

Abstract
Kratom is an unregulated kappa-opioid receptor agonist available for order on the internet that is used as a remedy for chronic pain. We present a case of a middle-aged man who suffered a cardiac arrest in the setting of kratom ingestion.
Keywords: arrhythmias, cardiovascular system, pacing and electrophysiology, complementary medicine
Background
Kratom is an complementary medicine used in non-western medicine for chronic pain, however it has potential side effect of QT prolongation along with others that can cause users to become severely ill with its use.
Case presentation
The patient was a 44-year-old man who presented to our emergency room after a witnessed cardiac arrest.
He was at a restaurant when he slumped over and became unresponsive, hitting his head. Bystander cardiopulmonary resuscitation was started almost immediately. After emergency medical services arrived, advanced cardiac life support was initiated and multiple episodes of ventricular fibrillation required three unsynchronised shocks, multiple rounds of epinephrine and the initiation of amiodarone.
At baseline the patient was very active, walking several miles a day. He had hypertension and hyperlipidemia, both controlled with medical therapy. A routine ECG with his yearly physical was unremarkable. The patient had no prior cardiac workup. The family reported the patient had recently begun consuming ‘Premium Maeng Da Kratom’ an energy supplement in addition to his chronic ingestion of 2–8 Monster energy drinks daily with each drink containing approximately 86 mg of caffeine.
Investigations
In the emergency department, initial laboratory analysis was significant for a potassium of 3.1 mg/dL and a troponin of <0.01 ng/mL. A urine toxicology report was positive for ethanol. The ECG on arrival to the emergency room showed prolonged QT interval and intraventricular conduction block (figure 1). His chest X-ray was remarkable for pulmonary vascular congestion (figure 2). He was intubated in the setting of hypoxic respiratory failure. A head CT showed no acute pathology including being negative for an acute bleed. Emergent cardiac catheterisation revealed normal coronary arteries. His ECG revealed normal global left ventricular (LV) function without LV dilation or significant valvular abnormalities. A cardiac MRI showed no late gadolinium hyperenhancement or abnormalities in T1/T2 images.
Figure 1.
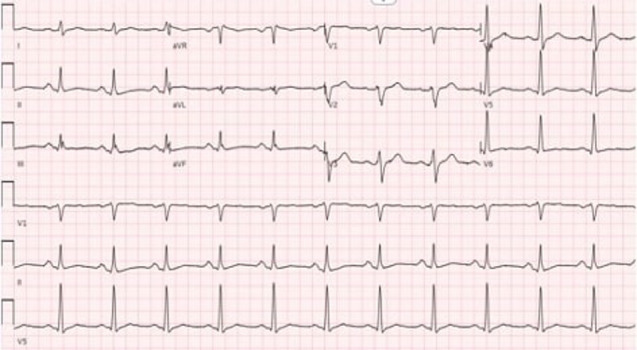
ECG showing QT interval >480 ms with a heart rate of 75 at paper speed of 25 mm/s.
Figure 2.

Severe congestion seen on portable anteroposterior view chest X-ray.
Differential diagnosis
Myocardial infarction with non-obstructive coronary arteries.
Idiopathic ventricular arrhythmia.
Cardiomyopathy secondary to infiltrative disease (haemochromatosis, amyloidosis).
Treatment
Targeted temperature management (TTM) was not used for this patient as he developed purposeful neurologic recovery after resuscitation. He was loaded with amiodarone for rhythm control and started on broad-spectrum antibiotics for aspiration pneumonia.
Outcome and follow-up
The patient was extubated, demonstrated mild retrograde amnaesia and a short-term memory difficulty which later improved prior to discharge. He received a subcutaneous defibrillator prior to discharge for secondary prevention with guidance to avoid supplement use, including Premium Maeng Da Kratom.
