

Abstract
As the SARS‐CoV‐2 infection rate decreased in spring 2020, phased reopening of Danish society began, including a reopening of elite football (soccer), adhering to a strict protocol. In this study, we report the consequences of resumption of competitive play in the two best football (soccer) leagues for men in Denmark measured by number of SARS‐CoV‐2 positive players. The players were tested weekly for SARS‐CoV‐2 for 11 consecutive weeks. The test protocol comprised 26 teams with 748 players. In total, 6511 tests were done with a positivity rate of 0.06%. The incidence rate of players testing positive for SARS‐CoV‐2 was 0.53% (4/748). There were no signs of a chain of infection. We found a low incidence rate of SARS‐CoV‐2, and based on this, a controlled reopening of professional football strictly following a detailed protocol appears safe for the players.
Keywords: 2019‐nCoV, athlete, coronavirus, COVID‐19, elite sport, football, SARS‐CoV‐2, soccer
1. INTRODUCTION
As the COVID‐19 pandemic caused by the virus SARS‐CoV‐2 spread throughout the world, most countries implemented measures to slow the spread, enforcing lockdowns of varying degrees. The first positive Danish COVID‐19 case was reported on February 27, 2020, and during the following weeks, there was a rapid increase in positive cases, reaching an initial peak on April 3, 2020. In an attempt to stop the spread of the virus, the Danish authorities closed all educational institutions and indoor cultural establishments—libraries, leisure facilities, etc; sent home all public servants not carrying out so‐called critical functions; and limited gatherings. These initiatives came into effect on March 13, 2020. All elite sport was paused, including that of the best football leagues.
As the infection rate decreased in Denmark in spring 2020, phased reopening of Danish society began. Phase 2 saw the reopening of the professional sports industry, and from May 7, professional sports matches without an audience were permitted. As part of the reopening, the Danish League (Divisionsforeningen) drew up a Protocol for the resumption of training and match play across all professional football competitions in Denmark during the SARS‐CoV‐2 pandemic. 1 The protocol was “produced to ensure the greatest possible safety for employees of the football clubs and to minimise the risk of spreading SARS‐CoV‐2 when training, external practice and competitive matches resume” and to “address both on‐ and off‐pitch risk factors for the health of the employees (players, club members and other staff) involved in training, external practice or competitive matches.” 2 The protocol sets out guidelines for clubs when planning individual training, external practice, and competitive matches. It is regularly revised and updated, taking into account the latest recommendations and guidelines issued by the Danish authorities and applying them to a footballing context.
In this study, we report the consequences of resumption of competitive play in the two best football leagues for men in Denmark measured by number of SARS‐CoV‐2‐positive players.
2. MATERIALS AND METHODS
As part of the protocol for the resumption of training and match play across all professional football competitions in Denmark during the COVID‐19 pandemic, it was described how to handle the players' health, monitoring of symptoms, and signs of infection with SARS‐CoV‐2. Players with typical symptoms of COVID‐19 were advised to immediately self‐isolate and follow the latest recommendations and guidelines from the Danish health authorities, contact their own general practitioner and follow the doctor's instructions. Further, self‐reported health checks for all on‐pitch staff were recommended, and players were instructed to complete a daily health questionnaire focusing on signs of SARS‐CoV‐2 infection, aiming to detect and heighten players' awareness of any symptoms. If a player had one or more symptoms (temperature >37.5 Celsius, sore throat, dry cough, headache, nausea, diarrhea, muscle pain, respiratory symptoms, or other symptoms), the player should report to the team's medical staff and was then allowed to train or play matches only if given clearance by the medical staff.
Further, a testing procedure was implemented for SARS‐CoV‐2 in asymptomatic on‐pitch staff and players. The test protocol comprised 26 teams: 14 from the best Danish national league (3F Superligaen) and 12 from the second best (NordicBet LIGA) league. The test program ran for the last 11 weeks of the 2019/2020 season, with the first tests performed on May 19 and the last tests on July 28.
The players were tested weekly for SARS‐CoV‐2 throughout the observation period using an isothermal amplification technology called strand invasion‐based amplification (SIBA®) 2 from Qlife Aps. The testing was not related to match days but was performed on the same day of the week every week. Only players were included in the present study. However, as part of the test protocol staff in the vicinity of the players were also tested, that is, coaches, health staff, etc.
A dry oropharyngeal swab was collected from all players. All samples were collected by external professional healthcare workers (doctors, nurses, or medical students) trained in collecting oropharyngeal swabs. The swab was dissolved in SIBA lysis/reaction buffer and an aliquot was transferred to the SIBA reaction mastermix and analyzed in a real‐time PCR instrument. The clinical study of the test method from Qlife is ongoing. All positive results were confirmed positive using E‐gene RT‐PCR assay. 3 Players who tested positive for SARS‐CoV‐2 were instructed to self‐isolate according to the latest guidelines from the health authorities. If a player tested positive, all other players from the same club underwent an additional test 4 days after the player's positive test result.
