

Abstract
Introduction.
Healing of tendon injuries is often plagued by significant scar formation and compromised biomechanical function. For those with diabetes, these injuries are further complicated by alterations to the extracellular matrix of the tendon, poor circulation, and delayed wound healing; consequently, complications and re-rupture rates for patients with diabetes are reported higher than the typical patient population. Placental derived membranes, specifically dehydrated human amnion/chorion membranes (dACMs), have been utilized clinically as an adhesion barrier, and these membranes have been shown to reduce scarring and aid in tissue repair.
Objective.
The purpose of this study was to evaluate the effect of dACMs on tendon repair in a diabetic model with impaired healing.
Materials and Methods.
Using a type II diabetic model (BBZDR/WOR rats), a full-thickness injury was made through the Achilles tendon and repaired using a modified Kessler method. Repaired tendons were wrapped with dACM or left unwrapped as a control (n = 15/group; n = 30 total). Tendons were retrieved at 14 (n = 5/group; n = 10 total) or 28 days (n = 10/group; n = 20 total) and evaluated using histology, immunofluorescence, and biomechanical testing.
Results.
Treatment of tendons with dACM resulted in reduced failure rates, increased cell migration, and improved mechanical properties (compared with unwrapped controls). The dACM-treated tendons also showed changes in the production of several important biomarkers to tendon healing at both 14 and 28 days; most notably, Scleraxis was found to be upregulated in dACM-treated tendons.
Conclusions.
This study highlights a promising treatment option for this challenging clinical population.
Keywords: dehydrated human amnion/chorion membrane, dACM, tendon ruptures, diabetic tendon healing, placental tissues, regenerative healing, animal study
Achilles tendon ruptures occur in about 18 per 100 000 people,1 with the incidence of acute Achilles tendon ruptures increasing.2 Rupture of Achilles tendons results in significant patient morbidity and prolonged healing times. Although some acute ruptures can be managed with either surgical or nonsurgical approaches, certain populations with comorbidities are at a higher risk of rupture/injury and significantly worse outcomes. The incidence rate ratio for tendon rupture for patients with diabetes mellitus (DM) compared with otherwise healthy patients has been reported as high as 1.84.3 Specifically, the rate of Achilles tendon rupture for individuals with type 2 diabetes mellitus (T2DM) is significantly higher than the rate for those without diabetes.3 In addition, T2DM has been associated with increased incidence of wound infection and poor healing of tendon tissue following surgical repair.3–5
Increased risk of tendon rupture with DM is largely due to structural changes of the tendon caused by hyperglycemia. These changes are the result of increased collagen crosslinking caused by advanced glycation end-products (AGEs),6 which is accelerated by hyperglycemia.7 The AGEs often result in structural changes to the tendon; for example, individuals with DM have abnormal tendon structures, including increased size and other changes characteristic of tendinopathy.8 In addition to structural changes, several animal models have shown diabetic tendons have reduced biomechanical properties, specifically peak load and stiffness.9
Under normal conditions, tendon healing is a complex but organized process that can be divided into 3 overlapping stages of healing: inflammation, repair, and remodeling. The inflammation phase occurs immediately following an injury and lasts for a few days. During this period, the surrounding tissue and fluid release growth factors, such as platelet-derived growth factor (PDGF), transforming growth factor β (TGFβ), insulin-like growth factors 1 and 2 (IGF-1, IGF-2), and basic fibroblast growth factor (bFGF). This release of factors results in an invasion of inflammatory cells (ie, neutrophils and macrophages) that serve to remove cellular debris from the injury site.10 After a few days, the repair process begins and lasts for about 4 to 6 weeks. In the repair phase, there is a marked increase in tenocyte proliferation as well as the development of a preliminary extracellular matrix (ECM).11 The ECM is initially comprised of collagen III, but as the repair process progresses, type I collagen becomes dominant. Also at this time, angiogenic growth factors promote blood vessel formation at the repair site.11 Finally, the remodeling phase, which consists of 2 subphases (consolidation and maturation), takes over. In the consolidation phase, the newly generated tissue converts from a cellular to a more fibrous structure and the fibers begin to align in the direction of applied mechanical stress.12 In the maturation phase, there is a decline in tendon vascularity and a drop in cell metabolism along with slow remodeling of the fibrous tissue.12 At the end of the normal healing process (which may be > 1 year), repaired tendons contain scar tissue, resulting in an overall weaker tendon that is more susceptible to injury.11
Compromised healing of patients with DM is a result of significant alterations to each phase of tendon healing. During the inflammatory phase (compared with otherwise healthy patients), animal studies have shown there is a marked decrease in the levels of several important growth factors, including IGF-1, vascular endothelial growth factor, and nerve growth factor.13,14 Additionally, in a diabetic rat tendon model, DM resulted in a decrease in inflammatory cell proliferation and angiogenesis at the site of tendon injury.15 Clinically, matrix metalloproteinases (MMPs) have been shown to be overexpressed in subjects with DM, resulting in a compromised ECM.16–19 During the repair phase of diabetic tendon healing, production of collagen I, collagen III, and glycosaminoglycans are decreased.20,21 Changes to the levels of growth factors, reduced cellular proliferation, decreased angiogenesis, and a compromised ECM are some of the contributing factors resulting in compromised tendon healing in patients with diabetes.
Human amniotic allografts are a potential method for improving healing in diabetic tendons.22–25 Placental tissue has been used extensively in patients for wound repair26 and more recently has been utilized in cases of tendon injury and repair.27,28 Animal studies utilizing amnion-derived cells and tissues to augment tendon repair have shown a reduction in healing time and overall improvements in tendon structure.25,29 Initial clinical evidence has indicated that patients with tendon-pathologies treated with placental-derived grafts report reduced pain and improved function.30–32 Human amniotic tissues are rich in many of the components critical for tendon repair, including growth factors and ECM.33,34
The purpose of this study was to evaluate the use of dehydrated human amnion/chorion membranes (dACMs) for the treatment of Achilles tendon ruptures in a diabetic rat model.
MATERIALS AND METHODS
The authors hypothesized that the use of dACM as a tendon wrap would result in the upregulation of factors important for tendon repair and healing and the repaired tendon would have improved mechanical properties. For this study, a BBZDR/WOR rat model (an obese, insulin-dependent T2DM animal model that carries the Leprfa mutation) was used. In the BBZDR/WOR model T2DM occurs through hyperleptinemia and hyperinsulinemia.35 This model was used because it closely mimics many of the comorbidities seen in the T2DM human population, including hyperglycemia, insulin resistance, hypertension, obesity, neuropathy, and coronary artery disease.36,37
The protocol for this study was reviewed and approved by the UMASS Medical School Institutional Animal Care and Use Committee (Worcester, MA; protocol # A-2537–15).
Surgical procedure
BBZDR/WOR rats were provided by Biomere Biomedical Research Models (Worcester, MA) and aged at least 60 days to ensure the animal had committed to T2DM. Prior to the generation of the tendon injury, fasting blood glucose levels were taken; confirmation of diabetes was based on blood glucose levels of > 140 mg/dL following overnight fasting.
