience to suicide ideation among older adults. Clinical Gerontologist, 31(4), 51–70. 10.1080/07317110801947177 [DOI] [Google Scholar]
- Hole, R. D. , Evans, M. , Berg, L. D. , Bottorff, J. L. , Dingwall, C. , Alexis, C. , … Smith, M. L. (2015). Visibility and voice: Aboriginal people experience culturally safe and unsafe health care. Qualitative Health Research, 25, 1662–1674. 10.1177/1049732314566325 [DOI] [PubMed] [Google Scholar]
- Hopkins, K. D. , Zubrick, S. R. , & Taylor, C. L. (2014). Resilience amongst Australian Aboriginal youth: An ecological analysis of factors associated with psychosocial functioning in high and low family risk contexts. PLoS One, 9(7), e102820. 10.1371/journal.pone.0102820 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jayasinghe, S. (2011). Conceptualising population health: From mechanistic thinking to complexity science. Emerging Themes in Epidemiology, 8(2), 1–7. 10.1186/1742-7622-8-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson, J. , Gooding, P. A. , Wood, A. M. , & Tarrier, N. (2010). Resilience as positive coping appraisals: Testing the schematic appraisals model of suicide (SAMS). Behaviour Research and Therapy, 48, 179–186. 10.1016/j.brat.2009.10.007 [DOI] [PubMed] [Google Scholar]
- Kelley, A. , Restad, D. , & Killsback, J. (2018). A public health approach: Documenting the risk and protective factors of suicide ideation in one American Indian community. Psychological Services, 15, 325–331. 10.1037/ser0000211 [DOI] [PubMed] [Google Scholar]
- Kidd, S. , & Shahar, G. (2008). Resilience in homeless youth: The key role of self‐esteem. American Journal of Orthopsychiatry, 78(2), 163–172. 10.1037/0002-9432.78.2.163 [DOI] [PubMed] [Google Scholar]
- Kirmayer, L. J. , Dandeneau, S. , Marshall, E. , Phillips, M. K. , & Williamson, K. J. (2012). Toward an ecology of stories: Indigenous perspectives on resilience. In Unger M. (Ed.), The social ecology of resilience: A handbook of theory and practice (pp. 399–414). New York, NY: Springer. [Google Scholar]
- Kleiman, E. M. , Adams, L. M. , Kashdan, T. B. , & Riskind, J. H. (2013). Gratitude and grit indirectly reduce risk of suicidal ideations by enhancing meaning in life: Evidence for a mediated moderation model. Journal of Research in Personality, 47, 539–546. 10.1016/j.jrp.2013.04.007 [DOI] [Google Scholar]
- Kleiman, E. M. , & Beaver, J. K. (2013). A meaningful life is worth living: Meaning in life as a suicide resiliency factor. Psychiatry Research, 210, 934–939. 10.1016/j.psychres.2013.08.002 [DOI] [PubMed] [Google Scholar]
- Kleiman, E. M. , Miller, A. B. , & Riskind, J. H. (2012). Enhancing attributional style as a protective factor in suicide. Journal of Affective Disorders, 143(1–3), 236–240. 10.1016/j.jad.2012.05.014 [DOI] [PubMed] [Google Scholar]
- Kumar, M. B. , Walls, M. , Janz, T. , Hutchinson, P. , Turner, T. , & Graham, C. (2012). Suicidal ideation among Métis adult men and women–associated risk and protective factors: Findings from a nationally representative survey. International Journal of Circumpolar Health, 71(1), 18829. 10.3402/ijch.v71i0.18829 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lamis, D. A. , & Lester, D. (2013). Gender differences in risk and protective factors for suicidal ideation among college students. Journal of College Student Psychotherapy, 27(1), 62–77. 10.1080/87568225.2013.739035 [DOI] [Google Scholar]
- Lerner, J. V. , Phelps, E. , Forman, Y. , & Bowers, E. P. (2009). Positive youth development. In Lerner R.M., & Steinberg L. (Eds.), Handbook of adolescent psychology: Individual bases of adolescent development (3rd ed., p. 524–558). Hoboken, NJ: John Wiley & Sons Inc. [Google Scholar]
- Lester, D. (2017). Participation in sports activities and suicidal behaviour: A risk or a protective factor? International Journal of Sport and Exercise Psychology, 15(1), 103–108. 10.1080/1612197X.2015.1073340 [DOI] [Google Scholar]
