

Abstract
The peripheral retina is affected in a variety of retinal disorders. Traditional fundus cameras capture only a part of the fundus even when montaging techniques are used. Ultra-wide field imaging enables us to delve into the retinal periphery in greater detail. It not only facilitates assessing color images of the fundus, but also fluorescein angiography, indocyanine green angiography, fundus autofluorescence, and red and green free images. In this review, a literature search using the keywords “ultra-widefield imaging”, “widefield imaging”, and “peripheral retinal imaging” in English and non-English languages was done and the relevant articles were included. Ultra-wide field imaging has made new observations in the normal population as well as in eyes with retinal disorders including vascular diseases, degenerative diseases, uveitis, age-related macular degeneration, retinal and choroidal tumors and hereditary retinal dystrophies. This review aims to describe the utility of ultra-wide field imaging in various retinal disorders.
Keywords: Retinal imaging, retinal disorders, Ultra-widefield, UWF autofluorescence, UWF fluorescein angiography, UWF Indocyanine angiography
The periphery of the retina is affected in a variety of retinal and choroidal disorders. Until now, traditional fundus cameras captured only 30-50° of retina and the peripheral retina remained undocumented. Documentation is important not only for management, monitoring and follow-up of the retinal diseases, but also serves an irreplaceable role in medical teaching, patient education and counselling. The role of documentation in the modern medico-legal and telemedicine era becomes even more critical.
While most of the peripheral retina can be assessed with good clinical examination and indirect ophthalmoscopy (especially by an experienced observer), documentation remains difficult. Color retinal charts remain reasonable preference but are flawed by inter-observer variability and drawing capabilities. Moreover, quantification remains a major problem. Diabetic retinopathy study (DRS) made the first attempt to capture more retinal area, by making a montage of 7 standard 30-degree fields.[1] This could capture up to 75 degrees of retina. The montaging techniques, however, depend upon good patient cooperation, fixation stability, and are time -consuming. In addition, peripheral optical phenomena and artifacts affect imaging. Several wide field imaging systems including RetCam (Clarity Medical Systems Inc, USA), Spectralis (Spectralis, Heidelberg Inc, Germany) with non-contact or contact lens and Clarus (Clarus 500, Zeiss Inc, Germany) have been developed since then. However, many of these (Retcam and Spectralis) involve direct contact with the patient and are cumbersome and uncomfortable for the capturing technician as well. Clarus does not require contact and provides true colour wide field images of up to 133°. Mirante (Nidek Inc. Japan) was introduced recently in 2019 with options of multimodal imaging and a view of 163°.
Optos (Optos Inc, Dunfermline, UK), an ultra-wide field (UWF) imaging system, allows capture of 200 degrees of retina (approximately 82% of retinal surface area) in a single click. It provides non-contact, high-resolution images of retina quickly even through a small pupil using an ellipsoid mirror and virtual point technology. Optos is based on confocal scanning laser ophthalmoscope and uses red (633 nm) and green (532 nm) lasers for color images, blue laser (488 nm) for fundus fluorescein angiography (FFA), green laser for fundus autofluorescence (FAF), and infrared laser (802 nm) for indocyanine green angiography (ICGA). In this review, we will discuss the utility of UWF imaging in various retinal and choroidal disorders.
Literature Search
A literature search including Medline, PubMed and Scopus was performed using the keywords “ultra-widefield imaging”, “widefield imaging”, and “peripheral retinal imaging” in English and non-English languages. All longitudinal studies, retrospective, prospective and case reports published before April 2020 where ultra-widefield was used as one of the methods of examination were included. Cited studies not identified through these sources were identified by reviewing the reference list in individual articles.
Ultra-Wide Field Imaging
Wide field and ultra-wide field imaging have been used interchangeably in literature without clear definitions. The Diabetic Retinopathy Clinical Research Network (DRCR.net) defined UWF images to have at least a 100° view of the fundus.[2] Recently, a consensus of experts in the field established that the term wide field should be used for images showing retinal features beyond the posterior pole but posterior to vortex vein ampulla in all four quadrants, while UWF should be restricted to images in a single capture showing retinal features anterior to vortex vein ampullae in all four quadrants.[3] An image which can detail ora to ora in 360 degrees, is termed “Panretinal”. Though montaging techniques with Optos can produce panretinal images, no device as of now can capture such an image in a single click.
UWF Imaging in normal retina
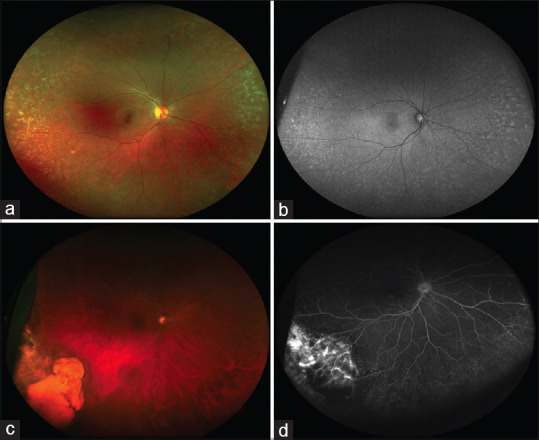
An adequate understanding of the normal retinal periphery especially on FFA is a prerequisite with increasing usage of UWF imaging. A study on UWF-FFA in normal eyes,[4] found common peripheral abnormalities such as absence of capillary details (98.28%), ground glass hyperfluorescence (87.93%), terminal networks (77.59%), drusen (34.48%), and microaneurysms (41.38%) [Fig. 1a and b]. Also, peripheral arterial circulation did not respect horizontal watershed in approximately 45% of eyes. Lu et al.[5] demonstrated granular background hyperfluorescence (with features of window defect) in the periphery of all 101 normal eyes and attributed it to decreased retinal pigment epithelium density in the periphery. Thus, several findings which were considered to be abnormal for decades are in fact found in the periphery of normal individuals as well.
Figure 1.
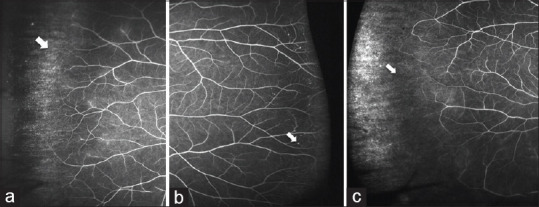
UWF-FFA of normal peripheral retina showing absence of capillary details, ground glass hyperfluorescence (arrow, a) and peripheral microaneurysms (arrow, b). In the setting of high myopia, UWF-FFA shows peripheral avascular retina (white arrow, c)
Singer et al.[6] studied mean distance from the center of optic disc to the peripheral vascular border using UWF-FFA after correcting for peripheral distortion. They found that this distance differed depending on the quadrant, with temporal (22.5 mm) being largest followed by inferior (20.4 mm), superior (19.2 mm) and nasal (17.4 mm) being the least. The distances to the perfused vascular borders were significantly shorter in elderly population more than 60 years of age. Similarly, areas of non-perfusion and retinal capillary microaneurysms in retinal periphery have been noted commonly in eyes with pathologic myopia [Fig. 1c].[7] Ability of UWF imaging to detect peripheral lesions even without mydriasis makes it useful for health screening because of its convenience and rapid acquisition.[8] But these findings in periphery of normal eyes should be kept in mind while interpreting the results of UWF-FFA.
UWF Imaging in retinal detachment (RD)
UWF imaging is a valuable adjunct for eyes with RD especially for documenting the extent of RD, proliferative vitreoretinopathy and changes occurring in retina before and after surgery [Fig. 2a-f].[9] The UWF imaging also allows accurate and reproducible assessment of peripheral breaks when compared with indirect ophthalmoscopy.[10] Thus, it not only helps in the documentation of peripheral lesions but acts as a good teaching tool [Fig. 2c].[11] It is useful for visualization in difficult situations like gas-filled eyes [Fig. 2b],[12] high myopia,[13] eyes with Boston Keratoprosthesis,[14] and hazy media[15] as well. However, one of the major problems is poor visualization of superior and inferior periphery, which can be partially overcome with steered images.
Figure 2.

UWF pseudocolour image showing rhegmatogenous retinal detachment with superior 180° giant retinal tear (arrow, a). Postoperative UWF image of the same eye with giant retinal tear showing gas-filled eye and attached retina (b). Old rhegmatogenous retinal detachment showing demarcation lines and intraretinal cyst (arrow, c) and subretinal bands (arrow, d). UWF image of an eye after scleral buckling showing infero-temporal cryo scar (arrow, e); re-detachment with extensive PVR changes following vitreoretinal surgery with silicone oil (f)
In a retrospective study, Wilmer et al. found that UWF-FAF permits demarcation of extent of RD and also aids in postoperative counseling.[16] A hyperautofluorescent leading edge may be seen in eyes with RD indicating shallow subretinal fluid. Additionally, postoperative granular changes on FAF indicated worse visual outcomes and possible functional deficits in certain eyes.[16] While UWF-FAF in eyes undergoing scleral buckling surgery revealed that the desired amount of cryopexy lead to central hypoautofluorescence with surrounding hyperautofluorescent halo,[17] UWF-FFA has revealed peripheral vascular changes like perivascular staining, capillary nonperfusion (CNP) areas, vascular tortuosity in eyes with RD that has helped us in understanding the pathophysiology of disease.[18]
UWF Imaging in diabetic retinopathy (DR)
Traditionally, the management of diabetic retinopathy (DR) has relied solely on the standard retinal imaging exploring the changes in the posterior pole [Fig. 3a].[19] It is now known that peripheral retinal abnormalities are equally notable in DR [Fig. 3b-d][20] and hence, the visualization of the peripheral retina becomes vital.
