

Abstract
Background
Bacteriophages have been introduced as living drugs for infectious diseases; thus, they may provide an alternative to conventional acne therapeutics in patients with non-responsive acne.
Objective
We investigated the effect of bacteriophages using an acne mouse model with Propionibacterium acnes-induced inflammatory nodules by clinical examination, pathology, and immunohistochemical analysis.
Methods
A human-isolated P. acnes suspension (109 colony forming units/µl) was injected into the backs of HR-1 mice. Group A was used as a control, Group B was injected on the back with P. acnes 4 weeks following the initial P. acnes suspension injection, and group C was injected on the back with P. acnes and bacteriophages 4 weeks following the initial P. acnes suspension injection. Clinical and histopathological evaluations were performed.
Results
Inflammatory nodule size decreased with time in all groups. Group C showed the greatest decrease in size, followed by group B and group A. The histopathological findings showed a decrease in epidermal thickness and the number and size of microcomedone-like cysts in groups B and C compared to group A. Immunohistochemistry revealed similar expression of integrin α6, the epidermal proliferation marker, infiltration of CD4/CD8 T cells and neutrophils, and expression of myeloperoxidase, interleukin-1β, toll-like receptor-2, LL-37, and matrix metalloproteinase-2/3/9 in all three groups.
Conclusion
Using an acne mouse model with P. acnes-induced inflammatory nodules, we demonstrate that bacteriophages may constitute an alternative to conventional acne therapies. However, additional studies are needed for human applications.
Keywords: Acne vulgaris, Bacteriophage, Mice, Propionibacterium acnes
INTRODUCTION
Acne vulgaris is a very common skin disease of the pilosebaceous follicles characterized by comedones, papules, pustules, nodules, and cysts1. One of the main causative factors of acne is colonization of the follicular infundibulum and sebaceous duct by Propionibacterium acnes. P. acnes plays an important role in inducing an inflammatory event2. In addition, P. acnes can lead to the development of abnormal differentiation and keratinization in epidermal keratinocytes1. Therefore, P. acnes may act as a major causative factor in early inflammatory papules of acne.
The establishment of animal models for various diseases is helpful for expanding research fields and developing the production of new therapeutic modalities. Although there are various acne animal models, such as the Mexican hairless dog, the Rhino mouse, and the rabbit ear assay, elucidative models are still needed3. Previously, we reported the establishment of an acne mouse model; HR-1 mice develop acne-like inflammatory nodules on their backs following injection of P. acnes, in contrast to BALB/c, VDR k/o, and SCID mice4.
Bacteriophages are bacterial viruses consisting of proteins that encapsulate a DNA or RNA genome5; they are widely distributed in sites populated by bacteria. Bacteriophages replicate within bacteria after injecting their genome into the bacterial cytoplasm. They tend to kill only specific pathogens without damaging the normal flora; thus, they can be used as living drugs for bacterial infections, including acne6. Bacteriophages targeting P. acnes have been isolated from acne patients7.
In this study, we investigated the efficacy of bacteriophages in a P. acnes-induced acne mouse model by clinical examination, histopathology, and immunohistochemical studies.
MATERIALS AND METHODS
P. acnes culturing
P. acnes (ATCC 11828) were isolated from pustular lesions of Korean patients with moderate inflammatory acne. P. acnes from post log phase cultures were grown on brain heart infusion agar under anaerobic conditions at 37℃. P. acnes cells were harvested by centrifugation at 5,000×g for 10 minutes, washed three times with phosphate buffered saline (PBS), and resuspended to a concentration of 109 colony forming units/ml in PBS for the experiments.
Acne mouse model using HR-1 mice and injection of P. acnes and/or bacteriophages into HR-1 mice
Six-week-old female Hos:HR-1 mice (HR-1; SLC Inc., Hamamatsu, Japan) were maintained under conventional laboratory conditions following 1 week of acclimation. A live P. acnes suspension was injected intradermally (20 µl aliquots), using a 30-gauge needle, on both sides of the backs of three mice per group (group A, group B, and group C). Group A was used as the control; Group B was re-injected with P. acnes on the back 4 weeks following the first P. acnes injection; and Group C was injected with P. acnes and bacteriophages on the back 4 weeks following the first P. acnes injection. Bacteriophages were injected intradermally in 20 µl aliquots at the P. acnes injection site. This procedure was performed in accordance with the institutional guidelines for the care and use of laboratory animals (KNU-2016-0112).
