

Summary
COVID‐19 has critically impacted the world. Recent works have found substantial changes in sleep and mental health during the COVID‐19 pandemic. Dreams could give us crucial information about people's well‐being, so here we have directly investigated the consequences of lockdown on the oneiric activity in a large Italian sample: 5,988 adults completed a web‐survey during lockdown. We investigated sociodemographic and COVID‐19‐related information, sleep quality (by the Medical Outcomes Study‐Sleep Scale), mental health (by the Depression, Anxiety, and Stress Scales), dream and nightmare frequency, and related emotional aspects (by the Mannheim Dream Questionnaire). Comparisons between our sample and a population‐based sample revealed that Italians are having more frequent nightmares and dreams during the pandemic. A multiple logistic regression model showed the predictors of high dream recall (young age, female gender, not having children, sleep duration) and high nightmare frequency (young age, female gender, modification of napping, sleep duration, intrasleep wakefulness, sleep problem index, anxiety, depression). Moreover, we found higher emotional features of dream activity in workers who have stopped working, in people who have relatives/friends infected by or who have died from COVID‐19 and in subjects who have changed their sleep habits. Our findings point to the fact that the predictors of high dream recall and nightmares are consistent with the continuity between sleep mentation and daily experiences. According to the arousal‐retrieval model, we found that poor sleep predicts a high nightmare frequency. We suggest monitoring dream changes during the epidemic, and also considering the implications for clinical treatment and prevention of mental and sleep disorders.
Keywords: adverse events, continuity hypothesis, health, mental sleep activity, sleep
1. INTRODUCTION
Since December 2019, the new coronavirus (COVID‐19) has critically impacted the world. The virus has shown a rapid spread and many countries have adopted extremely restrictive measures (e.g., home confinement and social distancing) to contain diffusion of the virus. The Italian government imposed a lockdown from 9 March to 4 May, and people's lifestyles underwent remarkable changes (Altena et al., 2020). Modifications of sleep habits, feelings of fear and mood alterations were reported during lockdown by recent studies both in Italy (Casagrande et al., 2020; Cellini et al., 2020) and other countries (Blume et al., 2020; Wright et al., 2020; Xiao et al., 2020).
Since the beginning of the COVID‐19 lockdown, many people worldwide have spontaneously reported recalling more vivid dreams and complained of nightmares on social media platforms and websites. However, to date very few studies have directly assessed the pandemic's impact on dream activity. Some authors have suggested that the pandemic experience could be considered a traumatic event, as evidenced by a high proportion of post‐traumatic stress disorder (PTSD)‐like symptoms in Italy (Forte et al., 2020), as well as in China (Sun et al., 2020) during this period. Accordingly, nightmares could be considered consequences of PTSD (Germain, 2013). In this vein, previous investigations have shown modifications in dream patterns and increased nightmares in association with adverse events, such as wars and infectious diseases (Hartmann & Brezler, 2008; Nielsen et al., 2006; Sandman et al., 2013; Tempesta et al., 2013). Pesonen et al. (2020) explored dream contents during the lockdown in Finland. By using network analysis, they revealed that many pandemic‐related factors were linked to distressing events.
Furthermore, a survey completed by 3,031 US subjects revealed that people most affected by the pandemic had higher dream recall, more negative content in their dreams and pandemic‐related content (Schredl & Bulkeley, 2020). The authors also observed a large negative effect on those of female gender and people with a higher education level (Schredl & Bulkeley, 2020). Dream imagery during the early phase of the COVID‐19 pandemic was investigated among Canadian university students (MacKay & DeCicco, 2020). The students reported higher dream experiences characterized by location changes, animals and virus‐related contents. In keeping with previous studies (Miller et al., 2017), the authors suggested that this type of mental sleep activity is related to anxiety experienced during wakefulness (MacKay & DeCicco, 2020).
To our knowledge, only one study assessed dream activity in an Italian sample (Iorio et al., 2020). A relatively small sample of participants (N = 796) completed a dream questionnaire and reported their most recent dream. The results revealed that women's dreams are characterized by higher dream recall frequency, higher emotion and negative emotional tone as compared with men (Iorio et al., 2020). Also, subjects with COVID‐19‐infected/dead relatives or friends reported dreams with high emotional intensity and sensory impressions (Iorio et al., 2020).
Because dreaming and emotional processing are tightly linked, and dreams can reflect emotional waking experiences (Scarpelli et al., 2019), we would expect that frightening dreams may increase during a pandemic.
Here, we investigated the impact of the pandemic on dreaming in a very large Italian sample. Specifically, we aimed to:
assess whether Italian people actually had higher dream and nightmare frequencies during the pandemic, as compared with a population‐based sample (Settineri et al., 2019);
identify the sociodemographic and COVID‐related aspects and psychological and sleep measures that predict the frequency of dreams and nightmares during the lockdown;
evaluate the qualitative‐emotional features of dreams and nightmares in the different groups, divided according to COVID‐related aspects.
We hypothesized that psychological symptoms during wake might impact dream activity, especially by increasing the frequency of nightmares. Moreover, we hypothesized that lower sleep quality was related to higher dream activity. Finally, we expected that subjects whose daytime life is more affected by the COVID‐19 pandemic and who have experienced COVID‐19‐related traumatic events (e.g., infected/dead relatives or friends) have more emotional dreams with a more negative tone.
2. METHODS
2.1. Participants and protocol
Subjects completed a cross‐sectional online survey on the Microsoft Azure platform specifically developed for the COVID‐19 pandemic health emergency. The survey took approximately 30 min and was available for a limited period: from 10 March to 4 May (end of lockdown). Only adults (aged ≥18 years) living in Italy were included in the study.
The survey study was publicized via university communication systems as well as online forums. For instance, virtual learning environments, Facebook accounts or WeChat groups were used to promote the online survey. The general aim of the project was explained to the participants in the online advertisement (see the Supporting information).
