

Abstract
This study aimed to propose an operational definition of late-onset hypogonadism (LOH) that incorporates both clinical symptoms and serum testosterone measurements to evaluate the prevalence of LOH in aging males in China. A population-based sample of 6296 men aged 40 years–79 years old was enrolled from six representative provinces in China. Serum total testosterone (TT), sex hormone-binding globulin (SHBG), and luteinizing hormone (LH) were measured and free testosterone (cFT) was calculated. The Aging Males' Symptoms (AMS) scale was used to evaluate the LOH symptoms. Finally, 5078 men were included in this analysis. The TT levels did not decrease with age (P = 0.59), and had no relationship with AMS symptoms (P = 0.87 for AMS total score, P = 0.74 for ≥ 3 sexual symptoms). The cFT levels decreased significantly with age (P < 0.01) and showed a negative association with the presence of ≥ 3 sexual symptoms (P = 0.03). The overall estimated prevalence of LOH was 7.8% (395/5078) if a cFT level <210 pmol l−1 combined with the presence of ≥ 3 sexual symptoms was used as the criterion of LOH. Among them, 26.1% (103/395) and 73.9% (292/395) had primary and secondary hypogonadism, respectively. After adjustment for confounding factors, primary and secondary hypogonadism was positively related to age and comorbidities. Body mass index was an independent risk factor for secondary hypogonadism. The results suggest that the AMS total score is not an appropriate indicator for decreased testosterone, and that the cFT level is more reliable than TT for LOH diagnosis. Secondary hypogonadism is the most common form of LOH.
Keywords: Aging Males' Symptoms, calculated free testosterone, late-onset hypogonadism, middle-aged and elderly male, total testosterone
INTRODUCTION
The aging population among Chinese adults has increased substantially over the past two decades, concurrent with an increase in age-related disease. Late-onset hypogonadism (LOH) is a clinical and biochemical syndrome associated with advancing age that is characterized by symptoms and a deficiency in serum testosterone levels (below the young healthy adult male reference range).1 This condition may result in a significant reduction in quality of life and may adversely affect the function of multiple organ systems.2 Although the clinical significance of LOH in adult men is becoming increasingly recognized, its prevalence in the general population is underexplored. A large number of men with LOH remain undiagnosed and untreated in China.3
The lack of a universally accepted definition for LOH makes estimating its prevalence a major challenge.4 While all guidelines agree that a combination of symptoms of testosterone deficiency and decreased serum testosterone levels are required for the diagnosis of LOH, no agreement on the threshold levels signifying low testosterone has been reached.2,5 In addition, the array of symptoms associated with LOH is wide, covering many, often nonspecific, findings associated with aging, such as sexual dysfunction; decreased bone mass, muscular mass, and strength; increased body fat; decreased vitality; and depressed mood.1,2,6 There is substantial overlap between symptoms arising from chronic diseases and hypogonadism (HG), posing a significant challenge to determining clinically relevant LOH.7 Moreover, hypogonadal symptoms tend to be specific to the individual, with not all men experiencing symptoms despite having low testosterone levels.8 The key question is what, if any, of the wide array of LOH-related symptoms show correlation with decreased serum concentrations of total testosterone (TT) or free testosterone (FT) levels.1,6
In addition, according to the etiology of testosterone deficiency, male HG is traditionally classified into primary (or hypergonadotropic HG) and secondary (or hypogonadotropic HG).9 LOH cannot be classified into only one of the HG categories described above. This complex disorder is associated with both primary and secondary HG and results in low testosterone levels and variable gonadotrophin levels.9 Primary HG was reported to be associated predominately with age, and secondary HG was reported to be associated with obesity and metabolic diseases.9,10 Classification of LOH into different categories by combining luteinizing hormone (LH) with testosterone may improve the diagnosis and management of LOH.
A number of epidemiological studies have reported the prevalence of LOH with the use of independently formulated diagnostic criteria for LOH. The European Male Ageing Study (EMAS) proposed a strict definition for LOH as the presence of three sexual symptoms (lessened sexual thoughts, weakened morning erections, and erectile dysfunction) combined with a serum TT level lower than 8 nmol l −1, or a serum TT level of 8 nmol l −1–11 nmol l −1 and a FT level <220 pmol l −1. With these criteria, LOH diagnosis was confirmed in only 2.1% of the participants.11 In a community-based study composed of 944 men aged 40 years–79 years from nine urban communities in China, the prevalence of LOH was 9.1% based on the criteria of the presence of three sexual symptoms (decreased ability/frequency of sexual activity, decreased number of morning erections, and decreased libido) with TT levels <13.21 nmol l −1 and calculated free testosterone (cFT) levels <268.89 pmol l −1.12 According to the criterion of both TT level <10.4 nmol l −1 and FT level <170 pmol l −1 and positive clinical symptoms on the Androgen Deficiency in the Aging Male (ADAM) questionnaire, the prevalence of androgen deficiency was 12.0% among 819 men over 40 years old in Kaohsiung, Taiwan, China.13 Using more relaxed diagnostic criteria, such as a serum TT level of <12.15 nmol l −1 with a positive response to the ADAM questionnaire, the prevalence of LOH has been found to be 25.6% in 534 men aged 40 years–79 years in Korea.14 However, many of the results cannot be used to accurately evaluate the current prevalence of LOH in China because there are ethnic differences in testosterone levels;11,14 the studies had strong selection bias because of single center recruitment;13,14 or they were based on small numbers of participants.12,13,14 Moreover, all the above studies did not classify LOH into primary or secondary except for EMAS.10
Therefore, in this study, using a large, national sample of Chinese men aged 40 years–79 years, we first investigated TT, sex hormone-binding globulin (SHBG), LH, and determined cFT using the Vermeulen formula in males. Moreover, we used the Aging Males' Symptoms (AMS) questionnaire to investigate the subjective symptoms of LOH in elderly males. Then, we explored the relationship between clinical symptoms and biochemical results to verify whether the indicators mentioned above can be used to diagnose LOH in clinical practice. Last, we proposed an operational definition of LOH that incorporates both clinical symptoms plus serum TT and cFT measurements to evaluate the prevalence of LOH in aging males in China and identify unique clinical characteristics and risk factors for primary and secondary HG.
PARTICIPANTS AND METHODS
Study design and population samples
The data were obtained from the Reproductive Health Assessment and Key Technology Research Project from 2012 to 2016, which is a nationally representative study that examines the reproductive health status and influencing factors in different age groups in China. The study protocol and informed consent forms were approved by the Ethics Committee Review Board of Tongji Medical College, Huazhong University of Science and Technology (2013S073). Written informed consent was obtained from each participant.