Figure 3.
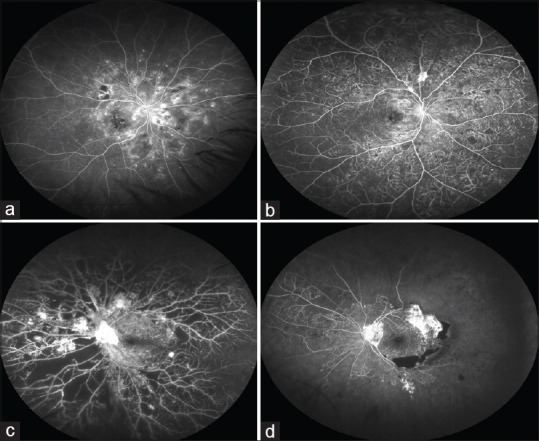
UWF-FFA in diabetic retinopathy showing predominantly posterior pole involvement (a) and panretinal involvement (b) with microaneurysm and vascular changes extending beyond posterior pole, NVEs are also seen along supero-temporal vascular arcade (b). UWF-FFA of proliferative diabetic retinopathy showing large NVD and multiple NVEs with extensive capillary non-perfusion areas (c) and almost total capillary drop out (d)
Screening and diagnosis of DR: UWF imaging improves the detection of DR lesions and leads to precise grading of DR. Additional cases of DR may be detected with UWF imaging as compared to the standard imaging.[21] Moreover, compared to the ETDRS seven-field images, UWF imaging detects a higher retinopathy level in around 10-15% of cases.[21,22,23] Not only UWF-FFA detects greater number of neovascularization and CNPs, but the UWF color images alone can improve the detection rates of peripheral neovascularization as well.[23] Rasmussen et al.[24] reported that the non-mydriatic UWF images had one-level-agreement of 100% with the mydriatic images and thus we may not always require mydriasis. This is important in diabetic patients who tend to have poor pupillary dilation and difficult image acquisition with traditional fundus photography.
Monitoring of DR: Silva et al.[20] introduced the concept of predominantly peripheral lesions (PPLs) in DR. When more than 50% of the graded lesions of DR occur in periphery (outside of ETDRS seven-field area), it is termed predominantly peripheral disease. The likelihood of DR progression and development of proliferative DR is greater in eyes with PPLs.[20] Also, UWF imaging helps in predicting the risk of post-vitrectomy bleed which tends to be higher in eyes with greater peripheral lesions.[25]
UWF imaging also helps in a better understanding of pathogenesis of diabetic macular edema (DME). Increased vitreous vascular endothelial growth factor (VEGF) levels from capillary drop-out and retinal ischemia have been found to be responsible for macular edema.[26] However, controversy regarding the role of peripheral CNP detected on UWF-FFA in the development and progression of DME continues.[27,28,29,30,31] While some studies report greater correlation between peripheral ischemia and DME,[27,29] others report increased risk of developing neovascularization but not DME with peripheral CNPs.[28,30,31] Future research may help to further elucidate the role of PPLs in the occurrence of DME and the type of DME.
Treatment of DR: UWF imaging allows precise application of targeted retinal photocoagulation (TRP) to peripheral CNPs [Fig. 3c and d], which keeps the side effects of laser to minimum by avoiding destruction of the perfused retina. Muqit et al.[32] compared TRP with standard pan-retinal photocoagulation (PRP) and found similar rates of proliferative DR regression but significant reduction in central retinal edema with TRP.
Role in telemedicine: UWF imaging has found utility in telemedicine programs for DR screening because of greater speed of acquisition and patient comfort.[22] Although UWF images are better than ETDRS seven-field images in terms of DR detection and gradeability, UWF imaging has only moderate agreement and lower gradeability rates than dilated fundus examination.[33]
UWF imaging in venous occlusions
UWF-FFA is important for accurate assessment of CNP areas in the setting of retinal vein occlusions (RVO, Fig. 4a-d).[34] Underassessment of peripheral CNP areas may lead to under-treatment resulting in unwanted sequelae like recurring/persistent macular edema, vitreous hemorrhage, and progression to neovascular glaucoma.
Figure 4.
UWF pseudocolour image (a) of CRVO along with inferotemporal BRVO showing dilated tortuous veins, 360° resolving hemorrhages and prominent inferotemporal area of intra-retinal hemorrhages. UWF-FFA in CRVO (b) and BRVO (c) showing panretinal and sectoral vessel wall staining (arrows) and capillary non-perfusion (CNP) areas extending up to retinal periphery. UWF-FFA in old BRVO (d) showing peripheral laser spots, large areas of uncovered CNP and collateral formation (red arrow) at junction of vascularized and non-vascularized retina
Method of assessing CNP: Two methods have been described to quantify CNPs in RVOs, one being ischemic index, while the other is anatomical extent (in mm2).[35,36] Ischemic index is the ratio of the number of pixels within the CNP to the total number of pixels in the visible retina. This index may vary from 0.1 to 61.3% in branch retinal vein occlusion (BRVO) and from zero to 99% in central retinal vein occlusion (CRVO).[34,35] Using the second method, Tan et al.[36] found that the area of non-perfusion was significantly larger in patients with CRVO (mean 135.8 mm2, range 5.3–365.4) compared to BRVO (mean 67.3 mm2, range 0–224.3). Total area of non-perfusion in this cohort of patients ranged from 0 to 365.4 mm2, with a mean of 95.1 mm2. This was equivalent to a mean of nearly 37 disc areas, with largest being 141 disc areas. These numbers of CNP areas are far in excess of previous landmark studies, thus, substantiating the role of UWF angiography.[37,38]
Management of CNP: The area of CNP has a bearing on the risk of neovascularization and macular edema. While one study[35] found higher ischemic index (75%) in patients with neovascularization as compared to ones without neovascularization (6%), others have reported higher retinal thickness in eyes with more CNPs.[34,39] Prasad et al.[40] showed that the areas of CNP anterior to equator, which remain undetected on conventional imaging had greater bearing on macular edema. The WAVE study concluded that the change in ischemic index for the total retina, peri-macular and near-peripheral retinal regions positively correlated with the change in CMT.[41] These findings led to the concept of TRP in RVO.[42] TRP leads to lesser chance of macular edema and decreases required number of anti-VEGF injections.[43,44]
UWF imaging in pediatric disorders
UWF imaging has an important role in pediatric diseases like Coats‘ disease, Familial exudative vitreoretinoapthy (FEVR) and retinopathy of prematurity (ROP) as primary pathology in these diseases lies in the retinal periphery. Capture of a large area in a single click is even more useful in children where patient cooperation is an issue.
UWF imaging has been used extensively in the evaluation and management of Coats disease.[45,46,47] UWF-FFA allows better visualization of telangiectatic vessels, light bulb aneurysms, early and progressive perivascular leak, and peripheral CNP, which helps greatly in management [Fig. 5a-c]. Kang et al.[45] showed areas of retinal telangiectasia and non-perfusion, much wider on UWF angiography than the 7-standard fields. This aided in assessment of the areas requiring treatment especially on UWF-FFA. Further, laser photocoagulation of these lesions resulted in better reduction in exudation and macular edema. UWF-FFA can be used in younger children without sedation as an outpatient modality.[46] Subtle vascular changes in the contralateral asymptomatic eyes of patients with Coats‘ disease could be detected using UWF imaging.[47] These findings point towards Coats‘ disease being an asymmetric bilateral disease. Also, avascular periphery anterior to telangiectasia is noted in eyes with adult-onset Coats disease.[48] This ischemic area is the source of continuous VEGF production and maybe the reason for appearance of new lesions over time.
Figure 5.

UWF pseudocolor image of Coat‘s disease showing peripheral avascular area and retinal neovascularization (a) UWF- FFA showing bulb like dilatations in addition (b). UWF-FFA of another case showing wide-spread involvement in Coat‘s disease (c). UWF image in familial exudative vitreoretinopathy (FEVR) showing retinal fold, peripheral tractional retinal detachment and disc-macula drag (d). UWF-FFA in FEVR shows temporal avascular retina, temporal straightening of vessels and super-numerary vascular branching in addition to early (e) and frank neovascularization (f)
Likewise, UWF imaging is beneficial in diagnosing the early stages of FEVR, especially in the asymptomatic fellow eye [Fig. 5d-f]. In comparison to standard fluorescein angiography, the UWF-FFA is highly effective in diagnosing FEVR in asymptomatic family members of diagnosed FEVR patients with a sensitivity and specificity of 93.0% and 97.5%, respectively.[49] Kashani et al.[50] described previously unrecognized anatomic and functional changes in FEVR using UWF-FFA. Anatomic changes included aberrant circumferential peripheral vessels, vascular tortuosity, late-phase disc leakage, central and peripheral telangiectasias and capillary anomalies. Functional changes included venous-venous shunting, delayed arteriovenous transit, and delayed or absent choroidal perfusion.
