

Abstract
PURPOSE OF REVIEW:
Widespread use of antiretroviral therapy (ART) has led to near-normal life expectancy in people with human immunodeficiency virus (HIV) infection. However, neurologic complications of HIV remain common; can affect any part of the neuraxis; and are due to direct effects of the virus, immunosuppression because of untreated HIV infection, aberrant immune responses in the setting of ART initiation, and ART toxicities.
RECENT FINDINGS:
HIV-associated neurocognitive disorder (HAND) remains one of the most common neurologic complications of HIV encountered today, but milder forms predominate in people on ART. No specific treatments for HAND exist, but small trials and epidemiologic evidence suggest paroxetine, intranasal insulin, and maraviroc may have utility in its treatment; further trials of these agents are ongoing. Widespread ART use has decreased the incidence of central nervous system opportunistic infections, but prognosis often remains poor in those who develop opportunistic infections. High-titer positive serum cryptococcal antigen is strongly predictive of cryptococcal meningitis and provides a tool to enhance diagnosis in areas with limited resources. HIV is an independent risk factor for stroke, and accelerated aging associated with HIV infection results in neurologic diseases of older age occurring at much younger ages in individuals infected with HIV. Ongoing HIV replication in the CSF despite peripheral virologic suppression may contribute to the development of HAND and may not improve despite adjusting the ART regimen to increase central nervous system penetrance.
SUMMARY:
Neurologists are likely to encounter patients infected with HIV in clinical practice. This article reviews the presentation, diagnosis, and management of the most common neurologic conditions associated with HIV infection and ART.
INTRODUCTION
While the advent of combination antiretroviral therapy (ART) in 1996 changed the course of human immunodeficiency virus (HIV) from a life-limiting infection to a chronic illness with near-normal life expectancy, neurologic complications of HIV remain common in both ART-naïve and ART-experienced patients who are HIV infected. These complications can affect any part of the neuraxis and stem primarily from four mechanisms: (1) direct effects of HIV (eg, neurocognitive impairment), (2) immunocompromise secondary to uncontrolled HIV infection (eg, opportunistic infections), (3) aberrant immune responses in the setting of ART initiation (eg, immune reconstitution inflammatory syndrome [IRIS]), and (4) adverse effects of ART (eg, peripheral neuropathy). With more than 1.1 million people who are HIV infected living in the United States1 and nearly 37 million people living with HIV worldwide,2 individuals who are HIV infected are likely to be encountered in clinical practice. Therefore, it is important that neurologists are familiar with the differential diagnosis and treatment of neurologic complications of HIV when confronted with either the ART-experienced patient with well-controlled HIV infection or the patient with newly diagnosed HIV infection with significant immunocompromise who is ART naïve. This article focuses on the clinical presentation, diagnosis, and management of neurologic complications of HIV and highlights current areas of HIV research relevant to neurologists.
DIRECT COMPLICATIONS OF HUMAN IMMUNODEFICIENCY VIRUS
HIV infection itself can affect any part of the nervous system at various points during the course of infection through a number of mechanisms, including toxic effects of viral proteins and low-level chronic inflammation induced by the infection. These conditions are reviewed in the following sections.
Human Immunodeficiency Virus–Associated Neurocognitive Disorder
HIV-associated neurocognitive disorder (HAND) represents a spectrum of conditions of varying severity, including (from mild to most severe) asymptomatic neurocognitive impairment, mild neurocognitive disorder, and HIV-associated dementia. Despite widespread ART use, HAND continues to affect up to 50% of patients with HIV and remains one of the most common neurologic complications of HIV encountered today.
EPIDEMIOLOGY.
Before the ART era, HIV-associated dementia occurred in up to 20% of individuals with acquired immunodeficiency syndrome (AIDS) and was almost always fatal.3 Today, HIV-associated dementia is rare in the developed world, occurring in fewer than 5% of patients with HIV. This decrease is largely attributed to widespread ART use, as patients with HIV who are on ART perform better on neuropsychological testing than their ART-naïve counterparts.3–7 However, while deficits associated with HAND remain stable in the majority of patients with HIV who are on ART, they rarely resolve even with optimal systemic virologic suppression (ie, undetectable plasma HIV RNA).8 Thus, the overall prevalence of HAND has remained nearly constant compared to the pre-ART era, with a shift toward less severe HAND stages being more common today (FIGURE 7-19).3,4 The persistence of HAND despite ART may reflect early brain involvement after HIV infection. For example, a study from Thailand found that one-fourth of participants with acute HIV infection demonstrated neurocognitive impairments that did not resolve with early initiation of ART, which correlated with higher levels of HIV RNA in the CSF.10 Blood-brain barrier disruption also occurs early in primary HIV infection and is unchanged in the first year of ART treatment,11 and changes in brain structure can be visualized within 3 months of primary HIV infection.12
FIGURE 7-1.
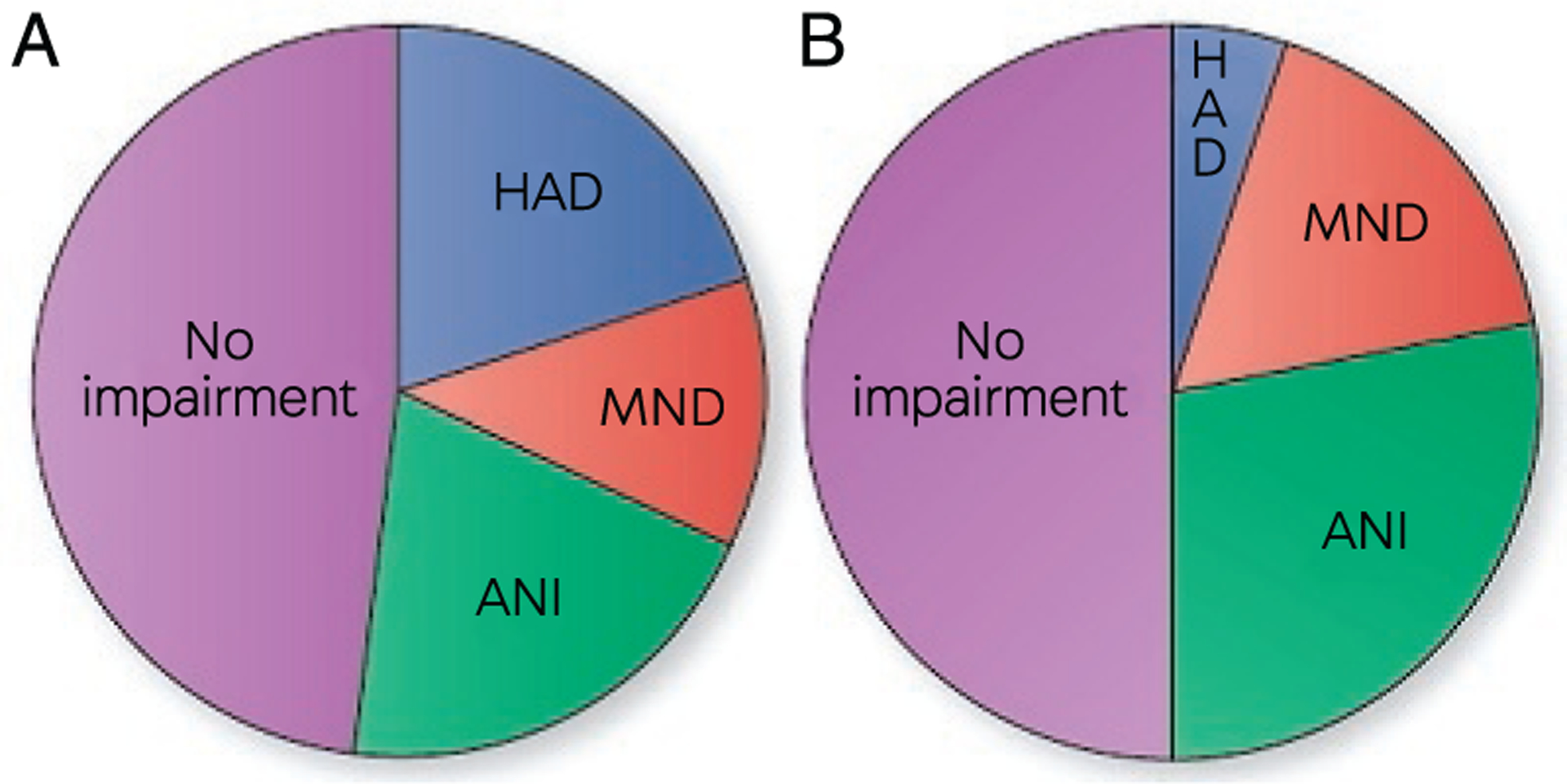
Proportion of patients with human immunodeficiency virus (HIV) infection with HIV-associated neurocognitive disorder (HAND) in the pre–antiretroviral therapy (ART) era (A) and ART era (B). The overall portion of people with HIV infection with HAND has not substantially changed between the pre-ART era and the current ART era. However, there has been a shift toward milder HAND stages with asymptomatic neurocognitive impairment (ANI) being much more common and HIV-associated dementia (HAD) being much less common, while minor neurocognitive disorder (MND) has remained relatively stable today compared to the pre-ART era.
Modified with permission from Saylor D, et al, Nat Rev Neurol.9 © 2016 The Authors.
CLINICAL PRESENTATION AND RISK FACTORS.
Unlike cortical dementias, such as Alzheimer disease, HAND is a subcortical cognitive disorder with prominent psychomotor retardation and motor symptoms, including bradykinesia, incoordination, and balance impairment. However, in the ART era, executive dysfunction, learning impairment, and problems with memory encoding and retrieval are becoming more prevalent.6 Deficits in impulse control, judgment, attention, and multitasking are also common (CASE 7-1).
CASE 7-1.
A 40-year-old woman presented to clinic with cognitive concerns. She was diagnosed with human immunodeficiency virus (HIV) 10 years previously, had been on a stable antiretroviral therapy (ART) regimen for the past 8 years, and had an undetectable plasma HIV RNA and a CD4+ T-cell count greater than 500 cells/mm3 for the past 5 years. Her CD4+ T-cell nadir was 34 cells/mm3. She worked as an office manager but reported trouble maintaining attention during meetings and difficulty organizing and executing tasks with multiple steps. Her partner noticed that she seemed “slower” than usual, and she recently had difficulty following a familiar recipe while cooking. Her past medical history was also significant for type 2 diabetes mellitus and tobacco use.
Neurologic examination was notable for slow finger tapping, saccadic interruptions of smooth pursuits, and a prominent snout reflex. Brain MRI revealed symmetric confluent subcortical leukoencephalopathy without enhancement and mild generalized cerebral atrophy (FIGURE 7-2). Vitamin B12 level and thyroid-stimulating hormone (TSH) were normal, and rapid plasmin reagin (RPR) was nonreactive. Lumbar puncture showed normal white blood cell count, protein, and glucose, and infectious workup was negative, including polymerase chain reaction (PCR) for JC virus.
COMMENT
This patient likely meets criteria for minor neurocognitive disorder, as she described mild to moderate cognitive symptoms that have negatively impacted her daily function. Formal neuropsychological testing could be obtained to further quantify and characterize her baseline cognitive deficits and could be repeated every 2 to 3 years to monitor her impairment. Workup for alternative etiologies of cognitive impairment was completed, but she should also be screened for depression and, if present, started on treatment. She has several risk factors for HIV-associated neurocognitive disorder (HAND), including a low nadir CD4+ T-cell count, tobacco use, and diabetes mellitus. Smoking cessation and tight control of her diabetes mellitus should be pursued to limit further cognitive impairment stemming from these conditions. No adjunctive treatment is currently available for HAND, but the patient may benefit from cognitive rehabilitation. In addition, her caregivers should be made aware of her cognitive deficits so they can provide extra support with complex tasks and ART adherence.
HAND can develop at any point during HIV infection, including in mild stages of immunosuppression,9 but lower nadir CD4+ T-cell count and a history of AIDS remain significant risk factors even in patients with HIV infection who are on ART with optimal virologic suppression.4,13,14 Cardiovascular risk factors, including hypertension, hyperlipidemia, tobacco use, diabetes mellitus, central obesity, and higher carotid intima-media thickness, increase the risk of cognitive impairment in adults who are HIV infected.15,16 Age older than 50 years has been significantly associated with HAND17,18 but may be confounded by the increased prevalence of cardiovascular risk factors in older adults.19 Substance abuse, especially methamphetamine, may also contribute,20–22 but recent studies have found no relationship between neurocognitive impairment and alcohol, marijuana, or cocaine use.23–25 Similarly, the effect of hepatitis C coinfection on neurocognitive function remains controversial,26,27 while higher levels of education are associated with less impairment.3
DIAGNOSIS.