Participants were requested to fill out a short self‐administered questionnaire on sociodemographic and COVID‐19 related information, along with self‐administered questionnaires to assess psychological and sleep variables in the web form. All individuals signed an electronic informed consent before filling out the survey. The subjects also explicitly agreed to provide an email contact and created an identification code to anonymize it. Participants could withdraw from the study at any moment, and no data were saved. The study was conducted in compliance with the Declaration of Helsinki and was approved by the Research Ethics Committee for Psychological Research of the University of Messina, Italy (no. 37442).
A total of 6,519 subjects completed the survey, and 531 subjects were excluded for several reasons (43 non‐Italian; 48 infected by COVID‐19; 440 missing data). The final sample consisted of 5,988 subjects (91.85% of respondents).
Data reported in the current study were part of a wider project, 'Resilience and the COVID‐19: how to react to perceived stress. Effects on sleep quality and diurnal behavior/thoughts', with different purposes regarding the impact of lockdown on the Italian population. Other data with different objectives have been presented elsewhere (Franceschini et al., 2020).
2.2. Outcomes
The webform was composed of four sections:
2.2.1. Sociodemographic and COVID‐related information
The variables collected in this section included: age, gender, marital status, presence/absence of children, education level, occupation, Italian area, cohabitants during lockdown, still working during lockdown, COVID‐19‐infected relatives or friends, relatives or friends who died from COVID‐19, forced quarantine period, COVID‐19 positivity, and modification of sleep habits (i.e., changes in the timing of sleep onset and morning awaking; changes in daytime napping compared to the pre‐lockdown period).
2.2.2. Psychological symptoms: The Depression Anxiety Stress Scale‐21
The Italian version of the Depression Anxiety Stress Scale‐21 (DASS‐21; short form; Bottesi et al., 2015) is a self‐report questionnaire in which participants rate the frequency and severity of depression, anxiety and stress symptoms. A detailed description of the questionnaire has been reported in the Supporting information.
All three subscales (depression, anxiety and stress symptoms) were considered for further analysis.
2.2.3. Sleep measures: The Medical Outcomes Study—Sleep Scale
The Medical Outcomes Study—Sleep Scale (MOS‐SS, Italian adaptation; Palagini & Manni, 2016) is a self‐administered questionnaire with 12 items to assess sleep quality and quantity within 4 weeks (details in the online Supporting information).
Here, three variables were extracted from the MOS‐SS for further analyses: (a) the Sleep Index II or sleep problem index, an aggregate measure of responses concerning four sleep domains (sleep disturbance, awakening with shortness of breath or with headache, sleep adequacy and somnolence), as a synthetic measure of sleep quality; (b) a sleep duration (item 2); and (c) self‐reported evaluation of intrasleep wakefulness (item 8), dichotomized as follows: ‘‘high intrasleep wakefulness’’ (answer 3, 4 or 5) and ‘‘low intrasleep wakefulness’’ (answer 1 or 2).
2.2.4. Dream variables: The Mannheim Dream Questionnaire
The Mannheim Dream Questionnaire (MADRE, Italian adaptation; Settineri et al., 2019) is a questionnaire with 20 self‐reported items about dreams and related phenomena (details in the Supporting information).
In the current study, we focused on items examining state variables of mental sleep activity (i.e., items 1, 2, 3, 4 and 5). In light of the previous literature, item 1 was dichotomized to discriminate high and low dream recall (Eichenlaub et al., 2014) as follows: ‘‘low recall’’ (answer from 0 [never] to 4 [about once a week]) and ‘‘high recall’’ (answer from 5 [several times a week] to 6 [almost every morning]). Similarly, considering previous studies, item 4 was dichotomized to distinguish frequent from non‐frequent nightmares (Schredl & Göritz, 2018), as follows: ‘‘non‐frequent nightmares’’ (answer from 0 [never] to 5 [about two/three times a month]) and ‘‘frequent nightmares’’ (answer from 6 [about once a week] to 7 [several times a week]).
2.3. Statistical analysis
All the data were analysed using the Statistical Package for Social Sciences (spss) version 20.0.
Descriptive analyses were conducted to outline the sociodemographic characteristics of the sample, as well as COVID‐19 related aspects, considering the following features: age, gender, marital status, education level, occupation, Italian area, cohabitants, still working during the lockdown, COVID‐19‐infected relatives or friends, relatives or friends who died from COVID‐19, forced quarantine period, and modification of sleep habits (sleep onset, morning awakenings, daytime napping).
The chi‐squared test was used to compare the two distributions (pandemic Italian sample versus population‐based sample) of the answers to item 1 (dream recall frequency [DRF]) and item 4 (nightmare frequency [NF]) in order to assess whether dream and nightmare frequency during the lockdown period differ from that reported in the population‐based Italian sample (Settineri et al., 2019). The population‐based group in the Settineri et al. (2019) dataset included 623 subjects (57% female; mean age ± standard deviation, 38.26 ± 14.71). This sample was recruited from two degree courses at the University of Messina.
Two binary multivariable logistic regression models were performed to explore the role of sociodemographic variables, COVID‐related aspects, and psychological and sleep measures on the DRF (item 1) and NF (item 4). We entered the variables simultaneously and calculated the adjusted odds ratio (aOR) to control for other predictor variables in the model.
The following variables were tested as potential predictors of dream and nightmare frequency: age; gender (male; female); Italian area (north; centre‐south); cohabitants (alone; no); having children (yes; no); days of lockdown; still working (yes; no); COVID‐19‐infected relatives or friends (yes; no); relatives or friends who have died from COVID‐19 (yes; no); forced quarantine period (yes; no); modification of sleep habits at sleep onset (yes; no); modifications of sleep habits at morning awakenings (yes; no); modification of daytime napping (yes; no); total sleep duration; intrasleep wakefulness; sleep problem index; anxiety, depression and stress scores.
Before running logistic analyses, we checked for multicollinearity among the independent variables. The false discovery rate (FDR) correction (Benjamini & Hochberg, 1995) was applied to adjust the α‐value (adjusted critical p = 0.0005 for the regression model predicting DR; adjusted critical p = 0.010 for the regression model predicting NR).
