

Abstract
Background:
Social anxiety (SA) and depression are prevalent, often comorbid disorders, associated with poor psychosocial functioning. Experimental psychopathology approaches can clarify the transdiagnostic mechanisms underlying these disorders, but most laboratory tasks are limited. We developed and validated the Audio–Dialogue Inductions of Social Stress (A-DISS) experimental task to model real-time rejection sensitivity in a realistic and developmentally relevant context. Participants are asked to imagine overhearing peers at a party talking badly about them (Rejection) or a teacher at their school (Neutral).
Methods:
Study 1 focused on identifying and refining stimuli that elicited relevant emotional responses for Rejection (e.g., increased anxiety) and Neutral (e.g., no emotional changes) conditions (N=48). Study 2 examined whether participants’ SA and depression symptoms moderated the effects of A-DISS condition (N=52).
Results:
The Rejection condition elicited higher negative affect/lower positive affect while the Neutral condition sustained stable affect. Findings were consistent across gender and race/ethnicity. Moderation analyses were statistically significant; participants with elevated SA or depression reported feeling more rejected, insecure, and anxious after Rejection than those with below average symptoms.
Conclusions:
Findings provide preliminary validation of a novel peer rejection task for research on understanding the affective experience of real-time rejection overall, especially for those with elevated SA and depression. SA and depression symptoms each uniquely moderating the effects of Rejection exposure on similar affective states, suggests individuals with SA or depression may benefit from interventions targeting specific reactions to rejection/stress and transdiagnostic risk factors.
Keywords: Rejection, Social Stress, Experimental Psychopathology, Anxiety, Depression
Introduction
Social anxiety (SA) and depression are relatively common and associated with significant social and occupational difficulties (Kessler & Wang, 2008; McKnight, Monfort, Kashdan, Blalock, & Calton, 2016). These disorders are also often comorbid with each other, sharing features associated with impairment and distress (Bruce et al., 2005; Kessler, Chiu, Demler & Walters, 2005). Scholars have increasingly focused on developing etiological models of SA and depression; biopsychosocial models highlight the role of negative reactivity to social stressors as causal and maintenance factors (Epkins & Heckler, 2011; Spence & Rapee, 2016). Better understanding transdiagnostic risk/maintenance factors, such as negative reactivity to social stress, may help clarify the shared mechanisms and differentiating features of these disorders (Cuthbert & Kozak, 2013). Experimental psychopathology techniques are an effective way to empirically examine these features; however, few studies have done so (Zvolensky, Lejuez, Stuart, & Curtin, 2001). Here, we describe a new laboratory method for eliciting interpersonal rejection, and its application to SA and depressive symptomatology.
Negative reactivity to social stress may maintain and exacerbate SA and depression symptoms by eliciting aversive social interactions and decreasing the availability of positive social support. For SA, Spence and Rapee (2004, 2016) propose a deleterious cycle wherein youth with elevated SA elicit more negative reactions from family and peers, resulting in increased anxiety. For depression, interpersonal and stress generation theories suggest depression symptoms may erode the quality of individuals’ relationships, elicit stress, and increase or maintain levels of depression (Coyne, 1976; Hammen, 2006). The Cumulative Interpersonal Risk Model of SA and depression indicate that negative reactivity to social stressors is a risk and maintenance factor for both disorders independently as well as their comorbidity (Epkins & Heckler, 2011). These theories on the etiology and maintenance of both SA and depression converge to suggest that both disorders are marked by significant difficulties in interpersonal relationships, which maintain and exacerbate symptoms. Critically, empirical data aligns with theory; for example, individuals with SA and depression are often considered less liked by peers (Blöte, Kint, & Westenberg, 2007; Erath, Flanagan, & Bierman, 2007; Gazelle & Ladd, 2003) and display greater difficulties in relationships with family and peers (McLaughlin & Nolen-Hoeksema, 2012; Starr & Davila, 2008; Tran, Cole, & Weiss, 2012) than individuals without SA and depression. One factor that may play a particularly strong role in explaining these difficulties is sensitivity to interpersonal rejection.
Previous work has identified a number of transdiagnostic constructs that may maintain features of both anxiety and depression (e.g., repetitive negative thinking; Klemanski, Curtiss, McLaughlin, & Nolen-Hoeksema, 2017). Critically, sensitivity to interpersonal rejection may represent another important transdiagnostic construct to consider in the maintenance and etiology of both SA and depression (Slavich, O’Donovan, Epel, & Kemeny, 2010; Spence & Rapee, 2004; 2016). Interpersonal rejection is a common experience that can influence affect and behavior (Williams, 2007), and both SA and depression are associated with hypersensitivity to criticism, vigilance to social threat, as well as interpreting ambiguous feedback as negative (Amir, Beard, & Bower, 2005; Roberts, Hart, & Eastwood, 2010). For individuals with elevated SA, interpersonal rejection can elicit depression-like attentional biases, possibly representing an important transdiagnostic feature of SA and depressive symptoms (Kraines, White, Grant, & Wells, 2019). Yet within this transdiagnostic vulnerability of hypersensitivity to rejection, the specific affective responses to rejection may differentiate SA (anxiety, insecurity) and depressive (sadness, anger) risk (APA, 2013; Garber & Weersing, 2010; Kupferberg, Bicks, & Hasler, 2016).
Most of the literature on SA symptoms, depression, and sensitivity to social rejection rests on retrospective self-report methodologies, opening the possibility that observed findings are influenced by method variance and/or reporting biases (Epkins & Heckler, 2011; Starr & Davila, 2008). For example, when recalling previous rejection experiences, people may overestimate the impact the experience actually had on their emotional response (Thomas & Diener, 1990). Laboratory-based approaches can elicit feelings of interpersonal rejection under controlled laboratory conditions, thus limiting the effects of self-report biases or general negative affectivity on associations with SA and depression (Blackhart, Nelson, Knowles, & Baumeister, 2009; Zvolensky et al., 2001).
Unfortunately, existing social rejection tasks tend to have fairly limited generalizability to real world situations or include fairly complex tasks that are difficult to standardize and implement. For example, Cyberball involves an online ball tossing game where participants are gradually excluded by two other pre-programmed 2-Dimensional avatars whom are presented as fellow participants participating from another room/location (Williams et al., 2000). While easy to implement, the online context may undermine the ecological validity of research questions seeking to clarify in-person processes and be less likely to generalize to real-world behaviors (e.g., Bacon, Cranford, & Blumenthal, 2015). More interpersonally engaging tasks, such as the Yale Interpersonal Stressor (i.e., trained confederates actively exclude participants from a conversation), may be both effective and generalizable, though often are logistically challenging and cost prohibitive (Stroud, Tanofsky-Kraff, Wilfley, & Salovey, 2000). Using mental imagery to instill states of rejection may balance concerns surrounding standardization, feasible implementation, internal reliability, and ecological validity (Blackhart et al., 2009; Holmes & Matthews, 2010). Of these, the Articulated Thoughts in Simulated Situations (ATSS) ‘overheard conversation’ paradigm, offers a generalizable and realistic setting, though is designed to stimulate cognitions to be qualitatively coded, rather than induce states of rejection or stress (Davison et al., 1984; 1997).
Meta-analyses and reviews on experimental psychopathology techniques, and studies of rejection specifically, highlight three additional limitations of this area (e.g., Blackhart et al., 2009; Waters, LeBeau, & Craske, 2017; Zvolensky et al., 2001): 1. comparison/control conditions often involve acceptance (e.g., inclusion in ball-tossing games) or are non-social (e.g., reading task), superficially exaggerating the effects of rejection with conceptually distinct implications; 2. assessing only positive and negative affect as outcomes of social rejection, masking important heterogeneity in unique affective responses (e.g., anxiety; anger) for certain individuals (e.g., as a function of gender, clinical disorders), central to intervention development; 3. certain reactions to rejection may be delayed or persist for longer periods of time for individuals with SA or depression, requiring the assessment of timing, not evaluated in most studies.
As symptoms of SA and depression often emerge during adolescence and early adulthood, ecologically valid laboratory tasks that can simulate rejection using standardized methods for individuals in this age range are required (Kessler et al., 2005). Identifying a social, personally neutral state to serve as a meaningful control condition without conceptual (e.g., social vs. non-social) or methodological (e.g., different tasks and/or times) confounds is challenging (Blackhart et al., 2009). Accordingly, we developed and validated the Audio – Dialogue Inductions of Social Stress (A-DISS): a realistic social rejection task (and corresponding Neutral condition) to effectively elicit relevant emotional responses (e.g., anxiety, rejection, insecurity) and compared participants’ reactions to the task on the basis SA and depressive symptoms. While the task was intended to elicit similar responses across gender, as women report greater negative reactions to rejection and higher levels of SA and depression than men, we tested gender as a potential moderator (Asher, Asnaani, & Aderka, 2017; Blackhart et al., 2009; Nolen-Hoeksema, 2001). As both SA and depression are marked by sensitivity to rejection, we expected SA and depression symptoms to each moderate the effect of condition (Rejection vs. Neutral), such that those with higher levels of SA or depression would report feeling more rejected and insecure during Rejection exposure (Slavich et al., 2010; Spence & Rapee, 2004; 2016). As fear and anxiety of negative evaluation is a core characteristic of SA, we expected those with elevated SA to also report elevated anxiety during rejection (Spence & Rapee, 2004; 2016). Lastly, as irritability is a common feature of depression, we expected those with elevated depression to also report elevated anger and annoyance during rejection (Sheeber et al., 2009). Gender was not expected to significantly moderate the effects of condition on any of the outcomes.
