

Summary
Background:
Paediatric non-alcoholic fatty liver disease (NAFLD) is highly prevalent among children with obesity. The primary objective of this study was determining whether obesity severity is associated with NAFLD severity. By using paediatric classifications for severe obesity, clinicians may be able to better risk stratify patients, which in turn would guide more effective management and treatment.
Methods:
Retrospective cohort study including patients followed at Cincinnati Children's Medical Center for NAFLD. Patients were categorized as overweight or class I, II, III obese based on established body mass index (BMI) cut-offs. Liver disease severity was determined using biochemical, imaging (magnetic resonance elastography [MRE]), and histologic evidence of liver injury.
Results:
Three cohorts were studied individually based on the method used to assess disease severity (biochemical n = 767, imaging n = 366, and histology n = 249). Between the three cohorts, there were significant differences in age, proportion of patients with class II and class III obesity, and serum alanine transaminase (ALT) levels. In the biochemistry cohort, the odds of having ALT > 80 U/L were highest in patients with class III obesity (P = .026). In the imaging cohort, liver stiffness was significantly different between BMI groups of patients (P = .001). In the histology cohort, those with class III obesity had significantly higher odds of NAFLD activity score (NAS) ≥ 5 (P = .012).
Discussion:
Obesity severity is associated with liver disease severity. Patients with more severe obesity are more likely to have more advanced liver disease, a finding that can assist in risk stratification, as well as monitoring and treatment approaches.
Keywords: fibrosis, liver stiffness, steatohepatitis
1 ∣. INTRODUCTION
Paediatric non-alcoholic fatty liver disease (NAFLD) is one of the most common chronic liver diseases in children and adolescents with a prevalence of 8% in the general population and 26% in children with obesity.1 Physiologic and psychosocial comorbidities in paediatric NAFLD include atherosclerosis, hypertension, structural cardiac disease, type 2 diabetes, obstructive sleep apnea, anxiety, and impaired quality of life.2-4 Over time, paediatric NAFLD is associated with a 13.6-fold higher risk of death or liver transplantation compared with the general population over 20 years.5 There are currently no available treatment options for paediatric NAFLD and management is focused on risk factor modification through lifestyle changes, particularly as most children with NAFLD are affected by being overweight or obesity.6-8 The ultimate goal is weight stabilization for young children and weight loss of 5% to 10% of baseline body weight for post-pubertal subjects.9,10
While children with NAFLD are often affected by being overweight or obesity (approximately 70-90%), most children with obesity do not have NAFLD.4,11 The limited literature available to date has failed to reveal an association between body mass index (BMI) and liver disease severity. In a cohort of 390 paediatric NAFLD patients (mean BMI 32.7 kg/m2) enrolled by the Nonalcoholic Steatohepatitis Clinical Research Network (NASH-CRN), histologic features such as zonality of steatosis and fibrosis were not significantly associated with BMI. 12 Similarly, in another study examining 158 adolescents undergoing bariatric surgery (mean BMI 51.6 kg/m2), 59% had histologically confirmed NAFLD, and in those patients, liver disease presence and severity was not significantly associated with BMI.13 However, these studies assessed BMI as a continuous variable. Further, both the NASH-CRN cohort and the bariatric cohort may not reflect the spectrum of obesity or liver disease severity among children with NAFLD. The NASH-CRN requires biopsy confirmation of NAFLD for enrollment and therefore may be subject to selection bias for children with more advanced NAFLD. Likewise, the bariatric cohort by definition includes only children with severe obesity and did not allow for comparison of the severity of NAFLD in children of less severe obesity classes.12,13
Analyzing severity of obesity categorically may be more informative in the context of NAFLD risk, as prevalence of multiple metabolic risk factors increases in children with severe obesity,12,14 which is currently defined in children as a BMI that is greater than or equal to 120% or 1.2× the 95th percentile for age and sex or BMI ≥ 35 kg/m2, whichever is lower.15 Given the close association of NAFLD with these risk factors, we hypothesized that severe paediatric obesity, as defined by current thresholds, is associated with severity of NAFLD. Understanding if severe obesity is an independent risk factor for more severe NAFLD could facilitate management decisions, such as whether to proceed with a liver biopsy, or guide treatment recommendations and frequency of follow-up.16
The primary objective of this study was to determine whether the severity of obesity is associated with NAFLD severity in children with NAFLD, as determined using histology, imaging, and serologic markers of disease severity, in patients with varying degrees of obesity.
2 ∣. METHODS
2.1 ∣. Study design
This was a retrospective cohort study performed at the Steatohepatitis Center of Cincinnati Children's Hospital Medical Center (CCHMC) in Cincinnati, Ohio. Patients are referred to the Steatohepatitis Center both via external referrals from primary care physicians as well as through internal referrals from subspecialists within CCHCM, such as emergency department physicians, endocrinologists, or cardiologists. Referrals are also received from the multidisciplinary obesity clinics at CCHMC. The most common reasons for referral include elevated liver enzymes and/or hepatic steatosis incidentally noted on imaging. Institutional Research Ethics Board approval was obtained prior to data collection. Participants were included from 2011 to 2017. They were excluded if they were lean (BMI < 85th percentile), had secondary liver disease, or had history of bariatric surgery.
