

Highlights
-
•
Eight weeks of hamstring flexibility exercises significantly increased hamstring optimal musculotendinous lengths and, thus, decreased peak hamstring musculotendinous strains in male athletes during sprinting.
-
•
Eight weeks of hamstring concentric and eccentric strength exercises also significantly increased hamstring optimal musculotendinous lengths and, thus, decreased peak hamstring musculotendinous strains in male athletes during sprinting.
-
•
The hamstring optimal musculotendinous lengths should be used as measures of the ability of being stretched in hamstring musculotendinous units in future studies of hamstring injury.
-
•
Flexibility straining and strength training may decrease the risk of hamstring injury.
Keywords: Hamstring injury, Injury mechanism, Injury prevention, Modifiable risk factors, Muscle biomechanics
Abstract
Background
Hamstring injury is one of the most common injuries in sports involving sprinting. Hamstring flexibility and strength are often considered to be modifiable risk factors in hamstring injury. Understanding the effects of hamstring flexibility or strength training on the biomechanics of the hamstring muscles during sprinting could assist in improving prevention strategies and rehabilitation related to these injuries. The purpose of this study was to determine the effects of altering hamstring flexibility or strength on peak hamstring musculotendinous strain during sprinting.
Methods
A total of 20 male college students (aged 18–24 years) participated and were randomly assigned to either a flexibility intervention group or a strength intervention group. Each participant executed exercise training 3 times a week for 8 weeks. Flexibility, sprinting, and isokinetic strength testing were performed before and after the 2 interventions. Paired t tests were performed to determine hamstring flexibility or strength intervention effects on optimal hamstring musculotendinous lengths and peak hamstring musculotendinous strains during sprinting.
Results
Participants in the flexibility intervention group significantly increased the optimal musculotendinous lengths of the semimembranosus and biceps long head (p ≤ 0.026) and decreased peak musculotendinous strains in all 3 bi-articulate hamstring muscles (p ≤ 0.004). Participants in the strength-intervention group significantly increased the optimal musculotendinous lengths of all 3 hamstring muscles (p ≤ 0.041) and significantly decreased their peak musculotendinous strain during sprinting (p ≤ 0.017).
Conclusion
Increasing hamstring flexibility or strength through exercise training may assist in reducing the risk of hamstring injury during sprinting for recreational male athletes.
Graphical abstract
1. Introduction
Hamstring muscle strain injury (hamstring injury) is one of the most common non-contact injuries with both short- and long-term consequences in sports that involve sprinting and kicking.1, 2, 3 This injury often causes significant time loss from competition and training,4,5 which not only impairs athletes’ sports performance6,7 but also results in tremendous financial burdens to sports organizations and to society.4 Some studies have found that the hamstring injury rate is increasing or remains unchanged,8 indicating a need for increasing efforts in research into prevention and rehabilitation.
Although hamstring flexibility and strength are often considered to be modifiable risk factors for hamstring injury,9, 10, 11, 12, 13 the literature on their roles in altering the risk of injury are still conflicting. Several epidemiological studies found significant effects of flexibility on the risk for hamstring injury.10,12 On the other hand, at least 3 prospective studies found no such effects.13, 14, 15 Similarly, several studies found significant effects of hamstring strength on the risk for hamstring injury,13,16,17 while the findings from other studies were inconclusive on this point, regardless of whether the hamstring strength was concentric or eccentric.10,18
Recent studies of hamstring muscle biomechanics provide a different view of flexibility and strength as risk factors for hamstring injury. Most studies suggest that the direct cause of muscle strain injury is excessive tissue strain.19, 20, 21 Muscle strain is defined as the ratio of muscle elongation to muscle optimal length.22 We recently reported a significant correlation between hamstring flexibility score, represented by the range of hip flexion in the passive straight leg raise test, and hamstring optimal musculotendinous lengths, at which hamstring muscles generate maximal isometric forces.23 In a follow-up study,24 we further demonstrated that peak hamstring musculotendinous strains during sprinting were negatively correlated with the hamstring flexibility score and optimal musculotendinous lengths. Taken together, these results suggest that hamstring optimal musculotendinous length may be a measure of risk for hamstring injury in individuals. Our recent intervention study demonstrated that improving hamstring flexibility scores and strength significantly increased hamstring optimal musculotendinous length for males but not for females.25 However, the effects of hamstring flexibility and strength intervention on peak hamstring musculotendinous strains during sprinting are still unknown.
This study was, therefore, designed to determine the effects of hamstring flexibility and strength training on peak hamstring musculotendinous strains during sprinting for male reactional athletes. We hypothesized that 8 weeks of hamstring flexibility training would significantly increase the optimal musculotendinous lengths and decrease the peak musculotendinous strains of 3 bi-articulated hamstring muscles during sprinting in male recreational athletes. We also hypothesized that 8 weeks of hamstring strength training would also significantly increase the optimal musculotendinous lengths and decrease peak musculotendinous strains of 3 bi-articulated hamstring muscles during sprinting for male recreational athletes.
2. Methods
2.1. Participants
A total of 28 male college students regularly participating in exercise and sport activities volunteered to participate in this study. We used G*Power software Version 3.00.10 (Franz Faul, Kiel University, Kiel, Germany) to estimate the sample size for type I error rate (≤0.05), statistical power (≥0.80), and anticipated Cohen d effect size (≥0.40). All subjects had no history of hamstring or other lower-extremity injury prior to participation. Using a block randomization procedure with a block size of 4 (Table 1), participants were randomly assigned to either a flexibility intervention group or a strength intervention group. A block was randomly picked by the 4th author (HL) for every 4 incoming participants. The assignment of each participant was revealed after the participant signed the consent. Each participant signed a written consent prior to any data collection or study participation. The consent form included information contained in the Helsinki Declaration as well as the purpose of the study and details about the study's protocols. The use of human subjects in this study was approved by the Institutional Review Board of Beijing Sport University (IRB approval ID #2016001H).
Table 1.