The BBZDR/WOR rats were divided randomly into 2 groups: tendon repair with dACM wrap (NuShield; Organogenesis Inc., Canton MA) or control (repair with no wrap). For each group (n = 15/group; n = 30 total), animals were euthanized with carbon dioxide asphyxiation and bilateral pneumothorax as a secondary confirmation at either 14 or 28 days, and the contralateral tendon served as a sham control. At 14 days, 5 animals per group were used for analysis of cell migration and hematoxylin and eosin (H&E) staining (n = 10 total). At 28 days, 10 animals per group were used (n = 20 total) with 5 animals per group used for cell migration and H&E staining, and 5 per group for mechanical testing.
Specifically, animals were anesthetized via inhalation of isoflurane, and both hind limbs where shaved and swabbed with betadine and 70% ethanol 3 times. A 1-cm longitudinal midline posterior incision was made to expose the Achilles tendon and the fascia surrounding the Achilles tendon was exposed. Upon exposure, surrounding fascia was dissected away (all groups), and the sham group was immediately closed. For the control and dACM-treated groups, a complete tendon tear was generated with a scalpel through the central region of the Achilles tendon. The Achilles tendon then was immediately repaired using the modified Kessler method with 6/0 polypropylene sutures. The dACM-treated tendons were wrapped with a section of dACM measuring 0.5 cm × 0.5 cm around the injured portion of the tendon with the stromal side of the graft oriented in contact with the tendon (control tendons were left unwrapped). The incision then was closed with 5/0 nylon sutures (Ethicon, Bridgewater, NJ), and postoperatively animals were given analgesics and returned to normal cage activity.
Histology
At 14 and 28 days, both injured and contralateral tendons (n = 5/group) were retrieved and fixed overnight using 4% paraformaldehyde in phosphate-buffered saline (PBS; Thermo Fisher, Waltham, MA). The fixed tissue was imbedded in optimum cutting temperature (OCT) compound (Thermo Fisher) and sectioned using a microtome at a 10-μm depth. Sections were stained with H&E to assess overall tendon structure. Immunofluorescence staining also was conducted to detect selected biomarkers relevant to tendon healing (Table). All primary antibodies used were rabbit polyclonal antibodies (Abcam, Cambridge, UK). All stained sections were counterstained with 4’,6-diamidino-2-phenylindole (DAPI) for cell nuclei. Confocal images were taken at a 63x oil objective on a laser scanning confocal microscope (model TCS SP5 II; Leica, Wetzlar, Germany) with AOBS (Acousto-Optical Beam Splitter; Leica), spectrophotometric detection, and a 405-nm laser.
Table.
Summary of biomarkers evaluated with immunofluorescence for this study
| TARGET | ANTIBODY | CAT NO. |
|---|---|---|
| COX2 | Anti-COX2/Cyclooxygenase 2 antibody rabbit polyclonal | ab15191 |
| IL-1β | Anti-IL1 beta antibody rabbit polyclonal | ab9722 |
| IL-6 | Anti-IL6 antibody mouse monoclonal | ab9324 |
| MMP-2 | Anti-MMP2 antibody rabbit polyclonal | ab37150 |
| TGF-β1 | Anti-TGF beta antibody rabbit polyclonal | ab66043 |
| TIMP1 | Anti-TIMP1 antibody rabbit polyclonal | ab61224 |
| TNFα | Anti-TNF alpha antibody [TNF706 + P/T2] mouse monoclonal | ab199013 |
| Scx | Anti-SCXA antibody rabbit polyclonal | ab58655 |
COX2: Cyclooxygenase 2; IL: Interleukin; MMP: matrix metalloproteinase; TGF: transforming growth factor; TIMP: tissue inhibitor of metalloproteinases; TNF: tumor necrosis factor; Scx: Scleraxis
To quantify cellular density at the repair site, DAPI-stained sections were blinded and cell density was calculated using Image J (National Institutes of Health, Bethesda, MD), with the cell counter plugin as described by the University of Chicago Imaging Facility (Chicago, IL). Briefly, the DAPI RGB (red, green, and blue) images were converted to grey scale and the threshold was adjusted to highlight only DAPI-stained nuclei. The cell nuclei then were automatically counted using the analyze function with the preset configuration for circularity and particle size. After unblinding, the sum of cell nuclei for each image then was used to obtain the average number of cell nuclei per mm2 in control, dACM-treated, and sham tendons.
Statistical analysis was conducted using a one-way analysis of variance (separately for 14 and 28 days) with a post-hoc Tukey test where P < .05 was considered significant.
Mechanical testing
At 28 days, dACM-wrapped and control tendons (unwrapped) (n = 5/group) were harvested together with the calcaneal bone and parts of the gastrocnemius and soleus muscle complex and tested to failure without preconditioning using a mechanical testing system (model MTS Bionix 370; MTS Systems Corporation, Minneapolis, MN). Tensile testing was conducted at room temperature with any remaining sutures removed from the tendon prior to testing. Tendons were loaded into the MTS machine with an initial grip separation of 10 mm and subjected to a grip separation of 100 mm per minute and tested to failure. The maximum force (N), and tendon stiffness (N/mm) were calculated using the MTS testing machine software. For both maximum tensile load and stiffness measurements, statistical analysis was conducted using an un-paired t test comparing repaired tendon groups (dACM-wrapped and unwrapped), where P < .05 was considered significant.
RESULTS
By 28 days, noticeable differences were observed in the overall integrity of the repaired tendons in each group. Interestingly, 20% (3/15) of the control tendons re-ruptured compared with 0% of the dACM-treated tendons (Figure 1A). This difference in re-rupture rates is especially interesting because control re-rupture rates of 20% corresponds closely with what is seen clinically in diabetic tendon repair, suggesting clear clinical implications relating to dACM utilization to augment tendon repair. Biomechanical tensile testing of tendons showed increases in the maximum tensile load for dACM-treated tendons compared with controls (39.34 ± 17.74 N vs. 26.74 ± 16.48 N, respectively [Figure 1B]). Additionally, wrapping tendons with dACM resulted in a significant increase in stiffness compared with controls (31.67 ± 19.43 N/mm vs. 12.83 ± 6.87 N/mm, respectively [Figure 1C, P < .05]). To compare with uninjured tendons, a representative sham tendon was tested. These results showed that by 28 days there is a substantial deficit in the mechanical strength of the injured tendons compared with the sham controls (Figure 1D–1F), showing the diabetic repair process is overall impaired, which is consistent with prior findings.20
Figure 1.