Finally, unpaired t tests were computed to assess the qualitative‐emotional dream and nightmare features among groups obtained on the basis of the COVID‐related aspects (still working; COVID‐19‐infected relatives or friends; relatives or friends who have died from COVID‐19; forced quarantine period; modifications of sleep habits at sleep onset; modifications of sleep habits at morning awakening; modifications of daytime napping). We considered emotional intensity and tone (items 2 and 3) and nightmare distress (item 5) as dependent variables. Before applying the above tests, the assumptions of normality or variances were checked. FDR correction (Benjamini & Hochberg, 1995) was applied to adjust the α‐value for multiple comparisons (adjusted critical p = 0.018).
3. RESULTS
3.1. Demographic and COVID‐related characteristics
The characteristics of participants are shown in Table 1. In short, data from 5,988 subjects revealed that the most represented age range was 18–25 years (40.8%; mean age ± standard deviation [SD], 33.54 ± 13.53) and most of the participants were female (73.3%). Among all respondents, 35% were single, 25.2% were married, 26.3% were engaged, and a small percentage were cohabiting (9.1%) or divorced/separated/widower (4.5%); most of the individuals received a high school education (47.5%) and were employed (51.5%); 4,009 individuals (67%) came from north Italy; 28.6% of the sample had children; most of the participants had at least one cohabitant during lockdown (92.8%); concerning job changes, 52.6% had stopped working during the lockdown; among respondents, 13.7% had COVID‐19‐infected relatives or friends and 6.4% had relatives or friends who had died from COVID‐19; a forced quarantine period was prescribed to 444 individuals (7.4%); and finally, most participants reported modifications in their sleep habits (60.9% at sleep onset, 63.5% at morning awakening and 60.8% in daytime napping).
TABLE 1.
Demographic characteristics and COVID‐related features
| N (overall sample: 5,988) | % | |
|---|---|---|
| Age, years | ||
| >60 | 228 | 3.8 |
| 18–25 | 2,442 | 40.8 |
| 26–30 | 964 | 16.1 |
| 31–40 | 855 | 14.3 |
| 41–50 | 741 | 12.4 |
| 51–60 | 758 | 12.7 |
| Gender | ||
| Male | 1,596 | 26.7 |
| Marital status | ||
| Single | 2,095 | 35.0 |
| Married | 1,506 | 25.2 |
| Cohabiting | 546 | 9.1 |
| Engaged | 1,573 | 26.3 |
| Divorced/separated/widower | 268 | 4.5 |
| Education level | ||
| Until middle school | 207 | 3.5 |
| High school | 2,846 | 47.5 |
| Bachelor's degree | 1,125 | 18.8 |
| Master's degree | 1,344 | 22.4 |
| PhD/postgraduate school | 466 | 7.8 |
| Occupation | ||
| Student | 2,521 | 42.1 |
| Employed | 3,085 | 51.5 |
| Retired | 108 | 1.8 |
| Unemployed | 274 | 4.6 |
| Italian area | ||
| North Italy | 4,009 | 67.0 |
| Having children | ||
| Yes | 1,713 | 28.6 |
| Cohabitants during lockdown | ||
| Yes | 5,557 | 92.8 |
| Still working during lockdown | ||
| Yes | 3,152 | 47.4 |
| COVID‐19‐infected relatives or friends | ||
| Yes | 821 | 13.7 |
| COVID‐19‐died relatives or friends | ||
| Yes | 385 | 6.4 |
| Forced quarantine period | ||
| Yes | 444 | 7.4 |
| Modification of sleep habits (sleep onset) | ||
| Yes | 3,645 | 60.9 |
| Modification of sleep habits (morning awakenings) | ||
| Yes | 3,803 | 63.5 |
| Modification of sleep habits (daytime nap) | ||
| Yes | 3,640 | 60.8 |
3.2. Comparison between Italian population‐based and pandemic sample
The distributions of dream recall and nightmare frequency for population‐based and pandemic samples are depicted in Figure 1a,b. Statistical comparisons by chi‐squared test showed that the distribution of DRF of the pandemic sample differs significantly from that of the population‐based Italian sample (chi‐squared = 745.06; p < 0.001). Similarly, the distributions of NF in population‐based and pandemic sample are significantly different (chi‐squared = 713.81; p < 0.001). Figure 1 illustrates that the answers indicating low dream recall (Figure 1a) and low nightmare (Figure 1b) frequency show higher percentages in the population‐based sample than in the pandemic one. Inversely, the answers indicating high dream recall (Figure 1a) and high nightmare (Figure 1b) frequency show lower percentages in the population‐based than the pandemic sample.
FIGURE 1.
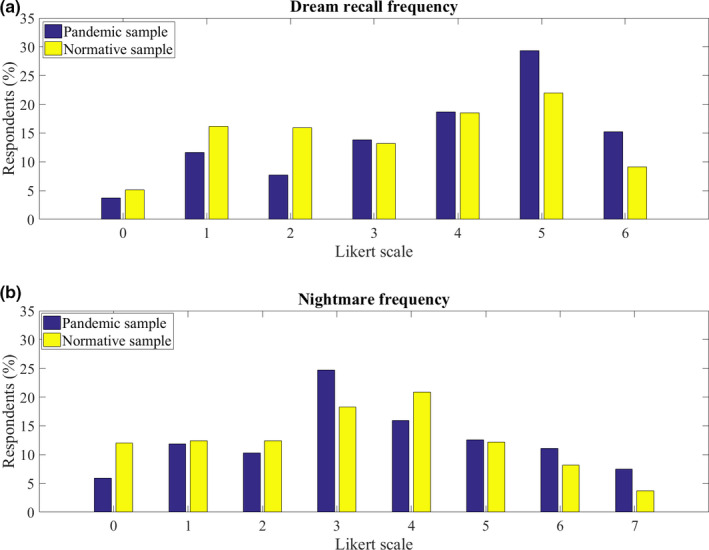
Distributions of dream recall and nightmare frequency for population‐based and pandemic samples. (a) The percentage distribution of respondent scores on a Likert scale (0–6) about dream recall frequency, in population‐based (yellow bars) and pandemic (blue bars) samples. (b) The percentage distribution of respondent scores on a Likert scale (0–7) about nightmare frequency, in population‐based (yellow bars) and pandemic (blue bars) samples
3.3. Predictors of pandemic dream activity
Multiple binary logistic regression analyses on DRF as the outcome provided a significant model (likelihood ratio: chi‐squared = 397.312, p < .001; Negelkerke's R 2 = 0.086). The results (see Figure 2 and Table S1) showed that age (p < 0.0001; odds ratios [aOR], 0.985; 95% confidence intervals [CI], 0.979–0.991), gender (p < 0.0001; aOR, 2.035; CI, 1.790–2.312), having children (p = 0.0005; aOR, 0.728; CI, 0.609–0.870) and sleep duration (p < 0.0001; aOR, 1.107; CI, 1.059–1.158) were significant predictors of DRF. Specifically, younger age, female gender, not having children and higher sleep duration were associated with higher DRF. No other variable predicted DRF.
