

Abstract
The study of any intervention able to counteract SARS‐CoV‐2 pandemic is considerably envisaged. It was previously shown, in in vitro models of infections, that the LED blue light is able to decrease the viral load of HSV‐1 and ZIKV. In our study, LED photobiomodulation therapy (PBMT) at blue wavelengths (450, 454 and 470 nm) was tested in an in vitro model of SARS‐CoV‐2 infection, employing three experimental settings: SARS‐CoV‐2 was irradiated and then transferred to cells; already infected cells were irradiated; cells were irradiated prior to infection. A decrement of the viral load was observed when previously infected cells were irradiated with all three tested wavelengths and relevant effects were registered especially at 48 hours post‐infection, possibly suggesting that the blue light could interfere with the intracellular viral replication machinery. Our in vitro findings could represent the starting point for translational applications of PBMT as a supportive approach to fight SARS‐CoV‐2.
Keywords: blue LED, photobiomodulation therapy, SARS‐CoV‐2, Vero E6 cell line
In previous studies, LED blue light was shown to be able to decrease the viral load of HSV‐1 and ZIKV. In our study, LED photobiomodulation therapy (PBMT) at three blue wavelengths was tested in an in vitro model of SARS‐CoV‐2 infection. A decrement of the viral load was observed when previously infected cells were irradiated with all three tested wavelengths and relevant effects were registered especially at 48 hours post‐infection, possibly suggesting that the blue light could interfere with the intracellular viral replication machinery.
Abbreviations
- APDT
antimicrobial photodynamic therapy
- COVID‐19
coronavirus disease 2019
- PBMT
photobiomodulation therapy
- SARS‐CoV‐2
severe acute respiratory syndrome coronavirus 2
1. INTRODUCTION
The severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) is a highly pathogenic and infectious virus, defined as the causative agent of the coronavirus disease 2019 (COVID‐19). A severe outbreak of SARS‐CoV‐2 has emerged at the end of 2019 and soon lead to the onset of a pandemic that is still strongly menacing human health and safety, thus having a great impact on society and economy [1]. By the end of November 2020, the rapid global widespread of SARS‐CoV‐2 has caused more than 108 million confirmed cases and over 2 million deaths (WHO dashboard, 14 February 2021). The current lack of vaccines and of effective global prophylactic strategies results in a scarce control of the viral spread, therefore giving inevitably rise to concerns relative to the management and prevention of viral transmission. In this critical context, there is a rush toward the identification of strategies/tools that might contribute to the reduction of viral spread primarily by modeling potential prophylactic and preventive treatments to be adopted for patients in high risk conditions, by limiting the environmental risk factors through the inactivation of virions on surfaces and aerosols [2], and by identifying novel therapeutic strategies able to effectively counteract SARS‐CoV‐2.
The usage of light sources at different wavelengths, in the so called Photobiomodulation Therapy (PBMT), have for long been known to exert beneficial effects on various human ailments and have also been intensively investigated for their antibacterial effects and recently also for antiviral properties. An emerging and promising novel approach that has been seen to efficiently counteract microorganisms' infections is given by the exploitation of blue wavelengths (400–470 nm) that result to be effective even at low irradiation doses [3] against different bacterial strains including Porphyromonas gingivalis, methicillin‐resistant Staphylococcus aureus (MRSA), Pseudomonas aeruginosa and Helicobacter pylori [4, 5]. Though the exact molecular mechanisms through which blue light promotes a direct antimicrobial activity have not yet been fully characterized, it is thought to probably depend on a photochemical effect linked to the intrinsic ability of blue light to excite porphyrins, event that results in the production of reactive oxygen species (ROS) and therefore to the killing of the bacterial cell [5, 6, 7]. Blue light presents different potential clinical applications, indeed it can be used for infection control in patients with skin acne (Propionibacterium acnes) or H. pylori gastric colonization [4], but it can also be employed for environmental decontamination of clinical hospital rooms [8], of biomaterials in implantation devices or of biological fluids [9].
