

Abstract
Aim:
To summarize a new and easy technique of double-J stent (DJ stent) placement after retroperitoneal laparoscopic ureterolithotomy (RLU).
Materials and Methods:
RLU for upper and upper half of mid ureteric stones was performed successfully in 172 patients during the 8-year period between March 2011 and February 2019. In all the cases, a ureteric DJ stent was successfully placed by this new technique. A small-bore antral puncture needle is inserted into the retroperitoneal space to push down a DJ stent with a guidewire into the lower ureter. The tip of the antral puncture needle is manipulated to bring it near the ureterotomy site for easy insertion of the stent. The whole stent is pushed down leaving only the upper end in the ureterotomy area. Then, the guidewire is removed and the upper end is pushed up slowly into the renal pelvis.
Results:
DJ stents were successfully inserted by this technique in all the 172 cases. In most cases, the stent could be placed in <3 min (range between 2 and 8 min). In two patients, the upper end failed to fully coil in the renal pelvis, but as the stent was passed beyond the ureterotomy site, it served its purpose of an internal drain. None of our cases had any urinary leak. Stents were removed cystoscopically after 6–12 weeks.
Conclusion:
This technique provides an easy, fast, and safe antegrade method of inserting a DJ stent after RLU.
Keywords: Antral puncture needle, double-J stent, retroperitoneal laparoscopic ureterolithotomy
INTRODUCTION
The first use of a double-J stent (DJ stent) was reported by Zimskind et al. in 1967.[1] Since then, after any open or endoscopic urological procedure, short duration placement of ureteric DJ stent has become almost routine. Of course, over the last few years, there is controversy on whether a DJ stent should routinely be kept after laparoscopic ureterolithotomy (LU).[2,3,4] However, placing a DJ stent has proven to be a very effective internal drainage method for maintaining the patency of the urinary tract.[5] It prevents any blockage or prolonged leakage, thereby allowing early and better healing, and prevents narrowing during healing.[6,7,8,9,10]
Stenting after LU is more difficult than in open ureterolithotomy because of the pliability and the terminal curls of the DJ stent.[7,11,12] Many surgeons have described either pre- or postoperative retrograde stenting through the ureterovesical junction. However, it is sometimes a difficult procedure and consumes a lot of operating room time.[7,13] Antegrade placement of the DJ stent during LU is even technically more demanding and often time-consuming.[7,11,14,15] It is more difficult in retroperitoneal laparoscopic ureterolithotomy (RLU) than in transperitoneal LU because of narrow working space with plenty of fat tissue[3,4,16] and twisted stents in the operative field when the whole stent with guidewire is placed in the retroperitoneal space.[17]
Here, we describe a new and an easy technique of putting a DJ stent in the ureter after RLU for upper and upper-mid ureteric stones.
MATERIALS AND METHODS
Over the last 8 years between January 2011 and February 2019, a total of 172 cases of RLU for upper and upper-mid ureteric obstructing stones were performed in a minimally invasive surgery unit of a tertiary care hospital in Northeast India. All patients with long-standing impacted stones of more than 15 mm diameter, patients with failed ureteroscopic lithotripsy (URSL), patients with bilateral ureteric stones with acute renal failure, and patients with obstructing stone and urosepsis were taken up for RLU. Patients with smaller stones who refused to undergo URSL and preferred surgical intervention were also taken up for RLU. The operations were carried out by a single experienced senior laparoscopic surgeon.
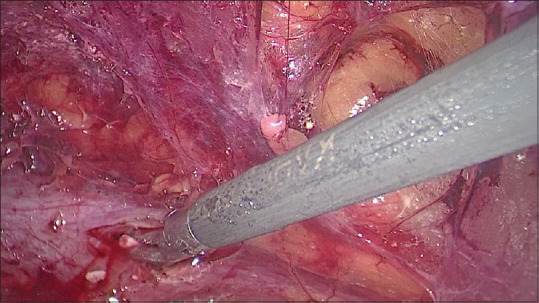
Patients were positioned in lateral decubitus kidney position. We used a Hasson port and two 5-mm working ports in the subcostal area. The ureter was identified and followed up to the stone. Ureterotomy was made over the stone using the monopolar hook and the stone was removed [Figure 1].