FIGURE 2.
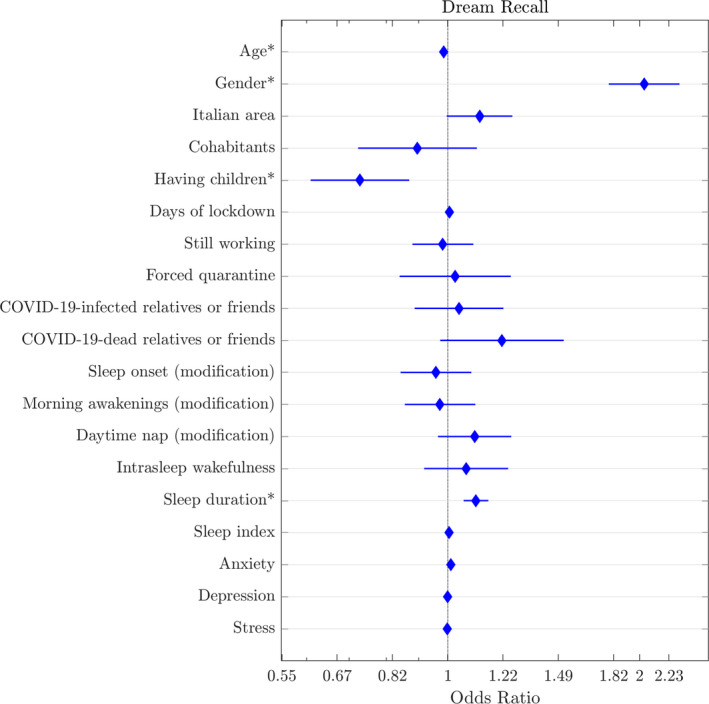
Multiple binary logistic regression model with dream recall frequency (high and low dream recall frequency) as dependent variable. Graphic representation of odds ratio and relative 95% confidence intervals for each predictor: age, gender (reference: male), Italian area (reference: north), cohabitants (reference: alone), having children (reference: no), days of lockdown, still working during lockdown (reference: no), COVID‐19‐infected relatives or friends (reference: no), relatives or friends who have died from COVID‐19 (reference: no), forced quarantine period (reference: no), modification of sleep habits at sleep onset (reference: no), modification of sleep habits at morning awakenings (reference: no), modifications in daytime napping (reference: no), intrasleep wakefulness (reference: low), sleep duration, sleep problem index, and anxiety, depression and stress scores. Independent significant predictors for each outcome are marked with asterisks
Multiple binary logistic regression analyses on NF as the outcome provided a significant model (likelihood ratio: chi‐squared = 819.012, p < 0.001; Negelkerke's R 2 = 0.207). The results (see Figure 3 and Table S2) showed that age (p < 0.0001; aOR, 0.972; CI, 0.963–0.982), gender (p < 0.0001; aOR, 1.825; CI, 1.504–2.213), daytime napping (p = 0.001; aOR, 1.351; CI, 1.133–1.612), intrasleep wakefulness (p = 0.010; aOR, 1.282; CI, 1.062–1.546); sleep duration (p = 0.001; aOR, 1.096; CI, 1.038–1.158), the sleep problem index (p < 0.0001; aOR, 1.023; CI, 1.017–1.029), anxiety score (p = 0.001; aOR, 1.021; CI, 1.009–1.034) and depression score (p = 0.001; aOR, 1.019; CI, 1.008–1.030) are significant predictors of NF. Specifically, younger age, female gender, modification of daytime napping, high intrasleep wakefulness, higher sleep duration, higher sleep problem index score, higher anxiety and depressive symptoms are associated with higher NF. No other variable predicted NF.
FIGURE 3.