The multiple-center cross-sectional survey was conducted from June 1, 2013, to March 28, 2014. According to the geographical characteristics and population density in mainland China, six representative provinces were selected for this study: Hebei (northern China), Jiangsu (eastern China), Guangdong (southern China), Hubei (central China), Shaanxi (northwest China), and Guizhou (southwest China). Five communities or villages from each of the six provinces were randomly chosen for subject recruitment. All men aged between 40 years and 79 years from the selected 30 districts were invited to undergo a health assessment involving a questionnaire and blood tests for hormone measurements.
Of the 6296 subjects recruited, 1218 were excluded because of incomplete responses to questionnaires, known diseases of the hypothalamus–pituitary–testis axis, current use of medications affecting the hormone levels, no kids, or previous vasectomy. Thus, 5078 subjects were eligible and enrolled in the final analysis. Of these, 933 came from northern China, 926 came from eastern China, 819 came from southern China, 706 came from central China, 886 came from northwest China, and 808 came from southwest China.
Data collection and measurements
Each eligible participant completed a questionnaire and clinical examination. The questionnaire consisted of questions on age, ethnicity, education level, occupation, marital status, behavior, history of disease, etc. The AMS scale 15 (present in Supplementary Table 1) was used to evaluate the presence or absence of symptoms that are thought to be related to LOH in aging males. The AMS scale contains 17 self-rating symptom-based questions ranging from the general feeling of well-being to the specific decrease in libido. Questions 1–5, 9 and 10 compose the physical subscale; questions 6–8, 11 and 13 compose mental subscale; and questions 12 and 14–17 compose sexual subscale. Each question is to be answered with a score from 1 to 5. The sum of all subscales is the total score. Total scores can range from a minimum of 17 to a maximum of 85. An AMS total score greater than or equal to 27 according to the findings of Heinemann et al.16 and Moore et al.17 is considered positive. For a single question, scores of 1–2 are regarded as negative, and scores of 3–5 are considered positive.
Supplementary Table 1.
Aging Males’ Symptoms Questionnaire
| Which of the following symptoms apply to you at this time? Please, mark the appropriate box for each symptom. For symptoms that do not apply, please mark “none” | ||||||
|---|---|---|---|---|---|---|
| Symptoms | None | Mild | Moderate | Severe | Extremely severe | |
| Score | ||||||
| 1 | 2 | 3 | 4 | 5 | ||
| 1 | Decline in your feeling of general well-being (general state of health, subjective feeling) | □ | □ | □ | □ | □ |
| 2 | Joint pain and muscular ache (lower back pain, joint pain, pain in a limb, general back ache) | □ | □ | □ | □ | □ |
| 3 | Excessive sweating (unexpected/sudden episodes of sweating, hot flushes independent of strain) | □ | □ | □ | □ | □ |
| 4 | Sleep problems (difficulty in falling asleep, difficulty in sleeping through, waking up early and feeling tired, poor sleep, sleeplessness) | □ | □ | □ | □ | □ |
| 5 | Increased need for sleep, often feeling tired | □ | □ | □ | □ | □ |
| 6 | Irritability (feeling aggressive, easily upset about little things, moody) | □ | □ | □ | □ | □ |
| 7 | Nervousness (inner tension, restlessness, feeling fidgety) | □ | □ | □ | □ | □ |
| 8 | Anxiety (feeling panicky) | □ | □ | □ | □ | □ |
| 9 | Physical exhaustion/lacking vitality (general decrease in performance, reduced activity, lacking interest in leisure activities, feeling of getting less done, of achieving less, of having to force oneself to undertake activities) | □ | □ | □ | □ | □ |
| 10 | Decrease in muscular strength (feeling of weakness) | □ | □ | □ | □ | □ |
| 11 | Depressive mood (feeling down, sad, on the verge of tears, lack of drive, mood swings, feeling nothing is of any use) | □ | □ | □ | □ | □ |
| 12 | Feeling that you have passed your peak | □ | □ | □ | □ | □ |
| 13 | Feeling burnt out, having hit rock-bottom | □ | □ | □ | □ | □ |
| 14 | Decrease in beard growth | □ | □ | □ | □ | □ |
| 15 | Decrease in ability/frequency to perform sexually | □ | □ | □ | □ | □ |
| 16 | Decrease in the number of morning erections | □ | □ | □ | □ | □ |
| 17 | Decrease in sexual desire/libido (lacking pleasure in sex, lacking desire for sexual intercourse) | □ | □ | □ | □ | □ |
After completing the questionnaire, a routine clinical examination involving height, weight, and waist circumference (WC) was conducted by a trained nurse. Body mass index (BMI) was calculated by dividing body weight (kg) by height in meters squared and categorized into four groups: underweight (BMI <18.5 kg m −2), normal weight (18.5 kg m −2 ≤ BMI <24 kg m −2), overweight (24 kg m −2 ≤ BMI <28 kg m −2), and obese (BMI ≥28 kg m −2) according to the Chinese BMI criteria.18 With respect to abdominal adiposity status, the Chinese criteria were used to classify males as normal risk (WC <85 cm), preobese (85 cm ≤ WC <90 cm) and obese (WC ≥90 cm).18
Fasting venous blood samples were drawn between 8:00 and 10:00 in the morning. Serum was stored at −70°C until hormone assessment. TT, LH, and SHBG were determined by chemiluminescent immunoassays on a UniCel DxI 800 analyzer (Beckman Coulter, Inc., Brea, CA, USA). FT was calculated using the formula developed.19 All biochemical evaluations were performed in Center of Reproductive Medicine, Tongji Medical College, Huazhong University of Science and Technology (Wuhan, China).
Operational definition of LOH
The operational definition of LOH is based on the Guidelines and expert consensus for the diagnosis and treatment of male disease in China,3 which was presented by the Society of Andrology of Chinese Medical Association in 2017.
The consensus stipulates that clinical symptoms of low testosterone should be used in conjunction with biochemical markers (low TT and/or cFT) to define LOH. According to the consensus, a TT level of <8.89 nmol l −1 (low TT) and an FT level of <210 pmol l −1 (low cFT) with the presence of at least three sexual symptoms are recommended for the diagnosis of LOH in the Chinese aging population.3,20 However, there was no operable questionnaire recommended to evaluate LOH-related symptoms in the expert consensus of China.
