

Summary
This systematic review synthesized the qualitative evidence on factors influencing obesogenic behaviours in adolescent girls and women of reproductive age in low‐ and middle‐income countries (LMICs). This qualitative evidence synthesis followed the framework synthesis approach to extract, analyse and synthesize data. Electronic searches were conducted in the Web of Science, SCOPUS, CABI Abstracts, MEDLINE, PsycINFO and Google Scholar. Studies were eligible if they were conducted in LMICs, of qualitative nature, and reported obesogenic behaviours of female adolescents (10–19 years of age) or women of reproductive age (15–49 years of age). The review resulted in 71 included studies from 27 different countries. Thirty‐two studies focused on dietary behaviours, 17 on physical activity and 22 on both behaviours. Gender norms and failures to recognize the importance of healthy behaviours across the life cycle were important factors. The abundance and promotion of affordable but unhealthy food, food safety concerns, taste preferences and social desirability of foods drive consumption of unhealthy foods. Busy lives and limited exercise spaces keep girls and women from being physically active. Obesogenic behaviours of adolescent girls and women of reproductive age are influenced by factors at individual, social, physical and environmental levels and require diverse solutions to address these factors in LMICs.
Keywords: adolescents, low‐ and middle‐income countries, obesogenic behaviour, qualitative, women
1. INTRODUCTION
Adolescent girls and women of reproductive age are particularly vulnerable to malnutrition (including undernutrition, micronutrient deficiency, overweight and obesity) due to poor dietary intakes, 1 inequitable distribution of food within households, 2 dietary taboos 3 and gender inequality. 4 Growth spurts, pregnancy and lactation during adolescence substantially increase nutrient requirements, putting adolescents even more at risk. 5 Furthermore, malnutrition can span generations and affect all stages of the life cycle. For example, women classified as underweight are more likely to give birth to infants with a low‐birth weight. 4 Obesity among mothers can also have adverse health effects on new‐borns and increase the risk for childhood obesity. 6
Overweight and obesity are rising in every part of the world, with women and adolescent girls particularly affected, and no country has successfully reversed this trend. 7 Globally, the prevalence of adult women with overweight and obesity increased significantly over a short period of time (from 32% in 2010 to 40% in 2016). 7 This burden is not equally distributed, as more than 70% of all adults with overweight and obesity live in low‐ and middle‐income countries (LMICs). 8 For adolescent girls (aged 15–19 years) in LMICs, more than 10% are classified as having obesity or overweight, with rates either being stagnant or on the rise between 2000 and 2017. 9 This increase in obesity has also been faster compared with adults. 10 As major risk factors for noncommunicable diseases (NCDs), overweight and obesity not only affect morbidity and mortality of individuals but also drive a growing economic burden on healthcare systems and societies. 11 , 12
Recognized drivers of overweight and obesity in LMICs include increasing urbanization, changing food environments with the expansion of modern retail, 13 and growing availability of ultra‐processed, energy‐dense, nutrient‐poor foods. 14 Additionally, rising numbers of women in the workforce increase the demand for convenience foods and out‐of‐home consumption. 15 Together with reduced physical activity due to more sedentary lifestyles and less conducive built environments, 16 these factors represent important contributors to overweight and obesity. 17 , 18 Other contributing factors relate to socio‐economic status, 19 genetics, 20 stress, early‐life undernutrition 4 and cultural beliefs about body size, 21 among others. 22 There is also evidence that food assistance programmes, which aim to improve undernutrition, actually contribute to adult overweight and obesity. 23 For adolescents in particular, exposure to food and drink advertising and the role of the family/home environment, as well as the school environment, are important influences on overweight and obesity. 24 , 25
Obesogenic behaviours are promoting or contributing to obesity through unhealthy diets, physical inactivity or high sedentary behaviours. Despite the apparent rise of overweight and obesity in LMICs, most research on obesogenic behaviours has been conducted in high‐income countries (HICs). Furthermore, previous systematic reviews focused only on Africa, 26 , 27 , 28 on diets of adolescents in LMICs, 1 on young children, 29 , 30 and on adolescents 31 , 32 or on considerations for interventions to prevent overweight and obesity. 21 , 33 Little of this evidence stems from qualitative research, 26 , 27 , 28 as this prior research primarily was aimed at quantifying the influence of different drivers. This limits the understanding of the specific factors influencing obesogenic behaviours in LMIC settings, 34 which are experiencing rapidly transitioning obesogenic environments and changing behaviours. To address these changing behaviours effectively with interventions throughout the life cycle, a better understanding of how and why adolescent girls and women of reproductive age (WRA) make their dietary choices is urgently needed. A synthesis of primary qualitative research studies would elicit multiple perspectives, views, beliefs and priorities in relation to such influencing factors and would go beyond the existing evidence. This review aims to serve this purpose and address these knowledge gaps, by synthesizing the qualitative evidence on factors influencing obesogenic behaviours among adolescent girls and WRA, specifically in LMICs.
2. METHODS
To identify factors influencing obesogenic behaviours in adolescent girls and WRA (aged 10–49 years) in LMICs, we applied a qualitative evidence synthesis (QES). QES is an ‘umbrella term for the methodologies associated with the systematic review of qualitative research evidence’. 35 It refers to all methods that bring together different types of qualitative evidence. In this QES, we perform a systematic review following a framework synthesis 36 methodology to extract, analyse and synthesize the qualitative data from primary research studies. This method helps connect and integrate findings from included primary research studies with existing theory. 36 For our review, it involved two complementary tasks of (a) identifying existing frameworks and theories and (b) identifying eligible studies. 37 The protocol was documented according to PRISMA‐P guidelines 38 and registered a priori to describe detailed inclusion criteria and analytic methods (PROSPERO CRD42019134044; available from https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42019134044). The Enhancing transparency in reporting the synthesis of qualitative research (ENTREQ) statement was followed to report this QES. 39
2.1. Theoretical framework
We aimed to identify existing frameworks and theories that conceptualized how factors influence the following obesogenic behaviours: unhealthy diets and physical inactivity. We searched for existing frameworks using a within‐topic search 40 on MEDLINE using the below described search strategy (Data S1) together with the following search syntax: framework* OR theor* or model* or concept*. We did not limit ourselves to the ‘Low‐ and Middle‐Income Countries’ concept to allow for inclusion of frameworks developed for various contexts. 41 This scoping search identified six frameworks. Four of them were adaptations of the socio‐ecological framework 42 , 43 , 44 , 45 , 46 , 47 ; two of the frameworks on physical activity and sedentary behaviours were structured differently. 48 , 49 None of the individual frameworks were sufficiently comprehensive to capture factors influencing obesogenic behaviours. 36 We therefore deconstructed the six identified frameworks 44 , 46 , 47 , 48 , 49 , 50 into individual constructs and fitted them within the levels of influence (individual, social, physical and macro) of the socio‐ecological framework, 45 which has also been previously adapted for dietary factors in the African context. 50 Subsequently, by merging or renaming these constructs, an a priori meta‐framework was developed including a total of 78 constructs across the four levels of influence (see supporting information). Constructs were omitted when they were not applicable to our research question, such as those relating to different age groups (geriatric syndromes/sarcopenia 48 ).
2.2. Identification of eligible studies
2.2.1. Search strategy
To identify eligible studies, searches were conducted in five electronic databases: Web of Science (http://www.webofknowledge.com), SCOPUS (https://www.scopus.com), CABI Abstracts (https://www.ovid.com/product-details.31.html), MEDLINE (Pubmed; http://www/ncbi.nlm.nih. gob/pubmed) and PsycINFO (https://www.ebsco.com/products/research-databases/apa-psycinfo). Google Scholar was searched for grey literature. Subsequently, citation searches were conducted for all included references on Google Scholar. Additional eligible studies were identified from the reference lists of included studies. The initial search strategy was developed in MEDLINE using the Setting, Perspective, Interest, phenomenon of, Comparison and Evaluation (SPICE) model 51 combining search terms for setting (LMICs), perspective (adolescent girls and WRA, 10–49 years of age), phenomenon of interest (perceptions and/or potential influencing factors of obesogenic behaviours) and evaluation (themes identified from original qualitative research). Scoping searches were conducted in MEDLINE to refine the search strategy, using database‐specific indexing terms. The search syntax was further adapted to the specific requirements of each database. A social science librarian provided input into the search strategy. The final search syntax included text words and MeSH terms (Data S1). The search was conducted in May 2019, citation alerts were set up in all the databases, and the search was updated in January 2020 to ensure inclusion of relevant publications since the first search.
2.3. Eligibility criteria
Studies were eligible if they were conducted in a LMIC (using the World Bank definition of LMICs as of 2019 52 ), were of qualitative nature and included female adolescents or WRA (10–49 years). The selection of the age group was based on the World health Organization (WHO) definition of adolescents (10–19 years) and WRA (15–49 years) and the importance of following a life‐cycle approach. If studies included a broader age range and/or male participants, verbatim quotations and/or authors' interpretation had to be clearly attributable to girls or women aged 10–49 years to be included. Studies with clinical populations were not included. Phenomena of interest were perceptions related to obesogenic behaviours and/or potential influencing factors of these behaviours of adolescent girls or WRA. Studies had to apply qualitative methods but were only included if qualitative findings were explicitly reported and distinguishable from quantitative data, in the case of mixed methods studies. The review was limited to studies published in English without any restrictions in terms of year of publication. Correspondence, commentaries and editorials were excluded.
2.4. Screening process
All retrieved references were imported into EndNote and, after de‐duplication, data on references were imported into Microsoft Excel. One reviewer (U. T.) conducted title and abstract screening following the eligibility criteria and retrieved and reviewed full texts of selected references for inclusion. To ensure the quality of inclusion, independent reviews at title and abstract screening (28% by K. B.) and full‐text screening (22% by K. B. and L. S.) were performed by co‐authors. In case of disagreement, discrepancies in selection of references were discussed between reviewers. In case of doubt at any stage, the record was carried forward to the subsequent stage. Reasons for exclusion were recorded at every stage of the screening (see Figure 1).
FIGURE 1.
