

Microcatheterization and viscodilation of Schlemm canal or canaloplasty has been shown to reduce intraocular pressure (IOP) in open-angle glaucoma.1,2 In separate studies, trabeculotomy performed with a catheter or a suture has been shown to lower IOP.3,4 The OMNI Surgical System (Sight Sciences Inc.) is the first microinvasive glaucoma surgery device that enables surgeons to perform canaloplasty and trabeculotomy in succession with a single instrument. This study reports the early results with this multimodal surgical technology.
METHODS
Eyes with open-angle glaucoma underwent phacoemulsification combined with 180 degrees of canaloplasty, followed by 180 degrees of trabeculotomy using the OMNI device. The preoperative IOP was determined by the mean value of IOPs from the 2 visits before surgery measured using a Goldmann applanation tonometer. The postoperative IOP was determined by the mean value of IOPs from the last 3 postoperative visits. The preoperative IOP was used to stratify the eyes into 3 groups (Figure 1). In each group, a paired 1-sample t test was used to determine whether there were statistically significant changes in IOP compared with baseline as a result of the operation.
Figure 1.
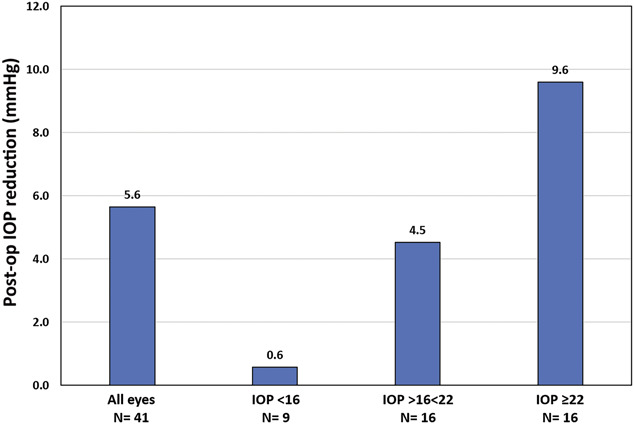
Postoperative IOP reduction in all eyes and in 3 groups stratified by preoperative IOP levels (IOP = intraocular pressure).
RESULTS
The study evaluated 41 eyes (24 patients). The mean IOP reduction in all eyes was 5.6 ± 4.5 mm Hg (P < .001) (Figure 1). The mean follow-up was 4.1 ± 1.9 months. There was a significant correlation between the magnitude of IOP reduction and preoperative IOP that is best described by a linear relationship (R2 = 0.7, P < .001) (Figure 2). In eyes with a preoperative IOP higher than 22 mm Hg, the mean IOP reduction was 9.6 ± 3.5 mm Hg (P < .001). In eyes with a preoperative IOP higher than 16 mm Hg, 100% had a decrease in IOP postoperatively.
Figure 2.
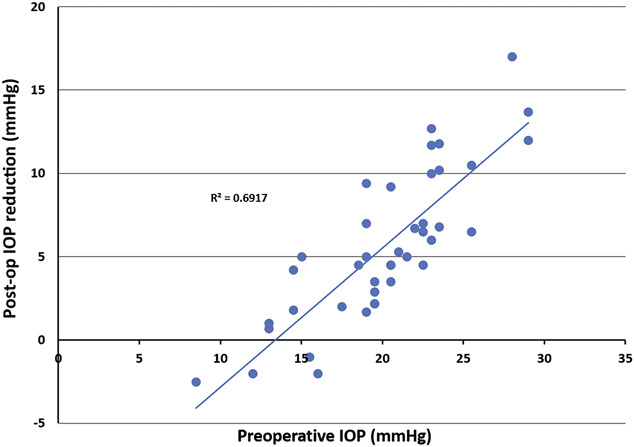
Relationship between the magnitude of IOP reduction and preoperative IOP (IOP = intraocular pressure).
There were no complications related to cataract surgery. There were 2 cases of hyphema (4%) that cleared within 1 week. There was no protocol for reducing medication usage postoperatively. The mean number of medications decreased slightly, but this was not significant. No eye has required secondary glaucoma surgery.
DISCUSSION
This study found that OMNI combined with phacoemulsification reduced IOP. The magnitude of pressure lowering with OMNI was highly correlated with the preoperative IOP (Figures 1 and 2). This is a similar finding to a previous study of the original iStent.5 However, the phaco-OMNI surgery had a mean overall IOP reduction of 5.6 mm Hg, whereas the mean phaco-iStent IOP reduction was 3.2 mm Hg.5
The decision to perform 180 degrees of OMNI in combined surgery was based on the goal of maximizing efficacy while minimizing the extent of surgery and to perform a smaller rather than a larger procedure. Some surgeons may choose to perform 360 degrees of canaloplasty with 180 degrees of trabeculotomy or some other combination. The extent of trabeculotomy and canaloplasty can be titrated easily depending on the clinical context.
Patients in this study generally had mild-to-moderate glaucoma, but some had more advanced disease. Follow-up was limited because the OMNI device has only been available in the United States since mid-2018. There was no protocol for reducing medications, but the level of pressure reduction suggests that some patients may benefit from a reduction in medications. However, longer-term studies are needed to assess the durability of reduction in IOP and the opportunity for decreasing the medication burden.
The OMNI device may give surgeons a safe, implant-free microinvasive glaucoma surgery option for combining trabeculotomy and canaloplasty in a single procedure. Combined with phacoemulsification the device reduced IOP more in eyes with higher preoperative pressures. Therefore, eyes with the greatest need for IOP reduction may experience the greatest benefit.
Footnotes
Disclosures: Dr. Brown is a consultant for Sight Sciences Inc. Dr. Dhamdhere is an employee of Sight Sciences Inc. None of the other authors have a financial or proprietary interest in any material or method mentioned.
REFERENCES
- 1.Lewis RA, von Wolff K, Tetz M, Koerber N, Kearney JR, Shingleton BJ, Samuelson TW. Canaloplasty: circumferential viscodilation and tensioning of Schlemm canal using a flexible microcatheter for the treatment of open-angle glaucoma in adults Two-year interim clinical study results. J Cataract Refract Surg 2009;35:814-24 [DOI] [PubMed] [Google Scholar]
- 2.Gallardo MJ, Supnet RA, Ahmed IIK. Viscodilation of Schlemm's canal for the reduction of IOP via an ab-interno approach. Clin Ophthalmol 2018;12:2149–2155 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Grover DS Smith O Fellman RL Godfrey DG. Gupta A Montes de Oca I Feuer WJ. Gonioscopy-assisted transluminal trabeculotomy: an ab interno circumferential trabeculotomy: 24 Months follow-up. J Glaucoma 2018;27:393–401. [DOI] [PubMed] [Google Scholar]
- 4.Sarkisian SR, Mathews B, Ding K, Patel A, Nicek Z. 360° ab-interno trabeculotomy in refractory primary open-angle glaucoma. Clin Ophthalmol 2019;13:161–168 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Brown RH, Gibson Z, Zhong L, Lynch MG. IOP reduction after cataract surgery with trabecular device. J Cataract Refract Surg 2015;41:1318–1319 [DOI] [PubMed] [Google Scholar]