Discussion
Mitragyna speciosa, commonly known as kratom, is a tropical evergreen tree found in Southeast Asia that has been used in non-western medicine practices for generations. Due to some of its opiate-like properties, kratom has been used for managing chronic pain, especially for those who experience opioid withdrawal symptoms.1 However, there are no Food and Drug Administration approved uses for kratom, and the agency has previously expressed concerns about its safety, banning its use in 2016 but removing the ban in 2018, perhaps due to public backlash.2 Additionally, there is concern that labelling kratom as a Schedule I controlled substance could impede further research as well as lead to worsening public health issues.3 A literature review performed by Singh et al compared the reported side effects of kratom in Southeast Asia and the West. However, the literature from Southeast Asia was primarily from public surveys while the literature from the West consisted mostly of case reports. The authors comment that more studies are needed prior to undertaking any legal ramifications of kratom.4
The growing popularity of kratom worldwide has drawn major concerns from many states. Several countries in the European Union along with Australia, South Korea, Malaysia and Israel have enacted laws to better regulate kratom.5 The prevalence of kratom use in the USA is unclear, but some studies have found up to 20% of individuals with substance-use disorders have reported using kratom,6 a major concern for public health officials during the current opioid epidemic. A retrospective review conducted by Eggleston et al revealed 2312 cases of kratom exposure in the USA reported to the National Poison Data System between 2011 and 2018. They also note that the number of cases in 2011 was only 18 but increased to 357 in 2018.7 A recent survey by Garcia-Romeu et al found that in the USA most users of kratom found over 90% of responders were Caucasian with a mean age of 40.8 We can conclude from this information that while there is still much to be learnt about the overall public use of kratom, its popularity in the USA and other areas of the world is increasing with demographics that extend beyond usage by the Asian community.
Both leaves and extracts of kratom have been used in traditional remedies for coughs, gastrointestinal symptoms, musculoskeletal pain and as a local anaesthetic. However, due to its psychoactive effects, kratom has also been abused in combination with caffeine and codeine. The plant’s active constituents include the alkaloids mitragynine and 7-hydroxymitragine.9 At high doses, both act as partial agonists to the mu-opioid receptors as well as competitive antagonists to the kappa-opioid and delta-opioid receptors.10 They also potentiate alpha-2 receptors, a potential cause of kratom’s stimulating effect.11
There are multiple reports of fatal outcomes in patients who ingested kratom. Autopsy findings from multiple deaths attributed to kratom have reported pulmonary congestion and oedema as well as urinary retention, which is consistent with findings from autopsies in opiate overdose cases.12–14 There are also reports that kratom can prolong the QT interval, increasing the risk for ventricular arrhythmias.15 The combination of these adverse effects is the hypothesised mechanism behind cardiac arrest. However, there is minimal data in the literature thus far to confirm this hypothesis.
Treatment in these cases is mostly supportive, though some have expired prior to or on arrival to the emergency room.12 13 In a case presented by Matson and Schenk, naloxone was given in the field to a 33-year-old patient who developed cardiac arrest from kratom ingestion, but with no meaningful response.12 Aggarwal et al presented a case in which lipid emulsion was used on a 26-year-old man who presented in similar fashion 24 hours after ingesting kratom with initial improvement in his oxygenation status but ultimate deterioration.16 Abdullah et al reported a patient in whom use of TTM resulted in improvement and ultimate discharge.15 Our patient responded to supportive care without receiving any of the interventions listed above. Given the lack of literature on the subject, it cannot yet be stated as fact which of these interventions, if any, is most beneficial to these patients.
The question of whether or not the patient’s consumption of energy drinks contributed to his condition remains uncertain. A causal relationship between energy drinks and cardiac events has not been defined in a well-designed prospective study. A statement from the European Cardiac Arrhythmia Society analysed 22 case reports of cardiac events in patients who consumed energy drinks, 8 of which developed life-threatening arrhythmias. And while there is concern based on these events, definitive causal relationship has yet to be identified.17
Learning points.
Kratom is a substance used for chronic pain.
While it has opiate-like properties, there is a potential for QT prolongation which can pre-dispose healthy individuals to ventricular arrhythmias.
Continued vigilance for the role of kratom use and its potential to cause life-threatening arrhythmias is warranted.
Footnotes
MS and NA contributed equally.