Descriptions of participants (mean ± SD).
| Group | n | Age (year) | Body mass (kg) | Standing height (cm) | Weekly physical activity (h) |
|---|---|---|---|---|---|
| Flexibility intervention | 10 | 20.6 ± 1.6 | 70.5 ± 5.2 | 178.9 ± 3.7 | 7.8 ± 2.5 |
| Strength intervention | 10 | 20.9 ± 1.9 | 66.0 ± 5.9 | 174.3 ± 5.1 | 7.6 ± 2.2 |
2.2. Procedures
The procedures for this study included a pre-intervention test, 8 weeks of intervention, and a post-intervention test. In each of the pre- and post-intervention evaluations, the participant was administered a sprinting test to collect lower-extremity, three-dimensional (3-D) kinematic data for each leg. The sprinting test was followed by an isokinetic strength test to collect knee isokinetic moment data as a function of knee joint angle.
2.2.1. Sprinting test
A total of 19 passive reflective markers were placed bilaterally on each participant's lower extremity, including the anterior superior iliac spine, top of the crista iliac, lateral and medial femur condyles, lateral and medial malleolus, tibial tuberosity, and middle of the 2nd and the 3rd metatarsals. An additional marker was attached at the junction of the 4th and 5th lumbar spine vertebra (L4 and L5). The markers on the medial femur condyles and malleolus were removed after a standing calibration. Using a standing-start technique, each participant then completed 3 sprinting trials with maximum effort for each leg, with 2 min of rest between consecutive trials. The distance from the starting line to the finish line was 40 m, with the data collection area in the middle 15 m. The 3-D coordinates of the reflective markers in each sprinting trial were recorded using a videographic data collection system (Raptor-4; Motion Analysis, Santa Rosa, CA, USA) comprising 12 cameras with a sampling rate of 200 frames/s.
2.2.2. Isokinetic strength test
After the sprinting test, each participant was seated on an IsoMed2000 isokinetic device (D&R Ferstl, Hemau, Germany) with the reflective markers still attached. The thigh and lower leg of the testing leg were secured on the seat and the dynamometer arm, respectively, with the hip flexed at 90°. The participant had 3 concentric isokinetic maximum knee flexion tests at an angular velocity of 10°/s for each leg to mimic isometric contraction, since muscle optimal length is referred to as the muscle length and corresponds to the maximum muscle isometric contraction force.26 The 3-D coordinates of the reflective markers in each trial of isokinetic strength were recorded by using a videographic data collection system (Oqus 400; Qualisys, Gothenburg, Sweden), with 12 cameras operating at a sampling rate of 100 frames/s. Knee flexion torque data were recorded at a sampling rate of 100 Hz and time-synchronized with videographic data collection using a MegaWin 2.4 system (Mega Electronics, Kuopio, Finland).
2.2.3. Interventions
Participants in each experimental group had 3 intervention sessions per week for 8 weeks, with at least 36 h between sessions. In each session, the participants had 6 min of standardized warm-up involving a series of dynamic exercises. Participants in the flexibility intervention group performed a series of static, dynamic, and proprioceptive neuromuscular facilitation stretches (Table 2) (Supplementary Fig. 1). Participants in the strength intervention group performed concentric as well as eccentric strengthening exercises (Table 2) (Supplementary Fig. 2). All interventions used in our study were based on recommendations by the National Strength and Conditioning Association27 and were carried out under the direction of a certified personal trainer. All participants were instructed to maintain their current level of physical activity and avoid any exercises specifically designed to improve hamstring flexibility or strength while participating in the study.
Table 2.
Exercises in each intervention group.
| Group | Week | Exercises (30-s rest between sets, 1-min rest between exercises) | |||
|---|---|---|---|---|---|
| Flexibility intervention | 1 | Walking knee lift (15 reps × 2 sets) |
Sitting toe touch (40 s/leg × 2 sets) |
PNF stretch (50 s/leg × 3 sets) |
Foam roll (40 s/leg × 3 sets) |
| 2–4 | Forward lunge (15 reps × 2 sets) |
Sitting toe touch (50 s/leg × 3 sets) |
PNF stretch (50 s/leg × 3 sets) |
Foam roll (50 s/leg × 1 set) |
|
| 5–8 | Forward lunge (15 reps × 2 sets) |
Semi-straddle (60 s/leg × 2 sets) |
PNF stretch (50 s/leg × 3 sets) |
Foam roll (50 s/leg × 1 set) |
|
| Strength intervention | 1 | NHC with bend (8 reps × 3 sets) |
Prone hamstrings curl (12 reps/leg × 4 sets) |
Physio-ball leg curl (8 reps × 3 sets) |
Glute bridge (50 s/leg × 2 sets) |
| 2–4 | NHC with bend (12 reps × 3 sets) |
Prone hamstrings curl (14 reps/leg × 3 sets) |
Physio-ball leg curl (10 reps × 3 sets) |
Glute bridge (50 s/leg × 2 sets) |
|
| 5–8 | NHC (12 reps × 3 sets) |
Prone hamstrings curl (15 reps/leg × 3 sets) |
Physio-ball roll (10 reps/leg × 2 sets) |
Glute bridge (60 s/leg × 2 sets) |
|
Abbreviations: NHC = Nordic hamstring curl; PNF = proprioceptive neuromuscular facilitation; reps = repetitions.
2.3. Data reduction
The raw 3-D trajectories of reflective markers in isokinetic strength testing were smoothed using a Butterworth low-pass filter at a cutoff frequency of 10 Hz to reduce random noise.28 Musculotendinous lengths of a given hamstring muscle were determined as the distances between the origin and the insertion of the muscle. The instantaneous force of each hamstring muscle was calculated from instantaneous knee-flexion-moment data, physiological cross-sectional areas, and the moment arms of each muscle. Calculations of hamstring musculotendinous lengths and forces have been described in detail in previous studies.23,29 The optimal musculotendinous length of each biarticulated hamstring muscle was identified as the musculotendinous length at which the calculated muscle force of the given hamstring muscle was maximum.