Figure 1.
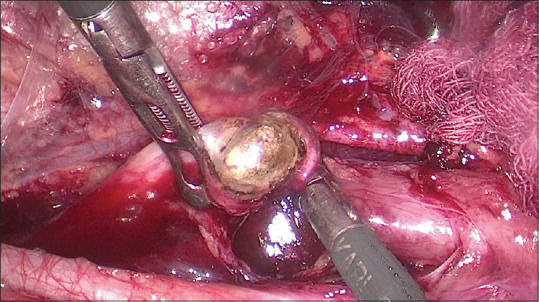
Ureterotomy and removal of the stone
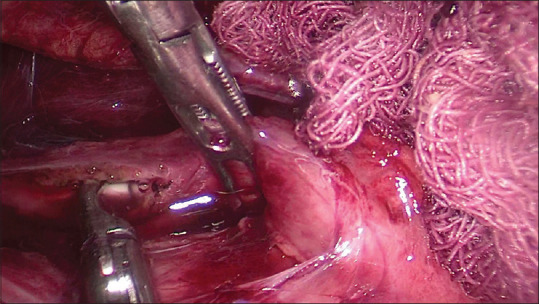
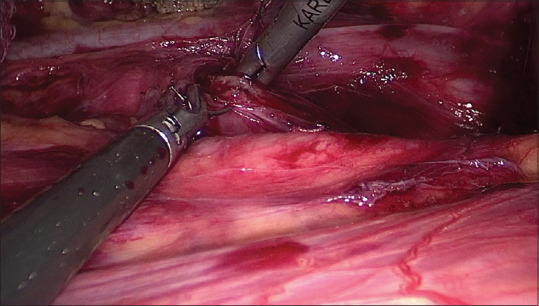
For introducing the DJ stent, we used a simple trocar cannula, long enough to reach near the ureterotomy from the skin and through which a No. 5 or 6 DJ stent can be passed. We used a simple antral puncture needle used by the ENT surgeons in the past [Figure 2]. One can also use a 3-mm laparoscopic port. One also needs a guidewire that can be passed into the DJ stent and is at least 10 to 15 cm longer than the stent. We used a femoral central line catheter guidewire which is readily available and can be reused after sterilization. We introduced the antral puncture needle into the retroperitoneal space through a small puncture wound near the camera port, parallel to the telescope to avoid any injury. The tip of the needle was manipulated to bring it very near the ureterotomy [Figure 3]. Then the stent with the guidewire was pushed down into the lower ureter and the bladder. The whole stent was pushed down so that only the upper tip remained visible [Figure 4]. This helped in keeping the upper end of the stent straight once the guidewire was removed. We never catheterized any patient preoperatively as the collapsed bladder may make it difficult to push down the stent into the bladder. When two to three centimeters of the stent had gone down the ureter, the rest can easily be pushed down from the outside. The guidewire was removed [Figure 4] and the upper end of the stent was advanced into the upper ureter and renal pelvis with the help of an atraumatic grasper and Maryland forceps [Figures 5 and 6]. One can calculate approximately how much the stent was to be pushed up by seeing the position of the stone in the ureter in a plain X-ray kidney, ureter, and bladder (KUB). Ureterotomy was closed by one to three interrupted 3-0 polyglactin sutures [Figure 7]. A retroperitoneal tube drain was kept for 3 days through the anterior 5-mm port site. The DJ stent was removed after 6 to 12 weeks.
Figure 2.