Bacteriophage preparation
Bacteriophages (KNU, Daegu, Korea) against P. acnes were cultured and diluted using tryptone agar plates, tryptone soft agar tubes, and tryptone broth tubes. The bacteriophages were prepared at a concentration of 2.5×106 plaque forming units (PFU)/ml. The concentration was determined using the following formula: PFU/ml=number of plaques/d×v (d: dilution, v: volume of diluted virus added to the plate).
Evaluation of clinical changes
The degree of clinical inflammatory changes was evaluated using digital photography at baseline and at week 1, 2, 3 and 4 post the first injection in group A and after the second injection in groups B and C.
Histological examination
Mouse tissue samples were collected at week 2 and 4 after the first injection in group A and after the second injection in groups B and C. Eight tissue samples were collected from group A, six from group B, and six from group C. Paraffin-embedded tissue sections (3-µm thick) were processed for hematoxylin and eosin staining. The histological changes were compared with an emphasis on changes in inflammation, epidermal/follicular wall thickness, and formation of cystic structures containing keratinized plugs (microcomedone-like cystic structures) in the dermis of groups A, B, and C.
Immunohistochemistry
Immunohistochemical staining was performed at week 2 after the first injection in group A and after the second injection in groups B and C using standard techniques. The primary antibodies included: integrin α6 (used at 1:150 dilution; Santa Cruz Biotechnology, Inc., Santa Cruz, CA, USA), CD4+ T cells (1:300 dilution; Abcam, Cambridge, UK), CD8+ T cells (1:100 dilution; Abcam), neutrophil (1:80 dilution; Abcam), myeloperoxidase (MPO, 1:200 dilution; Abcam), interleukin (IL)-1β (1:150 dilution; Abcam), matrix metalloproteinase (MMP)-2 (1:300 dilution; Abcam), MMP-3 (1:100 dilution; Abcam), MMP-9 (1:250 dilution; Abcam,), toll-like receptor (TLR)-2 (1:500 dilution; Abcam), and LL-37 (1:300 dilution; Abcam). The expression of inflammatory biomarkers per unit area in groups A, B, and C was measured using Image J (NIH Image, Bethesda, MD, USA).
Western blot analysis
Western blot analysis was performed at week 2 after the first injection in group A and after the second injection in groups B and C to detect the anti-immunoglobulin G (IgG) antibody against P. acnes. P. acnes was lysed in a lysis buffer (25 mM Tris-HCl [pH 7.2], 150 mM KCl, 0.1% sodium dodecyl sulfate, 1% Triton X-100, 5 mM EDTA [pH 8.0], and 2 mM phenylmethylsulfonyl fluoride) supplemented with a protease inhibitor cocktail. Equal protein amounts were resolved by sodium dodecyl sulfate-polyacrylamide gel electrophoresis, transferred to a polyvinylidene difluoride membrane, and blotted with the mouse serum obtained from each group, followed by enhanced chemiluminescence and autoradiography.
Statistical analysis
The data were statistically analyzed using ANOVA. A p-value <0.05 was considered significant. All statistical analyses were performed using PASW software (Version 18.0; IBM Co., Armonk, NY, USA).
RESULTS
Changes in inflammatory nodules in acne mouse model groups A, B, and C
The size of the inflammatory nodules in all three groups decreased with time (Fig. 1A, B). There was a statistically significant difference in the size of the inflammatory nodules in groups B and C compared to group A at week 1, 2, 3, and 4. Group C showed a statistically significant decrease in inflammatory nodule size compared to group B at week 2 and 4.
