

Abstract
Objectives:
There has been growing research interest in loneliness and wisdom in recent decades, but no cross-cultural comparisons of these constructs using standardized rating measures in older adults, especially the oldest-old. This was a cross-sectional study of loneliness and wisdom comparing middle-aged and oldest-old adults in Cilento, Italy and San Diego, United States.
Method:
We examined loneliness and wisdom, using the UCLA Loneliness Scale Version 3 (UCLA-3) and San Diego Wisdom Scale (SD-WISE), respectively, in four subject groups: adults aged 50–65 and those ≥90 years from Cilento, Italy (N = 212 and 47, respectively) and San Diego, California, USA (N = 138 and 85, respectively).
Results:
After controlling for education, there were no significant group differences in levels of loneliness, while on SD-WISE the Cilento ≥90 group had lower scores compared to the other three groups. There was a strong inverse correlation between loneliness and wisdom in each of the four subject groups. Loneliness was negatively associated while wisdom was positively associated with general health, sleep quality, and happiness in most groups, with varying levels of significance.
Conclusion:
These results largely support cross-cultural validity of the constructs of loneliness and wisdom, and extend previous findings of strong inverse correlations between these two entities. Loneliness has become a growing public health problem, and the results of our study suggest that wisdom could be a protective factor against loneliness, although alternative explanations are also possible. Research on interventions to reduce loneliness by enhancing wisdom in older adults is needed.
Keywords: longevity, health, happiness, social isolation, compassion
INTRODUCTION
The world population is aging rapidly (United Nations Department of Economic and Social Affairs, 2019). The fastest growing segment of the population is that of the oldest-old; it is also the segment that generates the highest healthcare costs because of medical comorbidities. In recent decades there has been growing concern about loneliness across all ages, but particularly in middle-aged and older adults (Anderson & Thayer, 2018; Dahlberg, Andersson, McKee, & Lennartsson, 2015; Holt-Lunstad, 2017). Empirical research on loneliness received prominence with Weiss’s seminal book (Weiss, 1973), followed by others (Peplau, 1982). Loneliness has been defined as the subjective feeling of being isolated (National Academies of Sciences & Medicine, 2020) or a subjective negative experience that results from inadequate meaningful connections (Fried et al., 2020). Loneliness is consistently associated with unhealthy aging. It has been identified as a major risk factor for adverse mental and physical health outcomes (L. C. Hawkley & Cacioppo, 2010; Holt-Lunstad, 2017; D. V. Jeste, Lee, & Cacioppo, 2020), including worse general health, poor quality of sleep, lower levels of well-being or happiness, depression (J. T. Cacioppo, Hawkley, Berntson, et al., 2002; J. T. Cacioppo, Hawkley, Crawford, et al., 2002), frailty, cardiovascular disease (Thurston & Kubzansky, 2009), Alzheimer’s disease (Wilson et al., 2007), accelerated biological aging (Louise C. Hawkley & Cacioppo, 2007), and premature mortality (Holt-Lunstad, 2017; Shiovitz-Ezra & Ayalon, 2010)). Conversely, increased morbidity has been shown to increase loneliness (Kristensen, König, & Hajek, 2019). The public health impact of loneliness is comparable to that of cigarette smoking and obesity (McGregor, 2017).
We previously found, in a study of community-dwelling individuals across adult lifespan, that the relationship between loneliness severity and age was non-linear, with loneliness peaking in late-20s, mid-50s, and late-80s (Ellen E. Lee et al., 2019). A novel finding from our study was a significant inverse correlation between loneliness and wisdom – i.e., people with higher scores on a measure of wisdom were less lonely and vice versa (Ellen E. Lee et al., 2019). This finding was supported in a qualitative study of loneliness in older adults (Morlett Paredes et al., 2019). Wisdom has been discussed in religious and philosophical literature since ancient times (Achenbaum & Orwoll, 1991; M. Ardelt, 1997; Monika Ardelt, 2000; Clayton & Birren, 1980; Smith & Baltes, 1990; Sternberg, 1990; Sternberg & Jordan, 2005), but has been receiving increasing attention as a topic of empirical research in the past few decades (Dilip V Jeste & Lee, 2019). Wisdom is a holistic, multidimensional human trait comprised of several specific components: prosocial behaviors including empathy, compassion, and altruism; emotional regulation; self-reflection; decisiveness in the face of uncertainty; acceptance of divergent value systems; and social advising (Dilip V Jeste et al., 2010; Dilip V Jeste & Lee, 2019; Dilip V Jeste & Ipsit V Vahia, 2008; Meeks & Jeste, 2009). Definitions of wisdom over centuries and across cultural and geographic boundaries share surprising similarities, suggesting a unique biological construct (D. V. Jeste & I. V. Vahia, 2008; Meeks & Jeste, 2009)). Recent studies have identified neural correlates of the components of wisdom, suggesting that the putative neurocircuitry of wisdom involves prefrontal cortex and limbic striatum (Dilip V Jeste & Lee, 2019; Meeks & Jeste, 2009).
Both loneliness and wisdom are personality traits. Most personality traits including loneliness are partially inherited and partly determined by environment – i.e., epigenetics (Abdellaoui et al., 2019; S. Cacioppo, Capitanio, & Cacioppo, 2014). While there are no large-scale genetic studies using a validated scale of wisdom, it is likely that wisdom too is determined partly by genes and partly by environment. Family upbringing as well as cultural factors affect personality development. Loneliness is more common among racial/ethnic minorities and immigrants (Louise C Hawkley et al., 2008). Grossmann, Weststrate, Ferrari, and Brienza (2020) examined cultural factors and related contexts that may impact wisdom, and found differences in both concepts of wisdom by culture and differences by group on performance in measures of wisdom. In contrast to loneliness, wisdom is reportedly associated with greater well-being, satisfaction with life, and overall better health, all indicators of successful aging (M. Ardelt, 1997; Dilip V. Jeste, Lee, Palmer, & Treichler, 2020).
Despite growing research, large gaps remain in our understanding of loneliness and wisdom – for example, rates and drivers of loneliness in different populations, including the effects of cultural and societal factors (Fried et al., 2020), key therapeutic elements of potential interventions to reduce loneliness (National Academies of Sciences & Medicine, 2020), and sociocultural differences in wisdom using standardized rating scales and appropriate covariates, especially in the oldest-old (Dilip V. Jeste et al., 2020).
The goals of the current study were to evaluate loneliness and wisdom and their relationship with relevant psychological and physical functioning, in samples of middle-aged and oldest-old adults from Cilento, Italy and San Diego, California, USA. The Cilento region in southwestern Italy is the birthplace of the Mediterranean diet (Keys & Keys, 1959). It is a relatively isolated, rural area believed to have a relatively high concentration of the oldest-old individuals (≥ 90 years). The present investigation was born out of the Cilento Initiative on Aging Outcomes (CIAO) study (Scelzo et al., 2018). We have previously reported that, compared to their younger (age 50–75) cohabitants, people aged ≥90 exhibited better mental well-being, with resilience, optimism, religiosity, family bonds, and stubbornness (Scelzo et al., 2018), a healthier metabolic and cardiovascular profile (Daniels et al., 2019), and no significant differences in the laboratory assessment of oxidative stress and APOE genotype (Pizza et al., 2020). The people > 90 did not have severe cognitive impairment, and the prevalence of dementia was low.
Our U.S. cohort came from the Successful AGing Evaluation (SAGE) Study at UC San Diego, comprised of community-dwelling individuals from predominantly urban and suburban areas of San Diego County. We have reported a “paradox of aging” in this sample, with better mental health than younger adults, despite declining physical function (Dilip V Jeste et al., 2013; Michael L Thomas et al., 2016).
In the present investigation, we compared loneliness and wisdom in middle-aged and oldest-old samples from Cilento and San Diego, using validated rating scales. We hypothesized that cross-cultural validity of these constructs would be supported by comparable levels of loneliness and wisdom as well as similar relationships of these constructs with relevant measures of physical and mental health. For the purposes of external validation, we sought to evaluate correlations of loneliness and wisdom with general health, quality of sleep, and happiness.
METHODS
Study Participants
CIAO Study:
This study is designed to assess the impact of lifestyle and other factors on healthy aging and aging-related diseases among residents of Cilento, Italy. Study participants included 212 individuals aged 50 to 65 years and 47 individuals aged 90 or above. Thirty general practitioners (GPs) from the Cilento region referred to this study their consenting patients in the specified age groups. Exclusion criteria were: 1) inability to complete study assessments, and 2) a diagnosis of dementia or other major neurological disorder. The GPs made an appointment with the invited subjects, from whom they first obtained a signed informed consent before enrolling in the CIAO Study. The study included 17 villages in the Cilento area: Asceai, Cannalonga, Casal Velino, Ceraso, Cuccaro, Futani, Mandia, Pollica, Laurino, Novi Velia, Montano Antilia, San Mauro La Bruca, Gioi, Stella Cilento, Stio, Sessa Cilento, and Vallo della Lucania. To visit and assess participants, trained study staff traveled across these villages.