On the contrary, the evaluation of the effects of blue light on viral particles is still in a preliminary stage, but certainly possesses the potential to expand soon. Also in this case, the identification of the exact mechanisms at the basis of blue light‐driven antiviral properties has yet to be clarified. For the first time to our knowledge, our research group registered an antiviral effect of blue laser light in two in vitro models of infections: herpes simplex type 1 (HSV‐1) in spontaneously immortalized keratinocyte cell line (HaCaT) [10]; Zika virus (ZIKV) in human glioblastoma cell line (U87‐MG) [11]. In both experimental setups, we observed a significant reduction of viral concentration following irradiation of the viral particles and also a positive outcome in terms of viral load decrement in an already established infection [10, 11].
In the context of SARS‐CoV‐2, a preprint redacted by de Santis et al. [12] showed that visible LED light with a peak at 413 nm, was able to reduce the viral load of virions that were illuminated for 40 or 60 minutes and then transferred to a cell culture.
In the present work, the possible antiviral effect against SARS‐CoV‐2 of 3 LED devices (wavelengths at 450, 454 and 470 nm) was investigated in an in vitro cellular model of infection by performing three experimental settings: SARS‐CoV‐2 was irradiated alone and then transferred to the cell culture; cells were irradiated prior to infection; previously infected cells were irradiated.
2. EXPERIMENTAL SECTION
2.1. Cell line and LED irradiation
Experiments were performed on Vero E6 epithelial normal cell line derived from the kidney of Cercopithecus aethiops (ATCC CRL‐1586). Cells were cultured in MEM + 10% fetal bovine serum, 2 mM glutamine, and 100 U/mL penicillin/streptomycin (Euroclone, Pero, Italy). Cells were seeded at a density of 1 × 104 cells/well in 96 multi‐well plates. For all experimental conditions cells were cultured in DMEM +2% FBS, 2 mM glutamine, and 100 U/mL penicillin/streptomycin (Euroclone, Pero, Italy).
LED treatments were carried out by using LED lights at 450, 454 and 470 nm (BLù series, developed by UV‐Core based on Cortem Group's EVML lighting Fixture, Cortem S.p.A, Villesse, Italy) with an irradiance of 40 mW/cm2, continuous waves. The irradiations were performed in dark conditions with the lid of the plate left open to avoid environmental light and plastic interference. The power emission was checked with a power meter and the beams were able to cover uniformly four attached wells in the 96 multi‐well plates.
Different fluences were initially tested in order to define the maximal dose that resulted to be not toxic for the cells (5, 10, 15, 20 J/cm2). Consecutively, the maximum safe irradiation time for Vero E6 cells was employed in the following experiments of virus infection (both for the irradiation of the cells pre‐ or post‐infection, and for the irradiation of the virus alone).
2.2. LED antiviral activity
SARS‐CoV‐2, kindly provided by the BLS3 facility (San Polo Monfalcone hospital, GO, Italy), was employed in the experiments at a multiplicity of infection (MOI) of 0.1 and 0.01.
The experimental settings were performed as follows:
SARS‐CoV‐2 was irradiated alone and then transferred to the cells for 1 hour to determine whether the blue light can exert a direct impact on virions;
Cells were irradiated and then infected with SARS‐CoV‐2 for 1 hour to assess if the PBMT can promote cellular activation by priming their response to external stimuli;
Pre‐infected cells with SARS‐CoV‐2 for 1 hour were irradiated to test whether LED light can interfere with intracellular viral replication.
At the end of the procedures, the medium was removed and replaced with a fresh one.
At 24, 48 and 72 hours post‐infection/irradiation, 15 microliters of the cell culture supernatants were collected and thermolyzed with 45 microliters of water (98°C for 3 minutes, followed by 4°C for 5 minutes). The viral RNA was then quantified using Real‐Time PCR with CDC primers and probe (Eurofins, Luxembourg) specific for the viral gene N (nucleocapsid, 500 nM forward primer 5′‐GGG AGC CTT GAA TAC ACC AAA A‐3′, 500 nM reverse primer 5′‐TGT AGC ACG ATT GCA GCA TTG‐3′, 125 nM probe 5′‐FAM‐AYC ACA TTG GCA CCC GCA ATC CTG‐BHQ1‐3′), with the Luna Universal Probe One‐Step RT‐qPCR Kit (New England Biolabs, Ipswich, Massachusetts) following the manufacturer's instructions. Amplification was carried out on the 7500 Fast Real‐Time PCR platform (Thermo Fisher Scientific, Waltham, Massachusetts), with the following protocol: 50°C for 10′, 95°C for 1′, and then 40 cycles at 95°for 10″, 60° for 30″. A standard with known amounts of nucleic acid (derived from nCoV‐CDC‐Control Plasmid, Eurofins) was employed in order to quantify the viral load.