Various questionnaires have been constructed over the years to monitor the symptoms of LOH and their response to testosterone treatment, such as the AMS, the ADAM and the Massachusetts Male Aging Study Questionnaire.1 In this study, the AMS scale was used to monitor the symptoms of LOH because of its high sensitivity (68.8% in screening androgen deficiency of older Chinese men), simplicity and convenience.15
We analyzed the relationship between AMS symptoms and serum testosterone values to determine which symptoms were correlated with decreased serum testosterone levels, and then proposed an operational definition to evaluate the prevalence of LOH.
Subjects diagnosed with LOH were divided into two different categories: primary HG (LH >10.3 IU l −1) and secondary HG (LH ≤10.3 IU l −1). The LH threshold corresponded to the 97.5th centile (the upper limit of normal) value in the youngest group (40 years–44 years) in our analysis cohort.
Statistical analyses
Descriptive statistics are provided in the form of the mean and standard deviation (mean ± s.d.) for quantitative variables and number and percentage (%) for categorical variables. Student's t-test or one-way ANOVA was used to compare parametric data. Differences in proportions were tested by Chi-square test and Fisher's exact test as appropriate. Linear regression analyses were used to examine the factors associated with serum hormonal levels. Risk factors related to primary and secondary HG were estimated using a logistic regression model. A two-sided P < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Participants' characteristics
The mean age, WC and BMI of the 5078 subjects were 55.7 ± 9.4 years, 86.9 ± 11.1 cm, and 24.3 ± 3.3 kg m −2, respectively (Table 1). Almost all of the participants (99.8%) were of Han nationality. The majority were from rural areas (88.9%), and 95.4% of them were married or living with a partner. Most men (55.5%) reported that they had received a secondary school education, with only 6.3% reporting illiteracy. A total of 56.8% of the subjects were current smokers, 43.5% of them reported 1 or more comorbidities, and 14.3% had self-reported diabetes mellitus (Table 1).
Table 1.
Characteristics of all participants and different gonadal status
| Parameter | All | Eugonadal | Primary HG | Secondary HG | *P |
|---|---|---|---|---|---|
| Subjects | 5078 (100) | 4683 (92.2) | 103 (2.0) | 292 (5.8) | NS |
| TT (nmol l−1) | 16.1±5.1 | 16.3±5.1 | 14.1±4.3 | 12.6±3.9 | <0.01 |
| cFT (pmol l−1) | 276.8±87.8 | 285.6±85.4 | 159.0±36.2 | 178.3±26.4 | <0.01 |
| SHBG (nmol l−1) | 46.3±22.5 | 45.0±21.3 | 77.5±30.4 | 56.2±26.6 | <0.01 |
| LH (IU l−1) | 6.2±4.2 | 6.0±3.7 | 19.2±9.2 | 5.6±2.2 | <0.01 |
| Age (year) | 55.7±9.4 | 55.0±9.2 | 67.9±6.8 | 62.0±8.0 | <0.01 |
| WC (cm) | 86.9±11.1 | 87.0±11.1 | 83.0±12.2 | 87.5±10.6 | <0.01 |
| BMI (kg m−2) | 24.3±3.3 | 24.3±3.3 | 24.0±3.3 | 26.5±3.5 | <0.01 |
| Han nationality | 5069 (99.8) | 4674 (99.8) | 103 (100.0) | 292 (100.0) | 1.00 |
| Rural | 4513 (88.9) | 4165 (88.9) | 92 (89.3) | 256 (87.7) | 0.79 |
| Married or with partner | 4843 (95.4) | 4477 (95.6) | 92 (89.3) | 274 (93.8) | <0.01 |
| Secondary education | 2820 (55.5) | 2668 (57.0) | 32 (31.1) | 120 (41.1) | <0.01 |
| Smoking status (current) | 2887 (56.8) | 2662 (56.8) | 60 (58.2) | 165 (56.5) | 0.65 |
| One or more comorbiditiesa | 2211 (43.5) | 1973 (42.1) | 66 (64.1) | 172 (58.9) | <0.01 |
| Self-reported diabetes | 728 (14.3) | 632 (13.5) | 29 (28.2) | 67 (22.9) | <0.01 |
Data are expressed as the n (%) or mean±standard deviation. aSelf-reported comorbidity including diabetes, hypertension, heart disease, chronic bronchitis or asthma, cancer, stoke, tuberculosis, liver disease, and prostate disease. *P shows differences between eugonadal men, men with primary HG, and with secondary HG. HG: hypogonadism; NS: not suitable; TT: total testosterone; cFT: calculated free testosterone; SHBG: sex hormone-binding globulin; LH: luteinizing hormone; WC: waist circumference; BMI: body mass index
Serum reproductive hormones
Relationships between hormone levels and age, BMI, smoking status, and comorbidities were assessed (Table 2). The linear regression analysis demonstrated that the TT level was not correlated with age (P = 0.59). The cFT level was negatively correlated with age (β = −0.32; P < 0.01). The SHBG (β = 0.35; P < 0.01) and LH (β = 0.34; P < 0.01) levels were positively correlated with age. BMI was an independent factor influencing the concentrations of TT (β = −0.33; P < 0.01), cFT (β = −0.04; P < 0.01), SHBG (β = −0.42; P < 0.01), and LH (β = −0.13; P < 0.01). Current cigarette smoking was positively related to TT (β = 0.09; P < 0.01), cFT (β = 0.07; P < 0.01), and SHBG (β = 0.04; P = 0.01) levels.
Table 2.