2.2 ∣. Variables
The following variables were collected: age, sex, race, ethnicity, BMI, anthropometrics at the time of interest (first visit, day of magnetic resonance imaging-proton density fat fraction/magnetic resonance elastography [MRI-PDFF/MRE], and day of liver biopsy), serum aminotransferase levels, haemoglobin A1c (HbA1c), lipid panel, liver biopsy results, and MRI-PDFF/MRE results. The use of the following medications 3 months preceding documented alanine transaminase (ALT), imaging, and liver biopsy, respectively, was recorded: insulin, metformin, vitamin E, statins, anti-hypertensives, levothyroxine, and psychotropic medications. Presence of type 2 diabetes mellitus (T2DM) and dyslipidemia were documented.
2.3 ∣. Definitions
Classifications of weight were as follows: overweight, class I obesity, class II severe obesity, or class III severe obesity, using recommended BMI percentile cutoffs (85th-95th, 95th to 1.19 × 95th, 1.2-1.4 × 95th, greater than 1.4 × 95th, respectively).16 T2DM was defined as HbA1c ≥ 6.5% and/or a positive oral glucose tolerance test (serum glucose level at 2 h ≥ 200 mg/dL) and/or a diagnosis of T2DM by an endocrinologist. Dyslipidemia was defined as either total cholesterol (TC) > 200 mg/dL, low-density lipoprotein (LDL) > 130 mg/dL, or triglycerides (TG) > 100 mg/dL for patients ages 0 to 9 years and greater than 130 mg/dL for age 10 to 19 years.17 Participants were separately categorized for low high-density lipoprotein (HDL) with a threshold set to less than 40 mg/dL.
Histologic scores for steatosis, ballooning, lobular inflammation, portal inflammation, and fibrosis were recorded along with the NAFLD activity score (NAS).18 A NAS cut off of greater than or equal to 5 was used to define disease severity (mild vs severe). Advanced fibrosis was defined as a fibrosis score greater than or equal to stage 2.19,20
2.4 ∣. Cohorts
Liver disease severity was categorized in three different ways to reflect the currently available clinical modalities for assessing NAFLD, generating three separate cohorts that were studied individually:
Biochemically determined liver disease severity: using the ALT level obtained closest to (and within 6 months from) the first clinic visit. ALT was analysed as both a continuous and a categorical variable as both approaches have significant associations with NASH.21 An ALT cutoff of greater than or equal to 80 U/L, which has been shown to have 62% specificity for the diagnosis of NASH in children with obesity, was used.21 The BMI at the time of the clinic visit was documented.
Radiographically determined liver disease severity: using magnetic resonance imaging proton density fat fraction (MRI-PDFF) and elastography (MRE) data previously obtained for clinical indications were used. At CCHMC, children are referred for MRI-PDFF/MRE if they have persistently elevated liver enzymes (ALT>50 U/L) in the context of a rising BMI or multiple concurrent metabolic comorbidities. BMI was recorded from the time of MRE or within 3 months of MRE if the former was unavailable. In participants with multiple MREs, only the first was included. The hepatic fat fraction (HFF), mean stiffness, and liver volume were documented. The proportion of participants with a liver stiffness above a cutoff of 2.71 kPa was determined, as this has demonstrated an 85% specificity for discriminating children with early versus late stages of fibrosis (stages 0-1 vs 2-4, respectively) in one study,22 while comparable stiffness values (2.70 and 2.77 kPa) had best classification threshold at greater than or equal to 90% specificity for detecting any fibrosis versus no fibrosis in another paediatric study.23
Histologically determined liver disease severity: liver biopsies previously obtained for clinical indications were reviewed. At CCHMC, children are referred for a liver biopsy if they have persistently elevated liver enzymes (ALT>80 U/L), a concerning MRE (eg, stiffness > 2.71 kPa), imaging concerns suggestive portal hypertension, or if there is suspicion of another or concurrent liver disease requiring biopsy confirmation (eg, autoimmune hepatitis).9 The BMI, height, and weight closest to and within 3 months of the liver biopsy were recorded.
2.5 ∣. Statistical analysis
Descriptive statistics of demographics and liver disease severity measurements were calculated for all three cohorts. Means (standard deviations) and medians (25th and 75th percentiles) were used to describe continuous variables based on their distribution; N and percentages were used to describe categorical variables. Linear trend for the continuous outcomes (serum biochemistries and MRI data, log transformed) with the obesity groups were tested using orthogonal contrast in one-way analysis of variance (ANOVA) to see if individual variables changed with increasing severity of obesity. For ordinal variables (histology), this trend was tested using nonzero correlation test. In addition to the marginal relationships, conditional relationships were also modelled between the liver severity outcomes and the BMI groups using analysis of covariance (ANCOVA) for the continuous outcomes, and logistic regression for the categorical outcomes. A backward model selection procedure was used to identify the final model for each cohort. The covariates considered in the model selection were age, sex, ethnicity, T2DM status, metformin, and vitamin E use. The BMI group variable was always included in the model regardless of whether it was selected or not. BMI was also assessed as a continuous variable. SAS 9.4 software was used. Statistical significance was claimed at the.05 level.
3 ∣. RESULTS
There were a total of 767 participants in the biochemical cohort, 366 in the radiographic, and 249 participants in the histologic. Baseline demographics of the three cohorts were similar in terms of ethnicity and sex; there were significant differences in age, the proportion of participants with class II and class III obesity, and ALT levels (Table 1).
TABLE 1.