SAGE Study:
The Successful AGing Evaluation (SAGE) study includes community-dwelling subjects across the adult lifespan (D. V. Jeste et al., 2013; M. L. Thomas et al., 2016). A structured multi-cohort design was employed to recruit a demographically representative sample of San Diego County residents using a modified form of random digit dialing. Study participants included 138 individuals aged 50–65 years and 85 individuals ages 90 years or above. Exclusion criteria were: 1) residence in a nursing home or need for daily skilled nursing care, 2) a diagnosis of dementia made by the subject’s treating clinician, as reported by the subject, and 3) terminal illness or need for hospice care. All the subjects signed a written informed consent form either online or in person, and completed a paper and pencil or online survey questionnaire.
The study protocol received the approval of the IRB of the ASL Salerno (ethics committee Campania Sud) number 48 and UC San Diego Human Research Subjects Protection Program. All study participants provided written consent to participate.
Sociodemographic and Clinical Characteristics
Sociodemographic and lifestyle characteristics (age, sex, race/ethnicity, education, marital status, employment status, smoking, and alcohol use) were obtained through structured interviews with participants in Cilento and through a survey questionnaire in San Diego. Italian versions of standardized published measures were used in Cilento. General health was assessed with a single question from the 36-item Medical Outcomes Study Short Form (MOS SF-36) (“In general, would you say your health is….”,(Ware & Sherbourne, 1992)), and sleep quality was evaluated with a single item from the PROMIS Sleep Disturbance Measure (“My sleep quality is …”, Cella et al., 2010 (Cella et al., 2010)), each to be rated on a 1-to-5 scale. Happiness was measured using the 4-item Happiness (positive affect) subscale of the Center for Epidemiologic Studies Depression Scale (CES-D) (Radloff, 1977). Additional measures of physical health included comorbid medical conditions reported as well as body mass index (BMI).
Loneliness Measure
The UCLA Loneliness Scale (Version 3) (UCLA-3) (Russell, 1996), a widely used measure of loneliness was administered. It consists of 20 statements that do not use the word “lonely” explicitly. Higher scores indicate greater loneliness. The UCLA-3 has demonstrated good to excellent test-retest reliability (Russell, 1996), internal consistency (Lasgaard, 2007; Russell, 1996; Vassar & Crosby, 2008), discriminant validity (Lasgaard, 2007), and convergent validity (Lasgaard, 2007; Russell, 1996).
Wisdom Measure
The San Diego Wisdom Scale (SD-WISE) (Thomas et al., 2019) was designed to assess six components or domains of wisdom (emotional regulation, self-reflection or insight, pro-social behaviors, acceptance of divergent values, decisiveness, and social advising), and to produce psychometric estimates of a higher-order and latent construct—a putative measure of personal wisdom. The words “wisdom” and “wise” are not used explicitly in any statement. The scale includes 24 items, with four items for each of the six components, and higher scores are indicative of higher levels of those components. The SD-WISE has shown good to excellent psychometric properties (Thomas et al., 2019).
Two bilingual coauthors from Rome (MS and AB) spent several months in San Diego, familiarizing themselves with the SAGE study, including the use of various measures. They translated the UCLA-3 and SD-WISE scales into Italian, back-translated them into English, and with input from various investigators from Italy and the U.S., retranslated into Italian to ensure cultural coherence of the scale items.
Statistical Analysis
The study cohorts were compared across the four age groups: CIAO age 50–65 (Group 1), SAGE age 50–65 (Group 2), CIAO age ≥90 (Group 3), and SAGE age ≥90 (Group 4). Participant sociodemographic and clinical characteristics, including loneliness and wisdom, were compared across the four groups using one-way analysis of variance (ANOVA) with post-hoc Holm Adjustment (Holm, 1979) for continuous variables and Chi-square tests for discrete variables. Please note that we conducted four post-hoc group comparisons: Groups 1 vs. 2, 1 vs. 3, 2 vs. 4, and 3 vs. 4. (We did not compare Groups 2 vs. 3 as they differed in both age and site.) A two-sided alpha level of p < 0.05 was used to determine statistical significance. Given that education level differed significantly between age groups in SAGE and CIAO cohorts (χ2 = 331, p < 0.0001), analyses were repeated, controlling for education. To improve robustness of study findings, estimating equations were used for inference (Tang, He, & Tu, 2012).
Pearson’s correlations were used to evaluate the relationship between loneliness and wisdom as well as the associations of these constructs with other variables including medical comorbidity, BMI, general health, sleep quality, and happiness. The Fisher r-to-z transformations were performed to compare the correlations across groups. To assess the associations of loneliness and wisdom across the subject groups and covariates, linear regression with backwards elimination was performed, with loneliness or wisdom as the dependent variable and all other covariates by group interactions as predictors. Unlike forward selection, backward elimination starts with a less biased model and thus provides more reliable variable selection (Wang et al., 2017).
RESULTS
Demographic and clinical characteristics of the four subject groups are presented in Tables 1a and 1b. The total sample comprised of 485 participants, including 262 from the CIAO cohort (Group 1: CIAO ages 50–65, n = 215; Group 3: CIAO ages ≥90, n = 47) and 223 from the SAGE cohort (Group 2: SAGE 50–65, n = 138; Group 4: SAGE ≥90, n = 85). The groups did not differ on sex distribution. Middle-aged adults were more likely to be married or cohabitating with a partner than the oldest-old. The CIAO cohort had considerably lower education level compared to the SAGE cohort, with CIAO oldest-old having the fewest proportion of individuals who obtained some college education. Among middle-aged adults, SAGE cohort was more likely to be employed compared to CIAO cohort. Unsurprisingly, the number of total medical conditions endorsed was higher and general health rating was lower in oldest-old adults compared to middle-aged adults among both CIAO and SAGE cohorts.
Table 1a:
CIAO vs. SAGE Study Comparisons by Age Groups
| Age 50–65 | Age >90 | F or x2 | p | |||
|---|---|---|---|---|---|---|
| CIAO | SAGE | CIAO | SAGE | |||
| (N=212) | (N=138) | (N=47) | (N=85) | |||
| Group 1 | Group 2 | Group 3 | Group 4 | |||
| Mean (SD) or % | Mean (SD) or % | Mean (SD) or % | Mean (SD) or % | |||
| Socio-demographics | ||||||
| Age (years) | 57.8 (4.5) | 58.1 (4.9) | 92.7 (3) | 93.2 (3.2) | 3018 | <.0001 |
| Sex | ||||||
| Female | 53% | 49% | 68% | 48% | 2 | 0.100 |
| Race | ||||||
| Caucasian | 100% | 75% | 100% | 94% | 83 | 0.020 |
| Marital Status | ||||||
| Married or cohabiting | 82% | 70% | 19% | 39% | 40 | <.0001 |
| Education | ||||||
| Some College and Above | 12% | 94% | 5% | 85% | 331 | <.0001 |
| Employment Status | ||||||
| Employed professionally (full-time or part-time) | 56% | 75% | 0% | 2% | 295 | <.0001 |
| Lifestyle Factors | ||||||
| Smoker - current | 29% | 11% | 0% | 4% | 42 | <.0001 |
| Smoker - ever | 56% | 26% | 16% | 48% | 46 | <.0001 |
| Alcohol Use (current) | ||||||
| Non-drinker | 37% | 15% | 56% | 33% | 119 | <.0001 |
| Drinker | 63% | 85% | 44% | 68% | ||
| Physical and Mental Health | ||||||
| Medical Conditions | ||||||
| High Blood Pressure | 45% | 31% | 77% | 67% | 17 | <.0001 |
| High Cholesterol | 46% | 29% | 34% | 37% | 4 | 0.010 |
| Diabetes | 9% | 4% | 18% | 17% | 4 | 0.010 |
| Heart Attack | 1% | 2% | 11% | 12% | 3 | 0.020 |
| Stroke | 1% | 1% | 7% | 11% | 4 | 0.005 |
| Cancer | 5% | 18% | 12% | 46% | 21 | <.0001 |
| Ulcer | 5% | 2% | 5% | 0% | 7 | 0.080 |
| Colitis | 2% | 1% | 9% | 0% | 15 | 0.002 |
| Emphysema/COPD | 4% | 2% | 23% | 4% | 4 | 0.006 |
| Total medical conditions endorsed | 1.1 (1.0) | 0.9 (0.9) | 1.9 (1.4) | 1.9 (1.3) | 18.11 | <.0001 |
| BMI | 28.4 (4.8) | 28.2 (6.3) | 26.9 (3.9) | 25.4 (3.9) | 11 | <.0001 |
| General Health Rating (range 1–5) | 3.4 (0.7) | 3.6 (0.9) | 3.1 (0.8) | 3.3 (0.9) | 6 | 0.0009 |
| Sleep Quality (range 1–5) | 3.4 (0.9) | 3.6 (0.9) | 3.2 (0.8) | 3.9 (0.8) | 7 | 0.0001 |
| CESD Happiness Scale (range 0–12) | 6.9 (3.3) | 9.8 (2.7) | 4.9 (2.2) | 9.3 (2.8) | 26 | <.0001 |
| Loneliness | ||||||
| UCLA Loneliness Scale Total Score (range 20–80) | 39.9 (8.4) | 36.8 (10) | 44.7 (8.1) | 37.0 (10.8) | 10 | <.0001 |
| Wisdom (range 1–5) | ||||||
| SD-WISE - Pro-Social Behaviors | 4.1 (0.6) | 4.2 (0.5) | 3.5 (0.7) | 4.2 (0.5) | 16 | <.0001 |
| SD-WISE - Emotional Regulation | 3.2 (0.7) | 3.8 (0.7) | 3.1 (0.7) | 3.6 (0.6) | 25 | <.0001 |
| SD-WISE - Self-Reflection (Insight) | 3.7 (0.6) | 3.8 (0.7) | 3.2 (0.5) | 3.5 (0.5) | 16 | <.0001 |
| SD-WISE - Acceptance for Divergent Values | 3.9 (0.6) | 4.0 (0.6) | 3.4 (0.7) | 3.8 (0.5) | 7 | <.0001 |
| SD-WISE - Decisiveness | 3.4 (0.8) | 3.8 (0.8) | 3.2 (0.7) | 3.7 (0.7) | 12 | <.0001 |
| SD-WISE - Social Advising | 3.6 (0.6) | 3.8 (0.6) | 3.3 (0.5) | 3.6 (0.6) | 13 | <.0001 |
| SD-WISE - Total | 3.7 (0.4) | 3.9 (0.4) | 3.3 (0.4) | 3.7 (0.4) | 24 | <.0001 |
Note: One-way ANOVA were performed for continuous variables and Chi-square tests were performed for categorical variables.