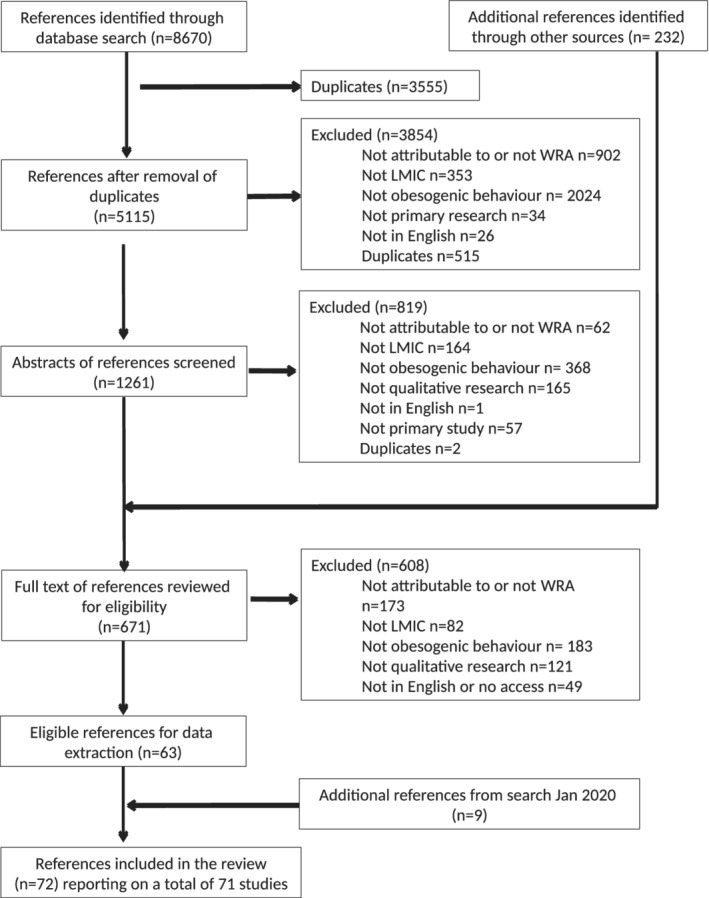
PRIMSA chart. LMIC, low‐ and middle‐income country; WRA, women of reproductive age
2.5. Data extraction and coding
Data extraction of the following descriptive characteristics was performed by U. T.: country/countries in which the study was conducted, income level of the country, setting of the study, characteristics of the participants (including number, age and gender in case of inclusion of a male population) and type of obesogenic behaviour. The a priori defined meta‐framework (supporting information) was used to code data, including verbatim quotations from participants as well as author interpretations, on influencing factors. Coding was performed independently by U. T. and the review team (K. B., L. S., M. H. and R. V.) in NVivo (12.5.0) and followed a stepwise approach. First, the coding framework was piloted by coding data from two papers (U. T., R. V., M. H., L. S., K. B.), which was further refined based on discussions. Subsequently, data of all included references were coded against the constructs of the meta‐framework. Finally, 11 of these coded references were checked by co‐reviewers to ensure quality control and harmonization of coding. Discrepancies were discussed and addressed in coding the remaining references.
2.6. Quality assessment
Methodological quality of included references was assessed using the Critical Appraisals Skills Programme (CASP) checklist for qualitative research assessing the validity of the results, the analysis and reporting of the data and the value of the research. 53 One reviewer (U. T.) assessed all references, and to ensure a consistent application of the CASP criteria, two reviewers (A. B. and R. V.) independently assessed 10% of the verdicts. Studies were not excluded based on their quality, but a sensitivity analysis was conducted to evaluate the relative contribution of quality on the review findings. 54
2.7. Data analysis and synthesis
The analysis used a deductive approach by systematically coding data with the a priori constructs included in the meta‐framework (supporting information) and was complemented by an inductive approach when data did not fit the meta‐framework. All coded quotations, including memos written throughout the coding process, were then analysed to identify themes inductively. Themes were then iteratively rearranged by refining and merging overlapping themes. Based on themes, a summary of findings was prepared for review by all authors. Identified themes were visualized in the data‐driven socio‐ecological framework (Figure 2). The supporting information provides an overview of all identified themes and studies supporting them.
FIGURE 2.
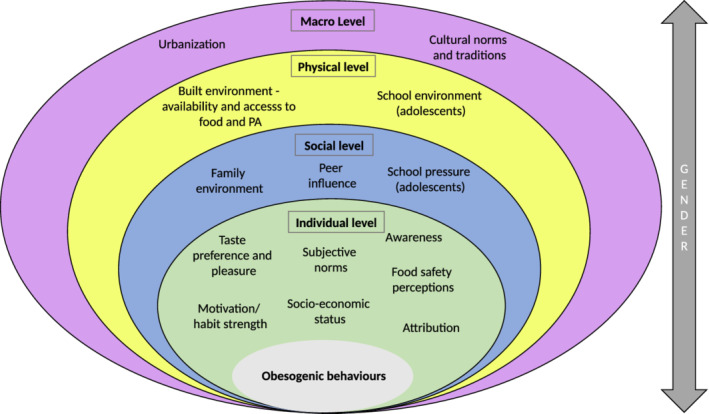
Conceptual framework. PA, physical activity
Sensitivity analyses were conducted for a number of subcategories, such as study quality (high or low), population (adolescent girls or adult women), continent (Africa, Asia or South America) and setting (rural or urban) in order to identify themes specific to those categories. This was conducted by bringing together and analysing data within these subgroups; quotes were rearranged by subgroup highlighting more granular findings. The additional eligible references identified through the search update were added to the synthesis in January 2020; they were coded and analysed for new emerging themes or for strengthening existing ones and underwent quality assessment. 55
3. RESULTS
Results of the data synthesis are presented by the level of the socio‐ecologic model, that is, individual, social, physical, and macro level and supported with quotations of participants (in quotation marks) as well as author interpretations from included references (reference, country and population). Findings of the sensitivity analyses are mentioned whenever we found a difference. Additional quotations are provided in the supporting information.
3.1. General characteristics
The full‐text review resulted in a total of 72 included references 56 , 57 , 58 , 59 , 60 , 61 , 62 , 63 , 64 , 65 , 66 , 67 , 68 , 69 , 70 , 71 , 72 , 73 , 74 , 75 , 76 , 77 , 78 , 79 , 80 , 81 , 82 , 83 , 84 , 85 , 86 , 87 , 88 , 89 , 90 , 91 , 92 , 93 , 94 , 95 , 96 , 97 , 98 , 99 , 100 , 101 , 102 , 103 , 104 , 105 , 106 , 107 , 108 , 109 , 110 , 111 , 112 , 113 , 114 , 115 , 116 , 117 , 118 , 119 , 120 , 121 , 122 , 123 , 124 , 125 , 126 , 127 reporting on a total of 71 studies from 27 different countries, with 23 studies conducted in Africa, 34 in Asia, and 14 in South America. Figure 1 shows details of references screened, included and excluded, and Table 1 shows the general characteristics of the included studies.
TABLE 1.
General characteristics—number of studies
| Characteristics | Africa (n) | Asia (n) | South America (n) |
|---|---|---|---|
| Phenomenon | |||
| Diet | 6 | 18 | 8 |
| Physical activity | 6 | 10 | 1 |
| Diet and physical activity | 11 | 6 | 5 |
| Population | |||
| Adolescents | 13 | 21 | 8 |
| Women | 6 | 9 | 5 |
| Adolescents and women | 4 | 4 | 1 |
| Setting | |||
| Urban | 17 | 25 | 8 |
| Rural | 4 | 2 | 2 |
| Urban and rural | 2 | 5 | 4 |
| Not specified | 0 | 2 | 0 |
| Income level of the country | |||
| Low income | 1 | 1 | 0 |
| Lower middle income | 8 | 14 | 4 |
| Upper middle income | 14 | 19 | 10 |
| Countries | |||
| South Africa (12) | Iran (11) | Mexico (5) | |
| Cameroon (2) | India (7) | Costa Rica (3) | |
| Ghana (2) | Indonesia (4) | Brazil (2) | |
| Kenya (2) | China (2) | Guatemala (2) | |
| Botswana (1) | Turkey (2) | El Salvador (1) | |
| Cape Verde (1) | Malaysia (2) | Bolivia (1) | |
| Libya (1) | Nepal (1) | ||
| Morocco (1) | Pakistan (1) | ||
| Uganda (1) | Samoa (1) | ||
| Sri Lanka (1) | |||
| Tonga (1) | |||
| Bangladesh (1) | |||
| Total | 23 | 34 | 14 |
Forty‐one studies were conducted with adolescent girls only, 24 with WRA and six with both. Thirty‐two studies focused on factors influencing dietary behaviours, 17 on factors influencing physical activity and 22 on factors influencing both behaviours. The majority of studies were conducted in urban areas (n = 50), 26 studies were conducted in low‐ and lower middle‐ and 45 in upper middle‐income countries.
3.2. Factors influencing obesogenic behaviours at the individual level
3.2.1. Attribution
A common perception among participants was considering one's health or body weight as a destiny 56 , 57 or ‘God's will’, 58 or blaming their current weight on their own mothers' concerns about their low childhood weight. 97 Obesity and individual body weight were also perceived as beyond an individual's control due to genetic predisposition. 56 , 59 , 60 , 61
Some even believed that ‘nothing can be done about it’ when overweight is inherited. ( 59 Ghana, WRA)
Adolescents did not perceive obesity as an immediate threat, but something older people struggle with, only to be faced in the future or when confronted with health problems. 57 , 65 , 72 , 73 , 99
3.2.2. Awareness
Participants in the included studies were aware of the importance of physical activity 62 , 63 , 64 , 65 and mental health, 66 as well as the potential negative effects of physical inactivity. 67 However, the perception that physical activity was only relevant for weight loss was also revealed. 68 , 69
I don't remember anybody who I've come across talking about exercising. Only when they want to lose weight, then they want to exercise. ( 69 South Africa, WRA)
Awareness of the importance of healthy diets included the importance of dietary diversity, 70 , 71 eating fresh or natural foods, 72 , 73 , 74 while avoiding fatty, salty, sugary or fast foods. 56 , 72 , 75 Healthy diet misconceptions were related to consuming snacks and skipping meals, which were perceived as positive due to eating less. 76 Some perceived that exercise could replace a healthy diet, 77 whereas others preferred to diet instead of engaging in physical activity. 78
Findings from the sensitivity analysis revealed that only participants from rural settings associated risks of underweight, food‐borne diseases, and the importance of food and micronutrients for growth with healthy diets. 79 , 80 , 81 , 82 , 83
3.2.3. Food safety concerns
Food safety concerns were related to food adulteration, expiry dates, hormones, and pesticides or other chemicals contained in foods. 71 , 73 , 84 , 85 , 86 Overall, (un)healthiness of food was perceived more in relation to food safety and hygiene than nutritional quality per se. 82 Participants perceived packaged foods as the safer option, 76 , 87 which could limit fruit and vegetable consumption. 88 , 89
A snack which is produced by dirty hands contains microbes and can cause illness. […] Therefore, I prefer packed puffs and chips to traditional bread and cheese because they are safer. ( 87 Iran, adolescents)
Food prepared outside the home was generally considered unhealthy whereas home‐cooked food was considered safer. 71 , 76 , 79 , 85 , 89 , 90 Food seen as unsafe was also perceived as tasty, so that participants ate food they considered unhealthy, 71 notwithstanding food safety concerns. 91 The sensitivity analysis revealed that in South America, food safety concerns were only expressed in relation to additives and processing level, whereas in Africa and Asia, hygiene concerns around street food were often raised.