Diagnosis and classification of HAND are based on the magnitude of deficits detected on neuropsychological testing and functional status assessments (TABLE 7-1).28 As with other cognitive disorders, a diagnosis of HAND should not be made in the setting of an acute illness. In the stable patient who is HIV infected and presents with cognitive symptoms, several HAND screening tools are available and easy to administer in an outpatient setting, including the HIV Dementia Scale (HDS),29 the International HIV Dementia Scale (IHDS),30 and the CogState computerized test battery.31 The CogState battery is more sensitive for detecting milder cognitive impairment but requires specialized computer software, while the HDS and IHDS are paper tests that are most sensitive for moderate to severe cognitive impairment.32 Patients with screening results concerning for HAND should be referred for formal neuropsychological testing and functional status assessments to confirm the diagnosis and assign a HAND stage.28 In addition, a careful search for other causes of cognitive impairment should be undertaken, including laboratory investigations for thyroid dysfunction, vitamin B12 deficiency, and syphilis, as a diagnosis of HAND should only be considered when alternative causes of cognitive impairment have been excluded. Central nervous system (CNS) imaging is not necessary to diagnose HAND but should be obtained to rule out alternative etiologies, including subdural hematoma, vascular dementia, and slowly progressive opportunistic infections such as progressive multifocal leukoencephalopathy (PML). The classic MRI finding in HAND is patchy or confluent symmetric subcortical T2 hyperintensities that do not enhance with gadolinium and do not demonstrate mass effect (FIGURE 7-2). CSF evaluation is not necessary in the routine workup of HAND. If undertaken to exclude other causes, CSF is usually normal but occasionally reveals a mild lymphocytic pleocytosis or elevated protein, especially in the setting of advanced HIV infection.
TABLE 7-1.
Classification of Human Immunodeficiency Virus–Associated Neurocognitive Disorder Stagea
| Diagnostic Criteria | ||
|---|---|---|
| HAND Stage | Neuropsychological Testing | Functional Status Assessment |
| Asymptomatic neurocognitive impairment | Impairment one or more standard deviations below the mean in two or more neurocognitive domains | Does not interfere with daily activities |
| Mild neurocognitive disorder | Impairment one or more standard deviations below the mean in two or more neurocognitive domains | Mild to moderate interference in daily activities |
| Human immunodeficiency virus (HIV)–associated dementia | Marked impairment two or more standard deviations below the mean in two or more neurocognitive domains | Marked interference in daily activities |
HAND = human immunodeficiency virus–associated neurocognitive disorder.
Modified with permission from Antinori A, et al, Neurology.28 © 2007 American Academy of Neurology.
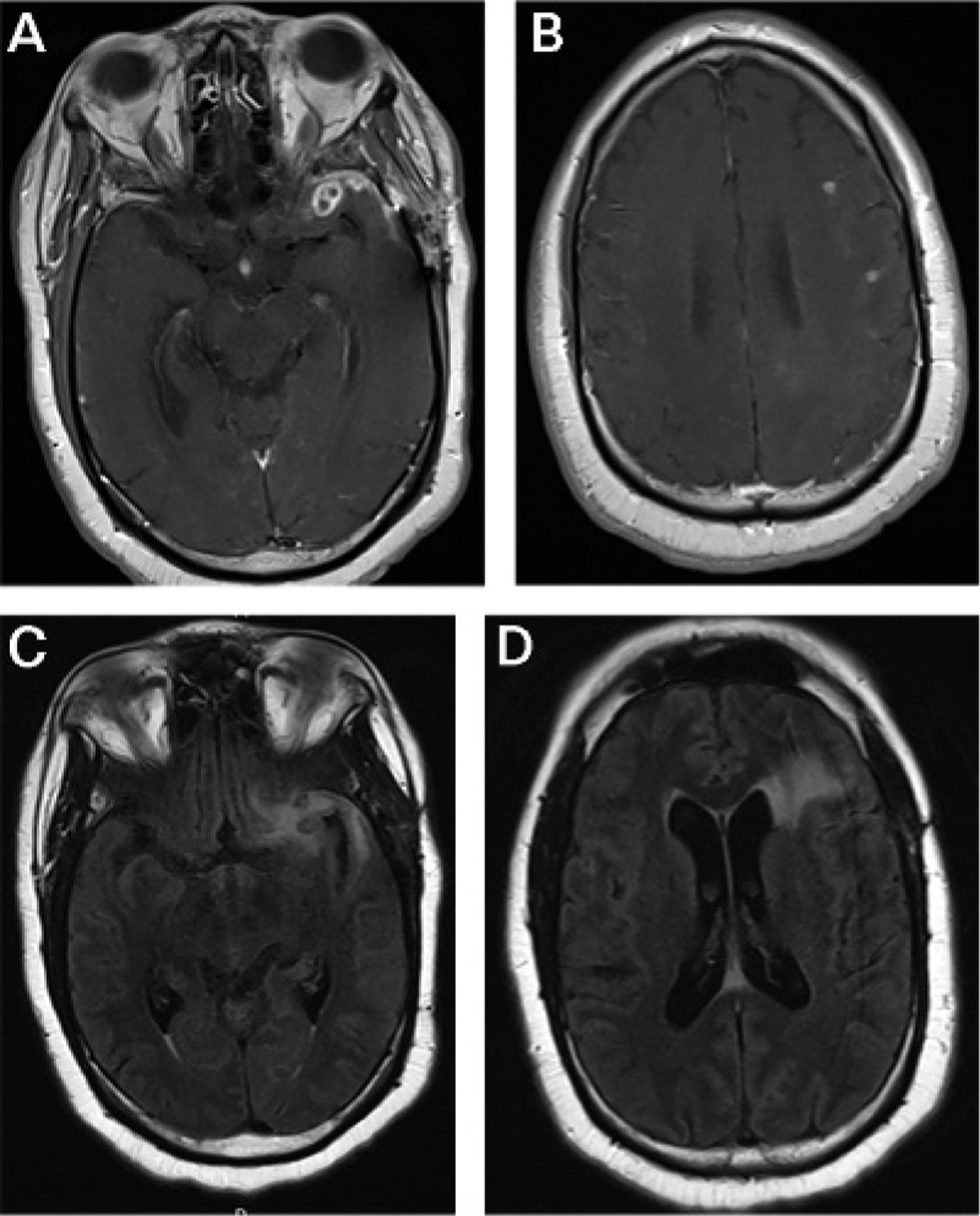
FIGURE 7-2.
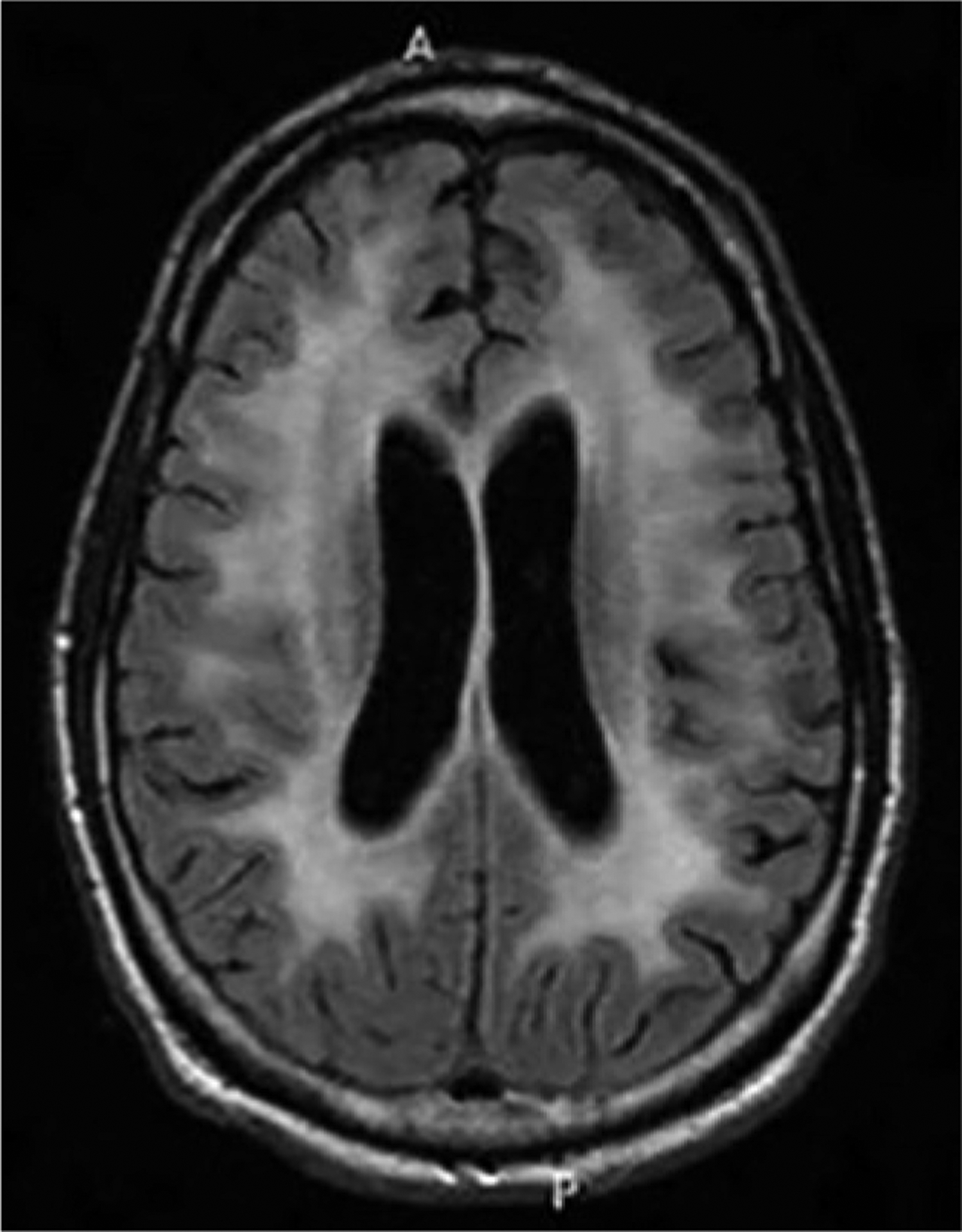
Imaging of the patient in CASE 7-1. Axial fluid-attenuated inversion recovery (FLAIR) MRI reveals symmetric confluent subcortical and periventricular white matter hyperintensities without mass effect. Mild cerebral atrophy is also present for the patient’s age.
MANAGEMENT.
Because individuals who are HIV infected and on ART exhibit better cognitive performance than those not on ART, all people with HAND should be on ART. ART may improve or resolve HAND in individuals with HIV infection who are ART naïve. However, many cases of HAND encountered in the United States today will occur in people who are HIV infected and on ART with optimal systemic virologic suppression, and HAND will persist in the majority of these individuals despite ART. Use of ART regimens with higher CNS penetrance has been proposed as a possible therapy to improve HAND in these people.33 However, subsequent studies have not demonstrated a beneficial effect with this approach, and several found worse neurocognitive outcomes among people on more highly penetrant ART regimens.34,35 This suggests highly penetrant drugs may have neurotoxic effects, possibly caused by impairing the bioenergetics of presynaptic nerve terminals.36 Early initiation of ART has also been proposed as a strategy to prevent HAND based on evidence that HIV enters the CNS very early in the course of infection. However, data from the Strategic Timing of AntiRetroviral Treatment (START) trial demonstrated that immediate ART initiation had a beneficial impact on AIDS-related outcomes but not neurocognitive outcomes when compared to delayed ART initiation after a mean follow-up of 3.3 years.37
In addition to ensuring that people with HAND are on ART, modifiable risk factors for cognitive impairment, including tobacco use, substance abuse, and sleep disorders such as obstructive sleep apnea, as well as cerebrovascular risk factors, should be identified and treated to minimize additional deleterious effects on cognitive function. Depression screening should be undertaken as depression often coexists with and worsens HAND. Routine monitoring of cognitive function with a tool such as the HDS or IHDS should be completed approximately every 6 months to ensure stability. Because most ART-experienced individuals with HAND exhibit stable levels of impairment, any significant changes in cognition should be reevaluated for other causes, such as new-onset thyroid dysfunction or subclinical cerebrovascular disease, especially in older people.
Currently no specific treatments for HAND exist, but they are urgently needed because even mild stages of HAND are associated with reduced quality of life and lower rates of ART adherence.38 A 2017 24-week randomized controlled trial in 45 people with HAND found paroxetine improved a summary neurocognitive performance measure.39 A trial of intranasal insulin is also ongoing after several studies revealed that insulin resistance, insulinlike growth factor, and soluble insulin receptor levels correlated with HAND.40,41 Cell culture data demonstrating a neuroprotective effect of insulin treatment provide further hope that it may have utility in HAND.42 Finally, maraviroc, a chemokine receptor CCR5 antagonist used to treat HIV infection, has shown neuroprotective effects in primate models of HIV,43 and its addition to standard ART regimens has been associated with improved neurocognitive performance in small pilot studies.44,45 A larger study of maraviroc intensification is ongoing.