- Little, T. D. , Roche, K. M. , Chow, S.‐M. , Schenck, A. P. , & Byam, L.‐A. (2016). National Institutes of Health Pathways to Prevention Workshop: Advancing research to prevent youth suicide. Annals of Internal Medicine, 165, 795–799. 10.7326/M16-1568 [DOI] [PubMed] [Google Scholar]
- Malone, K. M. , Oquendo, M. A. , Haas, G. L. , Ellis, S. P. , Li, S. , & Mann, J. J. (2000). Protective factors against suicidal acts in major depression: Reasons for living. American Journal of Psychiatry, 157, 1084–1088. 10.1176/appi.ajp.157.7.1084. [DOI] [PubMed] [Google Scholar]
- Marcellus, L. , & Shahram, S. Z. (2017). Starting at the beginning: The role of public health nursing in promoting infant and early childhood mental health. Nursing Leadership, 30(3), 43–53. 10.12927/cjnl.2018.25386 [DOI] [PubMed] [Google Scholar]
- Marmot, M. , Allen, J. , Bell, R. , Bloomer, E. , & Goldblatt, P. & Consortium for the European Review of Social Determinants of Health and the Health Divide (2012). WHO European review of social determinants of health and the health divide. Lancet, 380, 1011–1029. 10.1016/S0140-6736(12)61228-8 [DOI] [PubMed] [Google Scholar]
- Matel‐Anderson, D. M. , & Bekhet, A. K. (2016). Resilience in adolescents who survived a suicide attempt from the perspective of registered nurses in inpatient psychiatric facilities. Issues in Mental Health Nursing, 37, 839–846. 10.1080/01612840.2016.1193578 [DOI] [PubMed] [Google Scholar]
- Mays, N. , Pope, C. , & Popay, J. (2005). Systematically reviewing qualitative and quantitative evidence to inform management and policy‐making in the health field. Journal of Health Services Research and Policy, 10(Suppl. 1), 6–20. 10.1258/1355819054308576 [DOI] [PubMed] [Google Scholar]
- Moher, D. , Liberati, A. , Tetzlaff, J. , & Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta‐analyses: The PRISMA statement. PLoS Medicine, 6(7), e1000097. 10.1371/journal.pmed.1000097 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murphy, S. M. (2014). Determinants of adolescent suicidal ideation: Rural versus urban. The Journal of Rural Health, 30(2), 175–185. 10.1111/jrh.12042 [DOI] [PubMed] [Google Scholar]
- Mustanski, B. , & Liu, R. T. (2013). A longitudinal study of predictors of suicide attempts among lesbian, gay, bisexual, and transgender youth. Archives of Sexual Behavior, 42, 437–448. 10.1007/s10508-012-0013-9 [DOI] [PubMed] [Google Scholar]
- Nagra, G. S. , Lin, A. , & Upthegrove, R. (2016). What bridges the gap between self‐harm and suicidality? The role of forgiveness, resilience and attachment. Psychiatry Research, 241, 78–82. 10.1016/j.psychres.2016.04.103 [DOI] [PubMed] [Google Scholar]
- Navaneelan, T. (2012). Suicide rates: An overview (Catalogue no. 82–624‐X). Retrieved from Health Statistics Division, Statistics Canada website: https://www.suicideinfo.ca/wp‐content/uploads/2013/09/Suicide‐Rates‐An‐Overview_oa.pdf. [Google Scholar]
- O’Leary, V. E. (1998). Strength in the face of adversity: Individual and social thriving. Journal of Social Issues, 54, 425–446. 10.1111/0022-4537.751998075 [DOI] [Google Scholar]
- Pauly, B. , Shahram, S. Z. , van Roode, T. , Strosher, H. W. , & MacDonald, M. (2018). Reorienting health systems towards health equity: The systems health equity lens (SHEL). Victoria, BC: The Equity Lens in Public Health (ELPH) Research Project. Retrieved from https://www.uvic.ca/research/projects/elph/assets/docs/kte‐resource‐6‐‐‐systems‐health‐equity‐lens.pdf [Google Scholar]
- Peter, T. , & Taylor, C. (2014). Buried above ground: University‐based study of risk/protective factors for suicidality among sexual minority youth in Canada. Journal of LGBT Youth, 11(2), 125–149. 10.1080/19361653.2014.878563 [DOI] [Google Scholar]
