

Abstract
Orbital disorders may present with change in form or function or may be discovered incidentally during clinical or imaging evaluations. A standardized orbital clinical examination, with appropriate ancillary tests, is helpful in narrowing the differential diagnosis and in the development of plans for management, with an eye toward minimizing the morbidity of the disease or its treatment. Evaluation and management may best be performed with a multidisciplinary team, which has become more common in skull base surgery.
Keywords: orbit, skull base, neuro-ophthalmologist, optical coherence tomography, orbital echography, orbital, surgery
Introduction
Each patient deserves our attention and our best risk–benefit analysis to assist them in decision making—this is the process of informed consent. The clinical evaluation is the first step of the process, during which the physician–patient relationship begins, based on a foundation of knowledge, respect, and trust, and through which optimal therapeutic plans may be constructed.
It Takes a Village
We often “share” patients with colleagues, depend on our colleagues' expertise, and, at times, work together in multidisciplinary clinics and/or in the surgical theaters. The initial evaluation of the “orbital patient” may be in an emergency department, an urgent care facility, a primary care physician's office, or in the office of an internal medicine subspecialist, a neurologist, an ophthalmologist, an otolaryngologist, a plastic surgeon, or a neurosurgeon. Any patient with orbital disease requires a complete evaluation by an orbital specialist, and the subsequent communication of these findings to the referring physician and to the other members of the multidisciplinary team. 1 2
Chief Complaint
Orbital disease may first be evident to the patient, to others who may notice a change in the patient's appearance, to a physician during examination for unrelated reasons, or may be an “incidental finding” in an imaging study. The patient may complain of a change in his or her appearance or discomfort. The patient may have had changes in vision—“My vision is blurry … When I stand up, my vision blacks out for a second or two … When I look to the side, my vision blacks out … My peripheral vision is bad … I have double vision.” On occasion the chief complaint is, “I had a (CT/MRI) done for (headache/injury/weakness/etc.) and they found a tumor behind my eye.”
History of Present Illness
Onset, progression, and variability are important in the history. It is sometimes helpful to compare appearance with old photos. If prescription lenses have been in use, the history of initiation of use and stability or instability of the power of lenses needed may be helpful clues.
Medical History
Specifically, history of hypertension, diabetes, sinonasal disease, cranial or intracranial disease, cancer, thyroid disorder, autoimmune disease, immunosuppression, injuries, surgeries, complications of anesthesia or surgery, bleeding diatheses, tumors, and vascular malformations will be instructive family history of genetic disorders, bleeding disorders, tumors, and complications of anesthesia should be noted, and a proper social history should also be taken.
Review of Records
Of course, personal review of records, reports, and “films” (today known as images) by the orbital surgeon and/or neuro-ophthalmologist is invaluable.
Clinical Examination and Ancillary Tests
The examination rightly begins with inspection of eyewear, with determination of prescriptive power, including measurement of any prism correction within the spectacles, and/or notation of fit of contact lenses, if in use. Sometimes refraction is required as a diagnostic test. 3 Visual acuity, with best possible lens correction, should be measured at distance in Snellen notation. Near vision may also be measured but is not a substitute for determination of distance acuity. Establishment of “20/20 vision” does not indicate the absence of optic nerve compromise by an orbital process. 4 Vision may also be assessed with aid of contrast sensitivity testing, color vision testing, and perimetry (visual field analysis). Not every orbital patient requires formal contrast sensitivity and color plate testing, but it is helpful to hold a red target before the patient and to alternately occlude the eyes, inquiring if one eye perceives the red to be more or brighter red, as red desaturation may be an early sign of optic nerve compromise.
Perimetry should be done prior to instilling diagnostic eyedrops. Most often this is accomplished via quantitative static perimetry, such as Humphrey 24-2 or 30-2, but may be performed by other means, such as Goldmann perimetry, Octopus perimetry, or others. One strives to utilize testing which is standardized and may be performed in another part of the world on similar apparatus, allowing reliable comparisons of test results.
Inspection of eyelids and orbits follows. Is there asymmetry, eyelid edema, erythema, ecchymosis, tenderness? Is the eyelid contour normal? A lateral flared retraction of the upper eyelid is suggestive of thyroid eye disease or TED, 5 6 while an “S-shaped ptosis,” with lateral depression of the upper eyelid, is suggestive of a lacrimal gland mass or inflammatory process. The margin reflex distance (MRD) 7 of the upper (MRD-1) and lower (MRD-2) eyelids is measured and recorded ( Fig. 1 ). An exophthalmometer is used to record the anterior projection of each globe in reference to the lateral orbital rim, while also recording the base setting, so as to use the same base setting at subsequent visits to allow accurate assessment of change, if any. Globe displacement may also be horizontal or vertical and this relative position of one globe to the other should also be assessed and recorded. Taking and including photographs in the medical record is also useful.
Fig. 1.

A millimetric rule may be used to measure the distance from the upper eyelid margin to the light reflex (MRD-1) and from the lower eyelid margin to the light reflex (MRD-2), which in this case will demonstrate a relative 0.5 mm ptosis or the right upper eyelid. MRD, margin reflex distance.
Facial motor function is assessed and recorded. Unilateral orbicularis weakness may present with a complaint of “bulging” of the eye, due to a “wide-eyed” appearance, and/or a complaint or finding of “ptosis” on the opposite side. There may be attendant complaints of eye pain, redness, or tearing. Patients with a remote history of “recovered” facial palsy may have a combination of orbicularis weakness and spasm, sometimes accompanied by orbicularis “tics” or fasciculations.
Comparative sensitivity to light touch in the distribution of the first, second, and third branches of the trigeminal nerve is assessed and recorded. Pupils should be assessed and measured. The diameter of each should be measured and recorded under conditions of both dim and bright illumination, and if there is anisocoria in one or both circumstances, the cause of the anisocoria 8 should be determined before the patient leaves the examination suite, as this may be a sign of neurosurgical emergency in the case of an acute Horner's or third nerve palsy. Of course, there are many nonurgent causes of anisocoria, including, but not limited to, congenital anomaly, prior trauma or intraocular surgery, prior or active iritis, pseudoexfoliation syndrome, diabetic iridoplegia, or Adie's pupil. The presence or absence of a relative afferent pupil defect (RAPD) is critical in consideration of unilateral or asymmetric optic neuropathy.