Correlation study on factors related to the levels of hormones
| Variable | TT (nmol l−1) | cFT (pmol l−1) | SHBG (nmol l−1) | LH (IU l−1) | ||||
|---|---|---|---|---|---|---|---|---|
| β | P | β | P | β | P | β | P | |
| Age (year) | 0.01 | 0.59 | −0.32 | <0.01* | 0.35 | <0.01* | 0.34 | <0.01* |
| BMI (kg m−2) | −0.33 | <0.01* | −0.04 | 0.01* | −0.42 | <0.01* | −0.13 | <0.01* |
| Smoking status (current) | 0.09 | <0.01* | 0.07 | <0.01* | 0.04 | 0.01* | 0.03 | 0.08 |
| Smoking status (past) | 0.02 | 0.11 | 0.02 | 0.25 | 0.01 | 0.41 | 0.01 | 0.68 |
| 1 or more comorbiditiesa | 0.01 | 0.42 | 0.02 | 0.15 | −0.02 | 0.09 | 0.02 | 0.09 |
*P<0.05. β: standardized coefficient. aSelf-reported comorbidity including diabetes, hypertension, heart disease, chronic bronchitis or asthma, cancer, stoke, tuberculosis, liver disease, and prostate disease. TT: total testosterone; cFT: calculated free testosterone; SHBG: sex hormone-binding globulin; LH: luteinizing hormone; BMI: body mass index
Relationship between LOH symptoms and testosterone levels
As shown in Table 3, more than half (52.7%) of the 5078 subjects reported AMS positivity with a total score ≥27, and 35.6% experienced at least three sexual symptoms. The AMS total score was not significantly associated with either low TT or cFT (TT, P = 0.87; cFT, P = 0.25). The reverse relationship between low cFT and the presence of at least three sexual symptoms was observed. The percentage of men having at least three sexual symptoms was significantly increased in subjects with cFT <210 pmol l −1 compared with subjects with cFT ≥210 pmol l −1 (38.5% vs 34.9%; P = 0.03) but did not differ between different TT categories (36.7% vs 35.6%; P = 0.74).
Table 3.
Prevalence (%) of symptoms among 5078 subjects and different total testosterone and calculated free testosterone category
| All subjects (n=5078), % | TT (nmol l−1) | cFT (pmol l−1) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| <8.9 (n=229), % | ≥8.9 (n=4849), % | χ2 | P | <210 (n=1025), % | ≥210 (n=4053), % | χ2 | P | ||
| AMS total score ≥27 | 52.7 | 53.3 | 52.7 | 0.03 | 0.87 | 54.3 | 52.3 | 1.33 | 0.25 |
| Sexual symptoms | |||||||||
| Felt pass the peak | 17.6 | 17.0 | 17.6 | 0.05 | 0.83 | 15.7 | 18.0 | 3.06 | 0.08 |
| Decrease in beard growth | 5.6 | 7.4 | 5.5 | 1.49 | 0.22 | 6.2 | 5.5 | 0.97 | 0.33 |
| Decreased ability of sexual activity | 41.0 | 41.0 | 41.0 | 0.00 | 0.98 | 42.9 | 40.5 | 2.05 | 0.15 |
| Weakened morning erections | 39.5 | 40.2 | 39.5 | 0.04 | 0.84 | 42.0 | 38.9 | 3.43 | 0.06 |
| Lessened sexual desire/libido | 38.9 | 42.8 | 38.7 | 1.52 | 0.22 | 41.0 | 38.4 | 2.30 | 0.13 |
| At least three sexual symptoms | 35.6 | 36.7 | 35.6 | 0.11 | 0.74 | 38.5 | 34.9 | 4.68 | 0.03 |
AMS: Aging Males’ Symptoms; TT: total testosterone; cFT: calculated free testosterone
The proportion of subjects with low testosterone and sexual symptoms
As shown in Table 4. Of the 5078 subjects, 4.5% had a TT level <8.9 nmol l −1 (low TT), 20.2% had a cFT level <210 pmol l −1 (low cFT), and 35.6% experienced at least three sexual symptoms. Significant regional differences were observed in the prevalence of low TT, low cFT, and at least three sexual symptoms (all P < 0.05). Compared to subjects in urban areas, the men in rural areas presented a higher prevalence of low TT (4.6% vs 3.5%), low cFT (20.6% vs 17.0%), and at least three sexual symptoms (35.8% vs 34.3%), whereas significance was only observed for the prevalence of cFT (P = 0.045). There was no significant difference in the prevalence of low TT among different age groups (P = 0.199). However, the prevalence of low cFT and the prevalence of at least three sexual symptoms increased significantly with increasing age (all P < 0.05). Moreover, abdominal adiposity status and BMI categories were found to be significantly associated with the prevalence of low TT and low cFT but not associated with the prevalence of at least three sexual symptoms. Compared with nonsmokers, current smokers had the lowest prevalence of low TT and cFT. A significantly higher prevalence of low cFT and at least three sexual symptoms were seen in men who reported 1 or more comorbidities than in men without comorbidities.
Table 4.
Percentage of men with low testosterone values and had at least three sexual symptoms by demographics
| n | Low TT (%) | P | Low cFT (%) | P | ≥3 sexual symptoms (%) | P | |
|---|---|---|---|---|---|---|---|
| Total subjects | 5078 | 4.5 | 20.2 | 35.6 | |||
| Region | <0.001 | <0.001 | <0.001 | ||||
| Northern | 933 | 4.2 | 16.7 | 51.3 | |||
| Eastern | 926 | 7.6 | 23.5 | 42.2 | |||
| Southern | 819 | 5.5 | 33.1 | 5.3 | |||
| Central | 706 | 2.3 | 22.7 | 33.0 | |||
| Northwest | 886 | 4.5 | 15.2 | 29.1 | |||
| Southwest | 808 | 2.4 | 10.5 | 50.2 | |||
| Rural/urban division | 0.239 | 0.045 | 0.491 | ||||
| Rural | 4513 | 4.6 | 20.6 | 35.8 | |||
| Urban | 565 | 3.5 | 17.0 | 34.3 | |||
| Age groups (year) | 0.199 | <0.001 | <0.001 | ||||
| 40–44 | 668 | 3.3 | 7.8 | 14.5 | |||
| 45–49 | 917 | 5.2 | 9.8 | 22.0 | |||
| 50–54 | 778 | 5.7 | 14.7 | 27.9 | |||
| 55–59 | 907 | 4.0 | 20.7 | 39.8 | |||