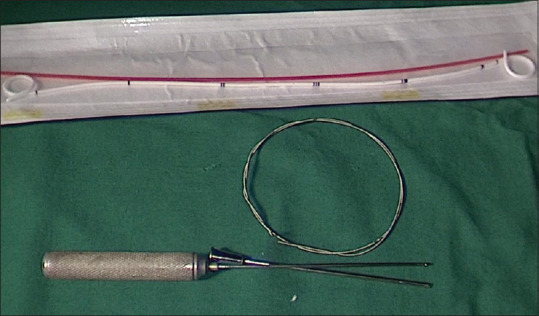
Requirements: Double-J stent, guidewire, and trocar cannula
Figure 3.
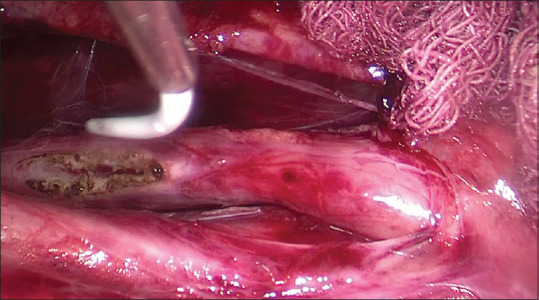
Tip of the Antral puncture needle with the lower tip of the ent brough near the ureterotomy site
Figure 4.
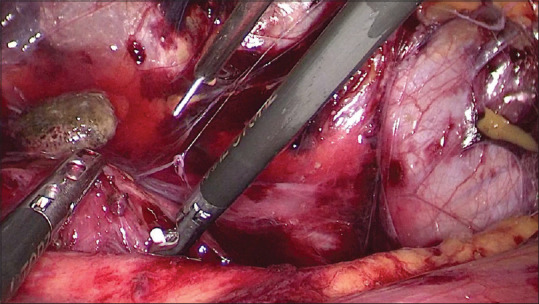
Pulling out the guidewire from the double-J stent
Figure 5.
Open upper end of the stent, ready to be pushed up the ureter into renal pelvis
Figure 6.
Manipulating the stent up into the renal pelvis
Figure 7.
Suturing the ureterotomy with 3-0 polyglactin sutures
RESULTS
DJ stents were successfully inserted by this technique in all the 172 cases of RLU. In 143 (83%) of our patients, we could place the stent in <3 min (range between 2 and 8 min). It took us longer time of up to 8 min in our initial few cases. In two patients, the upper end failed to fully coil in the renal pelvis, but as they were passed beyond the ureterotomy site, it served its purpose of an internal drain. None of our cases had any prolonged urinary leak. Stents were removed cystoscopically after 6–12 weeks. Patients were discharged on the third postoperative day after removing the drain, urethral catheter, and skin clips.
DISCUSSION
The management of ureteric stones has changed drastically since the introduction of extracorporeal shockwave lithotripsy (ESWL), ureterorenoscopy, percutaneous nephrolithotomy, and laser lithotripsy. The main aim of the treatment is to achieve a stone-free status and to preserve the renal function as soon, as safely, and as minimally as possible.[18] For patients with complex ureteric stones or those with some anatomic abnormalities, however, the best modality of treatment is still controversial.[18] Many surgeons advocate LU as the primary treatment for large proximal ureteric stone[2,3,4,8,10,16,19] or as second-line treatment of refractory calculi from either failed ureteroscopy or ESWL for any reasons.[2,3,4,8,10,20] There are many reports in literature that LU has the highest stone-free rates.[3,4,6,18,19,20,21]
Various reports in literature have described basically two methods of stenting after LU, either antegrade(intracorporeal) or retrograde (either pre- or postoperative). Antegrade stenting after RLU is very difficult and technically demanding because of the less working space and the curled ends of the stent.[7,11] Many surgeons perform either a pre- or postoperative retrograde stenting by cystoscopy or ureteroscopy. A few authors have mentioned that a preoperatively inserted stent also helps in identification of the ureter during operation, thereby reducing the operating time.[22] However, preoperative stenting in the presence of an obstructing stone sometime is unsuccessful or a difficult procedure to negotiate the stent beyond the stone and is usually time-consuming.[7,11,23] Furthermore, there is a need to change the patient's position from lithotomy to lateral decubitus kidney position for the operation.
