

It has been over a year since the first case of severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) infection was announced in China on 31 December 2019. By 21 December 2020, there were more than 70 million confirmed cases of coronavirus disease 2019 (COVID‐19), over 1.6 million deaths and about 46 million recovered patients 1 . We grieve for those who lost their lives to this unprecedented pandemic and we thank all healthcare workers for their outstanding effort in combating COVID‐19. In this Opinion, we provide a timeline of the scientific research and main events in relation to COVID‐19 (Figure 1), focusing mainly on the obstetric and gynecological settings and the contribution of Ultrasound in Obstetrics & Gynecology (UOG).
Figure 1.
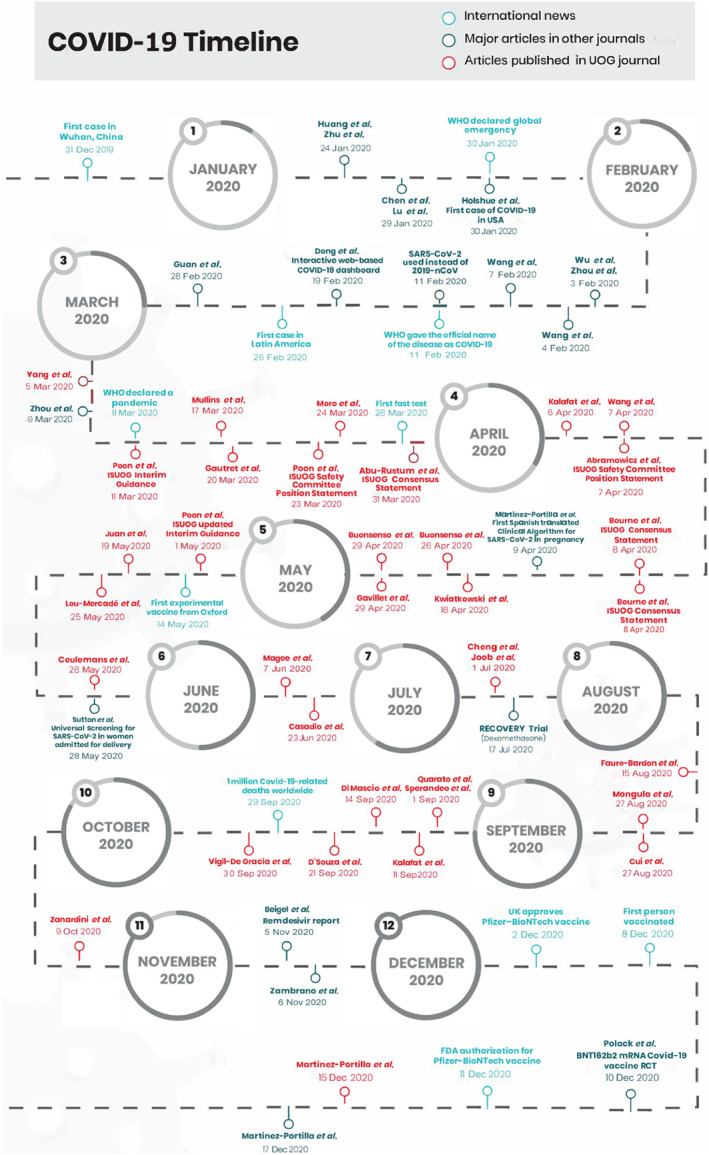
COVID‐19 timeline
The beginning of the unknown
On 31 December 2019, the Chinese government reported a series of patients with pneumonia of unknown cause. On 24 January 2020, Huang et al. 2 and Zhu et al. 3 reported a series of cases related to a previously unknown coronavirus, which was different from Middle East respiratory syndrome coronavirus (MERS‐CoV) and severe acute respiratory syndrome coronavirus (SARS‐CoV). On 29 January, Lu et al. 4 reported the genome sequence of the virus and stated that it was sufficiently divergent from that of SARS‐CoV to be considered a new infecting beta‐coronavirus, while on the same day, Chen et al. 5 described the clinical characteristics associated with the 2019 novel coronavirus (2019‐nCoV) infection and showed that older men with comorbidities were at an increased risk of severe and even fatal respiratory disease.