Fig. 1. (A) Changes in inflammatory nodule size in groups A, B, and C. The size of the inflammatory nodules in all groups decreased with time. (B) Changes in inflammatory nodule size in groups A, B, and C. The size of the inflammatory nodules in all groups decreased with time. The changes in size between groups B/C and group A were significantly different at weeks 1, 2, 3, and 4. The changes in size between group B and group C were significantly different at week 2 and 4.

Characteristics of histopathological findings in groups A, B, and C
Epidermal thickness and the number and size of the microcomedone-like cysts were decreased in groups B and C compared to group A at week 4 (Fig. 2A~D). However, there were no statistically significant differences.
Fig. 2. (A) Histopathological findings of group A, group B and group C at week 4 (H&E, ×200). (B) Changes in epidermal thickness. The epidermal thickness of the inflammatory nodules decreased with time, especially in group C, followed by group B and group A. However, there were no statistically significant differences. (C) Changes in the number of microcomedone-like cysts. The number of microcomedone-like cysts decreased with time, especially in group C, followed by group B and group A. However, there were no statistically significant differences. (D) Changes in the size of microcomedone-like cysts. The size of the microcomedone-like cysts decreased with time, especially in group C, followed by group B and group A. However, there were no statistically significant differences.

Expression of inflammatory biomarkers in groups A, B, and C
The immunohistochemistry results showed that infiltration of CD8 T cells and neutrophils and the expression of IL-1β, MMP-3 and MMP-9 in group B and group C were decreased when compared with group A (Fig. 3A). On the contrary, infiltration of CD4 T cells and the expression of LL-37 in group B and group C were increased when compared with group A (Fig. 3A). However, there were no statistically significant differences in all three groups (Fig. 3A). Integrin α6 expression was increased in group B and decreased in group C when compared with group A (Fig. 3A, B). Integrin α6 expression showed a statistically significant decrease in group B when compared with group B (p<0.05) (Fig. 3A).
Fig. 3. (A) Immunohistochemistry analysis. Inflammatory biomarker expression was similar in all groups. There were no statistically significant differences except for integrin α6 between group B and group C. (B) Immunohistochemistry with integrin α6 in group A, group B and group C at week 2 (×200). IL: interleukin, MMP: matrix metalloproteinase, MPO: myeloperoxidase, TLR: toll-like receptor.

Western blot analysis using an anti-IgG antibody
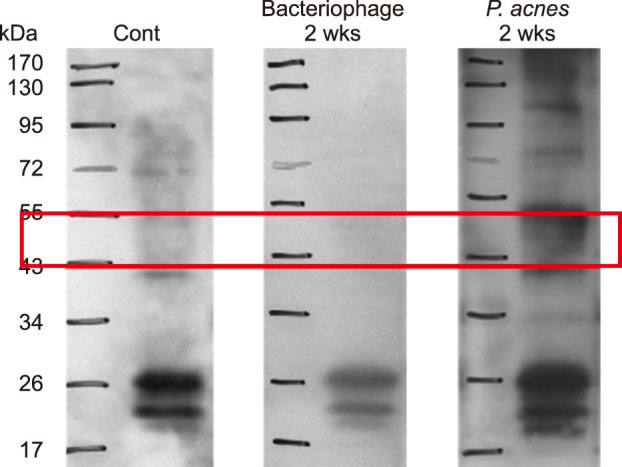
No immunoreactivity for an anti-IgG antibody against P. acnes was observed at week 2 after the first injection in the group A or at week 2 after the second injection in the group C. However, western blot analysis could detect an IgG antibody component against P. acnes (approximately 47 kDa) at week 2 after the second injection in the group B (Fig. 4).
Fig. 4. Western blot analysis showed immunoreactivity to the immunoglobulin G antibody against Propionibacterium acnes (P. acnes) following treatment with P. acnes.
DISCUSSION
Topical and systemic medications have been used for the treatment of acne8. However, bacterial resistance to antibiotics and adverse retinoid events have led to the development of new therapeutic modalities for acne9,10; vaccination has been introduced as one of the promising therapeutics for acne11.