Method
The A-DISS is an imagination procedure where participants are directly and explicitly rejected based on the existent literature (e.g., Blackhart et al., 2009). To activate social evaluation among adolescents/young adults, the imagined scenarios occur at a party setting with peers. Conditions are presented in a pre-recorded audio format to facilitate active engagement, enhance standardization, and allow experimenters to remain completely blind to condition assignments. Scripts were developed, and segment selection and validation for each condition occurred in two stages across two separate studies. The first stage empirically reduced the author-developed segments, resulting in eight, 15-25 second segments (final task time 4-5 minutes per condition). The second stage replicated the findings from stage one using the refined list of segments for each condition and explored potential individual differences in responding. To avoid carry-over effects, both studies were between-subjects designs where participants were randomly assigned to listen to, and provide feedback on, either the Neutral or Rejection segments. The Institutional Review Board at the University of North Texas approved all procedures prior to participant contact.
A-DISS Script Development & Audio Recording
The A-DISS content was based on the literature on related constructs (e.g., SA; rejection), laboratory paradigms (e.g., social stressors; emotional elicitation), and informal consultations with available adolescents/young adults (e.g., Blackhart et al., 2009; Williams, 2007; Zvolensky et al., 2001). Loosely following the format of the ATSS (Davison et al., 1987), the A-DISS is set at a party where the participant overhears a conversation about them (Rejection) or a teacher (Neutral). Graduate and undergraduate research assistants wrote scripts describing a man or woman, containing 15- 25 second ‘segments’ of dialogue to be read by two voice actors (1 man/ 1 woman), allowing for binary gender matching of pronouns/actors across conditions and to minimize potential gender bias. Segments were drafted over several months and revised through informal focus groups composed of men and women undergraduates (n = 12), non-college attending young adults (n = 2), and high-school students (n = 2). From this, 18 Rejection and 17 Neutral segments were identified for recording and validation testing.
Selected segments were audio recorded and edited in Audacity freeware (Audacity Team, 2019) to ensure high overall sound quality as well as consistency across segments, condition (Rejection vs. Neutral), and gender pronouns used (men vs. women). Once the substantive content of the recordings was finalized, background noise (e.g., indiscernible conversations) was added to build realism.
Stage 1: A-DISS Script Segment Selection & Preliminary Validation
Participants
College students 18+ years of age were recruited via SONA for a study on affective responding to social situations in exchange for course credit at a large Southwestern university. Fifty participants completed the study (Mage = 19.17 years, SDage = 1.74, range = 18-25 years; 70% Ciswomen; 30% Cismen). The plurality of participants identified as White (40%), followed by Black (22%), Hispanic (18%), multiracial (10%), Asian (2%), and other (2%).
Design & Procedure
Participants were informed that the study would examine how people react to certain social situations without reference to conditions or affective targets. After written consent, participants completed a brief set of demographic questionnaires (e.g., age, gender, race/ethnicity) and were introduced to the task by a research assistant. The research assistant instructed participants to close their eyes, tune into the thoughts running through their mind, then report on how they felt following each recorded segment (see Supplemental Materials for full instructions). Consistent with recommended best practices (Holmes & Mathews, 2010), participants were asked to imagine themselves in the situations that were being described as if it were happening in real time (rather than as an outside observer). After random assignment to task conditions via block randomization, participants were given pre-recorded condition-specific task instructions: “Imagine that you have arrived early to a party at a friend’s house in the late afternoon early evening. In the next room you overhear two people talking about [you a teacher you do not know]. They don’t know that you are listening, but you know that it’s [you/a teacher from your school] that they are talking about.”
Segments were presented in randomized order to minimize ordering effects within condition. Segments included gender-matched pronoun references for men and women. A sample segment for women in the Rejection condition:
Man: Did you see what she was wearing?
Woman: She looked ridiculous!
Man: I still can’t believe it!
Woman: Right? Like, who would walk out of the house like that?
Man: I have no idea!
Woman: And I mean, everyone was talking about it!
Man: I could never imagine wearing that in public.
A sample segment for men in the Neutral condition:
Man: How do you like that class by the way?
Woman: I dunno – it’s pretty boring.
Man: Yeah – the teacher kind of drones on.
Woman: It’s seriously so hard to sit through the entire class most days!
Man: Yeah, and it’s not like the material is hard I just can’t pay attention when the teacher sounds like a robot!
Woman: Do you think that’s what he always sounds like?
Man: Probably.
After each segment, participants rated their acute emotional states. After the final ‘blinded’ emotional reactivity rating, participants completed a brief post-task computer questionnaire and funneled debriefing interview. Once participants were informed about the purpose of the study, they were given printed transcripts of all of the segments they had listened to (either Rejection or Neutral) and asked to provide ‘unblinded’ feedback. As before, written transcripts were all presented in randomized order to minimize ordering effects.
Measures
Acute emotional reactivity (Blinded).
Self-reported emotional responses to each segment of the audio recordings were measured using single items from the well-established Subjective Units of Distress Scale (SUDS; Gotlib, Traill, Montoya, Joormann, & Chang, 2005; Wolpe, 1958). Participants rated current levels of feeling anxious, rejected, insecure, annoyed, bored, and happy from 1 (Not at all) to 9 (A lot) immediately pre-task (baseline) and following each individual segment.
Post-Task Measures (Unblinded).
Participants were provided written transcripts of each of the segments and asked to rate them on a scale of 0 (Not Realistic at All) to 10 (Very Realistic).
Baseline Measures (Blinded).
Participants completed demographic surveys and measures of SA during the baseline questionnaire period for descriptive purposes. The Social Interaction Anxiety Scale (SIAS; Mattick & Clarke, 1998) contains 20-items rated on a 0 (not at all) to 4 (extremely) scale indicating how much each characteristic is true of the participant (e.g., “I have difficulty talking with other people”) resulting in a possible sum score range of 0-80. The SIAS evidences good internal consistency (e.g., α = .95 in current sample) and stability over time (e.g., re-test coefficients >.90; Mattick & Clarke, 1998).
Data Quality.
Participants were assessed on their recall of study instructions with open-ended, face-valid, study-specific items (e.g., How many actors were present? Where did this scenario occur?) and confirmed whether they provided valid responses. Participants who failed multiple recall items or self-declared that they provided spurious responses were excluded from the final analyses.
Analytic Approach & Results
Data Quality and Descriptive Statistics.
One participant failed multiple data quality check/recall items and another participant self-disclosed providing spurious responses. Both were excluded, resulting in 25 participants in the Neutral (72% Ciswomen; M = 19.5 years, SD = 1.9) and 23 in the Rejection (70% Ciswomen, M = 18.8 years, SD = 1.4) condition. The total sample reported a mean level of 25.38 (SD = 17.59) on the SIAS; participants in the Neutral condition reported a mean of 22.8 (SD = 17.18) while those in the Rejection condition reported a mean of 28.8 (SD = 17.87). Chi Squared and independent sample t-tests did not reveal any statistically significant differences on gender, age, or SA symptoms across conditions (p’s > .05).
Identifying Segments.
Segments were evaluated based on the extent to which they elicited the expected emotional reactions under ‘true’ research task settings (i.e., blind to the purpose of the study) and the unblinded feedback after debriefing using descriptive analyses/figures. Rejection segments were rated on the extent to which they elicited greater anxiety, rejection, and insecurity compared to baseline levels and one another. Neutral segments were examined as to the extent negative affect was the same or lower than baseline levels and one another. All segments were further evaluated on realism ratings.
A series of one-way ANOVAs indicated no significant baseline differences across any SUDS rating F’s(1, 46) < 2.61, p’s > .05). Across all 18 of the Rejection segments, the mean SUDS values ranged from 5.05-6.35 on anxiety (as compared to M = 3.69, SD = 2.52 across the sample at baseline), 5.16-7.35 on rejection (M = 2.71, SD = 2.52 at baseline), 5.45-7.35 on insecurity (M = 3.77, SD = 2.74 baseline), 1.47-2.74 on happiness (M = 5.88, SD = 1.98 baseline), 5.05-7.25 on annoyance (M = 2.54, SD = 2.08 baseline), and 1.94-3.72 on boredom (M = 3.90, SD = 2.10). The mean realism ratings ranged from 6.00-7.73. As such, all Rejection segments were considered reasonably realistic, and determined to have increased negative affect, and decreased positive affect, from baseline.
Mean responses on the segments were then compared against each other to identify cutoffs for inclusion. As we wanted the Rejection condition to elicit above average feelings of rejection, insecurity, and anxiety we selected segments with the highest observed means, noting that 5 is the midpoint of the 1-9 rating scale. Thus, segments with an average rejection or insecurity rating below a 6.00 or anxiety rating below a 4.95 were excluded (n = 6). The remaining segments were ranked by realism ratings and the bottom four (with values < 6.62) were cut. The final eight Rejection segments averaged 5.64 (SD = 2.63) on anxiety, 6.88 on rejection (SD = 2.61), 6.65 (SD = 2.74) on insecurity, 1.94 (SD = 1.81) on happiness, 6.02 (SD = 2.78) on annoyance, and 2.71 (SD = 2.46) on boredom. For segment-specific ranges on core negative affect variables, see Figure 1.
Figure 1a-b.