For ROP screening, traditionally binocular indirect ophthalmoscopy has been considered the gold standard. However, the scarcity of retina specialists with adequate skills to screen these premature babies with indirect ophthalmoscope has been a limitation.[51] Telemedicine model for ROP screening has been validated in large studies in both the developed and developing world.[52,53] Most of these studies, however, use the RetCam shuttle (with 130°coverage, Natus Medical Incorporated, Pleasanton, CA) handled by a trained nurse/technician who captures the images and uploads them to a secure server. UWF imaging using Optos has also been used with variable success for imaging ROP babies using the ‘flying baby position‘.[54] The latter has advantages like being non-contact, no need for pupillary dilatation (useful in plus disease), and better view of the different stages of ROP at the posterior pole and peripheral retina simultaneously.[54]
UWF imaging in uveitis
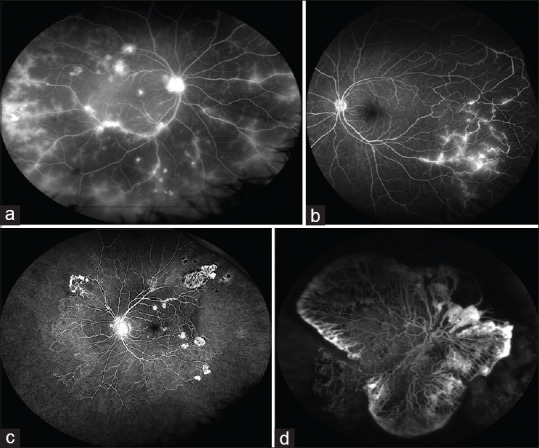
UWF imaging may be useful to make a correct diagnosis, determine the extent of involvement, identify secondary complications such as retinal detachment, and for follow-up to look for recurrence of activity in cases of uveitis [Fig. 6a-f]. Considering, patients with uveitis often develop posterior synechiae leading to poorly dilating pupils, UWF imaging may be very helpful in such cases.
Figure 6.

UWF pseudocolor image of VKH syndrome showing multiple neurosensory detachments (a). UWF-FFA showed multiple pin point leaks (b) which pool in the late phases (c) extending up to the periphery. UWF image of cytomegalovirus retinitis showing peripheral involvement (d); Multifocal choroiditis (e) showing areas of active as well as healed patches. Ocular Toxocariasis showing peripheral granuloma with falciform fold extending from the lesion to posterior pole (f)
Anterior uveitis: Retinal involvement can occur in anterior uveitis in the form of peripheral vascular leakage (PVL) and cystoid macular edema (CME). Chi et al.[55] found PVL in 42% and CME in 26% eyes with anterior uveitis. PVL has also been demonstrated in cases of mild anterior uveitis associated with tubulointerstitial nephritis.[56] The presence of peripheral leakage indicates that inflammatory mediators involved in anterior uveitis may also have some effect on peripheral retinal vessels. However, whether this mandate a change in treatment algorithm needs to be evaluated further.
Intermediate uveitis (IU) and vitreous haze: Different patterns of periphlebitis such as large or small vessel staining/leakage have been described in IU using UWF-FFA.[57] Diffuse leakage has been correlated with worse visual acuity as compared to peripheral leakage or absence of leakage.[58] More PVL has been reported using UWF-FFA as compared to conventional FFA or 9-field montage FFA.[59,60] The PVL implies persistence of disease activity, which may have implications on the amount of required immunosuppression.
An attempt has also been made to grade the vitreous haze using UWF imaging. Dickson et al.[61] showed good inter-observer correlation using UWF imaging regarding the degree of haze. However, UWF imaging was poor at detecting low levels of vitreous haze. More so, it could not be validated in presence of anterior segment opacities like cataract and corneal opacity. Using UWF imaging, vitreous haze in primary vitreo-retinal lymphoma has been described in various patterns such as Aurora borealis type, where there are linear opacities along the vitreous fibrils, string of pearl type where there are fine fibrils connecting the aggregated inflammatory cells or non-specific pattern.[62]
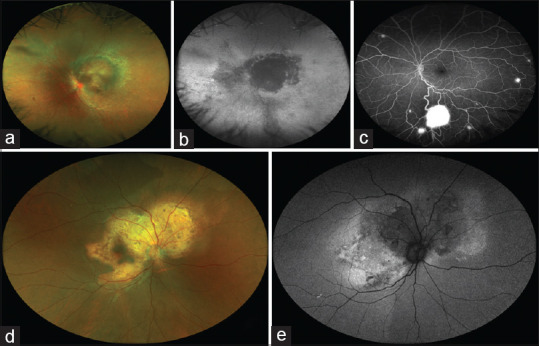
Vogt Koyanagi Harada (VKH) syndrome: The classical findings seen on angiography at posterior pole in VKH have been demonstrated in the peripheral fundus as well [Fig. 6a-c].[63] Lee et al.[64] has classified the sunset glow fundus seen in chronic VKH cases based on the extent of pigmentary changes seen on UWF imaging as early, intermediate and advanced. Patients with a higher grade of such changes tend to have a higher incidence of cataract, glaucoma and chronic uveitis but a lower incidence of exudative detachment.
White dot syndromes: UWF imaging detects the peripheral involvement in this subset of patients which may not be evident clinically. Hyperautofluorescent spots arising from the peripapillary retina and progressing beyond the arcades into the peripheral retina have been seen using UWF-FAF in the acute phase of multiple evanescent white dot syndrome. During the recovery phase, the auto-hyperfluorescent spots fade from the periphery towards the centre.[65] Even in acute zonal occult outer retinopathy (AZOOR), the extent of the pathology is better appreciated on UWF-FAF. Acute lesions are seen as diffuse hyperautofluorescent while chronic cases show central mottled or diffuse hypoautofluorescent area with surrounding hyperautofluorescent border. The pattern of spread of these lesions can vary from centrifugal to centripetal to a combination of centrifugal and centripetal. As compared to standard FAF, extensive involvement was seen on UWF-FAF.[66] Subclinical peripheral lesions have been demonstrated using UWF imaging in acute posterior multifocal placoid pigment epitheliopathy (APMPPE). Mrejen et al.[67] suggested that these lesions are more readily picked up with the 635 nm (red) filter light used for Optos wide field imaging because of its deeper penetration. Similarly, Knickelbein et al.[68] demonstrated that a higher percentage of patients with birdshot choroidopathy had lesions seen on 635 nm imaging than 532 nm as this is primarily a choroidal inflammatory disorder.
Infectious posterior uveitis: The extent of acute retinal necrosis, an important risk factor for development of retinal detachment, can be easily monitored using UWF imaging even through a hazy media.[69] Regression of lesions documented by UWF imaging provides objective evidence of disease regression and can help in patient education and counselling in this grave sight-threatening disorder. Similarly, UWF imaging is a useful tool for assessment and monitoring of cytomegalovirus retinitis, which predominantly affects the peripheral retina [Fig. 6d][70] In tubercular posterior uveitis, UWF imaging revealed additional peripheral retinal findings such as peripheral areas of vasculitis, choroiditis, neovascularization and capillary non-perfusion in 90% cases [Fig. 6e].[71]
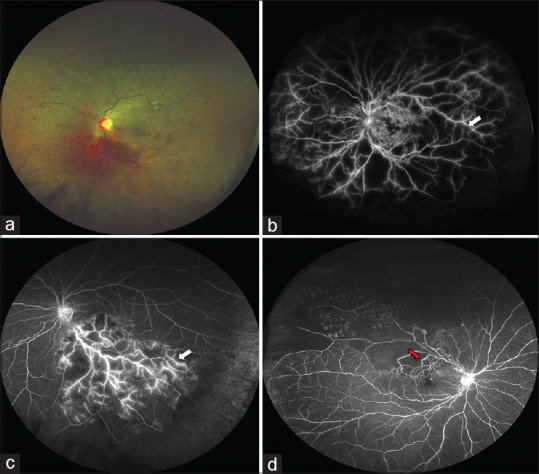
Vasculitis: UWF imaging and FFA play a pivotal role in the diagnosis and management of patients with retinal vasculitis. UWF imaging has been shown to be superior to both clinical examination and conventional angiography in detection of retinal pathology in the context of vasculitis [Fig. 7a-d]. In a prospective observational study, Leder et al.[72] found that UWF-FFA in retinal vasculitis revealed more signs than clinical examination or conventional fundus imaging. In this series, the percentage detection of disease activity was 38%, 45%, 50% and 67% using clinical examination, conventional angiography, UWF photography and UWF-FFA respectively.[72] Surprisingly, a series evaluating UWF imaging in patients with active Behcet‘s retinal vasculitis found that vasculitis was clinically missed in more than 80% of eyes.[73] Kumar et al.[74] studied UWF-FFA in patients with Eales disease and found that it was helpful in documentation of peripheral findings in 2/3rd of eyes with immediate change in management plan based on these UWF findings in 1/3rd of cases.
Figure 7.