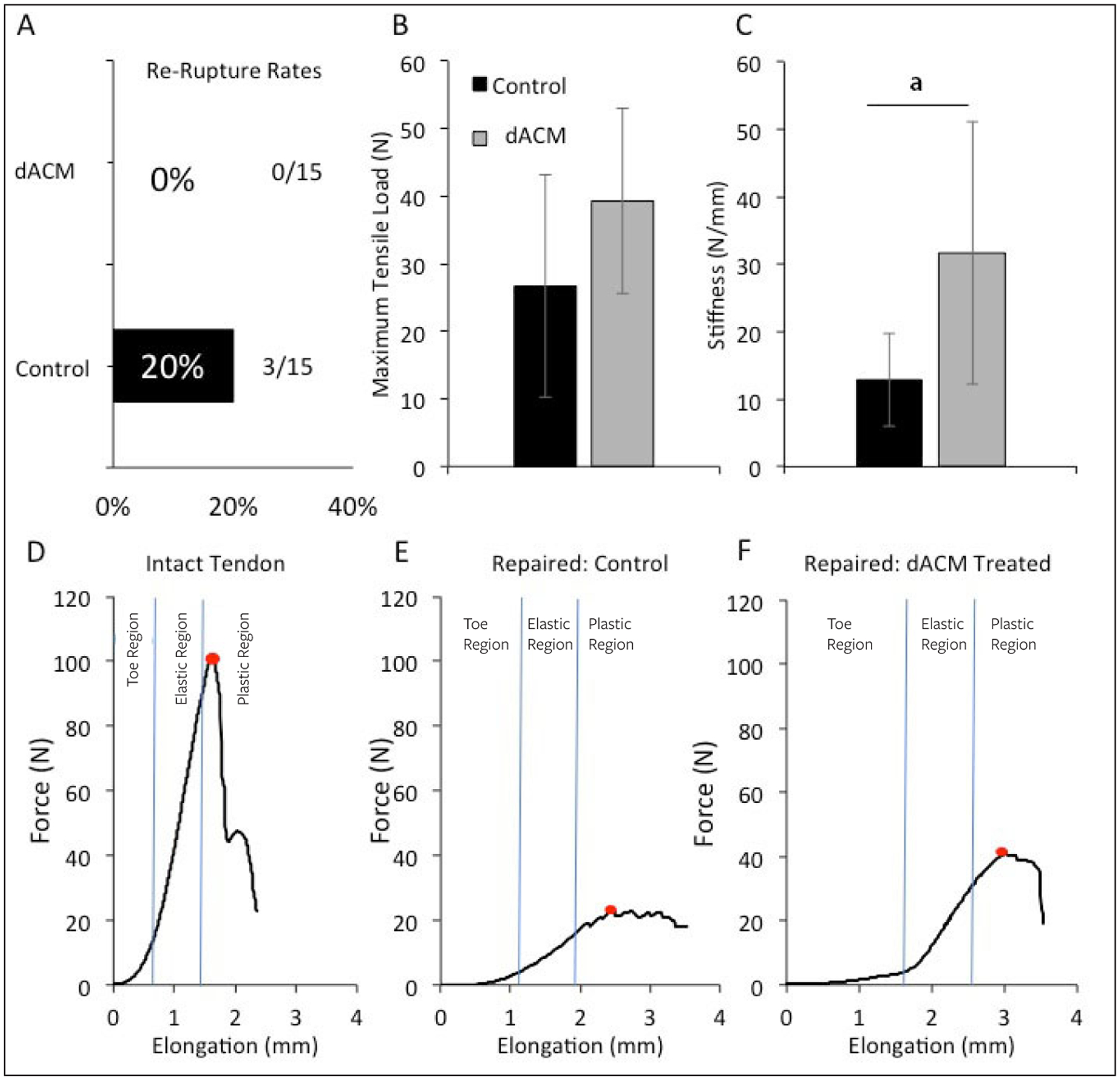
Biomechanical properties of repaired Achilles tendons at 28 days post injury. (A) By 28 days, control tendons had a 20% re-rupture rate (3/15), while no ruptures were observed with dACM-treated tendons; (B) maximum tensile load for both control and dACM-treated tendons retrieved 28 days post injury; (C) stiffness of control and dACM-treated tendons 28 days post injury. Representative force-displacement curves for (D) non-injured sham tendons (intact), (E) repaired control, and (F) repaired dACM-treated tendons at 28 days post injury. Red dot indicates the maximum failure load.
B and C: Averages are presented, and error bars represent standard deviation; N=5.
dACM: dehydrated amnion/chorion membrane
aP<.05
Retrieved tendons were evaluated for morphological changes based on H&Estained sections at 14 and 28 days (Figure 2). When compared with uninjured tendons (sham) at 14 and 28 days, the dACM and control groups were structurally inferior in terms of fiber structure and arrangement (Figure 2); however, dACM-treated tendons resulted in increased cell density and improvements in tendon fiber organization compared with unwrapped control tendons. Evaluation of DAPI-stained sections from retrieved tendons at 14 and 28 days found dACM-treated tendons resulted in significant increases in cell density compared with control and sham groups (Figure 3).
Figure 2.
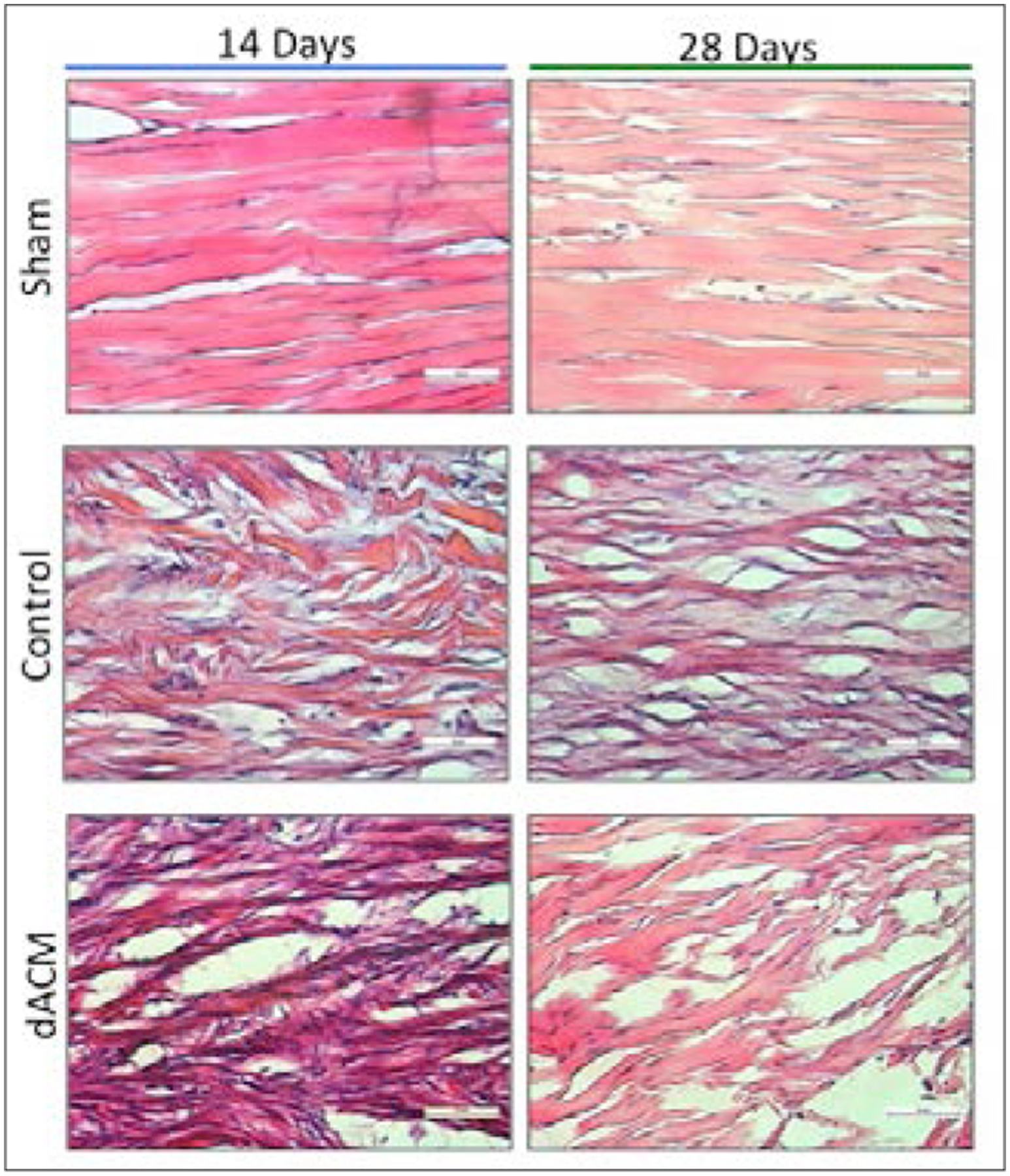
Representative hematoxylin and eosin stained images of retrieved tendons at 14 (left column) and 28 days (right column) following injury. Magnification, 40x objective. Scale bar 50μm.
dACM: dehydrated amnion/chorion membrane
Figure 3.