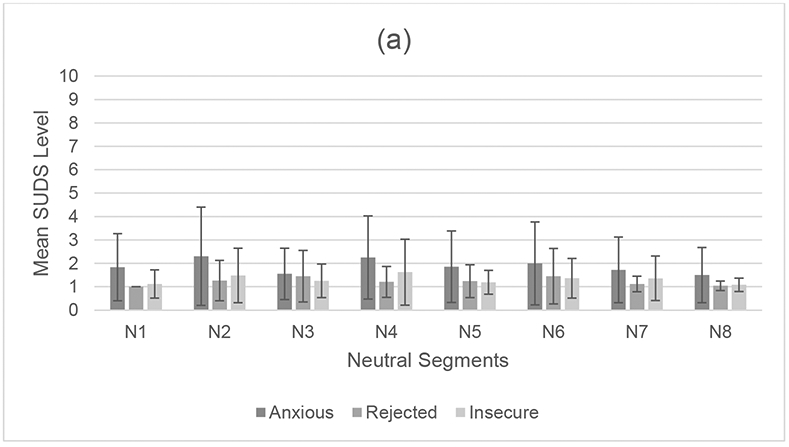
Study 1: Negative emotional responding of the final selected segments across (1a) Neutral and (1b) Rejection conditions. SUDS = Subjective Units of Distress Scale; Numbers paired with ‘N’ or ‘R’ along the X axis correspond to specific segments within the Neutral and Rejection conditions, respectively.
Across the 17 Neutral segments, the mean SUDS values ranged from 1.50-2.73 on anxiety, 1.00-3.10 on rejection, 1.08-4.00 on insecurity, 2.18-4.96 on happiness, 1.96-4.59 on annoyance, and 3.13-4.87 on boredom. The mean realistic ratings ranged from 6.13-8.04. Overall, the Neutral segments were considered reasonably realistic and most did not significantly increase/decrease any affect rating. As we did not want the Neutral condition to increase any of the negative affect responses connected to rejection, we sought segments associated with the lowest/below average feelings of rejection, insecurity and anxiety, as well as average-to-above average feelings of boredom. Thus, segments with an average rejection rating above 1.50 (primary comparator), insecurity rating above 2.00, or anxiety rating above 2.50 were cut (n = 4). Given the distribution of scores, segments with an average boredom rating below 3.50 were cut (n = 1). The remaining segments were ranked by realism ratings and the bottom four (values < 6.60) were cut. The final in eight Neutral segments averaged 1.88 on anxiety (SD = 1.56), 1.22 rejection (SD = 0.73), 1.31 on insecurity (SD = 0.89), 3.76 on happiness (SD = 2.29), 3.14 on annoyance, (SD = 2.55), and 4.10 on boredom (SD = 2.60). For segment-specific ranges on core negative affect variables, see Figure 1.
Stage 2: A-DISS Validation
Participants
College students 18+ years of age were again recruited from an online SONA pool at a large Southwestern university in exchange for course credit. Participants were excluded if they had participated in Study 1. Fifty-two participants aged 18-25 years attended the laboratory visit (See Table 1 for Sample Demographics and Between Group Comparisons across Experimental Conditions).
Table 1.
Study 2 Sample Demographics and Between Group Comparisons across Experimental Conditions
| Variable | Total Sample (n = 52) |
Rejection (n = 26) |
Neutral (n = 26) |
|---|---|---|---|
| Gender n (%) | |||
| Cismen | 20 (38.5%) | 13 (50.0%) | 19 (73.1%) |
| Ciswomen | 32 (61.5%) | 13 (50.0%) | 7 (26.9%) |
| Sexual Orientation n (%) | |||
| Heterosexual | 49 (94.2%) | 26 (100%) | 23 (88.5%) |
| Gay/Lesbian | 2 (3.8%) | 0 | 2 (7.7%) |
| Bisexual | 1 (1.9%) | 0 | 1 (3.8%) |
| Race/Ethnicity n (%) | |||
| Hispanic | 14 (26.9%) | 3 (11.5%) | 11 (42.3%) |
| White | 14 (26.9%) | 8 (30.8%) | 6 (42.9%) |
| Black | 21 (40.4%) | 14 (53.8%) | 7 (26.9%) |
| Asian | 0.0% | 0 | 0 |
| Multiple | 2 (3.8%) | 0 | 2 (7.7%) |
| Other | 1 (1.9%) | 1 (3.8%) | 0 |
| Age M (SD) | 20.40 (1.88) | 20.31 (1.91) | 20.5 (1.88) |
| Social Interaction Anxiety Scale M (SD) | 24.42 (12.75) | 22.15 (12.71) | 26.69 (12.62) |
| 1Center for Epidemiological Studies Depression Scale M (SD) | 14.53 (7.78) | 12.04 (6.39) | 16.92 (8.35) |
| Mental Imagery Engagement M (SD) | 6.65 (2.68) | 6.23 (2.83) | 7.08 (2.50) |
Note: Chi Square and one-way ANOVA tests evaluated whether experimental groups differed on any of the baseline characteristics; variables that were statistically different (p <.05) across groups are bolded.
n= 51 for analyses with depression included as one participant opted not to complete the CESD.
Design & Procedure
As outlined above, the first stage data was used to select the top 8 Rejection and 8 Neutral segments for the second stage (see Supplemental Material for final transcripts; for recordings, contact first author). The content of the selected segments was evaluated and organized in a set presentation order. As before, participants were randomized into conditions (presented by RAs blind to condition assignment), listened to each segment, and provided ‘blind’ emotional reactivity ratings. Unlike before, participants completed a longer baseline questionnaire to assess for potential moderators, provided one- and five-minute post-task emotional reactivity ratings to examine the duration of effects, provided additional task ratings, and did not provide ratings on written transcripts. After the task and before the one-minute rating, participants sat quietly. After the one-minute rating, participants completed post-task questionnaires on their recall of the task instructions/scenario (used as data quality/validity checks), then completed the five-minute post-task rating.
All SUDS data are presented for descriptive and comparative purposes. In addition to testing main effects of condition on acute emotional responding, baseline reported gender, SA, and depression symptoms were tested as potential moderators.
Measures
Acute emotional reactivity and post-task measures (Blinded).
Participants completed the same SUDS items as before (i.e., anxious, rejected, insecure, annoyed, bored, happy), plus ‘angry’, on the same 1 to 9 scale (Gotlib et al., 2005; Wolpe, 1958). All SUDS were assessed immediately pre-task, following each individual segment, and one- and five- minutes post-task. At the end of the task, participants were asked to rate the extent to which they were able to imagine themselves in the scenario on a scale of 1 (not at all) to 10 (very well).
Baseline Measures/Potential Moderators.
In addition to the demographic, data quality, and SA (SIAS α = .89 in current sample) measures described in Stage 1, participants in Stage 2 also reported on their depression symptoms. The Center for Epidemiological Studies Depression Scale (CESD; Radloff, 1977) contains 20-items rated on a 0 (rarely or none of the time [less than 1 day]) to 3 (most of the time [5-7 days]) scale, reflecting how often each of the symptoms occurred within the past week, resulting in a possible sum score range of 0-60. The CESD evidences good internal consistency (e.g., α = .82 in current study) as well as convergent and divergent validity with other measures of depression and anxiety (e.g., Amtmann et al., 2014).
Analytic Approach & Results
Data Quality & Coding.
Two participants failed multiple recall items; however, we elected to retain these cases as a more conservative test of task efficacy under conditions where data quality is not screened/questionable data is not identified (substantive findings do not change with their exclusion). One participant opted not to complete the CESD, but otherwise provided complete data; they were excluded from only the analyses where depression was included as a variable. Participants’ post-task ratings on their ability to imagine themselves in the scenarios were similarly high across conditions (Table 1).
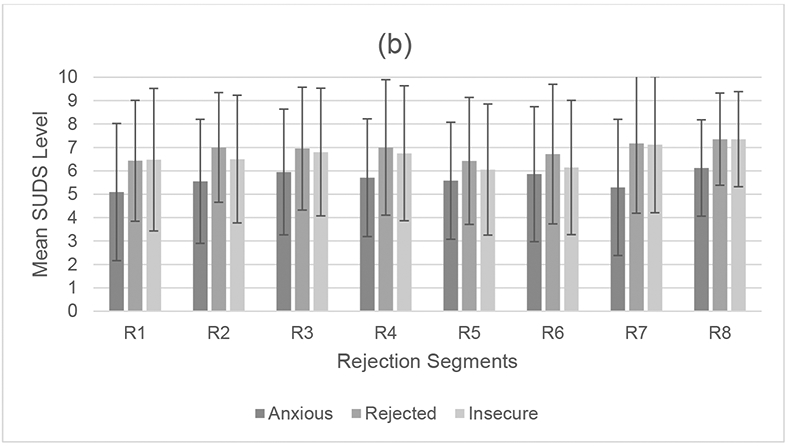
The single item SUDS were used to reflect each emotion at baseline, one-, and five-minute post-task. One-way ANOVAs confirmed no condition differences on any baseline SUDS values (p’s > .05). Within each condition, participants reported similar mean levels of all eight SUDs emotional responses to each segment. As shown in Figure 2, with the exception of the first Rejection segment (R1), all of the remaining Rejection segments (R2-R8) had average rejection and insecurity ratings above 5 and anxiety ratings above 4. With the exception of N4 and N6, all of the Neutral segments had negative affect ratings below 2. Therefore, we took the participants’ average of each SUDS emotion across the eight segments to reflect their “during task response” on that emotion (designated as T1 in Figures 3-4).
Figure 2a-b.
Study 2: Negative emotional responding at the segment level across (2a) Neutral and (2b) Rejection conditions. SUDS = Subjective Units of Distress Scale. Numbers paired with ‘N’ or ‘R’ along the X axis correspond to specific segments within the Neutral and Rejection conditions, respectively.