Comparisons of the three cohorts
| Biochemistry Cohort |
Imaging Cohort |
Histology Cohort |
||
|---|---|---|---|---|
| Variables | n = 767 | n = 366 | n = 249 | P value |
| Age (years) | 13 ± 3a | 13 ± 3 | 14 ± 3a | .004 |
| Hispanic Ethnicity, % | 19% | 21% | 22% | .730 |
| Male Sex, % | 62% | 66% | 67% | .301 |
| Body Mass Index groups | ||||
| Overweight | 4% | 3% | 2% | .0168 |
| Obese Class I | 22% | 20% | 19% | .520 |
| Obese Class II (CII) | 37%a | 29%a | 34%a | .048 |
| Obese Class III (CIII) | 37%a | 48%a | 46%a | .002 |
| T2DM, % | 7% | 6% | 10% | .182 |
| Vitamin E use, % | <1% | 7% | 4% | <.001 |
| Metformin use, % | 20% | 21% | 29% | .019 |
| ALT (U/L) | 75 ± 56 | 89 ± 65 | 110 ± 77 | <.001 |
Statistically significantly different variables. Pearson chi and Bartlett test for equal variances were performed.
3.1 ∣. Biochemical cohort
Of the 767 participants included, 4% were overweight while 22%, 37%, and 37% had class I, II, and III obesity, respectively. The majority of participants were male (62%) and non-Hispanic (81%), with a mean age of 13 ± 3 years. Four participants (less than 1%) were taking vitamin E, 156 (20%) were taking metformin, and 50 (7%) had T2DM at the time the serum biochemistries associated with the first clinic visit were obtained.
The four obesity severity groups within this cohort were different in terms of sex (greater representation of males in the severe obesity groups, P = .015), ethnicity (lower percentage of Hispanics in the class III severe obesity group, P = .006), and metformin use (less common in overweight participants, P = .023). There was no significant difference in the proportion of participants with T2DM (P = .920), or in use of vitamin E (P = .921) between the obesity groups (Table 2).
TABLE 2.
Differences in demographics
| Overweight | Obese Class I | Obese Class II | Obese Class III | P value* | |
|---|---|---|---|---|---|
| Biochemistry cohort | n = 30 | n = 169 | n = 281 | n = 287 | |
| Male Sex; n (%) | 15 (50%) | 90 (53%) | 187 (67%) | 185 (64%) | .015 |
| Hispanic Ethnicity; n (%) | 7 (23%) | 44 (26%) | 64 (23%) | 34 (12%) | .006 |
| T2DM; n (%) | 1 (4%) | 11 (7%) | 18 (7%) | 20 (7%) | .920 |
| Vitamin E use; n (%) | 0 (0%) | 1 (1%) | 1 (<1%) | 2 (1%) | .921 |
| Metformin use; n (%) | 1 (3%) | 31 (18%) | 53 (19%) | 71 (25%) | .023 |
| Imaging cohort | n = 10 | n = 74 | n = 107 | n = 174 | |
| Sex (%Male) | 4 (40%) | 40 (54%) | 75 (70%) | 122 (70%) | .02 |
| T2DM; n (%) | 1 (10%) | 4/71(6%) | 8/98 (8%) | 7/163 (4%) | .58 |
| Hispanic (n; %) | 2 (20%) | 20 (27%) | 27 (25%) | 28 (16%) | .39 |
| Metformin (n; %) | 4 (40%) | 13 (18%) | 24 (22%) | 35 (20%) | .40 |
| Vitamin E use (n; %) | 0 (0%) | 7 (9%) | 5 (5%) | 15 (9%) | .42 |
| Histology cohort | n = 4 | n = 48 | n = 84 | n = 113 | |
| Sex (%Male) | 3 (75%) | 28 (58%) | 57 (68%) | 78 (69%) | .58 |
| T2DM; n (%) | 0 (0%) | 3 (6%) | 9 (11%) | 12 (11%) | .72 |
| Hispanic (n; %) | 2 (50%) | 10 (21%) | 23 (27%) | 19 (17%) | .30 |
| Metformin (n; %) | 0 (0%) | 16 (33%) | 24 (29%) | 31 (28%) | .54 |
| Vitamin E use (n; %) | 0 (0%) | 3 (6%) | 2 (2%) | 5(4%) | .70 |
Note. Exact Chi-square tests were used for variables with at least one cell less than 5 in the frequency table. Otherwise asymptomatic Chi-square test was used. Percentages reflect the % within each weight subgroup unless otherwise noted.
Significant linear trends were seen in log-transformed serum ALT (P = .001) and gamma-glutamyl transferase (GGT; P < .001) levels with obesity severity. A similar trend was not seen with aspartate aminotransferase (AST) and alkaline phosphatase (ALP) levels (P = .16 and .60, respectively, Table 3). Neither serum lipid levels (total cholesterol, LDL, HDL, and TG) nor glucose and HbA1c levels displayed a linear trend with obesity severity (P > .05, Table 3).
TABLE 3.
