

Abstract
Objectives
The current report describes a single operator's experience of the first use of smartglass technology as a facilitator of virtual support during TAVR proctoring.
Background
Restricted gatherings and containment measures during the ongoing COVID‐19 pandemic have a major impact on daily clinical practice. Interaction between peers is crucial in science, clinical practice, and education. In addition, there is also a growing importance of proctoring in interventional cardiology for structural heart disease. Virtual support may facilitate the wide implementation of remote proctoring.
Methods
A collaboration between a smartglass provider (Rods & Cones) and self‐expandable transcatheter aortic heart valve system (Medtronic) was initiated and tested extensively prior to TAVR procedures. Two cases were randomly selected for remote support. The light‐weight smartglass consisted of a full HD central camera, a 720p ×5 optical zoom camera, built‐in LED light, speaker and earphone jack, and an external visor to project data in a nonobstructive manner in the operators' view.
Results
Preprocedural detailed discussion of the cases between the proctor and the operator occurred via teleconferencing. Successful procedural virtual support was determined by the presence of a session coordinator, high quality of the central camera, high‐speed and stable wireless internet connection. Limitations were the relative discomfort of the earpieces, discordance between the central and zoom camera and the absence of visual fixation during head motions.
Conclusion
In a highly complex and demanding context such as TAVR, remote proctoring by means of virtual support is feasible and efficacious.
Keywords: COVID‐19, TAVR, virtual support
Abbreviations
- COVID‐19
coronavirus disease 2019
- HD
high definition
- ICT
information and communications technology
- LED
light‐emitting diode
- TAVR
transcatheter aortic valve replacement
1. INTRODUCTION
The impact of coronavirus disease 2019 (COVID‐19) pandemic on society and healthcare systems is extraordinary that requires extraordinary measures. Social distancing, local or national lockdowns, and restricted gatherings were part of containment measures after the exponential spread of COVID‐19 throughout the world with high mortality rate and unforeseen burden on healthcare resources. 1 , 2
Clinical decision making, critical appraisal of information, and feedback are crucial elements often occurring in near physical distance or even interaction in daily clinical practice and medical training. Especially for invasive (surgical) procedures, it is of utmost importance that the supervisor is nearby to assist, advice or correct the apprentice. In a previous report in this Journal, alternative methods for physical heart team meetings were presented. It was shown how technological advances can ensure the quality of heart team meetings while respecting the measures for mitigating risks of COVID‐19 spread. 3 In this article, we describe a virtual support device, with its advantages and limitations, that was used during proctoring for transcatheter aortic valve replacement (TAVR) procedures.
2. METHODS
The online proctoring solution was provided by a collaborative initiative between Rods&Cones (Virtual Support hardware and application; Amsterdam, the Netherlands) and Medtronic (Evolut transcatheter aortic heart valve system; MN).
The day prior to the TAVR procedure, the patients were discussed in detail between the proctor and the operator via teleconferencing. Patient and clinical characteristics, anatomic assessment, potential hurdles or complications related to specific features of individual cases were critically reviewed and possible solutions and backstops were discussed. The most relevant clinical characteristics are highlighted in Table 1.
TABLE 1.
Clinical characteristics
| Case | Age | LVEF (%) | AVA (cm2) and mean PG (mmHg) | Relevant comorbidities | Complicating factors for procedure | Size |
|---|---|---|---|---|---|---|
| 1 | 76 | 60 | 0.9–45 | AF; radiotherapy and surgery for larynx‐ and oesophaguscarcinoma; bilateral bullectomy for COPD with bullae | Left‐ and right‐sided hypertrophy with kissing walls; horizontal ascending aorta | Evolut R 34 |
| 2 | 84 | 50 | 1.0–45 | AF; IDDM; CKD; impairment after ischemic CVA | Left‐ and right‐sided hypertrophy with kissing walls; horizontal ascending aorta; tortuous bilateral iliac arteries and aorta | Evolut R 34 |
Abbreviations: AF, atrial fibrillation; AVA, aortic valve area; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CVA, cerebrovascular accident; IDDM, insulin‐dependent diabetes mellitus; LVEF, left ventricular ejection fraction; PG, pressure gradient.
3. RESULTS
The integrated smartglass for virtual support consists of a full HD central camera and a 720p ×5 optical zoom camera. It has also a built‐in LED light, built‐in speaker, and plug‐in earphone jack and an external visor to project images/videos without obstructing the operator's view (Figure 1). The glasses are lightweight (70 g) and can be worn over a safety (leaded) goggle (Figure 2). The smartglass is connected to the pocket unit that contains a battery pack and a smartphone. The application for virtual support is running on the smartphone either though a 4G or Wi‐Fi internet connection. The pocket unit battery can last for at least 5 hr of active video connection, and can also be recharged during an active session.
FIGURE 1.

Smartglass
FIGURE 2.