On 30 January, the World Health Organization (WHO) declared a global emergency when the first case of 2019‐nCoV infection was reported in the USA by Holshue et al. 6 . On 3 February, when the number of confirmed new cases worldwide jumped to 2794, Wu et al. 7 and Zhou et al. 8 demonstrated that the genome sequence of 2019‐nCoV was 96% identical to that of a bat coronavirus, supporting the idea of a trans‐species mutation. On 4 February, Wang et al. 9 showed that remdesivir was effective against 2019‐nCoV in in‐vitro studies. Three days later, Wang et al. 10 reported a 4.3% mortality rate in 138 hospitalized patients with 2019‐nCoV in Wuhan, China. On 11 February, the name of the virus was changed from ‘2019‐nCoV’ to ‘SARS‐CoV‐2’ 11 , and subsequently, WHO designated ‘coronavirus disease 2019 (COVID‐19)’ as the official name for the disease caused by SARS‐CoV‐2. Shortly after, the Johns Hopkins Coronavirus Resource Center was created to track all cases around the world 1 . On 26 February, the first case of COVID‐19 in Latin America was described 12 . In order to better understand how this new disease affected the population, Guan et al. 13 reported on the first 1099 laboratory‐confirmed cases of COVID‐19 from 552 hospitals in 30 provinces in China, demonstrating a median incubation period of the virus of 4 days and that ground‐glass opacity was the most common finding on chest computed tomography (CT) imaging, observed in 56.4% of patients on admission.
Ultrasound in Obstetrics & Gynecology in action
On 5 March 2020, the first manuscript in UOG related to COVID‐19 was published, by Yang et al. 14 , describing the clinical manifestations of SARS‐CoV‐2 infection during pregnancy and raising concerns about the possibility of vertical transmission. Four days later, in The Lancet, Zhou et al. 15 described an association between poor prognosis of patients with COVID‐19 and risk factors, such as older age, high sequential organ failure assessment score and D‐dimer > 1 mg/mL on admission.
On 11 March, WHO declared the COVID‐19 outbreak a pandemic. It was on the same day that UOG published the first International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) Interim Guidance on COVID‐19 during pregnancy and puerperium 16 , providing important information for healthcare professionals about the diagnosis and management of SARS‐CoV‐2 infection in pregnant women. On 17 March, Mullins et al. 17 published the first rapid review on COVID‐19 in pregnancy, based on the first 32 reported cases of SARS‐CoV‐2 infection during pregnancy, according to which COVID‐19 appeared to be less lethal than SARS‐CoV and MERS‐CoV infection and to be associated with a preterm delivery rate of 47%, while there were no cases of vertical transmission. Soon after, Gautret et al. 18 published an open‐label non‐randomized clinical trial on the use of hydroxychloroquine (HCQ) and azithromycin as treatments for COVID‐19, showing promising results but lacking adequate methodology. The latest meta‐analysis, based on seven randomized trials and 14 cohort studies, showed that HCQ with and without azithromycin lacks efficacy in reducing short‐term mortality in hospitalized patients with COVID‐19 or the risk of hospitalization in outpatients with COVID‐19 19 . On 23 March, the ISUOG Safety Committee Position Statement on the safe performance of obstetric and gynecological scans and equipment cleaning in the context of COVID‐19 was published 20 . Subsequently, Moro et al. 21 illustrated a practical approach to perform lung ultrasound examination in pregnant women; lung ultrasound was utilized widely for the diagnosis of pneumonia in pregnant women at the peak of the epidemic in Italy, as it was not always possible to perform CT chest imaging. On 28 March, the first fast test for SARS‐CoV‐2 was developed 22 . On 31 March, the ISUOG Consensus Statement on how to organize routine and specialized obstetric ultrasound services in the context of COVID‐19 was published 23 .
In the eye of the storm
With the number of COVID‐19 cases increasing exponentially, the possibility of vertical transmission was a growing concern. On 7 April, Wang et al. 24 concluded that, based on available data, there was no concrete evidence of vertical transmission of SARS‐CoV‐2, but further high‐quality research was needed. At the same time, Kalafat et al. 25 published one of the first descriptions of CT and lung ultrasound findings in a pregnant woman with COVID‐19.
After 3 months of intense research into this new disease, information was gathered from different parts of the world and a number of key documents were published by ISUOG to ensure the safety and adequate practice of all sonographers. On 7 April, the ISUOG Safety Committee Position Statement on the safe use of personal protective equipment and hazard mitigation for practitioners undertaking obstetric and gynecological ultrasound 26 was published, describing steps to minimize the risk of SARS‐CoV‐2 transmission between the patient and the practitioner during ultrasound examinations. On the next day, two ISUOG Consensus Statements, one on rationalization of early‐pregnancy care and provision of ultrasonography 27 and the second on rationalization of gynecological ultrasound services 28 in the context of SARS‐CoV‐2, were published, acknowledging the need to perform only the most necessary scans during the COVID‐19 pandemic. On 9 April, the first Spanish‐translated algorithm for the management of pregnant women with suspected COVID‐19 was released for Latin American countries 29 . A few days later, Kwiatkowski et al. 30 advocated that clinicians should not stop prescribing aspirin to pregnant women who are identified as high risk for pre‐eclampsia and fetal growth restriction during the pandemic, stating that the benefits of pre‐eclampsia prevention outweigh the potential risks of adverse outcome related to the use of aspirin in patients with SARS‐CoV‐2 infection. In contrast to this opinion, Gavillet et al. 31 recommended that aspirin for the prevention of pre‐eclampsia should be stopped upon diagnosis of SARS‐CoV‐2 infection, especially in women in the third trimester in whom the benefit of aspirin is minimal and could contribute to severe bleeding. Currently, professional bodies do not recommend stopping clinically indicated non‐steroidal anti‐inflammatory drugs in patients with COVID‐19, and it has been shown that low‐dose aspirin is safe at all stages during pregnancy. Besides, studies in non‐pregnant populations suggest that low‐dose aspirin intake may improve COVID‐19 outcome 32 .