2.3. Statistical analysis
R software was employed to conduct the statistical analysis by using Kruskal‐Wallis (KW) test corrected for multiple comparisons with Dunn's test. Non‐irradiated cells (treated only with the virus) were compared with the other experimental conditions [13]. The experiments were performed in quadruplicate.
3. RESULTS AND DISCUSSION
In the current work, the potential antiviral effect of blue light was investigated on a cellular model of SARS‐CoV‐2 infection.
After the initial screening to determine the safety dosage of irradiation for the Vero E6 cells, the following protocols, presenting the highest fluences tolerated by the cells (95%–100% of cell survival when compared to not treated cells), were selected and include: 450 nm, 12.5 J/cm2; 454 nm, 10 J/cm2; 470 nm, 20 J/cm2.
To test the potential antiviral activity of the blue LED, three experimental settings were exploited. The first scenario comprehends the irradiation of the virus alone to determine the possible direct effects of blue light on SARS‐CoV‐2 viability, presumably acting on the virions' external structure and proteins. In the second setting, cells were irradiated prior to infection to verify whether the PBMT can reduce viral uptake and/or strengthen cell resistance and response against the virus; indeed, the metabolic stimulation of the cells after PBMT could positively affect their reaction and counterattack to external stimuli such as infections [14]. In the third tested condition, the irradiation of infected cells was considered in order to assess the effect of PBMT on the machinery involved in intracellular viral replication. The described experimental strategies were chosen since they strictly enclose critical aspects that need to be unraveled in order to properly manage SARS‐CoV‐2 widespread: the irradiation of the virus alone could mimic an environmental condition in which PBMT might act as a disinfectant for surfaces; the irradiation of cells prior to infection could model a preventive prophylactic treatment for high risk subjects by metabolically pre‐activating the cells of the oral and nasopharyngeal mucosa, known to be permissive to viral entry [15, 16]; the irradiation of infected cells might pioneer a new therapeutic strategy against SARS‐CoV‐2 based on light.
Our data show that the most promising setting is the third one, given by the irradiation of previously infected cells; indeed, when compared to untreated cells, a great reduction in viral load was observed both at 24 and 48 hours post‐infection (Figures 1 and 2, Figure S1), and statistical significance was registered at the MOI of 0.01. While the irradiation with LED at 450 and 454 nm was able to significantly reduce the viral load even at 24 hours (initial MOI 0.01, KW test P‐value = .04 and P‐value = .02 respectively), at 48 hours all the tested LED wavelengths (including that at 470 nm) seem to be effective (initial MOI 0.01, KW test, P‐value = .004, P‐value = .01, and P‐value = .04 respectively). Although the trend of the obtained data always shows a favorable outcome, it is presumable that an excessively high viral concentration prevents the detection of a clear‐cut antiviral effect of LEDs at the MOI of 0.1 and at increased time intervals (72 hours) (Figure 3, Figure S1). Previous to our work, in a preprint redacted by De Santis et al. [12], authors used a LED‐device with a combination of frequencies (400–420 nm, 430–460 nm, 500–780 nm) with a main peak at 413 nm, power of 4.67 mW/cm2 for 40 or 60 minutes. A reduction of SARS‐CoV‐2 plaques of 97.3% following the irradiation of 2 × 103 PFU/mL virions for 40 minutes and of 99.8% after the irradiation of 2 × 105 PFU/mL of viral particles for 60 minutes was observed. The work of De Santis et al. cannot be considered as directly comparable to ours, since their irradiation time was higher (40 and 60 minutes) if compared to our tested timings (maximum of 10 minutes). Moreover, they used a LED device possessing a wide range of wavelengths, while our lamps emitted a beam at a specific blue wavelength. Notably, the outcomes of the two studies are not in agreement; indeed, we did not detect a direct effect of the PBMT on the virus alone as reported by De Santis et al. but only following infection, when the viral particles already entered the host cell. Based on our results, we can speculate that the PBMT might be more efficient on intracellular viral particles, therefore leading to the assumption that PBMT might interfere with the replication machinery of the virus.