| 60–64 | 860 | 3.6 | 24.8 | 49.0 | |||
| 65–69 | 518 | 5.4 | 33.0 | 51.0 | |||
| 70–74 | 276 | 4.0 | 44.6 | 57.2 | |||
| 75–79 | 154 | 5.8 | 48.1 | 58.4 | |||
| Abdominal adiposity status | <0.001 | <0.001 | 0.221 | ||||
| Normal risk | 2071 | 1.9 | 18.1 | 36.9 | |||
| Preobese | 902 | 3.7 | 18.2 | 34.0 | |||
| bese | 2105 | 7.4 | 22.7 | 34.8 | |||
| BMI categories | <0.001 | <0.001 | 0.763 | ||||
| Under weight | 144 | 2.1 | 19.4 | 33.3 | |||
| Normal weight | 2338 | 2.0 | 17.0 | 36.4 | |||
| Overweight | 1930 | 5.0 | 21.8 | 35.1 | |||
| Obese | 666 | 12.6 | 39.6 | 35.3 | |||
| Marital status | 0.311* | <0.001 | 0.027 | ||||
| Unmarried | 45 | 6.7 | 13.3 | 31.1 | |||
| Married | 4843 | 4.6 | 19.8 | 35.4 | |||
| Divorce | 42 | 0.0 | 19.0 | 28.6 | |||
| Widowhood | 148 | 2.7 | 36.5 | 46.6 | |||
| Educational level | 0.355 | <0.001 | <0.001 | ||||
| Illiteracy | 313 | 3.2 | 31.1 | 55.9 | |||
| Primary | 1522 | 4.0 | 27.6 | 41.3 | |||
| Secondary | 2826 | 4.9 | 16.3 | 32.6 | |||
| Tertiary | 417 | 4.6 | 10.8 | 20.4 | |||
| Smoking status | 0.015 | 0.010 | <0.001 | ||||
| Current | 2887 | 3.8 | 18.7 | 37.7 | |||
| Past | 588 | 5.3 | 22.4 | 40.0 | |||
| Never | 1603 | 5.6 | 22.0 | 30.4 | |||
| Number of comorbiditiesa | 0.07 | 0.001 | <0.001 | ||||
| 0 | 2867 | 4.0 | 18.5 | 27.6 | |||
| One or more | 2211 | 5.1 | 22.3 | 46.1 |
aSelf-reported comorbidity including diabetes, hypertension, heart disease, chronic bronchitis or asthma, cancer, stoke, tuberculosis, liver disease, and prostate disease. *Fisher exact probability. TT: total testosterone; cFT: calculated free testosterone; BMI: body mass index
Estimated prevalence of LOH
In the current study, the TT level did not decrease with age (Table 2), and had no correlation with clinical symptoms (Table 3). However, the cFT level declined with age (Table 2), and the association between a low cFT level (>210 pmol l −1) and the presence of at least three sexual symptoms is shown in Table 3. Thus, a cFT level of <210 pmol l −1 with the presence of at least three sexual symptoms was suggested for the diagnosis of LOH.
Based on this criterion, the overall estimated prevalence of LOH was 7.8% (395 of 5078 subjects) and increased with age, from 0.9% for men 40 years–44 years of age, to 3.2% for those 50 years–54 years, to 11.2% for those 60 years–64 years and to 24.0% for those 75 years–79 years (P < 0.001). In urban areas, the overall LOH prevalence was 8.3%, and in rural areas, it was 7.7%, whereas the urban-rural difference was not statistically significant (P = 0.61). Furthermore, the LOH prevalence was 11.9% in northern China, 8.6% in eastern China, 2.0% in southern China, 10.1% in central China, 6.2% in northwest China, and 7.7% in southwest China, and this difference among regions was significant (P < 0.001; Figure 1).
Figure 1.
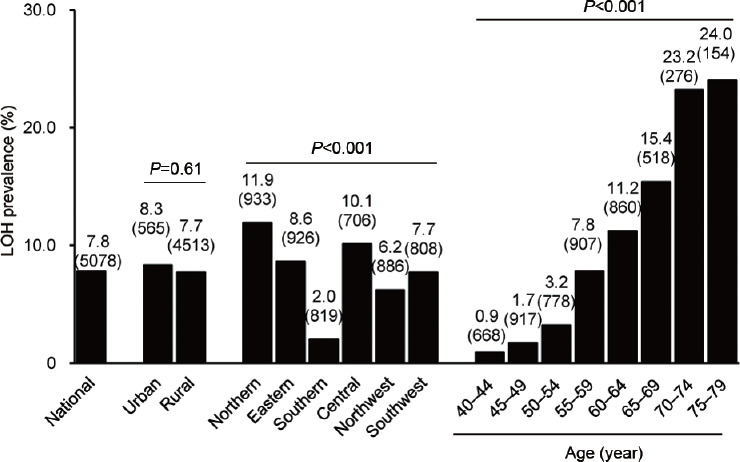
Prevalence of LOH by urban/rural, region and age. LOH: late-onset hypogonadism.
Categories of LOH
A total of 2.0% (103/5078) and 5.8% (292/5078) of subjects had primary and secondary HG, respectively (Table 1). SHBG levels in the primary (77.5 ± 30.4 nmol l −1) and secondary (56.2 ± 26.6 nmol l −1) HG groups were significantly higher than those in the eugonadal group (45.0 ± 21.3 nmol l −1). Men with primary (67.9 ± 6.8 years) and secondary (62.0 ± 8.0 years) HG were older than men in the eugonadal group (55.7 ± 9.4 years). BMI in the secondary HG group (26.5 ± 3.5 kg m −2) was higher than that in the other groups. The percentage of men who had 1 or more comorbidities in the primary (64.1%) and secondary (58.9%) HG groups was higher than that in the eugonadal group (42.1%; Table 1).
After adjusting for confounding factors (education, marital status, BMI and smoking status), the logistic regression analysis showed that older men were more likely to have primary or secondary HG, with odds ratios (ORs) of 1.152 (P < 0.001) and 1.073 (P < 0.001), respectively (Table 5). Those who reported one or more comorbidities had ORs of 1.603 (P = 0.029) and 1.463 (P = 0.003) for primary and secondary HG, respectively. BMI was an independent risk factor for secondary HG (OR = 1.123; 95% confidence interval [CI]= 1.053–1.199; P < 0.001; Table 5).
Table 5.
Risk factors associated with primary and secondary hypogonadism
| Parameter | Primary HG | Secondary HG | ||
|---|---|---|---|---|
| OR (95% CI) | P | OR (95% CI) | P | |
| Age (year) | 1.152 (1.122–1.183) | <0.001 | 1.073 (1.059–1.087) | <0.001 |
| BMI (kg m−2) | NS | NS | 1.123 (1.053–1.199) | <0.001 |
| One or more comorbiditiesa | 1.603 (1.049–2.449) | 0.029 | 1.463 (1.143–1.873) | 0.003 |
aSelf-reported comorbidity including diabetes, hypertension, heart disease, chronic bronchitis or asthma, cancer, stoke, tuberculosis, liver disease, and prostate disease. HG: hypogonadism; OR: odds ratio; CI: confidence interval; NS: not suitable; BMI: body mass index
DISCUSSION
The present study was a national community-based study on the estimated prevalence of LOH in aging Chinese males. Both biochemical and symptomatic information were used for the diagnosis of LOH.