Contributors: MS and NA were involved in the clinical care of the patient and in the preparation of the manuscript. HG and OC were involved in preparation and editing of the manuscript.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Patient consent for publication: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Cinosi E, Martinotti G, Simonato P, et al. Following "the Roots" of Kratom (Mitragyna speciosa): The Evolution of an Enhancer from a Traditional Use to Increase Work and Productivity in Southeast Asia to a Recreational Psychoactive Drug in Western Countries. Biomed Res Int 2015;2015:1–11. 10.1155/2015/968786 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Administration FaD . FDA and kratom: U.S. food and drug administration, 2019. Available: https://www.fda.gov/news-events/public-health-focus/fda-and-kratom
- 3.Prozialeck WC, Avery BA, Boyer EW, et al. Kratom policy: the challenge of balancing therapeutic potential with public safety. Int J Drug Policy 2019;70:70–7. 10.1016/j.drugpo.2019.05.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Singh D, Narayanan S, Vicknasingam B. Traditional and non-traditional uses of Mitragynine (Kratom): a survey of the literature. Brain Res Bull 2016;126:41–6. 10.1016/j.brainresbull.2016.05.004 [DOI] [PubMed] [Google Scholar]
- 5.Warner ML, Kaufman NC, Grundmann O. The pharmacology and toxicology of kratom: from traditional herb to drug of abuse. Int J Legal Med 2016;130:127–38. 10.1007/s00414-015-1279-y [DOI] [PubMed] [Google Scholar]
- 6.Smith KE, Lawson T. Prevalence and motivations for kratom use in a sample of substance users enrolled in a residential treatment program. Drug Alcohol Depend 2017;180:340–8. 10.1016/j.drugalcdep.2017.08.034 [DOI] [PubMed] [Google Scholar]
- 7.Eggleston W, Stoppacher R, Suen K, et al. Kratom use and toxicities in the United States. Pharmacotherapy 2019;39:775–7. 10.1002/phar.2280 [DOI] [PubMed] [Google Scholar]
- 8.Garcia-Romeu A, Cox DJ, Smith KE, et al. Kratom (Mitragyna speciosa): user demographics, use patterns, and implications for the opioid epidemic. Drug Alcohol Depend 2020;208:107849. 10.1016/j.drugalcdep.2020.107849 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rech MA, Donahey E, Cappiello Dziedzic JM, et al. New drugs of abuse. Pharmacotherapy 2015;35:189–97. 10.1002/phar.1522 [DOI] [PubMed] [Google Scholar]
- 10.Kruegel AC, Grundmann O. The medicinal chemistry and neuropharmacology of kratom: a preliminary discussion of a promising medicinal plant and analysis of its potential for abuse. Neuropharmacology 2018;134:108–20. 10.1016/j.neuropharm.2017.08.026 [DOI] [PubMed] [Google Scholar]
- 11.White CM. Pharmacologic and clinical assessment of kratom. Am J Health Syst Pharm 2018;75:261–7. 10.2146/ajhp161035 [DOI] [PubMed] [Google Scholar]
- 12.Matson M, Schenk N. Fatality of 33-year-old man involving Kratom toxicity. J Forensic Sci 2019;64:1933–5. 10.1111/1556-4029.14082 [DOI] [PubMed] [Google Scholar]
- 13.McIntyre IM, Trochta A, Stolberg S, et al. Mitragynine 'Kratom' related fatality: a case report with postmortem concentrations. J Anal Toxicol 2015;39:152–5. 10.1093/jat/bku137 [DOI] [PubMed] [Google Scholar]
- 14.Neerman MF, Frost RE, Deking J. A drug fatality involving Kratom. J Forensic Sci 2013;58 Suppl 1:S278–9. 10.1111/1556-4029.12009 [DOI] [PubMed] [Google Scholar]
- 15.Abdullah HMA, Haq I, Lamfers R. Cardiac arrest in a young healthy male patient secondary to kratom ingestion: is this 'legal high' substance more dangerous than initially thought ? BMJ Case Rep 2019;12:e229778. 10.1136/bcr-2019-229778 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Aggarwal G, Robertson E, McKinlay J, et al. Death from Kratom toxicity and the possible role of intralipid. J Intensive Care Soc 2018;19:61–3. 10.1177/1751143717712652 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lévy S, Santini L, Capucci A, et al. European cardiac arrhythmia Society statement on the cardiovascular events associated with the use or abuse of energy drinks. J Interv Card Electrophysiol 2019;56:99–115. 10.1007/s10840-019-00610-2 [DOI] [PubMed] [Google Scholar]