

Abstract
Context:
As a response to the CoronaVirus Disease 2019 (COVID-19) pandemic, India announced a nation-wide lockdown effective from March 25, 2020. Recent media reports and published studies from Western countries indicate a decrease in patients presenting to hospitals with stroke, acute coronary syndromes, and other emergencies.
Aims:
The purpose of this study was to assess the impact of the lockdown on the number of patients undergoing Computed Tomography (CT) in a public tertiary care hospital in India, and thus indirectly assess the effect of the lockdown on medical conditions other than COVID-19.
Settings and Design:
Retrospective observational study.
Materials and Methods:
Analysis of the CT reports from the hospital's PACS for the first three months of lockdown was performed and compared with those of the month prior to the imposition of the lockdown.
Statistical Analysis Used:
Frequency tables and percentages were calculated.
Results:
There was a 70% decrease in the number of total CTs in the first three months of lockdown compared to the month prior to lockdown. There was a decrease in CTs performed for various conditions such as tuberculosis follow up (decreased by 98%), brain infarcts, nontraumatic intracranial hemorrhage (decreased by 40%), and baseline CTs for neoplasms (decreased by 73%). CTs for trauma also decreased by 64% with a decrease in patients involved in road traffic accidents undergoing CT.
Conclusion:
Our study highlights the impact of the lockdown on medical conditions other than COVID-19 in India, with a substantial decrease in the number of patients undergoing CTs for a variety of conditions.
Keywords: Computed Tomography, COVID-19, lockdown, pandemic
Introduction
In view of the CoronaVirus Disease 2019 (COVID-19) pandemic, India announced a nation-wide lockdown of nonessential services for its population of 1.3 billion people, effective from midnight of March 25, 2020. The Ministry of Health and Family Welfare (MOHFW), Government of India also advised patients to avoid routine visits to outpatient clinics for nonemergencies. For those suffering from chronic diseases, it was advised by the MOHFW to visit primary or secondary health care facilities rather than tertiary hospitals to avoid crowding and mingling with COVID-19 patients. Directives were also given to postpone all nonessential elective surgeries.[1] Recent media reports and published studies from USA, UK, and the rest of Europe indicate a decrease in patients presenting to hospitals with stroke, acute coronary syndromes, and other emergencies.[2,3] Computed Tomography (CT) imaging in an urban public tertiary care hospital can be a good barometer of the number of patients of diverse pathologies seeking medical care in a city. The purpose of this study was to assess the impact of the lockdown on the spectrum of patients undergoing CT imaging after imposition of some of the world's most stringent restrictions in a densely populated metropolis of India, and thus to indirectly assess the effect of the lockdown on medical conditions other than COVID-19.
Materials and Methods
STROBE guidelines for observational studies were referred to when structuring the study methodology.[4] A retrospective observational study was performed by analyzing the reports of all the diagnostic CTs performed in the department of radiology at our hospital during the first month of the lockdown from March 25 to April 24, 2020, the second month of lockdown from April 25 to May 25, 2020 and the third month of lockdown from May 26 to June 25, 2020 (a period of 30 days for each). The reports of all the diagnostic CTs of the previous 30 days before the lockdown (February 22 to March 24, 2020) when the department was functioning routinely as before were analyzed for comparison. From the start of the lockdown, two triage wards were created in our hospital. Any patient coming to the hospital for nonemergent indications was first shifted to these triage wards where he/she underwent a reverse transcriptase polymerase chain reaction (RT-PCR) swab test for severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) and a chest radiograph. When results of both these tests were negative for COVID-19, the patient was shifted to the general wards. Patients from these general wards were then brought for CT imaging as indicated. Emergency room patients who required emergent CT imaging were brought directly from the emergency room to the CT suite without shifting to the triage wards and without prior RT-PCR test and chest radiograph. Figure 1 shows the flowchart for patients undergoing CT in our hospital in the first three months of lockdown. As per national guidelines in India, CT as a screening tool for suspected COVID-19 patients is not recommended;[5] hence, CT of such patients was not performed.
Figure 1.