With regard to diagnostic tools for COVID‐19, Buonsenso et al. 33 , 34 illustrated that lung ultrasound could be used by obstetricians to assess lung involvement in pregnant women with COVID‐19, and that this method is as sensitive as a chest X‐ray in detecting SARS‐CoV‐2 pneumonia. On 1 May 2020, ISUOG updated the Interim Guidance on SARS‐CoV‐2 during pregnancy and puerperium 35 , re‐defining the definition of suspected cases of COVID‐19 according to that proposed by WHO and adding new information with respect to mortality rates, diagnostic modalities, such as lung ultrasound, triage of patients, place of care, referral to the intensive care unit (ICU), management of non‐severe and critical disease during pregnancy, outpatient and inpatient antenatal care, fetal monitoring and ultrasound, management during childbirth and risk of vertical transmission. On 14 May, news regarding the first experimental vaccine from Oxford was like an oasis in the middle of the dessert, at a time when the pandemic in Europe was at a peak leading to a huge strain on healthcare systems. A few days later, a systematic review on the effect of COVID‐19 on maternal, perinatal and neonatal outcome was published in UOG, demonstrating that despite the increasing number of published studies on COVID‐19 in pregnancy, there were insufficient good‐quality data to draw unbiased conclusions with regard to complications in pregnant women as well as vertical transmission and perinatal complications 36 .
Concerns regarding COVID‐19‐associated thrombosis due to the inflammatory process in response to the disease, drove Lou‐Mercadé and colleagues 37 to propose a clinical management algorithm for the prevention of thrombosis in pregnant women with suspected SARS‐CoV‐2 infection. Meanwhile, Ceulemans et al. 38 evaluated the effectiveness of COVID‐19 screening at childbirth, showing a screen‐positive rate of 2.8% in 473 participants. On 28 May, at the time when New York City was at the center of the pandemic, the first study on universal screening for SARS‐CoV‐2 in an obstetric population was published in The New England Journal of Medicine, showing that, out of 215 pregnant women admitted to the labor and delivery unit of a hospital in New York City, 84.6% tested negative for SARS‐CoV‐2, while of those who tested positive, 87.7% were asymptomatic and only 12.3% were symptomatic 39 . These findings raised the alarm and indicated that all pregnant women, irrespective of symptoms, should be treated as SARS‐CoV‐2‐positive in areas with widespread transmission.
Six months and counting
On 7 June, Magee et al. 40 proposed a clinical management protocol for women with hypertension in pregnancy, showing that a shared model of care in order to diagnose and manage remotely pregnancy hypertension was possible. On 23 June, Casadio et al. 41 reported an 40.8% increase in the rate of ruptured ectopic pregnancy in northern Italy, likely reflecting the lack of consultations in early pregnancy due to lockdown.
At the beginning of July, Cheng et al. 42 raised concerns about the validity of the conclusion of a review 17 that COVID‐19 is associated with a low rate of maternal mortality, considering that this was based on a small number of affected cases. At the same time, Joob and Wiwanitkit 43 raised concerns about the usefulness of lung ultrasound, particularly in low‐resource countries with limited availability of ultrasound equipment. On 17 July, results from the RECOVERY trial 44 were published, showing that dexamethasone reduced mortality among COVID‐19‐hospitalized individuals; this was the first drug with positive results on COVID‐19.
In August, the possibility of vertical transmission due to the expression of angiotensin‐converting enzyme receptors on placental tissue was demonstrated 45 , 46 , but there was no clinical evidence. On 27 August, Mongula et al. 47 described a case of non‐reassuring fetal heart rate related to placental damage due to placental SARS‐CoV‐2 infection.