Sensorimotor examination 9 is vital in assessing and measuring eye movement abnormalities in patients with orbital disorders. Even in patients with no complaint of diplopia, there are often abnormalities. A simple screening tool is the “alternate cover test”: the patient is instructed to fixate on a distant target, such as one letter in the eye chart, and the eyes are alternately occluded, moving the cover from one eye to the other ( Fig. 2 ). If there is an inherent “imbalance,” you may see a refixation movement as the uncovered eye reacquires the target; in cases of small angle deviations, you may not see a refixation movement, and it is helpful to ask the patient, “As I go from one eye to the other, does the letter seem to move side-to-side or up or down?” If there is misalignment, 10 it should be measured quantitatively by means of neutralization with a prism ( Fig. 3 ). The assessment and measurement should be made in different fields of gaze. Following these measurements, ductions (movement of each eye individually) should be evaluated, noting, measuring, and recording the range of motion of each eye in all directions, either by lateral and vertical version light reflex testing or qualitative (0–4 scale) recording of under or overaction ( Fig. 4 ). If there is a ductional deficit, it should be determined if this is on the basis of weakness of an extraocular muscle, or a mechanical restriction of eye movement. A forced duction test 11 may be helpful, in which a toothed forceps is utilized to grasp the topically anesthetized globe while the patient attempts to look in the direction of deficit. If the examiner is able to rotate the eye farther than the patient can, the deficit is attributed to weakness rather than restriction. Determination of ductional deficits due to paresis or restriction may alternatively be made by measurement of intraocular pressure (IOP) in different gaze positions. 12 If the IOP remains stable in attempted gaze at the limit of the ductional deficit, this is due to weakness. In the case of restriction, the effort of contraction of the functional but restricted extraocular muscle leads to momentary compression of the globe and elevated IOP. The sensorimotor testing is then completed with assessment of the character of saccadic and smooth pursuit eye movements and notation of the presence or absence of nystagmus.
Fig. 2.

A cross cover test will reveal misalignment (tropia) or potential misalignment when fusion is interrupted (phoria).
Fig. 3.

Prism neutralization should be done to measure and record strabismic deviation in all gaze positions. This is useful diagnostically as well as to assess change over time.
Fig. 4.
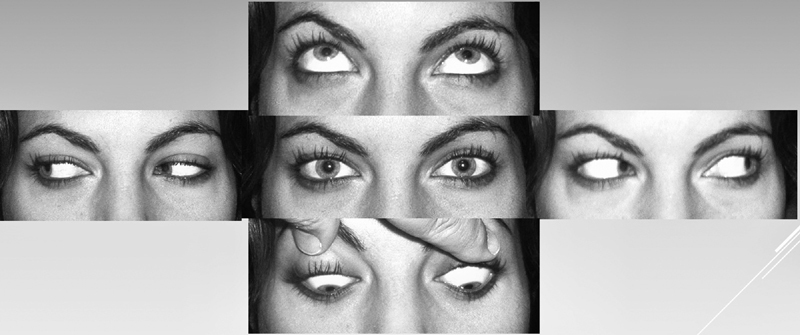
Ductions.
Slit lamp biomicroscopy is performed, with further assessment of the eyelid margins and the conjunctiva 13 ( Figs. 5 and 6 ). The cornea, anterior chamber, iris, pupil, and crystalline lens or intraocular lens implant are inspected. The tear film and cornea are stained with fluorescein and examined with a cobalt blue filter, allowing assessment of tear film adequacy and tear flow; adherent staining of the cornea is indicative of corneal epithelial disturbance. If there is blockage of egress of fluorescein, the lacrimal sac is compressed to assess presence or absence of reflux to assess patency of the nasolacrimal drainage system. IOP is then measured.
Fig. 5.
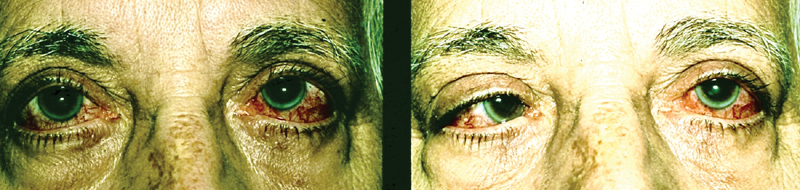
An elderly woman presented with complaint of “pressure” behind her eyes, redness of the eyes, and horizontal diplopia. Examination revealed bilateral sixth cranial nerve weakness and arterialization of conjunctival veins, leading to suspicion of unilateral or bilateral dural cavernous sinus fistula (or dural arteriovenous malformation).
Fig. 6.
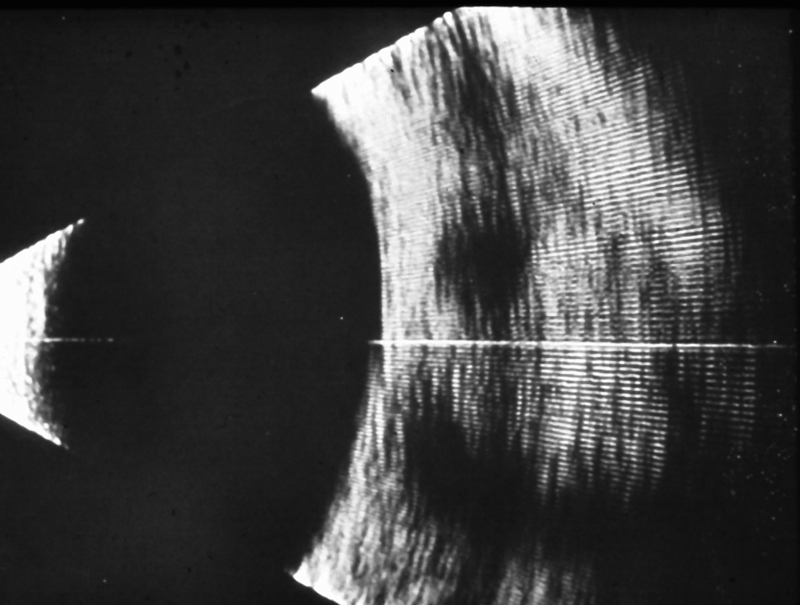
Vertically oriented B-mode echography of the left orbit revealed dilation of the superior orbital vein, seen in cross section above the optic nerve and below the superior rectus.