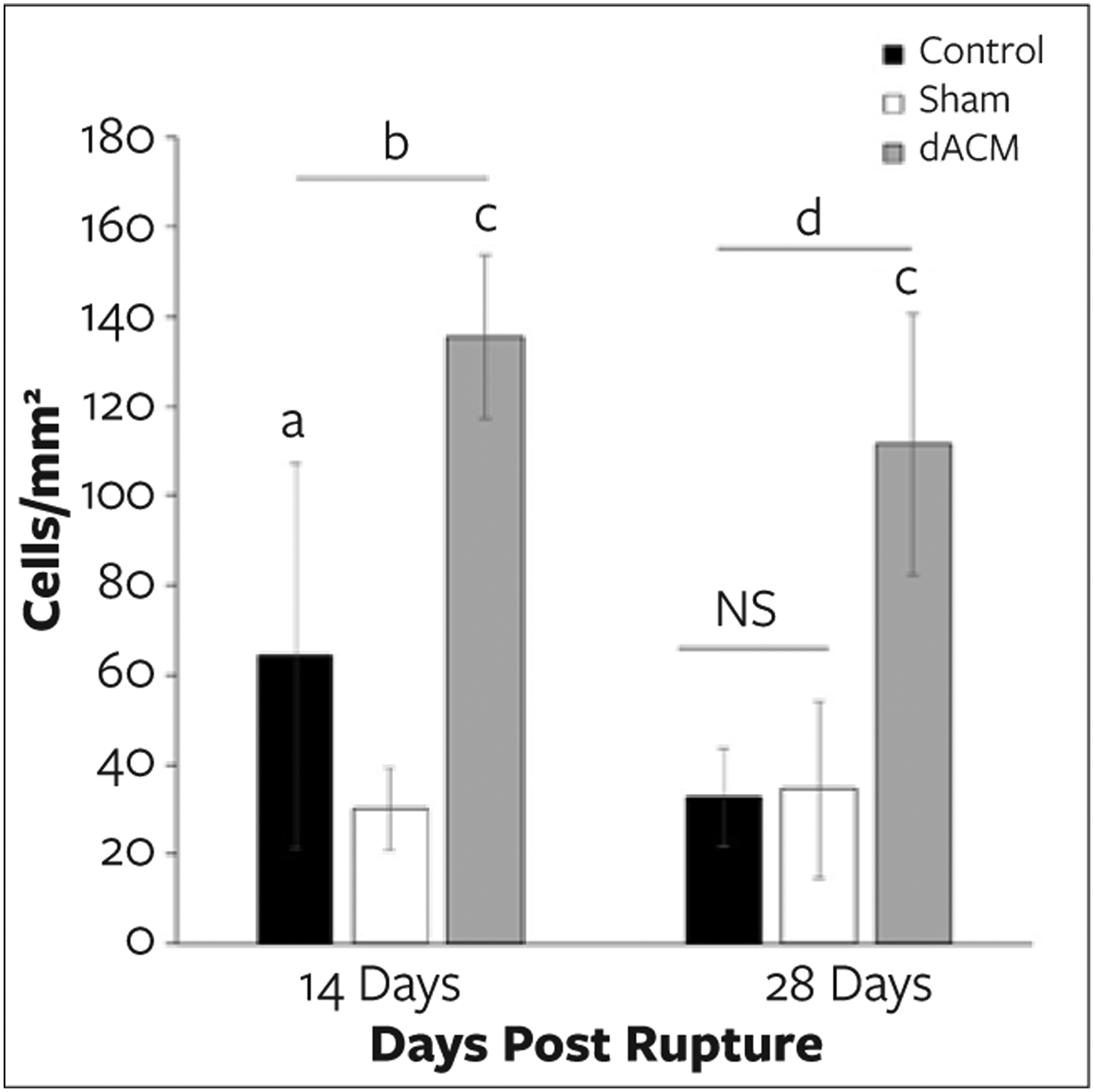
Cell density at the repair site at 14 and 28 days post injury. Cell density was measured using 4’,6-diamidino-2-phenylindole-stained sections. At 14 days, dehydrated amnion/chorion membrane (dACM)-treated tendons had a significantly higher cell density compared with both sham and control tendons. By 28 days there was no observable difference in the cell density between control and sham groups, while the dACM-treated group had a significantly higher cell density compared with both control and sham groups.
a P<.05 compared with sham group.
b P<.001 compared with control group.
c P<.0001 compared with sham group.
dP<.0001 compared with control group.
At 14 days, dACM-wrapped tendons had an average of 135.49 ± 18.36 cells/mm2, which was significantly higher than the sham (30.05 ± 9.29 cells/mm2, P < .0001) and control (64.13 ± 42.917 cells/mm2, P < .001) groups. By 28 days, the same trend was observed; dACM-wrapped tendons had an average of 111.38 ± 29.27 cells/mm2, which was significantly higher compared with the sham (34.45 ± 19.76, P < .0001) and control (32.75 ± 10.89, P < .0001) groups.
For normal tendons, the repair phase of tendon healing is marked by both rapid cell proliferation and an influx of cells to the site of injury, however diabetic tendons have been shown to have a reduced cell migration response.15 In this study, the authors observed only a small increase in the average number of cells present at 14 days in the unwrapped (control) tendon group, and no significant observed difference in the number of cells present at 28 days (compared with corresponding sham controls), this may be due to a reduced migratory response.