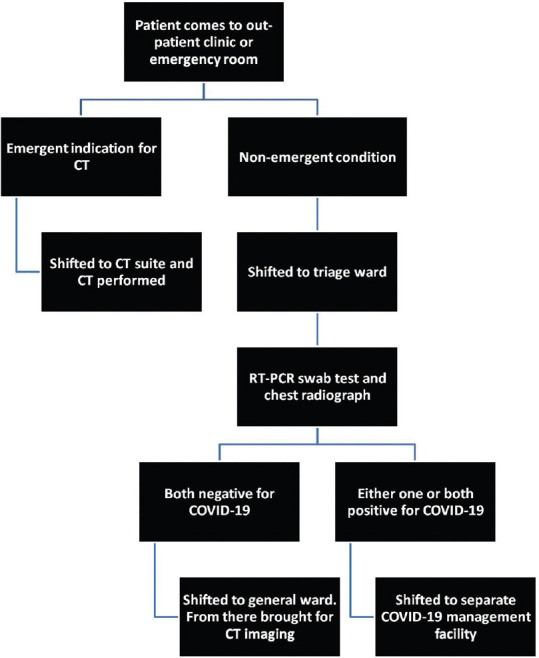
Flowchart depicting pathway of patients coming for CT during the first three months of lockdown
Associated clinical patient data was reviewed through the Hospital Information System (HIS). Data collection was performed by three staff radiologists having a mean experience of 4 years. Statistical analysis was performed by generating frequency tables and percentages. No author has any conflict of interest related to the study.
Results
A total of 1970 diagnostic CTs were performed in the department of radiology of our hospital in the month prior to the lockdown (M1). This number reduced drastically to 620 CTs in the first month of the lockdown (M2), 603 CTs in the second month of lockdown (M3), and 695 CTs in the third month of lockdown (M4), a decrease of 65% to 70% compared to the pre-lockdown month. Prelockdown, the gender distribution of the patients undergoing CTs was 61% male and 39% female. Post lockdown there was no significant difference in this gender distribution, with 63% of the patients being male and 37% female. The age distribution of patients undergoing CTs in M1, M2, M3, and M4 was as described in Table 1.
Table 1.
Age distribution of patients undergoing CTs in the month prior to lockdown and in the first three months of lockdown
| Age (in years) | Month prior to lockdown | First month of lockdown | Second month of lockdown | Third month of lockdown |
|---|---|---|---|---|
| <30 | 688 (35%) | 192 (31%) | 175 (29%) | 235 (33%) |
| 30 to 50 | 679 (35%) | 196 (32%) | 201 (33%) | 215 (31%) |
| 50 to 70 | 496 (25%) | 188 (30%) | 179 (30%) | 193 (28%) |
| >70 | 107 (5%) | 44 (7%) | 48 (8%) | 52 (8%) |
| Total | 1970 | 620 | 603 | 695 |
The number of CTs of each study type or body part performed in all the months are depicted in Figure 2. The common indications for which CT was performed in all the months are summarized in Table 2. The numbers of the common CT diagnoses for all the months are enumerated in Table 3.
Figure 2.
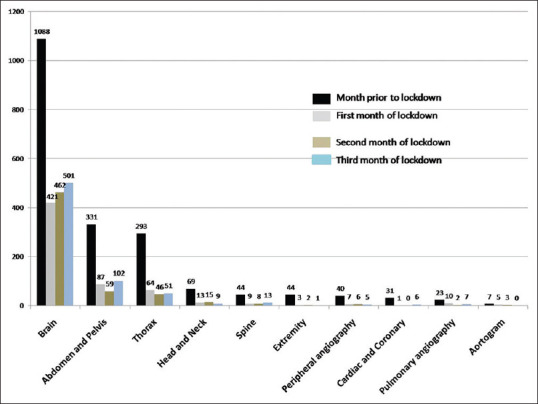
Chart showing the number of CTs of each body part / type of study performed in the month before and in the three months after lockdown. Black bars = month prior to lockdown. Grey bars = first month of lockdown. Brown bars = second month of lockdown. Blue bars = third month of lockdown. The numbers on top of the bars indicate the number of CTs done of that study type
Table 2.