3.2.4. Subjective norms
Perceived body weight
Overweight was perceived as a sign of a healthy, wealthy, and happy life 56 , 74 , 80 , 92 , 93 , 94 , 95 and as a symbol of beauty. 59 , 63 , 64 , 96 Thinness was conversely associated with illness. 63 , 69 , 74 , 93 For adolescent girls, thinness was the ideal in two studies, 77 , 97 whereas in another study, thin girls were teased for looking androgynous. 98 A higher body weight was also expected for older and married women, reflecting dignity, maturity, 59 , 93 , 94 , 96 motherhood or marriage. 56 , 93 , 94 , 99
In Africa, a larger body was associated with health, attractiveness and wealth, whereas in Asia and South America, thinner and ‘feminine’ looking bodies were more socially desirable.
Gender
Women and girls were expected to look beautiful and feminine. 64 , 78 , 96 , 97 , 100 , 101 Participants were also concerned about which types of physical activity were gender appropriate, making vigorous or outdoor activities less accessible for girls. 62 , 65 , 98 , 112 , 121
Soccer is for men, ballet is for women, this is like saying strength and delicacy … ( 98 Costa Rica, adolescents)
Girls were also not expected to show muscles, 64 look sweaty, messy or tanned, 64 , 66 , 98 , 102 because these were signs of poverty or masculinity. Menstruation, 66 school uniforms and religious dress codes also kept women and girls from being active. 60 , 103 , 104 Furthermore, women and girls were less likely to engage in physical activity due to prohibition in some countries on them being unaccompanied in public. 58 , 62 , 66 , 76 , 103 , 104 , 105 , 106 In addition, women and girls were faced with sexual harassment and objectification for wearing exercise clothes. 61 , 98 , 106
Age
Physical activity was perceived as more appropriate for schoolgirls and not for adult women. 61 , 63 , 69 , 74 , 99 This perception that any sport or physical activity was only appropriate for young people was most dominant in Africa.
Exercise was seen to be associated with what children and young people did, and it was not acceptable for women (particularly married women) to be seen exercising. ( 69 South Africa, WRA and adolescents)
Social status
Sedentary lifestyle and car ownership were associated with higher socio‐economic status, 63 , 64 , 105 whereas active transport was stigmatized as being for poor people. 105 Certain types of foods were also associated with higher social status. Traditional foods, homegrown vegetables or packed meals taken from home to school were considered less socially favourable. 57 , 71 , 96 , 107 , 108 However, an abundance of food, 97 eating out, eating packed food, modern snacks were seen as a sign of wealth. 56 , 76 , 82 , 83 , 96 , 100 , 107 , 108 Particularly for adolescents, unhealthy foods were perceived as more popular, while eating healthily made them feel like an outcast. 107
3.2.5. Motivation and habit strength
Participants emphasized the importance of making physical activity and healthy dietary practices a habit from childhood onwards. 56 , 57 , 65 , 68 , 72 , 85 , 94 , 106 At the same time, unhealthy habits ingrained from childhood were difficult to change for adults. 56 , 94 Adolescent girls reported a preference for indoor, sedentary activities involving screen time on different media devices, and a tendency to laziness, which kept them from engaging in physical activity, 62 , 66 , 76 , 96 , 102 , 104 , 109 , 110 , 111 while adult women struggled to establish good habits due to lack of time. 106 Motivations to lose weight, eat healthily or engage in physical activity were mostly related to an experience of poor health, a disease diagnosis 56 , 99 , 112 or the desire to look beautiful. 57 , 83 , 113
I am a fast food lover but the dream of being skinny forces me to have self‐control. In my age, appearance is the most important concern for a girl. ( 83 Pakistan, adolescents)
Taste, satisfaction and pleasure
Taste was an important factor in adolescents and women's dietary choices. Fast foods were perceived as tasty 56 , 70 , 87 due to their combination of salty, sweet and, sometimes, artificial flavours, 73 , 76 , 90 , 100 , 111 which made unprocessed foods such as fruit and vegetables less tasty or appealing to participants. 73
Nowadays people don't like taking the traditional foods, they despise the ‘mboga’ (green vegetables), they say it's not sweet. So they prefer taking the junk food like pizzas. ( 111 Kenya, adolescents)
In addition to taste, attractive and colourful packaging of snack food was a temptation. 57 , 100 While adolescents mostly referred to experimenting with new tastes of fast and snack foods, 76 , 90 , 91 , 96 , 108 women associated tastiness with meat, fried foods, traditional or spicy dishes. 70 , 72 , 74 , 84 , 114 In urban settings, participants put a stronger emphasis on taste, whereas for rural participants, foods primarily had to satisfy their appetite.
Pleasure and fun were important factors, particularly for physical activity. Lower intensity physical activity was associated with more fun. 63 Having fun with friends or making new friends while being physically active was also an important motivating factor. 62 , 64
3.2.6. Socio‐economic status
Affordability of physical activity was influenced by the cost of classes and membership fees for recreation facilities. 98 , 104 Healthy diets were seen as unaffordable; as fruit, vegetables, meat and wholegrain cereal were perceived as more expensive than staples, 61 , 63 , 77 , 82 , 95 snacks or fast foods. 73 , 76 , 83 , 90 , 111 Food insecurity during childhood was perceived as having a lasting impact on current habits, such as skipping breakfast and the tendency to overeat once people attained higher socio‐economic status in adulthood. 56 , 94 For adolescents, financial autonomy was associated with the amount of pocket money they received from their parents. Adolescents from poorer families did not tend to receive pocket money, 115 while most parents who gave their adolescent children pocket money were not concerned with how it was used. 79 , 119 , 122
3.3. Factors influencing obesogenic behaviours at the social level
3.3.1. Family environment
Traditional gender roles in the household, such as cooking for the family, tempted adult women to eat more, 94 and taking care of children kept women from engaging in physical activity. 112 Prioritizing and adapting to the husband and children's dietary preferences have also been reported. 85 , 86 , 116 While women would prefer home‐cooked meals, they agreed to eat at restaurants at children's request, 116 or previously, vegetarian women would start eating meat if their husband was not vegetarian. 85
… We do not eat green vegetables now. My husband does not like to eat. ( 85 India, WRA)
For adult women, time constraints were also a major factor given their traditional roles in the family and household. 106 , 112 , 117
For adolescents, parental support and parenting style had major impacts on obesogenic behaviours. For physical activity, parents were either supportive 102 , 117 , 118 or dissuasive, 65 , 69 , 71 , 98 , 101 , 104 , 106 financially or emotionally. Overall, adolescents reported that they had limited control over their own schedules and diets. Adolescents' diets were mostly perceived to be positively influenced by parental habits, through the information they provided about healthy diets, 62 , 77 , 107 the foods provided or prepared at home 73 , 79 , 83 , 91 , 111 , 119 or meals the adolescents shared together with their families. 100 Mothers prepared most of the food consumed at home 70 , 79 , 83 , 97 , 99 , 119 and therefore exerted the strongest influence. Overall, mothers cared about their children's diets and prepared food for them for school. 70 , 83
When we are with parents, we eat healthy foods, they don't allow us to eat junk foods when we are at home. ( 79 India, adolescents)
However, parents were also seen as negative role models with regard to diets 57 , 58 , 61 , 68 , 84 , 96 or being too busy to prepare food at home. 100 , 111 , 119
3.3.2. Academic pressure
Adolescents in all studies seem to struggle with lack of time due to academic pressure from the school or parents, which affected time available for engaging in physical activity. 58 , 60 , 62 , 68 , 77 , 101 , 102 , 104 , 109 , 110 , 111 , 120 , 121 They also reported a lack of time to prepare or pack food for school, 117 forcing them to skip meals 79 , 90 , 91 , 96 , 120 or displace meals with snacks. 76 In addition to the school, parents put pressure on their children to get good grades, prioritizing education over physical activity as a means to help their children escape poverty. 64 , 106
My family that always encouraged me to do exercise from childhood to high school, at the first year of high school told me: now the time for exercise is over. It is the time to study! ( 106 Iran, WRA)
While lack of time, both generally and related to school, was an issue for adolescents in all three continents, pressure from parents and the education system were featured only in Asia.
3.3.3. Peer influence
In most cases, peer pressure to join in with eating and sharing food did not encourage healthy eating. 75 , 107 , 113 One study found that peer influence was positive when adolescent girls exchanged knowledge about foods that could contribute to weight gain. 117 The amount of time spent with peers affected the increasing influence peers exerted in comparison with parents. Particularly, spending leisure time with friends or studying together was often associated with eating out and/or eating snacks, street or fast food, 59 , 71 , 73 , 76 , 87 , 93 , 119 which was often the only thing adolescent girls felt they could control in their otherwise busy, overscheduled lives. 91
Being in the social network of friends was expressed as one of the main factors causing unhealthy eating habits. In some cases, students declared that when they go out with their friends, they eat lot of junk foods as a routine way of social interaction. ( 122 Iran, adolescents)
For physical activity, peers also played an important role in encouraging adolescents to be more active 62 , 82 or more sedentary. 111 Meeting friends or making new friends as part of physical activity motivated girls. 62 , 64 , 102 For adult women, having a social network and friends with whom to engage in physical activity was motivating. 105 Not having a supportive network or friends could be detrimental to weight loss attempts. 63 , 116
3.4. Factors influencing obesogenic behaviours at the physical level
3.4.1. Built environment
Availability of opportunities for physical activity
Physical activity in public spaces, particularly in urban areas, was limited due to vehicular traffic and a lack of open spaces and sidewalks. 112 , 121 Publicly accessible spaces were considered unusable as they were dirty, 101 , 104 , 121 vandalized, 61 , 77 or unsafe due to dangerous waste. 101 , 121 Poor infrastructure influenced access to sport facilities, which, when available, 58 , 60 , 61 , 63 , 65 , 94 , 102 , 104 , 110 were lacking equipment, 62 , 63 , 112 were perceived dirty 106 or inappropriate for women in terms of open hours or equipment. 106 , 110 Access to sport facilities was also limited due to the lack of transport, 96 distance 62 or membership fees. 62 , 63 , 96 , 104 , 110 , 112
Safety
Getting to sport facilities or freely moving in public spaces was generally perceived as unsafe. Free spaces, such as parks and beaches, were not seen as safe due to crime, dogs, traffic or human trafficking. 60 , 61 , 62 , 65 , 95 , 96 , 102 , 105 , 106 , 109 , 110 , 112 , 121
The built environment was a major factor as most of the facilities like parks and playgrounds are not accessible or are not well managed. There is hardly any space for footpaths in Kerala, much of which is encroached by vehicle parking. Rain, traffic, and stray dogs are leading people to walk early in the morning and with a companion. ( 112 India, WRA)
For women, girls and parents, there was also a fear of sexual violence, of assault 62 , 64 , 121 or of getting kidnapped. 77
Two studies reported changes over time, when playing on the street was safe and accessible, compared with the densely built environment of the present. 69 , 104 The sensitivity analysis revealed that although rural areas offered more opportunities for active transport, they lacked facilities and opportunities for different types of physical activity.