Dilating drops are instilled (providing the patient does not have narrow, occludable angles) and ophthalmoscopy is performed with assessment of the vitreous, retina, and optic nerve head. Mid-orbital tumors may be accompanied by optic nerve swelling, whereas small orbital apex tumors may cause progressive optic atrophy in the absence of swelling. 14 A cilioretinal shunt vessel may be indicative of optic nerve sheath infiltration ( Fig. 7 ). 15 16 The appearance of the optic nerve and retina may be documented by fundus photography.
Fig. 7.
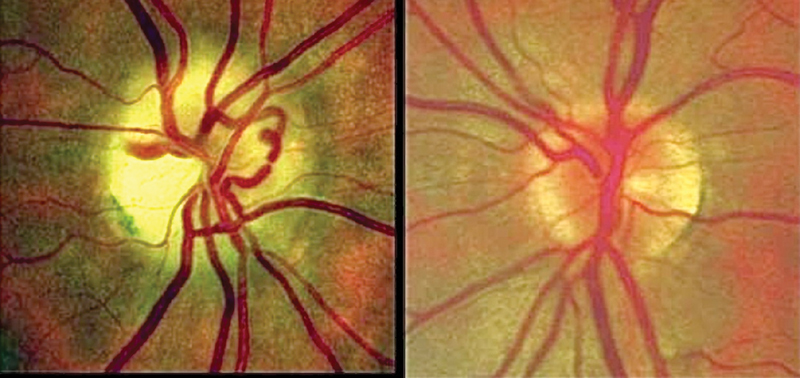
Fundus photos demonstrate normal appearance of the left optic nerve head, but right optic atrophy and a prominent cilioretinal shunt vessel in this patient with a history of progressive loss of vision of the right eye found to be secondary to optic nerve sheath meningioma (This image is provided courtesy of Steven A. Newman, MD).
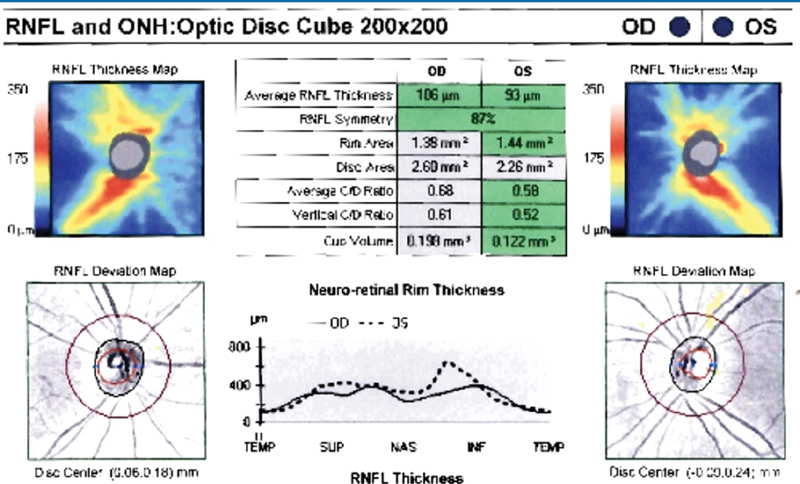
Optical coherence tomography (OCT) is an extremely helpful ancillary test. OCT is customarily performed for quantitative measurement of retinal nerve fiber layer (RNFL) thickness ( Fig. 8 ), retinal ganglion cell (RGC) layer thickness ( Fig. 9 ), and qualitative and quantitative assessment of macular health. In the presence of optic nerve damage, the RNFL and RGC layers will be thinned and the quantitative measurement is a reliable indicator of stability or progression of damage over time. In the presence of orbital disease, RGC layer thickness is a more reliable indicator than RNFL thickness because the RNFL thickness may be increased by venous congestion. So, as a consequence, one may view increasing RNFL thickness over time as an objective measurement of increasing venous congestion, and/or an indication of optic nerve head inflammation, infiltration, or ischemia. The OCT is more sensitive in the assessment of change over time than is ophthalmoscopy, serial fundus photography, or magnetic resonance imaging (MRI). A change of +/− 4 microns in average or regional RNFL or RGC layer regional thickness is often clinically significant, as compared with changes of +/− 500 microns for 3T MRI or +/− 100 microns for 7T MRI.
Fig. 8.
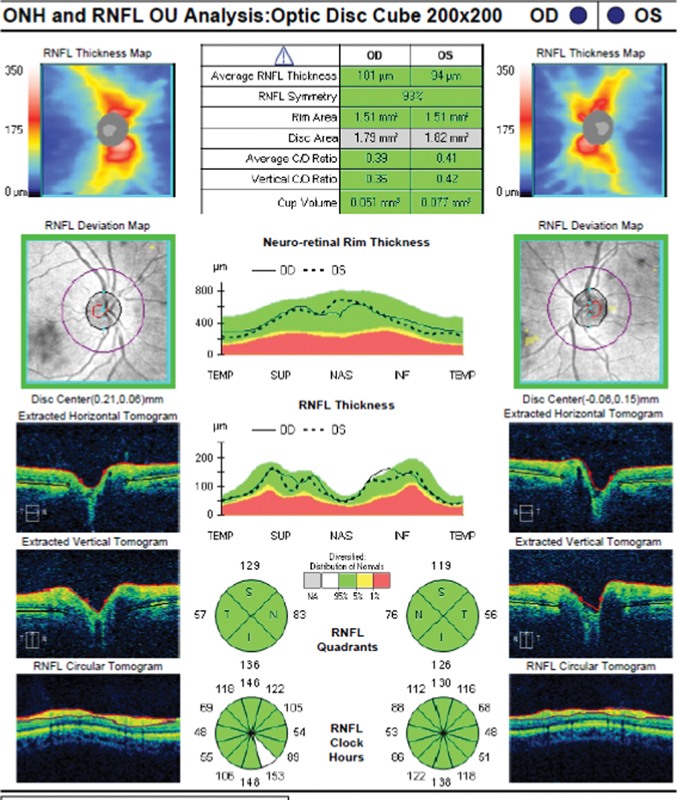
Optical coherence tomography of normal optic nerve heads (ONH) and retinal nerve fiber layer (RNFL)—the cross-sectional thickness of the RNFL is measured in microns, 360 degrees around each optic nerve head.