Laboratory characteristics (median 25th percentile, 75th percentile) for continuous and ordinal variables; n (%) for binary variables
| Variables | Overweight | Obese Class I | Obese Class II | Obese Class III | P value a | |
|---|---|---|---|---|---|---|
| Biochemistry | ALT (U/L) | 41 (26,63) | 59 (39,82) | 61 (42,91) | 64 (41,97) | .001 |
| Proportion of patients with ALT ≥ 80 U/L; n(%) | 4 (13%) | 43 (25%) | 86 (31%) | 103 (36%) | .002 | |
| AST (U/L) | 29 (24,42) | 35 (25,49) | 35 (27,53) | 37 (26,54) | .16 | |
| GGT (U/L) | 20.5 (14,36) | 27 (19.5,47) | 33 (22,50) | 39 (26,58) | <.0001 | |
| ALP (U/L) | 151 (112,301) | 195.5 (114.5,277) | 208 (123,293) | 184 (106,277.5) | .60 | |
| HbA1c (%) | 5.1 (5,5.2) | 5.2 (5,5.4) | 5.2 (5,5.4) | 5.3 (5,5.5) | .14 | |
| Triglycerides (mg/dL) | 102 (61,163) | 133 (85,199) | 135 (90.5,184) | 127 (95,168.5) | .072 | |
| HDL (mg/dL) | 44 (35,52) | 38 (31,45) | 38 (32,45) | 38.5 (32,44) | .072 | |
| LDL (mg/dL) | 151 (112,301) | 195.5 (114.5,277) | 207 (122,293) | 178 (103,272) | .78 | |
| Imaging | Liver volume (mL) | 1555.5 (1401,1846) | 1781.5 (1331,2103) | 2052 (1660,2307) | 2372.5 (1905,2755) | .0002 |
| PDFF | 11.7 (2.1,21) | 10 (4,17) | 10.6 (6,22) | 13 (7.03,21) | .19 | |
| Elastography (kPa) | 1.96 (1.6,2.2) | 2.37 (2.1,2.71) | 2.34 (2.1,2.77) | 2.5 (2.24,2.81) | .0007 | |
| N,% of patients with stiffness > 2.71 kPa | 2 (20%) | 16 (22%) | 29 (27%) | 53 (30%) | .13 | |
| Histology | Steatosis score | 2 (2,2.5) | 2 (1,3) | 2 (1,3) | 2 (1,3) | .25 |
| Lobular inflammation score | 1 (0.5,2) | 1 (1,2) | 1 (1,2) | 1 (1,2) | .93 | |
| Portal inflammation score | 0 (0,0.5) | 1 (0,1) | 1 (0,1) | 1 (0,1) | .76 | |
| Ballooning | 1 (0.5,1) | 1 (0,1) | 1 (0,1) | 1 (0,1) | .68 | |
| NAFLD activity score | 4.5 (3,5.5) | 4 (3,5) | 3.5 (3,5) | 4 (3,5) | .37 | |
| % of patients with NAS ≥ 5 | 2 (50%) | 13 (27%) | 23 (27%) | 49 (43%) | .075 | |
| Fibrosis score | 0.5 (0,1) | 1 (0,1) | 1 (0,2) | 1 (0,1) | .18 | |
| % of patients with ≥ F2 | 0 | 6 (13%) | 21 (25%) | 25 (22%) | .20 |
Orthogonal contrast for linear trend from one-way ANOVA was done for log transformed continuous variables (Lab and MRI); Nonzero correlation test was done for ordinal variables (Histology).
The proportion of participants with an ALT ≥ 80 U/L was different among the BMI groups and highest in those with severe obesity (P = .022, Table 4). After controlling for sex, ethnicity, and T2DM, the odds of having ALT ≥ 80 in participants with class III obesity were 3.2, 1.8, and 1.3 times higher than participants with overweight, class I, and class II obesity, respectively (p = .026).
TABLE 4.
Logistic regression for dichotomized ALT
| Outcome | Model | N | Variable | Effect | OR | Lower CI | Upper CI | P value |
|---|---|---|---|---|---|---|---|---|
| ALT ≥80 | 1a | 767 | BMI Group | .022 | ||||
| Overweight vs Class3 | 0.275 | 0.093 | 0.809 | |||||
| Class1 vs Class3 | 0.610 | 0.400 | 0.930 | |||||
| Class2 vs Class3 | 0.788 | 0.555 | 1.118 | |||||
| 2b | 721 | BMI Group | .026 | |||||
| Class3 vs Overweight | 3.152 | 1.038 | 9.571 | |||||
| Class3 vs Class1 | 1.791 | 1.135 | 2.827 | |||||
| Class3 vs Class2 | 1.321 | 0.915 | 1.907 | |||||
| Sex | Female vs. Male | 0.555 | 0.392 | 0.788 | .0010 | |||
| Ethnicity | Hispanic vs Non-Hispanic | 1.750 | 1.178 | 2.600 | .0056 | |||
| Type 2 DM | 0 vs 1 | 0.328 | 0.179 | 0.602 | .0003 |
Model 1 does not adjust for other covariates. BMI group is the only variable.
Model 2 is the model after backward selection with BMI group being forced in the model.
3.2 ∣. Radiographic cohort
In this cohort, 3% (n = 10) of participants were overweight, 20% (n = 74), 29% (n = 107), and 48% (n = 174) had class I, II, and III obesity, respectively. The majority of participants were male (66%) and non-Hispanic (79%), with a mean age of 13 ± 3 years. Twenty seven (7%) were on vitamin E, 76 (21%) were on metformin, and 20 (6%) met the criteria for T2DM at the time of the MRI.
The four obesity severity groups in the imaging cohort were different in terms of sex distribution (higher proportion of males in the more severe obesity categories, p = .020). Ethnicity, use of metformin, and prevalence of T2DM were not different between the obesity groups (Table 2).