Availability of and access to food
From most studies, it was apparent that availability of healthy options was perceived as limited whereas fast and snack foods were widely available. 60 , 61 , 70 , 76 , 77 , 79 , 81 , 90 , 111 , 122 , 123 , 124 , 125
Fruit and vegetables were perceived as less available in peri‐urban and urban areas than in rural areas. 85 , 88 Unhealthy foods were also perceived as cheaper 77 , 111 and available in small shops that were easily accessible in most neighbourhoods. 85 , 94 , 123 Supermarkets and open markets, which had cheaper and healthier options available such as fruit and vegetables, were often distant. 81 , 94 , 96 , 123
With large supermarkets located farther away from home, families regularly depend on neighbourhood tienditas and other local vendors for goods. ( 81 El Salvador, adolescents)
Distance to supermarkets was only mentioned in South America and Africa, while in Asia, small neighbourhood stores were used to purchase fresh fruit and vegetables. 85 Availability of unhealthy snack food was mentioned mostly in urban studies.
3.4.2. School environment
Availability and accessibility of physical activity
Schools were considered settings with safe and affordable facilities for physical activity. 60 , 82 , 111 , 117 However, sport facilities and equipment were not always available or appropriate. 62
Availability and accessibility of food
Schools with cafeterias offered healthy choices, 96 , 107 , 108 but due to long queues, poor food safety, inferior taste and high prices, 75 , 83 , 91 , 113 , 119 , 126 students felt compelled to buy cheaper snack food from small vendors.
A private school girl explained, ‘I think the fact that we have kiosks inside [the school] does not help, because it induces us to buy and eat junk food.’ ( 60 Guatemala, adolescents)
Healthy foods, such as fruit and vegetables were either unavailable or unaffordable at schools. 59 , 75 , 90 , 93 , 95 While in some countries, students were not allowed to leave the school compound, they had multiple opportunities to buy cheap fast or snack food from small vendors on the way to or from school. 60 , 76 , 80 , 87 , 90 , 91 , 96 , 107 , 108 , 117 , 126
Curriculum and teachers' support
Although curricula contained nutrition and physical education topics, they were often substituted for other subjects 62 , 102 , 106 or relied on teachers' motivation. 60 , 112 Girls also stated that physical education in schools primarily focused on competitive sports, in which girls are less interested, and that teachers prioritized boys in sports. 60 , 65 , 98 , 102 , 104 , 109
Boys are told to play soccer, jog, or do some kind of sport, but we're just told to sit in any place or do whatever you want. ( 98 Costa Rica, adolescents)
From the sensitivity analysis, it was apparent that the above‐mentioned gender issues in school were more prevalent in Asia and South America.
3.5. Factors influencing obesogenic behaviours at the macro level
3.5.1. Cultural norms and traditions
Several studies reported shifts in food culture. Overall, traditional and home‐cooked foods were perceived as healthier than food prepared outside the home, 71 , 79 , 85 , 87 , 89 , 90 , 96 , 107 , 124 and imported food was perceived as unhealthy. 74 , 124 , 127
Our own local food is better for health and even for Samoan people to be stronger. If we eat overseas food, we will get fat—it's not good for the body. ( 127 Samoa, WRA)
However, as described above, the taste of nontraditional food, 76 , 96 as well as the popularity of eating out at international food chains, 83 , 96 , 100 led to a perceived shift of nontraditional food increasingly replacing traditional or local foods. 91 , 107 , 127 This shift was also recognized in terms of older generations eating healthier and consuming more unprocessed, local foods, 86 , 127 which led to adolescents feeling torn between traditional and modern culture. 91 Cultural norms were associated with certain foods and behaviours. Particularly in South Africa, physical activity and consumption of raw vegetables was associated with white or rich people and not part of ‘black culture’. 69 , 96
3.5.2. Advertising
Food and beverage advertising was ubiquitous and mostly targeted unhealthy foods 57 , 75 , 76 , 83 , 103 , 119 across many platforms including TV, newspapers, social media, street flyers, free deliveries and displays within the store. 57 , 76 , 85 , 91 , 109 , 123 Participants appeared to be subconsciously influenced, stating trustworthiness of certain brands or claiming to use TV advertisements as a source of information. 108 , 109 , 115
There are many TV commercials for puffed cheese and crisps but not for healthy snacks such as raisins and fruits. ( 57 Iran, adolescents)
Social media and pop culture seem to exert an increasing influence, pushing adolescents towards more sedentary behaviours. Engaging in social media can also influence their dietary choices. 76 , 83 , 108
Extensive networks and use of social media infiltrated with information about eateries and snacks are likely contributing to the already strong yearning for snack foods. ( 76 Indonesia, adolescents)
On all continents, participants observed a transition from traditional and local to modern and imported foods. This was also apparent in terms of generational changes in diets between grandparents and the adolescents. 82 , 86 , 127 However, particularly in South American studies, participants framed this transition in terms of the loss of indigenous, not just traditional foods.
3.5.3. Urbanization
Food availability in urban areas was usually perceived as better than in rural areas. 56 , 85 , 88 This was more nuanced, as fruit and vegetables in rural areas were perceived as more accessible, available and of better quality, 83 , 85 , 86 , 88 whereas in urban areas, the availability of unhealthy foods was increasing. 86 Urban life was also associated with sedentary lifestyles due to increasing mechanization and technology. 69 , 85 , 111 , 112 , 116 As mentioned above, increasingly built environments were perceived as limiting opportunities for physical activity in urban spaces. 104
One impact of current technology is that we are not required to move physically. As a result, people become fatter because they are becoming lazier to move. ( 116 Indonesia, WRA)
Economic development, particularly in cities, including increasing consumerism was perceived as a barrier to healthy lifestyles. 58 Furthermore, the busy urban lifestyles with more women in the workforce and reduced appreciation of food preparation 73 impacted on cooking and eating habits. Studies highlighted the increasing need for quick, simple and convenient meals. 73 , 77 , 85 , 100 , 119 , 124
3.6. Data‐driven framework
Using the a priori meta‐framework allowed us to conceptualize the factors that are perceived to directly or indirectly influence obesogenic behaviours by adolescent girls and WRA. After synthesis, the identified themes through both the deductive and inductive approaches resulted in the data‐driven framework as presented in Figure 2. Individual‐level factors were prominent in our framework, identifying food safety concerns and attribution in addition to the constructs of the a priori meta‐framework. Data on physical and macro‐level factors were limited and are therefore represented to a limited extent in our framework. Gender was identified as cutting across all four levels in our framework.
4. DISCUSSION
This review sought to synthesize qualitative evidence on factors influencing obesogenic (eating and physical activity) behaviours in adolescent girls and WRA in LMICs. Influencing factors were examined across multiple contexts and within and across social, physical and macro levels using an a priori defined meta‐framework. The data synthesis revealed a data‐driven framework that included influencing factors on adolescent girls and WRA, as well as their obesogenic behaviours. These factors are interrelated and reflect their individual‐, social‐, physical‐ and macro‐level influences. The findings of this synthesis provide a greater insight into the obesogenic behaviours of adolescent girls and women in LMICs, which will help to inform design interventions for obesity prevention tailored to different stages of the life cycle.
Awareness of the value of a healthy diet and physical activity for good health was good overall, but it was overshadowed by a failure to recognize the importance of healthy behaviours for everyone across the life cycle. This attribution error appeared relevant for both dietary activity behaviour and physical activity behaviour. Adolescents perceived healthy lifestyles as only relevant for older people and, therefore, not of immediate concern to them, which has also been found in HICs. 128 , 129 Women, on the other hand, often perceived their body weight or health as predestined. Physical activity was considered more appropriate for children, older people with poor health and/or overweight, professional athletes or men. Reduced engagement with physical activity with increasing age could also be due to life transition periods, competing priorities such as schoolwork, 130 social activities and/or increased workload. 131
Fear of poor food hygiene and stronger trust in packaged, labelled and/or processed food were most dominant in studies from Africa and Asia. This immediate fear of food safety can overshadow concerns for more long‐term concerns related to nutrition. 132 Improving food hygiene of healthier foods and beverages, or even the perception of improved food hygiene, therefore, has a role to play in preventing obesity and related NCDs, while taking into account the role that informal vendors and markets play in providing fruit and vegetables. 133
Changes in diets and physical activity were apparent due to migration from rural to urban areas, and this held true across generations. At the same time, women across studies observed that increasing urbanization increased availability and affordability of unhealthy ultra‐processed and snack foods, and reduced access to safe and affordable spaces for physical activity and limited time for healthy behaviours due to busy lives. The shift from traditional to ultra‐processed food, limited time to prepare fresh food and the omnipresence and promotion of cheap, unhealthy ultra‐processed foods and drinks in school or neighbourhood environments tempted girls and women to buy them. These dietary shifts, alongside increasing availability and promotion of unhealthy foods, have been well defined as the ‘nutrition transition’ 14 , 15 in prior literature on LMICs and in low‐income communities of HICs. 134 Dietary shifts from traditional food towards more eating away from home and consuming convenience food high in sugar has been observed in other LMICs following migration to urban centres. 27 , 135 , 136 Participants have also observed changes in urban planning, which caused limited access to aesthetic, safe and secure recreation spaces or facilities. The latter has been associated with crime and fear of sexual harassment 27 as well as lower levels of physical activity. 16