In early September, Kalafat et al. 48 showed that the use of lung ultrasound scoring could facilitate the early diagnosis of symptomatic women with probable SARS‐CoV‐2 infection and could be useful for managing patients when testing capacity is strained or when waiting for testing results is not an option. At the same time, Quarato et al. 49 and Sperandeo and Trovato 50 challenged the role of lung ultrasound in the diagnosis and monitoring of SARS‐CoV‐2 pneumonia. On 14 September, The WAPM (World Association of Perinatal Medicine) Working Group reported on the maternal and perinatal outcomes of one of the largest cohorts (at the time) of pregnant women with SARS‐CoV‐2 infection 51 . In a multinational cohort of 388 women with a singleton pregnancy affected by SARS‐CoV‐2 infection, the authors found that 11.1% were admitted to the ICU, 9.3% required mechanical ventilation and 0.8% died. Only one (0.4%) newborn tested positive for SARS‐CoV‐2, suggesting that the risk of vertical transmission seems to be negligible 51 . On 21 September, D'Souza et al. 52 reported on the pharmacological considerations during pregnancy in the context of COVID‐19. On 29 September, sadly, the world reached 1 million COVID‐19‐related deaths. On the next day, Vigil‐De Gracia et al. 53 provided data on the perinatal outcome of 15 women who recovered from COVID‐19, and showed that, even after recovery, these women remained at high risk of preterm delivery.
In October, Zanardini et al. 54 raised awareness of the possibility of pregnant women retesting positive for SARS‐CoV‐2, and suggested that these women should be managed as potentially infectious.
The last stretch
At the beginning of November, Beigel et al. 55 published the final report of their randomized controlled trial on remdesivir, showing a faster recovery time compared to placebo in individuals who were hospitalized with COVID‐19 and demonstrating evidence of lower rate of respiratory tract infection. This was the second drug that showed a positive effect in hospitalized patients with COVID‐19.
On 2 December, the UK approved the use of the mRNA vaccine (Pfizer‐BioNTech) based on pre‐published data. On 8 December, the first person was vaccinated and we started to see the light at the end of the tunnel; the whole world, tired of the pandemic, watched the beginning of the possible end of this battle against COVID‐19. Two days later, Polack et al. 56 , in a large randomized trial on 43 448 participants, showed a 95% effectiveness of the Pfizer‐BioNTech mRNA vaccine in preventing COVID‐19 within the first 2 months following two doses of the vaccine. These promising results were celebrated by the whole world. On 11 December, the US Food and Drug Administration granted authorization for the emergency use of the Pfizer‐BioNTech mRNA vaccine. On 15 December, Martinez‐Portilla et al. 57 demonstrated, in the largest cohort of pregnant women with COVID‐19 (n = 5183) at the time, that pregnancy is a risk factor for mortality, pneumonia and ICU admission, similar to the data from the USA 58 . This was the last article, amongst a total of 31 manuscripts related to COVID‐19, published in UOG in 2020. Soon after, the same researchers showed that young age is not a protective factor for mortality and pneumonia among pregnant women with COVID‐19, and urged that all pregnant women with symptoms, irrespective of age, should seek medical attention immediately 59 .
Even though we are still fighting against COVID‐19, there is growing evidence that science will eventually beat this pandemic. We applaud the contribution of all practitioners and thank everyone involved in deciphering this novel virus. The combined effort of researchers around the world has led to better health practice and improved safety and care of pregnant women during the COVID‐19 pandemic.
ACKNOWLEDGMENT
We thank Alejadra Estefanía Santillán Macías for her help with developing the timeline.
REFERENCES
