

ABSTRACT
With the outbreak of COVID-19, there was widespread cessation of face-to-face teaching in medical schools from March 2020. 130 students in their first clinical year at a large London medical school were at risk of missing part of their clinical and practical procedure teaching. We mailed a teaching pack containing clinical consumables and gave instructions to prepare fruit, vegetables and kitchen sponges as a replacement for manikins. Students used cucumbers for bladder catheterisation, oranges for injections, bananas for suturing and cannulated sponges for practising intravenous drug administration. A student evaluation after the course was favourable. Hands-on practice had a positive effect on the students' feelings of belongingness and identity and helped them feel like they were not missing out or being left behind. Technology was challenging for both students and tutors. The intervention is being repeated for all incoming students from September 2020.
KEYWORDS: clinical, skills, virtual
The problem
Due to the outbreak of COVID-19, there was widespread cessation of face-to-face teaching in UK medical schools from March 2020. As a result, 130 fourth year (first clinical year) medical students at University College London Medical School (UCLMS) risked missing the ‘care of the critically ill patient’ day and the practical procedure course that would normally be part of their perioperative medicine placement. This represented one third of the year group. These courses include core practical skills and procedures listed in the General Medical Council's Outcomes for Graduates (2018) guidance document,1 which underpins undergraduate medical education in the UK. The pedagogical design to support the students' skills acquisition and expected degree of competence2,3 was dependent on both classroom instruction and experiential learning.4 ‘Care of the critically ill patient’ day involved short episodes of classroom teaching combined with bedside teaching in the emergency department (ED) and intensive care unit (ICU). In the classroom, students simulated treating patients presenting with anaphylaxis, heart failure, post-operative bleeding and pneumonia. In the ED we supervised students performing practical procedures on patients. These included recording a 12-lead ECG, venous cannulation, phlebotomy, urinalysis and blood sugar measurement. In ICU, students assessed patients using the Resuscitation Council's5 DR ABCDE approach to assessing a sick patient. The practical procedure course was taught in groups of 16 during 90-minute sessions in the clinical skills centre. Students used part-task trainer devices and consumables sourced from NHS supplies and were continuously assessed.
Although some students worked as volunteers in hospital trusts during the lockdown period, most were confined to their family homes. Our aim was to teach the students as much of the content of both courses as possible by delivering the sessions ‘live’ via synchronous online instruction. We mailed a teaching pack of equipment containing clinical consumables to equip students with the opportunity to practice procedural skills at home both during and after the teaching sessions.
The intervention
Clinical tutors collected manikins, consumables and suitable digital support to ensure they could deliver teaching synchronously via a digital platform from their homes. This was the first experience of synchronous practical and clinical skills teaching for the teaching team. A list of equipment and consumables packaged and mailed to those students who provided their postal address is shown in Box 1.
Box 1.
Contents of the teaching resource pack
|
122 out of 130 (94%) students were sent teaching resource packs. Several medical schools have reported moving rapidly to both synchronous and asynchronous sessions using both videos and direct demonstration.6, 7 However, at the time of writing, the authors are not aware of examples of care profession courses mailing equipment to students to help them practice skills at home.
Sessions taught were:
scrubbing, gloving and gowning
catheterisation
suturing
subcutaneous & intramuscular injection
intravenous drug administration
basic airway management
nasogastric tube insertion
basic life support
advanced life support
care of the critically ill patient algorithm
invasive and non-invasive respiratory support.
Before each session, students were asked to prepare fruit and vegetables that were used as substitute manikins. We illustrated this with instructional videos via our YouTube channel. They reviewed PowerPoint presentations and downloaded information sheets.
Students used cucumbers for bladder catheterisation (Fig 1), oranges for injections (Fig 2) and bananas for suturing (Fig 3). They were instructed to insert an intravenous cannula into a kitchen sponge as preparation for an intravenous drug administration session.
Fig 1.

A cucumber with a Foley catheter inserted.
Fig 2.
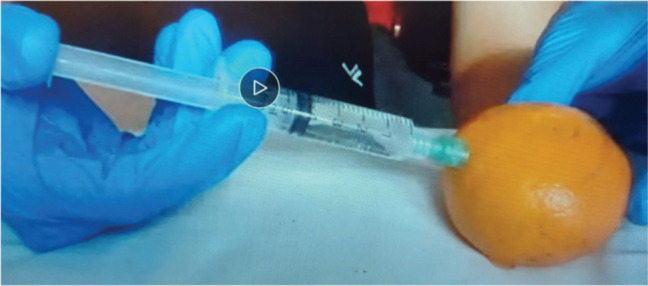
Injecting an orange.
Fig 3.