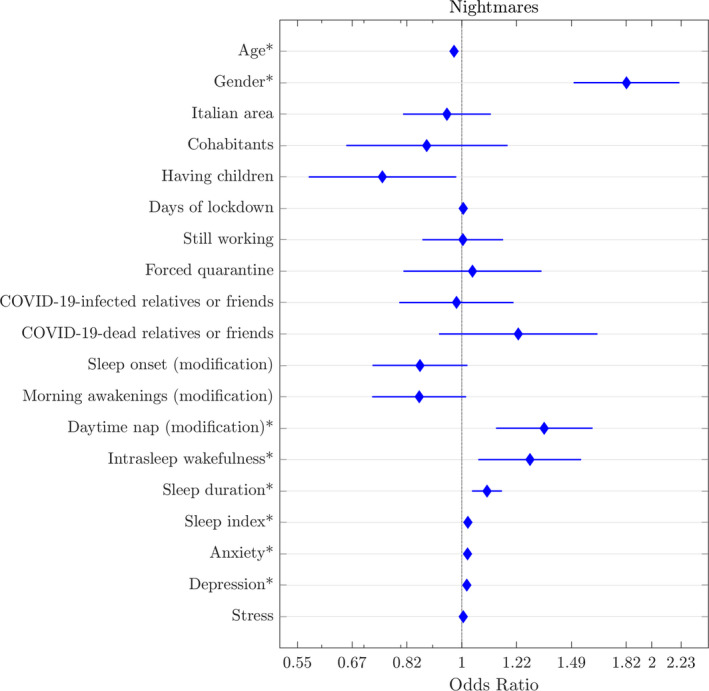
Multiple binary logistic regression model with nightmare frequency (high and low nightmare frequency) as dependent variable. Graphic representation of odds ratio and relative 95% confidence intervals for each predictor: age, gender (reference: male), Italian area (reference: north), cohabitants (reference: alone), having children (reference: no), days of lockdown, still working during lockdown (reference: no), COVID‐19‐infected relatives or friends (reference: no), relatives or friends who have died from COVID‐19 (reference: no), forced quarantine period (reference: no), modification of sleep habits at sleep onset (reference: no), modification of sleep habits at morning awakenings (reference: no), modifications in daytime napping (reference: no), intrasleep wakefulness (reference: low), sleep duration, sleep problem index, and anxiety, depression and stress scores. Independent significant predictors for each outcome are marked with asterisks
3.4. Emotional features of pandemic dream activity
Table 2 reports the group differences in emotional features of dream activity during the lockdown. People who had stopped working showed higher emotional intensity (t = 2.36; p = 0.018), higher negative emotional tone (t = −2.60; p = 0.009) and nightmare distress (t = 3.81; p < 0.001), compared to individuals who kept working. People having COVID‐19‐infected relatives or friends and relatives or friends who had died from COVID‐19 reported more nightmare distress than individuals not having these traumatic experiences (t = −3.59; p < 0.001 and t = −2.61; p = 0.009, respectively).
TABLE 2.
Mean and standard deviation (SD) of emotional intensity, emotional tone and nightmare distress for each group divided according COVID‐related aspects and results of statistical comparisons by unpaired t test. Significant effects are marked with asterisks (adjusted critical p = 0.018)
| Emotional intensity | Emotional tone | Nightmare distress | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | t‐values (p‐values) | Cohen's d | Mean (SD) | t‐values (p‐values) | Cohen's d | Mean (SD) | t‐values (p‐values) | Cohen's d | |
| Still working during lockdown | |||||||||
| Yes | 2.27 (1.088) | 2.361 (0.018*) | 0.064 | −0.04 (0.811) | −2.600 (0.009*) | 0.061 | 1.65 (1.064) | 3.806 (0.000*) | 0.103 |
| No | 2.34 (1.078) | −0.09 (0.807) | 1.76 (1.068) | ||||||
| Forced quarantine period | |||||||||
| Yes | 2.32 (1.090) | −0.257 (0.797) | 0.018 | −0.09 (0.822) | 0.700 (0.484) | 0.036 | 1.71 (1.016) | −0.107 (0.915) | 0.009 |
| No | 2.30 (1.083) | −0.06 (0.809) | 1.70 (1.071) | ||||||
| COVID‐19‐infected relatives or friends | |||||||||
| Yes | 2.33 (1.079) | −0.921 (0.357) | 0.027 | −0.06 (0.827) | −0.226 (0.821) | 0 | 1.83 (1.084) | −3.587 (0.000*) | 0.139 |
| No | 2.30 (1.084) | −0.06 (0.807) | 1.68 (1.064) | ||||||
| COVID‐19‐died relatives or friends | |||||||||
| Yes | 2.38 (1.071) | −1.434 (0.152) | 0.074 | −0.05 (0.854) | −0.316 (0.752) | 0.012 | 1.84 (1.103) | −2.611 (0.009*) | 0.138 |
| No | 2.30 (1.084) | −0.06 (0.807) | 1.69 (1.064) | ||||||
| Modification of sleep onset | |||||||||
| Yes | 2.36 (1.079) | −4.897 (0.000*) | 0.129 | −0.10 (0.817) | 4.231 (0.000*) | 0.111 | 1.79 (1.073) | −7.452 (0.000*) | 0.198 |
| No | 2.22 (1.085) | −0.01 (0.795) | 1.58 (1.046) | ||||||
| Modification of morning awakenings | |||||||||
| Yes | 2.34 (1.075) | −3.253 (0.001*) | 0.092 | −0.08 (0.816) | 2.633 (0.008*) | 0.061 | 1.74 (1.057) | −3.771 (0.000*) | 0.093 |
| No | 2.24 (1.096) | −0.03 (0.797) | 1.64 (1.081) | ||||||
| Modification of daytime nap | |||||||||
| Yes | 2.31 (1.091) | −1.039 (0.299) | 0.027 | −0.08 (0.825) | 2.043 (0.041) | 0.049 | 1.74 (1.081) | −3.464 (0.001*) | 0.094 |
| No | 2.28 (1.073) | −0.04 (0.784) | 1.64 (1.044) | ||||||
Subjects who reported modification at sleep onset had higher emotional intensity (t = −4.90; p < 0.001), a more negative tone (t = 4.23; p < 0.001) and higher nightmare distress (t = −7.45; p < 0.001) than people not reporting changes. Similarly, people who changed habits at morning awakening had higher emotional intensity (t = −3.25; p = 0.001), more negative tone (t = 2.63; p = 0.008) and higher nightmare distress (−3.77 p < 0.001 than people not reporting changes. People who changed napping habits reported higher nightmare distress (t = −3.46; p = 0.001) than people without modifications in daytime napping.
No difference was found between groups divided according to the forced quarantine period.
4. DISCUSSION
This is the first study investigating quantitative and qualitative aspects of dream activity during the spring 2020 lockdown in a large Italian sample. The current results show increased dream recall and nightmare frequency, as compared with a population‐based sample. Furthermore, we showed that specific sociodemographic characteristics along with COVID‐19‐related changes in psychological symptoms and sleep quality were able to impact dream and nightmare frequency during the lockdown. In line with our expectations, our results suggest a higher predictive power for nightmare frequency.