Number of CTs for common indications in the month prior to lockdown and in the first three months of lockdown (note: rare indications have not been included)
| Indication for CT | Month prior to lockdown | First month of lockdown | Second month of lockdown | Third month of lockdown |
|---|---|---|---|---|
| Trauma | 399 | 147 | 150 | 155 |
| Altered sensorium | 150 | 109 | 103 | 121 |
| Headache | 137 | 33 | 37 | 39 |
| Abdominal pain | 127 | 46 | 52 | 55 |
| Postoperative CTs | 113 | 15 | 19 | 22 |
| Hemiplegia | 99 | 84 | 82 | 91 |
| Respiratory symptoms (breathlessness, cough, etc) | 99 | 56 | 63 | 69 |
| Seizures | 81 | 37 | 32 | 44 |
| Posttreatment follow-up of tuberculosis | 70 | 1 | 1 | 7 |
| Rhinitis, sinusitis | 38 | 4 | 2 | 6 |
| Chest pain | 23 | 3 | 1 | 5 |
| Ear discharge, ear pain | 23 | 5 | 4 | 3 |
| Posttreatment follow-up of neoplasms | 12 | 7 | 8 | 7 |
| Head and neck swelling | 11 | 3 | 2 | 2 |
| Paraplegia | 9 | 2 | 2 | 3 |
| Suspected foreign body | 6 | 0 | 0 | 0 |
| Jaundice | 5 | 2 | 3 | 3 |
| Quadriplegia | 4 | 1 | 0 | 2 |
| Orbital swelling | 3 | 2 | 1 | 1 |
Table 3.
Number of common CT diagnoses in the month prior to lockdown and in the first three months of lockdown (note: rare diagnoses have not been included)
| CT Diagnoses | Month prior to lockdown | First month of lockdown | Second month of lockdown | Third month of lockdown |
|---|---|---|---|---|
| Normal | 595 | 202 | 200 | 229 |
| Posttraumatic injuries | 231 | 73 | 66 | 88 |
| Pulmonary infection (non-tubercular and non-COVID-19) | 118 | 25 | 27 | 20 |
| Intracranial hemorrhage (nontraumatic) | 80 | 47 | 43 | 51 |
| Cerebral/cerebellar/brainstem acute infarcts | 73 | 48 | 45 | 46 |
| Neoplasia (baseline CT) | 62 | 17 | 14 | 15 |
| Urinary system calculus (symptomatic) | 60 | 7 | 6 | 7 |
| Active tuberculosis (pulmonary and extra-pulmonary) | 56 | 16 | 14 | 22 |
| Peripheral vascular disease | 25 | 5 | 4 | 5 |
| Acute pancreatitis | 22 | 12 | 14 | 17 |
| Chronic otitis media/Cholesteatoma | 21 | 0 | 0 | 0 |
| Hydrocephalus | 19 | 8 | 7 | 8 |
| Interstitial lung disease | 11 | 0 | 0 | 2 |
| Congenital heart disease | 10 | 0 | 0 | 4 |
| Coronary artery disease | 9 | 1 | 0 | 2 |
| Hydronephrosis | 8 | 1 | 2 | 3 |
| Abdominal aortic aneurysm | 7 | 1 | 1 | 0 |
| Acute appendicitis | 6 | 6 | 7 | 7 |
| Pulmonary edema | 6 | 4 | 3 | 5 |
| Foreign body | 6 | 0 | 0 | 0 |
| Cholelithiasis or choledocholithiasis (symptomatic) | 6 | 1 | 2 | 1 |
| Liver abscess | 5 | 2 | 1 | 3 |
| Pulmonary embolism | 5 | 2 | 2 | 4 |
| Small or large bowel obstruction | 4 | 4 | 3 | 3 |
| Cerebral venous sinus thrombosis | 4 | 3 | 3 | 6 |
| Aspiration pneumonitis | 4 | 1 | 0 | 0 |
| Cholecystitis | 3 | 2 | 2 | 3 |
| Pyelonephritis | 3 | 3 | 2 | 2 |
| Meningitis | 5 | 2 | 4 | 7 |
Discussion
Of the indications for CTs in the first three months of lockdown in our hospital, of note is the 98% decrease in the number of tuberculosis patients (both pulmonary and extra-pulmonary tuberculosis) coming for their scheduled post-anti-tuberculosis treatment CT in the first two months of lockdown and a 90% decrease in the third month of lockdown compared to the prelockdown month [Table 2]. The number of active tuberculosis cases detected on CT also decreased by 62%–72% [Table 3].