Abbreviations:
BMI = Body Mass Index
CESD = Center for Epidemiologic Studies Depression Scale
COPD = Chronic Obstructive Pulmonary Disease
SD-WISE = San Diego Wisdom Scale
Table 1b:
CIAO vs. SAGE Study Comparisons by Age Groups - Pairwise Significance (p-values)
| 1 vs 2 | 1 vs 3 | 2 vs 4 | 3 vs 4 | |
|---|---|---|---|---|
| Socio-demographics | ||||
| Age (years) | 0.9754 | <.0001 | <.0001 | 0.9754 |
| Sex | ||||
| Female | N/A | N/A | N/A | N/A |
| Race | ||||
| Caucasian | 0.0000 | 1.0000 | 0.0000 | 0.5556 |
| Marital Status | ||||
| Married or cohabiting | 0.5430 | <.0001 | <.0001 | 0.1224 |
| Education | ||||
| Some College and Above | <.0001 | 0.0000 | 0.2213 | <.0001 |
| Employment Status | ||||
| Employed professionally (full-time or part-time) | 0.0000 | 0.1894 | 0.0477 | 0.8940 |
| Lifestyle Factors | ||||
| Smoker - current | 0.0003 | 0.0000 | 0.3902 | 0.5705 |
| Smoker - ever | 0.0000 | 0.0000 | 0.0035 | 0.0009 |
| Alcohol Use (current) | ||||
| Non-drinker | 0.0033 | 0.0016 | 0.6020 | 0.3777 |
| Drinker | ||||
| Physical and Mental Health | ||||
| Medical Conditions | ||||
| High Blood Pressure | 0.0201 | 0.0002 | 0.0000 | 0.2508 |
| High Cholesterol | 0.0079 | 0.7042 | 0.7042 | 1.0000 |
| Diabetes | 0.0622 | 0.0001 | 0.0000 | 0.9741 |
| Heart Attack | 0.3376 | 0.2008 | 0.0186 | 0.8098 |
| Stroke | 1.0000 | 0.0110 | 0.0032 | 1.0000 |
| Cancer | 0.9001 | 0.0634 | 0.0001 | 0.6710 |
| Ulcer | N/A | N/A | N/A | N/A |
| Colitis | 0.0020 | 0.4313 | 0.0000 | 0.0000 |
| Emphysema/COPD | 0.8384 | 0.0060 | 0.8384 | 0.0019 |
| Total medical conditions endorsed | 0.0620 | 0.0000 | 0.0000 | 0.9740 |
| BMI | 0.8203 | 0.2825 | 0.0005 | 0.3348 |
| General Health Rating (range 1–5) ↑ better | 0.2582 | 0.0235 | 0.0235 | 0.2582 |
| Sleep Quality (range 1–5) ↑ better | 0.1575 | 0.2203 | 0.0709 | 0.0006 |
| CESD Happiness Scale | 0.0000 | 0.0382 | 0.2807 | 0.0000 |
| Loneliness | ||||
| UCLA Loneliness Scale Total Score | 0.0123 | 0.0123 | 0.8873 | 0.0001 |
| Wisdom | ||||
| SD-WISE - Pro-Social Behaviors | 0.0473 | 0.0000 | 0.4815 | 0.0000 |
| SD-WISE - Emotional Regulation | 0.0000 | 0.2719 | 0.1767 | 0.0001 |
| SD-WISE - Self-Reflection (Insight) | 0.2566 | 0.0000 | 0.0049 | 0.0049 |
| SD-WISE - Acceptance for Divergent Values | 0.7698 | 0.0000 | 0.1747 | 0.0051 |
| SD-WISE - Decisiveness | 0.0000 | 0.1156 | 0.2131 | 0.0021 |
| SD-WISE - Social Advising | 0.0028 | 0.0028 | 0.0053 | 0.0105 |
| SD-WISE - Total | 0.0000 | 0.0000 | 0.0049 | 0.0000 |
Note: 1--Age 50–65 CIAO, 2--Age 50–65 SAGE, 3--Age ≥90 CIAO, 4--Age ≥90 SAGE.
Holm Adjustment was used to adjust for multiple comparisons of the pairwise significances.
NA = Not Applicable as the ANOVAs in Table 1b were not significant.
Comparison of Loneliness across Groups
Initial analysis of UCLA-3 scores across groups revealed differences among all the four groups, except between SAGE middle-aged and oldest-old adults (Tables 1a and 1b). Loneliness levels were highest in the CIAO ≥90 group, compared to CIAO 50–65 and SAGE ≥90 groups. CIAO middle-aged adults were also lonelier than their SAGE middle-aged counterparts. However, after controlling for education, there were no significant differences in loneliness among the four groups (Table 2a; Figure 1).
Table 2a:
Comparison of UCLA Loneliness and SD-WISE Scale Scores of CIAO vs. SAGE Study Comparisons by Age Groups, controlling for Education
| Age 50–65 | Age >90 | F or x2 | p | |||
|---|---|---|---|---|---|---|
| CIAO | SAGE | CIAO | SAGE | |||
| (N=212) | (N=138) | (N=47) | (N=85) | |||
| Mean (SD) or % | Mean (SD) or % | Mean (SD) or % | Mean (SD) or % | |||
| UCLA Loneliness Scale Total Score | 39.9 (8.4) | 36.8 (10) | 44.7 (8.1) | 37.0 (10.8) | 1.1025 | 0.2937 |
| SD-WISE - Pro-Social Behaviors | 4.1 (0.6) | 4.2 (0.5) | 3.5 (0.7) | 4.2 (0.5) | 8.4397 | 0.0037 |
| SD-WISE - Emotional Regulation | 3.2 (0.7) | 3.8 (0.7) | 3.1 (0.7) | 3.6 (0.6) | 0.1299 | 0.7186 |
| SD-WISE - Self-Reflection (Insight) | 3.7 (0.6) | 3.8 (0.7) | 3.2 (0.5) | 3.5 (0.5) | 36.9121 | <.0001 |