There was no significant linear trend in the fat fraction with the severity of obesity (P = .190; Table 3). Liver stiffness and volume, however, progressively increased as obesity severity increased (P < .001 for both). The proportion of participants with liver stiffness more than 2.71 kPa was not significantly different among obesity severity groups (Table 3).
After controlling for age, metformin use, and T2DM diagnosis, liver stiffness was significantly different among the BMI groups (P = .001).
3.3 ∣. Histology cohort
Of the 249 participants, 2% were overweight, 19%, 34%, and 46% had class I, II, and III obesity, respectively. The majority of participants were male (67%) and non-Hispanic (78%), with a mean age of 14 ± 3 years. Ten participants (4%) were on vitamin E, 71 (29%) were on metformin, and 24 (10%) met the criteria for T2DM at the time of biopsy.
The obesity severity groups in the histology cohort were not different in terms of sex and ethnicity distribution, use of vitamin E or metformin, and T2DM diagnosis (Table 2).
There was no significant difference between severity of steatosis, lobular inflammation, ballooning, portal inflammation, and fibrosis between the obesity severity groups (Table 3). The mean NAS also did not differ between the groups (Figure 1); however, there was a trend towards a significant difference in the proportion of participants with a NAS ≥ 5 among the groups (P = .075; Table 3). After controlling for age and metformin use, participants with class II obesity had 55% lower odds of NAS ≥ 5 compared with those with severe obesity (P = .012, Table 5). The proportion of participants with fibrosis greater than or equal to 2 was not significantly different among the groups (P = .130).
TABLE 5.
Logistic regression results for binary NAS and fibrosis (the outcome being modelled is the higher category)
| Outcome | Model | N | Covariate | Effect | OR | Lower CI | Upper CI | P value |
|---|---|---|---|---|---|---|---|---|
| NAS ≥ 5 | 1a | 249 | BMI Group | .075 | ||||
| Overweight vs Class3 | 1.326 | 0.18 | 9.75 | |||||
| Class1 vs Class3 | 0.563 | 0.272 | 1.164 | |||||
| Class2 vs Class3 | 0.471 | 0.255 | 0.868 | .016c | ||||
| 2b | 248 | BMI Group | .056 | |||||
| Overweight vs Class3 | 1.614 | 0.212 | 12.307 | |||||
| Class1 vs Class3 | 0.565 | 0.269 | 1.185 | |||||
| Class2 vs Class3 | 0.449 | 0.24 | 0.837 | .012c | ||||
| Age | 0.905 | 0.834 | 0.982 | .017 | ||||
| Metformin | Yes vs. No | 1.742 | 0.953 | 3.182 | .071 | |||
| FIB | 1a | 248 | BMI Group | .52 | ||||
| Overweight vs Class3 | 0.556 | 0.08 | 3.866 | |||||
| Class1 vs Class3 | 0.698 | 0.368 | 1.327 | |||||
| Class2 vs Class3 | 1.124 | 0.667 | 1.896 | |||||
| 2b | 246 | BMI Group | .69 | |||||
| Overweight vs Class3 | 0.594 | 0.084 | 4.224 | |||||
| Class1 vs Class3 | 0.745 | 0.389 | 1.426 | |||||
| Class2 vs Class3 | 1.088 | 0.642 | 1.844 | |||||
| Age | age | 0.91 | 0.848 | 0.977 | .009 | |||
| Type 2 DM | Yes vs. No | 1.91 | 0.871 | 4.189 | .11 | |||
| FIB≥2 | 1a | 249 | BMI Group | .19 | ||||
| Overweight-Class1 vs Class3 | 0.475 | 0.182 | 1.24 | |||||
| Class2 vs Class3 | 1.187 | 0.611 | 2.305 | |||||
| 2b | 249 | BMI Group | .25 | |||||
| Overweight-Class1 vs Class3 | 0.513 | 0.195 | 1.351 | |||||
| Class2 vs Class3 | 1.194 | 0.61 | 2.338 | |||||
| Age | age | 0.906 | 0.83 | 0.99 | .029 | |||
Model 1 does not adjust for other covariates. BMI group is the only variable.
Model 2 is the model after backward selection with BMI group being forced in the model.
The p-value was for the specific contrast.
3.4 ∣. BMI and continuous analyses
To compare the approach of using BMI cutoffs to group patients according to their obesity severity versus assessing BMI as a continuous measure, which is what has been done previously in the literature, we repeated the analyses using BMI as a continuous variable.
In the biochemistry cohort, non-Hispanic participants, as well as those on metformin, had higher BMI (P ≤ .001; Table S1). Otherwise, sex, presence of type 2 diabetes, and vitamin E use did not differ based on BMI. In terms of laboratory values, the following variables significantly correlated with BMI: GGT, ALP, and LDL (P < .001; Table S2). BMI was not significantly correlated with ALT levels (P = .546; Table S3).
In the imaging cohort, non-Hispanic patients had higher BMI P = .005; Table S1). Liver volume and liver stiffness both significantly correlated with BMI (P < .001; Table S2). Patients with a higher BMI had a higher stiffness after controlling for confounders (P < .0001; Table S3).