- Philip, J. , Ford, T. , Henry, D. , Rasmus, S. , & Allen, J. (2016). Relationship of social network to protective factors in suicide and alcohol use disorder intervention for rural Yup’ik Alaska Native youth. Psychosocial Intervention, 25(1), 45–54. 10.1016/j.psi.2015.08.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Plamondon, K. M. , & Bisung, E. (2019). The CCGHR principles for global health research: Centering equity in research, knowledge translation, and practice. Social Science and Medicine, 239, 112530. 10.1016/j.socscimed.2019.112530 [DOI] [PubMed] [Google Scholar]
- Rogers, K. H. , Luton, R. , Biggs, H. , Biggs, R. , Blignaut, S. , Choles, A. G. , … Tangwe, P. (2013). Fostering complexity thinking in action research for change in social‐ecological systems. Ecology and Society, 18(2), 31. 10.5751/ES-05330-180231 [DOI] [Google Scholar]
- Roy, A. , Sarchiapone, M. , & Carli, V. (2007). Low resilience in suicide attempters. Archives of Suicide Research, 11(3), 265–269. 10.1080/13811110701403916 [DOI] [PubMed] [Google Scholar]
- Schreier, M. (2014). Qualitative content analysis. In Flick U. (Ed.), The SAGE handbook of qualitative data analysis (pp. 170–183). Thousand Oaks, CA: Sage Publications Ltd. [Google Scholar]
- Shahram, S. Z. , Bottorff, J. L. , Oelke, N. D. , Kurtz, D. L. M. , Thomas, V. , & Spittal, P. M. & For the Cedar Project Partnership (2017). Mapping the social determinants of substance use for pregnant‐involved young Aboriginal women. International Journal of Qualitative Studies on Health and Well‐Being, 12(1), 1275155. 10.1080/17482631.2016.1275155 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shahram, S. Z. , Horsethief, C. , Pauly, B. , Kent, A. , & Pierre, S. (2020). The story of xaȼqanaǂ ʔitkiniǂ: Reconciling our truths within colonial health systems. Manuscript in preparation.
- Soor, G. S. , Vukin, I. , Bridgman‐Acker, K. , Marble, R. , Barnfield, P. , Edwards, J. , … Bhalerao, S. (2012). The effects of gender on adolescent suicide in Ontario, Canada. Journal of the Canadian Academy of Child and Adolescent Psychiatry, 21, 179–185. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3413467/pdf/ccap21_3p0179.pdf [PMC free article] [PubMed] [Google Scholar]
- Statistics Canada (2012). Canadian coroner and medical examiner database: Annual report 2006 to 2008 (Catalogue no. 82–214‐X). Retrieved from https://www150.statcan.gc.ca/n1/en/pub/82‐214‐x/82‐214‐x2012001‐eng.pdf. [Google Scholar]
- Taliaferro, L. A. , & Muehlenkamp, J. J. (2014). Risk and protective factors that distinguish adolescents who attempt suicide from those who only consider suicide in the past year. Suicide and Life‐Threatening Behavior, 44(1), 6–22. 10.1111/sltb.12046 [DOI] [PubMed] [Google Scholar]
- Taliaferro, L. A. , & Muehlenkamp, J. J. (2017). Nonsuicidal self‐injury and suicidality among sexual minority youth: Risk factors and protective connectedness factors. Academic Pediatrics, 17, 715–722. 10.1016/j.acap.2016.11.002 [DOI] [PubMed] [Google Scholar]
- Teevale, T. , Lee, A. C. L. , Tiatia‐Seath, J. , Clark, T. C. , Denny, S. , Bullen, P. … Peiris‐John, R. J. (2016). Risk and protective factors for suicidal behaviors among pacific youth in New Zealand. Crisis, 37, 335–346. 10.1027/0227-5910/a000396 [DOI] [PubMed] [Google Scholar]
- Thompson, M. P. , Kingree, J. B. , & Lamis, D. (2019). Associations of adverse childhood experiences and suicidal behaviors in adulthood in a U.S. nationally representative sample. Child: Care, Health and Development, 45(1), 121–128. 10.1111/cch.12617 [DOI] [PubMed] [Google Scholar]
- Ungar, M. (2011). The social ecology of resilience: Addressing contextual and cultural ambiguity of a nascent construct. American Journal of Orthopsychiatry, 81(1), 1–17. 10.1111/j.1939-0025.2010.01067.x [DOI] [PubMed] [Google Scholar]
- Ungar, M. (2018). Systemic resilience: Principles and processes for a science of change in contexts of adversity. Ecology and Society, 23, 34. 10.5751/ES-10385-230434 [DOI] [Google Scholar]