Killed-pathogen-based vaccines have been used as a vaccine for the treatment of acne12 and an intranasal killed whole P. acnes preparation has been tested12. P. acnes has been established as a potent immunomodulator13, which can produce antibodies against secretary enzymes or cell wall molecules14. However, antibodies against P. acnes do not completely protect against the recurrence of acne, most likely because of insufficient production of protective antibodies against P. acnes. This study also showed the production of antibody in mice after treatment with P. acnes. Bacteriophages inhibited the production of the antibody in mice after treatment with P. acnes.
Vaccination against cell wall-anchored sialidase has also been introduced15. Sialidase, a P. acnes virulence factor, is involved in degrading host tissue and inducing inflammation16. Nakatsuji et al.15 have reported that a sialidase-based acne vaccine showed good effects on P. acnes-induced ear inflammation. However, this vaccine may not be able to neutralize virulence factors secreted by P. acnes17. In addition, this vaccine may lack therapeutic effects for acne.
Monoclonal antibodies targeting Christie-Atkins-Munch-Peterson (CAMP) factor have demonstrated improvement of acne17. P. acnes possesses a CAMP that acts as a potential secretory virulence factor to enhance hemolysis and cytolysis16,18. Nakatsuji et al.17 also investigated the treatment of acne using vaccines. They showed that passive immunization targeting secretory CAMP factors proteins can neutralize P. acnes virulence without disturbing other bacteria17. Active immunization using a CAMP factor-targeted vaccine and passive neutralization of the CAMP factor showed roughly equal potency in terms of improving P. acnes-induced inflammation.
TLR vaccines and antimicrobial peptides (AMPs) constitute other optional vaccines for the treatment of acne. Recent studies have shown that TLRs and AMPs play an important role in the pathogenesis of inflammatory acne. Therefore, regulation of TLRs and AMPs could provide different therapeutic options for acne19.
Bacteriophages targeting P. acnes are also promising acne vaccine candidates20. Bacteriophages have several advantages over antibiotics against P. acnes. They are environmentally friendly, rapidly processed, less expensive, and well tolerated5. In this study, we confirmed the potential of bacteriophages for the treatment of acne. The inflammatory nodules of HR-I mice decreased in size and microcomedone-like cysts was reduced in number and in size following bacteriophage treatment. In addition, epidermal thickness was decreased in bacteriophage treatment group. Epidermal hyperplasia can be induced by skin barrier disruption, calcium channel activation, metabotrophic receptor activation or unsaturated fatty acids21. Epidermal hyperplasia may be related to the induction of abnormal keratinization, which can be one of the causative factors of comedone formation. Furthermore, the decreased expression of integrin α6 after bacteriophage application shows its beneficial effect for the treatment of acne. Integrin α6 expression can be a response to inflammation and related to epidermal hyperplasia, leading to the abnormal differentiation2. Inflammatory biomarkers and cells, such as CD8 T cells, neutrophils, IL-1β, MMP-3 and MMP-9, were also decreased after bacteriophage treatment. Antimicrobial peptides can play a protective role against P. acnes or induce inflammatory signal in acne vulgaris22. In this study, the increased expression of LL-37 by P. acnes was not inhibited by bacteriophages.
Several parameters for bacteriophages need to be resolved for a comprehensive acne vaccine: delivery route, time point of delivery, dose, phage stability, infection rate, availability of highly efficient antibiotics, poor understanding of general aspects of phage life cycles, bacterial resistance to phage infection, and the possibility of temperate phages that integrate into the human genome23. Understanding the integration of temperate phages into the human genome is critical for the safety of phage therapy.
Recently, bacteriophages have been applied in a semi-solid preparation for the treatment of acne24. In addition, bacteriophages have also been formulated in a water-oil nanoemulsion25. Bacteriophages against Acinetobacter baumannii have been applied in humans in the form of an antiseptic gel or a paraffin-oil-based product26. In light of these reports, a variety of formulations for the treatment of acne using bacteriophages that target P. acnes should be examined.
In conclusion, further investigation of bacteriophages targeting P. acnes should be conducted to gain a better understanding of bacteriophage characteristics and to develop more beneficial vaccines for the treatment of acne.
ACKNOWLEDGMENT
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (2012R1A1A2007017).