The 3-D trajectories of reflective markers in sprinting were digitally low-pass filtered at 13 Hz.28 Instantaneous musculotendinous lengths of the 3 bi-articulated hamstring muscles were calculated as previously described. Instantaneous musculotendinous strain (εt) of each of the 3 bi-articulated hamstring muscles of a given leg were calculated as:
where Lt and L0 were instantaneous musculotendinous length and optimal musculotendinous length, respectively.24
A running-step cycle was defined as the duration between 2 consecutive foot strikes. The time of a foot strike was defined as the time represented by the first frame in which any part of the foot was in contact with the ground. Sprinting speed was defined as the averaged horizontal velocity of the L4–L5 marker during the running step cycle in which data were collected. Step length was defined as the horizontal distance between the toes at 2 consecutive foot strikes. Step frequency was defined as the inverse of the time between 2 consecutive foot strikes. Peak musculotendinous strains of each bi-articulated hamstring muscle in each step cycle were identified for the swing leg.
2.4. Statistical analyses
Between-participant coefficients of multiple correlation (CMC) and within-participant relative errors30,31 in hamstring optimal musculotendinous length and peak musculotendinous strains were calculated before and after the interventions to evaluate the between- and within-participant reliability of estimated peak strains. To test our hypotheses, the optimal musculotendinous lengths and peak musculotendinous strains of 3 bi-articulated hamstring muscles of the flexibility and strength intervention groups were compared between pre- and post-intervention by using paired t tests. Sprinting speed, step length, and step frequency were also compared between pre- and post-intervention by using paired t tests. All statistical analyses were performed using SPSS Version 18.0 software (SPSS, Chicago, IL, USA). A type I error rate no greater than 0.05 was chosen as an indication of statistical significance.
3. Results
All participants completed the study as requested. Four participants in each group, however, had incomplete data due to equipment errors in data collection. The means of between-participant CMCs and within-participant relative errors of the estimated hamstring optimal musculotendinous lengths before and after the interventions were no less than 0.84% and no greater than 1.76%, respectively (Table 3). The means of between-participant CMCs and within-participant relative errors of the peak hamstring musculotendinous strains during sprinting before and after the interventions were no less than 0.96% and no greater than 1.03%, respectively (Table 3).
Table 3.
The reliability of hamstring optimal musculotendinous lengths and peak musculotendinous strains.
| Variable | Muscle | Pre-intervention |
Post-intervention |
||
|---|---|---|---|---|---|
| Error (mean ± SD, %) | CMC | Error (mean ± SD, %) | CMC | ||
| Optimal musculotendinous length | Semitendinosus | 1.47 ± 1.61 | 0.88 | 1.31 ± 1.28 | 0.89 |
| Semimembranosus | 1.76 ± 1.75 | 0.84 | 1.54 ± 1.44 | 0.85 | |
| Biceps long head | 1.69 ± 1.60 | 0.90 | 1.69 ± 1.49 | 0.85 | |
| Peak musculotendinous strain | Semitendinosus | 0.84 ± 0.53 | 0.98 | 0.85 ± 0.60 | 0.96 |
| Semimembranosus | 1.03 ± 0.70 | 0.98 | 0.85 ± 0.60 | 0.97 | |
| Biceps long head | 0.81 ± 0.49 | 0.99 | 0.91 ± 0.62 | 0.97 | |
Abbreviation: CMC = coefficients of multiple correlation.
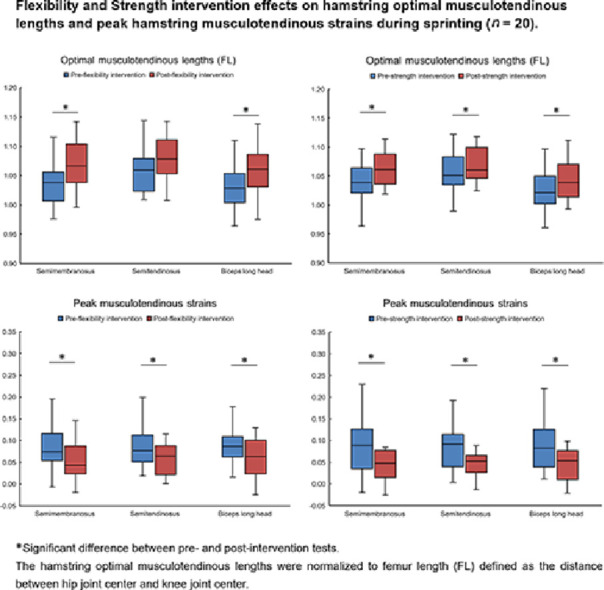
In the flexibility intervention group, the hamstring flexibility score significantly increased in the post-intervention test in comparison to the pre-intervention test (p = 0.001), while hamstring strength was not significantly changed in the post-intervention test (p = 0.393) (Table 4) (Supplementary Figs. 3 and 4). The optimal musculotendinous lengths of the semimembranosus and biceps long head were significantly increased in the post-intervention test (p = 0.011, p = 0.026), whereas there was no significant increase in the optimal musculotendinous length of semitendinosus after the intervention (p = 0.060) (Table 4) (Supplementary Fig. 7). Peak musculotendinous strain of the semitendinosus (p = 0.004), semimembranosus (p = 0.002), and biceps long head (p = 0.004) significantly decreased in the post-intervention test (Table 4) (Supplementary Fig. 8). No significant difference was observed in sprinting speed (p = 0.599), step length (p = 0.674), or step frequency (p = 0.539) between pre- and post-intervention tests (Table 4) (Supplementary Figs. 9–11).
Table 4.