There is continued debate concerning whether a general decrease in serum testosterone levels exists in older men. Although the average TT level was found to decline with age in many studies,14,21,22 this age-related decline in TT was not observed in the present study or in several studies carried out in China,23,24 Japan,25,26 and Australia.27 The precise causes for this variation are unknown, but biological factors, such as interindividual variability or ethnic factors, or the different methodological approaches for testosterone measurement may account for this variation. In the current study, approximately 4.5% of the subjects had a TT level <8.9 nmol l −1, while the proportion of men with a lower TT value (>8.9 nmol l −1) by age remained consistent, showing no effects of age. These findings challenge the theory that age-related reduction in TT contributes to LOH progression, indicating that TT may not be a proper marker for diagnosing LOH. The reason for the stability of testosterone concentrations with increasing age is not fully understood but may be due to the compensatory increase caused by the age-associated increase in LH levels, which could stimulate Leydig cells to produce testosterone.
We also found that cFT concentrations decreased and SHBG, LH level increased with increasing age, which is consistent with a number of reports from cross-sectional studies.28 Approximately 60% of testosterone in serum is strongly bound to SHBG, 38% is weakly bound to albumin, and only 2% of testosterone remains in free, nonprotein-bound form, representing the biologically active fraction.29 These proportions vary somewhat and are dependent on the relative concentrations and affinities of SHBG and albumin.30 It is known that the amount of SHBG increases in serum with age, indicating that the proportion of bioactive FT decreases.31 However, it is unclear why SHBG levels increase with age, but age-associated decreases in growth hormone and insulin-like growth factor I levels might contribute to the increase.26 In addition, the proportion of men with a lower cFT value (>210 pmol l −1) was 20.2% and significantly increased with aging, from 7.8% in the 40–44-year-old group to 48.1% in the 75–79-year-old group. Thus, we suggest that the occurrence of LOH may be due to the subsequent decrease in biological testosterone caused by the significant age-dependent increase in SHBG.
However, neither the AMS scale nor the ADAM questionnaire is recommended to be used alone to diagnosis LOH because of their poor specificity.1,3 These questionnaires help identify subjective LOH symptoms. Patients at risk or suspected of having positive AMS or ADAM results are recommended to undergo a complete biochemical checkup to determine their testosterone level. The AMS scale has been used more widely than the ADAM questionnaire in the Asian population.20 The AMS scale 15 was used to monitor LOH-related symptoms because of its high sensitivity, simplicity and convenience.
In this sample, 52.7% of the 5078 subjects reported AMS positivity with a total score ≥27, and 35.6% experienced at least three sexual symptoms. Moreover, about 51.3% and 50.2% of the males in northern and southwest China experienced at least three sexual symptoms. In a community-based study composed of 944 men aged 40 years–79 years from nine urban communities in China, 37.4% of the subjects had decreased ability/frequency to perform sexually, 35.0% had decreased frequency of morning erections, and 34.4% had decreased sexual desire/libido. Furthermore, 44.9% of the subjects experienced one of the three sexual symptoms, and 26.0% of the subjects experienced all three sexual symptoms.12 In a recent cross-sectional study, that recruited 9164 Chinese men aged 35 years–70 years at 33 study centers in 21 provinces, 4 municipalities, and 4 autonomous regions, 10% of the overall study population had AMS scores ≥50, with the incidence in men >40 years being 12% and in men ≤40 years being 2%.32 Our results together with previous findings suggest that sexual symptoms are common among middle-aged and elderly men in China. We also found that the AMS total score was not significantly associated with low TT or cFT, implying that the AMS total score may not be a proper predictor of low serum testosterone.
Further analyses revealed that the prevalence of low TT had no significant correlation with either AMS total score or sexual symptoms, which supports the results of some studies 23,33 and contradicts the results of another study.11 In contrast, a significant association between a cFT level of <210 pmol l −1 and an increasing frequency of at least three sexual symptoms was observed. Recent data from EMAS also indicated that low cFT, even in the presence of normal TT, is associated with androgen deficiency-related symptoms. Normal cFT, despite low TT, is not associated with cognate symptoms.34 Therefore, cFT may be more reliable than TT levels for diagnosing LOH in middle-aged and elderly males in China. In fact, the Japanese Urological Association and the Japanese Association of Men's Health have recommended an FT value of <225 pmol l −1 (65 pg ml −1) as the diagnostic criteria for LOH regardless of symptoms.20,28 Thus, we suggested a cFT level of <210 pmol l −1 combined with the presence of at least three sexual symptoms for the diagnosis of LOH in middle-aged and elderly men in China.
Based on this proposed criterion, the estimated prevalence of LOH was 7.8%, and increased significantly from 0.9% in 40–49-year-old men to 24.0% in men aged between 75 years and 79 years. The prevalence of LOH has previously been found to be 9.1% using the criteria of the presence of three sexual symptoms with TT levels <13.21 nmol l −1 and cFT levels <268.89 pmol l −1 in a community-based study composed of 944 men aged 40 years–79 years from nine urban communities in China.12 The expert consensus and guidelines for the diagnosis and treatment of male disease in China suggested that the prevalence of LOH in China is 10%–20%.3 Our results suggest that LOH is less common than previously thought, which is most likely due to the more stringent nature of our operational definition. In EMAS, the prevalence was 2.1% based on the criteria of TT level <8 nmol l −1 or TT level of 8 nmol l −1–11 nmol l −1 and FT level <220 pmol l −1 together with the presence of three sexual symptoms.11 Different races, cultures, and dietary customs of subjects may account for the difference in LOH prevalence between EMAS and our estimate. In addition, the prevalence of LOH was obviously different between regions but remained not significantly different between urban and rural areas (8.3% vs 7.7%; P = 0.61). These results may suggest that the rural-urban differences in ethnicities, living environment, dietary habits, and metabolism are decreasing due to the urbanization process of China.