UWF-FFA of active retinal vasculitis which can be generalized (a) or localised (b). UWF-FFA of healed retinal vasculitis with extensive capillary non-perfusion areas (CNP) in the retinal periphery and neovascularization (c). Fibro-vascular proliferation (d) in the background of large CNPs is evident in a case of healed retinal vasculitis on UWF-FFA
Sheemar et al.[75] studied 200 patients with retinal vasculitis using UWF imaging and FFA. They found, higher number of patients to have bilateral disease (72.5%) on UWF-FFA as compared to clinical examination alone (65%). In this study, the area confined to the posterior pole was designated as zone 1, between posterior pole and equator as zone 2 and area beyond equator as zone 3. Involvement of all 3 zones was noted in half the number of eyes. Veins were most commonly involved (78%) followed by mixed arterial and venous involvement (18%). As expected, peripheral neovascularization and non-perfusion areas were detected better on UWF imaging.
UWF is also uniquely suited to study children with retinal vasculitis due to the information carried within a single frame. In addition, this imaging modality helps in better understanding of the extent of pathology and sequelae of vasculitis syndrome like IRVAN (Idiopathic retinal vasculitis and neuroretinitis), acute hemorrhagic retinal vasculitis, frosted branch angitis, etc. It is also a useful method to ascertain the response and adequacy of treatment in retinal vasculitis, particularly, retinal photocoagulation.
UWF Imaging in age-related macular degeneration
The advent of UWF imaging has enabled us to observe and study peripheral retinal changes in age-related macular degeneration (AMD), although the significance of these changes is not fully understood at this time. Peripheral retinal changes commonly observed in eyes with AMD include drusen, atrophy, and retinal pigment epithelium changes.[76] Drusen, hallmark of AMD, may not be limited to the posterior pole, as thought previously. In fact, drusen have been described in both the mid and far periphery in several AMD eyes [Fig. 8a and b].[77] Also, the temporal sector is seen to be less affected by peripheral drusen since temporal mid-peripheral choriocapillaris perfusion is greater than that of other quadrants.[78] Domalpally et al.[77] found that patients with AMD showed FAF abnormalities in 82% of eyes in the mid-periphery and 49% of eyes in the far periphery, whereas normal control participants showed similar abnormalities in only 28% of eyes in the mid-periphery and 10% of eyes in the far periphery.
Figure 8.
UWF pseudocolor image showing peripheral drusen (a) which are more evident on UWF-FAF (b). UWF pseudocolour image shows retinal lesion in the periphery with subretinal and sub retinal pigment epithelium hemorrhage (c). UWF- FFA showed peripheral leakage along with blocked hypofluorescence confirming peripheral exudative hemorrhagic chorioretinopathy (d)
Another pathology, peripheral exudative hemorrhagic chorioretinopathy (PEHCR) is believed to be a peripheral variant of AMD [Fig. 8c and d]. The introduction of UWF imaging has changed the way PEHCR is diagnosed, classified, and managed. Tsui et al.[79] were the first to report UWF imaging in four patients of PEHCR. The authors found that accurate photographic documentation helped monitor growth in order to distinguish PEHCR from potentially treatable or life-threatening lesions such as choroidal metastatic tumor or primary choroidal melanoma. Kumar et al.[80] reported that in PEHCR, the pathology frequently lies anterior to the equator. The peripheral disciform scar, in their case, was visible only on the steered images, and that too with the help of UWF imaging. Further, using UWF-ICGA, studies have revealed presence of polyps in up to 70% of eyes with PEHCR and some now consider PEHCR as a peripheral variant of polypoidal choroidal vasculopathy.[81]
UWF Imaging in retinal and choroidal dystrophies
UWF imaging with a large field of view in a single click allows excellent documentation of retina and choroidal dystrophies since the patients tend to have poor vision and fixation, precluding montaging techniques [Fig. 9a-f]. In addition, many patients have nystagmus and are of pediatric age group which can further affect patient cooperation and image capture. UWF imaging allows good wide field images even in disorders like Leber congenital amaurosis [Fig. 9a], where absent fixation and nystagmus makes conventional capture nearly impossible.[82]
Figure 9.

UWF pseudocolour image of Leber congenital amaurosis showing chorioretinal degeneration, macular coloboma and peripheral bone-spicule like pigmentation (a). UWF-FAF shows peripheral involvement in a case of Stargardt disease (b). UWF pseudocolour image of pigmented paravenous retinochoroidal atrophy (c) showing perivascular pigmentary changes extending into periphery, which are better characterized on FAF (d). UWF-FFA of gyrate dystrophy (e) and choroideremia (f)
UWF imaging especially FAF has shed light on the pathophysiology of several inherited dystrophies. Stargardt disease (SD) has been considered to be a macular disorder for decades. However, Klufas et al.[83] using UWF FAF have shown that peripheral involvement may be seen in majority of the patients with SD and classified it into three types [Fig. 9b]. Type 1 are cases with no peripheral findings, type 2 includes macular atrophy with only flecks in the periphery, and type 3 are cases with macular and peripheral atrophy. Kumar et al.[84] studied UWF FAF in SD and found a coincidence of well-defined border of elevated background autofluorescence with the farthest extent of hyperautofluorescent flecks in addition to the peripheral findings. Peripheral lesions similar to congenital hypertrophy of retinal pigment epithelium have also been described in SD using UWF imaging.[85]
UWF imaging is useful for diagnosis and monitoring of patients with retinitis pigmentosa (RP). Decreased FAF in periphery of these eyes correlated well with scotoma on Goldmann perimetry and a system of grading RP in different genotypes has been proposed using UWF FAF.[85,86] In certain cases, UWF imaging can be used for correlation of phenotype with the genes affected.[86,87] Kumar et al. studied pigmented para-venous retino-choroidal atrophy on UWF imaging and found that affected areas demonstrated hypoautofluorescence with sharp hyperautofluorescent borders and considered it as a self-limited form of RP [Fig. 9c and d].[88] In addition, UWF-FFA also aids in documenting rare features like hemangioblastoma and Coats like response in RP.[89] UWF imaging has been studied in various choroidal dystrophies and has demonstrated distinctive patterns that may aid in their identification [Fig. 9e and f].[90] It is also useful in documenting striking peripheral changes in other rare disorders like Sveinsson chorioretinal atrophy and benign familial fleck retina.[91]
UWF imaging in tumors
UWF imaging has found a particular role in the field of oncology: for diagnosis and documentation of tumors, planning their management, following their course and monitoring complications [Fig. 10a-e].[92,93,94,95,96] Its utility has expanded from fundus photography initially, to include autofluorescence, angiography and optical coherence tomography.[95,96,97] UWF imaging is crucial in the context of multiple choroidal metastasis that occur anterior to the equator and could have been otherwise missed on examination. Furthermore, it may also aid in easier differentiation between choroidal melanoma and benign nevi by allowing meticulous measurements of the tumor size, assessment of overlying pigment changes, and evaluating change in the tumor size on follow-up.[96]
Figure 10.
UWF pseudocolour image (a) of choroidal hemangioma at posterior pole. UWF-FAF shows large hypoautofluorescent areas extending to inferior retina due to chronic fluid exudation and retinal pigment epithelium loss (b). UWF–FFA in Von-Hippel-Lindau shows multiple retinal capillary hemangioblastomas and inferior large lesion with feeder vessels (c). UWF imaging (d) of choroidal osteoma shows irregular, yellow-white, juxtrapapillary lesion which had central hypoautofluorescence (signifying decalcification) with surrounding hyperautofluorescence on UWF-FAF (e)
Ayres et al.[92] compared various radiological, conventional and UWF imaging techniques with clinical examination for measuring the choroidal tumors. UWF imaging was found to be more comparable to the clinically estimated tumor basal diameter than the findings of other imaging tools. Kernt et al.[98] also found UWF measurements to correlate well with ultrasound measurements for melanotic tumors. They also used 2 lasers of UWF imaging (red and green) to differentiate between malignant and benign lesions of the choroid, both sensitivity and specificity exceeding 70%, with malignant lesions being darker with red spectrum.[98] In tumors like retinoblastoma, UWF imaging or akin systems may be useful in documenting the effect of therapy and monitoring recurrences quantitatively. By changing the focus of the camera to anterior cavity, one can also document vitreous seeding and anterior involvement.[96] In tumors like choroidal hemangioma, UWF imaging can be used to monitor the extent of retinal detachment and determine response to therapy [Fig. 10a and b].