Intervention effects on hamstring flexibility score, strength, optimal musculotendinous lengths, sprinting speed, step length and frequency, and peak hamstring musculotendinous strains in sprinting for the flexibility intervention group (n = 20) (mean ± SD).
| Variable | Pre-intervention | Post-intervention | Difference | 95%CI | p | Cohen d |
|---|---|---|---|---|---|---|
| Hamstring flexibility score (o) | 96.7 ± 10.3 | 114.5 ± 12.7 | 17.8 ± 9.2 | 13.5 to 22.1 | 0.001 | 2.00 |
| Hamstring strength (N·m) | 142.0 ± 40.9 | 140.5 ± 31.1 | –1.5 ± 25.0 | –13.3 to 10.2 | 0.393 | 0.06 |
| Semitendinosus optimal musculotendinous length (FL) | 1.06 ± 0.04 | 1.08 ± 0.04 | 0.02 ± 0.05 | 0.00 to 0.04 | 0.060 | 0.37 |
| Semimembranosus optimal musculotendinous length (FL) | 1.04 ± 0.04 | 1.07 ± 0.04 | 0.03 ± 0.05 | 0.01 to 0.05 | 0.011 | 0.58 |
| Biceps long head optimal musculotendinous length (FL) | 1.04 ± 0.04 | 1.06 ± 0.05 | 0.02 ± 0.05 | 0.00 to 0.05 | 0.026 | 0.47 |
| Sprinting speed (m/s) | 7.49 ± 0.67 | 7.45 ± 0.50 | –0.04 ± 0.36 | –0.21 to 0.13 | 0.599 | 0.12 |
| Step length (m) | 1.95 ± 0.21 | 1.94 ± 0.21 | –0.01 ± 0.14 | –0.08 to 0.05 | 0.674 | 0.10 |
| Step frequency (steps/s) | 4.00 ± 0.33 | 4.04 ± 0.31 | 0.04 ± 0.27 | –0.09 to 0.16 | 0.539 | 0.14 |
| Peak semitendinosus musculotendinous strain | 0.09 ± 0.05 | 0.06 ± 0.04 | –0.03 ± 0.04 | –0.05 to –0.01 | 0.004 | 0.75 |
| Peak semimembranosus musculotendinous strain | 0.09 ± 0.06 | 0.05 ± 0.05 | –0.04 ± 0.05 | –0.06 to –0.02 | 0.002 | 0.83 |
| Peak biceps long head musculotendinous strain | 0.09 ± 0.06 | 0.06 ± 0.05 | –0.04 ± 0.05 | –0.06 to –0.01 | 0.004 | 0.76 |
Note: The hamstring optimal musculotendinous lengths were normalized to FL, defined as the distance between the hip joint center and knee joint center.
Abbreviations: CI = confidence interval; FL = femur length.
In the strength intervention group, the hamstring strength as well as the hamstring flexibility score significantly increased in the post-intervention test compared to the pre-intervention test (p = 0.001, p = 0.037) (Table 5) (Supplementary Figs. 5 and 6). The optimal musculotendinous lengths of all 3 bi-articulated hamstring muscles significantly increased in the post-intervention test (p ≤ 0.041) (Table 5) (Supplementary Fig. 12). The peak musculotendinous strain of all 3 bi-articulated hamstring muscles significantly decreased in the post-intervention test (p ≤ 0.017) (Table 5) (Supplementary Fig. 13). No significant difference was observed in sprinting speed (p = 0.134), step length (p = 0.527), or step frequency (p = 0.265) between pre- and post-intervention tests (Table 5) (Supplementary Figs.14–16).
Table 5.
Intervention effects on hamstring flexibility score, strength, optimal musculotendinous lengths, sprinting speed, step length and frequency, and peak hamstring musculotendinous strains in sprinting for the strength intervention group (n = 20) (mean ± SD).
| Variable | Pre-intervention | Post-intervention | Difference | 95%CI | p | Cohen d |
|---|---|---|---|---|---|---|
| Hamstring flexibility score (o) | 93.6 ± 6.9 | 97.9 ± 11.6 | 4.2 ± 10.0 | –0.5 to 8.9 | 0.037 | 0.43 |
| Hamstring strength (N·m) | 108.8 ± 34.3 | 118.5 ±35.8 | 9.8 ± 12.5 | 3.9 to 15.6 | 0.001 | 0.80 |
| Semitendinosus optimal musculotendinous length (FL) | 1.05 ± 0.05 | 1.07 ± 0.03 | 0.02 ± 0.04 | 0.00 to 0.04 | 0.041 | 0.42 |
| Semimembranosus optimal musculotendinous length (FL) | 1.04 ± 0.04 | 1.06 ± 0.03 | 0.03 ± 0.04 | 0.01 to 0.05 | 0.003 | 0.70 |
| Biceps long head optimal musculotendinous length (FL) | 1.02 ± 0.05 | 1.04 ± 0.03 | 0.02 ± 0.04 | 0.00 to 0.04 | 0.009 | 0.47 |
| Sprinting speed (m/s) | 7.25 ± 0.42 | 7.40 ± 0.60 | 0.15 ± 0.43 | –0.05 to 0.35 | 0.134 | 0.36 |
| Step length (m) | 1.87 ± 0.13 | 1.89 ± 0.15 | 0.02 ± 0.16 | –0.05 to 0.10 | 0.527 | 0.15 |
| Step frequency (steps/s) | 4.10 ± 0.37 | 4.01 ± 0.28 | –0.09 ± 0.37 | –0.27 to 0.08 | 0.265 | 0.26 |
| Peak semitendinosus musculotendinous strain | 0.09 ± 0.07 | 0.05 ± 0.03 | –0.05 ± 0.08 | –0.09 to –0.01 | 0.017 | 0.60 |
| Peak semimembranosus musculotendinous strain | 0.09 ± 0.06 | 0.04 ± 0.03 | –0.05 ± 0.07 | –0.08 to –0.01 | 0.011 | 0.64 |
| Peak biceps long head musculotendinous strain | 0.10 ± 0.07 | 0.05 ± 0.04 | –0.05 ± 0.08 | –0.09 to –0.01 | 0.009 | 0.67 |
Note: The hamstring optimal musculotendinous lengths were normalized to FL defined as the distance between hip joint center and knee joint center.
Abbreviations: CI = confidence interval; FL = femur length.