| SD-WISE - Acceptance for Divergent Values | 3.9 (0.6) | 4.0 (0.6) | 3.4 (0.7) | 3.8 (0.5) | 16.3054 | 0.0001 |
| SD-WISE - Decisiveness | 3.4 (0.8) | 3.8 (0.8) | 3.2 (0.7) | 3.7 (0.7) | 0.1736 | 0.6770 |
| SD-WISE - Social Advising | 3.6 (0.6) | 3.8 (0.6) | 3.3 (0.5) | 3.6 (0.6) | 13.0819 | 0.0003 |
| SD-WISE - Total | 3.7 (0.4) | 3.9 (0.4) | 3.3 (0.4) | 3.7 (0.4) | 15.7921 | 0.0001 |
Note: GEE was performed to compare the difference across 4 groups, controlling for Education
Figure 1:
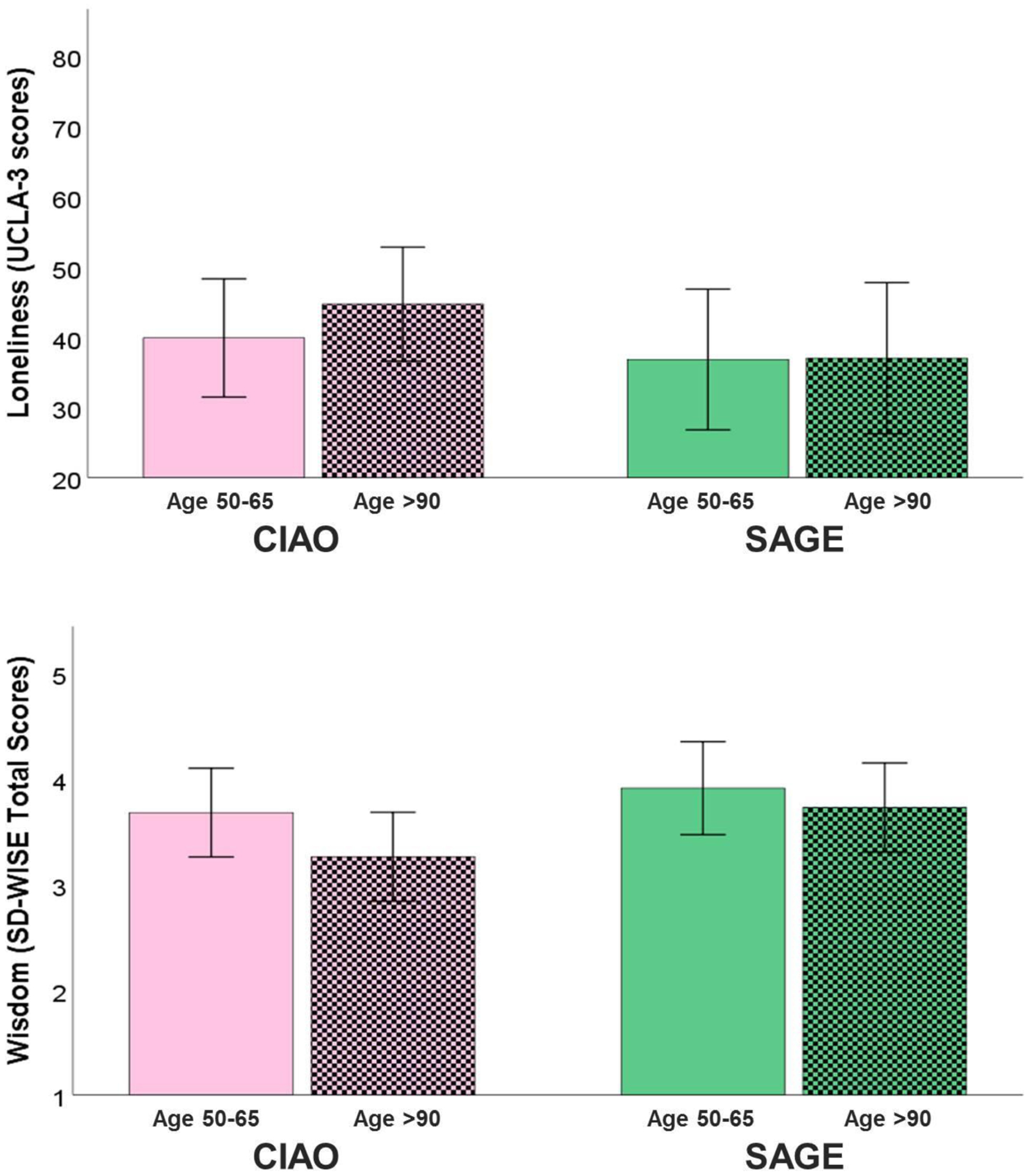
Comparison of Loneliness and Wisdom Scale Scores in the Cilento and San Diego Samples by Age Group (50–65 and >90 years)
Comparison of Wisdom across Groups
Initial analysis of the SD-WISE across groups revealed differences in total wisdom level among all the four groups (Tables 1a and 1b). Oldest-old adults had lower scores than middle-aged adults (in both CIAO and SAGE cohorts), and CIAO participants had lower scores than SAGE participants (in both middle-aged and oldest-old adults). The CIAO ≥90 group had lower scores than both CIAO 50–65 and SAGE ≥90 groups. Examination of SD-WISE subscales revealed that the CIAO ≥90 group had lower scores on each component compared to the SAGE ≥90 group, and on every component except for emotional regulation and decisiveness compared to CIAO 50–65 group.
However, after controlling for education, total wisdom score was no longer different between CIAO and SAGE middle-aged adults, but other differences remained: ≥90 adults had lower total SD-WISE scores than each of the other three groups (Tables 2a and 2b; Figure 1). On the SD-WISE subscales, middle-aged adults had higher scores on self-reflection and social advising components than oldest-old adults (in both CIAO and SAGE cohorts). The CIAO ≥90 group had lower scores on the pro-social behavior component compared to CIAO 50–65 and SAGE ≥90 groups. On the component of acceptance of diverse perspectives, the CIAO 50–65 group had lower scores compared to SAGE 50–65 group, and CIAO ≥90 had lower scores compared to CIAO 50–65 group. There were no group differences on emotional regulation and decisiveness components.
Table 2b:
Comparison of UCLA Loneliness and SD-WISE Scale Scores of CIAO vs. SAGE Study Comparisons by Age Groups, controlling for Education – Pairwise significance (p-values)
| 1 vs 2 | 1 vs 3 | 2 vs 4 | 3 vs 4 | |
|---|---|---|---|---|
| UCLA Loneliness Scale Total Score | N/A | N/A | N/A | N/A |
| SD-WISE - Pro-Social Behaviors | 0.9740 | <0.0001 | 0.4490 | <0.0001 |
| SD-WISE - Emotional Regulation | N/A | N/A | N/A | N/A |
| SD-WISE - Self-Reflection (Insight) | 0.0660 | 0.0001 | 0.0024 | 0.8198 |
| SD-WISE - Acceptance for Divergent Values | 0.0485 | 0.0023 | 0.1772 | 0.3781 |
| SD-WISE - Decisiveness | N/A | N/A | N/A | N/A |
| SD-WISE - Social Advising | 0.6059 | 0.0220 | 0.0065 | 0.7697 |
| SD-WISE - Total | 0.9220 | <0.0001 | 0.0020 | 0.0047 |
Note: GEE was performed to compare the difference across 4 groups, controlling for Education.
NA = Not Applicable as the ANOVAs in Table 2b were not significant.
Correlations of Loneliness and Wisdom
Pearson’s correlations revealed strong inverse associations (p <.001) between loneliness and total SD-WISE score, in all four subject groups (Figure 2; Table 3); there were no significant differences in r values, although the Cilento ≥90 group (r = −.755) had a numerically higher correlation than the other three groups (r = −.5 to −.6). Participants with higher scores on UCLA-3 had lower scores on SD-WISE, and vice versa. Loneliness also correlated inversely with most of the SD-WISE subscale scores in the four groups, though the level of significance varied. Loneliness was negatively correlated with general health, quality of sleep, and happiness while wisdom was positively correlated with those variables with the exception of happiness in the CIAO >90 group; however, the levels of significance varied considerably across groups (Supplemental Tables 1 and 2). There were very few significant correlations between either loneliness or wisdom and the total number of medical conditions reported or BMI.