UWF-FAF is another useful tool for differentiating melanomas from nevi. Reznicek et al.[99] reported mean FAF intensity to be significantly lower in malignant lesions as compared to the benign nevi. They described “mixed appearance” of melanoma on UWF FAF with “green laser separation technique”. Heimann et al.[93] described intrinsic and extrinsic FAF features of vascular tumors like choroidal hemangiomas, particularly relating to overlying pigment changes, fibrosis and subretinal fluid. Further, UWF-FFA has made evaluation of peripheral vascular tumors more thorough.[93] It helps in identifying several pathognomic features like rapid filling and quick wash out of dye seen in choroidal hemangiomas, identification of the “extremely peripheral” vasoproliferative tumors within the accompanying fibrosis and retinal detachment, and localizing small peripheral angiomas oblivious to ophthalmoscopic examination.[93,100] Novel features like abnormal capillary network, capillary leakage and telangiectasia have been described in retinal hemangioblastomas using UWF-FFA.[101]
Management of retinal angiomas is dependent on identification of feeder vessels in early stages, and for this, peripheral angiography offers a very reliable way of identification of feeders. This is especially true in syndromic involvement where new small retinal angiomas are known to develop over long term. UWF imaging has been suggested as a sole ophthalmic tool for screening these angiomas in Von Hippel-Lindau clinics [Fig. 10c].[102] Furthermore, UWF imaging with its angiographic features may also be useful in accurate classification of retinal capillary hemangioblastomas.[103] Conversely, it also helps in identifying and documenting non-neoplastic lesions like exudative-hemorrhagic chorioretinopathies which are known to simulate tumors.[79,80] UWF-FFA is particularly useful in identifying early peripheral features of radiation retinopathy and its classification, which is expected to become crucial given the current era of brachytherapy.[93,96]
However, one should be careful while using UWF imaging for measuring size of tumors as ultrasound may be better when tumor height exceeds 3 mm and in presence of exudative retinal detachment.[92] Further estimation of tumor dimensions can be tricky as peripheral most areas of the fundus appear to be stretched specifically in the horizontal axis.[94] UWF being largely based on pseudo-colour images, there have also been concerns over difficulty in differentiating between tumors on UWF, specifically between melanotic and vascular tumors.
Limitations
Although useful, UWF imaging has its own limitations. One of the major problems is high cost and limited availability. Others include common artefacts from eyelashes, lid margin and nose [Figs. 2 and 5]. However, all these can be reduced with simple measures like lid holding and proper centration of eye at a suitable distance. The learning curve of the photographer is also important. Inherent problem of projecting a curved area on a flat surface leads to peripheral distortion and magnification. This leads to errors especially in peripheral measurements. However recent advancements in hardware and software including stereographic projection software, help in correction of peripheral distortion. Absence of true colors in fundus images may lead to errors in diagnosis especially when diagnosis is based on the color of the lesion. Lastly, while UWF imaging is good for horizontal (temporal and nasal) periphery, superior and inferior periphery is not that well visualized. The latter may be rectified using steered images and automated montage, which is possible in advanced versions of the equipment.
Future direction
With continuing development of UWF imaging and recent inclusion of OCT, the future may see increased accuracy and efficiency in dealing with peripheral retinal lesions. UWF images will be further explored for automated detection and grading of various diseases and lesions including automated detection of CNP, determining ischemic index and management options including predicting the need of laser photocoagulation. Also, wider field of view, no pupillary dilatation, faster acquisition and high-resolution images make it an ideal candidate for telemedicine, however, high cost has limited its wider applicability. In specific situations, it is likely to transpire from an adjunct to a substitute of ophthalmoscopic examination.
Conclusion
UWF imaging has revolutionized the way we document the periphery of retina and has provided new insights into various retinal disorders.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Diabetic retinopathy study. Report Number 6. Design, methods, and baseline results. Report Number 7. A modification of the Airlie House classification of diabetic retinopathy. Prepared by the Diabetic Retinopathy. Invest Ophthalmol Vis Sci. 1981;21:1–226. [PubMed] [Google Scholar]
- 2.Diabetic Retinopathy Clinical Research Network. Peripheral diabetic retinopathy (DR) lesions on ultrawide-field fundus images and risk of DR worsening over time. DRCRnet. DRCR Retina Network-Public Site. Available from: https://public.jaeb.org/drcrnet .
- 3.Choudhry N, Duker JS, Freund KB, Kiss S, Querques G, Rosen R, et al. Classification and guidelines for widefield imaging: Recommendations from the International Widefield Imaging Study Group. Ophthalmol Retina. 2019;3:843–9. doi: 10.1016/j.oret.2019.05.007. [DOI] [PubMed] [Google Scholar]
- 4.Shah AR, Abbey AM, Yonekawa Y, Khandan S, Wolfe JD, Trese MT, et al. Widefield fluorescein angiography in patients without peripheral disease: A Study of Normal Peripheral Findings. Retina (Philadelphia, Pa) 2016;36:1087–92. doi: 10.1097/IAE.0000000000000878. [DOI] [PubMed] [Google Scholar]
- 5.Lu J, Mai G, Luo Y, Li M, Cao D, Wang X, et al. Appearance of far peripheral retina in normal eyes by ultra-widefield fluorescein angiography. Am J Ophthalmol. 2017;173:84–90. doi: 10.1016/j.ajo.2016.09.024. [DOI] [PubMed] [Google Scholar]
- 6.Singer M, Sagong M, van Hemert J, Kuehlewein L, Bell D, Sadda SR. Ultra-widefield imaging of the peripheral retinal vasculature in normal subjects. Ophthalmology. 2016;123:1053–9. doi: 10.1016/j.ophtha.2016.01.022. [DOI] [PubMed] [Google Scholar]
- 7.Kaneko Y, Moriyama M, Hirahara S, Ogura Y, Ohno-Matsui K. Areas of nonperfusion in peripheral retina of eyes with pathologic myopia detected by ultra-widefield fluorescein angiography. Invest Ophthalmol Vis Sci. 2014;55:1432–9. doi: 10.1167/iovs.13-13706. [DOI] [PubMed] [Google Scholar]
- 8.Kusumi Y, Sano M, Nakayama M, Koto T, Inoue M, Yamamoto M, et al. [Efficacy of ultra-wide angle fundus imaging without dilated pupils in annual health check-up examination] Nippon Ganka Gakkai Zasshi. 2016;120:35–40. [PubMed] [Google Scholar]
- 9.Kornberg DL, Klufas MA, Yannuzzi NA, Orlin A, D‘Amico DJ, Kiss S. Clinical utility of ultra-widefield imaging with the optos optomap compared with indirect ophthalmoscopy in the setting of non-traumatic rhegmatogenous retinal detachment. Semin Ophthalmol. 2016;31:505–12. doi: 10.3109/08820538.2014.981551. [DOI] [PubMed] [Google Scholar]
- 10.Fogliato G, Borrelli E, Iuliano L, Ramoni A, Querques L, Rabiolo A, et al. Comparison between ultra-widefield pseudocolor imaging and indirect ophthalmoscopy in the detection of peripheral retinal lesions. Ophthalmic Surg Lasers Imaging Retina. 2019;50:544–9. doi: 10.3928/23258160-20190905-02. [DOI] [PubMed] [Google Scholar]
- 11.Kumar V, Damodaran S, Sharma A. Vitreous base avulsion? BMJ Case Rep. 2017:2017. doi: 10.1136/bcr-2016-218303. published online. doi: 10.1136/bcr-2016-218303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Inoue M, Koto T, Hirota K, Hirakata A. Ultra-widefield fundus imaging in gas-filled eyes after vitrectomy. BMC Ophthalmology. 2017;17:114. doi: 10.1186/s12886-017-0510-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ohno-Matsui K. Proposed classification of posterior staphylomas based on analyses of eye shape by three-dimensional magnetic resonance imaging and wide-field fundus imaging. Ophthalmology. 2014;121:1798–809. doi: 10.1016/j.ophtha.2014.03.035. [DOI] [PubMed] [Google Scholar]