Fig. 9.
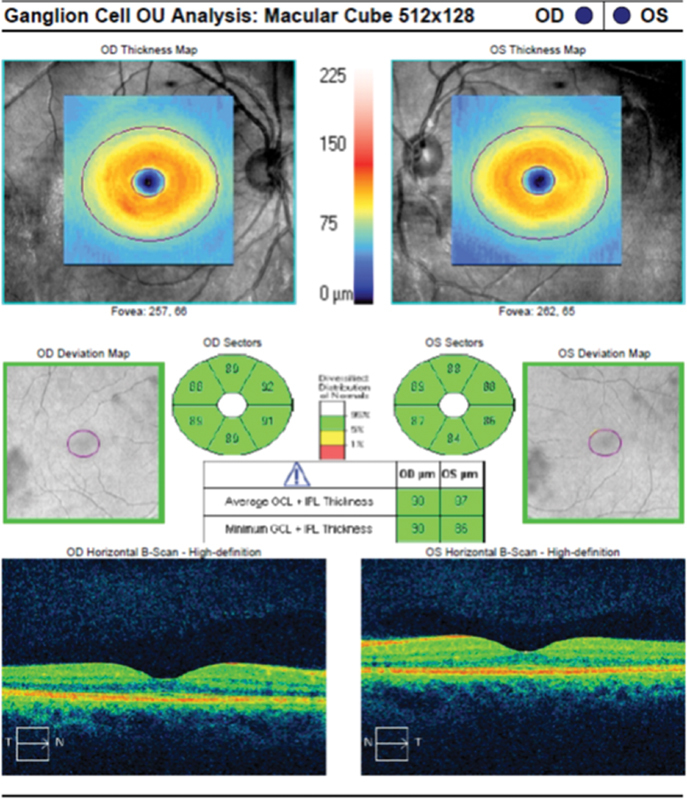
Optical coherence tomography of normal maculae, with measurement of the retinal ganglion cell layer thickness in microns.
Ophthalmic echography, performed by a skilled echographer, may also be a useful adjunctive test. It is more sensitive than computed tomography (CT) or MRI in the assessment of intraocular, retinal, or subretinal disease processes, and is additive to CT or MRI of the orbit in characterization of orbital disease. If CT or MRI has been used in the initial evaluation of an orbital abscess or mid- or anterior orbital inflammatory disease, such as posterior scleritis, serial B-mode echography is adequate in assuring response to treatment, thus minimizing the need for serial CT or MRI. 17 If CT or MRI has identified a mid- or anterior orbital tumor or infiltrative process, adjunctive echography is helpful in assessment of the internal acoustic characteristics of the lesion, in that lymphoma, melanoma, and cysts have no or low internal reflectivity, and other processes have mid- (such as schwannoma) to high internal reflectivity (such as many carcinomas or cavernous hemangioma). 18 Echography also allows for real-time dynamic assessment of adherence or infiltration of tumorous processes to adjacent tissues. B-mode echography is also a useful tool for image-guided fine needle aspiration biopsy (FNAB) of mid-orbital tumors, which is especially useful in the identification of metastatic tumor deposits, allowing definitive diagnosis without necessity of open biopsy. FNAB may also aid in evaluation of lacrimal gland masses, often allowing a cytopathologic diagnosis of inflammation, lymphoma, pleomorphic adenoma, or carcinoma, allowing planning of more definitive treatment without the need for an incision biopsy.
The Multidisciplinary Team
FNAB should be conducted by an experienced orbital specialist, ideally with the team cytopathologist at his or her side to immediately handle and microscopically evaluate the aspirate, and to guide whether or not additional passes may be required to best arrive at a tissue diagnosis. Some pathologists may not be well acquainted with typical orbital pathologic processes and may benefit through a closer clinical relationship with the orbital surgical team, and/or solicitation of tissue evaluation by more experienced colleagues; this holds true for incisional and excisional biopsies, as well as FNABs.
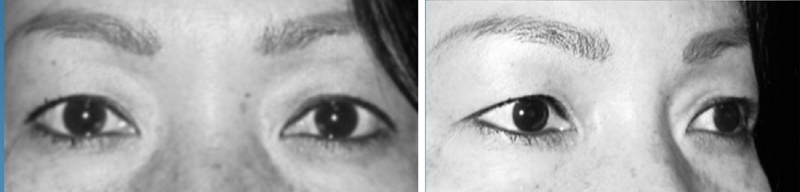
TED is the number one cause of proptosis, unilateral or bilateral. In most cases, a confident clinical diagnosis may be made without the need of an orbital imaging study ( Fig. 10 ). In severe TED with compressive optic neuropathy, or in stable, fibrotic TED with residual proptosis, noncontrast orbital CT is useful for surgical planning of orbital decompression. TED patients should be comanaged by an ophthalmologist and an endocrinologist who will maintain euthyroidism and avoid use of radioactive iodine.
Fig. 10.