Human Immunodeficiency Virus–Associated Peripheral Neuropathy
Distal symmetric polyneuropathy (DSPN), which affects 30% to 50% of individuals who are HIV infected,46 remains one of the most common neurologic complications of HIV in the ART era.47 DSPN can be directly caused by HIV, likely through both systemic and CNS immune activation, or can result from ART toxicity secondary to mitochondrial dysfunction.48,49
CLINICAL PRESENTATION AND RISK FACTORS.
HIV-associated DSPN presents similarly to other small fiber neuropathies, with slowly progressive numbness, tingling, and paresthesia in a stocking-glove distribution. Positive neuropathic symptoms (eg, burning, tingling) are more common than negative symptoms (eg, numbness). HIV-associated DSPN cannot be differentiated from ART-related DSPN based on clinical presentation. However, the temporal onset of symptoms may be helpful as ART-related DSPN usually begins in the first 3 to 6 months after ART initiation and may have a more subacute course. While HIV-related DSPN occurred primarily in people with CD4+ T-cell counts less than 200 cells/mm3 in the pre-ART era, higher CD4+ T-cell counts have been associated with DSPN during the ART era.50 Risk also increases with older age and tobacco use.50,51
DIAGNOSIS.
HIV-associated DSPN is a clinical diagnosis. Common signs include reduced distal pinprick, temperature, or vibratory sensation with reduced or absent ankle reflexes. Proprioception is usually spared, and weakness and hand involvement are uncommon. Nerve conduction studies are not necessary for the diagnosis but may show nonspecific signs of axonal neuropathy. Skin biopsy may show reduced epidermal nerve fiber layer density consistent with a small fiber neuropathy. Neither electrophysiologic nor pathologic studies can differentiate between HIV-associated and ART-associated DSPN. As many individuals who are HIV infected will have additional risk factors for DSPN, such as coexistent diabetes mellitus, hepatitis C infection, vitamin B12 deficiency, chronic kidney disease, or alcohol use, it is prudent to complete a standard workup for causes of DSPN in any individual who is HIV infected presenting with typical symptoms and address any additional identified risk factors.
MANAGEMENT.
The primary goals of treatment for DSPN are to prevent progression and alleviate pain. In ART-naïve individuals, DSPN often improves after ART initiation. In people with ART-related DSPN, the offending agent should be discontinued and a less neurotoxic agent initiated. Unfortunately, neuropathic symptoms may persist despite these strategies, and most standard neuropathic pain agents, including gabapentin, pregabalin, amitriptyline, lidocaine gel, topical capsaicin, lamotrigine, and mexiletine, have shown no efficacy for HIV-associated or ART-associated DSPN in clinical trials.46 However, many of these trials were complicated by high dropout rates, poor recruitment, and higher than expected placebo responses. Most experts offer trials of these agents to patients with significant neuropathic pain. In the author’s experience, amitriptyline, pregabalin, and topical capsaicin have been the most efficacious. Alternatively, nonpharmacologic strategies such as acupuncture,52 self-hypnosis,53 resistance exercises,54 and splinting55 have shown some promise in small clinical trials. Scrambler therapy, a noninvasive US Food and Drug Administration (FDA)–approved peripheral neuromodulator with demonstrated efficacy in treating chemotherapy-associated neuropathy, has also been anecdotally reported to have benefit.56
Other Direct Neurologic Complications of Human Immunodeficiency Virus
This section discusses less common direct neurologic complications of HIV infection.
ASEPTIC MENINGITIS.
During acute HIV infection, individuals can develop a nonspecific headache and neck stiffness with or without fever that is often accompanied by systemic symptoms of acute HIV infection, such as arthralgia, myalgia, fatigue, and lymphadenopathy. Lumbar puncture (LP) usually reveals a lymphocytic pleocytosis and elevated protein but negative bacterial culture and viral polymerase chain reactions (PCRs). This syndrome occurs before seroconversion, so rapid HIV tests (eg, HIV antibody tests) are often negative while the plasma HIV viral load is elevated. As such, in patients presenting with aseptic meningitis and risk factors for HIV infection, a plasma HIV viral load should be sent to exclude acute HIV infection as a cause of the aseptic meningitis. Of note, CSF HIV RNA is available on a research basis but is not useful clinically in this situation. Treatment is supportive, and the patient should be referred to an HIV care and treatment program for ART initiation.
VACUOLAR MYELOPATHY.
Vacuolar myelopathy usually presents after the onset of AIDS (defined by a CD4+ T-cell count <200 cells/mm3 or the development of an opportunistic infection)57 with slowly progressive lower extremity weakness, stiffness, and sensory loss. Gait difficulties and imbalance are prominent, and bowel, bladder, and erectile dysfunction are common. Upper extremity symptoms are a late finding. Examination reveals spastic paraparesis and vibratory and proprioceptive deficits more than pain and temperature abnormalities. A sensory level is usually absent, but hyperreflexia, extensor plantar responses, ataxia, and an abnormal Romberg sign are common. LP should be performed to evaluate for alternative infectious and inflammatory etiologies of myelopathy as this is a diagnosis of exclusion. CSF studies usually reveal a lymphocytic pleocytosis, elevated protein, and negative infectious studies. MRI may demonstrate cord atrophy or increased T2 signal without gadolinium enhancement that preferentially involves the posterior columns. The thoracic cord is the most common area of involvement. Treatment is supportive, with physical therapy, symptomatic medications, and either initiation or optimization of the ART regimen to improve the patient’s immune status. Unfortunately, the deficits are usually irreversible, but improvement in immune status can halt progression of the disorder.
BELL’S PALSY.
Acute HIV infection can cause either unilateral or bilateral Bell’s palsy. In patients with risk factors for HIV infection who present with Bell’s palsy, both an HIV antibody test and plasma HIV viral load should be considered as this condition often presents before seroconversion (ie, HIV antibody test remains negative).
ACUTE INFLAMMATORY DEMYELINATING POLYRADICULONEUROPATHY.
Patients with either acute or advanced HIV infection may present with an acute inflammatory demyelinating polyradiculoneuropathy (AIDP) syndrome that is similar to AIDP in individuals who are not HIV infected. CSF studies may reveal the classic finding of albuminocytologic dissociation or may show a mild to moderate lymphocytic pleocytosis with elevated protein. Both HIV antibody and viral load testing should be considered as this presentation may occur before seroconversion to a positive HIV antibody test. Treatment is identical to AIDP treatment in individuals who are not HIV infected. However, given the similarity in clinic presentation to cytomegalovirus (CMV) polyradiculitis, empiric treatment with ganciclovir or foscarnet should be considered in patients with advanced immunosuppression (CD4+ T-cell count <200 cells/mm3) until CMV PCR results are confirmed to be negative.
CHRONIC INFLAMMATORY DEMYELINATING POLYRADICULONEUROPATHY.
Chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) can occur anytime in the course of HIV infection. Its clinical presentation is nearly identical to that of CIDP in individuals who are not HIV infected, and diagnostic testing is also similar, with albuminocytologic dissociation in the CSF and findings consistent with a demyelinating neuropathy on nerve conduction studies. However, patients who are HIV positive with CIDP are more likely to be younger and female, have a monophasic course, and respond to steroids than individuals who are not HIV infected with CIDP.58
MOTOR NEURON DISEASE.
An amyotrophic lateral sclerosis–like syndrome has been reported in individuals who are HIV infected that often improves or resolves completely with initiation of ART. This syndrome occurs at younger ages compared to individuals with amyotrophic lateral sclerosis who are not HIV infected and may be related to the expression of the endogenous retrovirus HERV-K.59
HUMAN IMMUNODEFICIENCY VIRUS–ASSOCIATED MYOPATHY.
HIV-associated myopathy occurs anytime during the course of HIV infection and usually presents with slowly progressive proximal limb weakness with or without myalgia. Etiologies are varied and include direct toxicity of HIV infection, an aberrant immune response resulting in an inflammatory myopathy mimicking polymyositis or inclusion body myositis,60 ART toxicity (especially with zidovudine), vasculitis, and infection. Creatine kinase levels may be mildly to markedly elevated. Serologic testing for other infectious etiologies and a muscle biopsy are indicated. Treatment includes discontinuation of zidovudine and initiation of an alternative ART regimen (if applicable) or immunomodulatory medications (steroids, IV immunoglobulin [IVIg], plasma exchange) in inflammatory subtypes.60
OTHER PERIPHERAL NERVOUS SYSTEM MANIFESTATIONS.
Both vasculitic neuropathy and brachial plexopathy occur with increased incidence in individuals who are HIV positive and can occur at any stage in HIV infection. Clinical presentation, diagnosis, and treatment are identical to those in patients who are not HIV infected. Of note, brachial plexopathy has rarely been reported as a hypersensitivity reaction to the antiretroviral drug abacavir.61
OPPORTUNISTIC INFECTIONS
A variety of CNS opportunistic infections occur when the CD4+ T-cell count drops below 200 cells/mm3, and multiple concurrent opportunistic infections can occur. Therefore, it is imperative to complete a thorough infectious workup in people with advanced HIV infection who present with symptoms localizable to the CNS. The most common opportunistic infections are reviewed in detail in this section.
Cryptococcal Meningitis
Cryptococcal meningitis is the most common cause of meningitis in individuals who are HIV infected and one of the most common opportunistic infections in people with AIDS. It is most commonly caused by the ubiquitous encapsulated yeast Cryptococcus neoformans. Exposure occurs through inhalation of the fungus from soil or avian droppings, and the infection spreads hematogenously to the CNS, where it causes meningitis.
EPIDEMIOLOGY.
The incidence of cryptococcal meningitis has significantly decreased with wider use of ART. In the United States, incidence has declined tenfold over the past 2 decades.62 Still, cryptococcal meningitis remains a significant worldwide problem. In 2014, approximately 225,000 incident cases of cryptococcal meningitis and 181,000 deaths among people who were HIV infected were seen globally, three-fourths of which occurred in sub-Saharan Africa. Overall, cryptococcal meningitis is responsible for up to one-fifth of global AIDS-related mortality63 and accounts for an average of 4000 inpatient hospitalizations among people who are HIV infected in the United States each year.64 While the incidence has declined, little progress has been made in improving cryptococcal meningitis outcomes, with mortality rates of 10% to 50% in the United States and substantially higher rates in sub-Saharan Africa.62,64,65 Furthermore, a 2017 study in Uganda found that between 2013 and 2016, almost 40% of participants with cryptococcal meningitis were on ART for at least 1 month before presentation,66 suggesting widespread ART availability alone is insufficient to prevent cryptococcal meningitis. Rather, optimal virologic suppression and proper diagnosis and treatment of opportunistic infections are needed to improve outcomes.
CLINICAL PRESENTATION AND RISK FACTORS.
Cryptococcal meningitis usually occurs in individuals who are HIV infected and have CD4+ T-cell counts less than 100 cells/mm3. It often initially presents as a slowly progressive nonspecific headache with or without fever. At this stage, meningismus and other neurologic signs are usually lacking. Clinical symptoms evolve over several weeks, eventually including nausea, vomiting, photophobia, visual obscurations, diplopia, meningismus, and encephalopathy. These symptoms are often indicative of increased intracranial pressure (ICP), and neurologic examination will show corresponding signs such as papilledema and cranial neuropathies, especially sixth nerve palsy. Occasionally fulminant presentations more typical of acute meningitis occur. Late-stage complications of cryptococcal meningitis include seizures, strokes, persistent hydrocephalus, and herniation.
DIAGNOSIS.
Given that early features of cryptococcal meningitis can be subtle, any person with advanced HIV infection presenting with a new headache or headache that is atypical of their usual headaches should be evaluated for cryptococcal meningitis. Serum cryptococcal antigen is a sensitive but nonspecific test for cryptococcal meningitis, but serum cryptococcal antigen titer can help determine cryptococcal meningitis risk. Nearly 100% of people with titers greater than 1:640 have cryptococcal meningitis, and a titer greater than 1:160 is highly sensitive (88%) and specific (82%) for cryptococcal meningitis.67,68 Whenever possible, diagnosis should be confirmed via CSF fungal culture or CSF cryptococcal antigen. India ink testing is still performed in some resource-limited settings but is less sensitive than cryptococcal antigen. Other CSF parameters may be normal or may reveal a mild to moderate lymphocytic pleocytosis and elevated protein. A markedly abnormal CSF should prompt consideration of alternative diagnoses. Given the high rates of increased ICP, brain imaging should be obtained before LP. Imaging can also identify cryptococcomas, which can cause focal neurologic symptoms and may require additional treatment.