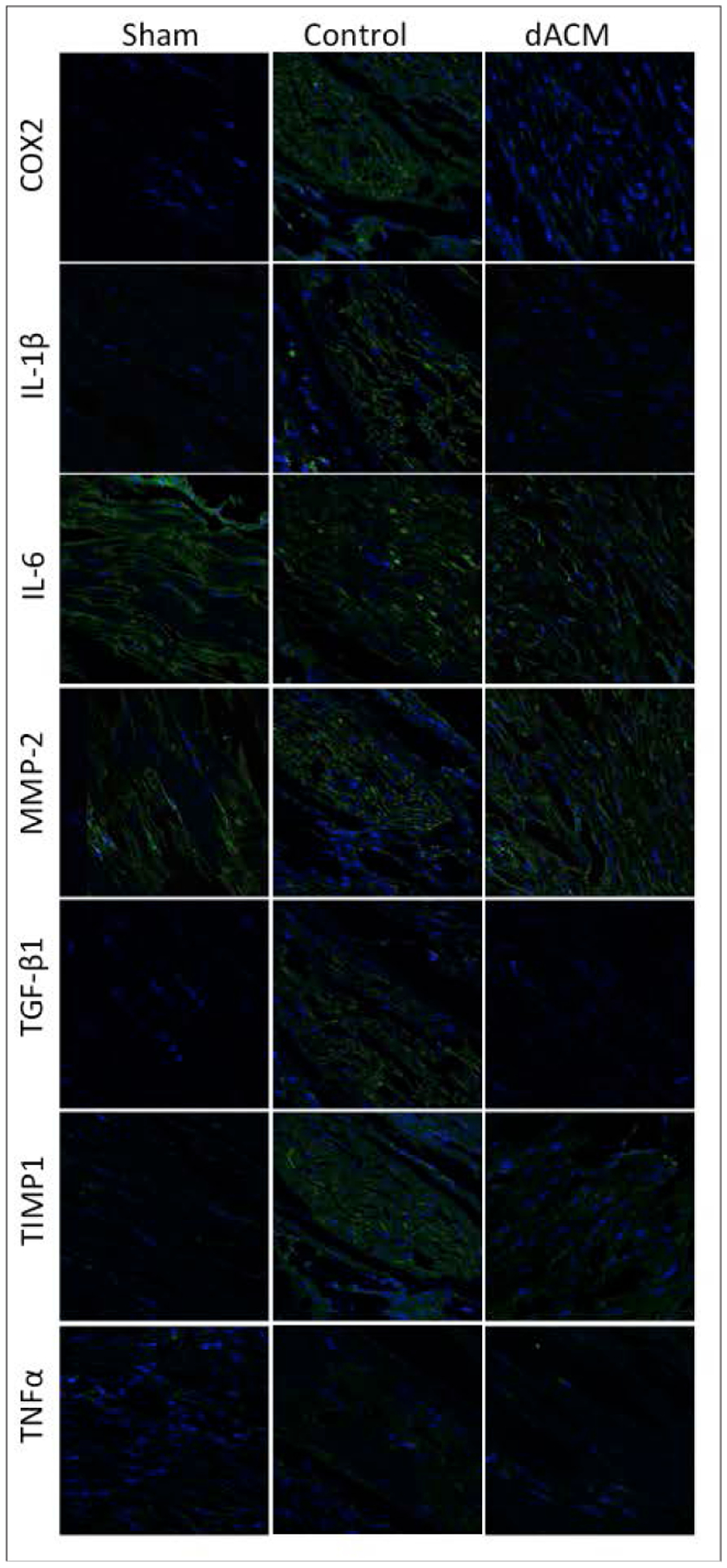
Immunofluorescent analysis of retrieved tendons at 14 days (Figure 4) showed that compared with the sham group, unwrapped tendons (control) had increased levels of cyclooxygenase-2 (COX2), interleukin (IL) 1β, IL-6, MMP-2, TGF-β1, and tissue inhibitor of metalloproteinases (TIMP) 1. When comparing dACM-treated tendons with control tendons at 14 days, IL-6 and MMP-2 levels were reduced in the dACM groups while TGF-β1 and TIMP1 were elevated in dACM-treated tendons.
Figure 4.
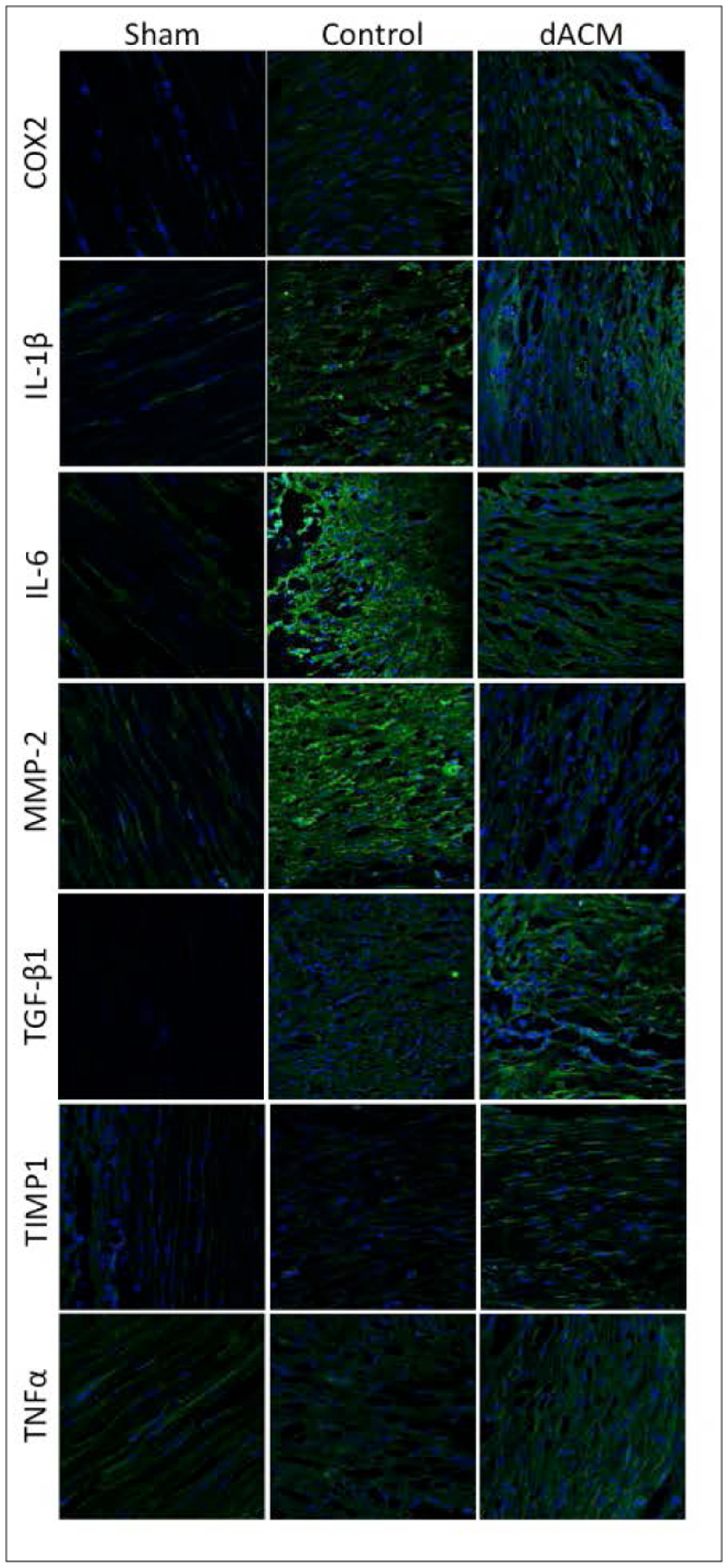
Immunofluorescent (IMF) staining of Achilles tendons at 14 days post injury. Biomarkers (green) expressed at 14 days post injury were assessed using IMF for sham tendons (left column), control/unwrapped tendons (center column), and dACM-treated tendons (right column). Magnification, 63x oil immersion objective. dACM: dehydrated human amnion/chorion membrane; COX2: cyclooxygenase-2; IL: Interleukin; MMP: matrix metalloproteinase; TGF: transforming growth factor; TIMP: tissue inhibitor of metalloproteinases; TNF: tumor necrosis factor
At 28 days (Figure 5), compared with the sham group, unwrapped tendons (control) still had slightly increased levels of COX2, IL-1β, TGF-β1, and TIMP1. When comparing dACM-treated tendons to unwrapped tendons (control) at 28 days, COX2, IL-1β, TGF-β1, and TIMP1 levels were lower in the dACM-treated groups. Interestingly, scleraxis (Scx), a transcription factor known to be critical for certain aspects of tenogenesis and repair, was consistently increased in dACM groups at both 14 and 28 days compared with both unwrapped control and sham groups (Figure 6). Scleraxis has been linked to expression of other important factors including collagen I and tenomodulin. Upregulation of this transcription factor (Scx) suggests overall activation and promotion of tendon repair processes in the dACM-wrapped tendon group.