FIGURE 1.
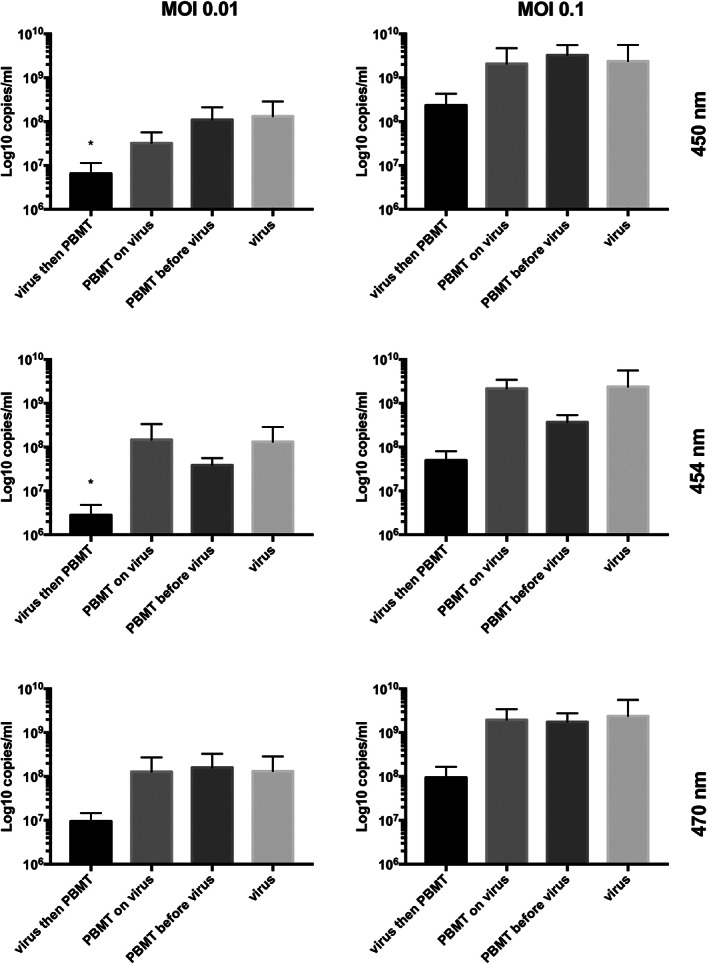
Effect of blue LED at 450, 454 and 470 nm on SARS‐CoV‐2 in Vero E6 cell line at 24 hours post‐infection. SARS‐CoV‐2 was used in the experiments at a multiplicity of infection (MOI) of 0.1 and 0.01. Three settings were employed: SARS‐CoV‐2 was irradiated alone and then transferred to the cells for 1 hour, already infected cells (1 hour) were irradiated, cells were irradiated and then infected with the virus for 1 hour. The viral load was quantified from the supernatants and is reported as Log10 viral copies/mL. Kruskal‐Wallis (KW) test corrected for multiple comparison with Dunn's test was utilized for the comparison between not irradiated cells (treated only with the virus) and the other experimental conditions (*P < .05, **P < .01). (A) SARS‐CoV‐2 viral load after PBMT at 450 nm (MOI of 0.1). (B) SARS‐CoV‐2 viral load after PBMT at 450 nm (MOI of 0.01). (C) SARS‐CoV‐2 viral load after PBMT at 454 nm (MOI of 0.1). (D) SARS‐CoV‐2 viral load after PBMT at 454 nm (MOI of 0.01). (E) SARS‐CoV‐2 viral load after PBMT at 470 nm (MOI of 0.1). (F) SARS‐CoV‐2 viral load after PBMT at 470 nm (MOI of 0.01)
FIGURE 2.