Consistently, many studies have highlighted that, after experiencing traumatic or stressful events, dreams underwent significant changes in their occurrence. Investigations on dream recall immediately after the 9/11 attacks revealed that people reported more intense dreams in that period (Hartmann & Brezler, 2008). More directly, a study in the Italian population showed that PTSD survivors of the L’Aquila earthquake living near the epicentre had more sleep disorders and nightmares (Tempesta et al., 2013). In line with our hypothesis, we found that both anxiety and depressive symptoms are positively associated with nightmares. During the day, a high level of anxiety could lead to more unpleasant dreams (Sikka et al., 2018). Accordingly, several aspects related to COVID‐19 are shrouded by fear and uncertainty. The scarce knowledge about this new virus, the absence of definitive treatment or vaccines, the fear of death and the economic collapse, are turning the pandemic into a sort of ‘‘collective trauma’’ (Forte et al., 2020). Moreover, home confinement and isolation may increase depressive feelings (Brooks et al., 2020), which may affect sleep and oneiric activity (Skancke et al., 2014).
Dreaming can reflect our inner suffering and is linked to memory mechanisms that could help us cope with the negative affects related to daytime life experiences. More directly, we explored the qualitative‐emotional features of dream activity, showing that people having COVID‐related traumatic experiences (death or illness of relatives or friends) reported increased distress associated with their oneiric contents. Similarly, groups with higher lifestyle modifications (in sleep habits or stopping working) showed greater emotion in their dreams. These findings are consistent with previous studies on pandemic dreams that highlighted the presence of high emotional intensity in people most affected by the pandemic (Schredl & Bulkeley, 2020) and individuals with death or illness of relatives or friends due to COVID‐19 (Iorio et al., 2020).
As a whole, in keeping with these findings and the well‐established hypothesis of continuity between cognitive processes during wakefulness and sleep (Schredl & Hofmann, 2003), we suggest that negative emotions during the lockdown could be incorporated in sleep mentation. In this vein, some authors have supposed that nightmares in the early aftermath of exposure to trauma could represent an attempt to metabolize and contextualize life changes and stressful events (Scarpelli et al., 2019b).
We also confirmed that sleep quality impacted dream activity. In particular, nightmares are associated with more significant sleep problems and intrasleep wakefulness. In this respect, Koulack and Goodenough (1976) claimed that sleep fragmentation and awakenings promote oneiric trace storage and recall (i.e., arousal‐retrieval model). In apparent contradiction with this result, we found that higher sleep duration predicts high dream activity (i.e., both DR and NR). Sleep–wake schedules were strongly affected by home confinement (Bottary et al., 2020), and multiple studies have found both increased sleep duration (Blume et al., 2020; Wright et al., 2020) and time spent in bed (Cellini et al., 2020; Wright et al., 2020) and a decrease in self‐reported sleep quality (Blume et al., 2020; Cellini et al., 2020). In line with electrophysiological evidence, we hypothesize that we are dealing with light and unstable sleep, probably characterized by cortical arousal and reduced slow‐wave activity (i.e., activation hypothesis; Scarpelli et al., 2017; van Wyk et al., 2019). Moreover, modifications to daytime napping predict higher NF. On the one hand, we could interpret this result as an expression of the multiple daily routine changes that may strongly affect dream activity. On the other, we could speculate that modifications to napping may be the consequence of changes in general sleep habits and quality (i.e., sleep extension and/or sleep fragmentation).
Quite surprisingly, our results show that having children predicts high DR. Considering that recent studies have suggested that COVID‐19‐related stressors can negatively impact parents' sleep (Peltz et al., 2020), the direction of our finding on DR and the lack of any effect for NR may appear counterintuitive. However, we did not have any information about the ages or numbers of children, which are crucial data for unravelling the issue of the impact of childcare at home on sleep and, consequently, dreaming.
In line with previous COVID‐19 dream studies (Barrett, 2020; Iorio et al., 2020; Schredl & Bulkeley, 2020), we showed that female gender and younger age are predictors of high DRF and NF. Indeed, sex differences in dream activity had been previously reported, evidencing that women have higher recall frequencies than men (Nielsen, 2012). Moreover, ageing is recognized as one of the key factors responsible for the drop in DR, and the frequency seems to be already reduced in early and middle adulthood (Scarpelli et al., 2019a). The decline was also observed for nightmares (Scarpelli et al., 2019a). The replication of these findings informs us about the goodness of our sample.
Nevertheless, it should be considered that the majority of the participants in the current study are women, so our sample cannot be considered as fully representative of the entire Italian population. However, this huge gender difference in the response rate to the web survey is similarly present in many COVID‐19 studies on sleep and dreaming (i.e., females make up around 70% of the sample; Casagrande et al., 2020; Cellini et al., 2020; McKay & DeCicco, 2020). The current investigation has the great advantage of including a large sample. However, we must underline some methodological constraints. Firstly, we did not collect dream contents but only self‐reported emotional features. This represents a limitation because we cannot directly assess the continuity between waking experiences and actual dream contents. Also, the information about sleep quality is not supported by any systematic sleep measures, neither daily sleep diaries nor objective measures. Moreover, our survey did not require information on any possible pharmacological treatment that can affect sleep and dreaming (Nicolas & Ruby, 2020).
Lastly, although we compared the actual distribution of DRF and NF with that of a population‐based Italian population, we are aware that the lack of a pre–post study design does not allow us to control potential confounding and stable factors unrelated to the epidemic (Nielsen, 2012; Scarpelli et al., 2019a). We should also mention that the comparison with the convenience sample by Settineri et al. (2019) should be made with caution as the recruitment strategy is very different and it is significantly smaller than our sample.
In conclusion, oneiric activity, such as sleep, can give us crucial information about people's well‐being (Scarpelli et al., 2019b; Sikka et al., 2018). Indeed, disturbing dreams and nightmares have been found to be signs of reactivation of PTSD symptoms in patients whose disorder was in remission during the lockdown period (Gupta, 2020).