Pronounced across most identified themes of our framework is the influence of gender norms. Culturally‐, socially‐ and religiously‐driven gender roles appear to hinder girls and women from being physically active and from consuming healthy food. Girls and women experienced physical activity and/or clothing restrictions based on familial, societal or religious norms. Additionally, girls and women have to fulfil their roles in the household and family, which further limits women's time available for physical activity, especially when added to employment and childcare responsibilities. Busier lives were also described, particularly by employed adult women. However, few studies focused on workplaces, which could have offered valuable insights into possible interventions for adult women given their increasing presence in the workforce. These types of time limitations have been associated with more women classified as having obesity. 137 Furthermore, girls and women might prefer different types of physical activity than men, 138 but school curricula, urban environments and/or gym facilities do not cater for their interests. 130 , 131 , 139 Globally, girls and women tend to be less physically active than men/boys, 140 with highest rates of insufficient physical activity in south/central Asia, the Middle East and north Africa. 140 These regions were also identified by our review as most culturally restrictive of public movement of girls and women. Similar to our findings, quantitative studies have identified limited opportunities for safe and accessible leisure time activity. 138 , 140 Also, the fact that physical education programmes in schools are not tailored to girls' needs, by focusing more on athletic abilities rather than encouragement, was confirmed by other studies in low‐income settings of HICs. 130 , 131 The tendency of women in the reviewed studies to conform with their husbands' and children's dietary choices could also affect their own dietary behaviours. 2 , 26 Poor decision‐making power and gender inequality in general appears to expose women more strongly to multiple burdens of malnutrition. 141 Furthermore, women and girls in the reviewed studies, particularly from South America and Asia, also felt pressure to conform to their society's feminine ideals, which for girls mostly meant being thin. This could push them towards dieting rather than eating a balanced diet, while avoiding looking sweaty/dirty from engaging in physical activity to maintain a ‘feminine’ appearance. 139 For adult women, larger body sizes were associated with maturity, dignity, wealth, good health and beauty, which has been acknowledged previously as relevant in poor, rural communities across Africa. 26 , 27
As revealed by our sensitivity analysis, the identified factors might differ between urban and rural settings and between adolescents and WRA. In rural settings, awareness of underweight and micronutrient deficiencies, as well as the importance of eating food that is filling rather than tasty, was more widespread. Accessing healthy, safe fruit and vegetables was a challenge, particularly in studies from South America and Africa, which could be due to a reduction in urban neighbourhood markets accompanied by a rise in remote supermarkets. 13 , 142 The perception that healthy foods are expensive is also supported by studies assessing price data in LMICs, 143 making healthy diets difficult to afford for lower socio‐economic populations. 144
For adolescent girls, choosing unhealthy, ‘modern’ foods gave them a feeling of empowerment. Even with the little pocket money they had, as their parents controlled most of their other choices, they were able to buy snacks at and around school based on taste, appearance and social desirability of their peers. Peer influence towards ‘modern’ food has also been described in HICs, but with more pressure towards expensive and branded products. 128 The increasing availability of mass/social media could make sedentary lifestyles more tempting for adolescent girls. Besides being poor role models for physical activity, parents pressured their adolescent children into studying over being physically active, which was also found in families of low‐income settings in HICs. 130 For adult women, lack of peer influence, lack of a social network and/or sufficient time besides family and household responsibilities could be limiting factors for physical activity and were also shown to affect women's overall autonomy. 145
4.1. Limitations and implications for future research/programming
Although this review followed a rigorous methodology and we have moderate to high confidence that the review findings are a reasonable representation of the phenomenon of interest, 146 it was not without limitations. Considering solely the perspectives of women and adolescent girls limited the findings of this review to the female perspective. Gender norms were identified as a strong cross‐cutting issue for almost all of the influencing factors. Thus, male perceptions would enrich insights into these societal issues. 28 Only two of the included studies were conducted in low‐income countries, which poses an important gap for future research. Furthermore, this review solely included factors influencing obesogenic behaviours and did not consider factors that influence underweight or micronutrient deficiencies. However, this review does acknowledge the role of early life food shortage as an important influencing factor to later life weight status. In light of the increasing double burden of malnutrition, this may be particularly relevant, as more than half of the included studies (n = 48) were conducted in countries with medium, high or very high double burden of malnutrition. 15
This QES revealed several implications for future research. Similar to the conclusions of a review on Africa‐only studies that included mainly quantitative research, we found that factors related to the physical and macro levels are insufficiently studied and require further investigation. 26 , 27
This could be due to the fact that participants in qualitative studies are more likely to focus on barriers or facilitators at individual and social levels and that qualitative studies are less likely to be used to capture the physical food environment 50 and the macro environment. More than 100 studies had to be excluded given a lack of data attributable to participant sex or age; data on the socio‐economic status of participants were also inconsistent. Clearer and attributable information on participants' demographic and socio‐economic situation would help put research findings into more specific contexts and has significant potential to strengthen the evidence base and inform future interventions. In most studies, data on individual level factors were predominant.
Finding programme and policy solutions to overcome the growing obesity pandemic is a significant challenge. As has been demonstrated in our framework, the drivers are complex and span multiple individual and environmental levels. Historically, obesity programmes have focused on education interventions targeting individual behaviours and responsibility. Our findings showed that improving education remains relevant, but that education interventions should put a stronger focus on the misconceived association between food safety and nutrient content of food. Furthermore, the importance of promoting healthy diets and physical activity for everyone across the whole life cycle should be addressed through interventions tailored specifically to adolescent girls and WRA. However, addressing determinants of the broader environment beyond the individual level through novel solutions is also called for. Gender norms need to be addressed with both men and women regarding traditional roles of women and girls in society that negatively impact on nutrition and by supporting employed women through workplace interventions.
Food system innovations 147 , 148 offer potential solutions to making healthy food more available, affordable, safe and appealing, while making unhealthy foods less available and affordable. This could be achieved by combining education, regulatory (advertising) and/or fiscal interventions (taxation) while improving implementation of hygiene and food safety standards in all settings, but particularly in schools. 8 , 149 Transport and urban planning policies could further improve access to healthy food and safe recreation spaces. 150 Education policies should focus more on curricula for nutrition and physical education 33 with the latter aiming to more strongly promote girls' participation. Guidelines for school food supply should target not only potential cafeterias but also vendors in and around schools. 151 Given the poor security in many LMIC urban areas, schools could also provide access to safe recreation facilities for the community, which would encourage physical activity of out‐of‐school adolescents and women.
In conclusion, some of the identified factors are similar to those identified in HICs, such as increasing availability, affordability and promotion of unhealthy food; peer pressure; social desirability; and time constraints related to food and physical activity, particularly in adolescents of lower income communities. Specific to LMICs is the concern for the food safety of perishable foods that increasingly drives consumption of unhealthy foods. Busier lives influenced by gender norms and limited safe and secure exercise spaces keep girls and women from being physically active. Diverse and flexible solutions, at different levels and for rural and urban settings, are urgently needed to address these obesogenic factors in LMICs, where most people with overweight and obesity live.
Supporting information
Data S1 Supporting Information
ACKNOWLEDGEMENTS
We would like to thank Joke Webbink for assistance during the protocol development and search. Financial support was provided by Agriculture for Nutrition and Health (A4NH) Supporting Policies, Programs, and Enabling Action through Research (SPEAR) Flagship (203004.001.424).
Trübswasser U, Verstraeten R, Salm L, et al. Factors influencing obesogenic behaviours of adolescent girls and women in low‐ and middle‐income countries: A qualitative evidence synthesis. Obesity Reviews. 2021;22:e13163. 10.1111/obr.13163
REFERENCES
- 1. Keats C, Rappaport A, Jain R, Oh C, Shah S, Bhutta ZA. Diet and eating practices among adolescent girls in low‐ and middle‐income countries: a systemic review. Arlington, VA: Strengthening Partnerships, Results, and Innovations in Nutrition Globally (SPRING) project; 2018.
- 2. Harris‐Fry H, Shrestha N, Costello A, Saville NM. Determinants of intra‐household food allocation between adults in South Asia—a systematic review. Int J Equity Health. 2017;16(1):107. 10.1186/s12939-017-0603-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Zerfu TA, Umeta M, Baye K. Dietary habits, food taboos, and perceptions towards weight gain during pregnancy in Arsi, rural Central Ethiopia: a qualitative cross‐sectional study. J Health Popul Nutr. 2016;35(1):22. 10.1186/s41043-016-0059-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Wells JC, Sawaya AL, Wibaek R, et al. The double burden of malnutrition: aetiological pathways and consequences for health. Lancet. 2020;395(10217):75‐88. 10.1016/S0140-6736(19)32472-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Webster‐Gandy J, Madden A, Holdsworth M. Oxford Handbook of Nutrition and Dietetics. Oxford Han: Oxford University Press. [Google Scholar]
- 6. Black RE, Victora CG, Walker SP, et al. Maternal and child undernutrition and overweight in low‐income and middle‐income countries. Lancet. 2013;382(9890):427‐451. 10.1016/S0140-6736(13)60937-X [DOI] [PubMed] [Google Scholar]
- 7. Development Initiatives . Global Nutrition Report: Shining a Light to Spur Action on Nutrition. Bristol, UK; 2018.
- 8. Shekar M, Popkin B. Obesity: Health and Economic Consequences of an Impending Global Challenge. Washington D.C.; 2020. [Google Scholar]
- 9. Benedict R, Schmale A, Namaste S. Adolescent nutrition 2000–2017: DHS data on adolescents age 15–19. DHS comparative report no. 47. Rockville, Maryland, USA; 2018.
- 10. Afshin A, Forouzanfar MH, Reitsma MB, et al Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med. 2017. 377, 1, 13, 27 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. WHO . Global status report on noncommunicable diseases 2010. Geneva; 2011.