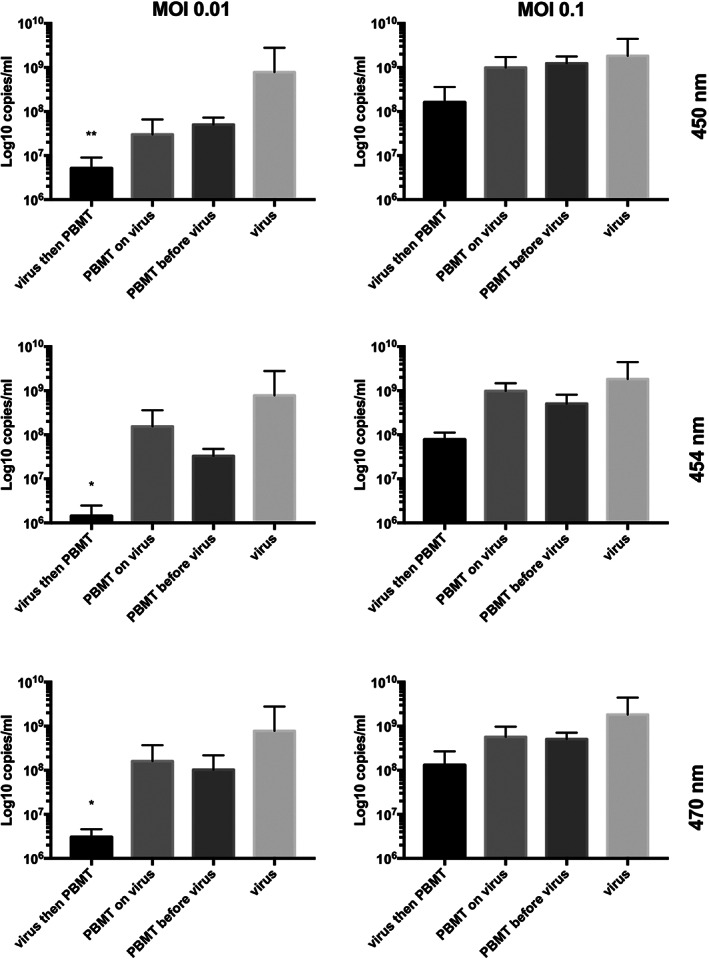
Effect of blue LED at 450, 454 and 470 nm on SARS‐CoV‐2 in Vero E6 cell line at 48 hours post‐infection. SARS‐CoV‐2 was used in the experiments at a multiplicity of infection (MOI) of 0.1 and 0.01. Three settings were employed: SARS‐CoV‐2 was irradiated alone and then transferred to the cells for 1 hour, already infected cells (1 hour) were irradiated, cells were irradiated and then infected with the virus for 1 hour. The viral load was quantified from the supernatants and is reported as Log10 viral copies/mL. Kruskal‐Wallis (KW) test corrected for multiple comparison with Dunn's test was utilized for the comparison between not irradiated cells (treated only with the virus) and the other experimental conditions (*P < .05, **P < .01). (A) SARS‐CoV‐2 viral load after PBMT at 450 nm (MOI of 0.1). (B) SARS‐CoV‐2 viral load after PBMT at 450 nm (MOI of 0.01). (C) SARS‐CoV‐2 viral load after PBMT at 454 nm (MOI of 0.1). (D) SARS‐CoV‐2 viral load after PBMT at 454 nm (MOI of 0.01). (E) SARS‐CoV‐2 viral load after PBMT at 470 nm (MOI of 0.1). (F) SARS‐CoV‐2 viral load after PBMT at 470 nm (MOI of 0.01)
FIGURE 3.