MANAGEMENT.
Treatment of cryptococcal meningitis includes antifungal agents and management of increased ICP. Recommended antimicrobial therapy consists of induction with IV amphotericin B (0.7 mg/kg/d to 1.0 mg/kg/d) and oral flucytosine (25 mg/kg every 6 hours) for 2 weeks or until the CSF is sterile, whichever is later. However, the 2018 Advancing Cryptococcal Meningitis Treatment for Africa study may result in a change to these guidelines. In this study, more than 700 patients with HIV infection were randomly assigned to receive either 1 or 2 weeks of amphotericin B therapy in combination with either flucytosine or fluconazole or 2 weeks of combination fluconazole (1200 mg/d) and flucytosine (25 mg/kg every 6 hours). Results showed that treatment with both 1 week of amphotericin B and flucytosine and 2 weeks of oral medications were as effective as the standard 2-week induction therapy with amphotericin B and flucytosine and associated with less serious adverse events.69
Following this, high-dose oral fluconazole (400 mg/d) is added to complete an 8- to 10-week course. Consolidation therapy is then begun with low-dose oral fluconazole (200 mg/d) until adequate immune reconstitution has occurred (CD4+ T-cell count >100 cells/mm3 and undetectable or very low HIV RNA for 3 or more months). In regions where amphotericin or flucytosine are unavailable, alternative regimens incorporating immediate treatment with higher-dose fluconazole (1200 mg/d or more) have proven effective. Management of increased ICP includes daily LPs with the goal of reducing opening pressure by 50% if extremely elevated or to normal (<20 cm H2O) until opening pressure has been normal and symptoms of increased ICP have been stable for at least 2 consecutive days. A lumbar drain or ventriculostomy may be needed in people with persistently increased ICP despite daily LPs; a permanent ventricular shunt may be needed in the rare patient who develops chronic hydrocephalus. Of note, depressed consciousness, elevated ICP, and higher CSF cryptococcal antigen titer all portend worse prognosis.70 Recurrent cryptococcal meningitis can occur if azole resistance develops or if eradication of CNS infection is incomplete.
Progressive Multifocal Leukoencephalopathy
PML is caused by the JC virus, a nearly ubiquitous polyomavirus that infects up to 80% of adults worldwide, and is a late complication of HIV infection. It usually occurs when CD4+ T-cell counts drop below 100 cells/mm3. JC virus remains latent until advanced immunosuppression allows a productive infection of oligodendrocytes to occur, leading to demyelination and focal neurologic deficits. Wider use of ART has resulted in declining PML incidence and some improvement in long-term prognosis.
CLINICAL PRESENTATION.
Patients typically present with slowly progressive focal neurologic deficits. PML is a multifocal process, so multiple symptoms are common and can include hemiparesis, aphasia, ataxia, visual deficits, and cognitive impairment (CASE 7-2). Visual symptoms are due to involvement of the visual pathways rather than optic neuritis and are the most common symptom, occurring in up to half of people. Seizures are not uncommon and become more common as the disease progresses. Rare reports exist of spinal cord involvement, but cranial nerves and the peripheral nervous system are typically spared. Alternative presentations of CNS JC virus infection include cerebellar granule cell neuronopathy, which presents with a slowly progressive cerebellar syndrome, diffuse encephalitis, and meningitis. Of note, two cases of PML recurrence in individuals with HIV infection who were on ART with long-standing virologic suppression and normal CD4+ T-cell counts (>500 cells/mm3) were recently reported.71 This suggests PML recurrence should be considered in people who are HIV infected and have a remote history of PML who present with new neurologic symptoms despite optimal virologic suppression.
CASE 7-2.
A 36-year-old ART-naïve woman with human immunodeficiency virus (HIV) infection presented to the emergency department with gait difficulty, clumsiness, and vertigo. She began to feel unsteady while walking 6 weeks earlier, and the unsteadiness had progressed to the point that she was nearly bedbound. One month before presentation, she began having difficulty using her left hand to eat and perform fine motor tasks. Two weeks later, she developed intermittent vertigo, which was constant at presentation. Examination was notable for direction-changing nystagmus; hypometric saccades to the left; and left-sided ataxia, dysmetria, and dysdiadochokinesia. She was unable to tandem walk and fell to the left with Romberg maneuver.
Plasma CD4+ T-cell count was 20 cells/mm3 (normal 500 cells/mm3 to 1500 cells/mm3), and plasma HIV RNA was 962,357 copies/mL. Brain MRI revealed a lesion in the left cerebellum extending into the middle cerebellar peduncle (FIGURE 7-3). CSF studies showed a normal white blood cell count, protein, and glucose, but CSF JC virus polymerase chain reaction (PCR) was positive.
COMMENT
This patient’s clinical presentation was consistent with progressive multifocal leukoencephalopathy (PML). While supratentorial lesions are more common than infratentorial, her MRI otherwise demonstrated the classic appearance of PML lesions: T2 hyperintense, T1 hypointense, nonenhancing, and demonstrating a hyperintense rim on diffusion-weighted imaging (DWI). If her CSF JC virus PCR had been negative, a brain biopsy would have been indicated to establish a diagnosis. The patient was initiated on antiretroviral therapy (ART) to facilitate immune reconstitution and started on mirtazapine as off-label empiric treatment for PML based on in vitro and anecdotal evidence. Her symptoms did not progress further, but 6 months later her neurologic symptoms and deficits were largely unchanged.
DIAGNOSIS.
A definitive diagnosis of PML requires clinical, radiographic, and virologic evidence.72 However, diagnosis can be difficult as the disease is not always progressive, symptoms are not always multifocal at presentation, and lesions are not always restricted to white matter. Furthermore, the imaging appearance is often not classic, and CSF diagnostics are not always sensitive. As a result, significant diagnostic delays of several months are common, which can lead to delays in treatment initiation and worsened outcomes.73 Therefore, a high degree of clinical suspicion is needed in people with advanced HIV infection presenting with focal neurologic deficits, and a brain biopsy may be necessary to confirm a diagnosis.
The classic MRI appearance of PML is multifocal lesions in the subcortical and periventricular white matter that often involve subcortical U fibers. Supratentorial lesions are most common, but the basal ganglia, brainstem, and cerebellum can be involved. Lesions are hyperintense on T2-weighted images and hypointense on T1-weighted images and do not exhibit mass effect. While most lesions do not enhance with gadolinium, approximately 5% to 10% of cases have associated enhancement.74 PML lesions are usually hypometabolic on positron emission tomography (PET). On diffusion-weighted imaging (DWI), lesions usually demonstrate a hyperintense rim and hypointense core, a finding that may be better visualized using b3000 DWI sequences.75 Recent evidence suggests that low signal on susceptibility-weighted imaging (SWI) in the U fibers of juxtacortical PML lesions may be a sensitive but nonspecific finding.76,77
Laboratory diagnosis can be made by a positive CSF JC virus PCR, while CSF protein and cell count are often normal or mildly elevated. While generally quite specific, the JC virus PCR assay demonstrates significant variations in sensitivity between laboratories and is often negative in the setting of histopathologically confirmed PML. Therefore, CSF testing can be used as a first step in making a diagnosis of PML, as people with a positive JC virus PCR do not need to undergo a brain biopsy. However, in the setting of clinical suspicion and a negative CSF JC virus PCR, brain biopsy should be pursued. Typical histopathologic findings include widespread demyelination, large bizarre astrocytes, enlarged oligodendrocytes with nuclear inclusions, and positive immunostaining with SV40 polyomavirus antibodies (FIGURE 7-4).
FIGURE 7-4.
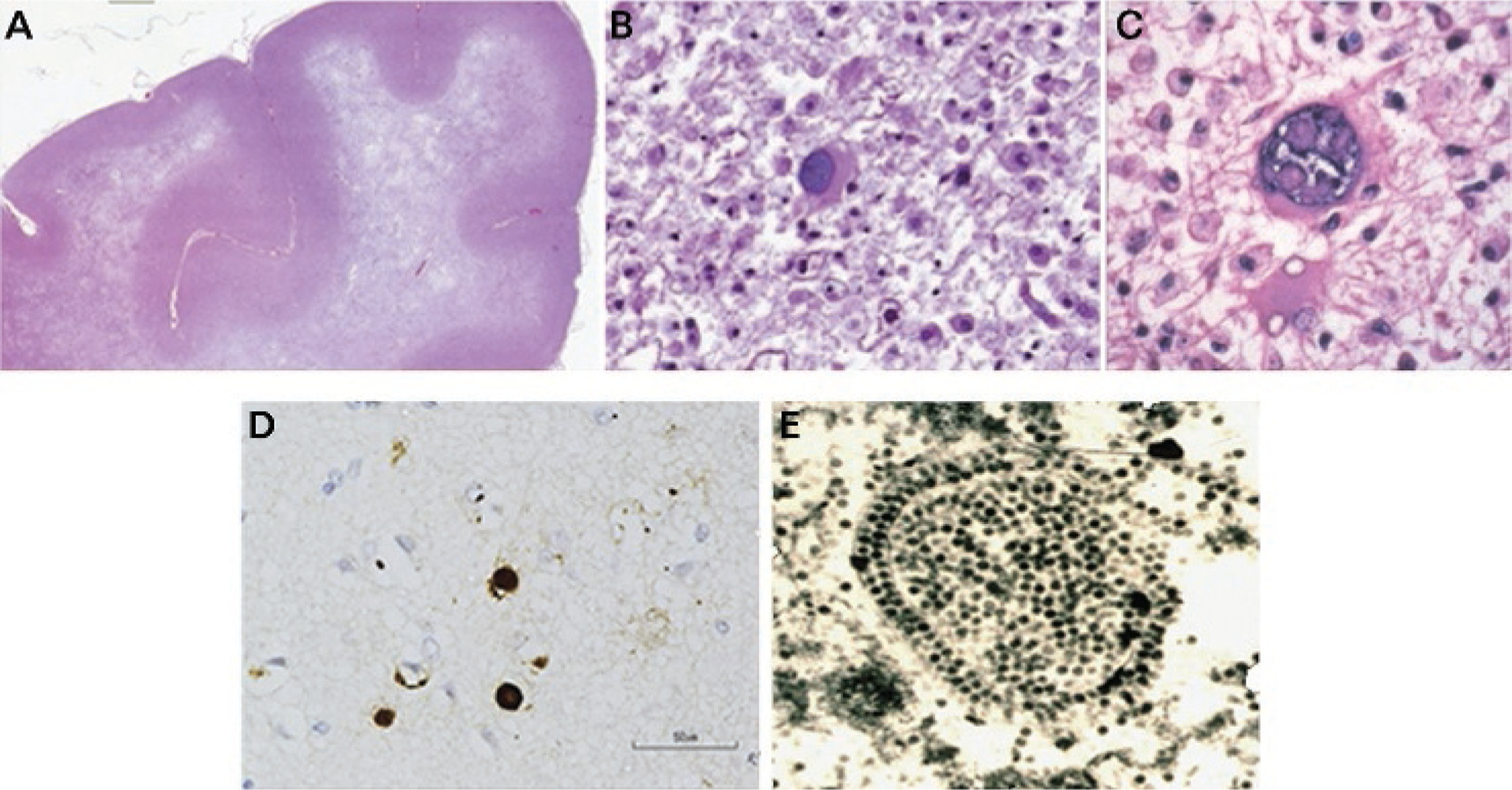
Pathology of progressive multifocal leukoencephalopathy. A, Luxol fast blue staining with hematoxylin counterstain of the frontal lobe in a patient with progressive multifocal leukoencephalopathy (PML) shows extensive multifocal and confluent areas of demyelination. Small islands of demyelination coalesce to produce large confluent areas resulting in a “ground glass” bright appearance on T2-weighted MRI scans. B, Enlarged oligodendrocyte with a large inclusion-bearing nucleus is characteristic of PML. No discrete intranuclear inclusion is seen. C, A large bizarre astrocyte is depicted. D, Immunostaining with polyclonal antibody to JC virus shows dark brown staining of nuclei of several oligodendrocytes. E, Electron micrograph of crystalline array of assembled JC virions in nuclei of infected oligodendrocyte in PML brain lesion. Virions measure 40 nm in diameter.
Reprinted with permission from Berger JR, et al, Neurology.72 © 2013 American Academy of Neurology.
MANAGEMENT.