Footnotes
CONFLICTS OF INTEREST: The authors have nothing to disclose.
References
- 1.Shaheen B, Gonzalez M. Acne sans P. acnes. J Eur Acad Dermatol Venereol. 2013;27:1–10. doi: 10.1111/j.1468-3083.2012.04516.x. [DOI] [PubMed] [Google Scholar]
- 2.Jeremy AH, Holland DB, Roberts SG, Thomson KF, Cunliffe WJ. Inflammatory events are involved in acne lesion initiation. J invest dermatol. 2003;121:20–27. doi: 10.1046/j.1523-1747.2003.12321.x. [DOI] [PubMed] [Google Scholar]
- 3.Mirshahpanah P, Maibach HI. Models in acnegenesis. Cutan Ocul Toxicol. 2007;26:195–202. doi: 10.1080/15569520701502815. [DOI] [PubMed] [Google Scholar]
- 4.Jang YH, Lee KC, Lee SJ, Kim DW, Lee WJ. HR-1 mice: a new inflammatory acne mouse model. Ann Dermatol. 2015;27:257–264. doi: 10.5021/ad.2015.27.3.257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jończyk-Matysiak E, Weber-Dąbrowska B, Żaczek M, Międzybrodzki R, Letkiewicz S, Łusiak-Szelchowska M, et al. Prospects of phage application in the treatment of acne caused by Propionibacterium acnes. Front Microbiol. 2017;8:164. doi: 10.3389/fmicb.2017.00164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jassim SA, Limoges RG. Natural solution to antibiotic resistance: bacteriophages ‘The Living Drugs’. World J Microbiol Biotechnol. 2014;30:2153–2170. doi: 10.1007/s11274-014-1655-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Marples RR. The microflora of the face and acne lesions. J Invest Dermatol. 1974;62:326–331. doi: 10.1111/1523-1747.ep12724285. [DOI] [PubMed] [Google Scholar]
- 8.Sandoval LF, Hartel JK, Feldman SR. Current and future evidence-based acne treatment: a review. Expert Opin Pharmacother. 2014;15:173–192. doi: 10.1517/14656566.2014.860965. [DOI] [PubMed] [Google Scholar]
- 9.Bienenfeld A, Nagler AR, Orlow SJ. Oral antibacterial therapy for acne vulgaris: an evidence-based review. Am J Clin Dermatol. 2017;18:469–490. doi: 10.1007/s40257-017-0267-z. [DOI] [PubMed] [Google Scholar]
- 10.Vallerand IA, Lewinson RT, Farris MS, Sibley CD, Ramien ML, Bulloch AGM, et al. Efficacy and adverse events of oral isotretinoin for acne: a systematic review. Br J Dermatol. 2018;178:76–85. doi: 10.1111/bjd.15668. [DOI] [PubMed] [Google Scholar]
- 11.Nakatsuji T, Rasochova L, Huang CM. Vaccine therapy for P. acnes-associated diseases. Infect Disord Drug Targets. 2008;8:160–165. doi: 10.2174/1871526510808030160. [DOI] [PubMed] [Google Scholar]
- 12.Nakatsuji T, Liu YT, Huang CP, Zoubouis CC, Gallo RL, Huang CM. Antibodies elicited by inactivated Propionibacterium acnes-based vaccines exert protective immunity and attenuate the IL-8 production in human sebocytes: relevance to therapy for acne vulgaris. J Invest Dermatol. 2008;128:2451–2457. doi: 10.1038/jid.2008.117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Mussalem JS, Vasconcelos JR, Squaiella CC, Ananias RZ, Braga EG, Rodrigues MM, et al. Adjuvant effect of the Propionibacterium acnes and its purified soluble polysaccharide on the immunization with plasmidial DNA containing a Trypanosoma cruzi gene. Microbiol Immunol. 2006;50:253–263. doi: 10.1111/j.1348-0421.2006.tb03791.x. [DOI] [PubMed] [Google Scholar]
- 14.Lodes MJ, Secrist H, Benson DR, Jen S, Shanebeck KD, Guderian J, et al. Variable expression of immunoreactive surface proteins of Propionibacterium acnes. Microbiology. 2006;152:3667–3681. doi: 10.1099/mic.0.29219-0. [DOI] [PubMed] [Google Scholar]