4. Discussion
4.1. Effects of flexibility and strength training
The results of this study partially support our first hypothesis that 8 weeks of hamstring flexibility exercises significantly increase hamstring optimal musculotendinous lengths and decrease peak musculotendinous strains during sprinting for male recreational athletes. Specifically, our results showed that the optimal musculotendinous lengths of both the semimembranosus and biceps long head significantly increased following the 8 weeks of flexibility training. Furthermore, we showed that the peak musculotendinous strains of all 3 bi-articulated hamstring muscles during sprinting significantly decreased after 8 weeks of flexibility training. In the same group, sprinting speed, step length, and frequency were not significantly changed over the 8 weeks of flexibility exercises. Taken together, these results suggest that the decreases in peak musculotendinous strains of the semimembranosus and biceps long head were due mainly to the increase in optimal musculotendinous lengths of these 2 muscles. Considering the p values and effect sizes, although the increase in the optimal musculotendinous length of semitendinosus after 8 weeks of flexibility training was not statistically significant, it still appears to be the most likely explanation for the decrease in the peak musculotendinous strain of this muscle during sprinting.
Our second hypothesis was that 8 weeks of strength training would increase the optimal musculotendinous lengths of the 3 bi-articulated hamstring muscles, while decreasing the peak musculotendinous strains of these muscles during sprinting. Once again, this hypothesis was partially supported by our findings. Optimal musculotendinous length for all 3 muscles significantly increased after 8 weeks of a strength training intervention, which included concentric as well as eccentric strengthening exercises, while peak musculotendinous strains for all 3 muscles significantly decreased. Interestingly, sprinting speed, step length, and frequency were not significantly changed over the 8 weeks. These results suggest that in this cohort of male recreational athletes, decreases in peak hamstring musculotendinous strains during sprinting were due mainly to the increases in the optimal length of the tissues.
4.2. Optimal musculotendinous lengths
The estimated optimal musculotendinous lengths and peak musculotendinous strains of hamstring muscles had high between-participant CMCs and relatively small within-participant errors. High between-participant CMCs indicate high correlation of a repeated measure across participants, whereas the low within-participant errors indicate a high degree of similarity in a repeated measure across trials. These results suggest an excellent reliability of estimated optimal musculotendinous lengths and peak musculotendinous strains of hamstring muscles in our study.
The optimal musculotendinous lengths of hamstring muscles may be a modifiable risk measure for hamstring injury within an individual as well as across individuals. Several studies have consistently demonstrated that excessive musculotendinous strain of the muscle is a primary cause of muscle-strain injuries.19, 20, 21 Musculotendinous strain of a muscle is the ratio of the musculotendinous length deformation to its optimal length. Therefore, for a given movement, a longer optimal musculotendinous length of the muscle will result in a lower tissue strain for the same deformation. Our previous cross-sectional study demonstrated that peak hamstring musculotendinous strains during sprinting are negatively correlated with the optimal musculotendinous length,24 suggesting that this parameter may be a predictive measure of hamstring injury across individuals. Our current results demonstrated that optimal musculotendinous lengths of hamstring muscles can be increased through both flexibility and strength interventions and that peak musculotendinous strains during sprinting are decreased with these training regimens. Taken together, these combined findings support the idea that the optimal musculotendinous length of hamstring muscles is a modifiable measure of the risk for hamstring strain injury within individuals as well as across individuals, at least for males.
In future studies of hamstring injuries, the optimal musculotendinous lengths of hamstring muscles should be used as a measure of the ability of these muscles to stretch. Several clinical tests have been used commonly for evaluation of hamstring flexibility, including the knee extension angle test, the straight leg raise test, and the sit-and-reach test.32 Knee or hip joint range of motion was used to present the ability of the hamstring muscles to be stretched. Joint range of motion, however, was affected not only by the ability of the hamstring muscles to be stretched but also by joint flexibility and muscle strength.32 This limitation of current clinical tests for hamstring flexibility may have contributed to the inconsistencies in the literature concerning hamstring flexibility as a risk factor for injury. As previously discussed,33 optimal musculotendinous length directly affects tissue strain, with excessive strain being a primary cause of muscle injury.19, 20, 21 The results herein demonstrated that our approach to estimating optimal musculotendinous lengths of the hamstring muscles is reliable and is related to peak musculotendinous strains during sprinting. Accordingly, the use of optimal musculotendinous lengths of the hamstring muscles as an estimate of the ability of these muscles to be stretched should be considered in future studies of hamstring injuries.
4.3. Interventions and injury risk
Strength intervention may be an effective way to reduce the risk of injury. Studies of the mechanism of muscle strain injury demonstrate that muscle force is not the direct cause of muscle strain injury.20,21 A literature review failed to find any study showing that muscle strength is correlated with optimal musculotendinous length or peak musculotendinous strains during movement. Epidemiological studies have yielded conflicting results about the correlation between muscle strength and muscle injury rate. Several studies support the belief that concentric34 and eccentric35 hamstring weakness, together with low ratios of concentric13 or eccentric36 hamstring strength to concentric quadriceps strength, are risk factors for hamstring injury. Some prospective studies have also demonstrated that a hamstring-strengthening program featuring eccentric contraction exercises can reduce the occurrence and severity of hamstring injuries.37,38 In contrast, other studies have found that hamstring strength is not correlated with injury rate.10,39,40 The results of our study, however, demonstrate that strength intervention can increase hamstring optimal musculotendinous lengths and, thus, decrease peak musculotendinous strains during sprinting. Our results are consistent with the literature showing that optimal musculotendinous length increases as muscle strength increases.41, 42, 43, 44 The literature demonstrates that strength training, especially eccentric strength training, can effectively increase muscle fascicle lengths.45,46 The literature also demonstrates that injury strain increases as the energy absorbed by the muscle increases due to increased muscle contraction force.47 The results of our study, combined with previous work, suggest that strength training may be an effective way to reduce the risk of hamstring injury. However, strength may not be an indicator of the relative risk of hamstring injury across individuals. This is likely an explanation for the inconsistencies in the literature concerning strength as a risk factor for hamstring injury.