Figure 5.
Immunofluorescent (IMF) staining of Achilles tendons at 28 days post injury. Biomarkers (green) expressed at 28 days post injury were assessed using IMF for sham tendons (left column), control/unwrapped tendons (center column), and dehydrated amnion/chorion membrane-treated tendons (right column). Magnification, 63x oil immersion objective. dACM: dehydrated human amnion/chorion membrane; COX2: cyclooxygenase-2; IL: Interleukin; MMP: matrix metalloproteinase; TGF: transforming growth factor; TIMP: tissue inhibitor of metalloproteinases; TNF: tumor necrosis factor
Figure 6.
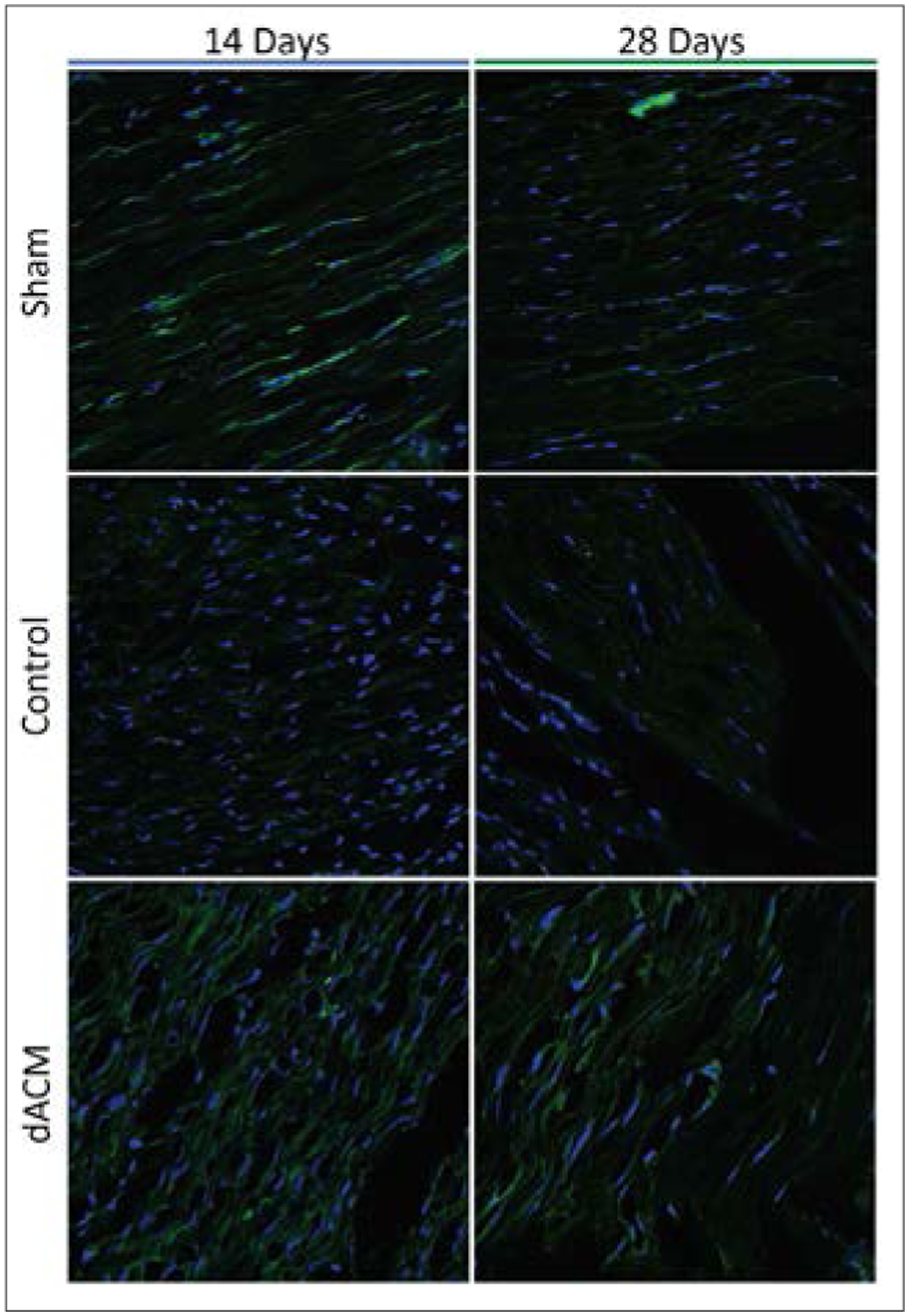
Immuno fluorescence of Scleraxis (Scx), a transcription factor involved in tendon repair at 14 days (left) and 28 days (right). Dehydrated amnion/chorion membrane (dACM)-treated tendons resulted in upregulation of Scx in tendons at days 14 and 28. In contrast, there is limited staining for Scx in the unwrapped and sham controls. Magnification, 63x oil immersion objective.
DISCUSSION
Diabetes mellitus increases the risk of tendon injury and inhibits the ability of tendons to heal normally.4,9 Previous studies have shown injured diabetic tendons have a poor recovery of their biomechanical properties,20 a drop in cell migration to the site of injury,15 and a reduction in biomarkers necessary for tendon repair.13 In this study, the authors observed that injured diabetic tendons showed a significant delay in healing as determined by reduced biomechanical properties at 28 days post injury, reduced cell density at the site of injury, and an inadequate proliferative healing phase as determined by the delay in the expression of biomarkers such as COX2, IL-1β, IL-6, TGF-β1, and TIMP1, which is consistent with the aforementioned studies.
Human amniotic allografts have been shown to improve tendon repair in both preclinical and early clinical reports.25,27–29 The results of this study are consistent with previous findings where tendons treated with amniotic tissues showed improvements in biomechanical properties.24,29 This study is novel in that it is the the first to evaluate the effect of an amniotic allograft in a delayed diabetic model of tendon healing; and also the first study to evaluate dACM grafts as an adjunct for Achilles tendon repair. Placental-derived grafts have been reported to contain numerous growth factors and cytokines thought to support tendon healing, including PDGF-BB, IGF-1, TGF-β1, and bFGF.38 Placental tissues also have been shown to promote cell proliferation and migration in a variety of cell types and promote angiogenesis39; these results along with other published work suggest a clinical benefit of dACM for augmenting tendon repair beyond the accepted adhesion barrier function.