In the present study, around three-fourths of men with LOH had secondary HG, which is comparable to the results of EMAS.10 A recent study from the USA also showed that 74.2% of hypogonadal men presenting to a tertiary care center had secondary HG.35 These similar data suggest that secondary HG appears to be the most common form of LOH. In addition, we confirmed that primary HG was positively associated with age and comorbidities, with ORs of 1.152 and 1.603, respectively. In EMAS, older men were more likely to have primary HG (relative risk ratio [RRR] = 3.04; P < 0.001). Those who reported more than one comorbid condition had an RRR of 2.25 (P < 0.05) for primary HG.10,36 Secondary HG was found to be positively associated with age, BMI and comorbidities, with ORs of 1.073, 1.123, and 1.463, respectively. In EMAS, obesity emerged to be the most potent risk factor for secondary HG, with a smaller contribution of comorbidities, while there was no significant relationship between the prevalence of secondary HG and aging.10 Findings from the recent USA study also showed that elevated BMI was associated with secondary HG.35
Our study strengths include a relatively large sample size compared to other studies performed in China and the definition of LOH that was proposed based on the Chinese guidelines. The study has limitations as well. First, although immunoassays (IAs) have been used for measuring testosterone in many large hospitals because they usually provide rapid, economical and reliable information about circulating hormone concentrations, the accuracy and precision of testosterone IAs remain a concern.1 Second, as reference laboratory methods for measuring FT by equilibrium dialysis are laborious, costly and nonautomatable, FT levels are often calculated (cFT) rather than measured.37 In the present study, the FT value was determined with the use of the formula developed by Vermeulen et al.19 based on measurements of TT, SHBG and albumin. While the accuracy of aforementioned equation for FT by Vermeulen has been recently criticized.37
CONCLUSIONS
Based on data from a national survey, we found that AMS total score is not an appropriate indicator for decreased testosterone. A cFT level of <210 pmol l −1 combined with the presence of at least three sexual symptoms was suggested for diagnosing LOH. According to this criterion, the estimated prevalence of LOH was 7.8% among middle-aged and elderly males in China and significantly increased with age. Secondary HG is the most common form of LOH. Both primary and secondary HG were positively associated with age and comorbidities. BMI was an independent risk factor for secondary HG.
AUTHOR CONTRIBUTIONS
YJL and XBS carried out the analysis of the data, drafted, and revised the manuscript; NY, XJS, YQG, LDZ, and CLX assisted in the study design and coordination of data collection; and ZY and YZZ conceived the study, participated in its design and coordination and helped revise the manuscript. All authors read and approved the final manuscript.
COMPETING INTERESTS
All authors declared no competing interests.
ACKNOWLEDGMENTS
This work was supported by the 12th Five-year Plan of National Science and Technology of China (No. 2012BAI32B03) and the Central Special Talent Construction Funds of China for Zunyi Medical University (No. Qiancaijiao 2015-134).
Supplementary Information is linked to the online version of the paper on the Asian Journal of Andrology website.
REFERENCES
- 1.Huhtaniemi I. Late-onset hypogonadism: current concepts and controversies of pathogenesis, diagnosis and treatment. Asian J Androl. 2014;16:192–202. doi: 10.4103/1008-682X.122336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Corona G, Goulis DG, Huhtaniemi I, Zitzmann M, Toppari J, et al. European Academy of Andrology (EAA) guidelines on investigation, treatment and monitoring of functional hypogonadism in males. Andrology. 2020;8:970–87. doi: 10.1111/andr.12770. [DOI] [PubMed] [Google Scholar]
- 3.Jiang H. Guidelines and Expert Consensus for the Diagnosis and Treatment of Male Disease. Beijing: People's Medical Publishing House; 2017. [Google Scholar]
- 4.Tharakan T, Miah S, Jayasena C, Minhas S. Investigating the basis of sexual dysfunction during late-onset hypogonadism F1000Res 2019; 8. F100Faculty Rev. :331. doi: 10.12688/f1000research.16561.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Nieschlag E. Late-onset hypogonadism: a concept comes of age. Andrology. 2019 doi: 10.1111/andr.12719. doi: 10.111/andr.12719. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 6.Lunenfeld B, Mskhalaya G, Zitzmann M, Arver S, Kalinchenko S, et al. Recommendations on the diagnosis, treatment and monitoring of hypogonadism in men. Aging Male. 2015;18:5–15. doi: 10.3109/13685538.2015.1004049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Swee DS, Gan EH. Late-onset hypogonadism as primary testicular failure. Front Endocrinol (Lausanne) 2019;10:372. doi: 10.3389/fendo.2019.00372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Golan R, Scovell JM, Ramasamy R. Age-related testosterone decline is due to waning of both testicular and hypothalamic-pituitary function. Aging Male. 2015;18:201–4. doi: 10.3109/13685538.2015.1052392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Braga PC, Pereira SC, Ribeiro JC, Sousa M, Monteiro MP, et al. Late-onset hypogonadism and lifestyle-related metabolic disorders. Andrology. 2020 doi: 10.1111/andr.12765. Doi:10.111/andr.12765. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 10.Tajar A, Forti G, O'Neill TW, Lee DM, Silman AJ, et al. Characteristics of secondary, primary, and compensated hypogonadism in aging men: evidence from the European male ageing study. J Clin Endocrinol Metab. 2010;95:1810–8. doi: 10.1210/jc.2009-1796. [DOI] [PubMed] [Google Scholar]
- 11.Wu FC, Abdelouahid T, Beynon JM, Pye SR, Silman AJ, et al. Identification of late-onset hypogonadism in middle-aged and elderly men. N Engl J Med. 2010;363:123–35. doi: 10.1056/NEJMoa0911101. [DOI] [PubMed] [Google Scholar]
- 12.Liu ZY, Zhou RY, Lu X, Zeng QS, Wang HQ, et al. Identification of late-onset hypogonadism in middle-aged and elderly men from a community of China. Asian J Androl. 2016;18:747–53. doi: 10.4103/1008-682X.160883. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Liu CC, Wu WJ, Lee YC, Wang CJ, Ke HL, et al. The prevalence of and risk factors for androgen deficiency in aging Taiwanese men. J Sex Med. 2009;6:936–46. doi: 10.1111/j.1743-6109.2008.01171.x. [DOI] [PubMed] [Google Scholar]