Figure 2:
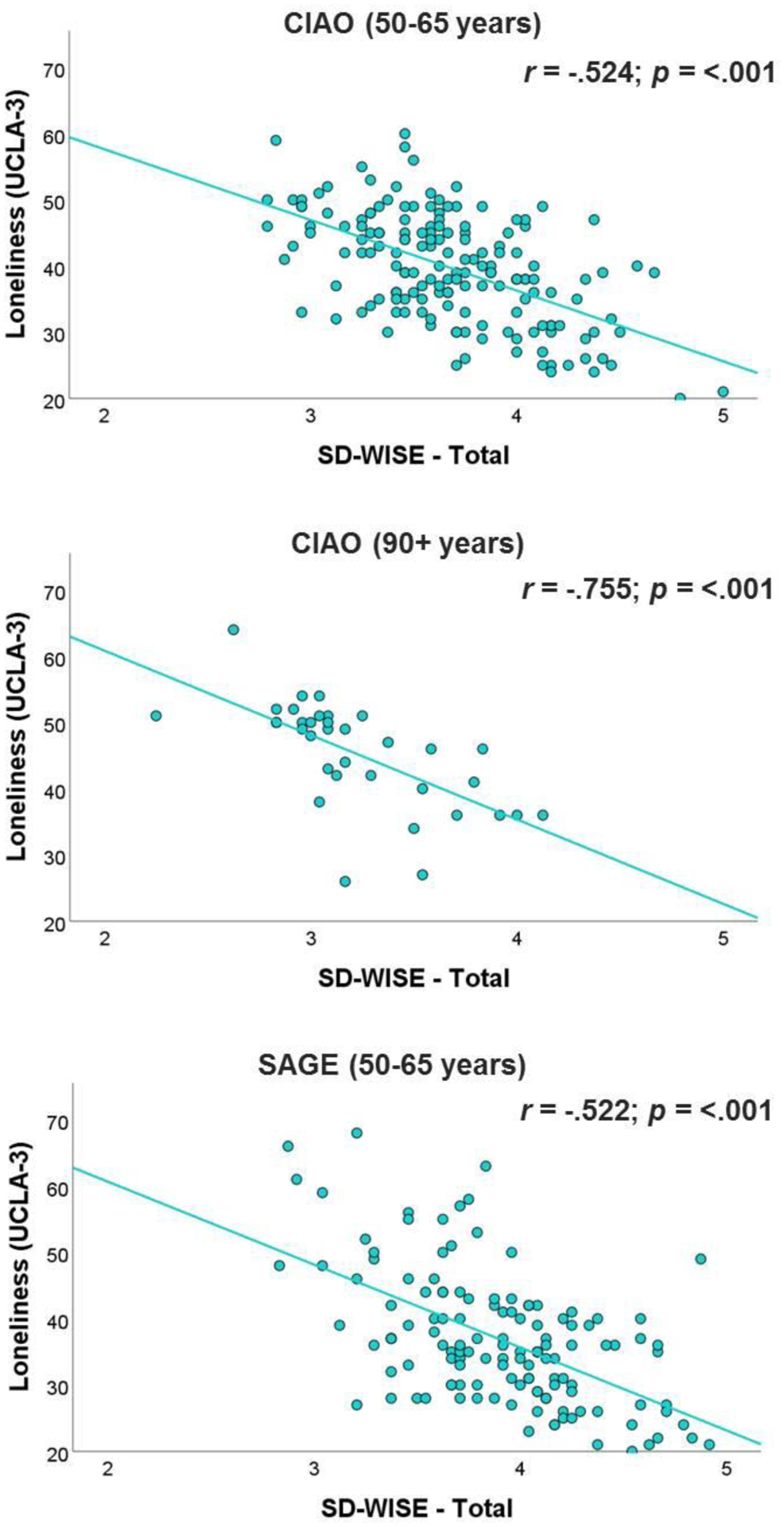
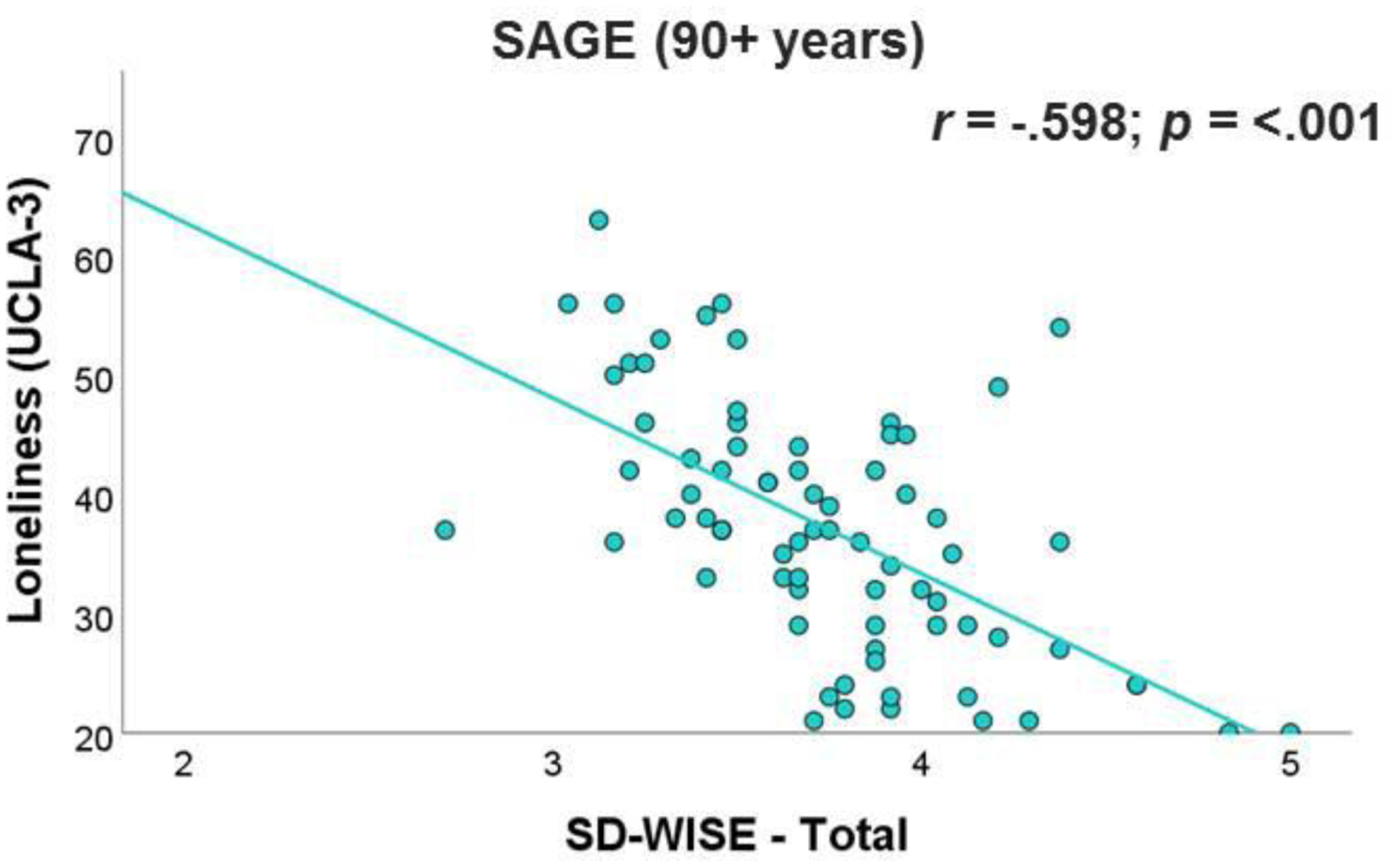
Pearson’s Correlations between Loneliness and Wisdom Scale Scores in the Cilento and San Diego Samples by Age Group (50–65 and >90 years)
Table 3:
Pearson’s Correlations of UCLA Loneliness Scale with SD-WISE Subscale Scores by Age Group and Site
| Age 50–65 | Age >90 | x 2 | p | |||
|---|---|---|---|---|---|---|
| CIAO | SAGE | CIAO | SAGE | |||
| (N=212) | (N=138) | (N=47) | (N=85) | |||
| Pro-Social Behaviors | −.370 *** | −.514 ** | −.426 * | −.606 *** | 5.32 | 0.150 |
| Emotional Regulation | −.306 *** | −.460 *** | −.406 * | −.483 *** | 3.39 | 0.336 |
| Self-Reflection (Insight) | −.275 *** | −.233 * | −0.023 | −.267 * | 2.47 | 0.482 |
| Acceptance of Divergent Behaviors | −.345 *** | −.277 * | −.574 ** | −.252 * | 4.94 | 0.176 |
| Decisiveness | −.398 *** | −.470 *** | −0.315 | −.435 *** | 1.12 | 0.773 |
| Social Advising | −.372 *** | −.428 *** | −.455 ** | −.465 *** | 0.826 | 0.843 |
p = <.01;
p = <.001;
p = <.001
DISCUSSION
We compared the psychological constructs of loneliness and wisdom, and examined their relationships to relevant measures of physical and mental health, in middle-aged and oldest-old adults in Cilento, Italy and San Diego, California, USA. Loneliness did not differ across age or cultural groups after controlling for education. The same was true for SD-WISE scores except for the oldest-old adults in Cilento, Italy, who had lower scores than the other groups. Loneliness was negatively correlated with wisdom in both age groups in both Cilento and San Diego, with no significant differences among the four cohorts. Similarly, loneliness had an inverse correlation with general health, sleep quality, and happiness whereas the reverse was true for wisdom (except for the CIAO >90 group), with varying levels of significance. Thus, the overall validity of the two constructs was largely supported, with the specified exception.
Educational attainment and other indicators of socioeconomic status are consistently reported to be associated with access to collectively desired resources (Oakes)and with health and life outcomes in old age (Darin-Mattsson, Fors, & Kåreholt, 2017) (Several studies in older adults have highlighted significant associations of loneliness with lower educational attainment (Chen, Conwell, & Chiu, 2014; Cohen-Mansfield, Hazan, Lerman, & Shalom, 2016). In the Chicago Health, Aging, and Social Relations Study, Hispanic and Black participants were lonelier than White participants; however, high school education and household income explained a substantial portion of this race/ethnicity variance (L. C. Hawkley et al., 2008). After controlling for these variables (education, income), the racial/ethnic difference in loneliness was no longer significant). Similarly, several studies have shown a positive association between educational attainment and intelligence in youth and later life (Hegelund et al., 2020)). As noted earlier, intelligence is necessary but not sufficient for wisdom. Therefore, controlling for education may have some impact on associations with wisdom.
In the present study, educational levels differed significantly between the Cilento and San Diego samples. The CIAO cohorts had lower level of education than the SAGE cohorts. This could be related to the rural setting in Cilento in contrast to the urban/suburban setting in San Diego. The Cilento participants aged >90 had the smallest proportion of individuals who had obtained some college education. This difference in the years of formal education between the groups could reflect on possible impact of World War II on educational infrastructure in Italy (versus US) during the 1940s and 1950s. When we statistically controlled for education, group differences in loneliness and wisdom were no longer significant (except for wisdom in the oldest-old CIAO sample). Thus, differences in education level seemed to explain, at least partially, the observed reginal differences in loneliness and to a smaller extent, wisdom. However, caution is warranted in interpreting the results of statistical control, especially when the samples are unbalanced on that specific variable. Larger studies of Italian and US samples with comparable educational attainment are needed to confirm similarity in levels of loneliness and wisdom in the two populations.