Many authors have described a preoperative cystoscopically inserted guidewire, with an open tip stent or a ureteric catheter, under fluoroscopic guidance inserted just up to the stone. After the removal of the stone, under laparoscopic vision, the stent was pushed through the ureterotomy over the guidewire.[16,22,23] Some authors pulled out the upper end of the guidewire through a laparoscopic port and over that an antegrade stent was kept, first the lower end and then the upper end.[14] They mentioned this technique for laparoscopic stenting in dismembered retroperitoneal pyeloplasty. Others after completing the operation put the patient back into lithotomy position and advanced the stent under fluoroscopy guidance.[4,23] Here, the risk of radiation exposure to the patient, surgeon, and the other OT staffs exists.
Few authors in some of their cases introduced a guidewire by percutaneous renal puncture over which they introduced a DJ stent in an antegrade manner.[9] In cases of lower ureteric stones, they gave another incision in the upper ureter to put the guidewire and the stent.
Some surgeons have mentioned a postoperative ureteroscope-assisted DJ stenting as a simple and safe method.[7] They mentioned that it allows correct placement of the stent under direct vision and prompt treatment of any residual stone fragments without any radiation exposure. However, the major concern of postoperative ureteroscope-guided stent placement is the negative effect of the continuous saline irrigation on the suture line causing dehiscence and prolonged urinary leakage.[7]
In one of the earliest publications, the authors described an antegrade method where they used a guidewire 2 cm shorter than the stent.[24] The smooth uncut end of the guidewire is passed down to the closed end and the cut hard end passed up to the open end through two holes in the stent approximately below and above the level of the stone as shown on a KUB X-ray. They adjusted the guidewire in such a way that the upper end remained almost straight and the lower end slightly curved. They inserted the whole stent down first till the upper end reached the level of ureterotomy. The upper end was pushed up and the guidewire was removed by holding in the part remaining outside the stent. Very recently in another publication, a similar technique using a short guidewire with a DJ stent closed at both ends was mentioned.[25]
In another technique, a DJ stent with both ends closed was threaded on a guidewire which was 1 cm longer than the stent, passed through the side holes, so that 1–2 cm of the guidewire remained outside the stent.[10,12] After insertion of the stent, the guidewire was removed by grasping this portion. One surgeon in his paper described a method where he calculates approximately the position of the stone in the ureter on a digital X-ray KUB.[13] At that point, he makes a slit in the DJ stent to put a silk tie on the guidewire to pull it out. However, by making a split in the stent, the tensile strength may be compromised. Also after insertion of the stent when pulling the guidewire, this split may become wider, further increasing the risk of stent fracture. Sometimes pulling out the guidewire may be difficult and it may pull out the stent.
In a similar technique, some authors used a DJ stent with both ends closed but with two guidewires.[11,15,17] They inserted the guidewires through two side holes into the stent without splitting it. In this method, pushing the stent along with the two guidewires into the narrow retroperitoneal space and then manipulating the tips of the stent into the narrow ureterotomy may sometimes be difficult.[17] These wires can become entangled and create problems when the folded DJ stent is pushed down into the working space.[24] Moreover, the introduction of the two ends of the folded stent through the ureterotomy in opposite directions might damage the ureter.[24] Some confirmed the correct positioning of the lower end of stent in the urinary bladder by flexible cystoscopy before closing the ureterotomy site.[15]
In a similar method using two guidewires, the authors replaced the metallic guidewires with plastic wires found in No. 8 pediatric catheters.[21] Few authors described another percutaneous technique through an 18-gauge needle, in which the distal part of the stent with a guidewire through a side hole is pushed down the ureterotomy site into the urinary bladder and the guidewire is removed. The upper end of the stent is than pushed up retrograde into the renal pelvis.[17]
Our technique does not need any costly equipment like the ureteroscope. Furthermore, if there is any resistance when passing the stent up or down, one should suspect any undiagnosed missed stone. There is no need to change the position of the patient for insertion of the stent. As the tip of our guidewire is very soft and malleable, none of our patients had any complications such as perforation of the ureter or submucosal dissection. After putting the lower end, one can confirm its placement into the bladder by pressing over the suprapubic area and observing urine coming out from the upper end of the stent.