- 12. Rtveladze K, Marsh T, Webber L, et al. Health and economic burden of obesity in Brazil. PLoS One. 2013;8(7):e68785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Reardon T, Timmer CP, Barrett CB, Berdegué J. The rise of supermarkets in Africa, Asia, and Latin America. Am J Agric Econ. 2003;85(5):1140‐1146. http://www.jstor.org/stable/1244885 [Google Scholar]
- 14. Monteiro CA, Moubarac JC, Cannon G, Ng SW, Popkin B. Ultra‐processed products are becoming dominant in the global food system. Obes Rev. 2013;14(Suppl 2):21‐28. 10.1111/obr.12107 [DOI] [PubMed] [Google Scholar]
- 15. Popkin BM, Corvalan C, Grummer‐Strawn LM. Dynamics of the double burden of malnutrition and the changing nutrition reality. Lancet. 2020;395(10217):65‐74. 10.1016/S0140-6736(19)32497-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Bauman AE, Reis RS, Sallis JF, Wells JC, Loos RJF, Martin BW. Correlates of physical activity: why are some people physically active and others not? Lancet. 2012;380(9838):258‐271. 10.1016/S0140-6736(12)60735-1 [DOI] [PubMed] [Google Scholar]
- 17. Ford ND, Patel SA, Narayan KM. Obesity in low‐ and middle‐income countries: burden, drivers, and emerging challenges. Annu Rev Public Health. 2017;38:145‐164. 10.1146/annurev-publhealth-031816-044604 [DOI] [PubMed] [Google Scholar]
- 18. Popkin BM. The shift in stages of the nutrition transition in the developing world differs from past experiences! Public Health Nutr. 2002;5(1A):205‐214. 10.1079/PHN2001295 [DOI] [PubMed] [Google Scholar]
- 19. Monteiro CA, Moura EC, Conde WL, Popkin BM. Socioeconomic status and obesity in adult populations of developing countries: a review. Bull World Health Organ. 2004;82(12):940‐946. [PMC free article] [PubMed] [Google Scholar]
- 20. Agurs‐Collins T, Bouchard C. Gene‐nutrition and gene‐physical activity interactions in the etiology of obesity. Introduction. Obesity (Silver Spring). 2008;16(Suppl 3):S2‐S4. 10.1038/oby.2008.510 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Jaacks LM, Kavle J, Perry A, Nyaku A. Programming maternal and child overweight and obesity in the context of undernutrition: current evidence and key considerations for low‐ and middle‐income countries. Public Health Nutr. 2017;20(7):1286‐1296. 10.1017/S1368980016003323 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Butland B, Jebb S, Koppelman P. Tackling obesities: future choices—project report. Foresight 2007. [DOI] [PubMed]
- 23. Leroy JL, Olney DK, Ruel MT. PROCOMIDA, a food‐assisted maternal and child health and nutrition program, contributes to postpartum weight retention in Guatemala: a cluster‐randomized controlled intervention trial. J Nutr. 2019;149(12):2219‐2227. 10.1093/jn/nxz175 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Lobstein T, Jackson‐Leach R, Moodie ML, et al. Child and adolescent obesity: part of a bigger picture. Lancet (London, England). 2015;385(9986):2510‐2520. 10.1016/S0140-6736(14)61746-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Lobstein T, Dibb S. Evidence of a possible link between obesogenic food advertising and child overweight. Obes Rev. 2005;6(3):203‐208. 10.1111/j.1467-789X.2005.00191.x [DOI] [PubMed] [Google Scholar]
- 26. Gissing SC, Pradeilles R, Osei‐Kwasi HA, Cohen E, Holdsworth M. Drivers of dietary behaviours in women living in urban Africa: a systematic mapping review. Public Health Nutr. 2017;20(12):2104‐2113. 10.1017/S1368980017000970 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Ozodiegwu ID, Littleton MA, Nwabueze C, et al. A qualitative research synthesis of contextual factors contributing to female overweight and obesity over the life course in sub‐Saharan Africa. PLoS One. 2019;14(11):e0224612. 10.1371/journal.pone.0224612 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Osei‐Kwasi HA, Mohindra A, Booth A, et al. Factors influencing dietary behaviours in urban food environments in Africa: a systematic mapping review. Public Health Nutr (In Press). 2020;23(14):2584‐2601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Osei‐Assibey G, Dick S, Macdiarmid J, et al. The influence of the food environment on overweight and obesity in young children: a systematic review. BMJ Open. 2012;2(6):1–12. 10.1136/bmjopen-2012-001538 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Mazarello Paes V, Ong KK, Lakshman R. Factors influencing obesogenic dietary intake in young children (0–6 years): systematic review of qualitative evidence. BMJ Open. 2015;5(9):e007396. 10.1136/bmjopen-2014-007396 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Leandro CG, Fonseca EV, de Lim CR, Tchamo ME, Ferreira‐e‐Silva WT. Barriers and enablers that influence overweight/obesity/obesogenic behavior in adolescents from lower‐middle income countries: a systematic review. Food Nutr Bull. 2019;40(4):562‐571. 10.1177/0379572119853926 [DOI] [PubMed] [Google Scholar]
- 32. Madjdian DS, Azupogo F, Osendarp SJM, Bras H, Brouwer ID. Socio‐cultural and economic determinants and consequences of adolescent undernutrition and micronutrient deficiencies in LLMICs: a systematic narrative review. Ann N Y Acad Sci. 2018;1416(1):117‐139. [Google Scholar]
- 33. Verstraeten R, Roberfroid D, Lachat C, et al. Effectiveness of preventive school‐based obesity interventions in low‐ and middle‐income countries: a systematic review. Am J Clin Nutr. 2012;96(2):415‐438. 10.3945/ajcn.112.035378 [DOI] [PubMed] [Google Scholar]
- 34. Romieu I, Dossus L, Barquera S, et al. Energy balance and obesity: what are the main drivers? Cancer Causes Control. 2017;28(3):247‐258. 10.1007/s10552-017-0869-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Flemming K, Booth A, Garside R, Tunçalp Ö, Noyes J. Qualitative evidence synthesis for complex interventions and guideline development: clarification of the purpose, designs and relevant methods. BMJ Glob Health. 2019;4(Suppl 1):e000882. 10.1136/bmjgh-2018-000882 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Booth A, Carroll C. How to build up the actionable knowledge base: the role of ‘best fit’ framework synthesis for studies of improvement in healthcare. BMJ Qual Saf. 2015;24:bmjqs‐2014(11):700‐708. 10.1136/bmjqs-2014-003642 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Ziemann A, Brown L, Sadler E, Ocloo J, Boaz A, Sandall J. Influence of external contextual factors on the implementation of health and social care interventions into practice within or across countries—a protocol for a ‘best fit’ framework synthesis. Syst Rev. 2019;8(1):258. 10.1186/s13643-019-1180-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Shamseer L, Moher D, Clarke M, et al. Preferred reporting items for systematic review and meta‐analysis protocols (PRISMA‐P) 2015: elaboration and explanation. BMJ. 2015;349:1–25. 10.1136/bmj.g7647 [DOI] [PubMed] [Google Scholar]
- 39. Tong A, Flemming K, McInnes E, Oliver S, Craig J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med Res Methodol. 2012;12(1):181. 10.1186/1471-2288-12-181 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Booth A, Carroll C. Systematic searching for theory to inform systematic reviews: is it feasible? Is it desirable? Health Info Libr J. 2015;32(3):220‐235. 10.1111/hir.12108 [DOI] [PubMed] [Google Scholar]
- 41. Booth A. Unpacking your literature search toolbox: on search styles and tactics. Health Info Libr J. 2008;25(4):313‐317. 10.1111/j.1471-1842.2008.00825.x [DOI] [PubMed] [Google Scholar]
- 42. Simmons A, Mavoa HM, Bell AC, et al. Creating community action plans for obesity prevention using the ANGELO (analysis grid for elements linked to obesity) framework. Health Promot Int. 2009;24(4):311‐324. 10.1093/heapro/dap029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Swinburn BA, Sacks G, Hall KD, et al. The global obesity pandemic: shaped by global drivers and local environments. Lancet. 2011;378(9793):804‐814. 10.1016/S0140-6736(11)60813-1 [DOI] [PubMed] [Google Scholar]
- 44. Stok FM, Hoffmann S, Volkert D, et al. The DONE framework: creation, evaluation, and updating of an interdisciplinary, dynamic framework 2.0 of determinants of nutrition and eating. PLoS One. 2017;12(2):e0171077. 10.1371/journal.pone.0171077 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Story M, Kaphingst KM, Robinson‐O'Brien R, Glanz K. Creating healthy food and eating environments: policy and environmental approaches. Annu Rev Public Health. 2008;29:253‐272. 10.1146/annurev.publhealth.29.020907.090926 [DOI] [PubMed] [Google Scholar]
- 46. Booth SL, Sallis JF, Ritenbaugh C, et al. Environmental and societal factors affect food choice and physical activity: rationale, influences, and leverage points. Nutr Rev. 2001;59(3 Pt 2):S21‐S39; discussion S57–65. 10.1111/j.1753-4887.2001.tb06983.x [DOI] [PubMed] [Google Scholar]
- 47. Sallis JF, Cervero RB, Ascher W, Henderson KA, Kraft MK, Kerr J. An ecological approach to creating active living communities. Annu Rev Public Health. 2006;27:297‐322. 10.1146/annurev.publhealth.27.021405.102100 [DOI] [PubMed] [Google Scholar]
- 48. Chastin SF, De Craemer M, Lien N, et al. The SOS‐framework (systems of sedentary behaviours): an international transdisciplinary consensus framework for the study of determinants, research priorities and policy on sedentary behaviour across the life course: a DEDIPAC study. Int J Behav Nutr Phys Act. 2016;13(1):83. 10.1186/s12966-016-0409-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Condello G, Ling FC, Bianco A, et al. Using concept mapping in the development of the EU‐PAD framework (EUropean‐physical activity determinants across the life course): a DEDIPAC‐study. BMC Public Health. 2016;16(1):1145. 10.1186/s12889-016-3800-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Holdsworth M, Landais E. Urban food environments in Africa: implications for policy and research. Proc Nutr Soc. 2019;78(4):513‐525. 10.1017/S0029665118002938 [DOI] [PubMed] [Google Scholar]
- 51. Booth A. Clear and present questions: formulating questions for evidence based practice. Libr HI TECH. 2006;24(3):355‐368. 10.1108/07378830610692127 [DOI] [Google Scholar]
- 52. World Bank Country and Lending Groups . https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups2019. Accessed March 1, 2019.
- 53. CASP . Critical appraisal skills programme. CASP (Sytematic Review) Checklist. www.casp-uk.net. Published 2018. Accessed September 1, 2019.
- 54. Carroll C, Booth A, Lloyd‐Jones M. Should we exclude inadequately reported studies from qualitative systematic reviews? An evaluation of sensitivity analyses in two case study reviews. Qual Health Res. 2012;22(10):1425‐1434. 10.1177/1049732312452937 [DOI] [PubMed] [Google Scholar]
- 55. France EF, Wells M, Lang H, Williams B. Why, when and how to update a meta‐ethnography qualitative synthesis. Syst Rev. 2016;5(1):44. 10.1186/s13643-016-0218-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Caamano MC, Ronquillo D, Kimoto R, Garcia OP, Long KZ, Rosado JL. Beliefs and motives related to eating and body size: a comparison of high‐BMI and normal‐weight young adult women from rural and urban areas in Mexico. BMC Public Health. 2016;16(1):1014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Karimi‐Shahanjarini A, Omidvar N, Bazargan M, Rashidian A, Majdzadeh R, Shojaeizadeh D. Iranian female adolescent's views on unhealthy snacks consumption: a qualitative study. Iran J Public Health. 2010;39(3):92–101. [PMC free article] [PubMed] [Google Scholar]
- 58. Amiri P, Ghofranipour F, Ahmadi F, Hooman H, Hosseinpanah F, Jalali‐Farahani S. Barriers to a healthy lifestyle among obese adolescents: a qualitative study from Iran. Int J Public Health. 2011;56(2):181‐189. [DOI] [PubMed] [Google Scholar]
- 59. Aryeetey RNO. Perceptions and experiences of overweight among women in the Ga East District, Ghana. Front Nutr. 2016;3:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Madrigal L, Adams I, Chacon V, Barnoya J. Perceived barriers to achieving a healthy weight: a qualitative study using focus groups at public and private schools in Guatemala City. BMC Public Health. 2017;17(1):16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Ware LJ, Prioreschi A, Bosire E, et al. Environmental, social, and structural constraints for health behavior: perceptions of young urban Black women during the preconception period‐a healthy life trajectories initiative. J Nutr Educ Behav. 2019;51(8):946‐957. [DOI] [PubMed] [Google Scholar]
- 62. Abdelghaffar E‐A, Hicham EK, Siham B, Samira EF, Youness EA. Perspectives of adolescents, parents, and teachers on barriers and facilitators of physical activity among school‐age adolescents: a qualitative analysis. Environ Health Prev Med. 2019;24(1):21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Draper CE, Davidowitz KJ, Goedecke JH. Perceptions relating to body size, weight loss and weight‐loss interventions in black South African women: a qualitative study. Public Health Nutr. 2016;19(3):548‐556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Kinsman J, Norris SA, Kahn K, et al. A model for promoting physical activity among rural South African adolescent girls. Glob Health Action. 2015;8(1):28790. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Monge‐Rojas R, Garita‐Arce C, Sánchez‐López M, Colon‐Ramos U, Sanchez‐Lopez M. Barriers to and suggestions for a healthful, active lifestyle as perceived by rural and urban Costa Rican adolescents. J Nutr Educ Behav. 2009;41(3):152‐160. [DOI] [PubMed] [Google Scholar]
- 66. Rajaraman D, Correa N, Punthakee Z, et al. Perceived benefits, facilitators, disadvantages, and barriers for physical activity amongst South Asian adolescents in India and Canada. J Phys Act Health. 2015;12(7):931‐941. [DOI] [PubMed] [Google Scholar]
- 67. Baheiraei A, Hamzehgardeshi Z, Mohammadi MR, Mohammadi E, Nedjat S. Iranian adolescents' insufficient physical activity: a mixed methods explanatory sequential study. Int J Adolesc Med Health. 2016;28(1):79‐89. [DOI] [PubMed] [Google Scholar]
- 68. Doegah P, Amoateng A Misconceptions about physical activity among Ghanaian youth. In: 2017 International Population Conference. IUSSP; 2017.