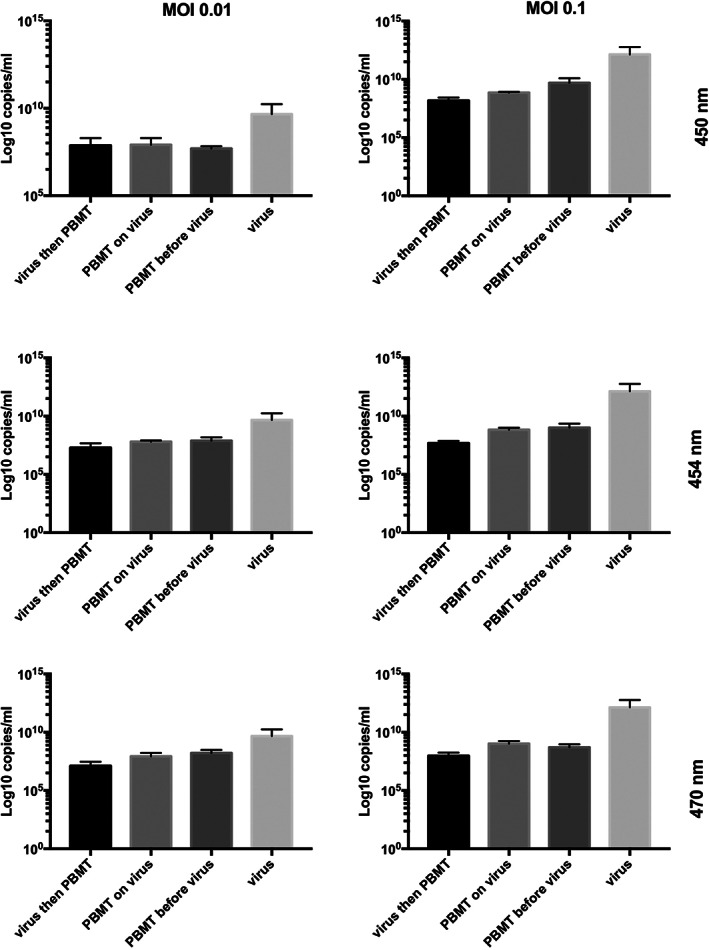
Effect of blue LED at 450, 454 and 470 nm on SARS‐CoV‐2 in Vero E6 cell line at 72 hours post‐infection. SARS‐CoV‐2 was used in the experiments at a multiplicity of infection (MOI) of 0.1 and 0.01. Three settings were employed: SARS‐CoV‐2 was irradiated alone and then transferred to the cells for 1 hour, already infected cells (1 hour) were irradiated, cells were irradiated and then infected with the virus for 1 hour. The viral load was quantified from the supernatants and is reported as Log10 viral copies/mL. Kruskal‐Wallis (KW) test corrected for multiple comparison with Dunn's test was utilized for the comparison between not irradiated cells (treated only with the virus) and the other experimental conditions (*P < .05, **P < .01). (A) SARS‐CoV‐2 viral load after PBMT at 450 nm (MOI of 0.1). (B) SARS‐CoV‐2 viral load after PBMT at 450 nm (MOI of 0.01). (C) SARS‐CoV‐2 viral load after PBMT at 454 nm (MOI of 0.1). (D) SARS‐CoV‐2 viral load after PBMT at 454 nm (MOI of 0.01). (E) SARS‐CoV‐2 viral load after PBMT at 470 nm (MOI of 0.1). (F) SARS‐CoV‐2 viral load after PBMT at 470 nm (MOI of 0.01)
We could speculate that, under our experimental conditions, the intact virions are resistant and not susceptible to LED blue light, while when the virus enters the host cell and uncoats, it becomes more sensitive to the effect of an external perturbing treatment. As a consequence, if laser light is delivered during this phase, the stability of SARS‐CoV‐2 might be affected and the virus may not be able to replicate efficiently.
In previous works conducted by our research group, we used a 445 nm laser device on HSV‐1 and ZIKV. In this case we registered both a direct effect of the blue light on the virus and also in pre‐infected cells for 1 hour that were then irradiated [10, 11]. The last mentioned observation confirms the results obtained in the current work on SARS‐CoV‐2.
Very recently, the usage of PBMT on COVID‐19 patients has been suggested with the intent of possibly performing a transthoracic PBMT to promote the regeneration of the lung, a transcutaneous or intravenous PBMT to reach the blood thus stimulating a systemic effect, and a PBMT at the level of the tibia (bone marrow), thymus or lymph nodes in order to stimulate the immune system [17, 18]. Under these circumstances, it is worth considering that since blue light presents very low penetration properties across the skin [19], the transthoracic/transcutaneous application of PBMT should not be able to reach and target the pulmonary region. A possible alternative may reside in the development of a tracheal probe that could deliver the light to the affected pulmonary sites. Furthermore, the usage of antimicrobial photodynamic therapy (APDT), already assessed against other viruses [20], has been speculated to be functional for the disinfection of the oropharynx of COVID‐19 patients by promoting the decrease of the viral load and therefore potentiality counteracting viral invasion and infection [21].