One of our findings was that wisdom score was lower in oldest-old adults. The literature on the relationship between age and wisdom is surprisingly limited. There are no published longitudinal studies of changes in wisdom with aging, employing a validated rating scale of wisdom. Most research on wisdom and aging is based on cross-sectional comparisons of younger and older adults on specific wisdom-related ability areas. Early studies of wisdom, which focused on cognitive rather than emotional components of wisdom, reported that wisdom was not significantly related to age from 20 to 80 years (Staudinger, 1999). Above age 80, however, there was a negative relationship between age and wisdom, likely due to cognitive decline. However, the number of participants over age 80 was too small to draw firm conclusions. On the other hand, more recent studies have reported that several wisdom components are present at a higher level in older (ages 58 to 84) than in younger (ages 18 to 30) adults; these include decision making, pragmatic reasoning, theory of mind, and self-knowledge (Grossmann et al., 2020; Mickler & Staudinger, 2008; Worthy, Gorlick, Pacheco, Schnyer, & Maddox, 2011). There is clearly a need for longitudinal studies of wisdom across the adult lifespan, including the oldest-old adults.
Rather surprisingly, the oldest-old adults in Cilento had lower scores on SD-WISE total as well as several subscales than the other three groups. This finding suggests a potential cohort effect in this specific group and possible cultural variations involving differences in the fundamental pragmatics of current life in a rural environment in Cilento compared to the urban and suburban milieu in San Diego. We also need to consider the different personal narratives and values among the Cilento nonagenarians and centenarians (Scelzo et al., 2018), who had to weather economic depression and World War II, which did not directly involve most of the people in any of the other three cohorts. Other possibilities may relate to varied experience with participation in research protocols and responses to assessments of mental functioning. Finally, while the UCLA-3 and SD-WISE scales were translated and adapted in Italian, their validity in the context of Italy, specifically the rural communities of Cilento, remains unknown.
The inverse association between loneliness and wisdom is consistent with findings from our previous study of loneliness in adults across the lifespan (Ellen E. Lee et al., 2019). Extending the results from that prior study, we explored relationships between loneliness and specific components of wisdom. While loneliness levels were negatively correlated with most subscales of the SD-WISE in most of the subject groups, the effect sizes and levels of significance varied. Notably, the effect sizes were consistently in the medium to large range (from −.370 to −.606) for prosocial behaviors versus small (range from −.023 to −.275) for self-reflection.
The strong inverse association between loneliness and wisdom in all the four cohorts in our study suggests that wisdom may serve as a protective factor and a potential intervention against loneliness. However, this interpretation is limited by the cross-sectional nature of this study. Thus, an alternative explanation would be that loneliness prevents people from gaining wisdom. Considering the detrimental health implications of loneliness, the need for unique solutions is imperative. Unlike interventions that emphasize external factors such as facilitation of social interactions, interventions based on increasing wisdom may be focused internally on increasing components like pro-social behaviors which may positively impact the quality (and not necessarily the quantity) of social relationships. With increased empathy, lonely individuals may be more apt to recognize and process social and emotional cues relevant to social decision making.
As expected, loneliness was negatively correlated with happiness and sleep quality in most groups. Previous studies have also reported loneliness to be associated with lower levels of positive psychological traits/states, including optimism, resilience, and satisfaction with life, and lower levels of adverse mental states such as depression, anxiety, and sleep disturbances (Etezadi & Pushkar, 2013; Ellen E. Lee et al., 2019; Zebhauser et al., 2014). Although associated with mental health measures and self-rated general health, loneliness did not correlate with physical comorbidity or BMI, suggesting that physical health is impacted to a greater extent by other psychosocial or environmental factors.
Wisdom was associated with happiness (except in the CIAO ≥90 group) and better self-reported general health and sleep quality. Prior studies suggest that adaptive coping (problem-solving, positive reappraisal), sense of self-efficacy, and meaning in life may mediate the positive relationship between wisdom and positive affect (Etezadi & Pushkar, 2013). The lack of a significant association between wisdom and happiness in the CIAO >90 group may suggest that in this oldest-old, rural population, happiness is based on placing greater value on eudemonic than hedonic well-being and growth. This is consistent with our previous finding of a high level of religiosity in Cilento’s oldest-old (Scelzo et al., 2018). We did not assess religiosity or spirituality in the present study.
The present study compared two markedly different cultures – a rural region of southern Italy and an urban/suburban county in the US, both with different native languages and unique historical backgrounds. Yet, we found only quantitative differences in loneliness and wisdom between the two cultures, with similar associations of those constricts with each other and with other variables like health, sleep, and happiness (except for the CIAO >90 group). Therefore, we believe that the basic constructs of loneliness and wisdom appear to be similar across these cultures.
Strengths and Limitations
This investigation is, to our knowledge, the first comparison of loneliness and wisdom using validated rating scales in middle-aged and oldest-old adults from two different countries thousands of miles away from each other and with markedly different histories as well as native languages. Considering that the fastest growing segment of the modern western population is that of the oldest-old, it is important to examine nuances in positive and negative psychological states and traits in this subgroup of older adults. This study extends previous findings showing an inverse correlation between loneliness and wisdom, with an examination of the relationships of different components of wisdom with loneliness.
At the same time, the present study also has several limitations. As this was a cross-sectional study, no definitive causal interpretations can be made. While wisdom may serve as a protective factor against loneliness, it is also plausible that loneliness may limit a person’s ability to develop or enhance components of wisdom. Furthermore, our sample may be biased in that the oldest-old participants in this study were functional, capable of completing interviews or survey questionnaires. We should add, however, that these were not super-normal older adults as they had a number of comorbid medical conditions. Not surprisingly, the sample sizes were smaller for the oldest-old groups. Our Cilento and San Diego samples may not represent the general population in Italy or the US, respectively. The differences between the two sites may relate to other variations such as the fact that the Cilento sample was from a rural region unlike the more urban and suburban San Diego sample. Reflecting this, there was a large difference in the level of education, with a much greater proportion of the San Diego sample having had at least some college education than the Cilento participants. To address this issue, we re-ran the analyses after controlling for education. Our results may not generalize to non-Western cultures. All our measures were subjective and thus likely to include self-report bias. Finally, we did not have neurocognitive assessments.
Future work should examine the cultural equivalency of the UCLA-3 and SD-WISE in eastern cultures. Whereas western conceptualizations of wisdom place greater value on personal and hedonic well-being and growth, eastern interpretations of wisdom tend to emphasize eudemonic well-being and social judgment (Dilip V Jeste & Ipsit V Vahia, 2008; Takahashi & Bordia, 2000). Also, future clinical studies should be accompanied by an evaluation of objective measures of the behavioral constructs as well as relevant blood-based biomarkers of pathological processes like inflammation which underlie unhealthy aging. Similarly, functional neuroimaging studies may help shed light on the neurobiology of loneliness and wisdom.
Our study has implications for interventions to reduce loneliness by enhancing wisdom. Unlike interventions that emphasize external factors such as increasing social interactions to reduce objective social isolation, interventions aimed at reducing loneliness would be focused internally on increasing levels of components of wisdom. For example, with increased empathy, lonely individuals may become more apt to recognize and process social and emotional cues, thereby positively impacting the quality (and not necessarily the quantity) of social relationships. Lonely people may differ from one another in levels of different components of wisdom, even when their total scores on the wisdom scale are similar. Therefore, some people may need help in improving emotional regulation while others may require therapy to promote pro-social behaviors. Several randomized controlled trials have shown that behavioral interventions can increase components of wisdom like emotional regulation and pro-social behaviors (E. E. Lee et al., 2020) and even overall wisdom (Treichler et al., 2020).
CONCLUSION
Our cross-country study results largely support the validity of the constructs of loneliness and wisdom, and extend previous findings of a strong negative correlation between these two entities. Loneliness has become a modern behavioral pandemic contributing to worse physical, cognitive, and mental health as well as greater mortality (D. V. Jeste et al., 2020). While the cross-sectional nature of the present study prevents causal inferences, the notably consistent and highly significant inverse correlations between loneliness and wisdom in middle-aged and oldest-old people from two markedly different cultures suggest that wisdom may be a protective factor against loneliness. Furthermore, loneliness was consistently associated with poor general health, worse quality of sleep, and less happiness, whereas the reverse was generally true for wisdom.
Much of the literature on interventions for loneliness is limited by methodological shortcomings, and there is currently insufficient evidence to identify the most effective interventions for loneliness (National Academies of Sciences & Medicine, 2020). Therefore, multi-site randomized controlled trials of interventions to enhance wisdom should be conducted in efforts to reduce loneliness and promote healthy aging. Healthier aging with reduced loneliness may also lead to lower healthcare costs for older people. This will have important implications for clinical practice as well as healthcare policy. Routine assessment of loneliness with a validated brief measure and evidence-based wisdom-focused interventions for prevention and management of loneliness should become an integral part of geriatric clinical practice.
Supplementary Material
Acknowledgments
This work was supported, in part, by a grant from the Center for Healthy Aging and the Sam and Rose Stein Institute for Research on Aging at the University of California San Diego.