No JC virus–specific treatment exists, so the mainstay of treatment remains immune reconstitution with immediate ART initiation. With timely immune reconstitution, survival is common. However, reversal of neurologic deficits is uncommon, and JC virus–specific treatments are urgently needed. In vitro evidence has led to anecdotal reports of successful outcomes with off-label use of several medications, including mirtazapine and interleukin-7, but these agents have not been systematically studied in clinical trials.78,79 Topotecan showed a trend toward improved radiographic outcomes and increased survival in a phase 2 trial80,81; however, no phase 3 trial has been performed. These reports should be interpreted with caution as multiple agents with in vitro and anecdotal evidence supporting efficacy against PML have failed in clinical trials, including mefloquine, cidofovir, and cytosine arabinoside. Given the favorable side effect profile, ease of administration, and potential benefit of mirtazapine, it is this author’s practice to initiate mirtazapine treatment (30 mg/d) in addition to ART at the time of PML diagnosis unless a contraindication exists.
Other Opportunistic Infections and Processes
Other common opportunistic infections and processes include toxoplasmosis, primary CNS lymphoma, varicella-zoster virus vasculitis, and CMV infection.
TOXOPLASMOSIS.
Toxoplasmosis usually occurs with CD4+T-cell counts less than 200 cells/mm3 and often presents with headache, fever, focal neurologic deficits, and seizures. Because of its predilection for the basal ganglia, movement disorders are not uncommon. Imaging usually reveals multiple ring-enhancing lesions, often in the basal ganglia or gray-white junction, with mass effect. LP is often contraindicated because of the mass effect, and the CSF profile is nonspecific. Serum Toxoplasma IgG is usually positive but can be falsely negative, while the CSF PCR has a low sensitivity but is helpful if it is positive. Treatment is with pyrimethamine, sulfadiazine, and leucovorin for 6 weeks or until enhancement resolves. In general, empiric treatment is initiated in patients with AIDS found to have ring-enhancing lesions. Clinical and radiographic improvements are expected within 2 weeks of treatment initiation. If none are seen, brain biopsy should be considered to evaluate for primary CNS lymphoma.
PRIMARY CENTRAL NERVOUS SYSTEM LYMPHOMA.
The clinical and radiographic presentation of primary CNS lymphoma is similar to that of CNS toxoplasmosis. Clinically, fever and systemic manifestations are less common with primary CNS lymphoma. Radiographically, imaging usually reveals a single heterogeneously enhancing lesion, although lesions may be multiple and ring enhancing. CSF studies show a mildly elevated protein and mild lymphocytic pleocytosis. A positive Epstein-Barr virus PCR is highly suggestive but not diagnostic of primary CNS lymphoma, and cytology is helpful when abnormal but does not exclude the diagnosis if normal. Brain biopsy is sometimes needed for a definitive diagnosis, especially when lesions do not improve with empiric treatment for toxoplasmosis. Management involves immediate initiation of ART to optimize immune status and consideration of whole-brain radiation and chemotherapy. High-dose methotrexate in combination with ART has been associated with high rates of long-term survival and low relapse rates.82 Steroids are a useful adjunct to treat vasogenic edema but should be delayed, if possible, until after a definitive diagnosis is made as they can decrease diagnostic yields of CSF testing and brain biopsy.
VARICELLA-ZOSTER VIRUS VASCULITIS.
Varicella-zoster virus vasculitis usually occurs with CD4+ T-cell count less than 200 cells/mm3. It may present with encephalopathy, cranial nerve deficits, seizures, and strokes as well as a myelopathy, which usually occurs weeks to months after a typical zoster rash. CSF studies reveal a lymphocytic or monocytic pleocytosis, mildly elevated protein and normal to low glucose. A positive CSF varicella-zoster virus PCR or IgM antibody confirms the diagnosis. Brain or meningeal biopsy can be considered to confirm the diagnosis when less invasive testing is unrevealing. Treatment is at least 14 days of IV acyclovir 10 mg/kg every 8 hours.
CYTOMEGALOVIRUS INFECTION.
CMV infections typically occur with marked immunosuppression (CD4+ T-cell count <50 cells/mm3) and can present with ventriculoencephalitis, micronodular encephalitis, retinitis, or polyradiculitis, often in the presence of a concurrent CMV-related systemic infection. CSF studies show a neutrophilic or mononuclear pleocytosis, elevated protein, and low glucose. CSF CMV PCR is both sensitive and specific. Treatment is a combination of ganciclovir (5 mg/kg IV every 12 hours) and foscarnet (60 mg/kg IV every 8 hours) for at least 2 to 3 weeks, followed by valganciclovir (900 mg/d) until the CD4+ T-cell count is greater than 100 cells/mm3 for at least 3 to 6 months.
IMMUNE RECONSTITUTION INFLAMMATORY SYNDROME
IRIS manifests as clinical deterioration in the setting of immune recovery from an immunocompromised state. In people who are HIV infected, this usually occurs in the weeks after ART initiation as the patient’s CD4+ T-cell count is increasing. Lower CD4+ T-cell count (especially <50 cells/mm3) at the time of ART initiation and faster immune recovery, defined as a rapid decline in plasma HIV RNA, are risk factors for IRIS. IRIS can occur in individuals with a previously undiagnosed or untreated opportunistic infection in which the recovering immune system mounts a robust inflammatory response to the pathogen, often referred to as unmasking IRIS. Alternatively, the recovering immune system can mount a marked response to persistent antigens remaining after a previously treated opportunistic infection, resulting in recurrence or progression of symptoms, a scenario known as paradoxical IRIS. IRIS can affect any organ system, but systemic IRIS is much more common than CNS IRIS, which occurs in only about 1% of individuals initiating ART.83 In the CNS, IRIS is most commonly seen in response to cryptococcal meningitis and PML (CASE 7-3). However, it can occur in response to any infection and has been reported with toxoplasmosis, tuberculosis, primary CNS lymphoma, neurosyphilis, and cytomegalovirus infection, among others. Occasionally, CNS IRIS can present as a fulminant encephalitis with leukoencephalopathy on MRI but in which no infectious pathogen is identified.86 In these cases, HIV itself is thought to be the infectious trigger.
CASE 7-3.
A 55-year-old man with HIV infection with a past medical history of previously treated cryptococcal meningitis 3 years prior presented with a 1-month history of progressively worsening headache. He described the headache as a global, pressurelike pain that was worse when supine. His sister also reported that he seemed apathetic and withdrawn over the past month. He had reinitiated antiretroviral therapy (ART) 3 months before presentation after being nonadherent to ART for 5 years. His CD4+ T-cell count at the time of ART reinitiation was 14 cells/mm3, and his plasma HIV RNA was greater than 1,000,000 copies/mL.
Neurologic examination on presentation was notable for disorientation (oriented to person and place only), abulia, psychomotor slowing, and mild bilateral papilledema. His CD4+ T-cell count was 343 cells/mm3, and plasma HIV RNA was undetectable. Brain MRI showed multiple parenchymal and meningeal-based ring-enhancing lesions with surrounding vasogenic edema (FIGURE 7-5). Lumbar puncture demonstrated 43 white blood cells/mm3 (lymphocytes), protein of 14 mg/dL, and normal glucose. CSF bacterial and acid-fast bacilli cultures were negative, as were polymerase chain reaction (PCR) for Epstein-Barr virus, cytomegalovirus, and JC virus. Serum and CSF toxoplasma antibodies were negative. CSF cryptococcal antigen was negative.
COMMENT
This patient’s presentation was consistent with paradoxical immune reconstitution inflammatory syndrome (IRIS) associated with cryptococcal meningitis. In paradoxical cryptococcal meningitis IRIS, CSF cryptococcal antigen and fungal cultures are usually negative. However, CSF profiles are usually more inflammatory than would be expected in cases of cryptococcal meningitis alone.84 This patient’s MRI findings are also most consistent with cryptococcal meningitis IRIS, as people who develop cryptococcal meningitis IRIS after starting ART are more likely to show focal contrast-enhancing meningeal and parenchymal lesions than individuals with cryptococcal meningitis who are not on ART.85 The patient was continued on ART and started on cryptococcal meningitis induction therapy with amphotericin and flucytosine. He required daily lumbar punctures to reduce increased intracranial pressure, but his mental status continued to worsen. Repeat brain imaging revealed worsening vasogenic edema, so he was initiated on high-dose methylprednisolone (1 g/d IV for 5 days), with improvement in clinical and imaging findings. He was then transitioned to prednisone 60 mg/d and planned for a gradual taper over 6 weeks.
Importantly, prevention of IRIS may be possible in some cases. Initiation of ART at higher CD4+ T-cell counts may result in a dramatically reduced incidence of IRIS.87 Furthermore, in patients with coinfections, delaying initiation of ART until several weeks after treatment of the coinfection has begun can reduce rates of IRIS and improve survival, likely by reducing the total antigen burden in the brain before reconstituting the immune system. For cryptococcal meningitis, delaying ART initiation for 5 weeks resulted in 15% lower mortality compared to that of people in whom ART was initiated during the first 2 weeks of treatment for cryptococcal meningitis.88 Delaying ART initiation for up to 2 months is also indicated in individuals who are HIV infected and have tuberculous meningitis, as earlier initiation was associated with an increased rate of life-threatening adverse events, although no difference in overall survival.89
Management of IRIS varies with the underlying infection, the magnitude of clinical deterioration, and the degree of inflammation. ART should be continued to prevent the development of ART resistance and further progression of the underlying infection. When available, treatment of the underlying opportunistic infection should be instituted as soon as possible. In people with significant clinical deterioration and evidence of cerebral edema, high-dose corticosteroids are indicated. IV steroids (methylprednisolone 1 g/d or equivalent corticosteroid for 5 days) should be used in individuals with impending herniation, while oral regimens (prednisone 60 mg/d for 2 weeks) can be used in people in whom edema is causing neurologic impairment without risk of herniation. Most people will then require a gradual taper over the next 4 to 6 weeks.90 However, not all individuals with IRIS require corticosteroids. In particular, in PML IRIS, the immune response is necessary for controlling the underlying infection as no specific antiviral therapies for JC virus infection have been established. Therefore, in people with opportunistic infections and radiographic evidence of IRIS (ie, gadolinium enhancement or mild cerebral edema visualized on MRI) without significant clinical correlation, steroids are usually not indicated.
NEUROLOGIC COMPLICATIONS OF ANTIRETROVIRAL THERAPY
Neurotoxicity was more common with older ART agents that are now uncommon in the United States, but these drugs are still common in some areas of sub-Saharan Africa. In addition, these toxicities may not completely resolve with discontinuation of these agents, so a complete ART history is important, as many people who are HIV infected encountered in clinical practice today were exposed to one or more of these agents in the past. The most common neurologic toxicities of ART are reviewed in TABLE 7-2.
TABLE 7-2.
Neurotoxicities Associated With Antiretroviral Medications
| Syndrome | Antiretroviral Therapy Medication | Characteristics |
|---|---|---|
| Distal symmetric polyneuropathy | “D-drugs”: stavudine (d4T), didanosine (ddl), zalcitabine (ddC) | Subacute to slowly progressive distal sensory symptoms that begin within a few months of initiation of the offending agent |
| While uncommonly used today, many people in the United States who are HIV infected were exposed to these drugs in the past and may have residual neuropathy and neuropathic pain as a result | ||
| Likely due to mitochondrial toxicity in peripheral nerve axons | ||
| Neuropsychiatric symptoms | Efavirenz | Symptoms occur in >50% of people but usually resolve within 1 month of initiation |
| Common symptoms include vivid nightmares, headaches, depression, anxiety | ||
| Less common symptoms include dissociative symptoms and psychosis | ||
| Neuromuscular weakness | Nucleoside analogue reverse transcriptase inhibitors, especially stavudine (d4T) | Rapidly progressive weakness with or without sensory symptoms resembling acute inflammatory demyelinating polyradiculoneuropathy (AIDP) |
| Systemic symptoms, including nausea, vomiting, fatigue, and abdominal distention | ||
| Occurs in the setting of lactic acidosis | ||
| Treatment is supportive, with management of lactic acidosis and withdrawal of offending agent | ||
| Myopathy | Zidovudine | Proximal weakness primarily involving the lower extremities with or without myalgia |
| Elevated serum creatinine kinase | ||
| Muscle biopsy may show signs of mitochondrial dysfunction (ie, ragged red fibers) |
CURRENT TOPICS RELEVANT TO CLINICAL NEUROLOGISTS
With people living with HIV now surviving to older ages, new clinically pertinent issues are arriving in the setting of chronic HIV infection. Several of these issues are relevant to neurologists, including the construct of accelerated aging, HIV as an independent risk factor for cerebrovascular disease, and CSF viral escape.
Accelerated Aging
Conditions often associated with older age, including coronary artery disease, stroke, type 2 diabetes mellitus, and dementia, are occurring at earlier ages in people with chronic HIV infection. This may be due to the effects of chronic systemic inflammation that occurs despite optimal virologic suppression, long-term ART toxicity, lifestyle factors, or a combination of these factors.91 Neurologists should be aware of this phenomenon as neurologic diseases of older age may occur a decade or more earlier in people with long-standing HIV infection.