- 1. Dong E, Du H, Gardner L. An interactive web‐based dashboard to track COVID‐19 in real time. Lancet Infect Dis 2020; 20: 533–534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng Z, Yu T, Xia J, Wei Y, Wu W, Xie X, Yin W, Li H, Liu M, Xiao Y, Gao H, Guo L, Xie J, Wang G, Jiang R, Gao Z, Jin Q, Wang J, Cao B. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020; 395: 497–506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, Zhao X, Huang B, Shi W, Lu R, Niu P, Zhan F, Ma X, Wang D, Xu W, Wu G, Gao GF, Tan W, China Novel Coronavirus Investigating and Research Team . A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med 2020; 382: 727–733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Lu R, Zhao X, Li J, Niu P, Yang B, Wu H, Wang W, Song H, Huang B, Zhu N, Bi Y, Ma X, Zhan F, Wang L, Hu T, Zhou H, Hu Z, Zhou W, Zhao L, Chen J, Meng Y, Wang J, Lin Y, Yuan J, Xie Z, Ma J, Liu WJ, Wang D, Xu W, Holmes EC, Gao GF, Wu G, Chen W, Shi W, Tan W. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet 2020; 395: 565–574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, Qiu Y, Wang J, Liu Y, Wei Y, Xia J, Yu T, Zhang X, Zhang L. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 2020; 395: 507–513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Holshue ML, DeBolt C, Lindquist S, Lofy KH, Wiesman J, Bruce H, Spitters C, Ericson K, Wilkerson S, Tural A, Diaz G, Cohn A, Fox L, Patel A, Gerber SI, Kim L, Tong S, Lu X, Lindstrom S, Pallansch MA, Weldon WC, Biggs HM, Uyeki TM, Pillai SK, Washington State 2019‐nCoV Case Investigation Team . First Case of 2019 Novel Coronavirus in the United States. N Engl J Med 2020; 382: 929–936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Wu F, Zhao S, Yu B, Chen YM, Wang W, Song ZG, Hu Y, Tao ZW, Tian JH, Pei YY, Yuan ML, Zhang YL, Dai FH, Liu Y, Wang QM, Zheng JJ, Xu L, Holmes EC, Zhang YZ. A new coronavirus associated with human respiratory disease in China. Nature 2020; 579: 265–269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Zhou P, Yang XL, Wang XG, Hu B, Zhang L, Zhang W, Si HR, Zhu Y, Li B, Huang CL, Chen HD, Chen J, Luo Y, Guo H, Jiang RD, Liu MQ, Chen Y, Shen XR, Wang X, Zheng XS, Zhao K, Chen QJ, Deng F, Liu LL, Yan B, Zhan FX, Wang YY, Xiao GF, Shi ZL. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020; 579: 270–273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Wang M, Cao R, Zhang L, Yang X, Liu J, Xu M, Shi Z, Hu Z, Zhong W, Xiao G. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019‐nCoV) in vitro. Cell Res 2020; 30: 269–271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, Wang B, Xiang H, Cheng Z, Xiong Y, Zhao Y, Li Y, Wang X, Peng Z. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus‐Infected Pneumonia in Wuhan, China. JAMA 2020; 323: 1061–1069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Coronaviridae Study Group of the International Committee on Taxonomy of V . The species Severe acute respiratory syndrome‐related coronavirus: classifying 2019‐nCoV and naming it SARS‐CoV‐2. Nat Microbiol 2020; 5: 536–544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Schwartz L. Brazil Confirms First Case of COVID‐19 in Latin America. https://www.medscape.com/viewarticle/925806
- 13. Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, Liu L, Shan H, Lei CL, Hui DSC, Du B, Li LJ, Zeng G, Yuen KY, Chen RC, Tang CL, Wang T, Chen PY, Xiang J, Li SY, Wang JL, Liang ZJ, Peng YX, Wei L, Liu Y, Hu YH, Peng P, Wang JM, Liu JY, Chen Z, Li G, Zheng ZJ, Qiu SQ, Luo J, Ye CJ, Zhu SY, Zhong NS, for the China Medical Treatment Expert Group for Covid‐19 . Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med 2020; 382: 1708–1720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Yang H, Wang C, Poon LC. Novel coronavirus infection and pregnancy. Ultrasound Obstet Gynecol 2020; 55: 435–437. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, Xiang J, Wang Y, Song B, Gu X, Guan L, Wei Y, Li H, Wu X, Xu J, Tu S, Zhang Y, Chen H, Cao B. Clinical course and risk factors for mortality of adult inpatients with COVID‐19 in Wuhan, China: a retrospective cohort study. Lancet 2020; 395: 1054–1062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Poon LC, Yang H, Lee JCS, Copel JA, Leung TY, Zhang Y, Chen D, Prefumo F. ISUOG Interim Guidance on 2019 novel coronavirus infection during pregnancy and puerperium: information for healthcare professionals. Ultrasound Obstet Gynecol 2020; 55: 700–708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Mullins E, Evans D, Viner RM, O'Brien P, Morris E. Coronavirus in pregnancy and delivery: rapid review. Ultrasound Obstet Gynecol 2020; 55: 586–592. [DOI] [PubMed] [Google Scholar]