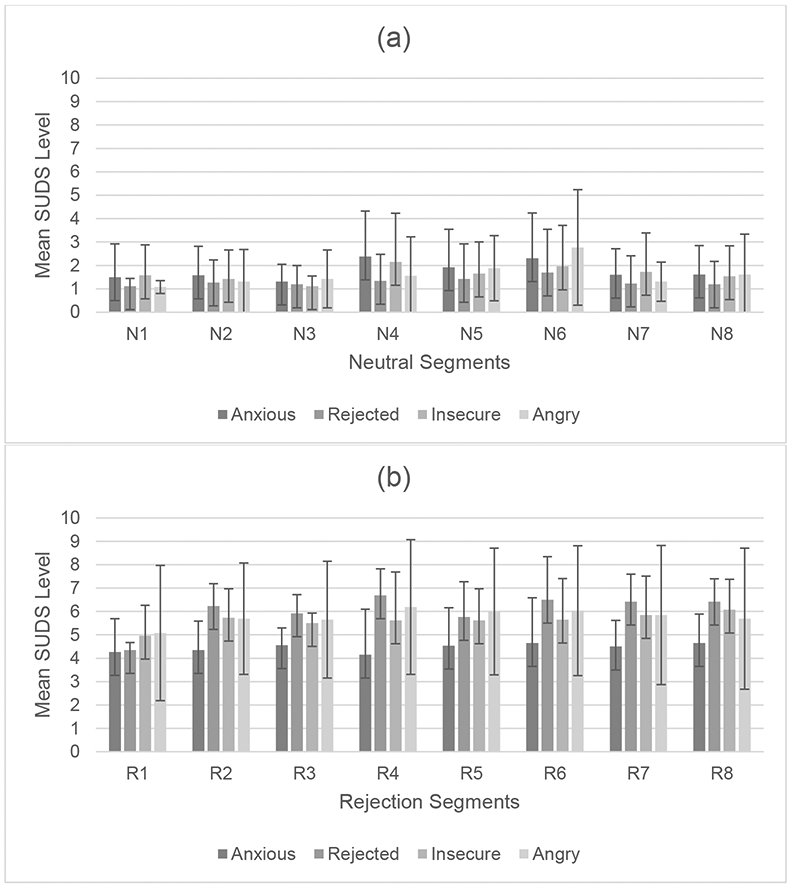
Figure 3a-g.
Condition x time RM ANCOVA predicting Subjective Units of Distress Scale (SUDS) during the task (segment average), one- and five-minute post task (controlling for baseline). Adjusted means and 95% CI are plotted. T1 = during task (segment average); T2 = one-minute post-task; T3 = five-minute post-task.
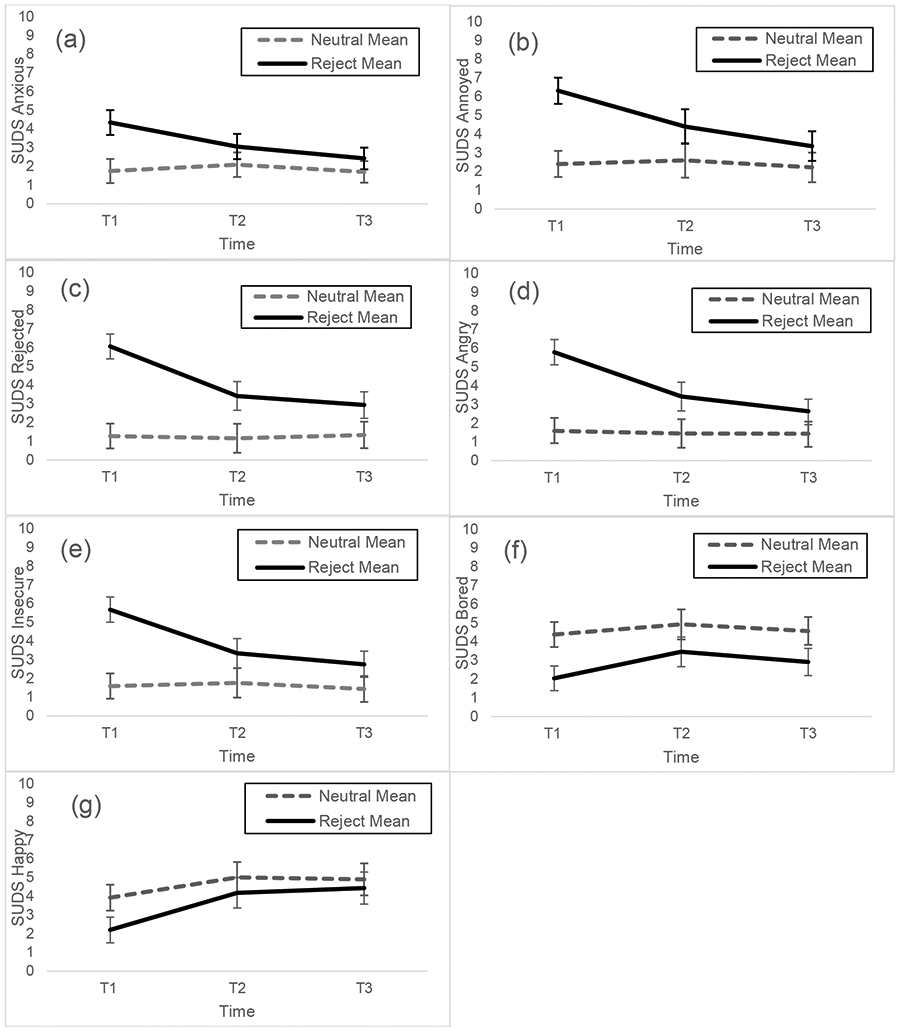
Figure 4a-f.
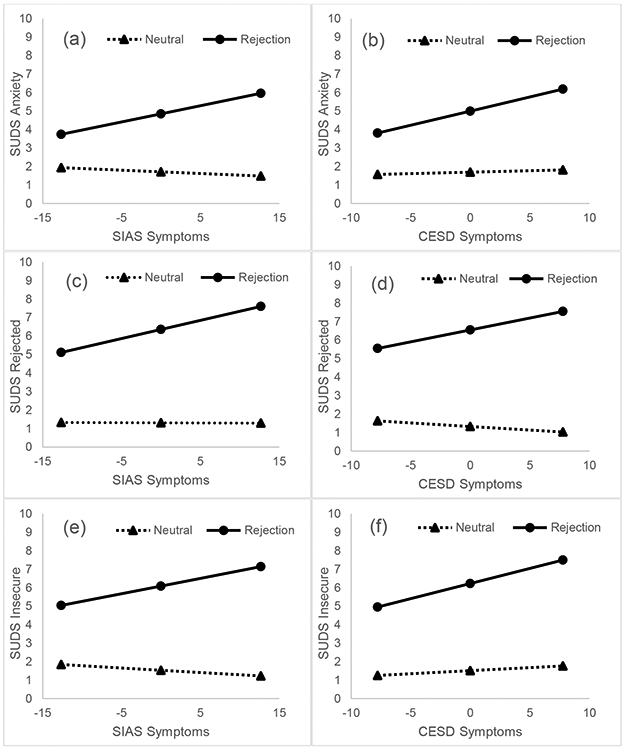
Statistically significant condition x social anxiety (SIAS; 4a,c,e) and condition x depression (CESD; 4b,d,f) regressions predicting relevant task (T1) Subjective Units of Distress Scale (SUDS; segment average) while controlling for baseline values as well as SA and depression symptoms.
A-DISS Condition on Acute Emotional Responding.
A series of repeated measures ANCOVAs with a between-subjects factor (condition) were conducted predicting the acute emotional responses during the task (T1), 1-minute post-task (T2), and 5 minutes post-task (T3) while controlling for baseline values. Significant between-subjects’ effects (condition) on all emotional responses and within-subjects (time) effects for feeling anxious, rejected, insecure, annoyed, and angry (but not bored or happy), were found (Table 2). There were also between x within subjects’ effects on feeling anxious, rejected, insecure, annoyed, and angry, but not happy or bored. Within-subjects contrasts indicated significant condition x time linear effects for feeling anxious, F(1, 48) = 20.79, p < .001, Partial η2 = .30, rejected, F(1, 49) = 31.08, p < .001, Partial η2 = .39, insecure, F(1,49) = 29.44, p < .001, Partial η2 = .38, annoyed, F(1, 49) = 16.78, p < .001, Partial η2 = .26, angry, F(1, 49) = 34.31, p < .001, Partial η2 = .41, and happy, F(1, 49) = 4.60, p = .037, Partial η2 = .09. There were also significant condition x time quadratic effects for feeling rejected, F(1, 49) = 5.93, p = .019, Partial η2 = .11, and insecure, F(1, 49) = 10.24, p = .002, Partial η2 = .17. Neither linear nor quadratic effects were statistically significant for boredom (p’s > .05). Figure 3 depicts the adjusted mean and 95% Confidence Intervals for all of the condition x time effects.
Table 2.
Condition x Time Repeated Measures ANCOVA on Acute Emotional Responding
| SUDS | Between Subjects | Within Subjects | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Condition | Error | Time | Condition x Time | Error | |||||||
| df | F | Partial η2 |
df | df | F | Partial η2 |
df | F | Partial η2 |
df | |
| Anxious | 1 | 13.41 | .22** | 48 | 2 | 4.65 | .09* | 2 | 11.91 | .20*** | 96 |
| Rejected | 1 | 46.24 | .49*** | 49 | 2 | 16.33 | .25*** | 2 | 21.70 | .31*** | 98 |
| Insecure | 1 | 27.09 | .36*** | 49 | 2 | 11.34 | .19*** | 2 | 22.04 | .31*** | 98 |
| Angry | 1 | 38.69 | .44*** | 49 | 2 | 18.76 | .28*** | 2 | 15.97 | .25*** | 98 |
| Annoyed | 1 | 22.91 | .32*** | 49 | 2 | 6.65 | .12** | 2 | 11.05 | .18*** | 98 |
| Happy | 1 | 4.10 | .08* | 49 | 2 | 0.81 | .02 | 2 | 2.93 | .06 | 98 |
| Bored | 1 | 16.28 | .25*** | 48 | 2 | 1.70 | .03 | 2 | 1.81 | .04 | 96 |
Note. SUDS = Subjective Units of Distress Scale.
p < .05.
p < .01.
p < .001.