Trauma as an indication for CT decreased by 64% in M2, M3, and M4 compared to M1, presumably due to a decrease in the number of patients involved in road traffic accidents (279 patients involved in road traffic accidents undergoing CT in M1 compared to 72 patients in M2, 63 in M3, and 75 in M4). The number of patients undergoing CT in M2, M3, and M4 decreased as compared to M1 for many common indications such as seizures (a decrease of 45%–55%), headache (a decrease of 76%), and abdominal pain (a decrease of 64%). Postoperative CTs decreased by 87% in M2, M3, and M4 compared to M1 [Table 2].
Of the common CT diagnoses, there was a 38%–42% decrease in the combined number of cases of nontraumatic intracranial hemorrhage and acute ischemic brain infarcts, from a total of 153 in M1 to 95 in M2, 88 in M3, and 97 in M4. This is in line with the findings of Kansagra et al. who noted a 39% decrease in patients undergoing stroke imaging in the postpandemic era compared to the prepandemic era.[6] Decrease was also seen in the number of patients presenting with symptomatic urinary tract calculi (a decrease of 89%) and baseline CTs for neoplasms (a decrease of 73%) [Table 3].
Limitation of our study is the retrospective analysis of all CT reports from the department, which were reported by multiple staff radiologists (mean experience ranging from 2 to 20 years).
Conclusion
Our study highlights the impact of the lockdown on medical conditions other than COVID-19 in a developing country like India, with a substantial decrease in the number of patients undergoing CTs for a variety of conditions including tuberculosis, strokes, seizures, neoplasms, congenital heart diseases and coronary artery disease among many others. CTs performed for trauma also decreased in the lockdown months, with a corresponding decrease in the number of patients involved in road traffic accidents undergoing CT. Overall decrease in public movement during the lockdown may have contributed to these decreased trauma CTs. Many patients with non-COVID-19 diseases are probably not seeking timely medical care during this lockdown, which may be due to a combination of factors such as reluctance to visit hospitals due to the fear of contracting COVID-19, absence or scarcity of public transport, initial government advisories in the lockdown for patients to visit tertiary hospitals only for critical emergencies, and also closure of many outpatient clinics of other specialities leading to less patients being referred for CTs. Unfortunately, the other non-COVID-19 diseases remaining underdiagnosed seems to be a collateral damage of this pandemic, and there is probably a “hidden burden” of these diseases in society which will prove devastating for the patients themselves.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Directives for Hospitals and Medical Institutions. Ministry of Health and Family Welfare, Government of India website. 2020. [Last accessed on 2020 May 26]. Available from: https://www.mohfw.gov.in/pdf/AdvisoryforHospitalsandMedicalInstitutions.pdf .
- 2.Garcia S, Albaghdadi MS, Meraj PM, Schmidt C, Garberich R, Jaffer FA, et al. Reduction in ST-segment elevation cardiac catheterization laboratory activations in the United States during COVID-19 pandemic. J Am Coll Cardiol. 2020;75:2871–2. doi: 10.1016/j.jacc.2020.04.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bernstein L, Stead Sellers F. Patients with heart attacks, strokes and even appendicitis vanish from hospitals. The Washington Post website. 2020. [Last accessed on 2020 May 26]. Available from: https://www.washingtonpost.com/health/patients-with-heart-attacks-strokes-and-evenappendicitis-vanish-from-hospitals/2020/04/19/ 9ca3ef24-7eb4-11ea-9040-68981f488eed_story.html .
- 4.von Elm E, Altman DG, Egger M, Pocock S, Gotzsche PC, Vandenbroucke JP. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ. 2007;335:806. doi: 10.1136/bmj.39335.541782.AD. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Chest Radiology Subspecialty Group, Indian College of Radiology and Imaging. Imaging In Covid 19 Patients: Indian Guidelines Recommendations Of IRIA ICRI Chest Subspecialty Group. 2020. [Last accessed on 2020 May 26]. Available from: https://irp-cdn.multiscreensite.com/e482ea7d/files/uploaded/IRIA_ICRI_guidlines_on_Imaging_in_COVID-19_Patients.pdf .
- 6.Kansagra AP, Goyal MS, Hamilton S, Albers GW. Collateral effect of Covid-19 on stroke evaluation in the United States. NEJM. 2020 doi: 10.1056/NEJMc2014816. doi: 10.1056/NEJMc2014816. [DOI] [PMC free article] [PubMed] [Google Scholar]