- 18. Gautret P, Lagier JC, Parola P, Hoang VT, Meddeb L, Mailhe M, Doudier B, Courjon J, Giordanengo V, Vieira VE, Tissot Dupont H, Honore S, Colson P, Chabriere E, La Scola B, Rolain JM, Brouqui P, Raoult D. Hydroxychloroquine and azithromycin as a treatment of COVID‐19: results of an open‐label non‐randomized clinical trial. Int J Antimicrob Agents 2020; 56: 105949. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 19. Kashour Z, Riaz M, Garbati MA, AlDosary O, Tlayjeh H, Gerberi D, Murad MH, Sohail MR, Kashour T, Tleyjeh IM. Efficacy of chloroquine or hydroxychloroquine in COVID‐19 patients: a systematic review and meta‐analysis. J Antimicrob Chemother 2021; 76: 30–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Poon LC, Abramowicz JS, Dall'Asta A, Sande R, Ter Haar G, Marsal K, Brezinka C, Miloro P, Basseal J, Westerway SC, Abu‐Rustum RS, Lees C. ISUOG Safety Committee Position Statement on safe performance of obstetric and gynecological scans and equipment cleaning in context of COVID‐19. Ultrasound Obstet Gynecol 2020; 55: 709–712. [DOI] [PubMed] [Google Scholar]
- 21. Moro F, Buonsenso D, Moruzzi MC, Inchingolo R, Smargiassi A, Demi L, Larici AR, Scambia G, Lanzone A, Testa AC. How to perform lung ultrasound in pregnant women with suspected COVID‐19. Ultrasound Obstet Gynecol 2020; 55: 593–598. [DOI] [PubMed] [Google Scholar]
- 22. Hauck G. ‘A game changer’: FDA authorizes Abbott Labs' portable, 5‐minute coronavirus test the size of a toaster. https://eu.usatoday.com/story/news/health/2020/03/28/coronavirus‐fda‐authorizes‐abbott‐labs‐fast‐portable‐covid‐test/2932766001/
- 23. Abu‐Rustum RS, Akolekar R, Sotiriadis A, Salomon LJ, Costa FDS, Wu Q, Frusca T, Bilardo CM, Prefumo F, Poon LC. ISUOG Consensus Statement on organization of routine and specialist obstetric ultrasound services in context of COVID‐19. Ultrasound Obstet Gynecol 2020; 55: 863–870. [DOI] [PubMed] [Google Scholar]
- 24. Wang C, Zhou YH, Yang HX, Poon LC. Intrauterine vertical transmission of SARS‐CoV‐2: what we know so far. Ultrasound Obstet Gynecol 2020; 55: 724–725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Kalafat E, Yaprak E, Cinar G, Varli B, Ozisik S, Uzun C, Azap A, Koc A. Lung ultrasound and computed tomographic findings in pregnant woman with COVID‐19. Ultrasound Obstet Gynecol 2020; 55: 835–837. [DOI] [PubMed] [Google Scholar]
- 26. Abramowicz JS, Basseal JM, Brezinka C, Dall'Asta A, Deng J, Harrison G, Lee JCS, Lim A, Marsal K, Miloro P, Poon LC, Salvesen KA, Sande R, Ter Haar G, Westerway SC, Xie MX, Lees C. ISUOG Safety Committee Position Statement on use of personal protective equipment and hazard mitigation in relation to SARS‐CoV‐2 for practitioners undertaking obstetric and gynecological ultrasound. Ultrasound Obstet Gynecol 2020; 55: 886–891. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Bourne T, Kyriacou C, Coomarasamy A, Al‐Memar M, Leonardi M, Kirk E, Landolfo C, Blanchette‐Porter M, Small R, Condous G, Timmerman D. ISUOG Consensus Statement on rationalization of early‐pregnancy care and provision of ultrasonography in context of SARS‐CoV‐2. Ultrasound Obstet Gynecol 2020; 55: 871–878. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Bourne T, Leonardi M, Kyriacou C, Al‐Memar M, Landolfo C, Cibula D, Condous G, Metzger U, Fischerova D, Timmerman D, van den Bosch T. ISUOG Consensus Statement on rationalization of gynecological ultrasound services in context of SARS‐CoV‐2. Ultrasound Obstet Gynecol 2020; 55: 879–885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Martinez‐Portilla RJ, Gonce A, Hawkins‐Villarreal A, Figueras F. A Spanish‐translated clinical algorithm for management of suspected SARS‐CoV‐2 infection in pregnant women. Lancet Infect Dis 2020; 20: 655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Kwiatkowski S, Borowski D, Kajdy A, Poon LC, Rokita W, Wielgos M. Why we should not stop giving aspirin to pregnant women during the COVID‐19 pandemic. Ultrasound Obstet Gynecol 2020; 55: 841–843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Gavillet M, Rolnik DL, Hoffman MK, Panchaud A, Baud D. Should we stop aspirin prophylaxis in pregnant women diagnosed with COVID‐19? Ultrasound Obstet Gynecol 2020; 55: 843–844. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Chow JH, Khanna AK, Kethireddy S, Yamane D, Levine A, Jackson AM, McCurdy MT, Tabatabai A, Kumar G, Park P, Benjenk I, Menaker J, Ahmed N, Glidewell E, Presutto E, Cain S, Haridasa N, Field W, Fowler JG, Trinh D, Johnson KN, Kaur A, Lee A, Sebastian K, Ulrich A, Pena S, Carpenter R, Sudhakar S, Uppal P, Fedeles BT, Sachs A, Dahbour L, Teeter W, Tanaka K, Galvagno SM, Herr DL, Scalea TM, Mazzeffi MA. Aspirin Use is Associated with Decreased Mechanical Ventilation, ICU Admission, and In‐Hospital Mortality in Hospitalized Patients with COVID‐19. Anesth Analg 2020. DOI: 10.1213/ANE.0000000000005292. [DOI] [PubMed] [Google Scholar]