- 15.Nakatsuji T, Liu YT, Huang CP, Zouboulis CC, Gallo RL, Huang CM. Vaccination targeting a surface sialidase of P. acnes: implication for new treatment of acne vulgaris. PLoS One. 2008;3:e1551. doi: 10.1371/journal.pone.0001551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Brüggemann H. Insights in the pathogenic potential of Propionibacterium acnes from its complete genome. Semin Cutan Med Surg. 2005;24:67–72. doi: 10.1016/j.sder.2005.03.001. [DOI] [PubMed] [Google Scholar]
- 17.Nakatsuji T, Tang DC, Zhang L, Gallo RL, Huang CM. Propionibacterium acnes CAMP factor and host acid sphingomyelinase contribute to bacterial virulence: potential targets for inflammatory acne treatment. PLoS One. 2011;6:e14797. doi: 10.1371/journal.pone.0014797. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lo CW, Lai YK, Liu YT, Gallo RL, Huang CM. Staphylococcus aureus hijacks a skin commensal to intensify its virulence: immunization targeting beta-hemolysin and CAMP factor. J Invest Dermatol. 2011;131:401–409. doi: 10.1038/jid.2010.319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ozlu E, Karadag AS, Ozkanli S, Oguztuzun S, Kilic M, Zemheri E, et al. Comparison of TLR-2, TLR-4, and antimicrobial peptide levels in different lesions of acne vulgaris. Cutan Ocul Toxicol. 2016;35:300–309. doi: 10.3109/15569527.2015.1120742. [DOI] [PubMed] [Google Scholar]
- 20.Górski A, Dąbrowska K, Hodyra-Stefaniak K, Borysowski J, Międzybrodzki R, Weber-Dąbrowska B. Phages targeting infected tissues: novel approach to phage therapy. Future Microbiol. 2015;10:199–204. doi: 10.2217/fmb.14.126. [DOI] [PubMed] [Google Scholar]
- 21.Katsuta Y, Iida T, Inomata S, Denda M. Unsaturated fatty acids induce calcium influx into keratinocytes and cause abnormal differentiation of epidermis. J Invest Dermatol. 2005;124:1008–1013. doi: 10.1111/j.0022-202X.2005.23682.x. [DOI] [PubMed] [Google Scholar]
- 22.Borovaya A, Dombrowski Y, Zwicker S, Olisova O, Ruzicka T, Wolf R, et al. Isotretinoin therapy changes the expression of antimicrobial peptides in acne vulgaris. Arch Dermatol Res. 2014;306:689–700. doi: 10.1007/s00403-014-1477-3. [DOI] [PubMed] [Google Scholar]
- 23.Brüggemann H, Lood R. Bacteriophages infecting propionibacterium acnes. Biomed Res Int. 2013;2013:705741. doi: 10.1155/2013/705741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Brown TL, Petrovski S, Dyson ZA, Seviour R, Tucci J. The formulation of bacteriophage in a semi solid preparation for control of Propionibacterium acnes growth. PLoS One. 2016;10:e0151184. doi: 10.1371/journal.pone.0151184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Esteban PP, Alves DR, Enright MC, Bean JE, Gaudion A, Jenkins AT, et al. Enhancement of the antimicrobial properties of bacteriophage-K via stabilization using oil-in-water nano-emulsions. Biotechnol Prog. 2014;30:932–944. doi: 10.1002/btpr.1898. [DOI] [PubMed] [Google Scholar]
- 26.Chen LK, Liu LY, Hu A, Chang KC, Lin NT, Lai MJ, et al. Potential of bacteriophage ΦAB2 as an environmental biocontrol agent for the control of multidrug-resistant Acinetobacter baumannii. BMC Microbiol. 2013;13:154. doi: 10.1186/1471-2180-13-154. [DOI] [PMC free article] [PubMed] [Google Scholar]