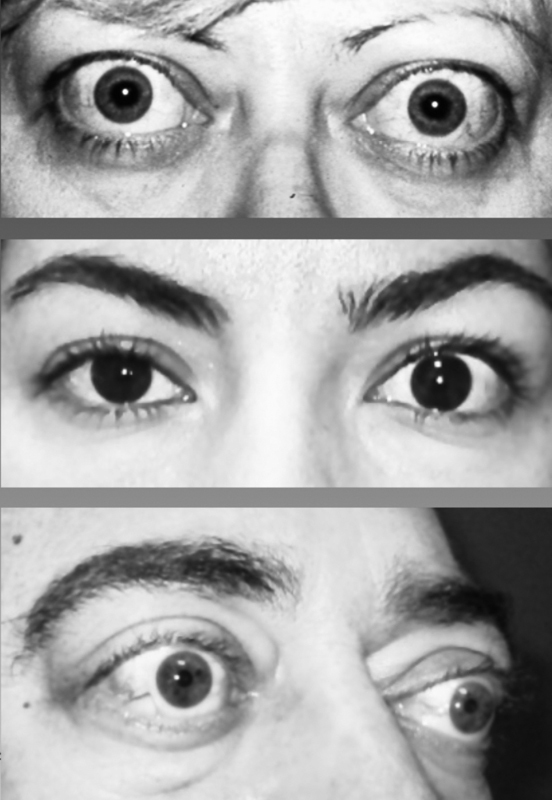
These three unrelated patients presented with histories and findings allowing secure diagnoses of thyroid eye disease, without need for orbital echography, computed tomography, or magnetic resonance imaging.
Lesions which displace the globe or extend to the mid- or posterior orbit should be assessed by orbital MRI with and without contrast. If the orbital MRI reveals associated sinonasal or intracranial disease, appropriate otolaryngologic and/or neurosurgical consultations should be obtained, following which further evaluation and management should be team based.
Whether the orbital disorder will be observed, treated medically, and/or operated, the orbital specialist's service does not end at the completion of any surgery. Acute and convalescent postoperative care is important to minimize complications and optimize outcomes. Continued involvement in the monitoring and treatment of the patient is of benefit to the whole team, and, ultimately, to the patient.
Assessment and Plan
An adequate clinical neuro-ophthalmologic examination narrows the differential diagnosis for a given patient, facilitating a more focused selection of diagnostic testing. For example, most patients with a secure clinical diagnosis of TED, with no clinical evidence of compressive optic neuropathy do not require orbital imaging; the focus of medical attention may remain on assessment and treatment of associated thyroid disorders and management of the orbital disease, which may include treatment with teprotumumab. 19
Illustrative Cases
Case 1
A 39-year-old woman visited an optometrist with a complaint of 1 year of progressive left frontal headache and left cheek pain. Uncorrected visual acuity was 20/20 oculus dexter (OD) and 20/80 oculus sinister (OS). Refraction was plano (zero) OD and +3.00 OS, which improved the visual acuity to 20/25. The headache and periorbital pain were attributed to the refractive difference; a contact lens was prescribed for the left eye, and the patient's symptoms were resolved. At follow-up, 1 year later, the optometrist noted mild anisocoria and “indistinct borders” around the left optic nerve, and the patient was referred for neuro-ophthalmic consultation; 3 mm of left axial proptosis was measured by exophthalmometry, as well as mild anisocoria, left pupil larger than right ( Fig. 11 ). A left RAPD was found. There was mild discomfort and diplopia in upgaze, in association with mild restriction of left supraduction. Quantitative perimetry (visual field testing) demonstrated mild relative generalized depression of sensitivity of the left eye (OS) ( Fig. 12 ). Ophthalmoscopy revealed normal findings OD and swelling of the left optic nerve ( Fig. 13 ). OCT demonstrated moderate thickening of the RNFL OS, secondary to optic nerve head edema ( Figs. 14 and 15 ). OCT of the RGC layer demonstrated normal findings ( Fig. 16 ), suggestive of a good prognosis for recovery of good vision with effective treatment, as well as choroidal folds ( Fig. 17 ). MRI ( Fig. 18 ) revealed an enhancing 2 cm diameter left intraconal mass, inferior to the optic nerve, isointense with brain on T1, and bright on T2. There was expansion of the left bony orbit, consistent with and suggestive of chronicity. Dynamic B-mode echography in office demonstrated high internal reflectivity, and easy mobility of the rectus muscles and optic nerve over the surface of the mass, consistent with a noninvasive and nonadherent nature. The mass was removed by lateral orbitotomy with no postoperative morbidity. Tissue diagnosis was cavernous hemangioma.
Fig. 11.

The patient had been unaware of mild left proptosis and anisocoria.
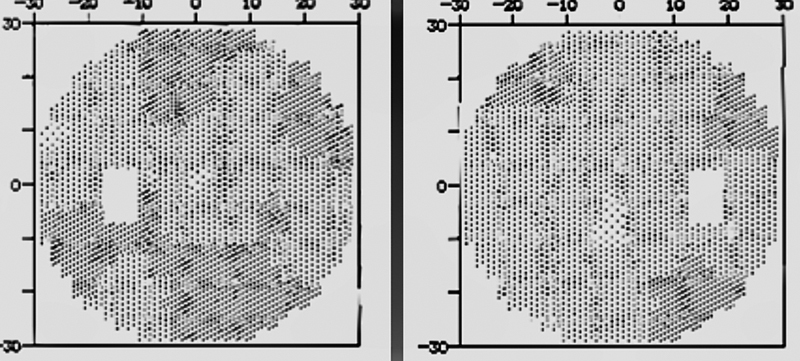
Fig. 12.
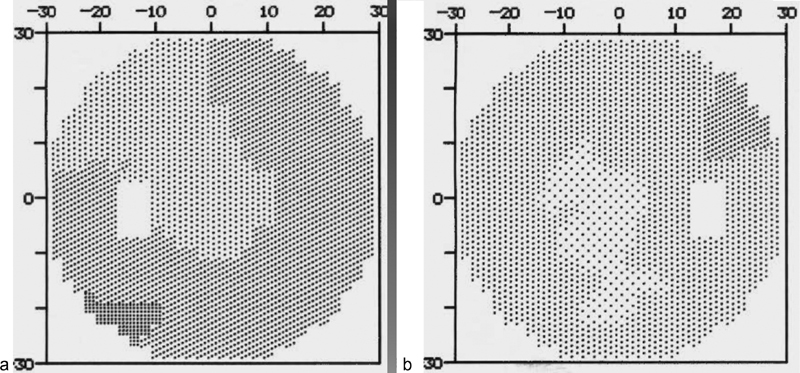
Quantitative perimetry demonstrated ( a ) visual field of the left eye; ( b ) mild relative generalized depression of sensitivity of the left eye.