Cerebrovascular Disease
HIV infection is an independent risk factor for stroke,92 and stroke is now one of the most common reasons for referral to the author’s neuro-HIV clinic. In addition to the effects of accelerated aging, HIV-associated endothelial dysfunction, vasculopathy, and hyperviscosity may contribute to this increased risk.93 Cerebrovascular risk factors should be aggressively managed in individuals who are HIV infected, and undiagnosed HIV infection should be considered in younger adults presenting with cryptogenic stroke.
Cerebrospinal Fluid Escape
There is increasing appreciation that 5% to 10% of individuals who are HIV infected have CSF escape, or undetectable plasma HIV RNA with detectable CSF HIV RNA. Escape may be sustained or nonsustained and can occur repeatedly.94 Virus detected in the CSF may be phylogenetically different from systemic strains of the virus (ie, CNS compartmentalization) or may have developed unique resistance mutations that confer resistance to an individual’s current ART. Ongoing viral replication in the CNS may lead to higher rates of HAND. Moreover, CSF escape poses a challenge to emerging strategies for an HIV cure as the CNS could serve as a reservoir for latent virus that could later reseed a productive systemic infection.9
CONCLUSION
With the widespread availability of effective ART in the United States and, increasingly, throughout the world, HIV infection has evolved from a life-limiting disease to a chronic condition that requires lifelong management but does not substantially alter life expectancy. However, neurologic complications of chronic HIV infection, including HAND and DSPN, persist at nearly identical rates to the pre-ART era, although with milder severity. In addition, conditions associated with marked immunosuppression still occur in people who are unaware of their HIV status or have difficulty with ART adherence. Furthermore, we are only beginning to understand the long-term health consequences of chronic HIV infection, leading to higher rates of several neurologic disorders, including stroke, dementia, and peripheral neuropathy, which are also occurring at younger ages in people who are HIV infected. Finally, several current areas of research, including strategies to prevent the chronic inflammation associated with HIV infection and strategies to cure HIV, may directly impact the incidence of neurologic complications of HIV. With a large population of individuals who are HIV infected in the United States and worldwide who are aging, neurologists should be aware of these conditions and comfortable with their diagnosis and management.
FIGURE 7-3.
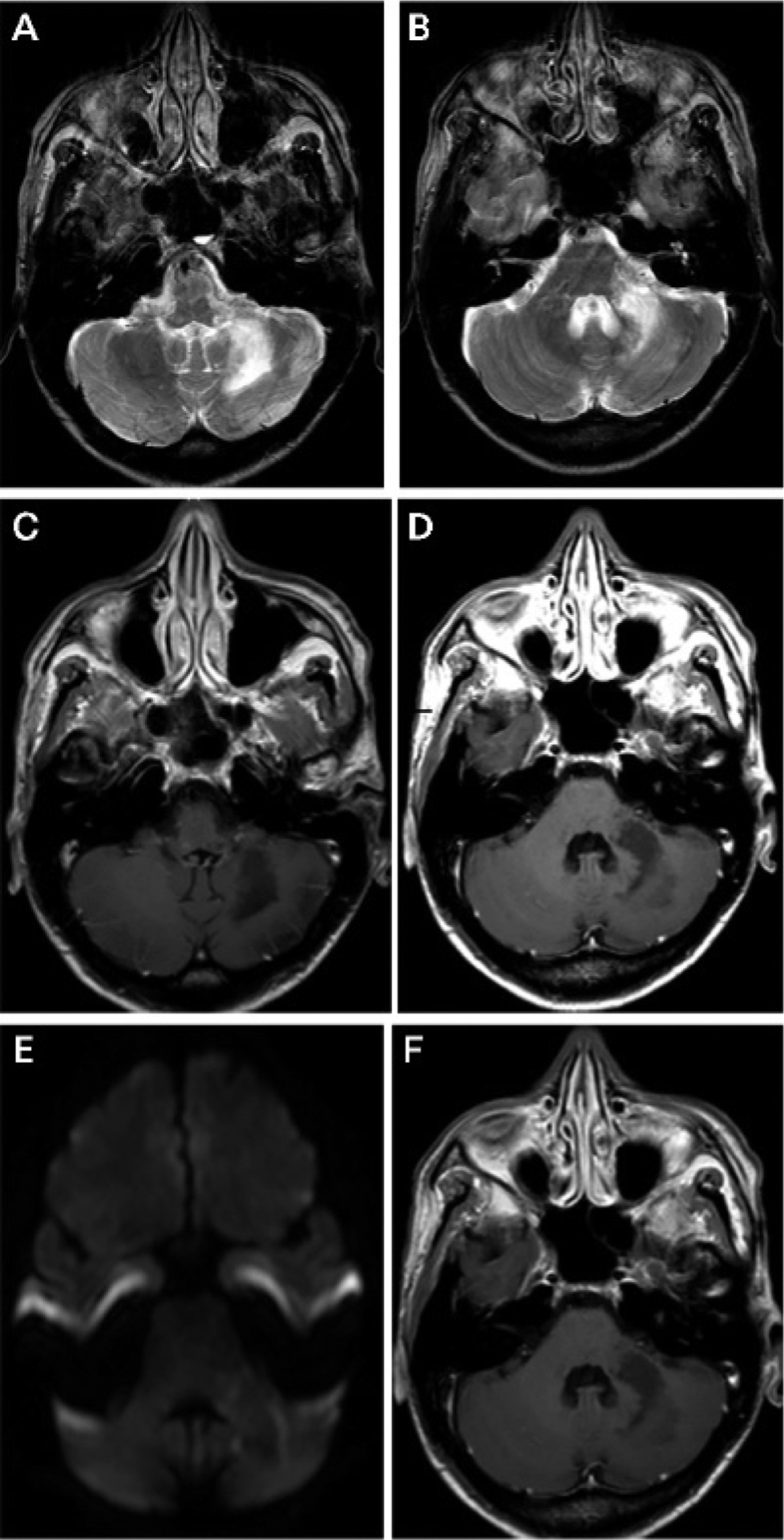
Imaging of the patient in CASE 7-2. Axial brain MRI revealing a left cerebellar and left middle cerebellar peduncle lesion that is hyperintense on T2-weighted imaging (A, B) and hypointense on T1-weighted imaging (C, D), has a rim that restricts diffusion on diffusion-weighted imaging (DWI) (E), and does not enhance with gadolinium administration (F).
FIGURE 7-5.
Imaging of the patient in CASE 7-3. Brain MRI showing multiple parenchymal and meningeal-based enhancing lesions (A, B) with associated vasogenic edema on fluid-attenuated inversion recovery (FLAIR) images (C, D).
KEY POINTS.
Neurologic complications of human immunodeficiency virus (HIV) infection affect every part of the neuraxis and stem primarily from four mechanisms: (1) direct effects of HIV, (2) opportunistic infections secondary to immunocompromise, (3) aberrant immune responses in the setting of antiretroviral therapy initiation, and (4) antiretroviral toxicity.
HIV-associated neurocognitive disorder represents a spectrum of conditions of varying severity, including asymptomatic neurocognitive impairment, mild neurocognitive disorder, and HIV-associated dementia.
HIV-associated neurocognitive disorder affects up to 50% of patients who are HIV infected today. This is largely unchanged from the pre–antiretroviral therapy era, but milder stages predominate in the antiretroviral therapy era.
HIV-associated neurocognitive disorder is a subcortical cognitive disorder that can occur at any point in the course of HIV infection, but lower nadir CD4+ T-cell count is a risk factor for its development.
Diagnosis and classification of HIV-associated neurocognitive disorder is based on the magnitude of deficits on neuropsychological testing and functional status assessments.
Before diagnosing a patient with HIV-associated neurocognitive disorder, a careful workup, including laboratory and radiologic investigations, should be undertaken as the diagnosis should only be considered when alternative causes of cognitive impairment have been excluded.
All individuals with HIV-associated neurocognitive disorder should be on antiretroviral therapy, and modifiable risk factors for cognitive impairment should be identified and treated to minimize their deleterious effects on cognitive function.
Currently, no specific treatments for HIV-associated neurocognitive disorder have been identified, but studies of paroxetine, intranasal insulin, and maraviroc are ongoing.
Distal symmetric polyneuropathy remains one of the most common neurologic complications of HIV encountered today.
HIV-associated distal symmetric polyneuropathy presents with slowly progressive numbness, tingling, and paresthesia in a stocking-glove distribution.
A clinical diagnosis of HIV-associated distal symmetric polyneuropathy is sufficient, with additional testing used only for atypical presentations, but a standard workup for additional causes of distal symmetric polyneuropathy should also be completed.
The primary goals of treatment for HIV-associated distal symmetric polyneuropathy are to prevent progression with optimal virologic suppression and to alleviate pain using standard neuropathic pain agents, nonpharmacologic strategies such as acupuncture, or both.
Central nervous system opportunistic infections tend to occur at particular levels of immunosuppression but may have overlapping presentations and may occur concurrently.
Cryptococcal meningitis is the most common cause of meningitis in people who are HIV infected and accounts for approximately one-fifth of acquired immunodeficiency syndrome–related mortality worldwide.
Cryptococcal meningitis usually occurs at CD4+ T-cell counts of less than 100 cells/mm3 and initially presents as a slowly progressive nonspecific headache with or without fever.
A serum cryptococcal antigen titer greater than 1:160 is highly sensitive and specific for a diagnosis of cryptococcal meningitis.
Treatment of cryptococcal meningitis includes antifungal agents to sterilize the CSF and management of increased intracranial pressure.
Progressive multifocal leukoencephalopathy usually occurs at CD4+ T-cell counts of less than 100 cells/mm3 and presents with slowly to subacutely progressive focal neurologic deficits.
A definitive diagnosis of progressive multifocal leukoencephalopathy requires clinical, radiographic, and virologic evidence.
In the setting of clinical suspicion and a negative CSF JC virus polymerase chain reaction, brain biopsy should be pursued to confirm a diagnosis of progressive multifocal leukoencephalopathy.
No JC virus–specific treatment exists, so the mainstay of treatment for progressive multifocal leukoencephalopathy remains immune reconstitution with immediate antiretroviral therapy initiation.
Immune reconstitution inflammatory syndrome manifests as clinical deterioration in the setting of immune recovery after an immunocompromised state.
In the central nervous system, immune reconstitution inflammatory syndrome is most commonly seen in response to cryptococcal meningitis and progressive multifocal leukoencephalopathy.
Management of immune reconstitution inflammatory syndrome includes continuation of antiretroviral therapy, initiation of specific antimicrobials for the underlying infection (if available) and use of corticosteroids in people with significant clinical deterioration due to cerebral edema.
A complete antiretroviral therapy history is important as many people who are HIV infected encountered in clinical practice today were exposed to neurotoxic antiretroviral therapy agents in the past.
Conditions often associated with older age, including stroke and dementia, are occurring at earlier ages in people with chronic HIV infection.
HIV is an independent risk factor for stroke.
CSF escape (undetectable plasma HIV RNA with detectable CSF HIV RNA) may develop in 5% to 10% of individuals who are HIV infected and may lead to higher rates of HIV-associated neurocognitive disorder and limit emerging HIV cure strategies.
With a large population of people who are HIV infected in the United States and globally who are aging, neurologists should be aware of the neurologic complications of HIV and comfortable with their diagnosis and management.
ACKNOWLEDGMENT
This work was supported by grants from the National Institutes of Health (P30MH07565673-11A1, R01 MH099733, NS081196091, P30AI094189-01A1, L30 NS088658, R25 NS065729-05S2, R25 MH080661-08).
RELATIONSHIP DISCLOSURE:
Dr Saylor receives research/grant support from the National Institutes of Health (P30MH07565673-11A1, R01 MH099733, NS081196091, P30AI094189-01A1, L30 NS088658, R25 NS065729-05S2, R25 MH080661-08), Sara’s Wish Foundation, and the United States Department of State (Fulbright Scholar Award).
Footnotes
UNLABELED USE OF PRODUCTS/INVESTIGATIONAL USE DISCLOSURE:
Dr Saylor discusses recent or ongoing clinical trials of intranasal insulin, maraviroc, and paroxetine for treatment of human immunodeficiency virus–associated neurocognitive disorder and the off-label use of interleukin-7, mirtazapine, and topotecan for the treatment of progressive multifocal leukoencephalopathy.
REFERENCES
- 1.Centers for Disease Control. HIV/AIDS statistics overview. cdc.gov/hiv/statistics/overview/index.html. Updated May 7, 2018. Accessed July 30, 2018.
- 2.UNAIDS. Global HIV statistics fact sheet. unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf. Published July 2017. Accessed July 30, 2018.