- 14.Kornberg DL, Yannuzzi NA, Klufas MA, D‘Amico DJ, Orlin A, Kiss S. Ultra-widefield imaging of posterior segment pathology in the setting of the boston keratoprosthesis. Retina (Philadelphia, Pa) 2016;36:1101–10. doi: 10.1097/IAE.0000000000000833. [DOI] [PubMed] [Google Scholar]
- 15.Chen WS, Friberg TR, Eller AW, Medina C. Advances in retinal imaging of eyes with hazy media: Further studies. Invest Ophthalmol Vis Sci. 2011;52:4036. [Google Scholar]
- 16.Witmer MT, Cho M, Favarone G, Paul Chan RV, D‘Amico DJ, Kiss S. Ultra-wide-field autofluorescence imaging in non-traumatic rhegmatogenous retinal detachment. Eye (Lond) 2012;26:1209–16. doi: 10.1038/eye.2012.122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Salvanos P, Navaratnam J, Ma J, Bragadóttir R, Moe MC. Ultra-widefield autofluorescence imaging in the evaluation of scleral buckling surgery for retinal detachment. Retina (Philadelphia, Pa) 2013;33:1421–7. doi: 10.1097/IAE.0b013e318283138d. [DOI] [PubMed] [Google Scholar]
- 18.Tripathy K, Chawla R, Wadekar BR, Venkatesh P, Sharma YR. Evaluation of rhegmatogenous retinal detachments using Optos ultrawide field fundus fluorescein angiography and comparison with ETDRS 7 field overlay. J Curr Ophthalmol. 2018;30:263–7. doi: 10.1016/j.joco.2018.06.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Grading diabetic retinopathy from stereoscopic color fundus photographs--An extension of the modified Airlie House classification. ETDRS report number 10. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology. 1991;98(5 Suppl):786–806. [PubMed] [Google Scholar]
- 20.Silva PS, Cavallerano JD, Haddad NMN, Kwak H, Dyer KH, Omar AF, et al. Peripheral lesions identified on ultrawide field imaging predict increased risk of diabetic retinopathy progression over 4 years. Ophthalmology. 2015;122:949–56. doi: 10.1016/j.ophtha.2015.01.008. [DOI] [PubMed] [Google Scholar]
- 21.Price LD, Au S, Chong NV. Optomap ultrawide field imaging identifies additional retinal abnormalities in patients with diabetic retinopathy. Clin Ophthalmol. 2015;9:527–31. doi: 10.2147/OPTH.S79448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Silva PS, Cavallerano JD, Sun JK, Soliman AZ, Aiello LM, Aiello LP. Peripheral lesions identified by mydriatic ultrawide field imaging: Distribution and potential impact on diabetic retinopathy severity. Ophthalmology. 2013;120:2587–95. doi: 10.1016/j.ophtha.2013.05.004. [DOI] [PubMed] [Google Scholar]
- 23.Wessel MM, Aaker GD, Parlitsis G, Cho M, D‘Amico DJ, Kiss S. Ultra-wide-field angiography improves the detection and classification of diabetic retinopathy. Retina (Philadelphia, Pa) 2012;32:785–91. doi: 10.1097/IAE.0b013e3182278b64. [DOI] [PubMed] [Google Scholar]
- 24.Rasmussen ML, Broe R, Frydkjaer-Olsen U, Olsen BS, Mortensen HB, Peto T, et al. Comparison between early treatment diabetic retinopathy study 7-field retinal photos and non-mydriatic, mydriatic and mydriatic steered widefield scanning laser ophthalmoscopy for assessment of diabetic retinopathy. J Diabetes Complications. 2015;29:99–104. doi: 10.1016/j.jdiacomp.2014.08.009. [DOI] [PubMed] [Google Scholar]
- 25.Kim DY, Kim J-G, Kim YJ, Joe SG, Lee JY. Ultra-widefield fluorescein angiographic findings in patients with recurrent vitreous hemorrhage after diabetic vitrectomy. Invest Ophthalmol Vis Sci. 2014;55:7040–6. doi: 10.1167/iovs.14-15112. [DOI] [PubMed] [Google Scholar]
- 26.Bhagat N, Grigorian RA, Tutela A, Zarbin MA. Diabetic macular edema: Pathogenesis and treatment. Surv Ophthalmol. 2009;54:1–32. doi: 10.1016/j.survophthal.2008.10.001. [DOI] [PubMed] [Google Scholar]
- 27.Wessel MM, Nair N, Aaker GD, Ehrlich JR, D‘Amico DJ, Kiss S. Peripheral retinal ischaemia, as evaluated by ultra-widefield fluorescein angiography, is associated with diabetic macular oedema. Br J Ophthalmol. 2012;96:694–8. doi: 10.1136/bjophthalmol-2011-300774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Oliver SCN, Schwartz SD. Peripheral vessel leakage (PVL): A new angiographic finding in diabetic retinopathy identified with ultra wide-field fluorescein angiography. Semin Ophthalmol. 2010;25:27–33. doi: 10.3109/08820538.2010.481239. [DOI] [PubMed] [Google Scholar]
- 29.Patel RD, Messner LV, Teitelbaum B, Michel KA, Hariprasad SM. Characterization of ischemic index using ultra-widefield fluorescein angiography in patients with focal and diffuse recalcitrant diabetic macular edema. Am J Ophthalmol. 2013;155:1038–44.e2. doi: 10.1016/j.ajo.2013.01.007. [DOI] [PubMed] [Google Scholar]
- 30.Sim DA, Keane PA, Rajendram R, Karampelas M, Selvam S, Powner MB, et al. Patterns of peripheral retinal and central macula ischemia in diabetic retinopathy as evaluated by ultra-widefield fluorescein angiography. Am J Ophthalmol. 2014;158:144–153.e1. doi: 10.1016/j.ajo.2014.03.009. [DOI] [PubMed] [Google Scholar]
- 31.Silva PS, Dela Cruz AJ, Ledesma MG, van Hemert J, Radwan A, Cavallerano JD, et al. Diabetic retinopathy severity and peripheral lesions are associated with nonperfusion on ultrawide field angiography. Ophthalmology. 2015;122:2465–72. doi: 10.1016/j.ophtha.2015.07.034. [DOI] [PubMed] [Google Scholar]
- 32.Muqit MMK, Young LB, McKenzie R, John B, Marcellino GR, Henson DB, et al. Pilot randomised clinical trial of Pascal TargETEd Retinal versus variable fluence PANretinal 20 ms laser in diabetic retinopathy: PETER PAN study. Br J Ophthalmol. 2013;97:220–7. doi: 10.1136/bjophthalmol-2012-302189. [DOI] [PubMed] [Google Scholar]
- 33.Singh RP, Hsueh J, Han MM, Kuriyan AE, Conti FF, Steinle N, et al. Protecting vision in patients with diabetes with ultra-widefield imaging: A review of current literature. Ophthalmic Surg Lasers Imaging Retina. 2019;50:639–48. doi: 10.3928/23258160-20191009-07. [DOI] [PubMed] [Google Scholar]
- 34.Singer M, Tan CS, Bell D, Sadda SR. Area of peripheral retinal nonperfusion and treatment response in branch and central retinal vein occlusion. Retina (Philadelphia, Pa) 2014;34:1736–42. doi: 10.1097/IAE.0000000000000148. [DOI] [PubMed] [Google Scholar]
- 35.Tsui I, Kaines A, Havunjian MA, Hubschman S, Heilweil G, Prasad PS, et al. Ischemic index and neovascularization in central retinal vein occlusion. Retina (Philadelphia, Pa) 2011;31:105–10. doi: 10.1097/IAE.0b013e3181e36c6d. [DOI] [PubMed] [Google Scholar]
- 36.Tan CS, Chew MC, van Hemert J, Singer MA, Bell D, Sadda SR. Measuring the precise area of peripheral retinal non-perfusion using ultra-widefield imaging and its correlation with the ischaemic index. Br J Ophthalmol. 2016;100:235–9. doi: 10.1136/bjophthalmol-2015-306652. [DOI] [PubMed] [Google Scholar]
- 37.Argon laser photocoagulation for macular edema in branch vein occlusion. The Branch Vein Occlusion Study Group. Am J Ophthalmol. 1984;9:271–82. doi: 10.1016/0002-9394(84)90316-7. [DOI] [PubMed] [Google Scholar]
- 38.Natural history and clinical management of central retinal vein occlusion. The Central Vein Occlusion Study Group. Arch Ophthalmol. 1997;115:486–91. doi: 10.1001/archopht.1997.01100150488006. [DOI] [PubMed] [Google Scholar]
- 39.Abri Aghdam K, Reznicek L, Soltan Sanjari M, Framme C, Bajor A, Klingenstein A, et al. Peripheral retinal non-perfusion and treatment response in branch retinal vein occlusion. Int J Ophthalmol. 2016;9:858–62. doi: 10.18240/ijo.2016.06.12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Prasad PS, Oliver SCN, Coffee RE, Hubschman J-P, Schwartz SD. Ultra wide-field angiographic characteristics of branch retinal and hemicentral retinal vein occlusion. Ophthalmology. 2010;117:780–4. doi: 10.1016/j.ophtha.2009.09.019. [DOI] [PubMed] [Google Scholar]
- 41.Kwon S, Wykoff CC, Brown DM, van Hemert J, Fan W, Sadda SR. Changes in retinal ischaemic index correlate with recalcitrant macular oedema in retinal vein occlusion: WAVE study. Br J Ophthalmol. 2018;102:1066–71. doi: 10.1136/bjophthalmol-2017-311475. [DOI] [PubMed] [Google Scholar]
- 42.Muqit MMK, Marcellino GR, Henson DB, Young LB, Patton N, Charles SJ, et al. Optos-guided pattern scan laser (Pascal)-targeted retinal photocoagulation in proliferative diabetic retinopathy. Acta Ophthalmol. 2013;91:251–8. doi: 10.1111/j.1755-3768.2011.02307.x. [DOI] [PubMed] [Google Scholar]