Criterion & Discriminant Validity for Rejection.
During the task (T1; Figure 3), the Rejection condition was associated with increased negative affect (anxiety, rejection, insecurity, annoyance, and anger), decreased positive affect (happiness), and decreased boredom levels. One minute after the task (T2), Rejected participants continued to report elevated feelings of rejection and anger (but not other negative affect) compared to the Neutral condition. Rejected participants also reported elevations in feeling happy and bored relative to T1, but not as happy or bored as those in the Neutral condition at the same timepoint.
Criterion & Discriminant Validity for Neutral.
Neutral condition participants did not evidence any statistically significant increases on any emotion during or after the task. Overall, the Neutral condition reported stable, or slightly (but not statistically significant) lower, negative emotions compared to baseline levels.
Task Recovery.
Five minutes after the task (T3), participants returned to their conditions’ respective baseline mean and generally had similar means to each other. The only exception was boredom – where those in the Neutral condition reported higher levels than those in the Rejection condition.
Generalizability.
A series of 2 (Condition) x 2 (Gender) ANCOVAs tested for gender differences on task emotions (T1) controlling for baseline levels. There were no main nor interaction effects of gender on any acute emotions (p’s > .05); as such, no additional data are reported. A post-hoc 2 (Condition) x 3 (Race/Ethnicity) ANCOVA tested for differences on task emotions (T1) controlling for baseline levels among participants who identified as White, Black, or Hispanic (see Table 1 for identity distributions across condition). There were no main nor interaction effects of race/ethnicity on any acute emotions (p’s > .05); as such, no additional data are reported.
Differential Emotional Responding (Condition x SA/Depression Symptoms).
A series of regressions were conducted using Model 1 of the SPSS 26.0 PROCESS Macro (Hayes, 2018). Relevant task SUDS (T1) were specified as the outcome with the Condition x symptoms as the primary predictor, while controlling for main effects of Condition, SIAS scores, and CESD scores as well as baseline SUDS levels. All continuous variables were mean centered to ease interpretations of the plots. As main effects of Condition remained significant across analyses, only moderation effects are discussed below. Figure 4 depicts estimated means for statistically significant effects.
To examine SA, a series of regressions were conducted for SIAS on task (T1) anxiety, rejection, insecurity, angry, and annoyed controlling for baseline levels of that same emotion, main effects, and CESD scores. Analyses indicated significant SA x Condition moderation effects on T1 anxiety, F(5,45) = 14.27, p < .001, R2 = .61, T1 rejection, F(5,45) = 30.04, p < .001, R2 = .77, and T1 insecurity, F(5,45) = 26.30, p < .001, R2 = .75. Of the total variance, the interaction terms specifically accounted for 8.3% variance in T1 anxiety, 4.3% variance in T1 rejection, and 5.8% variance in T1 insecurity. Among those in the Rejection condition only, those with greater SA became more anxious, rejected, and insecure than those with below average SA. While the overall models were statistically significant, there were no main nor moderation effects of SA on feeling angry or annoyed (p’s >.05).
To examine depression, a series of regressions were conducted for CESD on task (T1) anxiety, rejection, insecurity, anger, and annoyance while controlling for SIAS scores. Analyses indicated a statistically significant moderation of depression on T1 anxiety, F(5,45) = 12.15, p < .001, R2 = .58, T1 rejection, F(5,45) = 29.00, p < .001, R2 = .76, and T1 insecurity, F(5,45) = 22.36, p < .001, R2 = .71. Of the total variance, the interaction terms specifically accounted for 4.3% variance in T1 anxiety, 3.6% variance in T1 rejection, and 2.6% variance in T1 insecurity. Within the Rejection condition alone, those with greater depression reported feeling more anxious, rejected, and insecure than those with below average depression. While the overall models were statistically significant, there were no main or moderation effects of depression on feeling angry or annoyed (p’s >.05).
Discussion
The aim of the present study was to develop and validate a social rejection task to clarify the distinct and transdiagnostic mechanisms of SA and depression. From the outset, the task needed to effectively elicit relevant emotional responses (e.g., anxiety, rejection, insecurity), include a comparable control condition, be realistic, and feasible for most researchers. Preliminary findings support the reliability, validity, and perceived realism of the A-DISS as well as the ability for participants to imagine themselves in both conditions. The Rejection condition segments successfully and consistently elicited greater negative affect (rejection, anxiety, insecurity, annoyance, anger) compared to baseline values and the Neutral condition segments. The Neutral condition evidenced stable affect levels across time. These effects were consistent across gender and the major racial/ethnic categories represented in our sample (White, Black, Hispanic). As expected, participants with elevated SA randomized to the Rejection condition reported greater rejection, insecurity, and anxiety. Participants with elevated depression also reported greater rejection and insecurity. Unexpectedly, participants with elevated depression also reported elevated anxiety, but not anger, during the Rejection condition. As SA and depression symptoms were both included as covariates in testing for moderating effects, the interaction terms reflect the unique variance accounted for above and beyond main effects or co-occurring symptoms. Overall, findings provide preliminary validation data for the A-DISS as a novel peer rejection task that sheds light on some of the transdiagnostic vulnerabilities associated with SA and depression.
Findings with the A-DISS replicate effects suggested by theory and existing rejection tasks (e.g., Blackhart et al., 2009) and extends the existing work in critical ways. The Neutral and Rejection conditions effectively elicited affective reactions across two studies, providing strong initial support for the internal validity of the task. We extend previous research by using a matched Neutral condition where participants imagined the same scenario, in the same social setting, where similar negative language was used to talk about a teacher (i.e., language was relevant other- rather than self-focused). The Neutral condition controls for important conceptual (e.g., social setting) and methodological (e.g., time, instructions) confounds present in other experimental manipulations of rejection. Effects were driven entirely by response to Rejection specifically, rather than features of the A-DISS manipulation broadly (e.g., imagining oneself at a party) or competing effects driven by the Neutral condition response (e.g., decreased negative affect that could result from acceptance). Consistent with other work, the current findings also show that the affective reactions to, and recoveries from, rejection were multidimensional and occurred on different timescales (e.g., Zadro et al., 2006), highlighting the importance of examining affective responses beyond positive and negative response types.
SA moderated the effects of rejection on the A-DISS on acute anxiety, rejection, and insecurity, consistent with prior work and theory indicating that individuals with SA are more vulnerable to perceived rejection (e.g., Bautista & Hope, 2015; Levinson, Langer, & Rodebaugh, 2013; Spence & Rapee, 2016). Individuals high in SA report greater anxiety and negative cognitions about themselves in response to negative feedback and display a more pronounced attentional bias toward negative social cues than those low in SA (Bautista & Hope, 2015). Taken together, these results suggest one path wherein SA symptoms may be maintained: exaggerated reactivity to social rejection may strengthen fears of rejection, leading to an increase in social avoidance and a decrease in social skills practice, further maintaining symptoms of SA, potentiating reactivity, and increasing the possibility of rejection in the future. As this specific pathway was not tested in the current study, future research is needed. For example, future studies could examine whether cognitions related to fear of rejection mediate the associations between SA and social avoidance or withdrawal.
Findings for depression only partially supported prior work and theory (Platt, Kadosh, & Lau, 2013; Seidl et al., 2020; Slavich et al., 2010). Individuals with elevated depression felt more rejected, insecure, and anxious after the Rejection condition compared to those with low depression or those exposed to the Neutral condition. Repeated exposure to rejection paired with greater sensitivity to rejection may account for the development and maintenance of depressive symptoms (e.g., social withdrawal; negative cognitions of self-worth); in turn, depression symptoms may also increase rejection experiences and perpetuate into ever increasing problems (Kupferberg et al., 2016; Platt et al., 2013; Slavich et al., 2010). That depression was associated with anxiety, even after controlling for SA symptoms, suggests a greater convergence in affective experiences during acute states of rejection than expected (see Eysenck & Fajkowska, 2017). That depression was not associated with anger or annoyance during Rejection in spite of prior work showing these effects (e.g., Jobst et al., 2015), could be a function of differing methodologies (e.g., Cyberball vs. A-DISS) or gender compositions in study samples (e.g., 70% men in Jobst et al., 2015 vs. 62% ciswomen in Study 2). Prior work has noted that men who adhere to traditional gender norms and display externalizing behavior, such as anger, are at greater risk for depression and are more prone to reporting anger/resentment in response to Rejection, whereas women are more prone to internalizing responses such as anxiety (Genuchi, 2015; Jobst et al., 2015). Our sample size was too small to test possible three-way interactions across gender, symptoms, and condition or more complex models that considers intersecting identities (e.g., race/ethnicity and gender; Vargas, Huey, & Miranda, 2020). Future work should directly test this in larger samples adequately powered to do so.