- 33. Buonsenso D, Raffaelli F, Tamburrini E, Biasucci DG, Salvi S, Smargiassi A, Inchingolo R, Scambia G, Lanzone A, Testa AC, Moro F. Clinical role of lung ultrasound for diagnosis and monitoring of COVID‐19 pneumonia in pregnant women. Ultrasound Obstet Gynecol 2020; 56: 106–109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Buonsenso D, Moro F, Inchingolo R, Smargiassi A, Demi L, Soldati G, Moroni R, Lanzone A, Scambia G, Testa AC. Effectiveness of rapid lung ultrasound training program for gynecologists and obstetricians managing pregnant women with suspected COVID‐19. Ultrasound Obstet Gynecol 2020; 56: 110–111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Poon LC, Yang H, Dumont S, Lee JCS, Copel JA, Danneels L, Wright A, Costa FDS, Leung TY, Zhang Y, Chen D, Prefumo F. ISUOG Interim Guidance on coronavirus disease 2019 (COVID‐19) during pregnancy and puerperium: information for healthcare professionals – an update. Ultrasound Obstet Gynecol 2020; 55: 848–862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Juan J, Gil MM, Rong Z, Zhang Y, Yang H, Poon LC. Effect of coronavirus disease 2019 (COVID‐19) on maternal, perinatal and neonatal outcome: systematic review. Ultrasound Obstet Gynecol 2020; 56: 15–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Lou‐Mercadé AC, Gavin O, Oros D, Paules C, Saviron‐Cornudella R, Mateo P, Paramo JA, Ruiz‐Martinez S. Prevention of thrombosis in pregnant women with suspected SARS‐CoV‐2 infection: clinical management algorithm. Ultrasound Obstet Gynecol 2020; 56: 111–112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Ceulemans D, Thijs I, Schreurs A, Vercammen J, Lannoo L, Deprest J, Richter J, De Catte L, Devlieger R. Screening for COVID‐19 at childbirth: is it effective? Ultrasound Obstet Gynecol 2020; 56: 113–114. [DOI] [PubMed] [Google Scholar]
- 39. Sutton D, Fuchs K, D'Alton M, Goffman D. Universal Screening for SARS‐CoV‐2 in Women Admitted for Delivery. N Engl J Med 2020; 382: 2163–2164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Magee LA, Khalil A, von Dadelszen P. Pregnancy hypertension diagnosis and care in COVID‐19 era and beyond. Ultrasound Obstet Gynecol 2020; 56: 7–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Casadio P, Youssef A, Arena A, Gamal N, Pilu G, Seracchioli R. Increased rate of ruptured ectopic pregnancy in COVID‐19 pandemic: analysis from the North of Italy. Ultrasound Obstet Gynecol 2020; 56: 289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Cheng SO, Khan S, Alsafi Z. Maternal death in pregnancy due to COVID‐19. Ultrasound Obstet Gynecol 2020; 56: 122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Joob B, Wiwanitkit V. Lung ultrasound in pregnant women with suspicion of COVID‐19. Ultrasound Obstet Gynecol 2020; 56: 123–124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. RECOVERY Collaborative Group , Horby P, Lim WS, Emberson JR, Mafham M, Bell JL, Linsell L, Staplin N, Brightling C, Ustianowski A, Elmahi E, Prudon B, Green C, Felton T, Chadwick D, Rege K, Fegan C, Chappell LC, Faust SN, Jaki T, Jeffery K, Montgomery A, Rowan K, Juszczak E, Baillie JK, Haynes R, Landray MJ. Dexamethasone in Hospitalized Patients with Covid‐19 – Preliminary Report. N Engl J Med 2020. DOI: 10.1056/NEJMoa2021436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Faure‐Bardon V, Isnard P, Roux N, Leruez‐Ville M, Molina T, Bessieres B, Ville Y. Protein expression of angiotensin‐converting enzyme 2, a SARS‐CoV‐2 specific receptor, in fetal and placental tissues throughout gestation: new insight for perinatal counseling. Ultrasound Obstet Gynecol 2021; 57: 242–247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Cui D, Liu Y, Jiang X, Ding C, Poon LC, Wang H, Yang H. Single‐cell RNA expression profiling of SARS‐CoV‐2‐related ACE2 and TMPRSS2 in human trophectoderm and placenta. Ultrasound Obstet Gynecol 2021; 57: 248–256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Mongula JE, Frenken MWE, van Lijnschoten G, Arents NLA, de Wit‐Zuurendonk LD, Schimmel‐de Kok APA, van Runnard Heimel PJ, Porath MM, Goossens S. COVID‐19 during pregnancy: non‐reassuring fetal heart rate, placental pathology and coagulopathy. Ultrasound Obstet Gynecol 2020; 56: 773–776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Kalafat E, Yassa M, Koc A, Tug N, the TULIP collaboration . Utility of lung ultrasound assessment for probable SARS‐CoV‐2 infection during pregnancy and universal screening of asymptomatic individuals. Ultrasound Obstet Gynecol 2020; 56: 624–626. [DOI] [PubMed] [Google Scholar]