- 69. Walter CM, Du Randt R. Socio‐cultural barriers to physical activity among black Isixhosa speaking professional women in the Nelson Mandela metropolitan municipality. South African J Res Sport Phys Educ Recreat. 2011;33(2):143‐155. [Google Scholar]
- 70. Habibie IY, Brouwer I, Februhartanty J. Eating behaviour of young female workers with low socioeconomic status in Malang City, East Java: a qualitative study. Malays J Nutr. 2019;25:S75‐S86. [Google Scholar]
- 71. Islam MR, Trenholm J, Rahman A, Pervin J, Ekström E‐C, Rahman SM. Sociocultural influences on dietary practices and physical activity behaviors of rural adolescents—a qualitative exploration. Nutrients. 2019;11(12):1‐20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Carrete L, Arroyo P. Social marketing to improve healthy dietary decisions: insights from a qualitative study in Mexico. Qual Mark Res an Int J. 2014;17(3):239‐263. [Google Scholar]
- 73. Chan K, Tse T, Tam D, Huang A. Perception of healthy and unhealthy food among Chinese adolescents. Young Consum. 2016;17(1):32‐45. [Google Scholar]
- 74. Mugo A. Obesity Among Women in Rural Kenya: Knowledge, Beliefs, and Perceptions. ProQuest Diss Theses 2016.
- 75. Monge‐Rojas R, Garita C, Sánchez M, Muñoz L, Sanchez M, Munoz L. Barriers to and motivators for healthful eating as perceived by rural and urban Costa Rican adolescents. J Nutr Educ Behav. 2005;37(1):33‐40. [DOI] [PubMed] [Google Scholar]
- 76. Blum L, Mellisa A, Sari EK, et al. Snacking behavior in adolescent girls living in urban cities in Java, Indonesia. Ann Nutr Metab. 2017;71:568. [Google Scholar]
- 77. Wrottesley SV, Bosire EN, Mukoma G, et al. Age and gender influence healthy eating and physical activity behaviours in South African adolescents and their caregivers: transforming adolescent lives through nutrition initiative (TALENT). Public Health Nutr. 2019;1‐20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Monge‐Rojas R, Fuster‐Baraona T, Garita C, et al. The influence of gender stereotypes on eating habits among Costa Rican adolescents. Am J Health Promot. 2015;29(5):303‐310. [DOI] [PubMed] [Google Scholar]
- 79. Correa N, Rajaraman D, Swaminathan S, et al. Perceptions of healthy eating amongst Indian adolescents in India and Canada. Appetite. 2017;116:471‐479. [DOI] [PubMed] [Google Scholar]
- 80. Dapi LN, Omoloko C, Janlert U, Dahlgren L, Haglin L, Håglin LI. Eat to be happy, to be strong, and to live—perceptions of rural and urban adolescents in Cameroon, Africa. J Nutr Educ Behav. 2007;39(6):320‐326. [DOI] [PubMed] [Google Scholar]
- 81. Romero MYM, Jeitner EC, Francis LA. Visualizing perceived enablers of and barriers to healthy eating by youth in rural El Salvador. J Nutr Educ Behav. 2019;51(3):348‐356. [DOI] [PubMed] [Google Scholar]
- 82. Sedibe HM, Kahn K, Edin K, Gitau T, Ivarsson A, Norris SA. Qualitative study exploring healthy eating practices and physical activity among adolescent girls in rural South Africa. BMC Pediatr. 2014;14(1):211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83. Usman A, Javed M, Amjad A, Jalil A, Shaheen I, Amjad U. Food, city and young Globavores: perceptions of Pakistani urban youth about food choices and healthy eating. Anthropologie. 2017;27(1–3):143‐151. [Google Scholar]
- 84. Abdi N, Sadeghi R, Zamani‐Alavijeh F, Taghdisi MH, Shojaeezadeh D. Explaining nutritional habits and behaviors of low socioeconomic status women in Sanandaj: a qualitative content analysis. Electron Physician. 2016;8(1):1733‐1739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85. Bailey C, Garg V, Deksha K, Wasser H, Dorairaj P, Jaacks LM. Food choice drivers in the context of the nutrition transition in Delhi, India. J Nutr Educ Behav. 2018;50(7):675‐686. [DOI] [PubMed] [Google Scholar]
- 86. Lipus AC, Leon JS, Calle SC, Andes KL. “It is not natural anymore”: nutrition, urbanization, and indigenous identity on Bolivia's Andean plateau. (special issue: connundrums of care.). Qual Health Res. 2018;28(11):1802‐1812. [DOI] [PubMed] [Google Scholar]
- 87. Bastami F, Zamani‐Alavijeh F, Mostafavi F. Factors behind healthy snack consumption at school among high‐school students: a qualitative study. BMC Public Health. 2019;19(1):1342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88. Hunter‐Adams J, Battersby J, Oni T. Food insecurity in relation to obesity in peri‐urban Cape Town, South Africa: implications for diet‐related non‐communicable disease. Appetite. 2019;137:244‐249. [DOI] [PubMed] [Google Scholar]
- 89. Pahlm J, Svensson J, Joshi SK, Swahnberg K. Physical activity and diet among adolescents of Kathmandu, Nepal: knowledge and attitudes. J Kathmandu Med Coll. 2014;2(2):51‐58. [Google Scholar]
- 90. Sondari M, Brouwer I, Februhartanty J. Eating behaviour of adolescent schoolgirls in Malang, East Java: a qualitative study. Malays J Nutr. 2019;25:S87‐S96. [Google Scholar]
- 91. Veeck A, Grace Yu F, Yu H, Veeck G, Gentry JW. Influences on food choices of urban Chinese teenagers. Young Consum. 2014;15(4):296‐311. [Google Scholar]
- 92. Cohen E, Amougou N, Ponty A, et al. Nutrition transition and biocultural determinants of obesity among Cameroonian migrants in urban Cameroon and France. Int J Environ Res Public Health. 2017;14(7):696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93. Georgina S. Body size perceptions of women and obesity in urban Uganda. Afr Study Monogr. 2019;40(1):1‐21. [Google Scholar]
- 94. Kimoto R, Ronquillo D, Caamaño MC, et al. Food, eating and body image in the lives of low socioeconomic status rural Mexican women living in Queretaro State, Mexico. In: Heal Place; 2014. [DOI] [PubMed] [Google Scholar]
- 95. Rodriguez‐Ventura AL, Pelaez‐Ballestas I, Samano‐Samano R, Jimenez‐Gutierrez C, Aguilar‐Salinas C. Barriers to lose weight from the perspective of children with overweight/obesity and their parents: a sociocultural approach. J Obes. 2014;2014:575184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96. Stupar D, Eide WB, Bourne L, Hendricks M, Iversen PO, Wandel M. The nutrition transition and the human right to adequate food for adolescents in the Cape Town metropolitan area: implications for nutrition policy. Food Policy. 2012;37(3):199‐206. [Google Scholar]
- 97. Gonçalves H, González DA, Araújo CP, et al. Adolescents' perception of causes of obesity: unhealthy lifestyles or heritage? J Adolesc Health. 2012;51(6):S46‐S52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98. Monge‐Rojas R, Fuster‐Baraona T, Garita‐Arce C, Sanchez‐Lopez M, Colon‐Ramos U, Smith‐Castro V. How self‐objectification impacts physical activity among adolescent girls in Costa Rica. J Phys Act Health. 2017;14(2):123‐129. [DOI] [PubMed] [Google Scholar]
- 99. Phillips EA, Comeau DL, Pisa PT, Stein AD, Norris SA. Perceptions of diet, physical activity, and obesity‐related health among black daughter–mother pairs in Soweto, South Africa: a qualitative study. BMC Public Health. 2016;16:750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100. Majabadi HA, Solhi M, Montazeri A, et al. Factors influencing fast‐food consumption among adolescents in Tehran: a qualitative study. Iran Red Crescent Med J. 2016;18(3):1‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101. Phillips JS, Awotidebe AW. The influence of the social environment on youth physical activity: sport education and community development. (special issue: current issues in sport, physical activity, recreation and health.). African J Phys Heal Educ Recreat Danc. 2015;21(Suppl. 1):263‐271. [Google Scholar]
- 102. Satija A, Khandpur N, Satija S, et al. Physical activity among adolescents in India: a qualitative study of barriers and enablers. Health Educ Behav. 2018;45(6):926‐934. [DOI] [PubMed] [Google Scholar]
- 103. Lemamsha H, Papadopoulos C, Randhawa G. Understanding the risk and protective factors associated with obesity amongst Libyan adults—a qualitative study. BMC Public Health. 2018;18(1):493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104. Öztürk P, Koca C. Generational analysis of leisure time physical activity participation of women in Turkey. Leis Stud. 2019;38(2):232‐244. [Google Scholar]
- 105. De Silva Weliange S, Fernando D, Gunatilake J. Neighbourhood social environment on physical activity among adults in Sri Lanka: a qualitative inquiry. J Coll Commun Phys Sri Lanka. 2018;24:28‐35. [Google Scholar]
- 106. Kalani ZM, Pourmovahed ZM, Farajkhoda TP, Bagheri IMA. Qualitative approach to Women's perspectives on exercise in Iran. Int J Community Based Nurs Midwifery. 2018;6(2):156‐166. [PMC free article] [PubMed] [Google Scholar]
- 107. Brown C, Shaibu S, Maruapula S, Malete L, Compher C. Perceptions and attitudes towards food choice in adolescents in Gaborone, Botswana. Appetite. 2015;95:29‐35. [DOI] [PubMed] [Google Scholar]
- 108. Kroone D, Alant B. Understanding influences on teenage food choices in a Durban high school with a view to improving praxis. Int J Consum Stud. 2012;36(4):472‐479. [Google Scholar]
- 109. Gavaravarapu SM, Rao KM, Nagalla B, Avula L. Assessing differences in risk perceptions about obesity among “normal‐weight” and “overweight” adolescents—a qualitative study. J Nutr Educ Behav. 2015;47(6):488‐497. [DOI] [PubMed] [Google Scholar]
- 110. Peykari N, Eftekhari MB, Tehrani FR, et al. Promoting physical activity participation among adolescents: the barriers and the suggestions. Int J Prev Med. 2015;12:1‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111. Ssewanyana D, van Baar A, Newton CR, Abubakar A. A contextually relevant approach to assessing health risk behavior in a rural sub‐Saharan Africa setting: the Kilifi health risk behavior questionnaire. BMC Public Health. 2018;18(1):774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112. Garg S, Raman Kutty V. Do I need exercise? A qualitative study on factors affecting leisure‐time physical activity in India. Qual Rep. 2019;24(5):1065‐1082. [Google Scholar]