Bearing in mind that the epidemic produced a real ‘‘psychiatric emergency’’, we suggest looking at oneiric activity from a clinical perspective. That is, future investigations should monitor the changes in dreams and nightmares across the pandemic, also considering the implications for clinical treatment and prevention of mental and sleep disorders.
CONFLICT OF INTEREST
GP served on advisory boards for Jazz, UCB, Bioprojet and Idorsia.
AUTHOR CONTRIBUTIONS
All the authors developed the study concept, contributed to the study design, data collection and data analysis, interpreted the data, drafted the manuscript and approved the final version for submission.
Supporting information
Supplementary Material
ACKNOWLEDGMENTS
This research received no specific grant from any funding agency, or commercial or not‐for‐profit sectors
Scarpelli S, Alfonsi V, Mangiaruga A, et al. Pandemic nightmares: Effects on dream activity of the COVID‐19 lockdown in Italy. J Sleep Res. 2021;30:e13300. 10.1111/jsr.13300
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon request.
REFERENCES
- Altena, E. , Baglioni, C. , Espie, C. A. , Ellis, J. , Gavriloff, D. , Holzinger, B. , Schlarb, A. , Frase, L. , Jernelöv, S. , & Riemann, D. (2020). Dealing with sleep problems during home confinement due to the COVID‐19 outbreak: Practical recommendations from a task force of the European CBT‐I Academy. Journal of Sleep Research, 29(4), e13052. 10.1111/jsr.13052 [DOI] [PubMed] [Google Scholar]
- Barrett, D. (2020). Dreams about COVID‐19 versus normative dreams: Trends by gender. Dreaming, 30(3), 216–221. 10.1037/drm0000149 [DOI] [Google Scholar]
- Benjamini, Y. , & Hochberg, Y. (1995). Controlling the false discovery rate: A practical and powerful approach to multiple testing. Journal of the Royal Statistical Society: Series B (Methodological), 57(1), 289–300. [Google Scholar]
- Blume, C. , Schmidt, M. H. , & Cajochen, C. (2020). Effects of the COVID‐19 lockdown on human sleep and rest‐activity rhythms. Current Biology, 30(14), 795–797. 10.1016/j.cub.2020.06.021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bottary, R. , Simonelli, G. , Cunningham, T. J. , Kensinger, E. A. , & Mantua, J. (2020). Sleep extension: An explanation for increased pandemic dream recall? Sleep, 43(11), 131. 10.1093/sleep/zsaa131 [DOI] [PubMed] [Google Scholar]
- Bottesi, G. , Ghisi, M. , Altoè, G. , Conforti, E. , Melli, G. , & Sica, C. (2015). The Italian version of the Depression Anxiety Stress Scales‐21: Factor structure and psychometric properties on community and clinical samples. Comprehensive Psychiatry, 60, 170–181. 10.1016/j.comppsych.2015.04.005 [DOI] [PubMed] [Google Scholar]
- Brooks, S. K. , Webster, R. K. , Smith, L. E. , Woodland, L. , Wessely, S. , Greenberg, N. , & Rubin, G. J. (2020). The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. The Lancet, 395(10227), 912–920. 10.1016/S0140-6736(20)30460-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Casagrande, M. , Favieri, F. , Tambelli, R. , & Forte, G. (2020). The enemy who sealed the world: Effects quarantine due to the COVID‐19 on sleep quality, anxiety, and psychological distress in the Italian population. Sleep Medicine, 75, 12–20. 10.1016/j.sleep.2020.05.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cellini, N. , Canale, N. , Mioni, G. , & Costa, S. (2020). Changes in sleep pattern, sense of time and digital media use during COVID‐19 lockdown in Italy. Journal of Sleep Research, 29(4), e13074. 10.1111/jsr.13074 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eichenlaub, J.‐B. , Nicolas, A. , Daltrozzo, J. , Redouté, J. , Costes, N. , & Ruby, P. (2014). Resting brain activity varies with dream recall frequency between subjects. Neuropsychopharmacology, 39(7), 1594–1602. 10.1038/npp.2014.6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Forte, G. , Favieri, F. , Tambelli, R. , & Casagrande, M. (2020). COVID‐19 pandemic in the Italian population: Validation of a post‐traumatic stress disorder questionnaire and prevalence of PTSD symptomatology. International Journal of Environmental Research and Public Health, 17(11), 4151. 10.3390/ijerph17114151 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Franceschini, C. , Musetti, A. , Zenesini, C. , Palagini, L. , Pelosi, A. , Quattropani, M. C. , & Vegni, E. (2020). Poor quality of sleep and its consequences on mental health during COVID‐19 lockdown in Italy. Frontiers in Psychology, 11, 3072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Germain, A. (2013). Sleep disturbances as the hallmark of PTSD: Where are we now? American Journal of Psychiatry, 170(4), 372–382. 10.1176/appi.ajp.2012.12040432 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gupta, M. A. (2020). Spontaneous reporting of onset of disturbing dreams and nightmares related to early life traumatic experiences during the COVID‐19 pandemic by patients with posttraumatic stress disorder in remission. Journal of Clinical Sleep Medicine, 16(8), 1419–1420. 10.5664/jcsm.8562 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hartmann, E. , & Brezler, T. (2008). A systematic change in dreams after 9/11/01. Sleep, 31(2), 213–218. 10.1093/sleep/31.2.213 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iorio, I. , Sommantico, M. , & Parrello, S. (2020). Dreaming in the time of COVID‐19: A quali‐quantitative Italian study. Dreaming, 30(3), 199. 10.1037/drm0000142 [DOI] [Google Scholar]
- Koulack, D. , & Goodenough, D. R. (1976). Dream recall and dream recall failure: An arousal‐retrieval model. Psychological Bulletin, 83(5), 975. 10.1037/0033-2909.83.5.975 [DOI] [Google Scholar]
- MacKay, C. , & DeCicco, T. L. (2020). Pandemic dreaming: The effect of COVID‐19 on dream imagery, a pilot study. Dreaming, 30(3), 222. 10.1037/drm0000148 [DOI] [Google Scholar]