The present study did not include a control group because it had been demonstrated previously that hamstring flexibility and strength are not improved without specific training.48, 49, 50 In the present study, the 2 experimental groups were instructed to maintain their current level of physical activity and to avoid any exercises specifically designed to improve hamstring flexibility or strength, except for the required intervention programs in our study. Our results showed that the flexibility intervention group did not experience significant changes in strength, and the significant improvements in strength and flexibility of the strength intervention group are consistent with the literature.50, 51, 52 Also, in a previous study, we demonstrated that the optimal musculotendinous lengths of the hamstring muscles are correlated to the flexibility score of the passive straight leg raise test.23 Combined, the results reported in the literature and in our study suggest that the changes in the optimal musculotendinous lengths of the hamstring muscles, as well as the strains of those muscles, are likely to be caused directly by the specific interventions.
4.4. Limitations
Because the present study included only male participants, future studies should investigate the effects of flexibility and strength training on females’ hamstring biomechanics. Increased sample sizes should also be used in future studies in order to confirm the results of our study because the testing of our hypotheses involved a relatively large number of tests, a condition that might have increased the overall probability of type I errors. The retention of the effects of flexibility and strength training on optimal musculotendinous lengths of the hamstring muscles and peak musculotendinous strains in sports activities should be determined in future studies because our study evaluated only the immediate effects of the interventions. Furthermore, the effects of flexibility and strength training on the hamstring injury rate need to be determined in future epidemiological studies. Likewise, future studies should compare the effects of flexibility interventions vs. strength interventions on hamstring biomechanics. Finally, the effects of previous hamstring injuries on optimal musculotendinous lengths of the hamstring muscles should be investigated, given that the literature demonstrates that previous hamstring injuries can have a significant impact on hamstring strength and flexibility.53
5. Conclusion
Increasing hamstring flexibility or hamstring strength through exercise interventions increased optimal musculotendinous lengths of the hamstring muscles and, thus, decreased peak musculotendinous strains during sprinting for male athletes. Future studies of the prevention and rehabilitation of hamstring injuries should investigate the optimal musculotendinous lengths of the hamstring muscles as a measure of the ability of these muscles to be stretched.
Acknowledgments
This study is in memory of our colleague and friend Dr William E. Garrett. This work was partially supported by a research grant from the National Natural Science Foundation of China (Grant No. 81572212) and the Fundamental Research Funds for the Central Universities of China (Grant No. 2019PT015). We also thank Drs Chen Yang and Zhipeng Zhou, as well as Ms Qingman Wei, for their assistance in the collection and reduction of the data used in this study.
Authors’ contributions
XW and SL carried out the experiments, performed the data processing and statistical analysis, and drafted the manuscript; BY and HJL conceived the study, participated in its design and coordination, and helped to draft the manuscript; TMB and HL helped to draft the manuscript. All authors have read and approved the final version of the manuscript, and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Peer review under responsibility of Shanghai University of Sport.
Supplementary material associated with this article can be found in the online version at doi:10.1016/j.jshs.2020.08.001.
Contributor Information
Hanjun Li, Email: lihanjun@bsu.edu.cn.
Bing Yu, Email: byu@med.unc.edu.
Supplementary materials
References
- 1.Elliott MC, Zarins B, Powell JW, Kenyon CD. Hamstring muscle strains in professional football players: a 10-year review. Am J Sports Med. 2011;39:843–850. doi: 10.1177/0363546510394647. [DOI] [PubMed] [Google Scholar]
- 2.Opar DA, Drezner J, Shield A. Acute hamstring strain injury in track-and-field athletes: a 3-year observational study at the Penn Relay Carnival. Scand J Med Sci Sports. 2014;24:254–259. doi: 10.1111/sms.12159. [DOI] [PubMed] [Google Scholar]
- 3.Jones A, Jones G, Greig N. Epidemiology of injury in English professional football players: a cohort study. Phys Ther Sport. 2019;35:18–22. doi: 10.1016/j.ptsp.2018.10.011. [DOI] [PubMed] [Google Scholar]
- 4.Roe M, Murphy JC, Gissane C, Blake C. Hamstring injuries in elite gaelic football: an 8-year investigation to identify injury rates, time-loss patterns and players at increased risk. Br J Sports Med. 2018;52:982–988. doi: 10.1136/bjsports-2016-096401. [DOI] [PubMed] [Google Scholar]
- 5.Macdonald B, McAleer S, Kelly S, Chakraverty R, Johnston M, Pollock N. Hamstring rehabilitation in elite track and field athletes: applying the British Athletics Muscle Injury Classification in clinical practice. Br J Sports Med. 2019;53:1464–1473. doi: 10.1136/bjsports-2017-098971. [DOI] [PubMed] [Google Scholar]