Fig. 13.
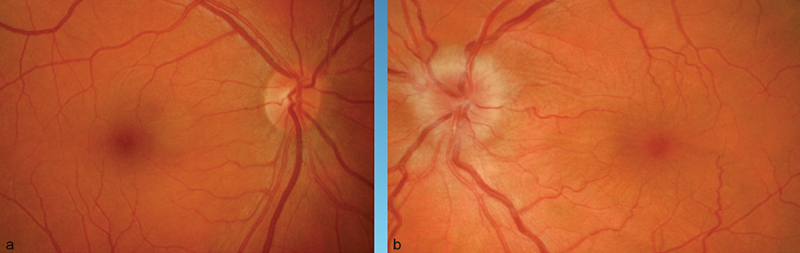
Ophthalmoscopy revealed normal findings OD ( a ) and swelling of the left optic nerve ( b ).
Fig. 14.
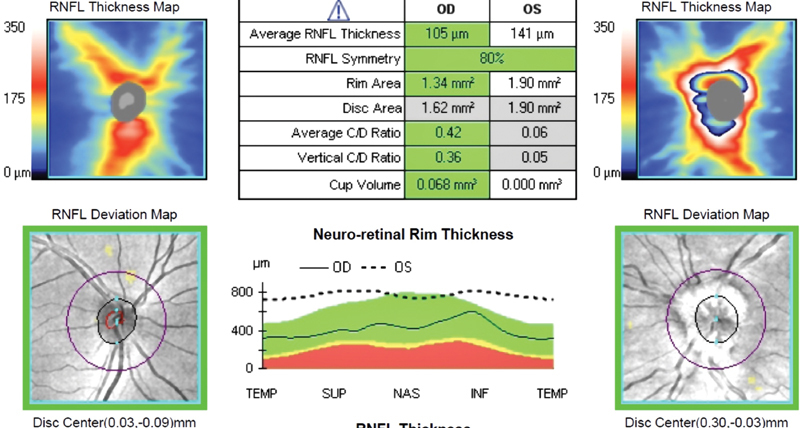
Optical coherence tomography demonstrated moderate thickening of the retinal nerve fiber layer (RNFL) OS, secondary to optic nerve head edema.
Fig. 15.
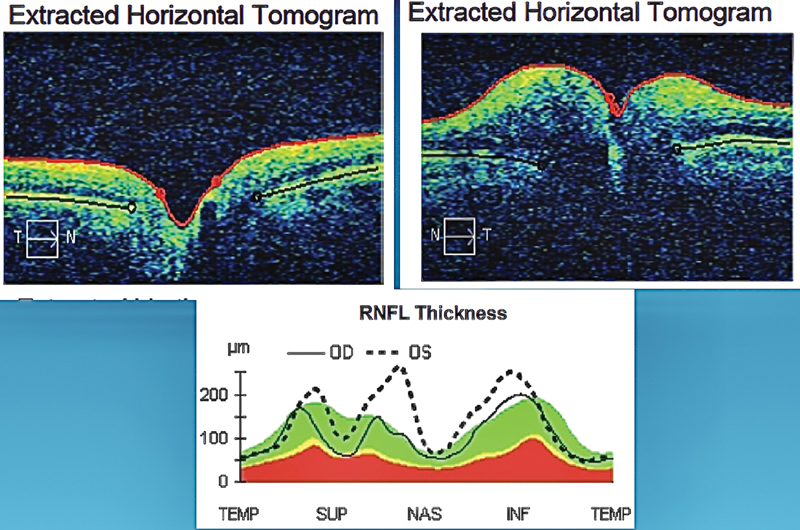
Optical coherence tomography demonstrated the cross-sectional swelling of the left optic nerve head, as well as thickening of the retinal nerve fiber layer (RNFL).
Fig. 16.
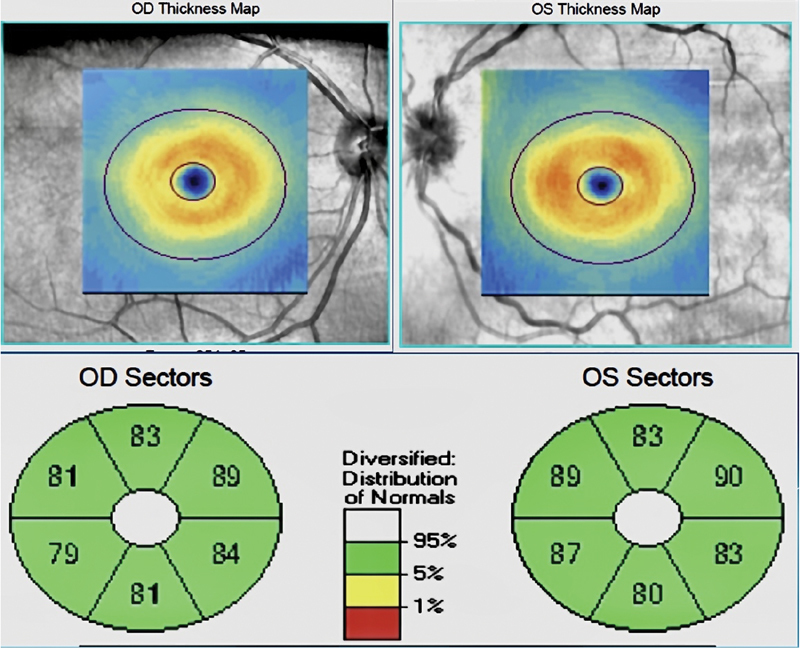
Optical coherence tomography of the retinal ganglion cell layer demonstrated normal findings, suggestive of a good prognosis for recovery of good vision with effective treatment.
Fig. 17.
Optical coherence tomography (OCT) further revealed choroidal folds OS, consistent with compression of the posterior aspect of the globe. The choroidal folds were more evident in OCT than in ophthalmoscopy or fundus photography.