CONCLUSION
Our technique of stenting is a very fast, safe, and easy technique. With more and more use of laparoscopy in the management of ureteropelvic stones, pyeloplasty, and ureteroureterostomy, one needs to find out an easy technique of DJ stenting.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Zimskind PD, Fetter TR, Wilkerson JL. Clinical use of long-term indwelling silicone rubber ureteral splints inserted cystoscopically. J Urol. 1967;97:840–4. doi: 10.1016/S0022-5347(17)63130-6. [DOI] [PubMed] [Google Scholar]
- 2.You JH, Kim YG, Kim MK. Should we place ureteral stents in retroperitoneal laparoscopic ureterolithotomy? Consideration of surgical techniques and complications. Korean J Urol. 2014;55:511–4. doi: 10.4111/kju.2014.55.8.511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Şahin S, Aras B, Ekşi M, Şener NC, Tugču V. Laparoscopic ureterolithotomy. JSLS. 2016;20:1–7. doi: 10.4293/JSLS.2016.00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hammady A, Gamal WM, Zaki M, Hussein M, Abuzeid A. Evaluation of ureteral stent placement after retroperitoneal laparoscopic ureterolithotomy for upper ureteral stone: Randomized controlled study. J Endourol. 2011;25:825–30. doi: 10.1089/end.2010.0628. [DOI] [PubMed] [Google Scholar]
- 5.Lai CJ, Wong WJ, Tsai PK, Wu HC, Chen J. Management of a retained double–J catheter with severe encrustations: A case report. JTUA. 2009;20:187–9. [Google Scholar]
- 6.Ray RP, Mahapatra RS, Mondal PP, Pal DK. Long-term complications of JJ stent and its management: A 5 years review. Urol Ann. 2015;7:41–5. doi: 10.4103/0974-7796.148599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chen IH, Tsai JY, Yu CC, Wu T, Huang JK, Lin JT. Ureteroscope-assisted double-J stenting following laparoscopic ureterolithotomy. Kaohsiung J Med Sci. 2014;30:243–7. doi: 10.1016/j.kjms.2013.09.013. [DOI] [PubMed] [Google Scholar]
- 8.Gaur DD, Trivedi S, Prabhudesai MR, Madhusudhana HR, Gopichand M. Laparoscopic ureterolithotomy: Technical considerations and long-term follow-up. BJU Int. 2002;89:339–43. doi: 10.1046/j.1464-4096.2001.01562.x. [DOI] [PubMed] [Google Scholar]
- 9.Cavalli AC, Tambara Filho R, Slongo LE, Cavalli RC, Rocha LC. The use of double-J catheter decreases complications of retroperitoneoscopic ureterolithotomy. Rev Col Bras Cir. 2012;39:112–8. [PubMed] [Google Scholar]
- 10.Farooq Qadri SJ, Khan N, Khan M. Retroperitoneal laparoscopic ureterolithotomy–A single centre 10 year experience. Int J Surg. 2011;9:160–4. doi: 10.1016/j.ijsu.2010.10.012. [DOI] [PubMed] [Google Scholar]
- 11.Yoo D, Shim S, Seo M, Yim J, Joonhwa N. V1722 The New Technique to insert a double-J stent conveniently in laparoscopic ureterolithotomy: Noh & Prime's method. J Urol. 2012;187:e694. [Google Scholar]
- 12.Khan M, Khan F. Innovative technique for ureteral stenting during retroperitoneal laparoscopic ureterolithotomy. J Endourol. 2005;19:994–6. doi: 10.1089/end.2005.19.994. [DOI] [PubMed] [Google Scholar]
- 13.Mandhani A. A technique of stenting after laparoscopic ureterolithotomy. Indian J Urol. 2011;27:418–9. doi: 10.4103/0970-1591.85455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nouira Y, Horchani A. How to insert a double J stent in laparoscopic retroperitoneal dismembered pyeloplasty: A new technique. Surg Laparosc Endosc Percutan Tech. 2004;14:306–8. doi: 10.1097/00129689-200410000-00018. [DOI] [PubMed] [Google Scholar]