- 6.Røksund OD, Kristoffersen M, Bogen BE. Higher drop in speed during a repeated sprint test in soccer players reporting former hamstring strain injury. Front Physiol. 2017;8:25. doi: 10.3389/fphys.2017.00025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Verrall GM, Kalairajah Y, Slavotinek JP, Spriggins AJ. Assessment of player performance following return to sport after hamstring muscle strain injury. J Sci Med Sport. 2006;9:87–90. doi: 10.1016/j.jsams.2006.03.007. [DOI] [PubMed] [Google Scholar]
- 8.Lu D, McCall A, Jones M. Injury epidemiology in Australian male professional soccer. J Sci Med Sport. 2020;23:574–579. doi: 10.1016/j.jsams.2020.01.006. [DOI] [PubMed] [Google Scholar]
- 9.Cameron M, Adams R, Maher C. Motor control and strength as predictors of hamstring injury in elite players of Australian football. Phys Ther Sport. 2003;4:159–166. [Google Scholar]
- 10.Henderson G, Barnes CA, Portas MD. Factors associated with increased propensity for hamstring injury in English premier league soccer players. J Sci Med Sport. 2010;13:397–402. doi: 10.1016/j.jsams.2009.08.003. [DOI] [PubMed] [Google Scholar]
- 11.Petersen J, Thorborg K, Nielsen MB, Budtz-Jorgensen E, Holmich P. Preventive effect of eccentric training on acute hamstring injuries in men's soccer: a cluster-randomized controlled trial. Am J Sports Med. 2011;39:2296–2303. doi: 10.1177/0363546511419277. [DOI] [PubMed] [Google Scholar]
- 12.Witvrouw E, Danneels L, Asselman P, D'Have T, Cambier D. Muscle flexibility as a risk factor for developing muscle injuries in male professional soccer players: a prospective study. Am J Sports Med. 2003;31:41–46. doi: 10.1177/03635465030310011801. [DOI] [PubMed] [Google Scholar]
- 13.Yeung SS, Suen AMY, Yeung EW. A prospective cohort study of hamstring injuries in competitive sprinters: preseason muscle imbalance as a possible risk factor. Br J Sports Med. 2009;43:589–594. doi: 10.1136/bjsm.2008.056283. [DOI] [PubMed] [Google Scholar]
- 14.Arnason A, Sigurdsson SB, Gudmundsson A, Holme I, Engebretsen L, Bahr R. Risk factors for injuries in football. Am J Sports Med. 2004;32(Suppl. 1):S5–16. doi: 10.1177/0363546503258912. [DOI] [PubMed] [Google Scholar]
- 15.van Doormaal MC, van der Horst N, Backx FJG, Smits DW, Huisstede BMA. No relationship between hamstring flexibility and hamstring injuries in male amateur soccer players: a prospective study. Am J Sports Med. 2017;45:121–126. doi: 10.1177/0363546516664162. [DOI] [PubMed] [Google Scholar]
- 16.van Dyk N, Bahr R, Whiteley R. Hamstring and quadriceps isokinetic strength deficits are weak risk factors for hamstring strain injuries: a 4-year cohort study. Am J Sports Med. 2016;44:1789–1795. doi: 10.1177/0363546516632526. [DOI] [PubMed] [Google Scholar]
- 17.Ishoi L, Krommes K, Husted RS, Juhl CB, Thorborg K. Diagnosis, prevention and treatment of common lower extremity muscle injuries in sport: grading the evidence: a statement paper commissioned by the Danish Society of Sports Physical Therapy (DSSF) Br J Sports Med. 2020;54:528–537. doi: 10.1136/bjsports-2019-101228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Goode AP, Reiman MP, Harris L. Eccentric training for prevention of hamstring injuries may depend on intervention compliance: a systematic review and meta-analysis. Br J Sports Med. 2015;49:349–356. doi: 10.1136/bjsports-2014-093466. [DOI] [PubMed] [Google Scholar]
- 19.Best TM, McElhaney JH, Garrett WJ, Myers BS. Axial strain measurements in skeletal muscle at various strain rates. J Biomech Eng. 1995;117:262–265. doi: 10.1115/1.2794179. [DOI] [PubMed] [Google Scholar]
- 20.Garrett Jr WE, Safran MR, Seaber AV, Glisson RR, Ribbeck BM. Biomechanical comparison of stimulated and nonstimulated skeletal muscle pulled to failure. Am J Sports Med. 1987;15:448–454. doi: 10.1177/036354658701500504. [DOI] [PubMed] [Google Scholar]
- 21.Lieber RL, Friden J. Muscle damage is not a function of muscle force but active muscle strain. J Appl Physiol (1985) 1993;74:520–526. doi: 10.1152/jappl.1993.74.2.520. [DOI] [PubMed] [Google Scholar]
- 22.Enoka RM. Human kinetics; Champaign, IL: 2008. Neuromechanics of human movement. [Google Scholar]
- 23.Wan X, Qu F, Garrett WE, Liu H, Yu B. Relationships among hamstring muscle optimal length and hamstring flexibility and strength. J Sport Health Sci. 2017;6:275–282. doi: 10.1016/j.jshs.2016.04.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Wan X, Qu F, Garrett WE, Liu H, Yu B. The effect of hamstring flexibility on peak hamstring muscle strain in sprinting. J Sport Health Sci. 2017;6:283–289. doi: 10.1016/j.jshs.2017.03.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Li S, Garrett WE, Best TM. Effects of flexibility and strength interventions on optimal lengths of hamstring muscle-tendon units. J Sci Med Sport. 2020;23:200–205. doi: 10.1016/j.jsams.2019.09.017. [DOI] [PubMed] [Google Scholar]
- 26.Chang YW, Su FC, Wu HW, An KN. Optimum length of muscle contraction. Clin Biomech (Bristol, Avon) 1999;14:537–542. doi: 10.1016/s0268-0033(99)00014-5. [DOI] [PubMed] [Google Scholar]
- 27.Haff GG, Triplett NT. Human Kinetics; Champaign, IL: 2015. Essentials of strength training and conditioning. [Google Scholar]
- 28.Yu B, Gabriel D, Noble L, An K. Estimate of the optimum cutoff frequency for the Butterworth low-pass digital filter. J Appl Biomech. 1999;15:319–329. [Google Scholar]
- 29.Yu B, Queen RM, Abbey AN. Hamstring muscle kinematics and activation during overground sprinting. J Biomech. 2008;41:3121–3126. doi: 10.1016/j.jbiomech.2008.09.005. [DOI] [PubMed] [Google Scholar]
- 30.Kadaba MP, Ramakrishnan HK, Wootten ME, Gainey J, Gorton G, Cochran GV. Repeatability of kinematic, kinetic, and electromyographic data in normal adult gait. J Orthop Res. 1989;7:849–860. doi: 10.1002/jor.1100070611. [DOI] [PubMed] [Google Scholar]