Remarkably, PBMT at infrared wavelengths is already exploited for the treatment of viral ailments, such as the warts caused by human papillomavirus (HPV) [22], or herpetic oral lesions induced by herpes simplex virus 1 [23].
Although the potentiality of PBMT in the context of SARS‐CoV2 infection is worth of consideration, only a case report, in which a supportive treatment at 808 to 905 nm improved pneumonia, strongly reinforces the possible usage of PBMT on COVID‐19 patients [24]. Moreover, a very recent article described the employment of methylene blue and visible light to inactivate residual SARS‐CoV‐2 in the plasma of a patient recovered from COVID‐19 prior to the transfusion in patients with active severe disease [25].
4. CONCLUSION
Our promising results can endorse the possible exploitation of blue light to face the challenges linked to SARS‐CoV‐2 infection. A relevant aspect to bear in mind is that the applied wavelengths are defined as safe for eukaryotic cells. Considering this aspect, a possible and intriguing option might be the application of a combination of different wavelengths: the infrared component could help the recovery from pneumonia as reported by Sigman et al. [24], while blue wavelengths might tackle SARS‐CoV‐2 replication as shown by our work.
The investigation of PBMT antiviral activity against SARS‐CoV‐2 on human cell lines (we employed a very general permissive cell model), is envisaged in order to propose translationality for this interesting new supportive approach on COVID‐19 affected individuals, also considering that PBMT is widely known to be safe, without side effects and to be well tolerated by the patients.
CONFLICT OF INTEREST
The authors declare no potential conflict of interest.
AUTHOR CONTRIBUTIONS
Luisa Zupin, Rossella Gratton and Libera Clemente were involved in performing the experiments and writing—original draft. Francesco Fontana, and Maurizio Ruscio were involved in supervision of the experiments conducted in the BLS3 facility, writing—review and editing. Lorella Pascolo was involved in writing—review and editing. Sergio Crovella was involved in conceptualization of the study, writing—review and editing, project management.
Supporting information
Figure S1: Effect of blue LED at 450, 454 and 470 nm on SARS‐CoV‐2 in Vero E6 cell line showing the time course (24, 48 and 72 hours post infection).
ACKNOWLEDGMENTS
This work was approved by IRCCS Burlo Garofolo (RC 47/2020) and granted by IRCCS Burlo Garofolo/Italian Ministry of Health (RC 15/2017 and RC 03/2020). We are grateful to Dr Cristiano Decorte and Antonio Frattaruolo for the technical assistance in LED device development. The Graphical Abstract was created with Biorender.com.
Zupin L, Gratton R, Fontana F, et al. Blue photobiomodulation LED therapy impacts SARS‐CoV‐2 by limiting its replication in Vero cells. J. Biophotonics. 2021;14:e202000496. 10.1002/jbio.202000496
Funding information IRCCS Burlo Garofolo/Italian Ministry of Health, Grant/Award Numbers: RC 03/2020, RC 15/2017; IRCCS Burlo Garofolo, Grant/Award Number: RC 47/2020
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- 1. Hu B., Guo H., Zhou P., Shi Z.‐L., Nat. Rev. Microbiol. 2021, 19, 141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. van Doremalen N., Bushmaker T., Morris D. H., Holbrook M. G., Gamble A., Williamson B. N., Tamin A., Harcourt J. L., Thornburg N. J., Gerber S. I., Lloyd‐Smith J. O., de Wit E., Munster V. J., N. Engl. J. Med. 2020, 382, 1564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Guffey J. S., Wilborn J., Photomed. Laser Surg. 2006, 24, 684. [DOI] [PubMed] [Google Scholar]