- Miller, K. E. , Brownlow, J. A. , Woodward, S. , & Gehrman, P. R. (2017). Sleep and dreaming in posttraumatic stress disorder. Current Psychiatry Reports, 19(10), 71. 10.1007/s11920-017-0827-1 [DOI] [PubMed] [Google Scholar]
- Nicolas, A. , & Ruby, P. M. (2020). Dreams, sleep, and psychotropic drugs. Frontiers in Neurology, 11, 10.3389/fneur.2020.507495 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nielsen, T. (2012). Variations in dream recall frequency and dream theme diversity by age and sex. Frontiers in Neurology, 3, 106. 10.3389/fneur.2012.00106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nielsen, T. A. , Stenstrom, P. , & Levin, R. (2006). Nightmare frequency as a function of age, gender, and September 11, 2001: Findings from an Internet questionnaire. Dreaming, 16(3), 145. 10.1037/1053-0797.16.3.145 [DOI] [Google Scholar]
- Palagini, L. , & Manni, R. (2016). Misurare il sonno : Repertorio delle scale di valutazione dei disturbi del sonno (pp. 3–4). Minerva medica. [Google Scholar]
- Peltz, J. S. , Daks, J. S. , & Rogge, R. D. (2020). Mediators of the association between COVID‐19‐related stressors and parents’ psychological flexibility and inflexibility: The roles of perceived sleep quality and energy. Journal of Contextual Behavioral Science, 17, 168–176. 10.1016/j.jcbs.2020.07.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pesonen, A.‐K. , Lipsanen, J. , Halonen, R. , Elovainio, M. , Sandman, N. , Mäkelä, J.‐M. , & Kuula, L. (2020). Pandemic dreams: Network analysis of dream content during the COVID‐19 lockdown. Frontiers in Psychology, 11, 2569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sandman, N. , Valli, K. , Kronholm, E. , Ollila, H. M. , Revonsuo, A. , Laatikainen, T. , & Paunio, T. (2013). Nightmares: Prevalence among the Finnish general adult population and war veterans during 1972–2007. Sleep, 36(7), 1041–1050. 10.5665/sleep.2806 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scarpelli, S. , Bartolacci, C. , D’Atri, A. , Gorgoni, M. , & De Gennaro, L. (2019a). Mental sleep activity and disturbing dreams in the lifespan. International Journal of Environmental Research and Public Health, 16(19), 3658. 10.3390/ijerph16193658 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scarpelli, S. , Bartolacci, C. , D’Atri, A. , Gorgoni, M. , & De Gennaro, L. (2019b). The functional role of dreaming in emotional processes. Frontiers in Psychology, 10, 459. 10.3389/fpsyg.2019.00459 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scarpelli, S. , D’Atri, A. , Mangiaruga, A. , Marzano, C. , Gorgoni, M. , Schiappa, C. , Ferrara, M. , & De Gennaro, L. (2017). Predicting dream recall: EEG activation during NREM sleep or shared mechanisms with wakefulness? Brain Topography, 30(5), 629–638. 10.1007/s10548-017-0563-1 [DOI] [PubMed] [Google Scholar]
- Schredl, M. , & Bulkeley, K. (2020). Dreaming and the COVID‐19 pandemic: A survey in a US sample. Dreaming, 30(3), 189. 10.1037/drm0000146 [DOI] [Google Scholar]
- Schredl, M. , & Göritz, A. S. (2018). Nightmare themes: An online study of most recent nightmares and childhood nightmares. Journal of Clinical Sleep Medicine, 14(3), 465–471. 10.5664/jcsm.7002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schredl, M. , & Hofmann, F. (2003). Continuity between waking activities and dream activities. Consciousness and Cognition, 12(2), 298–308. 10.1016/S1053-8100(02)00072-7 [DOI] [PubMed] [Google Scholar]
- Settineri, S. , Frisone, F. , Alibrandi, A. , & Merlo, E. M. (2019). Italian adaptation of the Mannheim Dream Questionnaire (MADRE): Age, gender and dream recall effects. International Journal of Dream Research, 12(1), 119–129. [Google Scholar]
- Sikka, P. , Pesonen, H. , & Revonsuo, A. (2018). Peace of mind and anxiety in the waking state are related to the affective content of dreams. Scientific Reports, 8(1), 1–13. 10.1038/s41598-018-30721-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Skancke, J. F. , Holsen, I. , & Schredl, M. (2014). Continuity between waking life and dreams of psychiatric patients: A review and discussion of the implications for dream research. International Journal of Dream Research, 7(1), 39–53. [Google Scholar]
- Sun, L. , Sun, Z. , Wu, L. , Zhu, Z. , Zhang, F. , Shang, Z. , & Wang, Y. (2020). Prevalence and risk factors of acute posttraumatic stress symptoms during the COVID‐19 outbreak in Wuhan, China. Preprint from MedRxiv. 10.1101/2020.03.06.20032425 [DOI]
- Tempesta, D. , Curcio, G. , De Gennaro, L. , & Ferrara, M. (2013). Long‐term impact of earthquakes on sleep quality. PLoS One, 8(2), e55936. 10.1371/journal.pone.0055936 [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Wyk, M. , Solms, M. L. , & Lipinska, G. (2019). Increased awakenings from non‐rapid eye movement sleep explains differences in dream recall frequency in healthy high and low recallers. Frontiers in Human Neuroscience, 13, 370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wright, K. P. , Linton, S. K. , Withrow, D. , Casiraghi, L. , Lanza, S. M. , Iglesia, H. D. L. , Vetter, C. , & Depner, C. M. (2020). Sleep in university students prior to and during COVID‐19 stay‐at‐home orders. Current Biology, 30(14), 797–798. 10.1016/j.cub.2020.06.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Xiao, H. , Zhang, Y. , Kong, D. , Li, S. , & Yang, N. (2020). The effects of social support on sleep quality of medical staff treating patients with coronavirus disease 2019 (COVID‐19) in January and February 2020 in China. Medical Science Monitor, 26, e923549. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Material
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon request.