We are most thankful to the study participants and their family members. We also greatly appreciate the contributions of a number of physicians and staff members in Cilento, who did all the groundwork necessary. These include the following general practitioners who referred their patients to us for this study: Drs. Luigi Buonadonna, Enzo Passaro, Maria Rizzo, Giuseppe Scarano, Antonio Polcaro, Michelina De Cristofaro, and Luigi di Gregorio. We also would like to thank Drs. Serena Lucibello (psychologist), Vincenzo Pizza (neurologist), Rossella Marino, Silvia Navarin, Cristopher Bartoli (Cardiology assessment), Marianna Rizzo (nutritionist), and Giovanni D’Arena (laboratory tests), and Giuseppe Pastore (data collection and project management) as well as Drs. Andreas Bergmann, Lori D. Krummen, Frank Peacock, Ute Kilgor, and Gaetano Pacente.
We also want to thank other investigators from the UC San Diego team who are involved in this ongoing comprehensive study: Drs. Lori Daniels, Carol Franz, Mohit Jain, Anthony Molina, Tatiana Kisseleva, Rob Knight, William Kremen, and Robert Rissman.
We also appreciate help for this study from several UC San Diego Stein Institute staff members, especially Paula Smith.
Footnotes
Conflicts of interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this report.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- Achenbaum WA, & Orwoll L (1991). Becoming wise: A psycho-gerontological interpretation of the book of Job. The International Journal of Aging & Human Development, 32(1), 21–39. [DOI] [PubMed] [Google Scholar]
- Abdellaoui A, Sanchez-Roige S, Sealock J, Treur JL, Dennis J, Fontanillas P, … Boomsma DI (2019). Phenome-wide investigation of health outcomes associated with genetic predisposition to loneliness. Hum Mol Genet, 28(22), 3853–3865. doi: 10.1093/hmg/ddz219 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Achenbaum WA, & Orwoll L (1991). Becoming Wise: A Psycho-Gerontological Interpretation of the Book of Job. The International Journal of Aging and Human Development, 32(1), 21–39. doi: 10.2190/419r-x8fc-q6ne-0m85 [DOI] [PubMed] [Google Scholar]
- Anderson GO, & Thayer CE (2018). Loneliness and social connections: A national survey of adults 45 and older. Washington, DC: AARP Foundation [Google Scholar]
- Ardelt M (1997). Wisdom and Life Satisfaction in Old Age. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 52B(1), P15–P27. doi: 10.1093/geronb/52b.1.p15 [DOI] [PubMed] [Google Scholar]
- Ardelt M (2000). Antecedents and effects of wisdom in old age: A longitudinal perspective on aging well. Research on Aging, 22(4), 360–394. doi: 10.1177/0164027500224003 [DOI] [Google Scholar]
- Cacioppo JT, Hawkley LC, Berntson GG, Ernst JM, Gibbs AC, Stickgold R, & Hobson JA (2002). Do lonely days invade the nights? Potential social modulation of sleep efficiency. Psychol Sci, 13(4), 384–387. doi: 10.1111/1467-9280.00469 [DOI] [PubMed] [Google Scholar]
- Cacioppo JT, Hawkley LC, Crawford LE, Ernst JM, Burleson MH, Kowalewski RB, … Berntson GG (2002). Loneliness and health: potential mechanisms. Psychosom Med, 64(3), 407–417 [DOI] [PubMed] [Google Scholar]
- Cacioppo S, Capitanio JP, & Cacioppo JT (2014). Toward a neurology of loneliness. Psychol Bull, 140(6), 1464–1504. doi: 10.1037/a0037618 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cella D, Riley W, Stone A, Rothrock N, Reeve B, Yount S, … Group PC (2010). The Patient-Reported Outcomes Measurement Information System (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005–2008. Journal of clinical epidemiology, 63(11), 1179–1194. doi: 10.1016/j.jclinepi.2010.04.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen S, Conwell Y, & Chiu HFK (2014). Loneliness and aging in China-a public health problem in need of solutions. International psychogeriatrics, 26(11), 1771. [DOI] [PubMed] [Google Scholar]
- Clayton VP, & Birren JE (1980). The development of wisdom across the life span: A reexamination of an ancient topic. Life-span development and behavior, 3, 103–135 [Google Scholar]
- Cohen-Mansfield J, Hazan H, Lerman Y, & Shalom V (2016). Correlates and predictors of loneliness in older-adults: a review of quantitative results informed by qualitative insights. Int Psychogeriatr, 28(4), 557–576. doi: 10.1017/s1041610215001532 [DOI] [PubMed] [Google Scholar]
- Dahlberg L, Andersson L, McKee KJ, & Lennartsson C (2015). Predictors of loneliness among older women and men in Sweden: A national longitudinal study. Aging & mental health, 19(5), 409–417 [DOI] [PubMed] [Google Scholar]
- Daniels LB, Antonini P, Marino R, Rizzo M, Navarin S, Lucibello SG, … Di Somma S (2019). Cardiovascular health of nonagenarians in southern Italy: a cross-sectional, home-based pilot study of longevity. J Cardiovasc Med (Hagerstown). doi: 10.2459/JCM.0000000000000910 [DOI] [PubMed] [Google Scholar]
- Darin-Mattsson A, Fors S, & Kåreholt I (2017). Different indicators of socioeconomic status and their relative importance as determinants of health in old age. International Journal for Equity in Health, 16(1). doi: 10.1186/s12939-017-0670-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Etezadi S, & Pushkar D (2013). Why are Wise People Happier? An Explanatory Model of Wisdom and Emotional Well-Being in Older Adults. Journal of Happiness Studies, 14(3), 929–950. doi: 10.1007/s10902-012-9362-2 [DOI] [Google Scholar]
- Fried L, Prohaska T, Burholt V, Burns A, Golden J, Hawkley L, … Victor C (2020). A unified approach to loneliness. The Lancet, 395(10218), 114. doi: 10.1016/s0140-6736(19)32533-4 [DOI] [PubMed] [Google Scholar]
- Grossmann I, Weststrate NM, Ferrari M, & Brienza JP (2020). A Common Model Is Essential for a Cumulative Science of Wisdom. Psychological Inquiry, 31(2), 185–194. doi: 10.1080/1047840x.2020.1750920 [DOI] [Google Scholar]
- Hawkley LC, & Cacioppo JT (2007). Aging and loneliness: Downhill quickly? Current Directions in Psychological Science, 16(4), 187–191. doi: 10.1111/j.1467-8721.2007.00501.x [DOI] [Google Scholar]
- Hawkley LC, & Cacioppo JT (2010). Loneliness matters: a theoretical and empirical review of consequences and mechanisms. Ann Behav Med, 40(2), 218–227. doi: 10.1007/s12160-010-9210-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hawkley LC, Hughes ME, Waite LJ, Masi CM, Thisted RA, & Cacioppo JT (2008). From social structural factors to perceptions of relationship quality and loneliness: the Chicago health, aging, and social relations study. J Gerontol B Psychol Sci Soc Sci, 63(6), S375–384 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hawkley LC, Hughes ME, Waite LJ, Masi CM, Thisted RA, & Cacioppo JT (2008). From social structural factors to perceptions of relationship quality and loneliness: the Chicago health, aging, and social relations study. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 63(6), S375–S384 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hegelund ER, Grønkjær M, Osler M, Dammeyer J, Flensborg-Madsen T, & Mortensen EL (2020). The influence of educational attainment on intelligence. Intelligence, 78, 101419. doi: 10.1016/j.intell.2019.101419 [DOI] [Google Scholar]
- Holm S (1979). A Simple Sequentially Rejective Multiple Test Procedure. Scandinavian Journal of Statistics, 6(2), 65–70 [Google Scholar]
- Holt-Lunstad J (2017). The potential public health relevance of social isolation and loneliness: Prevalence, epidemiology, and risk factors. Public Policy & Aging Report, 27(4), 127–130 [Google Scholar]
- Jeste DV, Ardelt M, Blazer D, Kraemer HC, Vaillant G, & Meeks TW (2010). Expert consensus on characteristics of wisdom: A Delphi method study. The Gerontologist, 50(5), 668–680 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jeste DV, & Lee EE (2019). The Emerging Empirical Science of Wisdom: Definition, Measurement, Neurobiology, Longevity, and Interventions. Harvard review of psychiatry, 27(3), 127–140 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jeste DV, Lee EE, & Cacioppo S (2020). Battling the Modern Behavioral Epidemic of Loneliness: Suggestions for Research and Interventions. JAMA Psychiatry. doi: 10.1001/jamapsychiatry.2020.0027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jeste DV, Lee EE, Palmer BW, & Treichler EBH (2020). Moving from Humanities to Sciences: A New Model of Wisdom Fortified by Sciences of Neurobiology, Medicine, and Evolution. Psychological Inquiry, 31(2), 134–143. doi: 10.1080/1047840x.2020.1757984 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jeste DV, Savla GN, Thompson WK, Vahia IV, Glorioso DK, Martin AS, … Depp CA (2013). Association between older age and more successful aging: critical role of resilience and depression. Am J Psychiatry, 170(2), 188–196. doi: 10.1176/appi.ajp.2012.12030386 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jeste DV, Savla GN, Thompson WK, Vahia IV, Glorioso DK, Martin A. v. S., … Kraemer HC (2013). Association between older age and more successful aging: critical role of resilience and depression. American Journal of Psychiatry, 170(2), 188–196 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jeste DV, & Vahia IV (2008). Comparison of the conceptualization of wisdom in ancient Indian literature with modern views: Focus on the Bhagavad Gita. Psychiatry: Interpersonal and Biological Processes, 71(3), 197–209 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jeste DV, & Vahia IV (2008). Comparison of the conceptualization of wisdom in ancient Indian literature with modern views: focus on the Bhagavad Gita. Psychiatry, 71(3), 197–209. doi: 10.1521/psyc.2008.71.3.197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keys A, & Keys M (1959). Eat Well and Stay Well. New York: Doubleday. [Google Scholar]