- 31.Schwartz MH, Trost JP, Wervey RA. Measurement and management of errors in quantitative gait data. Gait Posture. 2004;20:196–203. doi: 10.1016/j.gaitpost.2003.09.011. [DOI] [PubMed] [Google Scholar]
- 32.Davis DS, Quinn RO, Whiteman CT, Williams JD, Young CR. Concurrent validity of four clinical tests used to measure hamstring flexibility. J Strength Cond Res. 2008;22:583–588. doi: 10.1519/JSC.0b013e31816359f2. [DOI] [PubMed] [Google Scholar]
- 33.Yu B, Liu H, Garrett WE. Mechanism of hamstring muscle strain injury in sprinting. J Sport Health Sci. 2017;6:130–132. doi: 10.1016/j.jshs.2017.02.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Orchard J, Marsden J, Lord S, Garlick D. Preseason hamstring muscle weakness associated with hamstring muscle injury in Australian footballers. Am J Sports Med. 1997;25:81–85. doi: 10.1177/036354659702500116. [DOI] [PubMed] [Google Scholar]
- 35.Timmins RG, Bourne MN, Shield AJ, Williams MD, Lorenzen C, Opar DA. Short biceps femoris fascicles and eccentric knee flexor weakness increase the risk of hamstring injury in elite football (soccer): a prospective cohort study. Br J Sports Med. 2016;50:1524–1535. doi: 10.1136/bjsports-2015-095362. [DOI] [PubMed] [Google Scholar]
- 36.Sugiura Y, Saito T, Sakuraba K, Sakuma K, Suzuki E. Strength deficits identified with concentric action of the hip extensors and eccentric action of the hamstrings predispose to hamstring injury in elite sprinters. J Orthop Sports Phys Ther. 2008;38:457–464. doi: 10.2519/jospt.2008.2575. [DOI] [PubMed] [Google Scholar]
- 37.Arnason A, Andersen TE, Holme I, Engebretsen L, Bahr R. Prevention of hamstring strains in elite soccer: an intervention study. Scand J Med Sci Sports. 2008;18:40–48. doi: 10.1111/j.1600-0838.2006.00634.x. [DOI] [PubMed] [Google Scholar]
- 38.Askling C, Karlsson J, Thorstensson A. Hamstring injury occurrence in elite soccer players after preseason strength training with eccentric overload. Scand J Med Sci Sports. 2003;13:244–250. doi: 10.1034/j.1600-0838.2003.00312.x. [DOI] [PubMed] [Google Scholar]
- 39.Worrell TW, Perrin DH, Gansneder BM, Gieck JH. Comparison of isokinetic strength and flexibility measures between hamstring injured and noninjured athletes. J Orthop Sports Phys Ther. 1991;13:118–125. doi: 10.2519/jospt.1991.13.3.118. [DOI] [PubMed] [Google Scholar]
- 40.Engebretsen AH, Myklebust G, Holme I, Engebretsen L, Bahr R. Prevention of injuries among male soccer players: a prospective, randomized intervention study targeting players with previous injuries or reduced function. Am J Sports Med. 2008;36:1052–1060. doi: 10.1177/0363546508314432. [DOI] [PubMed] [Google Scholar]
- 41.Blazevich AJ, Cannavan D, Coleman DR, Horne S. Influence of concentric and eccentric resistance training on architectural adaptation in human quadriceps muscles. J Appl Physiol (1985) 2007;103:1565–1575. doi: 10.1152/japplphysiol.00578.2007. [DOI] [PubMed] [Google Scholar]
- 42.Brockett CL, Morgan DL, Proske U. Human hamstring muscles adapt to eccentric exercise by changing optimum length. Med Sci Sports Exerc. 2001;33:783–790. doi: 10.1097/00005768-200105000-00017. [DOI] [PubMed] [Google Scholar]
- 43.Kilgallon M, Donnelly AE, Shafat A. Progressive resistance training temporarily alters hamstring torque-angle relationship. Scand J Med Sci Sports. 2007;17:18–24. doi: 10.1111/j.1600-0838.2005.00491.x. [DOI] [PubMed] [Google Scholar]
- 44.Philippou A, Bogdanis GC, Nevill AM, Maridaki M. Changes in the angle-force curve of human elbow flexors following eccentric and isometric exercise. Eur J Appl Physiol. 2004;93:237–244. doi: 10.1007/s00421-004-1209-z. [DOI] [PubMed] [Google Scholar]
- 45.Timmins RG, Ruddy JD, Presland J. Architectural changes of the biceps femoris long head after concentric or eccentric training. Med Sci Sports Exerc. 2016;48:499–508. doi: 10.1249/MSS.0000000000000795. [DOI] [PubMed] [Google Scholar]
- 46.Lynn R, Talbot JA, Morgan DL. Differences in rat skeletal muscles after incline and decline running. J Appl Physiol (1985) 1998;85:98–104. doi: 10.1152/jappl.1998.85.1.98. [DOI] [PubMed] [Google Scholar]
- 47.Hasselman CT, Best TM, Seaber AV, Garrett WE., Jr A threshold and continuum of injury during active stretch of rabbit skeletal muscle. Am J Sports Med. 1995;23:65–73. doi: 10.1177/036354659502300111. [DOI] [PubMed] [Google Scholar]
- 48.Nelson RT, Bandy WD. Eccentric training and static stretching improve hamstring flexibility of high school males. J Athl Train. 2004;39:254–258. [PMC free article] [PubMed] [Google Scholar]
- 49.Mahieu NN, McNair P, Cools A, D'Haen C, Vandermeulen K, Witvrouw E. Effect of eccentric training on the plantar flexor muscle-tendon tissue properties. Med Sci Sports Exerc. 2008;40:117–123. doi: 10.1249/mss.0b013e3181599254. [DOI] [PubMed] [Google Scholar]
- 50.Potier TG, Alexander CM, Seynnes OR. Effects of eccentric strength training on biceps femoris muscle architecture and knee joint range of movement. Eur J Appl Physiol. 2009;105:939–944. doi: 10.1007/s00421-008-0980-7. [DOI] [PubMed] [Google Scholar]
- 51.Behm DG, Bradbury EE, Haynes AT, Hodder JN, Leonard AM, Paddock NR. Flexibility is not related to stretch-induced deficits in force or power. J Sport Sci Med. 2006;5:33–42. [PMC free article] [PubMed] [Google Scholar]
- 52.Junior RS, Leite T, Reis VM. Influence of the number of sets at a strength training in the flexibility gains. J Hum Kinet. 2011;29A:47–52. doi: 10.2478/v10078-011-0058-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Maniar N, Shield AJ, Williams MD, Timmins RG, Opar DA. Hamstring strength and flexibility after hamstring strain injury: a systematic review and meta-analysis. Br J Sports Med. 2016;50:909–920. doi: 10.1136/bjsports-2015-095311. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.