- 3.Becker JT, Kingsley LA, Molsberry S, et al. Cohort profile: recruitment cohorts in the neuropsychological substudy of the Multicenter AIDS Cohort Study. Int J Epidemiol 2015;44(5): 1506–1516. doi: 10.1093/ije/dyu092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Heaton RK, Clifford DB, Franklin DR Jr, et al. HIV-associated neurocognitive disorders persist in the era of potent antiretroviral therapy: CHARTER Study. Neurology 2010;75(23): 2087–2096. doi: 10.1212/WNL.0b013e318200d727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Heaton RK, Franklin DR Jr, Deutsch R, et al. Neurocognitive change in the era of HIV combination antiretroviral therapy: the longitudinal CHARTER study. Clin Infect Dis 2015; 60(3):473–480. doi: 10.1093/cid/ciu862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Heaton RK, Franklin DR, Ellis RJ, et al. HIV-associated neurocognitive disorders before and during the era of combination antiretroviral therapy: differences in rates, nature, and predictors. J Neurovirol 2011;17(1):3–16. doi: 10.1007/s13365-010-0006-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sacktor N, Nakasujja N, Skolasky R, et al. Antiretroviral therapy improves cognitive impairment in HIV+ individuals in sub-Saharan Africa. Neurology 2006;67(2):311–314. doi: 10.1212/01.wnl.0000225183.74521.72. [DOI] [PubMed] [Google Scholar]
- 8.Sacktor N, Skolasky RL, Seaberg E, et al. Prevalence of HIV-associated neurocognitive disorders in the Multicenter AIDS Cohort Study. Neurology 2016;86(4):334–340. doi: 10.1212/WNL.0000000000002277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Saylor D, Dickens AM, Sacktor N, et al. HIV-associated neurocognitive disorder—pathogenesis and prospects for treatment. Nat Rev Neurol 2016;12(5):309. doi: 10.1038/nrneurol.2016.53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kore I, Ananworanich J, Valcour V, et al. Neuropsychological impairment in acute HIV and the effect of immediate antiretroviral therapy. J Acquir Immune Defic Syndr 2015;70(4):393–399. doi: 10.1097/QAI.0000000000000746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Rahimy E, Li FY, Hagberg L, et al. Blood-brain barrier disruption is initiated during primary HIV infection and not rapidly altered by antiretroviral therapy. J Infect Dis 2017;215(7):1132–1140. doi: 10.1093/infdis/jix013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ragin AB, Wu Y, Gao Y, et al. Brain alterations within the first 100 days of HIV infection. Ann Clin Transl Neurol 2015;2(1):12–21. doi: 10.1002/acn3.136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Molsberry SA, Lecci F, Kingsley L, et al. Mixed membership trajectory models of cognitive impairment in the multicenter AIDS cohort study. AIDS 2015;29(6):713–721. doi: 10.1097/QAD.0000000000000561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ellis RJ, Badiee J, Vaida F, et al. CD4 nadir is a predictor of HIV neurocognitive impairment in the era of combination antiretroviral therapy. AIDS 2011;25(14):1747–1751. doi: 10.1097/QAD.0b013e32834a40cd. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.McCutchan JA, Marquie-Beck JA, Fitzsimons CA, et al. Role of obesity, metabolic variables, and diabetes in HIV-associated neurocognitive disorder. Neurology 2012;78(7):485–492. doi: 10.1212/WNL.0b013e3182478d64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Fabbiani M, Ciccarelli N, Tana M, et al. Cardiovascular risk factors and carotid intima-media thickness are associated with lower cognitive performance in HIV-infected patients. HIV Med 2013;14(3):136–144. doi: 10.1111/j.1468-1293.2012.01044.x. [DOI] [PubMed] [Google Scholar]
- 17.Fazeli PL, Crowe M, Ross LA, et al. Cognitive functioning in adults aging with HIV: a cross-sectional analysis of cognitive subtypes and influential factors. J Clin Res HIV AIDS Prev 2014;1(4):155–169. doi: 10.14302/issn.2324-7339.jcrhap-13-191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Joska JA, Westgarth-Taylor J, Hoare J, et al. Neuropsychological outcomes in adults commencing highly active anti-retroviral treatment in South Africa: a prospective study. BMC Infect Dis 2012;12:39. doi: 10.1186/1471-2334-12-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Heaton R, Franklin D, Letendre S, et al. Aging amplifies HIV neurocognitive impairment: the effects may be related to vascular and metabolic factors. J Neurovirol 2012;18:S46. [Google Scholar]
- 20.Weber E, Morgan EE, Iudicello JE, et al. Substance use is a risk factor for neurocognitive deficits and neuropsychiatric distress in acute and early HIV infection. J Neurovirol 2013;19(1):65–74. doi: 10.1007/s13365-012-0141-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Gongvatana A, Morgan EE, Iudicello JE, et al. A history of alcohol dependence augments HIV-associated neurocognitive deficits in persons aged 60 and older. J Neurovirol 2014; 20(5):505–513. doi: 10.1007/s13365-014-0277-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Monnig MA, Kahler CW, Lee H, et al. Effects of smoking and alcohol use on neurocognitive functioning in heavy drinking, HIV-positive men who have sex with men. AIDS Care 2016;28(3): 300–305. doi: 10.1080/09540121.2015.1093595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Meade CS, Towe SL, Skalski LM, Robertson KR. Independent effects of HIV infection and cocaine dependence on neurocognitive impairment in a community sample living in the southern United States. Drug Alcohol Depend 2015;149:128–135. doi: 10.1016/j.drugalcdep.2015.01.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Douglas-Newman KR, Smith RV, Spiers MV, et al. Effects of recent alcohol consumption level on neurocognitive performance in HIV+ individuals. Addict Disord Their Treat 2017;16(3):95–107. doi: 10.1097/ADT.0000000000000109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Thames AD, Kuhn TP, Williamson TJ, et al. Marijuana effects on changes in brain structure and cognitive function among HIV+ and HIV− adults. Drug Alcohol Depend 2017;170: 120–127. doi: 10.1016/j.drugalcdep.2016.11.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Vivithanaporn P, Nelles K, DeBlock L, et al. Hepatitis C virus co-infection increases neurocognitive impairment severity and risk of death in treated HIV/AIDS. J Neurol Sci 2012; 312(1–2):45–51. doi: 10.1016/j.jns.2011.08.025. [DOI] [PubMed] [Google Scholar]
- 27.Clifford DB, Vaida F, Kao YT, et al. Absence of neurocognitive effect of hepatitis C infection in HIV-coinfected people. Neurology 2015;84(3): 241–250. doi: 10.1212/WNL.0000000000001156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Antinori A, Arendt G, Becker JT, et al. Updated research nosology for HIV-associated neurocognitive disorders. Neurology 2007; 69(18):1789–1799. doi: 10.1212/01.WNL.0000287431.88658.8b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Power C, Selnes OA, Grim JA, McArthur JC. HIV Dementia Scale: a rapid screening test. J Acquir Immune Defic Syndr Hum Retrovirol 1995;8(3): 273–278. doi: 10.1097/00042560-199503010-00008. [DOI] [PubMed] [Google Scholar]
- 30.Sacktor NC, Wong M, Nakasujja N, et al. The International HIV Dementia Scale: a new rapid screening test for HIV dementia. AIDS 2005;19(13):1367–1374. doi: 10.1097/01.aids.0000180790.77379.3a. [DOI] [PubMed] [Google Scholar]
- 31.Cysique LA, Maruff P, Darby D, Brew BJ. The assessment of cognitive function in advanced HIV-1 infection and AIDS dementia complex using a new computerised cognitive test battery. Arch Clin Neuropsychol 2006;21(2):185–194. doi: 10.1016/j.acn.2005.07.011. [DOI] [PubMed] [Google Scholar]
- 32.Kamminga J, Lal L, Wright EJ, et al. Monitoring HIV-associated neurocognitive disorder using screenings: a critical review including guidelines for clinical and research use. Curr HIV/AIDS Rep 2017;14(3):83–92. doi: 10.1007/s11904-017-0349-9. [DOI] [PubMed] [Google Scholar]
- 33.Letendre S, Marquie-Beck J, Capparelli E, et al. Validation of the CNS Penetration-Effectiveness rank for quantifying antiretroviral penetration into the central nervous system. Arch Neurol 2008;65(1):65–70. doi: 10.1001/archneurol.2007.31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Ellis RJ, Letendre S, Vaida F, et al. Randomized trial of central nervous system-targeted antiretrovirals for HIV-associated neurocognitive disorder. Clin Infect Dis 2014;58(7):1015–1022. doi: 10.1093/cid/cit921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Libertone R, Lorenzini P, Balestra P, et al. Central nervous system penetration-effectiveness rank does not reliably predict neurocognitive impairment in HIV-infected individuals. J Int AIDS Soc 2014;17(4 suppl 3):19655. doi: 10.7448/IAS.17.4.19655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Stauch KL, Emanuel K, Lamberty BG, et al. Central nervous system-penetrating antiretrovirals impair energetic reserve in striatal nerve terminals. J Neurovirol 2017;23(6)795–807. doi: 10.1007/s13365-017-0573-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Wright EJ, Grund B, Cysique LA, et al. No difference between the effects of immediate versus deferred ART on neuropsychological test performance in HIV+ adults with CD4 counts above 500 cells/microliter: the Strategic Timing of Anti-Retroviral Treatment (START) Neurology Substudy. Poster presented at:15th European AIDS Conference; October 21–24, 2015; Barcelona, Spain. [Google Scholar]
- 38.Kamal S, Locatelli I, Wandeler G, et al. The presence of human immunodeficiency virus-associated neurocognitive disorders is associated with a lower adherence to combined antiretroviral treatment. Open Forum Infect Dis 2017;4(2):ofx070. doi: 10.1093/ofid/ofx070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Sacktor N, Skolasky RL, Moxley R, et al. Paroxetine and fluconazole therapy for HIV-associated neurocognitive impairment: results from a double-blind, placebo-controlled trial. J Neurovirol 2018;24(1):16–27. doi: 10.1007/s13365-017-0587-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Gerena Y, Menéndez-Delmestre R, Skolasky RL, et al. Soluble insulin receptor as a source of insulin resistance and cognitive impairment in HIV-seropositive women. J Neurovirol 2015;21(2): 113–119. doi: 10.1007/s13365-014-0310-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Suh HS, Lo Y, Choi N, et al. Insulin-like growth factors and related proteins in plasma and cerebrospinal fluids of HIV-positive individuals. J Neuroinflammation 2015;12:72. doi: 10.1186/s12974-015-0288-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Mamik MK, Asahchop EL, Chan WF, et al. Insulin treatment prevents neuroinflammation and neuronal injury with restored neurobehavioral function in models of HIV/AIDS neurodegeneration. J Neurosci 2016; 36(41):10683–10695. doi: 10.1523/JNEUROSCI.1287-16.2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kelly KM, Beck SE, Metcalf Pate KA, et al. Neuroprotective maraviroc monotherapy in simian immunodeficiency virus-infected macaques: reduced replicating and latent SIV in the brain. AIDS 2013;27(18):F21–F28. doi: 10.1097/QAD.0000000000000074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Ndhlovu LC, Umaki T, Chew GM, et al. Treatment intensification with maraviroc (CCR5 antagonist) leads to declines in CD16-expressing monocytes in cART-suppressed chronic HIV-infected subjects and is associated with improvements in neurocognitive test performance: implications for HIV-associated neurocognitive disease (HAND). J Neurovirol 2014;20(6):571–582. doi: 10.1007/s13365-014-0279-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Gates TM, Cysique LA, Siefried KJ, et al. Maraviroc-intensified combined antiretroviral therapy improves cognition in virally suppressed HIV-associated neurocognitive disorder. AIDS 2016;30(4):591–600. doi: 10.1097/QAD.0000000000000951. [DOI] [PubMed] [Google Scholar]
- 46.Aziz-Donnelly A, Harrison TB. Update of HIV-associated sensory neuropathies. Curr Treat Options Neurol 2017;19(10):36. doi: 10.1007/s11940-017-0472-3. [DOI] [PubMed] [Google Scholar]
- 47.Kaku M, Simpson DM. HIV, antiretrovirals and peripheral neuropathy: a moving target. Muscle Nerve 2018;57(3):347–349. doi: 10.1002/mus.25990. [DOI] [PubMed] [Google Scholar]
- 48.Wang SX, Ho EL, Grill M, et al. Peripheral neuropathy in primary HIV infection associates with systemic and central nervous system immune activation. J Acquir Immune Defic Syndr 2014;66(3):303–310. doi: 10.1097/QAI.0000000000000167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Gardner K, Hall PA, Chinnery PF, Payne BA. HIV treatment and associated mitochondrial pathology: review of 25 years of in vitro, animal, and human studies. Toxicol Pathol 2014;42(5): 811–822. doi: 10.1177/0192623313503519. [DOI] [PubMed] [Google Scholar]
- 50.Benevides ML, Filho SB, Debona R, et al. Prevalence of peripheral neuropathy and associated factors in HIV-infected patients. J Neurol Sci 2017;375:316–320. doi: 10.1016/j.jns.2017.02.011. [DOI] [PubMed] [Google Scholar]
- 51.Saylor D, Nakigozi G, Nakasujja N, et al. Peripheral neuropathy in HIV-infected and uninfected patients in Rakai, Uganda. Neurology 2017;89(5): 485–491. doi: 10.1212/WNL.0000000000004136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Dimitrova A, Murchison C, Oken B. Acupuncture for the treatment of peripheral neuropathy: a systematic review and meta-analysis. J Altern Complement Med 2017;23(3):164–179. doi: 10.1089/acm.2016.0155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Dorfman D, George MC, Schnur J, et al. Hypnosis for treatment of HIV neuropathic pain: a preliminary report. Pain Med 2013;14(7): 1048–1056. doi: 10.1111/pme.12074. [DOI] [PubMed] [Google Scholar]
- 54.Mkandla K, Myezwa H, Musenge E. The effects of progressive-resisted exercises on muscle strength and health-related quality of life in persons with HIV-related poly-neuropathy in Zimbabwe. AIDS Care 2016;28(5):639–643. doi: 10.1080/09540121.2015.1125418. [DOI] [PubMed] [Google Scholar]
- 55.Sandoval R, Roddey T, Giordano TP, et al. Randomized trial of lower extremity splinting to manage neuropathic pain and sleep disturbances in people living with HIV/AIDS. J Int Assoc Provid AIDS Care 2016;15(3):240–247. doi: 10.1177/2325957413511112. [DOI] [PubMed] [Google Scholar]
- 56.Smith TJ, Auwaerter P, Knowlton A, et al. Treatment of human immunodeficiency virus-related peripheral neuropathy with Scrambler Therapy: a case report. Int J STD AIDS 2017;28(2):202–204. doi: 10.1177/0956462416656688. [DOI] [PubMed] [Google Scholar]
- 57.HIV.gov. What are HIV and AIDS? hiv.gov/hiv-basics/overview/about-hiv-and-aids/what-are-hiv-and-aids. Updated May 15, 2017. Accessed July 30, 2018.