- 43.Goel S, Kumar A, Ravani RD, Chandra P, Chandra M, Kumar V. Comparison of ranibizumab alone versus ranibizumab with targeted retinal laser for branch retinal vein occlusion with macular edema. Indian J Ophthalmol. 2019;67:1105–8. doi: 10.4103/ijo.IJO_1364_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Singer MA, Tan CS, Surapaneni KR, Sadda SR. Targeted photocoagulation of peripheral ischemia to treat rebound edema. Clin Ophthalmol. 2015;9:337–41. doi: 10.2147/OPTH.S75842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Kang KB, Wessel MM, Tong J, D‘Amico DJ, Chan RVP. Ultra-widefield imaging for the management of pediatric retinal diseases. J Pediatr Ophthalmol Strabismus. 2013;50:282–8. doi: 10.3928/01913913-20130528-04. [DOI] [PubMed] [Google Scholar]
- 46.Tsui I, Franco-Cardenas V, Hubschman J-P, Schwartz SD. Pediatric retinal conditions imaged by ultra wide field fluorescein angiography. Ophthalmic Surg Lasers Imaging Retina. 2013;44:59–67. doi: 10.3928/23258160-20121221-14. [DOI] [PubMed] [Google Scholar]
- 47.Rabiolo A, Marchese A, Sacconi R, Cicinelli MV, Grosso A, Querques L, et al. Refining Coats‘ disease by ultra-widefield imaging and optical coherence tomography angiography. Graefes Arch Clin Exp Ophthalmol. 2017;255:1881–90. doi: 10.1007/s00417-017-3794-7. [DOI] [PubMed] [Google Scholar]
- 48.Kumar V, Chandra P, Kumar A. Ultra-wide field imaging in the diagnosis and management of adult-onset Coats‘ disease. Clin Exp Optom. 2017;100:79–82. doi: 10.1111/cxo.12418. [DOI] [PubMed] [Google Scholar]
- 49.Lyu J, Zhang Q, Wang SY, Chen YY, Xu Y, Zhao PQ. Ultra-wide-field scanning laser ophthalmoscopy assists in the clinical detection and evaluation of asymptomatic early-stage familial exudative vitreoretinopathy. Graefes Arch Clin Exp Ophthalmol. 2017;255:39–47. doi: 10.1007/s00417-016-3415-x. [DOI] [PubMed] [Google Scholar]
- 50.Kashani AH, Brown KT, Chang E, Drenser KA, Capone A, Trese MT. Diversity of retinal vascular anomalies in patients with familial exudative vitreoretinopathy. Ophthalmology. 2014;121:2220–7. doi: 10.1016/j.ophtha.2014.05.029. [DOI] [PubMed] [Google Scholar]
- 51.Trese MT. What is the real gold standard for ROP screening? Retina (Philadelphia, Pa) 2008;28(3 Suppl):S1–2. doi: 10.1097/IAE.0b013e31816a5587. [DOI] [PubMed] [Google Scholar]
- 52.Richter GM, Williams SL, Starren J, Flynn JT, Chiang MF. Telemedicine for retinopathy of prematurity diagnosis: Evaluation and challenges. Surv Ophthalmol. 2009;54:671–85. doi: 10.1016/j.survophthal.2009.02.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Vinekar A, Jayadev C, Mangalesh S, Shetty B, Vidyasagar D. Role of tele-medicine in retinopathy of prematurity screening in rural outreach centers in India - A report of 20,214 imaging sessions in the KIDROP program. Semin Fetal Neonatal Med. 2015;20:335–45. doi: 10.1016/j.siny.2015.05.002. [DOI] [PubMed] [Google Scholar]
- 54.Patel CK, Fung THM, Muqit MMK, Mordant DJ, Brett J, Smith L, et al. Non-contact ultra-widefield imaging of retinopathy of prematurity using the Optos dual wavelength scanning laser ophthalmoscope. Eye (Lond) 2013;27:589–96. doi: 10.1038/eye.2013.45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Chi Y, Guo C, Peng Y, Qiao L, Yang L. A prospective, observational study on the application of ultra-wide-field angiography in the evaluation and management of patients with anterior uveitis. PLOS One. 2015;10:e0122749. doi: 10.1371/journal.pone.0122749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Yang M, Chi Y, Guo C, Huang J, Yang L, Yang L. Clinical profile, ultra-wide-field fluorescence angiography findings, and long-term prognosis of uveitis in tubulointerstitial nephritis and uveitis syndrome at one Tertiary Medical Institute in China. Ocul Immunol Inflamm. 2019;27:371–9. doi: 10.1080/09273948.2017.1394469. [DOI] [PubMed] [Google Scholar]
- 57.Tsui I, Kaines A, Schwartz S. Patterns of periphlebitis in intermediate uveitis using ultra wide field fluorescein angiography. Semin Ophthalmol. 2009;24:29–33. doi: 10.1080/08820530802520186. [DOI] [PubMed] [Google Scholar]
- 58.Laovirojjanakul W, Acharya N, Gonzales JA. Ultra-widefield fluorescein angiography in intermediate uveitis. Ocul Immunol Inflamm. 2019;27:356–61. doi: 10.1080/09273948.2017.1371764. [DOI] [PubMed] [Google Scholar]
- 59.Tanaka R, Kaburaki T, Yoshida A, Takamoto M, Miyaji T, Yamaguchi T. Fluorescein angiography scoring system using ultra-wide-field fluorescein angiography versus standard fluorescein angiography in patients with sarcoid uveitis? Ocul Immunol Inflamm. 2020:1–5. doi: 10.1080/09273948.2020.1737141. Published online. doi: 10.1080/09273948.2020.1737141. [DOI] [PubMed] [Google Scholar]
- 60.Nicholson BP, Nigam D, Miller D, Agrón E, Dalal M, Jacobs-El N, et al. Comparison of wide-field fluorescein angiography and nine-field montage angiography in uveitis. Am J Ophthalmol. 2014;157:673–7. doi: 10.1016/j.ajo.2013.12.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Dickson D, Agarwal A, Sadiq MA, Hassan M, High R, Nguyen QD, et al. Assessment of vitreous haze using ultra-wide field retinal imaging. J Ophthalmic Inflamm Infect. 2016;6:35. doi: 10.1186/s12348-016-0105-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Marchese A, Miserocchi E, Giuffrè C, Cicinelli MV, Querques G, Bandello F, et al. Aurora borealis and string of pearls in vitreoretinal lymphoma: Patterns of vitreous haze. Br J Ophthalmol. 2019;103:1656–9. doi: 10.1136/bjophthalmol-2018-313491. [DOI] [PubMed] [Google Scholar]
- 63.Kim P, Sun HJ, Ham D-I. Ultra-wide-field angiography findings in acute Vogt-Koyanagi-Harada disease. Br J Ophthalmol. 2019;103:942–8. doi: 10.1136/bjophthalmol-2018-312569. [DOI] [PubMed] [Google Scholar]
- 64.Lee EK, Lee S-Y, Yu HG. A clinical grading system based on ultra-wide field retinal imaging for sunset glow fundus in Vogt-Koyanagi-Harada disease. Graefes Arch Clin Exp Ophthalmol. 2015;253:359–68. doi: 10.1007/s00417-014-2710-7. [DOI] [PubMed] [Google Scholar]
- 65.Hashimoto H, Kishi S. Ultra-wide-field fundus autofluorescence in multiple evanescent white dot syndrome. Am J Ophthalmol. 2015;159:698–706. doi: 10.1016/j.ajo.2015.01.015. [DOI] [PubMed] [Google Scholar]
- 66.Shifera AS, Pennesi ME, Yang P, Lin P. ULtra-wide-field fundus autofluorescence findings in patients with acute zonal occult outer retinopathy. Retina (Philadelphia, Pa) 2017;37:1104–19. doi: 10.1097/IAE.0000000000001311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Mrejen S, Sarraf D, Chexal S, Wald K, Freund KB. Choroidal involvement in acute posterior multifocal placoid pigment epitheliopathy. Ophthalmic Surg Lasers Imaging Retina. 2016;47:20–6. doi: 10.3928/23258160-20151214-03. [DOI] [PubMed] [Google Scholar]
- 68.Knickelbein JE, Hasan J, Nussenblatt RB, Sen HN. Delineation of choroidal and retinal lesions in posterior uveitis by multispectral wide-field scanning laser ophthalmoscopy. Retina (Philadelphia, Pa) 2016;36:2213–9. doi: 10.1097/IAE.0000000000001050. [DOI] [PubMed] [Google Scholar]
- 69.Lei B, Zhou M, Wang Z, Chang Q, Xu G, Jiang R. Ultra-wide-field fundus imaging of acute retinal necrosis: Clinical characteristics and visual significance. Eye (Lond) 2020;34:864–72. doi: 10.1038/s41433-019-0587-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Tadepalli S, Bajgai P, Dogra M, Singh SR, Sharma A, Gupta V, et al. Ultra-widefield fundus autofluorescence in cytomegalovirus retinitis. Ocul Immunol Inflamm. 2020;28:446–52. doi: 10.1080/09273948.2019.1595671. [DOI] [PubMed] [Google Scholar]
- 71.Aggarwal K, Mulkutkar S, Mahajan S, Singh R, Sharma A, Bansal R, et al. Role of ultra-wide field imaging in the management of tubercular posterior uveitis. Ocul Immunol Inflamm. 2016;24:631–6. doi: 10.3109/09273948.2015.1099681. [DOI] [PubMed] [Google Scholar]
- 72.Leder HA, Campbell JP, Sepah YJ, Gan T, Dunn JP, Hatef E, et al. Ultra-wide-field retinal imaging in the management of non-infectious retinal vasculitis. J Ophthalmic Inflamm Infect. 2013;3:30. doi: 10.1186/1869-5760-3-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Mesquida M, Llorenç V, Fontenla JR, Navarro MJ, Adán A. Use of ultra-wide-field retinal imaging in the management of active Behçet retinal vasculitis. Retina (Philadelphia, Pa) 2014;34:2121–7. doi: 10.1097/IAE.0000000000000197. [DOI] [PubMed] [Google Scholar]