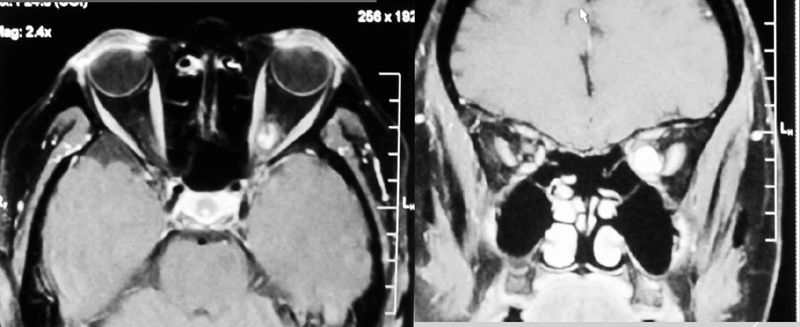
Fig. 18.
Magnetic resonance imaging revealed a large left intraconal mass, inferior to the optic nerve, isointense with brain on T1 and enhancing homogenously. There was expansion of the left bony orbit, consistent with and suggestive of chronicity.
Case 2
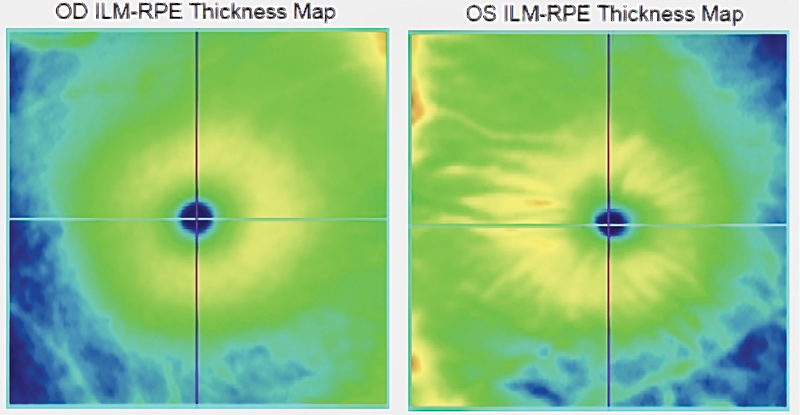
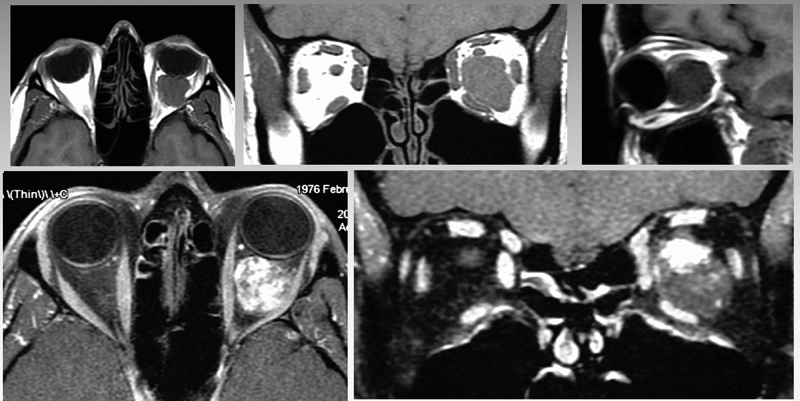
A 47-year-old woman was aware of diminishing vision of the left eye for 1 year, which was rapidly worsening over 3 months prior to presentation. She noted intermittent mild pain of the left eye, especially when flying ( Fig. 19 ). Visual acuity was 20/25 OD and 20/50 OS. There was no proptosis, no enophthalmos, and no hyper- or hypoglobus. She was orthophoric in all gaze positions and ductions were full. There was a moderate left RAPD. Findings on slit lamp biomicroscopy and ophthalmoscopy were normal, with neither optic atrophy nor optic nerve head edema evident. Quantitative perimetry ( Fig. 20 ) revealed marked depression of sensitivity OS, especially in the temporal visual field. Although OCT revealed the RNFL thickness ( Fig. 21 ) to be “normal,” there was a significant relative thinning OS in comparison to OD. MRI ( Fig. 22 ) demonstrated an intraconal posterior orbital apex mass, inferior to the optic nerve, avidly enhancing with contrast. The mass ( Fig. 23 ) was removed in entirety by a transnasal endoscopic route and found to be a cavernous hemangioma. There was a near complete recovery of vision, with only mild generalized depression of sensitivity evident in quantitative perimetry performed 2 weeks postoperatively ( Fig. 24 ).
Fig. 19.
A 47-year-old woman complained of progressive loss of vision, OS.
Fig. 20.
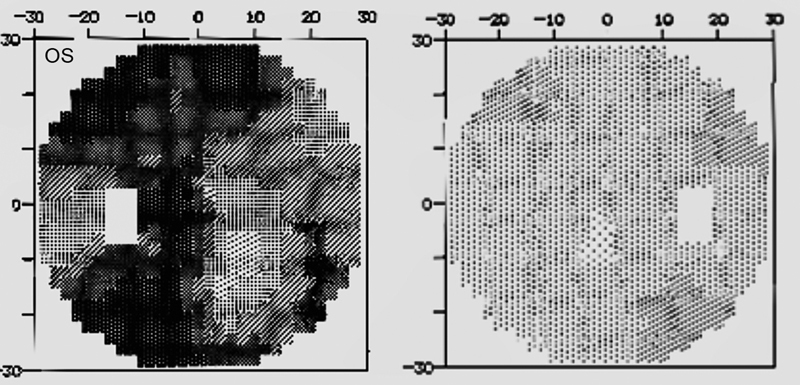
Quantitative perimetry revealed marked depression of sensitivity OS, especially in the temporal visual field.
Fig. 21.
Although the retinal nerve fiber layer (RNFL) thickness was “normal,” there was a significant relative thinning oculus sinister (OS) in comparison to oculus dexter (OD). ONH, optic nerve heads.
Fig. 22.
Magnetic resonance imaging demonstrated an intraconal posterior orbital apex mass, inferior to the optic nerve, avidly enhancing with contrast.
Fig. 23.

The mass was removed in entirety and found to be a cavernous hemangioma.
Fig. 24.