The changes in biomarker expression between dACM-treated and unwrapped tendons observed in this study suggest one mechanism for increased mechanical integrity with dACM-wrapped tendons may be related to the faster progression out of the inflammatory and into the repair phase of tendon healing. Of particular interest is Scx, which was increased in dACM-treated tendons at both 14 and 28 days compared with controls. Scleraxis is a basic helix-loop-helix transcription factor that is critical for certain aspects of tenogenesis and repair, and it is expressed in both tendon and ligament progenitor cell populations.40 Scleraxis is linked with ECM development, including the expression of Col1α1 and Tenomodulin in tenocytes.23,41 The deletion of the Scx gene has been shown to lead to severely mechanically compromised tendons.42 Following tendon injury, Scx is known to be upregulated.43 It plays a role in tenogenic differentiation of mesenchymal stem cells,44 and transducing tendon progenitor cells with Scx has been shown to result in improved tendon repair.42 Interestingly, Scx expression has been reported to be upregulated in response to fibroblast growth factor 2 and TGF-β1,45,46 both of which are present in placental-derived tissues.38 Future work will focus on evaluating the interplay of placental membranes and cells important for tendon healing to further elucidate potential mechanisms of action.
LIMITATIONS
One limitation of this study, common to animal studies, is the number of animals and time points evaluated. Ethical standards call for utilization of animals judiciously; however, healing is a continuous course and evaluation at a few time points leads to snapshots of the process, potentially limiting complete understanding of the progression of repair. Other limitations for this study include the evaluation of tendon healing in an animal model. While the BBZDR/WOR rat model has been widely published and validated as a T2DM model with corresponding comorbidities, these results should still be validated and studied in a human clinical study.
CONCLUSIONS
Injuries to the Achilles tendon require significant recovery time in otherwise healthy individuals. Diabetes mellitus increases the overall risk of ruptures and complications following tendon repair and results in delayed or inhibited tendon healing. This study demonstrates a potential strategy to overcome some of these difficulties, where dACM-wrapped tendons resulted in reduced failures, improved mechanical integrity, and greater cell migration to the site of injury in a T2DM animal model. Biomarker analysis also indicated that treating injured tendons with dACM reduced the time to repair; however, by 28 days both dACM-wrapped and unwrapped (control) tendon groups were inferior to the noninjured group (sham), illustrating the effects DM has on delaying tendon healing.
ACKNOWLEDGMENTS
The authors thank the Core Facilities at UMASS Medical School (Worcester, MA) that performed the animal husbandry, tissue sectioning, immunostaining, and biomechanical testing. Specifically, they would like to thank Animal Medicine and the Orthopedics and Physical Rehabilitation facilities.
Footnotes
Disclosure: Dr. John McQuilling and Dr. Katie Mowry are paid employees of Organogenesis Inc. There is no conflict of interest for Mitchell Sanders, Lindsay Poland, Mia Sanders, Giacomo Basadonna, and Norman E. Waldrop. This research was funded by Organogenesis Inc to AliraHealth and the animal studies were performed at UMASS Medical School.
REFERENCES
- 1.Raikin SM, Garras DN, Krapchev PV. Achilles tendon injuries in a United States population [published online February 5, 2013]. Foot Ankle Int. 2013;34(4):475–480. [DOI] [PubMed] [Google Scholar]
- 2.Ganestam A, Kallemose T, Troelsen A, Barfod KW. Increasing incidence of acute Achilles tendon rupture and a noticeable decline in surgical treatment from 1994 to 2013. A nationwide registry study of 33,160 patients [published online February 20, 2015]. Knee Surg Sports Traumatol Arthrosc. 2016;24(12):3730–3737. [DOI] [PubMed] [Google Scholar]
- 3.Zakaria MH, Davis WA, Davis TM. Incidence and predictors of hospitalization for tendon rupture in type 2 diabetes: the Fremantle diabetes study [published online November 16, 2013]. Diabet Med. 2014;31(4):425–430. [DOI] [PubMed] [Google Scholar]
- 4.Wolfson TS, Hamula MJ, Jazrawi LM. Impact of diabetes mellitus on surgical outcomes in sports medicine. Phys Sportsmed. 2013;41(4):64–77. [DOI] [PubMed] [Google Scholar]
- 5.Wukich DK, McMillen RL, Lowery NJ, Frykberg RG. Surgical site infections after foot and ankle surgery: a comparison of patients with and without diabetes [published online August 4, 2011]. Diabetes Care. 2011;34(10):2211–2213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Reddy GK. 2004. Cross-linking in collagen by nonenzymatic glycation increases the matrix stiffness in rabbit Achilles tendon. Exp Diabesity Res. 2004;5(2):143–153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Snedeker JG, Gautieri A. The role of collagen crosslinks in ageing and diabetes - the good, the bad, and the ugly. Muscles Ligaments Tendons J. 2014;4(3):303–308. [PMC free article] [PubMed] [Google Scholar]
- 8.de Oliveira RR, Lemos A, de Castro Silveira PV, de Silva RJ, de Moraes SR. Alterations of tendons in patients with diabetes mellitus: a systematic review. Diabet Med. 2011;28(8):886–895. [DOI] [PubMed] [Google Scholar]
- 9.Fox AJS, Bedi A, Deng X-H, et al. Diabetes mellitus alters the mechanical properties of the native tendon in an experimental rat model [published online January 18, 2011]. J Orthop Res. 2011;29(6):880–885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Molloy T, Wang Y, Murrell G. The roles of growth factors in tendon and ligament healing. Sports Med. 2003;33(5):381–394. [DOI] [PubMed] [Google Scholar]
- 11.Voleti PB, Buckley MR, Soslowsky LJ. Tendon healing: repair and regeneration. Annu Rev Biomed Eng. 2012;14(1):47–71. [DOI] [PubMed] [Google Scholar]
- 12.Sharma P, Maffulli N. Biology of tendon injury: healing, modeling and remodeling. J Musculoskelet Neuronal Interact. 2006;6(2):181–190. [PubMed] [Google Scholar]
- 13.Ahmed AS, Li J, Schizas N, et al. Expressional changes in growth and inflammatory mediators during Achilles tendon repair in diabetic rats: new insights into a possible basis for compromised healing [published online May 6, 2014]. Cell Tissue Res. 2014;357(1):109–117. [DOI] [PubMed] [Google Scholar]
- 14.Janssen JA, Jacobs ML, Derkx FH, Weber RF, van der Lely AJ, Lamberts SW. Free and total insulin-like growth factor I (IGF-I), IGF-binding protein-1 (IGFBP-1), and IGFBP-3 and their relationships to the presence of diabetic retinopathy and glomerular hyperfiltration in insulin-dependent diabetes mellitus. J Clin Endocrinol Metab. 1997;82(9):2809–2815. [DOI] [PubMed] [Google Scholar]
- 15.Chbinou N, Frenette J. Insulin-dependent diabetes impairs the inflammatory response and delays angiogenesis following Achilles tendon injury [published online January 8, 2004]. Am J Physiol Regul Integr Comp Physiol. 2004;286(5):R952–R957. [DOI] [PubMed] [Google Scholar]