Smartglass on the operator over protective goggles
3.1. Smartglass app
Before starting the video call, the status of the remote expert is checked and the smartglass user is informed (on the visor) whether the remote expert is logged in. The application initiates a video call between the operator and the remote expert by focusing at the dedicated QR code which then translates into a command that triggers the session to be started. The remote expert is able to watch and follow the procedure together with the operator through the smartglass. The operator is able to communicate one‐on‐one with the remote expert through an ear‐ and microphone set plugged into the smartglass. In addition, written commands can be given that are projected in the visor (Figure 3).
FIGURE 3.
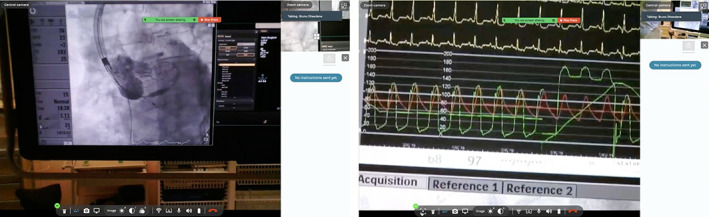
Remote expert's view through the central (left panel) and zoom (right panel) camera. Please note the blank area on the right side in each view that can be used for written commands from the remote expert to the operator
3.2. Coordinator
The active participation of a coordinator is shown to be crucial in the entire process of case preparation and online virtual support. In depth knowledge about the technology, its limitation and tweaking during a live session are critical to facilitate the operator and the remote expert in an optimal virtual environment. Wireless network quality with volatile down‐ and upload speed are known factors that often cause hitches during online sessions. A dedicated coordinator who can troubleshoot immediately is of utmost importance to facilitate a smooth experience for the operator and remote expert.
The coordinator can be someone from the hospital with vast experience in the used soft‐ and hardware, or a representative from the company related to the technology.
4. DISCUSSION
Telecommunication solutions have shown to be a necessity to continue our medical practice in the context of a global pandemic with restrictions to physical interaction. Given the growing interest in and interventions for structural heart disease, proctoring has become even more relevant to maintain a high standard for (interventional) skills and patient care. Virtual reality with extended functions (e.g., augmented reality and extended reality) with graphic avatars are being developed for surgical procedures in order to improve surgical precision and medical training. 4 , 5
In augmented reality mode, the most advantageous feature of a virtual environment is the simultaneous availability of complex data (e.g., imaging, physiology, clinical chemistry, etc.) in the physical world of the operating room. The next level of augmented reality would be the immediate adjustment of augmented data to unexpected changes during an invasive procedure, for example changes in physiological parameters or clinical chemistry during a complication.
The option to record an on‐line session is of great value for educational purposes. For the current proctoring sessions, it was the off‐line availability of the procedures that enabled all involved to critically appraise the procedure, the operator's handling and the remote expert's instructions. Since the procedures were recorded “through the eyes” of the operator, it also provides an opportunity to assess off‐line the frame of reference of the operator as part of the operating team.
4.1. Limitations
Technologies to improve or support the visual world are using devices that resemble eyeglasses. These so‐called smartglasses are usually made of light‐weight material and produced in one size or anatomic shape of the head. Hence, comfort in wearing these devices is usually suboptimal, especially when worn over protective goggles. In the current sessions, the maximum duration without experiencing pain by the operator at the ear region was just about 1 hr. The central and zoom camera's positions on the smartglass are not at the same place on the smartglass. Each time the remote expert wanted a zoom of the operator's view, the operator had to adjust the position of his head to find the area of interest. This results in unnecessary movements during a complex invasive procedure. The newer version of the used smartglass will have improved earpiece for wearing comfort, zoom function in the central camera (no need for additional zoom camera) and leaded protective glasses. A final device‐related disadvantage is the lack of visual fixation in smartglasses while the head is moving. The remote expert's view is entirely based on the visual information passed through the camera located on the smartglass, thus every single and little movement of the operator's head is transported 1:1 to the remote expert's screen with significant motion artifacts. Humans are capable of visual fixation to maintain their visual gaze on a certain (limited) area in space, while they move their head. Future studies and innovations in soft‐ and hardware technology are needed to simulate fixation.
It is without question that all virtual solutions are strongly depended on the quality of their (wireless) network through which they up‐ and download data. A well‐organized ICT department with high speed (preferably ultra‐high) network connections are key for a successful and enjoyable experience.
5. CONCLUSION
During COVID‐19 and perhaps beyond, remote proctoring by means of virtual support is feasible and efficacious. The most important advantage besides adhering to physical restrictions is the off‐line availability of a recorded session for critical appraisal of the procedure and proctor–operator interaction. The major limitations are the suboptimal wearing comfort, separated central and zoom camera and lack of visual fixation. A combined use of the presented technology and fixed imaging sources (X‐ray screen and hemodynamic monitor) could improve the interaction. Nevertheless, in an era of growing interest for proctoring among peers from different continents, virtual interactions are here to stay.
CONFLICT OF INTEREST
Fatih Arslan has no conflicts of interest to declare. Ulrich Gerckens is an international proctor for Medtronic.
ACKNOWLEDGMENTS
We would like to thank Dorien Peeters (technical consultant Structural Heart for Medtronic) and Bruno Dheedene (Founding Partner at Rods & Cones) for their technical support.
Arslan F, Gerckens U. Virtual support for remote proctoring in TAVR during COVID‐19. Catheter Cardiovasc Interv. 2021;98:E733–E736. 10.1002/ccd.29504
REFERENCES
- 1. EU . COVID‐19: the EU's response in the field of public health. https://wwwconsiliumeuropaeu/en/policies/coronavirus/covid-19-public-health/.
- 2. WHO . Coronavirus disease (COVID‐19) advice for the public. https://wwwwhoint/emergencies/diseases/novel‐coronavirus‐2019/advice‐for‐public.
- 3. Wahadat AR, Sadeghi AH, Tanis W. Heart team meetings during COVID‐19. Eur Heart J. 2020;41(20):1872‐1874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. NHS . Surgeons use virtual reality to operate from different sides of the world. https://wwwbartshealthnhsuk/news/surgeons-use-virtual-reality-to-operate-from-different-sides-of-the-world—2171.
- 5. NOS . Longkankeroperaties kunnen preciezer door VR‐bril, “Een absolute revolutie”. https://nosnl/artikel/2348972-longkankeroperaties-kunnen-preciezer-door-vr-bril-een-absolute-revolutiehtml.