- Kristensen K, König HH, & Hajek A (2019). The longitudinal association of multimorbidity on loneliness and network size: Findings from a population‐based study. International journal of geriatric psychiatry, 34(10), 1490–1497 [DOI] [PubMed] [Google Scholar]
- Lasgaard M (2007). Reliability and validity of the Danish version of the UCLA Loneliness Scale. Personality and Individual Differences, 42(7), 1359–1366 [Google Scholar]
- Lee EE, Bangen KJ, Avanzino JA, Hou B, Ramsey M, Eglit G, … Jeste DV (2020). Outcomes of Randomized Clinical Trials of Interventions to Enhance Social, Emotional, and Spiritual Components of Wisdom: A Systematic Review and Meta-analysis. JAMA Psychiatry. doi: 10.1001/jamapsychiatry.2020.0821 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee EE, Depp C, Palmer BW, Glorioso D, Daly R, Liu J, … Jeste DV (2019). High prevalence and adverse health effects of loneliness in community-dwelling adults across the lifespan: role of wisdom as a protective factor. International Psychogeriatrics, 31(10), 1447–1462. doi: 10.1017/S1041610218002120 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGregor J (2017, October 4, 2017). This former surgeon general says there’s a ‘loneliness epidemic’ and work is partly to blame, Washington Post. Retrieved from https://www.washingtonpost.com/news/on-leadership/wp/2017/10/04/this-former-surgeon-general-says-theres-a-loneliness-epidemic-and-work-is-partly-to-blame/?utm_term=.f33381010716 [Google Scholar]
- Meeks TW, & Jeste DV (2009). Neurobiology of wisdom: a literature overview. Arch Gen Psychiatry, 66(4), 355–365. doi: 10.1001/archgenpsychiatry.2009.8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mickler C, & Staudinger UM (2008). Personal wisdom: Validation and age-related differences of a performance measure. Psychology and aging, 23(4), 787. [DOI] [PubMed] [Google Scholar]
- Morlett Paredes A, Lee EE, Chik L, Gupta S, Palmer BW, Palinkas LA, … Jeste DV (2019). Qualitative study of loneliness in a senior housing community: the importance of wisdom and other coping strategies. Aging & Mental Health, 1–8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Academies of Sciences, E., & Medicine. (2020). Social Isolation and Loneliness in Older Adults: Opportunities for the Health Care System. Washington, DC: The National Academies Press. [PubMed] [Google Scholar]
- Oakes M Measuring Socioeconomic StatusThe Authority on Behavioral & Social Science Research: Office of Behavioral and Social Sciences Research. Retrieved from http://www.esourceresearch.org/Portals/0/Uploads/Documents/Public/Oakes_FullChapter.pdf.
- Peplau LA (1982). Loneliness: A sourcebook of current theory, research, and therapy (Vol. 36): John Wiley & Sons Inc. [Google Scholar]
- Pizza V, Antonini P, Marino R, D’Arena G, Lucibello SG, Rizzo M, … Di Somma S (2020). Cognitive Health of Nonagenarians in Southern Italy: A Descriptive Analysis from a Cross-Sectional, Home-Based Pilot Study of Exceptional Longevity (Cilento Initiative on Aging Outcomes or CIAO). Medicina, 56(5), 218. doi: 10.3390/medicina56050218 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Radloff LS (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied psychological measurement, 1(3), 385–401 [Google Scholar]
- Russell DW (1996). UCLA Loneliness Scale (Version 3): reliability, validity, and factor structure. J Pers Assess, 66(1), 20–40. doi: 10.1207/s15327752jpa6601_2 [DOI] [PubMed] [Google Scholar]
- Scelzo A, Di Somma S, Antonini P, Montross LP, Schork N, Brenner D, & Jeste DV (2018). Mixed-methods quantitative-qualitative study of 29 nonagenarians and centenarians in rural Southern Italy: focus on positive psychological traits. Int Psychogeriatr, 30(1), 31–38. doi: 10.1017/S1041610217002721 [DOI] [PubMed] [Google Scholar]
- Shiovitz-Ezra S, & Ayalon L (2010). Situational versus chronic loneliness as risk factors for all-cause mortality. Int Psychogeriatr, 22(3), 455–462. doi: 10.1017/s1041610209991426 [DOI] [PubMed] [Google Scholar]
- Smith J, & Baltes PB (1990). Wisdom-related knowledge: Age/cohort differences in response to life-planning problems. Developmental Psychology, 26(3), 494–505. doi: 10.1037/0012-1649.26.3.494 [DOI] [Google Scholar]
- Staudinger UM (1999). Older and wiser? Integrating results on the relationship between age and wisdom-related performance. International Journal of Behavioral Development, 23(3), 641–664 [Google Scholar]
- Sternberg RJ (1990). Wisdom: Its nature, origins and development. New York: Cambridge University Press. [Google Scholar]
- Sternberg RJ, & Jordan J (2005). A handbook of wisdom: Psychological perspectives. New York: Cambridge University Press. [Google Scholar]
- Takahashi M, & Bordia P (2000). The Concept of Wisdom: A Cross-cultural Comparison. International Journal of Psychology, 35(1), 1–9. doi: 10.1080/002075900399475 [DOI] [Google Scholar]
- Tang W, He H, & Tu X (2012). Applied categorical and count data analysis: Chapman and Hall/CRC. [Google Scholar]
- Thomas ML, Bangen KJ, Palmer BW, Sirkin Martin A, Avanzino JA, Depp CA, … Jeste DV (2019). A new scale for assessing wisdom based on common domains and a neurobiological model: The San Diego Wisdom Scale (SD-WISE). J Psychiatr Res, 108, 40–47. doi: 10.1016/j.jpsychires.2017.09.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thomas ML, Kaufmann CN, Palmer BW, Depp CA, Martin AS, Glorioso DK, … Jeste DV (2016). Paradoxical Trend for Improvement in Mental Health With Aging: A Community-Based Study of 1,546 Adults Aged 21–100 Years. J Clin Psychiatry, 77(8), e1019–1025. doi: 10.4088/JCP.16m10671 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thomas ML, Kaufmann CN, Palmer BW, Depp CA, Martin AS, Glorioso DK, … Jeste DV (2016). Paradoxical trend for improvement in mental health with aging: a community-based study of 1,546 adults aged 21–100 years. The Journal of clinical psychiatry, 77(8), e1019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thurston RC, & Kubzansky LD (2009). Women, loneliness, and incident coronary heart disease. Psychosom Med, 71(8), 836–842. doi: 10.1097/PSY.0b013e3181b40efc [DOI] [PMC free article] [PubMed] [Google Scholar]
- Treichler EBH, Glorioso D, Lee EE, Wu TC, Tu XM, Daly R, … Jeste DV (2020). A pragmatic trial of a group intervention in senior housing communities to increase resilience. Int Psychogeriatr, 32(2), 173–182. doi: 10.1017/s1041610219002096 [DOI] [PMC free article] [PubMed] [Google Scholar]
- United Nations Department of Economic and Social Affairs, P. D. (2019). World Population Prospects 2019: Highlights (ST/ESA/SER.A/423). http://esa.un.org/unpd/wpp/index.htm. [Google Scholar]
- Vassar M, & Crosby JW (2008). A reliability generalization study of coefficient alpha for the UCLA Loneliness Scale. Journal of Personality Assessment, 90(6), 601–607 [DOI] [PubMed] [Google Scholar]
- Wang H, Peng J, Wang B, Lu XL, Zheng JZ, Wang K, … Feng C (2017). Inconsistency between univariate and multiple logistic regressions. Shanghai archives of psychiatry, 29(2), 124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ware JE Jr., & Sherbourne CD (1992). The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care, 30(6), 473–483 [PubMed] [Google Scholar]
- Weiss RS (1973). Loneliness: The experience of emotional and social isolation: The MIT Press, Cambridge, MA. [Google Scholar]
- Wilson RS, Krueger KR, Arnold SE, Schneider JA, Kelly JF, Barnes LL, … Bennett DA (2007). Loneliness and risk of Alzheimer disease. Arch Gen Psychiatry, 64(2), 234–240. doi: 10.1001/archpsyc.64.2.234 [DOI] [PubMed] [Google Scholar]
- Worthy DA, Gorlick MA, Pacheco JL, Schnyer DM, & Maddox WT (2011). With age comes wisdom: Decision making in younger and older adults. Psychological science, 22(11), 1375–1380 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zebhauser A, Hofmann-Xu L, Baumert J, Häfner S, Lacruz ME, Emeny RT, … Ladwig KH (2014). How much does it hurt to be lonely? Mental and physical differences between older men and women in the KORA-Age Study. International Journal of Geriatric Psychiatry, 29(3), 245–252. doi: 10.1002/gps.3998 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.