The A-DISS differs from other rejection tasks in important ways. The most commonly used tasks in the field are not feasible in most research settings due to cost, staffing, and time (e.g., Yale Interpersonal Stressor; Stroud et al., 2000) or lack a socially-oriented Neutral condition and have questionable ecological validity (Cyberball; Williams et al., 2000). Less commonly used tasks that we are aware of address some, but not all, of these issues. For example, the Island Getaway Task is engaging, computerized, and involves negative peer feedback; however, it is contextualized as a game and the social-oriented comparison conditions are not neutral (Funkhouser et al., 2018; Kujawa, Arfer, Klein, & Proudfit, 2014). The recently developed Behind Your Back (Cole et al., 2014) task for adolescents is similar to the Rejection condition of the A-DISS; however, to our knowledge it has not been validated with young adults, includes only mean/rejection content, and differs on the level of imagined engagement. The A-DISS is most similar to the ATSS paradigm overheard conversation and teaching assistant tapes (Davison et al., 1984; 1997), but differs largely in terms of purpose (i.e., mood induction procedure vs. stimulating certain cognitions and qualitatively coding content), specific content, and standardization. The use of a Neutral condition that was procedurally and conceptually identical to the Rejection condition (i.e., in both cases overhearing people talking at a party) was designed to minimize methodological biases. Prior studies where the social stressor (e.g., giving a speech) and neutral conditions (e.g., reading a magazine) differ both procedurally (e.g., the extent to which the participant has to actively do something; Buckner et al., 2011) and conceptually (e.g., giving a speech is clearly a social context whereas reading a magazine alone has no clear social components to it), confounds the extent to which social stress or rejection is eliciting real-time symptoms, rather than social context or stress more broadly. Having a teacher (c.f., themselves) as the target of the conversation was designed to provide a meaningful control with similar content that most adolescent/young adult participants could connect to, while also minimizing the potential perception of rejection. Whereas tasks like Cyberball attempt to extinguish the less tangible features of the social context to avoid any potential confounds (e.g., physical setting; verbal cues), the A-DISS attempts to model some of the features of the social context to improve the generalizability of findings to populations at high risk for SA and depression (adolescents/young adults in school). Nevertheless, tailoring the Neutral content in this way does make the task less generalizable to other samples and contexts (e.g., non-college attending young adults); researchers seeking to use both conditions of the A-DISS in different populations may consider incorporating other conversation targets and contexts in the Neutral scripts that are developmentally/contextually relevant (e.g., employers for non-college attending young adults). Ultimately, researchers may find the A-DISS more or less preferable to that of existing rejection tasks based on conceptual (e.g., the party setting), methodological (e.g., online administration), or feasibility (e.g., software access) concerns.
The current study should be considered in light of several limitations. Although these data offer preliminary support for a fairly generalizable sample of young college students, future validation work with adolescents is needed. As a preliminary test, we did not select participants for specific levels of clinical symptoms nor exclude for any comorbidities which may have attenuated or conflated the effects of SA and depression. We also did not measure participants’ prior experiences of rejection, which may have influenced their interpretations and responses to the A-DISS while also being confounded with their current level of SA or depression symptoms (Blöte, Kint, & Westenberg, 2007; Erath, Flanagan, & Bierman, 2007; Gazelle & Ladd, 2003). In designing the A-DISS scripts, we further sought to balance the need to attenuate the possible effects of gendered language to achieve internal validity, while also acknowledging that gender dynamics are not standardized in daily life and contribute to differential experiences of rejection, SA, and depression (Akibar, Niemann, Blumenthal, & Vosvick, 2019). For example, as shown in the Supplemental Materials, the actors read identical lines for the recordings designated for men and women across conditions. The exception to this were the final two Rejection segments where one actor taunts the other about being attracted to the participant. As we expected the majority of participants to more easily and closely identify with a heteronormative culture, the lines were swapped so that the male voice actor was taunted about their attraction to participants identified as women, while the female voice actor was taunted about their attraction to participants identified as men. In the current study, 0% of participants self-identified as a gender minority and the three cases who identified as a sexual minority were randomly assigned to the Neutral condition which precluded us from exploring these dynamics further. However, considering the use of gender pronouns in laboratory tasks and measures as well as the impact on real-time responding is an important avenue for future research (Cloutier, Dunham, Cochrane, & Blumenthal, in press; Lindner, Martell, Bergstrom, Andersson, & Carlbring, 2013). Finally, we conducted relatively intense assessments across an ~10-minute period. Some work has noted that the strongest effects of rejection on affect may be delayed following a period of rumination (Blackhart et al., 2009). As such, studies with longer post-task assessment periods are warranted.
The current study offers preliminary findings that may inform a breadth of methodologically and clinically innovative research. Methodologically, future work could consider incorporating additional contextual cues (e.g., video/picture of a party scene) and task-specific moderators (e.g., specifying relationships to the voice actors) into the manipulations, collecting physiological data to examine parallel physiological processes (e.g., increased skin conductance, heart rate, cortisol), or conducting multi-level models on segment level data to better quantify rejection reactivity (Bilsky, Cloutier, Bynion, Feldner, & Leen-Feldner, 2018; Cole et al., 2014; Litt & Stock, 2011; Teunissen et al., 2012; Venturini et al., 2016). Additional work could also employ within subjects designs as well as focus on other features of validity and examine specific clinical targets such as vividness, engagement, negative appraisals, and post-task rumination (Cole, Zelkowitz, Nick, Lubarsky, & Rightsm 2019; Holmes & Matthews, 2010; Lackner & Fresco, 2016; Scheveneels, Boddez, Vervliet, & Hermans, 2016). Such efforts might incorporate clinical or transdiagnostic assessments to identify converging and diverging features of task reactivity while clarifying or ruling out comorbidities (Conway, Starr, Espejo, Brennan, & Hammen, 2016; Stanton, McDonnell, Hayden, & Watson, 2020). Given the broad theoretical relevance of rejection to other emerging problems (e.g., substance use), research examining the extent to which reactivity to laboratory-induced rejection is associated with concurrent and long-term problems is a particularly promising area (Blumenthal, Cloutier, Douglas, Kearns, & Carey, under review; Cloutier, Blumenthal, Trim, Douglas, & Anderson, 2019; Lakin, Chartrand, & Arkin, 2008). Lastly, although findings were consistent across study samples with differing racial/ethnic backgrounds as well as in the post-hoc explorations of White, Black, and Hispanic identities as moderators, studies with larger, more diverse samples are needed to directly test for generalizability and consider potential cultural differences (Gerrard et al., 2014).
Clinical Implications
Our work, in conjunction with past findings, suggests that effective SA and depression treatments may share a broad overarching structure (e.g., cognitive behavioral therapies) that target similar affective reactions elicited by social rejection (Epkins & Heckler, 2011; Garber & Weersing, 2010). Individuals experiencing elevated SA, depression, or both may benefit from reducing anxious arousal, restructuring maladaptive cognitions, and increasing behavioral engagement in response to social rejections. These findings suggest that tailoring broad evidence-based approaches to target specific affective reactions to transdiagnostic stressors may improve outcomes for individuals with SA and depression symptoms.
Supplementary Material
Acknowledgments:
The authors would like to thank Kinsie Dunham, Laura Jamison, Patrick Melugin, Erik Tristan, and all of the other members of the Teen Stress and Alcohol Research Laboratory at the University of North Texas for their early contributions to this study.
Funding:
Research supported by: R. Cloutier was partially supported by a National Institute of Health National Research Service Award (1F31DA041105) while at the University of North Texas (presently at the Pennsylvania State University where she is now supported by T32DA017629). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Abbreviations:
- A-DISS
Audio – Dialogue Inductions of Social Stress
- SA
social anxiety
Footnotes
Publisher's Disclaimer: This Author Accepted Manuscript is a PDF file of an unedited peer-reviewed manuscript that has been accepted for publication but has not been copyedited or corrected. The official version of record that is published in the journal is kept up to date and so may therefore differ from this version.
Conflict of interest
Renee Cloutier, Sarah Bilsky, Catherine Baxley, Kristen Anderson, and Heidemarie Blumenthal declare that they have no conflicts of interest.
Ethics Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Approval was granted by the Ethics Committee of the University of North Texas on August 29, 2016 (IRB# 16-336).
Informed Consent
Informed consent was obtained from all individual subjects participating in the study.
Animal Rights
No animal studies were carried out by the authors for this article.