There was a near complete recovery of vision, with only mild generalized depression of sensitivity evident in quantitative perimetry performed 2 weeks postoperatively.
Conclusion
Many—perhaps most–patients with orbital disease do not require surgery. Even for those for whom surgery is the best course of action, adequate clinical evaluation by a neuro-ophthalmologist or orbital surgeon narrows the differential diagnosis, aids in surgical planning, and is of great value in improving the accuracy of the preoperative risk–benefit analysis associated with informed consent. The preoperative clinical evaluation also establishes baseline for a variety of measures which may be quantitatively and objectively reassessed postoperatively. In those cases where decline in form or function is documented over time, an objective impetus for intervention by surgical, radiotherapeutic, or medical means may be established.
Funding Statement
Funding None.
Footnotes
Conflict of Interest None declared.
Pearls and Tips.
“It takes a village” - include medical and surgical neuro-ophthalmology and/or oculoplastic surgery in your multidisciplinary skull base team.
Meet with your team to develop a standardised methodology of evaluation a standardized methodology of evaluation.
Valuable ancillary testing includes, but is not limited to, automated perimetry, optical coherence tomography, fundus photography and orbital echography.
In some cases, orbital fine needle aspiration biopsy (FNAB) may obviate the need for open surgery, or may aid in surgical planning.
Not every orbital disease calls for a surgical “solution”.
References
- 1.McLaughlin N, Carrau R L, Kelly D F, Prevedello D M, Kassam A B. Teamwork in skull base surgery: an avenue for improvement in patient care. Surg Neurol Int. 2013;4:36. doi: 10.4103/2152-7806.109527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.African proverb of indeterminate attribution
- 3.Karlin J N, Krauss H R. Ophthalmic and orbital considerations in the evaluation of skull base malignancies. J Neurooncol. 2020;150(03):483–491. doi: 10.1007/s11060-020-03516-6. [DOI] [PubMed] [Google Scholar]
- 4.Scheuerle A F, Steiner H H, Kolling G, Kunze S, Aschoff A. Treatment and long-term outcome of patients with orbital cavernomas. Am J Ophthalmol. 2004;138(02):237–244. doi: 10.1016/j.ajo.2004.03.011. [DOI] [PubMed] [Google Scholar]
- 5.Cruz A AV, Ribeiro S FT, Garcia D M, Akaishi P M, Pinto C T. Graves upper eyelid retraction. Surv Ophthalmol. 2013;58(01):63–76. doi: 10.1016/j.survophthal.2012.02.007. [DOI] [PubMed] [Google Scholar]
- 6.Tanwani L K, Lohano V, Ewart R, Broadstone V L, Mokshagundam S P. Myasthenia gravis in conjunction with Graves' disease: a diagnostic challenge. Endocr Pract. 2001;7(04):275–278. doi: 10.4158/EP.7.4.275. [DOI] [PubMed] [Google Scholar]
- 7.Putterman A M. Margin reflex distance (MRD) 1, 2, and 3. Ophthal Plast Reconstr Surg. 2012;28(04):308–311. doi: 10.1097/IOP.0b013e3182523b7f. [DOI] [PubMed] [Google Scholar]
- 8.Falardeau J. Anisocoria. Int Ophthalmol Clin. 2019;59(03):125–139. doi: 10.1097/IIO.0000000000000276. [DOI] [PubMed] [Google Scholar]
- 9.Christoff A. Sensorimotor characteristics of neuro-ophthalmology and oculo-plastics patients. Am Orthopt J. 2015;65:47–57. doi: 10.3368/aoj.65.1.47. [DOI] [PubMed] [Google Scholar]
- 10.Liebermann L, Leske D A, Hatt S R, Holmes J M. Test-retest variability of cyclodeviations measured using the double Maddox rod test. J AAPOS. 2018;22(02):146–1480. doi: 10.1016/j.jaapos.2017.09.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Metz H S. Forced duction, active force generation, and saccadic velocity tests. Int Ophthalmol Clin. 1976;16(03):47–73. [PubMed] [Google Scholar]
- 12.Metz H S. Restrictive factors in strabismus. Surv Ophthalmol. 1983;28(02):71–83. doi: 10.1016/0039-6257(83)90075-9. [DOI] [PubMed] [Google Scholar]
- 13.Krauss H R, Kennerdell J S. Orbital disease: dural-cavernous sinus fistula. Clinical Decisions in Ophthalmology. 1983;7:4–9. [Google Scholar]
- 14.Griffiths C F, Krauss H R. Transnasal endoscopic image-guided orbital apex surgery. Skull Base. 2008;18:A208. [Google Scholar]
- 15.Sibony P A, Kennerdell J S, Slamovits T L, Lessell S, Krauss H R. Intrapapillary refractile bodies in optic nerve sheath meningioma. Arch Ophthalmol. 1985;103(03):383–385. doi: 10.1001/archopht.1985.01050030079026. [DOI] [PubMed] [Google Scholar]
- 16.Sibony P A, Krauss H R, Kennerdell J S, Maroon J C, Slamovits T L. Optic nerve sheath meningiomas. Clinical manifestations. Ophthalmology. 1984;91(11):1313–1326. doi: 10.1016/s0161-6420(84)34148-3. [DOI] [PubMed] [Google Scholar]
- 17.Mair M H, Geley T, Judmaier W, Gassner I. Using orbital sonography to diagnose and monitor treatment of acute swelling of the eyelids in pediatric patients. AJR Am J Roentgenol. 2002;179(06):1529–1534. doi: 10.2214/ajr.179.6.1791529. [DOI] [PubMed] [Google Scholar]
- 18.Byrne S R, Glaser J S. Orbital tissue differentiation with standardized echography. Ophthalmology. 1983;90(09):1071–1090. doi: 10.1016/s0161-6420(83)80050-5. [DOI] [PubMed] [Google Scholar]
- 19.Douglas R S, Kahaly G J, Patel A. Teprotumumab for the treatment of active thyroid eye disease. N Engl J Med. 2020;382(04):341–352. doi: 10.1056/NEJMoa1910434. [DOI] [PubMed] [Google Scholar]