- 15.Kim JY, Kang SH, Cheon J, Lee JG, Kim JJ, Kang SG. The usefulness of flexible cystoscopy for preventing double-J stent malposition after laparoscopic ureterolithotomy. BMC Urol. 2017;17:44. doi: 10.1186/s12894-017-0232-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.El-Moula MG, Abdallah A, El-Anany F, Abdelsalam Y, Abolyosr A, Abdelhameed D, et al. Laparoscopic ureterolithotomy: Our experience with 74 cases. Int J Urol. 2008;15:593–7. doi: 10.1111/j.1442-2042.2008.02065.x. [DOI] [PubMed] [Google Scholar]
- 17.Choi H, Kim JH, Park JY, Shim JS, Bae JH. A modified laparoscopic ureterolithotomy by pulling ureter with Carter-Thomason fascial closure and ureter incision by broken 15th blade. Scand J Surg. 2014;103:195–200. doi: 10.1177/1457496913509983. [DOI] [PubMed] [Google Scholar]
- 18.Hu Q, Ding W, Gou Y, Ho Y, Xu K, Gu B, et al. Retroperitoneal laparoscopic ureterolithotomy for proximal ureteral calculi in selected patients. Sci World J. 2014;2014:1–5. doi: 10.1155/2014/687876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ko YH, Kang SG, Park JY, Bae JH, Kang SH, Cho DY, et al. Laparoscopic ureterolitho-Tomy as a primary modality for large proximal ureteral calculi: Comparison to rigid ureteroscopic pneumatic lithotripsy. J Laparoendos Adv Surg Tech. 2011;21:7–13. doi: 10.1089/lap.2010.0340. [DOI] [PubMed] [Google Scholar]
- 20.Turk C, Knoll T, Petrik A, Sarica K, Skolarikos A, Straub M, et al. Specific stone management of ureteral stones. In: Turk C, editor. EAU Guidelines on Urolithiasis. 3. Arnhem, Netherland: European Association of Urology; 2016. [Last accessed on 2019 Feb]. pp. 25–30. Available from: http://www.uroweb.org/qls/pdf/18 . [Google Scholar]
- 21.Fang YQ, Qiu JG, Wang DJ, Zhan HL, Situ J. Comparative study on ureteroscopic lithotripsy and laparoscopic ureterolithotomy for treatment of unilateral upper ureteral stones. Acta Cir Bras. 2012;27:266–70. doi: 10.1590/s0102-86502012000300011. [DOI] [PubMed] [Google Scholar]
- 22.Garg M, Singh V, Sinha RJ, Sankhwar SN, Kumar M, Kumar A, et al. Prospective randomized comparison of open versus transperitoneal laparoscopic ureterolithotomy: Experience of a single center from Northern India. Curr Urol. 2013;7:83–9. doi: 10.1159/000356254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Goel A, Hemal AK. Upper and mid-ureteric stones: A prospective unrandomized comparison of retroperitoneoscopic and open ureterolithotomy. BJU Int. 2001;88:679–82. doi: 10.1046/j.1464-4096.2001.00150.x. [DOI] [PubMed] [Google Scholar]
- 24.Gaur DD, Joshi NR, Dubey M, Acharya UP. A simple technique for retroperitoneal laparoscopic JJ stenting of the ureter. BJU Int. 2003;91:725–6. doi: 10.1046/j.1464-410x.2003.04184.x. [DOI] [PubMed] [Google Scholar]
- 25.Wani MM, Durrani AM. Laparoscopic ureterolithotomy: Experience of 60 cases from a developing world hospital. J Minim Access Surg. 2018;15:103–8. doi: 10.4103/jmas.JMAS_203_17. [DOI] [PMC free article] [PubMed] [Google Scholar]