- 58.Moodley K, Bill PL, Patel VB. A comparative study of CIDP in a cohort of HIV-infected and HIV-uninfected patients. Neurol Neuroimmunol Neuroinflamm 2016;4(2):e315. doi: 10.1212/NXI.0000000000000315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Bowen LN, Tyagi R, Li W, et al. HIV-associated motor neuron disease: HERV-K activation and response to antiretroviral therapy. Neurology 2016;87(17):1756–1762. doi: 10.1212/WNL.0000000000003258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Lloyd TE, Pinal-Fernandez I, Michelle EH, et al. Overlapping features of polymyositis and inclusion body myositis in HIV-infected patients. Neurology 2017;88(15):1454–1460. doi: 10.1212/WNL.0000000000003821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Bellagamba R, Tommasi C, De Marco M, Narciso P. Parsonage-Turner syndrome: a rare case of abacavir hypersensitivity reaction in HIV-infected patients. J Infect 2008;57(1):88–90. doi: 10.1016/j.jinf.2008.05.001. [DOI] [PubMed] [Google Scholar]
- 62.Touma M, Rasmussen LD, Martin-Iguacel R, et al. Incidence, clinical presentation, and outcome of HIV-1-associated cryptococcal meningitis during the highly active antiretroviral therapy era: a nationwide cohort study. Clin Epidemiol 2017;9: 385–392. doi: 10.2147/CLEP.S135309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Rajasingham R, Smith RM, Park BJ, et al. Global burden of disease of HIV-associated cryptococcal meningitis: an updated analysis. Lancet Infect Dis 2017;17(8):873–881. doi: 10.1016/S1473-3099(17)30243-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Shaheen AA, Somayaji R, Myers R, Mody CH. Epidemiology and trends of cryptococcosis in the United States from 2000 to 2007: a population-based study. Int J STD AIDS 2017: 956462417732649. doi: 10.1177/0956462417732649. [DOI] [PubMed] [Google Scholar]
- 65.Pasquier E, Kunda J, De Beaudrap P, et al. Long-term mortality and disability in cryptococcal meningitis: a systematic literature review. Clin Infect Dis 2017. doi: 10.1093/cid/cix870. [DOI] [PubMed] [Google Scholar]
- 66.Flynn AG, Meya DB, Hullsiek KH, et al. Evolving failures in the delivery of human immunodeficiency virus care: lessons from a Ugandan meningitis cohort 2006–2016. Open Forum Infect Dis 2017;4(2):ofx077. doi: 10.1093/ofid/ofx077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Beyene T, Zewde AG, Balcha A, et al. Inadequacy of high-dose fluconazole monotherapy among cerebrospinal fluid cryptococcal antigen (CrAg)-positive human immunodeficiency virus-infected persons in an Ethiopian CrAg screening program. Clin Infect Dis 2017;65(12): 2126–2129. doi: 10.1093/cid/cix613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Wake RM, Britz E, Sriruttan C, et al. High cryptococcal antigen titers in blood are predictive of subclinical cryptococcal meningitis among human immunodeficiency virus–infected patients. Clin Infect Dis 2018;66(5):686–692. doi: 10.1093/cid/cix872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Molloy SF, Kanyama C, Heyderman RS, et al. Antifungal combinations for treatment of cryptococcal meningitis in Africa. N Engl J Med 2018;378(11):1004–1017. doi: 10.1056/NEJMoa1710922. [DOI] [PubMed] [Google Scholar]
- 70.Concha-Velasco F, González-Lagos E, Seas C, Bustamante B. Factors associated with early mycological clearance in HIV-associated cryptococcal meningitis. PLoS One 2017;12(3): e0174459. doi: 10.1371/journal.pone.0174459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Crossley KM, Agnihotri S, Chaganti J, et al. Recurrence of progressive multifocal leukoencephalopathy despite immune recovery in two HIV seropositive individuals. J Neurovirol 2016;22(4):541–545. doi: 10.1007/s13365-015-0419-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Berger JR, Aksamit AJ, Clifford DB, et al. PML diagnostic criteria: consensus statement from the AAN Neuroinfectious Disease Section. Neurology 2013;80(15):1430–1438. doi: 10.1212/WNL.0b013e31828c2fa1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Miskin DP, Ngo LH, Koralnik IJ. Diagnostic delay in progressive multifocal leukoencephalopathy. Ann Clin Transl Neurol 2016;3(5):386–391. doi: 10.1002/acn3.301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Shah R, Bag AK, Chapman PR, Curé JK. Imaging manifestations of progressive multifocal leukoencephalopathy. Clin Radiol 2010;65(6): 431–439. doi: 10.1016/j.crad.2010.03.001. [DOI] [PubMed] [Google Scholar]
- 75.Godi C, De Vita E, Tombetti E, et al. High b-value diffusion-weighted imaging in progressive multifocal leukoencephalopathy in HIV patients. Eur Radiol 2017;27(9):3593–3599. doi: 10.1007/s00330-017-4761-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Miyagawa M, Maeda M, Umino M, et al. Low signal intensity in U-fiber identified by susceptibility-weighted imaging in two cases of progressive multifocal leukoencephalopathy. J Neurol Sci 2014;344(1–2):198–202. doi: 10.1016/j.jns.2014.06.018. [DOI] [PubMed] [Google Scholar]
- 77.Umino M, Maeda M, Ii Y, et al. Low-signal-intensity rim on susceptibility-weighted imaging is not a specific finding to progressive multifocal leukoencephalopathy. J Neurol Sci 2016;362: 155–159. doi: 10.1016/j.jns.2016.01.036. [DOI] [PubMed] [Google Scholar]
- 78.Cettomai D, McArthur JC. Mirtazapine use in human immunodeficiency virus-infected patients with progressive multifocal leukoencephalopathy. Arch Neurol 2009;66(2): 255–258. doi: 10.1001/archneurol.2008.557. [DOI] [PubMed] [Google Scholar]
- 79.Miskin DP, Chalkias SG, Dang X, et al. Interleukin-7 treatment of PML in a patient with idiopathic lymphocytopenia. Neurol Neuroimmunol Neuroinflamm 2016;3(2):e213. doi: 10.1212/NXI.0000000000000213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Royal W 3rd, Dupont B, McGuire D, et al. Topotecan in the treatment of acquired immunodeficiency syndrome-related progressive multifocal leukoencephalopathy. J Neurovirol 2003;9(3):411–419. doi: 10.1080/13550280390201740. [DOI] [PubMed] [Google Scholar]
- 81.Nukuzuma S, Nakamichi K, Kameoka M, et al. Suppressive effect of topoisomerase inhibitors on JC polyomavirus propagation in human neuroblastoma cells. Microbiol Immunol 2016; 60(4):253–260. doi: 10.1111/1348-0421.12372. [DOI] [PubMed] [Google Scholar]
- 82.Moulignier A, Lamirel C, Picard H, et al. Long-term AIDS-related PCNSL outcomes with HD-MTX and combined antiretroviral therapy. Neurology 2017;89(8):796–804. doi: 10.1212/WNL.0000000000004265. [DOI] [PubMed] [Google Scholar]
- 83.McCombe JA, Auer RN, Maingat FG, et al. Neurologic immune reconstitution inflammatory syndrome in HIV/AIDS: outcome and epidemiology. Neurology 2009;72(9):835–841. doi: 10.1212/01.wnl.0000343854.80344.69. [DOI] [PubMed] [Google Scholar]
- 84.Boulware DR, Bonham SC, Meya DB, et al. Paucity of initial cerebrospinal fluid inflammation in cryptococcal meningitis is associated with subsequent immune reconstitution inflammatory syndrome. J Infect Dis 2010;202(6):962–970. doi: 10.1086/655785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Katchanov J, Branding G, Jefferys L, et al. Neuroimaging of HIV-associated cryptococcal meningitis: comparison of magnetic resonance imaging findings in patients with and without immune reconstitution. Int J STD AIDS 2016;27(2): 110–117. doi: 10.1177/0956462415574633. [DOI] [PubMed] [Google Scholar]
- 86.Johnson T, Nath A. Immune reconstitution inflammatory syndrome and the central nervous system. Curr Opin Neurol 2011;24(3):284–290. doi: 10.1097/WCO.0b013e328346be57. [DOI] [PubMed] [Google Scholar]
- 87.Müller M, Wandel S, Colebunders R, et al. Immune reconstitution inflammatory syndrome in patients starting antiretroviral therapy for HIV infection: a systematic review and meta-analysis. Lancet Infect Dis 2010;10(4):251–261. doi: 10.1016/S1473-3099(10)70026-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Boulware DR, Meya DB, Muzoora C, et al. Timing of antiretroviral therapy after diagnosis of cryptococcal meningitis. N Engl J Med 2014; 370(26):2487–2498. doi: 10.1056/NEJMoa1312884. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Török ME, Yen NT, Chau TT, et al. Timing of initiation of antiretroviral therapy in human immunodeficiency virus (HIV)—associated tuberculous meningitis. Clin Infect Dis 2011;52(11): 1374–1383. doi: 10.1093/cid/cir230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Nath A. Neurologic complications of human immunodeficiency virus infection. Continuum (Minneap Minn) 2015;21(6 Neuroinfectious Disease):1557–1576. doi: 10.1212/CON.0000000000000244. [DOI] [PubMed] [Google Scholar]
- 91.Raghavan A, Rimmelin DE, Fitch KV, Zanni MV. Sex differences in select non-communicable HIV-associated comorbidities: exploring the role of systemic immune activation/inflammation. Curr HIV/AIDS Rep 2017;14(6):220–228. doi: 10.1007/s11904-017-0366-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Gutierrez J, Albuquerque ALA, Falzon L. HIV infection as vascular risk: a systematic review of the literature and meta-analysis. PLoS One 2017; 12(5):e0176686. doi: 10.1371/journal.pone.0176686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Chow FC, Li Y, Hu Y, et al. Relationship between HIV infection, antiretroviral therapy, inflammatory markers, and cerebrovascular endothelial function among adults in urban China. J Acquir Immune Defic Syndr 2017;74(3):339–346. doi: 10.1097/QAI.0000000000001254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Mukerji SS, Misra V, Lorenz D, et al. Temporal patterns and drug resistance in CSF viral escape among ART-experienced HIV-1 infected adults. J Acquir Immune Defic Syndr 2017;75(2):246–255. doi: 10.1097/QAI.0000000000001362. [DOI] [PMC free article] [PubMed] [Google Scholar]