- Veale, J. F. , Peter, T. , Travers, R. , & Saewyc, E. M. (2017). Enacted stigma, mental health, and protective factors among transgender youth in Canada. Transgender Health, 2(1), 207–216. 10.1089/trgh.2017.0031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Veale, J. F. , Watson, R. J. , Peter, T. , & Saewyc, E. M. (2017). The mental health of Canadian transgender youth compared with the Canadian population. Journal of Adolescent Health, 60(1), 44–49. 10.1016/j.jadohealth.2016.09.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wesley‐Esquimaux, C. (2009). Trauma to resilience: Notes on decolonization. In Valaskakis G.G., Stout M.D., & Guimond E. (Eds.), Restoring the balance: First Nations women, community, and culture (pp. 13–34). Winnipeg, MB: University of Manitoba Press. https://uofmpress.ca/files/Restoring_the_Balance.pdf. [Google Scholar]
- Westefeld, J. S. , Bell, A. , Bermingham, C. , Button, C. , Shaw, K. , Skow, C. , … Woods, T. (2010). Suicide among preadolescents: A call to action. Journal of Loss and Trauma, 15, 381–407. 10.1080/15325024.2010.507655 [DOI] [Google Scholar]
- Whitaker, K. , Shapiro, V. B. , & Shields, J. P. (2016). School‐based protective factors related to suicide for lesbian, gay, and bisexual adolescents. Journal of Adolescent Health, 58(1), 63–68. 10.1016/j.jadohealth.2015.09.008 [DOI] [PubMed] [Google Scholar]
- White, J. (2014). Expanding and democratizing the agenda for preventing youth suicide: Youth participation, cultural responsiveness, and social transformation. Canadian Journal of Community Mental Health, 33(1), 95–107. 10.7870/cjcmh-2014-009 [DOI] [Google Scholar]
- White, J. (2016). Preventing youth suicide: A guide for practitioners. Retrieved from Ministry of Child and Family Development, Government of British Columbia website: https://www2.gov.bc.ca/assets/gov/health/managing‐your‐health/mental‐health‐substance‐use/child‐teen‐mental‐health/preventing_youth_suicide_practitioners_guide.pdf. [Google Scholar]
- White, J. (2017). What can critical suicidology do? Death Studies, 41, 472–480. 10.1080/07481187.2017.1332901 [DOI] [PubMed] [Google Scholar]
- White, J. , & Mushquash, C. (2016). We belong: Life promotion to address Indigenous suicide. Bothwell, ON: Thunderbird Partnership Foundation. Retrieved from https://wisepractices.ca/wp‐content/uploads/2017/12/White‐Mushquash‐2016‐FINAL.pdf. [Google Scholar]
- Whitehead, M. , & Dahlgren, G. (2006). Concepts and principles for tackling social inequities in health: Levelling up part 1 (World Health Organization: Studies on Social and Economic Determinants of Population Health No. 2). Retrieved from WHO Office for Europe website: https://www.euro.who.int/__data/assets/pdf_file/0010/74737/E89383.pdf. [Google Scholar]
- Woodford, M. R. , Weber, G. , Nicolazzo, Z. , Hunt, R. , Kulick, A. , Coleman, T. ., … Renn, K. A. (2018). Depression and attempted suicide among LGBTQ college students: Fostering resilience to the effects of heterosexism and cisgenderism on campus. Journal of College Student Development, 59, 421–438. 10.1353/csd.2018.0040 [DOI] [Google Scholar]
- World Health Organization (2019). Suicide [Fact sheet]. Retrieved October 26 2019, from https://www.who.int/en/news‐room/fact‐sheets/detail/suicide. [Google Scholar]
- Wyatt, L. C. , Ung, T. , Park, R. , Kwon, S. C. , & Trinh‐Shevrin, C. (2015). Risk factors of suicide and depression among Asian American, Native Hawaiian, and Pacific Islander youth: A systematic literature review. Journal of Health Care for the Poor and Underserved, 26(2), 191–237. 10.1353/hpu.2015.0059 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zimmerman, M. A. , Bingenheimer, J. B. , & Notaro, P. C. (2002). Natural mentors and adolescent resiliency: A study with urban youth. American Journal of Community Psychology, 30, 221–243. 10.1023/A:1014632911622 [DOI] [PubMed] [Google Scholar]
- Zuckerman, D. , & Pedersen, S. (n.d.). How childhood and youth experiences link to suicide. Retrieved from https://www.center4research.org/childhood‐youth‐experiences‐link‐suicide/.