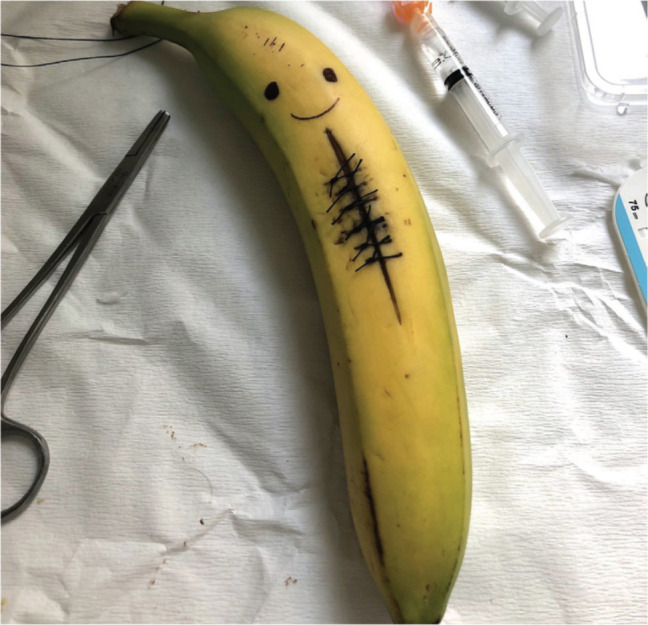
A banana with interrupted sutures.
An empty glass jar with a secure lid was recommended to store sharps before their return to UCLMS for disposal.
Each lesson followed a similar format to face-to-face sessions. Students were welcomed, presented with aims and objectives, questioned about prior experience and given guidance on the structure of the lesson. We used George and Doto's 2001 adaptation8 of Peyton's ‘Four stages of teaching a skill’ concept (2001)9 (Box 2) within the main body of the lesson. We used breakout rooms where students supported each other to perform procedures using guidance sheets and tutors dropped in to troubleshoot when necessary. We avoided formal assessment or rating of competence of skills performance due to the unpredictable nature of the teaching platform. Instead, the students were assured they would be provided with revision sessions in the next academic year.
Box 2.
The Five Stages of Teaching a Skill8
| Conceptualisation: The learner must understand the cognitive elements of the skill: that is, why it's done, when it's done, when it's not done, and the precautions involved. The learner must know the instruments and tools involved in the skill's performance. |
| Visualisation: The learner must see the skill demonstrated in its entirety from beginning to end so as to have a model of the performance expected. |
| Verbalisation: The learner must hear a narration of the steps of the skill along with a second demonstration. If the learner is able to narrate correctly the steps of the skill before demonstrating, there is a greater likelihood that the learner will correctly perform the skill. |
| Practice: The learner having seen the skill, heard a narration, and repeated the narration, now performs the skill. The skill may be broken down into discreet units for practice: subcomponent practice – practicing a small portion of the skill; linkage practice –practicing small portions linked together; contiguous practice – practicing the entire skill repetitively. |
| Correction and reinforcement: Skill errors need immediate correction. Positive reinforcement should be used to cement correct performance. |
Sessions were scheduled twice weekly in groups of 10 for critical care and 21 for practical procedures. Each session was delivered by one tutor. All sessions were recorded to enable students to review material and allow those who missed sessions to catch up.
Student reaction during planning and execution of this project was positive.
A post-course evaluative questionnaire created using Survey Monkey was emailed to students one week after the final session. We asked the following questions requiring a free text response in an attempt to elicit quality feedback detailing how we might improve the teaching experience should we need to repeat the experience in the new academic year:
What was your motivation for engaging in the clinical skills online teaching?
Which aspects of the sessions do you feel worked well?
Which aspects of the sessions do you feel require improvement?
Have you any other comments, suggestions or advice in relation to the teaching provided by the skills team?
The outcome
The response rate was 22/130 (17%). Several themes were generated from free text comments (Table 1). Students favoured teaching packs and the ability to practice the skill along with the tutor, with comments including ‘Having all of the equipment to have a go ourselves rather than just watching videos was great’ and ‘Being able to put on the video and ask if I was doing something right.’
Table 1.
Summary of themes generated from post-course evaluative questionnaire
| What went well? | Mentions |
|---|---|
| Hands on approach/equipment | 13 |
| Small groups/breakout rooms | 11 |
| Continue to learn to be a competent doctor | 10 |
| Connection with peers and tutors | 9 |
| Five stages of teaching a skill | 6 |
| Fun and enjoyable | 5 |
| Not being left behind | 5 |
| Asynchronous preparation | 2 |
| Suggestions for improvement | |
| Visibility on camera sometimes poor/tech issues | 6 |
| Pace of session too slow | 5 |
| Overuse of breakout sessions | 3 |
| Pace of session too fast | 2 |
| Lots of asynchronous prep | 1 |
The response rate was low. A questionnaire combining yes/no answers with free text options might have improved the response rate. In addition, the students were now preparing for end-of-year summative examinations and so may not have prioritised replying to the questionnaire. The limited data show that students enjoyed the learning opportunity provided within small breakout groups. This overlapped with the importance of connecting with peers and tutors. They valued being able to turn on the cameras for reassurance and feedback and to socialise with peers. This was reflected in the high attendance numbers. Most classes had 100% attendance. Comments included: ‘I missed engaging with people at uni and seeing my peers, so this was a great way to do that’ and ‘Having some contact with students/the medical school each week was fun and I think important to keep me motivated in lockdown!’