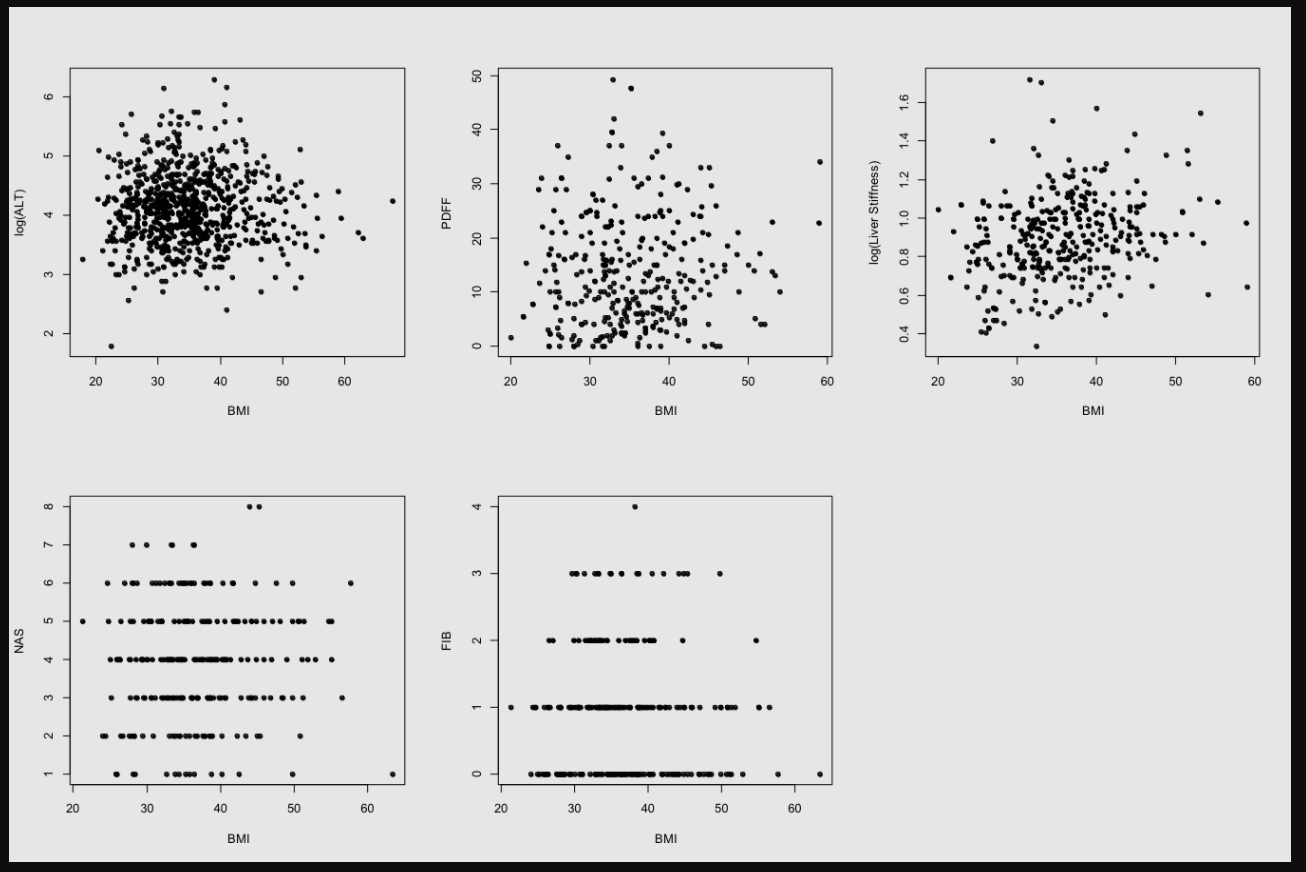
Regarding the histologic cohort, non-Hispanic patients had higher BMI (P = .004; Table S1). BMI significantly correlated with steatosis score (P = .044), but not with the NAS, lobular inflammation, portal inflammation, ballooning, or fibrosis score (Table S2). Lastly, there was no correlation between BMI and NAS or fibrosis (Table S3; Figure S1).
4 ∣. DISCUSSION
To our knowledge, this is the largest study assessing whether severity of obesity is associated with liver disease severity in paediatric NAFLD and the first assessing severity of obesity using appropriate paediatric classifications of obesity. In all three cohorts where NAFLD severity was determined differently, there was evidence of more severe liver disease in those with class III obesity. This is despite the fact that the cohorts were different in variables that reflect disease severity (eg, prevalence of T2DM and use of vitamin E treatment). The association of NAFLD severity with severe paediatric obesity extends the field, as pre-existing literature, which had analysed BMI as a continuous variable and had determined disease severity using histology, had not identified an association with higher BMI and liver disease severity.12,13
While ALT is considered an imprecise marker of liver disease severity,24 it is the tool of choice to screen for and monitor the progression of liver disease severity in the clinical setting.9 In our study, participants with class III obesity had higher serum ALT levels and increased odds of an ALT level > 80 U/L compared with participants with less obesity. A histologic diagnosis of non-alcoholic steatohepatitis (NASH) is almost twice as common in those with serum ALT levels > 80 U/L,21 which is in accordance with our findings of an increased proportion of participants with NAS ≥ 5 in those with class III obesity. While no NAS cutoff confirms a diagnosis of NASH, scores ≥ 5 have been used in research studies as a proxy for NASH. Interestingly, when studying BMI as a continuous, rather than a categorical variable, there was no association between BMI and ALT levels or BMI and NAS. This highlights the importance of using the predefined BMI thresholds of paediatric obesity classification in clinical practice.