- 14.Kang S, Park HJ, Park NC. Serum total testosterone level and identification of late-onset hypogonadism: a community-based study. Korean J Urol. 2013;54:619–23. doi: 10.4111/kju.2013.54.9.619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kong XB, Guan HT, Li HG, Zhou Y, Xiong CL. The ageing males' symptoms scale for Chinese men: reliability, validation and applicability of the Chinese version. Andrology. 2014;2:856–61. doi: 10.1111/j.2047-2927.2013.00145.x. [DOI] [PubMed] [Google Scholar]
- 16.Heinemann L, Zimmermann T, Vermeulen A, Thiel C, Hummel W. A new 'aging males' symptoms' rating scale. Aging Male. 1999;2:105–14. [Google Scholar]
- 17.Moore C, Huebler D, Zimmermann T, Heinemann LA, Saad F. The Aging Males' Symptoms scale (AMS) as outcome measure for treatment of androgen deficiency. Eur Urol. 2004;46:80–7. doi: 10.1016/j.eururo.2004.01.009. [DOI] [PubMed] [Google Scholar]
- 18.National Health and Family Planning Commission of the People's Republic of China. WS/T 428–2013 Criteria of Weight for Adults. Beijing: Standards Press of China; 2013. p. 4. [Google Scholar]
- 19.Vermeulen A, Verdonck L, Kaufman JM. A critical evaluation of simple methods for the estimation of free testosterone in serum. J Clin Endocrinol Metab. 1999;84:3666–72. doi: 10.1210/jcem.84.10.6079. [DOI] [PubMed] [Google Scholar]
- 20.An Q, Gu YQ. Testosterone replacement therapy: dilemmas and challenges in China and Asia. Asian J Androl. 2018;20:149–51. doi: 10.4103/aja.aja_16_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Araujo AB, O'Donnell AB, Brambilla DJ, Simpson WB, Longcope C, et al. Prevalence and incidence of androgen deficiency in middle-aged and older men: estimates from the Massachusetts Male Aging Study. J Clin Endocrinol Metab. 2004;89:5920–6. doi: 10.1210/jc.2003-031719. [DOI] [PubMed] [Google Scholar]
- 22.Wu FC, Tajar A, Pye SR, Silman AJ, Finn JD, et al. Hypothalamic-pituitary-testicular axis disruptions in older men are differentially linked to age and modifiable risk factors: the European Male Aging Study. J Clin Endocrinol Metab. 2008;93:2737–45. doi: 10.1210/jc.2007-1972. [DOI] [PubMed] [Google Scholar]
- 23.Liu Z, Liu J, Shi X, Wang L, Yang Y, et al. Comparing calculated free testosterone with total testosterone for screening and diagnosing late-onset hypogonadism in aged males: a cross-sectional study. J Clin Lab Anal. 2017;31:e22073. doi: 10.1002/jcla.22073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Sun K, Liang GQ, Chen XF, Ping P, Yao WL, et al. Survey for late-onset hypogonadism among old and middle-aged males in Shanghai communities. Asian J Androl. 2012;14:338–40. doi: 10.1038/aja.2011.171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kurobe M, Kawai K, Suetomi T, Iwamoto T, Waku N, et al. High prevalence of hypogonadism determined by serum free testosterone level in Japanese testicular cancer survivors. Int J Urol. 2018;25:457–62. doi: 10.1111/iju.13537. [DOI] [PubMed] [Google Scholar]
- 26.Taya M, Koh E, Izumi K, Iijima M, Maeda Y, et al. Comparison of testosterone fractions between Framingham Heart Study participants and Japanese participants. Int J Urol. 2014;21:689–95. doi: 10.1111/iju.12393. [DOI] [PubMed] [Google Scholar]
- 27.Handelsman DJ, Sikaris K, Ly LP. Estimating age-specific trends in circulating testosterone and sex hormone-binding globulin in males and females across the lifespan. Ann Clin Biochem. 2016;53:377–84. doi: 10.1177/0004563215610589. [DOI] [PubMed] [Google Scholar]
- 28.Iwamoto T, Yanase T, Horie H, Namiki M, Okuyama A. Late-onset hypogonadism (LOH) and androgens: validity of the measurement of free testosterone levels in the diagnostic criteria in Japan. Int J Urol. 2009;16:168–74. doi: 10.1111/j.1442-2042.2008.02203.x. [DOI] [PubMed] [Google Scholar]
- 29.Goodale T, Sadhu A, Petak S, Robbins R. Testosterone and the Heart. Methodist Debakey Cardiovasc J. 2017;13:68–72. doi: 10.14797/mdcj-13-2-68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ho CK, Beckett GJ. Late-onset male hypogonadism: clinical and laboratory evaluation. J Clin pathol. 2011;64:459–65. doi: 10.1136/jcp.2010.076968. [DOI] [PubMed] [Google Scholar]
- 31.Rolf C, Zitzmann M, Nieschlag E. The aging male and late-onset hypogonadism. In: Nieschlag E, Behre HM, Nieschlag S, editors. Andrology: Male Reproductive Health and Dysfunction. Berlin, Heidelberg: Springer Berlin Heidelberg; 2010. pp. 239–61. [Google Scholar]
- 32.Li H, Zhang X, Wang H, Yang B, Li N, et al. A Chinese cross sectional study on symptoms in aging males: prevalence and associated factors. Am J Mens Health. 2019;13:1557988319838113. doi: 10.1177/1557988319838113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hamanoue N, Tanabe M, Tanaka T, zAkehi Y, Murakami J, et al. A higher score on the Aging Males' Symptoms scale is associated with insulin resistance in middle-aged men. Endocr J. 2017;64:521–30. doi: 10.1507/endocrj.EJ16-0619. [DOI] [PubMed] [Google Scholar]
- 34.Antonio L, Wu FC, O'Neill TW, Pye SR, Ahern TB, et al. Low free testosterone is associated with hypogonadal signs and symptoms in men with normal total testosterone. J Clin Endocrinol Metab. 2016;101:2647–57. doi: 10.1210/jc.2015-4106. [DOI] [PubMed] [Google Scholar]
- 35.Masterson JM, Soodana-Prakash N, Patel AS, Kargi AY, Ramasamy R. Elevated body mass index is associated with secondary hypogonadism among men presenting to a tertiary academic medical center. World J Mens Health. 2019;37:93–8. doi: 10.5534/wjmh.180047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ahern T, Swiecicka A, Eendebak RJ, Carter EL, Finn JD, et al. Natural history, risk factors and clinical features of primary hypogonadism in ageing men: longitudinal data from the European Male Ageing Study. Clin Endocrinol (Oxf) 2016;85:891–901. doi: 10.1111/cen.13152. [DOI] [PubMed] [Google Scholar]
- 37.Ly LP, Sartorius G, Hull L, Leung A, Swerdloff RS, et al. Accuracy of calculated free testosterone formulae in men. Clin Endocrinol (Oxf) 2010;73:382–8. doi: 10.1111/j.1365-2265.2010.03804.x. [DOI] [PubMed] [Google Scholar]