References
- Akibar A, Niemann YF, Blumenthal H, & Vosvick M (2019). Dimensions of sexuality and social anxiety in emerging adulthood. Journal of Gay & Lesbian Mental Health, 23(2), 244–266. [Google Scholar]
- Amir N, Beard C, & Bower E (2005). Interpretation bias and social anxiety. Cognitive Therapy and Research, 29(4), 433–443. 10.1007/s10608-005-2834-5 [DOI] [Google Scholar]
- Amtmann D, Kim J, Chung H, Bamer AM, Askew RL, Wu S, … & Johnson KL (2014). Comparing CESD-10, PHQ-9, and PROMIS depression instruments in individuals with multiple sclerosis. Rehabilitation Psychology, 59(2), 220–229. 10.1037/a0035919 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Asher M, Asnaani A, & Aderka IM (2017). Gender differences in social anxiety disorder: A review. Clinical Psychology Review, 56, 1–12. https://doi-org.umiss.idm.oclc.org/10.1016/j.cpr.2017.05.004 [DOI] [PubMed] [Google Scholar]
- Audacity Team (2019). Audacity(R): Free Audio Editor and Recorder [Computer application]. Version 2.3.2 retrieved May 20th 2019 from https://audacityteam.org/ [1]. [Google Scholar]
- Bacon AK, Cranford AN, & Blumenthal H (2015). Effects of ostracism and sex on alcohol consumption in a clinical laboratory setting. Psychology of Addictive Behaviors, 29(3), 664–672. 10.1037/adb0000054 [DOI] [PubMed] [Google Scholar]
- Bautista C, & Hope D (2015). Fear of negative evaluation, social anxiety and response to positive and negative online social cues. Cognitive Therapy & Research, 39(5), 658–668. 10.1007/s10608-015-9687-3 [DOI] [Google Scholar]
- Blackhart GC, Nelson BC, Knowles ML, & Baumeister RF (2009). Rejection elicits emotional reactions but neither causes immediate distress nor lowers self-esteem: A meta-analytic review of 192 studies on social exclusion. Personality and Social Psychology Review, 13(4), 269–309. 10.1177/1088868309346065 [DOI] [PubMed] [Google Scholar]
- Blöte AW, Kint MJW, & Westenberg PM (2007). Peer behavior toward socially anxious adolescents: Classroom observations. Behaviour Research and Therapy, 45(11), 2773–2779. https://doi-org.umiss.idm.oclc.org/10.1016/j.brat.2007.06.011 [DOI] [PubMed] [Google Scholar]
- Blumenthal H, Cloutier RM, Douglas ME, Kearns NT, & Carey CN (Under Review). Desire to drink as a function of laboratory-induced social stress among adolescents. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown EJ, Turovsky J, Heimberg RG, Juster HR, Brown TA, & Barlow DH (1997). Validation of the Social Interaction Anxiety Scale and the Social Phobia Scale across the anxiety disorders. Psychological Assessment, 9(1), 21–27. 10.1037/1040-3590.9.1.21 [DOI] [Google Scholar]
- Bruce SE, Yonkers KA, Otto MW, Eisen JL, Weisberg RB, Pagano M, … Keller MB (2005). Influence of psychiatric comorbidity on recovery and recurrence in generalized anxiety disorder, social phobia, and panic disorder: A 12-year prospective study. American Journal of Psychiatry, 162(6), 1179–1187. https://doi-org.umiss.idm.oclc.org/10.1176/appi.ajp.162.6.1179 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bilsky SA, Cloutier RM, Bynion T, Feldner MT, & Leen-Feldner EW (2018). An experimental test of the impact of adolescent anxiety on parental sick role reinforcement behavior. Behavior Research and Therapy 109, 37–48. 10.1016/j.brat.2018.07.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cloutier RM, Blumenthal H, Trim RS, Douglas ME, & Anderson KG (2019). Real-time social stress response and subsequent alcohol use initiation among female adolescents. Psychology of Addictive Behaviors, 3(33), 254–265. 10.1037/adb0000454 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cloutier RM, Dunham KJ, Cochrane B, & Blumenthal H Beyond the binary: A ‘real world’ example to inform identity-affirming laboratory methods with substance using youth. In Press. [Google Scholar]
- Cole DA, Martin NC, Sterba SK, Sinclair-McBride K, Roeder KM, Zelkowitz R, & Bilsky SA (2014). Peer victimization (and harsh parenting) as developmental correlates of cognitive reactivity, a diathesis for depression. Journal of Abnormal Psychology, 123(2), 336–349. https://doi-org.umiss.idm.oclc.org/10.1037/a0036489.supp (Supplemental) [DOI] [PubMed] [Google Scholar]
- Cole DA, Zelkowitz RL, Nick EA, Lubarsky SR, & Rights JD (2019). Simultaneously examining negative appraisals, emotion reactivity, and cognitive reactivity in relation to depressive symptoms in children. Development and Psychopathology, 31(4), 1527–1540. 10.1017/s0954579418001207 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conway CC, Starr LR, Espejo EP, Brennan PA, & Hammen C (2016). Stress responsivity and the structure of common mental disorders: Transdiagnostic internalizing and externalizing dimensions are associated with contrasting stress appraisal biases. Journal of Abnormal Psychology, 125(8), 1079. doi: 10.1037/abn0000163 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coyne JC (1976). Depression and the response of others. Journal of Abnormal Psychology, 85, 186–193. 10.1037//0021-843X.85.2.186. [DOI] [PubMed] [Google Scholar]
- Cuthbert BN, & Kozak MJ (2013). Constructing constructs for psychopathology: The NIMH research domain criteria. Journal of Abnormal Psychology, 122, 928–937. 10.1037/a0034028 [DOI] [PubMed] [Google Scholar]
- Davison GC, Feldman PM, & Osborn CE (1984). Articulated thoughts, irrational beliefs, and fear of negative evaluation. Cognitive Therapy and Research, 8(4), 349–362. 10.1007/BF01173310 [DOI] [Google Scholar]
- Davison GC, & Zighelboim V (1987). Irrational beliefs in the articulated thoughts of college students with social anxiety. Journal of Rational Emotive Therapy, 5(4), 238–254. 10.1007/BF01073815 [DOI] [Google Scholar]
- Epkins CC & Heckler DR (2011). Integrating etiological models of social anxiety and depression in youth: Evidence for a cumulative interpersonal risk model. Clinical Child and Family Psychology Review, 14(4), 329–376. https://doi-org.umiss.idm.oclc.org/10.1007/s10567-011-0101-8 [DOI] [PubMed] [Google Scholar]
- Erath SA, Flanagan KS, & Bierman KL (2007). Social anxiety and peer relations in early adolescence: Behavioral and cognitive factors. Journal of Abnormal Child Psychology, 35(3), 405–416. 10.1007/s10802-007-9099-2 [DOI] [PubMed] [Google Scholar]
- Eysenck MW, & Fajkowska M (2017). Anxiety and depression: Toward overlapping and distinctive features. Cognition and Emotion, 37(7), 1391–1400. 10.1080/02699931.2017.1330255 [DOI] [PubMed] [Google Scholar]
- Funkhouser CJ, Auerbach RP, Kujawa A, Morelli SA, Phan KL, & Shankman SA (2018). Social feedback valence differentially modulates the reward positivity, P300, and late positive potential. Journal of Psychophysiology. doi.org/ 10.1027/0269-8803/a000253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garber J, & Weersing VR (2010). Comorbidity of Anxiety and Depression in Youth: Implications for Treatment and Prevention. Clinical psychology: A publication of the Division of Clinical Psychology of the American Psychological Association, 17(4), 293–306. 10.1111/j.1468-2850.2010.01221.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gazelle H, & Ladd GW (2003). Anxious solitude and peer exclusion: A diathesis–stress model of internalizing trajectories in childhood. Child Development, 74(1), 257–278. 10.1111/1467-8624.00534 [DOI] [PubMed] [Google Scholar]
- Genuchi M (2015). Anger and hostility as primary externalizing features of depression in college men. International Journal of Men's Health, 14(2), 113–128. 10.3149/jmh.1402.113 [DOI] [Google Scholar]
- Gotlib IH, Traill SK, Montoya RL, Joormann J, & Chang K (2005). Attention and memory biases in the offspring of parents with bipolar disorder: Indications from a pilot study. Journal of Child Psychology and Psychiatry, 46(1), 84–93. 10.1111/j.1469-7610.2004.00333.x [DOI] [PubMed] [Google Scholar]
- Hammen C (2006). Stress generation in depression: Reflections on origins, research, and future directions. Journal of Clinical Psychology, 62, 1065–1082. 10.1002/jclp.20293 [DOI] [PubMed] [Google Scholar]
- Hayes AF (2018). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach (2nd Ed.) New York: The Guilford Press. [Google Scholar]
- Heimberg RG, Mueller GP, Holt CS, Hope DA, & Liebowitz MR (1992). Assessment of anxiety in social interaction and being observed by others: The Social Interaction Anxiety Scale and the Social Phobia Scale. Behavior Therapy, 23(1), 53–73. 10.1016/S0005-7894(05)80308-9 [DOI] [Google Scholar]
- Holmes EA, & Mathews A (2010). Mental imagery in emotion and emotional disorders. Clinical Psychology Review, 30(3), 349–362. https://doi-org.umiss.idm.oclc.org/10.1016/j.cpr.2010.01.001 [DOI] [PubMed] [Google Scholar]
- Jobst A, Sabass L, Palagyi A, Bauriedl-Schmidt C, Mauer MC, Sarubin N, … & Padberg F (2015). Effects of social exclusion on emotions and oxytocin and cortisol levels in patients with chronic depression. Journal of Psychiatric Research, 60, 170–177. 10.1016/j.jpsychires.2014.11.001 [DOI] [PubMed] [Google Scholar]
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, & Walters EE (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 593–602. https://doi-org.umiss.idm.oclc.org/10.1001/archpsyc.62.6.593 [DOI] [PubMed] [Google Scholar]
- Kessler RC, Chiu WT, Demler O, & Walters EE (2005). Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 617–627. https://doi-org.umiss.idm.oclc.org/10.1001/archpsyc.62.6.617 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kessler RC, & Wang PS (2008). The descriptive epidemiology of commonly occurring mental disorders in the United States. Annual Review of Public Health, 29, 115–129. 10.1146/annurev.publhealth.29.020907.090847. [DOI] [PubMed] [Google Scholar]