While the proportion of patient with stiffness greater than 2.71 kPa did not differ among obesity groups, median liver stiffness values were highest among the children with class III obesity. Although liver stiffness using ultrasound or MR is well validated as a marker of advanced hepatic fibrosis, we did not find significant differences in the fibrosis stage or the frequency of advanced fibrosis by obesity class in the histology cohort.23 However, as MRE samples a greater proportion of the liver compared with biopsy, there may be potential for discordance between liver stiffness and histology due to sampling error, plus the limitation of assessing agreement between a continuous variable (liver stiffness) with categorical histological grading. MRE may be helpful for noninvasively assessing severity of fibrosis, particularly in children with severe obesity in whom ultrasound assessment can be limited by excess subcutaneous tissue.
Our study surprisingly did not show a difference in HbA1c, dyslipidemia, or proportion of participants with T2DM among obesity groups, all of which are traditional risk factors for metabolic syndrome. This may have occurred as a large percentage of participants in each cohort (20%-29%), particularly the histologic (29%), were on metformin with many of those participants prophylactically on it in the absence of T2DM for reasons such as polycystic ovarian syndrome (PCOS) or use of psychotropic medications. Additionally, visceral adiposity plays a significant role in the pathogenesis of NAFLD, and we did not have available waist circumferences for all participants. Lastly, other variables not assessed in our study, such as dietary intake, oxidative stress, sleep apnea, hormonal dysregulation, genetic polymorphisms, dysbiosis, and altered bile acid physiology may have contributed to the higher proportion with NAS ≥ 5 seen in participants with class III obesity.25-28 This remains to be investigated further.
There are several limitations to our study. The retrospective nature introduces the potential for referral and selection bias. The three study cohorts were different, as shown by the proportion of participants with class II and III obesity among them. The three cohorts also differed significantly in terms of age, vitamin E use, and ALT levels. The ALT level was highest in the histology cohort, reflecting that those with higher ALT levels were more likely to be referred for biopsy. We also had a limited number of participants in the overweight group, which may reflect a regionally higher proportion of severe obesity in our NAFLD programme. The racial and ethnic diversity are also reflective of our region, but whether these findings apply to children of different racial or ethnic background will need to be validated. These limitations are mitigated by the large sample size, relatively equal distribution of the cohort across the three different paediatric classes of obesity, and the analysis of liver disease severity using three current, clinically relevant approaches to assess liver disease severity
As the prevalence of NAFLD continues to rise, it will be imperative to improve our ability to non-invasively assess the risk of more severe liver disease severity to help guide management and determine which children merit more intensive evaluation or interventions. Our data show that increasing severity of obesity, defined using current clinical classifications for paediatric severe obesity rather than BMI alone, is indeed associated with liver disease severity. Given the heightened burden of NAFLD, as well as the difficulty of treating the underlying severe obesity with routine lifestyle counselling alone, children and adolescents with severe class II or III obesity should promptly be offered more intensive multidisciplinary lifestyle interventions, including consideration of a discussion regarding bariatric surgery if currently recommended clinical criteria are met.9,29
Supplementary Material
{kind=link}
ACKNOWLEDGEMENTS
No grant support or writing assistance was utilized.
Abbreviations:
- NAFLD
non-alcoholic fatty liver disease
- BMI
body mass index
- MRI-PDFF
magnetic resonance imaging-proton density fat fraction
- MRE
magnetic resonance elastography
- ALT
alanine transaminase
- HbA1c
haemoglobin A1c
- T2DM
type 2 diabetes mellitus
- LDL
low-density lipoprotein
- TG
triglycerides
- HDL
high-density lipoprotein
- NAS
NAFLD activity score
- GGT
gamma-glutamyl transferase
- AST
aspartate aminotransferase
- NASH
non-alcoholic steatohepatitis
- PCOS
polycystic ovarian syndrome
Footnotes
CONFLICT OF INTEREST
No conflict of interest was declared.
SUPPORTING INFORMATION
Additional supporting information may be found online in the Supporting Information section at the end of the article.