- 4. Dai T., Gupta A., Murray C. K., Vrahas M. S., Tegos G. P., Hamblin M. R., Drug Resist. Updat. 2012, 15, 223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Rupel K., Zupin L., Ottaviani G., Bertani I., Martinelli V., Porrelli D., Vodret S., Vuerich R., Passos da Silva D., Bussani R., Crovella S., Parsek M., Venturi V., Di Lenarda R., Biasotto M., Zacchigna S., NPJ Biofilms Microbiom. 2019, 5, 29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Amin R. M., Bhayana B., Hamblin M. R., Dai T., Lasers Surg. Med. 2016, 48, 562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Yang H., Inokuchi H., Adler J., Proc. Natl. Acad. Sci. 1995, 92, 7332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Cabral J., Ag R., Antibiotics 2019, 8, 58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Wang Y., Wang Y., Wang Y., Murray C. K., Hamblin M. R., Hooper D. C., Dai T., Drug Resist. Updat. 2017, 33, 1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Zupin L., Caracciolo I., Tricarico P. M., Ottaviani G., D'Agaro P., Crovella S., Microbiol. Immunol. 2018, 62, 477. [DOI] [PubMed] [Google Scholar]
- 11. Zupin L., Caracciolo I., Tricarico P. M., Ottaviani G., D'Agaro P., Crovella S., Lasers Med. Sci. 2018, 33, 2011. [DOI] [PubMed] [Google Scholar]
- 12. De Santis R., Luca V., Faggioni G., Fillo S., Stefanelli P., Rezza G., Lista F., 2020,. http://medrxiv.org/lookup/doi/10.1101/2020.06.18.20134577 (accessed December 7, 2020).
- 13. R core Team, 2019. http://www.R-project.org.
- 14. Ayres J. S., Nat. Rev. Immunol. 2020, 20, 79. [DOI] [PubMed] [Google Scholar]
- 15. Wölfel R., Corman V. M., Guggemos W., Seilmaier M., Zange S., Müller M. A., Niemeyer D., Jones T. C., Vollmar P., Rothe C., Hoelscher M., Bleicker T., Brünink S., Schneider J., Ehmann R., Zwirglmaier K., Drosten C., Wendtner C., Nature 2020, 581, 465. [DOI] [PubMed] [Google Scholar]
- 16. Zhang S., Carriere J., Lin X., Xie N., Feng P., Viruses 2018, 10, 521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Fekrazad R., Photobiomodul. Photomed. Laser Surg. 2020, 38, 255. [DOI] [PubMed] [Google Scholar]
- 18. Domínguez A., Velásquez S. A., David M. A., Photobiomodul. Photomed. Laser Surg. 2020, 38, 258. [DOI] [PubMed] [Google Scholar]
- 19. Ash C., Dubec M., Donne K., Bashford T., Lasers Med. Sci. 2017, 32, 1909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Costa L., Faustino M. A. F., Neves M. G. P. M. S., Cunha Â., Almeida A., Viruses 2012, 4, 1034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Dias L. D., Blanco K. C., Bagnato V. S., Photodiagnosis Photodyn. Ther. 2020, 31, 101804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Hsu V. M., Aldahan A. S., Tsatalis J. P., Perper M., Nouri K., Lasers Med. Sci. 2017, 32, 1207. [DOI] [PubMed] [Google Scholar]
- 23. Verma S., Chaudhari P., Maheshwari S., Singh R., Nat. J. Maxillofac. Surg. 2012, 3, 124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Sigman S. A., Mokmeli S., Monici M., Vetrici M. A., Am. J. Case Rep. 2020, 21, e926779. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Duan K., Liu B., Li C., Zhang H., Yu T., Qu J., Zhou M., Chen L., Meng S., Hu Y., Peng C., Yuan M., Huang J., Wang Z., Yu J., Gao X., Wang D., Yu X., Li L., Zhang J., Wu X., Li B., Xu Y., Chen W., Peng Y., Hu Y., Lin L., Liu X., Huang S., Zhou Z., Zhang L., Wang Y., Zhang Z., Deng K., Xia Z., Gong Q., Zhang W., Zheng X., Liu Y., Yang H., Zhou D., Yu D., Hou J., Shi Z., Chen S., Chen Z., Zhang X., Yang X., Proc. Natl. Acad. Sci. 2020, 117, 9490. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1: Effect of blue LED at 450, 454 and 470 nm on SARS‐CoV‐2 in Vero E6 cell line showing the time course (24, 48 and 72 hours post infection).
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.