- 16.Gharagozlian S, Svennevig K, Bangstad HJ, Winberg JO, Kolset SO. Matrix metalloproteinases in subjects with type 1 diabetes. BMC Clin Pathol. 2009;9:7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kadoglou NP, Daskalopoulou SS, Perrea D, Liapis CD. Matrix metalloproteinases and diabetic vascular complications. Angiology. 2005;56(2):173–189. [DOI] [PubMed] [Google Scholar]
- 18.Ryan ME, Ramamurthy NS, Sorsa T, Golub LM. 1999. MMP-mediated events in diabetes. Ann N Y Acad Sci. 1999;878:311–334. [DOI] [PubMed] [Google Scholar]
- 19.Tsai WC, Liang FC, Cheng JW, et al. 2013. High glucose concentration up-regulates the expression of matrix metalloproteinase-9 and -13 in tendon cells. BMC Musculoskelet Disord. 2013;14:255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ahmed AS, Schizas N, Li J, et al. Type 2 diabetes impairs tendon repair after injury in a rat model [published online October 4, 2012]. J Appl Physiol. 2012;113(11):1784–1791. [DOI] [PubMed] [Google Scholar]
- 21.Burner T, Gohr C, Mitton-Fitzgerald E, Rosenthal AK. Hyperglycemia reduces proteoglycan levels in tendons [published online August 14, 2012]. Connect Tissue Res. 2012;53(6):535–541. [DOI] [PubMed] [Google Scholar]
- 22.Ozbölük S, Ozkan Y, Oztürk A, Güi N, Ozdemir RM, Yanik K. The effects of human amniotic membrane and periosteal autograft on tendon healing: experimental study in rabbits [published online August 17, 2009]. J Hand Surg Eur Vol. 2010;35(4):262–268. [DOI] [PubMed] [Google Scholar]
- 23.Özgenel GY. 2004. The effects of a combination of hyaluronic and amniotic membrane on the formation of peritendinous adhesions after flexor tendon surgery in chickens. J Bone Joint Surg Br. 2004;86(2):301–307 [DOI] [PubMed] [Google Scholar]
- 24.Özgenel GY, Şamli B, Özcan M. Effects of human amniotic fluid on peritendinous adhesion formation and tendon healing after flexor tendon surgery in rabbits. J Hand Surg Am. 2001;26(2):332–339. [DOI] [PubMed] [Google Scholar]
- 25.Barboni B, Russo V, Curini V, et al. 2012. Achilles tendon regeneration can be improved by amniotic epithelial cell allotransplantation [published online April 10, 2012]. Cell Transplant. 2012;21(11):2377–2395. [DOI] [PubMed] [Google Scholar]
- 26.Stern M The grafting of preserved amniotic membrane to burned and ulcerated surfaces, substituting skin grafts. A preliminary report. JAMA. 1913;60(13):973–974. [Google Scholar]
- 27.Millar NL, Murrell GA, McInnes IB. Inflammatory mechanisms in tendinopathy – towards translation. Nat Rev Rheumatol. 2017;13(2):110–122. [DOI] [PubMed] [Google Scholar]
- 28.McIntyre JA, Jones IA, Danilkovich A, Vangsness CT. 2017. The Placenta: Applications in Orthopaedic Sports Medicine [published online April 4, 2017]. Am J Sports Med. 2018;46(1):234–247. [DOI] [PubMed] [Google Scholar]
- 29.Nicodemo M de C, das Nevesii LR, Aguiar J, et al. Amniotic membrane as an option for treatment of acute Achilles tendon\ninjury in rats. Acta Cir Bras. 2017;32(2):125–139. [DOI] [PubMed] [Google Scholar]
- 30.Lullove E A flowable placental tissue matrix allograft in lower extremity injuries: a pilot study. Cureus. 2015;7(6):e275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Warner M, Lasyone L. An open-label, single-center, retrospective study of cryopreserved amniotic membrane and umbilical cord tissue as an adjunct for foot and ankle surgery. Surg Technol Int. 2014;25:251–255. [PubMed] [Google Scholar]
- 32.Werber B 2015. Amniotic tissues for the treatment of chronic plantar fasciosis and Achilles tendinosis [published online September 27, 2015]. J Sport Med. 2015:219896. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hanselman AE, Lalli TAJ, Santrock RD. Topical review: use of fetal tissue in foot and ankle surgery [published online March 26, 2015]. Foot Ankle Spec. 2015;8(4):297–304 [DOI] [PubMed] [Google Scholar]
- 34.Riboh JC, Saltzman BM, Yanke AB, Cole BJ. Human amniotic membrane-derived products in sports medicine: basic science, early results, and potential clinical applications [published online November 19, 2015]. Am J Sports Med. 2016;44(9):2425–2434. [DOI] [PubMed] [Google Scholar]
- 35.Tirabassi RS, Flanagan JF, Wu T, Kislauskis EH, Birckbichler PJ, Guberski DL. The BBZDR/Wor rat model for investigating the complications of type 2 diabetes mellitus. ILAR J. 2004;45(3):292–302. [DOI] [PubMed] [Google Scholar]
- 36.de Oliveira RR, de Lira KD, Silveira PV, et al. Mechanical properties of achilles tendon in rats induced to experimental diabetes [published online January 12, 2011]. Ann Biomed Eng. 2011;39(5):1528–1534. [DOI] [PubMed] [Google Scholar]
- 37.Sima AA, Zhang W, Xu G, Sugimoto K, Guberski D, Yorek MA. A comparison of diabetic polyneuropathy in type II diabetic BBZDR/Wor rats and in type I diabetic BB/Wor rats. Diabetologia. 2000;43(6):786–793. [DOI] [PubMed] [Google Scholar]
- 38.McQuilling JP, Vines JB, Kimmerling KA, Mowry KC. Proteomic comparison of amnion and chorion and evaluation of the effects of processing on placental membranes. Wounds. 2017;29(6):E38–E42. [PMC free article] [PubMed] [Google Scholar]
- 39.McQuilling JP, Vines JB, Mowry KC. 2017. In vitro assessment of a novel, hypothermically stored amniotic membrane for use in a chronic wound environment [published online March 29, 2017]. Int Wound J. 2017;14(6):993–1005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Schweitzer R, Chyung JH, Murtaugh LC, et al. Analysis of the tendon cell fate using Scleraxis, a specific marker for tendons and ligaments. Development. 2001;128(19):3855–3866. [DOI] [PubMed] [Google Scholar]
- 41.Shukunami C, Takimoto A, Oro M, Hiraki Y. Scleraxis positively regulates the expression of tenomodulin, a differentiation marker of tenocytes [published online June 27, 2006]. Dev Biol. 2006;298(1):234–47. [DOI] [PubMed] [Google Scholar]
- 42.Tan C, Lui PP, Lee YW, Wong YM. Scx-transduced tendon-derived stem cells (tdscs) promoted better tendon repair compared to mock-transduced cells in a rat patellar tendon window injury model. PLoS One. 2014;9(5):e97453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Nourissat G, Berenbaum F, Duprez D. Tendon injury: from biology to tendon repair [published online March 3, 2015]. Nat Rev Rheumatol. 2015;11(4):223–233. [DOI] [PubMed] [Google Scholar]
- 44.Alberton P, Popov C, Prägert M, et al. Conversion of human bone marrow-derived mesenchymal stem cells into tendon progenitor cells by ectopic expression of scleraxis [published online October 11, 2011]. Stem Cells Dev. 2012;21(6):846–858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Tokunaga T, Shukunami C, Okamoto N, et al. FGF-2 stimulates the growth of tenogenic progenitor cells to facilitate the generation of tenomodulin-positive tenocytes in a rat rotator cuff healing model [published online August 26, 2015]. Am J Sports Med. 2015;43(10):2411–2422. [DOI] [PubMed] [Google Scholar]
- 46.Arimura H, Shukunami C, Tokunaga T, et al. TGF-β1 Improves biomechanical strength by extracellular matrix accumulation without increasing the number of tenogenic lineage cells in a rat rotator cuff repair model [published online June 6, 2017]. Am J Sports Med. 2017;45(10):2394–2404. [DOI] [PubMed] [Google Scholar]