- Klemanski DH, Curtiss J, McLaughlin KA, & Nolen-Hoeksema S (2017). Emotion regulation and the transdiagnostic role of repetitive negative thinking in adolescents with social anxiety and depression. Cognitive Therapy and Research, 41(2), 206–219. https://doi-org.umiss.idm.oclc.org/10.1007/s10608-016-9817-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kraines MA, White EJ, Grant DM, & Wells TT (2019). Social anxiety as a precursor for depression: Influence of interpersonal rejection and attention to emotional stimuli. Psychiatry Research, 275, 296–303. https://doi-org.umiss.idm.oclc.org/10.1016/j.psychres.2019.04.001 [DOI] [PubMed] [Google Scholar]
- Kujawa A, Arfer KB, Klein DN & Proudfit GH (2014). Electrocortical reactivity to social feedback in youth: A pilot study of the Island Getaway task. Developmental Cognitive Neuroscience, 10, 140–147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kupferberg A, Bicks L & Hasler G (2016). Social functioning in major depressive disorder. Neuroscience & Biobehavioral Reviews, 69, 313–332. 10.1016/j.neubiorev.2016.07.002 [DOI] [PubMed] [Google Scholar]
- Lackner RJ, & Fresco DM (2016). Interaction effect of brooding rumination and interoceptive awareness on depression and anxiety symptoms. Behaviour Research and Therapy, 85, 43–52. 10.1016/j.brat.2016.08.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lakin JL, Chartrand TL, & Arkin RM (2008). I am too just like you: Nonconscious mimicry as an automatic behavioral response to social exclusion. Psychological Science, 19(8), 816–822. 10.1111/j.1467-9280.2008.02162.x [DOI] [PubMed] [Google Scholar]
- Levinson CA, Langer JK, & Rodebaugh TL (2013). Reactivity to exclusion prospectively predicts social anxiety symptoms in young adults. Behavior Therapy, 44(3), 470–478. 10.1016/j.beth.2013.04.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewinsohn PM, Seeley JR, Roberts RE, & Allen NB (1997). Center for Epidemiologic Studies Depression Scale (CESD) as a screening instrument for depression among community-residing older adults. Psychology and Aging, 12(2), 277–287. 10.1037/0882-7974.12.2.277 [DOI] [PubMed] [Google Scholar]
- Lindner P, Martell C, Bergstr€om J, Andersson G, & Carlbring P (2013). Clinical validation of a non-heteronormative version of the Social Interaction Anxiety Scale (SIAS). Health and Quality of Life Outcomes, 11(1), 1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Litt DM, & Stock ML (2011). Adolescent alcohol-related risk cognitions: The roles of social norms and social networking sites. Psychology of Addictive Behaviors, 25, 708–713. 10.1037/a0024226 [DOI] [PubMed] [Google Scholar]
- Mattick RP, & Clarke JC (1998). Development and validation of measures of social phobia scrutiny fear and social interaction anxiety. Behaviour Research and Therapy, 36(4), 455–470. 10.1016/s0005-7967(97)10031-6 [DOI] [PubMed] [Google Scholar]
- McKnight PE, Monfort SS, Kashdan TB, Blalock DV, & Calton JM (2016). Anxiety symptoms and functional impairment: A systematic review of the correlation between the two measures. Clinical Psychology Review, 45, 115–130. 10.1016/j.cpr.2015.10.005 [DOI] [PubMed] [Google Scholar]
- McLaughlin KA & Nolen-Hoeksema S (2012). Interpersonal stress generation as a mechanism linking rumination to internalizing symptoms in early adolescents. Journal of Clinical Child and Adolescent Psychology, 41(5), 584–597. https://doi-org.umiss.idm.oclc.org/10.1080/15374416.2012.704840 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nezlek JB, Kowalski RM, Leary MR, Blevins T, & Holgate S (1997). Personality moderators of reactions to interpersonal rejection: Depression and trait self-esteem. Personality and Social Psychology Bulletin, 23(12), 1235–1244. https://doi-org.umiss.idm.oclc.org/10.1177/01461672972312001 [Google Scholar]
- Nolen-Hoeksema S (2001). Gender differences in depression. Current Directions in Psychological Science, 10(5), 173–176. 10.1111/1467-8721.00142 [DOI] [Google Scholar]
- Oaten M, Williams KD, Jones A & Zadro L (2008). The effects of ostracism on self-regulation in the socially anxious. Journal of Social and Clinical Psychology, 27(5), 471–504. https://doi-org.umiss.idm.oclc.org/10.1521/jscp.2008.27.5.471 [Google Scholar]
- Platt B, Kadosh KC & Lau JY (2013). The role of peer rejection in adolescent depression. Depression and Anxiety, 30(9), 809–821. 10.1002/da.22120 [DOI] [PubMed] [Google Scholar]
- Radloff LS (1977). The CESD scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1(3), 385–401. 10.1177/014662167700100306 [DOI] [Google Scholar]
- Rapee RM, & Spence SH (2004). The etiology of social phobia: Empirical evidence and an initial model. Clinical Psychology Review, 24(7), 737–767. 10.1016/j.cpr.2004.06.004 [DOI] [PubMed] [Google Scholar]
- Roberts KE, Hart TA, & Eastwood JD (2010). Attentional biases to social and health threat words in individuals with and without high social anxiety or depression. Cognitive Therapy and Research, 34(4), 388–399. https://doi-org.umiss.idm.oclc.org/10.1007/s10608-009-9245-y [Google Scholar]
- Scheveneels S, Boddez Y, Vervliet B, & Hermans D (2016). The validity of laboratory-based treatment research: Bridging the gap between fear extinction and exposure treatment. Behaviour Research and Therapy, 86, 87–94. [DOI] [PubMed] [Google Scholar]
- Sheeber LB, Allen NB, Leve C, Davis B, Shortt JW, & Katz LF (2009). Dynamics of affective experience and behavior in depressed adolescents. Journal of Child Psychology and Psychiatry and Allied Disciplines, 50(11), 1419–1427. 10.1111/j.1469-7610.2009.02148.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seidl E, Padberg F, Bauriedl-Schmidt C, Albert A, Daltrozzo T, Hall J, … Jobst A (2020). Response to ostracism in patients with chronic depression, episodic depression and borderline personality disorder: A study using Cyberball. Journal of Affective Disorders. 10.1016/j.jad.2019.09.021 [DOI] [PubMed] [Google Scholar]
- Slavich GM, O’Donovan A, Epel ES & Kemeny ME (2010). Black sheep get the blues: A psychobiological model of social rejection and depression. Neuroscience and Biobehavioral Reviews, 35(1), 39–45. 10.1016/j.neubiorev.2010.01.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spence SH, & Rapee RM (2016). The etiology of social anxiety disorder: An evidence-based model. Behaviour Research and Therapy, 86, 50–67. 10.1016/j.brat.2016.06.007 [DOI] [PubMed] [Google Scholar]
- Starr LR & Davila J (2008). Excessive reassurance seeking, depression, and interpersonal rejection: A meta-analytic review. Journal of Abnormal Psychology, 117(4), 762–775. https://doi-org.umiss.idm.oclc.org/10.1037/a0013866 [DOI] [PubMed] [Google Scholar]
- Stroud LR, Tanofsky-Kraff M, Wilfley DE, & Salovey P (2000). The Yale Interpersonal Stressor (YIPS): Affective, physiological, and behavioral responses to a novel interpersonal rejection paradigm. Annals of Behavioral Medicine, 22(3), 204–213. 10.1007/BF02895115 [DOI] [PubMed] [Google Scholar]
- Thomas DL & Diener E (1990). Memory accuracy in the recall of emotions. Journal of Personality and Social Psychology, 59(2), 291–297. 10.1037//0022-3514.59.2.291 [DOI] [Google Scholar]
- Teunissen HA, Spijkerman R, Prinstein MJ, Cohen GL, Engels RC & Scholte RH (2012). Adolescents’ conformity to their peers’ pro-alcohol and anti-alcohol norms: The power of popularity. Alcoholism: Clinical and Experimental Research, 36(7), 1257–1267. 10.1111/j.1530-0277.2011.01728.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tran CV, Cole DA & Weiss B (2012). Testing reciprocal longitudinal relations between peer victimization and depressive symptoms in young adolescents. Journal of Clinical Child and Adolescent Psychology, 41(3), 353–360. 10.1080/15374416.2012.662674 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vargas SM, Huey SJ, & Miranda J (2020). A Critical Review of Current Evidence on Multiple Types of Discrimination and Mental Health. American Journal of Orthopsychiatry, 90(3), 374–390. 10.1037/ort0000441 [DOI] [PubMed] [Google Scholar]
- Venturini E, Riva P, Serpetti F, Romero L, Pallavincini F, Mantovani F, … Parsons TD (2016). A comparison of 3D versus 2D virtual environments on the feelings of social exclusion, inclusion and over-inclusion. Annual Review of CyberTherapy and Telemedicine, 14, 89–94. [Google Scholar]
- Waters AM, LeBeau RT, & Craske MG (2017). Experimental psychopathology and clinical psychology: An integrative model to guide clinical science and practice. Psychopathology Review, 4(2), 112–128. 10.5127/pr.038015 [DOI] [Google Scholar]
- Watson D (2005). Rethinking the mood and anxiety disorders: A quantitative hierarchical model for DSM-V. Journal of Abnormal Psychology, 114(4), 522–536. 10.1037/0021-843x.114.4.522 [DOI] [PubMed] [Google Scholar]
- Williams KD, Cheung CK, & Choi W (2000). Cyberostracism: Effects of being ignored over the Internet. Journal of Personality and Social Psychology, 79(5), 748–762. 10.1037//0022-3514.79.5.748 [DOI] [PubMed] [Google Scholar]
- Williams KD (2007). Ostracism. Annual Review ofPpsychology, 58. 425–452. 10.1146/annurev.psych.58.110405.085641 [DOI] [PubMed] [Google Scholar]
- Wolpe J (1958). Psychotherapy by reciprocal inhibition. Stanford, CA: Stanford University Press. [Google Scholar]
- Zadro L, Boland C & Richardson R (2006). How long does it last? The persistence of the effects of ostracism in the socially anxious. Journal of Experimental Social Psychology, 42(5), 692–697. https://doi-org.umiss.idm.oclc.org/10.1016/j.jesp.2005.10.007 [Google Scholar]
- Zvolensky MJ, Lejuez CW, Stuart GL, & Curtin JJ (2001). Experimental psychopathology in psychological science. Review of General Psychology, 5(4), 371–381. 10.1037/1089-2680.5.4.371 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.