- 49. Quarato CMI, Venuti M, Lacedonia D, Simeone A, Sperandeo M. Diagnosis and monitoring of COVID‐19 pneumonia in pregnant women: is lung ultrasound appropriate? Ultrasound Obstet Gynecol 2020; 56: 467–468. [DOI] [PubMed] [Google Scholar]
- 50. Sperandeo M, Trovato GM. Care of future mothers amid the COVID‐19 outbreak: is there a monitoring role for lung ultrasound? Ultrasound Obstet Gynecol 2020; 56: 469–470. [DOI] [PubMed] [Google Scholar]
- 51. The WAPM (World Association of Perinatal Medicine) Working Group on COVID‐19. Maternal and perinatal outcomes of pregnant women with SARS‐CoV‐2 infection. Ultrasound Obstet Gynecol 2021; 57: 232–241. [DOI] [PubMed] [Google Scholar]
- 52. D'Souza R, Ashraf R, Rowe H, Zipursky J, Clarfield L, Maxwell C, Arzola C, Lapinsky S, Paquette K, Murthy S, Cheng MP, Malhame I. Pregnancy and COVID‐19: pharmacologic considerations. Ultrasound Obstet Gynecol 2021; 57: 195–203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Vigil‐De Gracia P, Caballero LC, Sanchez J, Espinosa J, Campana S, Quintero A, Luo C, Ng J. Pregnancies recovered from SARS‐CoV‐2 infection in second or third trimester: obstetric evolution. Ultrasound Obstet Gynecol 2020; 56: 777–778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Zanardini C, Saccani B, Franceschetti L, Zatti S, Sartori E, Prefumo F. Retest positive for SARS‐CoV‐2 RNA in pregnant women recovered from COVID‐19. Ultrasound Obstet Gynecol 2020; 56: 948–949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Beigel JH, Tomashek KM, Dodd LE, Mehta AK, Zingman BS, Kalil AC, Hohmann E, Chu HY, Luetkemeyer A, Kline S, Lopez de Castilla D, Finberg RW, Dierberg K, Tapson V, Hsieh L, Patterson TF, Paredes R, Sweeney DA, Short WR, Touloumi G, Lye DC, Ohmagari N, Oh MD, Ruiz‐Palacios GM, Benfield T, Fatkenheuer G, Kortepeter MG, Atmar RL, Creech CB, Lundgren J, Babiker AG, Pett S, Neaton JD, Burgess TH, Bonnett T, Green M, Makowski M, Osinusi A, Nayak S, Lane HC, ACTT‐1 Study Group Members. Remdesivir for the Treatment of Covid‐19 – Final Report. N Engl J Med 2020; 383: 1813–1826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S, Perez JL, Perez Marc G, Moreira ED, Zerbini C, Bailey R, Swanson KA, Roychoudhury S, Koury K, Li P, Kalina WV, Cooper D, Frenck RW, Jr. , Hammitt LL, Tureci O, Nell H, Schaefer A, Unal S, Tresnan DB, Mather S, Dormitzer PR, Sahin U, Jansen KU, Gruber WC, C4591001 Clinical Trial Group . Safety and Efficacy of the BNT162b2 mRNA Covid‐19 Vaccine. N Engl J Med 2020; 383: 2603–2615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Martinez‐Portilla RJ, Sotiriadis A, Chatzakis C, Torres‐Torres J, Espino YSS, Sandoval‐Mandujano K, Castro‐Bernabe DA, Medina‐Jimenez V, Monarrez‐Martin JC, Figueras F, Poon LC. Pregnant women with SARS‐CoV‐2 infection are at higher risk of death and pneumonia: propensity score matched analysis of a nationwide prospective cohort (COV19Mx). Ultrasound Obstet Gynecol 2021; 57: 224–231. [DOI] [PubMed] [Google Scholar]
- 58. Zambrano LD, Ellington S, Strid P, Galang RR, Oduyebo T, Tong VT, Woodworth KR, Nahabedian JF 3rd, Azziz‐Baumgartner E, Gilboa SM, Meaney‐Delman D; CDC COVID‐19 Response Pregnancy and Infant Linked Outcomes Team. Update: Characteristics of Symptomatic Women of Reproductive Age with Laboratory‐Confirmed SARS‐CoV‐2 Infection by Pregnancy Status – United States, January 22 – October 3, 2020. MMWR Morb Mortal Wkly Rep 2020; 69: 1641–1647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Martinez Portilla RJ, Smith ER, He S, Torres JT, Espino‐Y‐Sosa S, Solis‐Paredes JM, Poon LC. Young pregnant women are also at an increased risk of mortality and severe illness due to COVID‐19: Analysis of the Mexican National Surveillance Program. Am J Obstet Gynecol 2020; S0002‐9378(20)32573‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]