REFERENCES
- 1.Elizabeth LY, Golshan S, Harlow KE, et al. Prevalence of nonalcoholic fatty liver disease in children with obesity. J Paediatr. 2019;207:64–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bush H, Golabi P, Younossi ZM. Pediatric non-alcoholic fatty liver disease. Children (Basel). 2017;4(6). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kerkar N, Durso C, Nostrand K, et al. Psychosocial outcomes for children with nonalcoholic fatty liver disease over time and compared with obese controls. J Pediatr Gastroenterol Nutr. 2013;56(1):77–82. [DOI] [PubMed] [Google Scholar]
- 4.Schwimmer JB. Clinical advances in pediatric nonalcoholic fatty liver disease. Hepatology. 2016;63(5):1718–1725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Feldstein C, Treeprasertsuk B, Enders A. The natural history of non-alcoholic fatty liver disease in children: a follow-up study for up to 20 years. Gut. 2009;58(11):1538–1544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Nobili V, Manco M, Devito R, et al. Lifestyle intervention and antioxidant therapy in children with nonalcoholic fatty liver disease: a randomized, controlled trial. Hepatology. 2008;48(1):119–128. [DOI] [PubMed] [Google Scholar]
- 7.Giorgio V, Prono F, Graziano F, Nobili V. Pediatric non alcoholic fatty liver disease: old and new concepts on development, progression, metabolic insight and potential treatment targets. BMC Pediatr. 2013;13:40. 10.1186/1471-2431-13-40 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lavine JE, Schwimmer JB, Natta VM, et al. Effect of vitamin E or metformin for treatment of nonalcoholic fatty liver disease in children and adolescents: the TONIC randomized controlled trial. JAMA. 2011;305(16):1659–1668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Vos MB, Abrams SH, Barlow SE, et al. NASPHGAN Clinical practice guidelines for the diagnosis and treamtent of non-alcoholic fatty liver disease in children: recommendations from the Expert Committee on NAFLD (ECON) and the North American Society of Pediatric Gastroenterology, Hepatology and Nutrition. J Pediatr Gastroenterol Nutr. 2017;64(2):319–334. 10.1097/MPG.0000000000001482 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.DeVore S, Kohli R, Lake K, et al. A multidisciplinary clinical program is effective in stabilizing BMI and reducing transaminase levels in pediatric patients with NAFLD. J Pediatr Gastroenterol Nutr. 2013;57(1):119–123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Schwimmer JB, Deutsch R, Kahen T, Lavine JE, Stanley C, Behling C. Prevalence of fatty liver in children and adolescents. Pediatrics. 2006;118(4):1388–1393. [DOI] [PubMed] [Google Scholar]
- 12.Africa JA, Behling CA, Brunt EM, et al. In children with nonalcoholic fatty liver disease, zone 1 steatosis is associated with advanced fibrosis. Clin Gastroenterol Hepatol. 2018. March;16(3):438–446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Xanthakos S, Jenkins T, Kleiner D, et al. High prevalence of nonalcoholic fatty liver disease in adolescents undergoing bariatric surgery. Gastroenterology. 2015;149(3):623–634.e8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cook S, Weitzman M, Auinger P, et al. Prevalence of a metabolic syndrome phenotype in adolescents: findings from the third National Health and Nutrition Examination Survey, 1988-1994. Arch Pediatr Adolesc Med. 2003;157(8):821–827. [DOI] [PubMed] [Google Scholar]
- 15.Kelly A, Barlow S, Rao G, et al. Severe obesity in children and adolescents: identification, associated health risks, and treatment approaches. Circulation. 2013;128(15):1689–1712. [DOI] [PubMed] [Google Scholar]
- 16.Lam C, Bandsma R, Ling S, Mouzaki M. More frequent clinic visits are associated with improved outcomes for children with NAFLD. Can J Gastroenterol Hepatol. 2016;2016:8205494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.For EO, Children RI. Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: summary report. Pediatrics. 2011;128(Suppl 5):S213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kleiner D, Brunt E, Natta M, et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology. 2005;41(6):1313–1321. [DOI] [PubMed] [Google Scholar]
- 19.Schwimmer JB, Behling C, Newbury R, et al. Histopathology of pediatric nonalcoholic fatty liver disease. Hepatology. 2005;42(3):641–649. [DOI] [PubMed] [Google Scholar]
- 20.Patton H, Lavine J, Natta M, et al. Clinical correlates of histopathology in pediatric nonalcoholic steatohepatitis. Gastroenterology. 2008;135(6):1961–1971.e2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Schwimmer JB, Newton KP, Awai HI, et al. Paediatric gastroenterology evaluation of overweight and obese children referred from primary care for suspected non-alcoholic fatty liver disease. Aliment Pharmacol Ther. 2013;38(10):1267–1277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Xanthakos S, Podberesky D, Serai S, et al. Use of magnetic resonance elastography to assess hepatic fibrosis in children with chronic liver disease. J Pediatr. 2014;164(1):186–188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Schwimmer JB, Behling C, Angeles JE, et al. Magnetic resonance elastography measured shear stiffness as a biomarker of fibrosis in pediatric nonalcoholic fatty liver disease. Hepatology. 2017;66(5):1474–1484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Mouzaki M, Trout AT, Arce-Clachar AC, et al. Assessment of nonalcoholic fatty liver disease progression in children using magnetic resonance imaging. J Pediatr. 2018;201:86–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Nobili V, Cutrera R, Liccardo D, et al. Obstructive sleep apnea syndrome affects liver histology and inflammatory cell activation in pediatric nonalcoholic fatty liver disease, regardless of obesity/insulin resistance. Am J Respir Crit Care Med. 2014;189(1):66–76. [DOI] [PubMed] [Google Scholar]
- 26.Valenti L, Alisi A, Galmozzi E, et al. I148M patatin-like phospholipase domain-containing 3 gene variant and severity of pediatric nonalcoholic fatty liver disease. Hepatology. 2010;52(4):1274–1280. [DOI] [PubMed] [Google Scholar]
- 27.Mouzaki M, Wang AY, Bandsma R, et al. Bile acids and dysbiosis in non-alcoholic fatty liver disease. PLoS ONE. 2016;11(5):e0151829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Mouzaki M, Comelli EM, Arendt BM, et al. Intestinal microbiota in patients with nonalcoholic fatty liver disease. Hepatology. 2013;58(1):120–127. [DOI] [PubMed] [Google Scholar]
- 29.Pratt J, Browne A, Brown NT, et al. ASMBS pediatric metabolic and bariatric surgery guidelines. Surg Obes Relat Dis. 2018;14(7):882–901. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.