Students were concerned about the impact on their education, being left behind and their future role as doctors. One student commented ‘I got the chance to continue my education and all the skills we learned are essential to being a doctor’ and another commented ‘Catching up with the skills my peers have learned earlier in the year so I don't feel behind.’
Themes for improvement focused on technological issues relating to camera angles, size of images and unpredictable internet connections.
Some students felt sessions were too long. Time spent in breakout groups contributed to this. Students recommended reducing the number of times breakout sessions are used. In contrast, several students wanted to spend more time practising the skills under supervision.
Conclusion
University College London adopted the term ‘remote not distant’ for staff and students when we entered a state of emergency in March 2020 due to COVID-19. There is no doubt mailing the medical students consumables to enable them to practice procedures during and after teaching was a success.
Being given the opportunity to use equipment, connect with peers and staff and not be left behind in their education was of particular importance. Regular contact with the same tutor and group of peers provided both teachers and students with connection, identity and a purpose during a time of significant uncertainty. Connection is important for maintaining self-esteem, identity development, well-being and sense of belonging.10–13
Both students and tutors faced technological challenges when WiFi connections were weak and camera angles were unsuitable. Tutors faced further challenges; becoming fluent with the digital platform and attempting to maximise the pedagogical experience for students while avoiding technical errors was time consuming. Finding a suitable virtual classroom to teach from within their homes that maximised visibility of the manikins and the full procedure was difficult, particularly for those who were home-schooling children.
Insufficient or missing equipment was also an issue. The rush to collect equipment before the university closed and time pressure to post packs to students resulted in consumables being rationed between students and staff. Both staff and students had to re-use consumables between sessions.
Despite the successes it is our view that remote learning of practical procedures is not a permanent or adequate alternative method of teaching these skills. All students will need to attend revision sessions once we are able to resume face-to-face teaching in order to achieve a suitable level of competency.
Next steps
For Term 1 of the 2020–2021 academic year, UCLMS's COVID-mitigation strategy proposed a blended approach to clinical skills teaching.14 Students are taught some procedures face-to-face in clinical spaces and some synchronously via the virtual platform. All 319 fourth year students were provided with similar packs. They collected them during an induction day in September. The content of the teaching packs was revised to include more items and a small sharps bin. From January 2021, students will revise the skills face-to-face in the clinical skills centres.
References
- 1.General Medical Council . Outcomes for graduates. GMC, 2018. www.gmc-uk.org/-/media/documents/dc11326-outcomes-for-graduates-2018_pdf-75040796.pdf. [Accessed 24 October 2020]. [Google Scholar]
- 2.Dreyfus SE, Dreyfus H. A five-stage model of the mental activities involved in directed skill acquisition. University of California Berkeley, 1980. [Google Scholar]
- 3.Miller GE. The assessment of clinical skills/competence/performance. Acad Med 1990;65:S63–7. [DOI] [PubMed] [Google Scholar]
- 4.Kolb DA. Experiential learning: Experience as the source of learning and development. Englewood Cliffs, N.J: Prentice-Hall, 1984. [Google Scholar]
- 5.Resuscitation Council UK . The ABCDE approach. Resuscitation Council UK, 2015. www.resus.org.uk/library/2015-resuscitation-guidelines/abcde-approach [Accessed 23 November 2020]. [Google Scholar]
- 6.Khan H. An adaptation of Peyton's 4-stage approach to deliver clinical skills teaching remotely. Med Ed Publish 2020;9:73. [Google Scholar]
- 7.Co Shih K, Chan JC-H, Chen JY, Lai JS-M. Ophthalmic clinical skills teaching in the time of COVID-19: A crisis and opportunity. Med Educ 2020;54:663–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.George J, Doto F. A simple five-step method for teaching clinical skills. Family Med 2001;33:577–8. [PubMed] [Google Scholar]
- 9.Peyton JW. Teaching and learning in medical practice. Heronsgate Rickmansworth, Herts: Manticore Europe Ltd, 1998. [Google Scholar]
- 10.Levett-Jones T, Lathlean J. Belongingness: A prerequisite for nursing students' clinical learning. Nurse Ed Prac 2008;8:103–11. [DOI] [PubMed] [Google Scholar]
- 11.Vivekananda-Schmidt P, Sandars J. Belongingness and its implications for undergraduate health professions education: a scoping review. Ed Prim Care 2018;29:268–75. [DOI] [PubMed] [Google Scholar]
- 12.Maslow A. Motivation and personality. New York: Harper & Row, 1954. [Google Scholar]
- 13.Maslow A. Toward a psychology of being. New York: Van Nostrand Reinhold Company, 1968. [Google Scholar]
- 14.University College London . Planning for the Autumn term 20–21. UCL, 2020. www.ucl.ac.uk/teaching-learning/node/8275/. [Google Scholar]