- 113. Voorend CGN, Norris SA, Griffiths PL, Sedibe MH, Westerman MJ, Doak CM. “We eat together; today she buys, tomorrow I will buy the food”: adolescent best friends' food choices and dietary practices in Soweto, South Africa. Public Health Nutr. 2013;16(3):559‐567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114. Chang CT, Chang KH, Cheah WL. Adults' perceptions of being overweight or obese: a focus group study. Asia Pac J Clin Nutr. 2009;18(2):257‐264. [PubMed] [Google Scholar]
- 115. Atik D, Ertekin ZO. Children's perception of food and healthy eating: dynamics behind their food preferences. Int J Consum Stud. 2013;37(1):59‐65. [Google Scholar]
- 116. Fachruddin II, Februhartanty J, Bardosono S, Khusun H, Worsley A. Perceptions of the causes of obesity among normal weight, overweight and obese Indonesian women: a mixed methods approach. Malays J Nutr. 2019;25:S97‐S110. [Google Scholar]
- 117. Kurschner S, Madrigal L, Chacon V, Barnoya J, Rohloff P. Impact of school and work status on diet and physical activity in rural Guatemalan adolescent girls: a qualitative study. Ann N Y Acad Sci. 2019;1468(1):16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118. Hosseini SV, Anoosheh M, Abbaszadeh A, Ehsani M. Qualitative Iranian study of parents' roles in adolescent girls' physical activity habit development. Nurs Health Sci. 2013;15(2):207‐212. [DOI] [PubMed] [Google Scholar]
- 119. Rathi N, Riddell L, Worsley A. What influences urban Indian secondary school students' food consumption?—a qualitative study. Appetite. 2016;105:790‐797. [DOI] [PubMed] [Google Scholar]
- 120. Bagherniya M, Darani FM, Sharma M, Allipour‐Birgani R, Taghipour A, Safarian M. Qualitative study to determine stressors influencing dietary and physical activity behaviors of overweight and obese adolescents in Iran. Int J Prev Med. 2019;10(1):1‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121. Saimon R, Choo WY, Bulgiba A. “Feeling unsafe”: a photovoice analysis of factors influencing physical activity behavior among Malaysian adolescents. Asia‐Pacific J Public Heal. 2015;27(2):NP2079‐NP2092. [DOI] [PubMed] [Google Scholar]
- 122. Bagherniya M, Darani FM, Keshavarz SA, et al. The impact of adolescent friendships on unhealthy eating behaviors of overweight and obese adolescents: a qualitative study. Int J Pediatr. 2018;6(10):8385‐8398. [Google Scholar]
- 123. Bridle‐Fitzpatrick S. Food deserts or food swamps?: a mixed‐methods study of local food environments in a Mexican city. Soc Sci Med. 2015;142:202‐213. [DOI] [PubMed] [Google Scholar]
- 124. Craveiro I, Alves D, Amado M, et al. Determinants, health problems, and food insecurity in urban areas of the largest city in Cape Verde. Int J Environ Res Public Health. 2016;13(11):1155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125. Lacroix E, Oliveira E, de Castro JS, Cabral JR, Tavares H, von Ranson KM. “There is no way to avoid the first bite”: a qualitative investigation of addictive‐like eating in treatment‐seeking Brazilian women and men. Appetite. 2019;137:35‐46. [DOI] [PubMed] [Google Scholar]
- 126. Cacavas K, Mavoa H, Kremer P, et al. Tongan adolescents' eating patterns: opportunities for intervention. Asia Pac J Public Health. 2011;23(1):24‐33. [DOI] [PubMed] [Google Scholar]
- 127. Farrell P, Thow AM, Schuster S, Vizintin P, Negin J. Access to a nutritious diet in Samoa: local insights. Ecol Food Nutr. 2019;58(3):189‐206. [DOI] [PubMed] [Google Scholar]
- 128. Scott S, Reilly J, Giles EL, et al. Socio‐ecological influences on adolescent (aged 10–17) alcohol use and linked unhealthy eating behaviours: protocol for a systematic review and synthesis of qualitative studies. Syst Rev. 2017;6(1):1‐8. 10.1186/s13643-017-0574-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129. Neumark‐Sztainer D, Story M, Perry C, Casey MA. Factors influencing food choices of adolescents: findings from focus‐group discussions with adolescents. J am Diet Assoc. 1999;99(8):929‐937. 10.1016/S0002-8223(99)00222-9 [DOI] [PubMed] [Google Scholar]
- 130. Corr M, McSharry J, Murtagh EM. Adolescent Girls' perceptions of physical activity: a systematic review of qualitative studies. Am J Health Promot. 2019;33(5):806‐819. 10.1177/0890117118818747 [DOI] [PubMed] [Google Scholar]
- 131. Martins J, Marques A, Sarmento H, Carreiro Da Costa F. Adolescents' perspectives on the barriers and facilitators of physical activity: a systematic review of qualitative studies. Health Educ Res. 2014;30(5):742‐755. 10.1093/her/cyv042 [DOI] [PubMed] [Google Scholar]
- 132. Walls H, Baker P, Chirwa E, Hawkins B. Food security, food safety & healthy nutrition: are they compatible? Glob Food Sec. 2019;21:69‐71. 10.1016/j.gfs.2019.05.005 [DOI] [Google Scholar]
- 133. Wertheim‐Heck SCO, Raneri JE. A cross‐disciplinary mixed‐method approach to understand how food retail environment transformations influence food choice and intake among the urban poor: experiences from Vietnam. Appetite. 2019;142:104370. 10.1016/j.appet.2019.104370 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134. Pitt E, Gallegos D, Comans T, Cameron C, Thornton L. Exploring the influence of local food environments on food behaviours: a systematic review of qualitative literature. Public Health Nutr. 2017;20(13):2393‐2405. 10.1017/S1368980017001069 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135. Cockx L, Colen L, De Weerdt J. From corn to popcorn? Urbanization and dietary change: evidence from rural‐urban migrants in Tanzania. World Dev. 2018;110:140‐159. 10.1016/j.worlddev.2018.04.018 [DOI] [Google Scholar]
- 136. Bren d'Amour C, Pandey B, Reba M, Ahmad S, Creutzig F, Seto KC. Urbanization, processed foods, and eating out in India. Glob Food Sec. 2020:1‐9. 10.1016/j.gfs.2020.100361 [DOI] [Google Scholar]
- 137. Pinto KA, Griep RH, Rotenberg L, da Conceição Chagas Almeida M, Barreto RS, Aquino EML. Gender, time use and overweight and obesity in adults: results of the Brazilian longitudinal study of adult health (ELSA‐Brasil). PLoS One. 2018;13(3):e0194190. 10.1371/journal.pone.0194190 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138. Azevedo MR, Araújo CLP, Reichert FF, Siqueira FV, da Silva MC, Hallal PC. Gender differences in leisure‐time physical activity. Int J Public Health. 2007;52(1):8‐15. 10.1007/s00038-006-5062-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139. Spencer RA, Rehman L, Kirk SFL. Understanding gender norms, nutrition, and physical activity in adolescent girls: a scoping review. Int J Behav Nutr Phys Act. 2015;12(6):1‐10. 10.1186/s12966-015-0166-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140. Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population‐based surveys with 1.9 million participants. Lancet Glob Health. 2018;6(10):e1077‐e1086. 10.1016/S2214-109X(18)30357-7 [DOI] [PubMed] [Google Scholar]
- 141. Wells JCK, Marphatia AA, Cole TJ, McCoy D. Associations of economic and gender inequality with global obesity prevalence: understanding the female excess. Soc Sci Med. 2012;75(3):482‐490. 10.1016/j.socscimed.2012.03.029 [DOI] [PubMed] [Google Scholar]
- 142. Popkin BM, Reardon T. Obesity and the food system transformation in Latin America. Obes Rev. 2018;19(8):1028‐1064. 10.1111/obr.12694 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143. Headey DD, Alderman HH. The relative caloric prices of healthy and unhealthy foods differ systematically across income levels and continents. J Nutr. 2019;149(11):2020‐2033. 10.1093/jn/nxz158 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144. Hirvonen K, Bai Y, Headey D, Masters WA. Affordability of the EAT–Lancet reference diet: a global analysis. Lancet Glob Health. 2020;8(1):e59‐e66. 10.1016/S2214-109X(19)30447-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145. Kandpal E, Baylis K. The social lives of married women: peer effects in female autonomy and investments in children (English). Policy Research Working Paper; No. WPS 8831. Washington D.C.; 2019.
- 146. Lewin S, Booth A, Glenton C, et al. Applying GRADE‐CERQual to qualitative evidence synthesis findings: Introduction to the series. Implement Sci. 2018;13(S1):2. 10.1186/s13012-017-0688-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147. De Brauw A, Van den Berg M, Brouwer ID, et al. Food System Innovations for Healthier Diets in Low and Middle‐Income Countries. Washington, DC: International Food Policy Research Institute (IFPRI; 2019. [Google Scholar]
- 148. Hawkes C, Ruel MT, Salm L, Sinclair B, Branca F. Double‐duty actions: seizing programme and policy opportunities to address malnutrition in all its forms. Lancet. 2020;395(10218):142‐155. 10.1016/S0140-6736(19)32506-1 [DOI] [PubMed] [Google Scholar]
- 149. Micha R, Karageorgou D, Bakogianni I, et al. Effectiveness of school food environment policies on children's dietary behaviors: a systematic review and meta‐analysis. PLoS One. 2018;13(3):e0194555. 10.1371/journal.pone.0194555 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150. Heath GW, Parra DC, Sarmiento OL, et al. Evidence‐based intervention in physical activity: lessons from around the world. Lancet (London, England). 2012;380(9838):272‐281. 10.1016/S0140-6736(12)60816-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151. L'Abbe M, Schermel A, Minaker L, et al. Monitoring foods and beverages provided and sold in public sector settings. Obes Rev. 2013;14(Suppl 1):96‐107. 10.1111/obr.12079 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1 Supporting Information