- 74.Kumar V, Chandra P, Kumar A. Ultra-wide field angiography in the management of Eales disease. Indian J Ophthalmol. 2016;64:504–7. doi: 10.4103/0301-4738.190138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Sheemar A, Temkar S, Takkar B, Sood R, Sinha S, Chawla R, et al. Ultra-wide field imaging characteristics of primary retinal vasculitis: Risk factors for retinal neovascularization. Ocul Immunol Inflamm. 2019;27:383–8. doi: 10.1080/09273948.2018.1508729. [DOI] [PubMed] [Google Scholar]
- 76.Forshaw TRJ, Minör ÅS, Subhi Y, Sørensen TL. Peripheral retinal lesions in eyes with age-related macular degeneration using ultra-widefield imaging: A systematic review with meta-analyses. Ophthalmol Retina. 2019;3:734–43. doi: 10.1016/j.oret.2019.04.014. [DOI] [PubMed] [Google Scholar]
- 77.Writing Committee for the OPTOS PEripheral RetinA (OPERA) study (Ancillary Study of Age-Related Eye Disease Study 2) Domalpally A, Clemons TE, Danis RP, Sadda SR, Cukras CA, et al. Peripheral retinal changes associated with age-related macular degeneration in the age-related eye disease study 2: Age-related eye disease study 2 report number 12 by the age-related eye disease study 2 Optos PEripheral RetinA (OPERA) Study Research Group. Ophthalmology. 2017;124:479–87. doi: 10.1016/j.ophtha.2016.12.004. [DOI] [PubMed] [Google Scholar]
- 78.Corbelli E, Borrelli E, Parravano M, Sacconi R, Gilardi M, Costanzo E, et al. Multimodal imaging characterization of peripheral drusen. Graefes Arch Clin Exp Ophthalmol. 2020;258:543–9. doi: 10.1007/s00417-019-04586-7. [DOI] [PubMed] [Google Scholar]
- 79.Tsui I, Jain A, Shah S, Schwartz SD, McCannel TA. Ultra widefield imaging of peripheral exudative hemorrhagic chorioretinopathy. Semin Ophthalmol. 2009;24:25–8. doi: 10.1080/08820530802520178. [DOI] [PubMed] [Google Scholar]
- 80.Kumar V, Janakiraman D, Chandra P, Kumar A. Ultra-wide field imaging in peripheral exudative haemorrhagic chorioretinopathy (PEHCR) BMJ Case Reports. 2015:bcr2015213628. doi: 10.1136/bcr-2015-213628. Published online. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Goldman DR, Freund KB, McCannel CA, Sarraf D. Peripheral polypoidal choroidal vasculopathy as a cause of peripheral exudative hemorrhagic chorioretinopathy: A report of 10 eyes. Retina (Philadelphia, Pa) 2013;33:48–55. doi: 10.1097/IAE.0b013e31825df12a. [DOI] [PubMed] [Google Scholar]
- 82.Kumar V, Tewari R, Chandra P, kumar A. Ultra wide field imaging of coats like response in Leber‘s congenital amaurosis. Saudi J Ophthalmol. 2017;31:122–3. doi: 10.1016/j.sjopt.2017.02.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Klufas MA, Tsui I, Sadda SR, Hosseini H, Schwartz SD. Ultrawidefield autofluoresence in ABCA4 stargardt disease. Retina. 2018;38:403–15. doi: 10.1097/IAE.0000000000001567. [DOI] [PubMed] [Google Scholar]
- 84.Kumar V. Insights into autofluorescence patterns in Stargardt macular dystrophy using ultra-wide-field imaging. Graefes Arch Clin Exp Ophthalmol. 2017;255:1917–22. doi: 10.1007/s00417-017-3736-4. [DOI] [PubMed] [Google Scholar]
- 85.Zhao PY, Abalem MF, Nadelman D, Qian CX, Branham K, Schlegel D, et al. Peripheral pigmented retinal lesions in Stargardt disease. Am J Ophthalmol. 2018;188:104–10. doi: 10.1016/j.ajo.2017.12.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Hariri AH, Gui W, Datoo O‘Keefe GA, Ip MS, Sadda SR, Gorin MB. Ultra-widefield fundus autofluorescence imaging of patients with retinitis pigmentosa: A standardized grading system in different genotypes. Ophthalmol Retina. 2018;2:735–45. doi: 10.1016/j.oret.2017.10.018. [DOI] [PubMed] [Google Scholar]
- 87.Trichonas G, Traboulsi EI, Ehlers JP. Correlation of ultra-widefield fundus autofluorescence patterns with the underlying genotype in retinal dystrophies and retinitis pigmentosa. Ophthalmic Genet. 2017;38:320–4. doi: 10.1080/13816810.2016.1227450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Kumar V, Kumawat D, Tewari R, Venkatesh P. Ultra-wide field imaging of pigmented para-venous retino-choroidal atrophy. Eur J Ophthalmol. 2019;29:444–52. doi: 10.1177/1120672118795056. [DOI] [PubMed] [Google Scholar]
- 89.Jain S, Gupta S, Kumar V. Ultra-widefield imaging in Coats‘-type retinitis pigmentosa. Indian J Ophthalmol. 2018;66:997–8. doi: 10.4103/ijo.IJO_1109_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Yuan A, Kaines A, Jain A, Reddy S, Schwartz SD, Sarraf D. Ultra-wide-field and autofluorescence imaging of choroidal dystrophies? Ophthalmic Surg Lasers Imaging. 2010;41:e1–5. doi: 10.3928/15428877-20101025-10. Online. doi: 10.3928/15428877-20101025-10. [DOI] [PubMed] [Google Scholar]
- 91.Kumar V, Trehan H, Goel N. Sveinsson chorioretinal atrophy: Helicoid peripapillary chorioretinal degeneration. JAMA Ophthalmol. 2017;135:e173236. doi: 10.1001/jamaophthalmol.2017.3236. [DOI] [PubMed] [Google Scholar]
- 92.Ayres B, Stacey A, Grant J, McClendon T, Demirci H. Comparative study of clinical, ultrasonographic, conventional imaging, and ultra-wide-field fundus for measurements of the longest basal diameter of choroidal tumors. Ophthalmic Surg Lasers Imaging Retina. 2017;48:459–64. doi: 10.3928/23258160-20170601-03. [DOI] [PubMed] [Google Scholar]
- 93.Heimann H, Jmor F, Damato B. Imaging of retinal and choroidal vascular tumours. Eye (Lond) 2013;27:208–16. doi: 10.1038/eye.2012.251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Nagiel A, Lalane RA, Sadda SR, Schwartz SD. Ultra-widefield fundus imaging: A review of clinical applications and future trends. Retina (Philadelphia, Pa) 2016;36:660–78. doi: 10.1097/IAE.0000000000000937. [DOI] [PubMed] [Google Scholar]
- 95.Shoughy SS, Arevalo JF, Kozak I. Update on wide- and ultra-widefield retinal imaging. Indian J Ophthalmol. 2015;63:575–81. doi: 10.4103/0301-4738.167122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Callaway NF, Mruthyunjaya P. Widefield imaging of retinal and choroidal tumors. Int J Retin Vitr. 2019;5:49. doi: 10.1186/s40942-019-0196-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Ye PP, Xu J, Su ZT, Fang XY, Yao K. The application of ultra-wide-field fundus autofluorescence in early metastatic choroidal tumor screening. Int J Ophthalmol. 2019;12:1978–81. doi: 10.18240/ijo.2019.12.22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Kernt M, Schaller UC, Stumpf C, Ulbig MW, Kampik A, Neubauer AS. Choroidal pigmented lesions imaged by ultra-wide-field scanning laser ophthalmoscopy with two laser wavelengths (Optomap) Clin Ophthalmol. 2010;4:829–36. doi: 10.2147/opth.s11864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Reznicek L, Stumpf C, Seidensticker F, Kampik A, Neubauer AS, Kernt M. Role of wide-field autofluorescence imaging and scanning laser ophthalmoscopy in differentiation of choroidal pigmented lesions. Int J Ophthalmol. 2014;7:697–703. doi: 10.3980/j.issn.2222-3959.2014.04.21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Chen X, Sanfilippo CJ, Nagiel A, Hosseini H, Mitchell D, McCannel CA, et al. Early detection of retinal hemangioblastomas in Von hippel-lindau disease using ultra-widefield fluorescein angiography. Retina (Philadelphia, Pa) 2018;38:748–54. doi: 10.1097/IAE.0000000000001601. [DOI] [PubMed] [Google Scholar]
- 101.Kumar P, Ravani R, Agarwal S, Dhanda S, Kumar V. Insights into retinal hemangioblastoma using ultra widefield imaging. Indian J Ophthalmol. 2019;67:2029–34. doi: 10.4103/ijo.IJO_802_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Mansfield Smith S, Makam R, Sullivan L, Sandford R, Allen L. Is ultra wide-field retinal imaging alone appropriate for retinal angioma screening in lower risk subjects attending Von Hippel-Lindau (VHL) clinics? Ophthalmic Genet. 2019;40:403–6. doi: 10.1080/13816810.2019.1678177. [DOI] [PubMed] [Google Scholar]
- 103.Venkatesh P, Takkar B. Proposed classification system for retinal capillary angiomatosis. Ophthalmic Res. 2019;61:115–9. doi: 10.1159/000494498. [DOI] [PubMed] [Google Scholar]