The project was presented to the Committee on Health Research Ethics for the Capital Region of Denmark; the study was deemed not to need ethics approval (ref. no. 20067687).
3. RESULTS
In total, 6511 tests were done in 748 different players, with a median of 673 (range 79‐770) tests performed each week. The clubs carried out a median of 244 (range 180‐332) tests during the observation period. Due to the structure of the playoffs with relegation and promotion matches as well as final playoff, some teams ended the playoff season earlier than others, and only clubs that played matches (friendly or competitive) were tested. As part of the playoff, only four teams played matches and were tested in the last test week of the observation period. Thus, not all clubs were tested every week and the number of weekly tests within the clubs also varied due to factors such as injuries and young players being added to the first team for certain matches. The players underwent a median of 9 tests (range 1‐12) (Figure 1).
FIGURE 1.
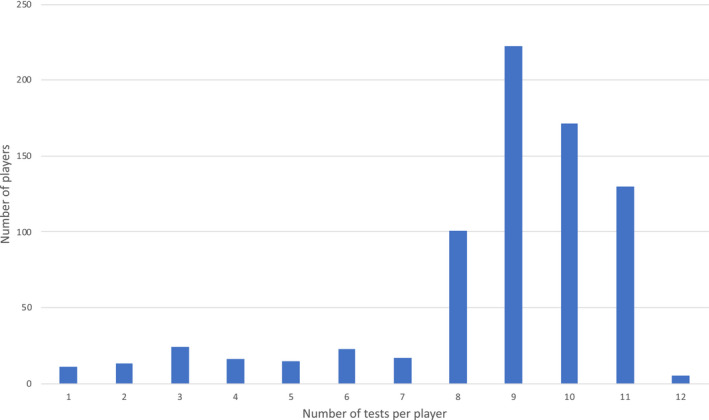
Tests per player during the observation period
Four tests were positive for SARS‐CoV‐2, giving a positivity rate of 0.06% positive tests during the observation period. The incidence rate of players testing positive for SARS‐CoV‐2 was 0.53% (4/748) in the 11‐week observation period. All the players testing positive were asymptomatic at the time of testing.
Among the players, one club had two, two clubs had one, and 23 had no positive cases. We have no data or information to conclude whether or not the two simultaneous cases in the same club occurred due to transmission between the players. No clubs had positive cases for consecutive weeks and no teams had positive cases more than once during the observation period.
4. DISCUSSION
Denmark was one of the first European countries to relax the restrictions to counter COVID‐19 and one of the first countries to allow return to elite football. To our knowledge, this is one of the first studies to report the consequences for the players of a controlled reopening of competitive sport.
We found a SARS‐CoV‐2 incidence rate of 0.53% in elite football players, with four players testing positive in the two best football leagues for men during an 11‐week observation period.
We do not have directly comparable data from the general Danish population as the results from elite football players are based on a weekly screening of all players, whereas the results from the general population represent a selected population. The incidence of COVID‐19 has varied considerably over time within the same country and substantial differences in incidences between countries have been found, making comparisons difficult. However, in the same period as this study, 0.06% of the tests performed on 20‐ to 39‐year‐olds in the general Danish population were positive. 4 We have no data on SARS‐CoV‐2 antibodies in Danish elite football players, but an observational study performed in April 2020 found a seroprevalence of 3.04% for IgG or IgM against SARS‐CoV‐2 in Danish blood donors. 5 Another Danish study looking at the effect of wearing face masks during April‐June 2020 found an incidence of SARS‐CoV‐2 infection (defined as a positive result of an oropharyngeal/nasal swab, development of a positive SARS‐CoV‐2 antibody test result, or hospital‐based diagnosis of SARS‐CoV‐2 infection or COVID‐19) of 2.1% in the control group during a 4‐week study period. 6 In a British screening of healthcare workers, 3% of those who were asymptomatic tested positive for SARS‐CoV‐2 using RT‐PCR from combined oropharyngeal and nasopharyngeal swabs. 7 In a screening for SARS‐CoV‐2 in women admitted for delivery in New York City during March 22‐April 4, 2020, 15.4% were positive for SARS‐CoV‐2 with the majority being asymptomatic when tested. 8 Compared with these numbers, the incidence rate of 0.53% in our study seems low. The low incidence rate is in accordance with a recently published cohort study in the two highest German leagues where ten out of 1079 players tested positive for SARS‐CoV‐2 during the 2 months study period. 9
We found no signs of a chain of infection as no team had positive cases for consecutive weeks. However, the low incidence of SARS‐CoV‐2 infection in the football players as well as in the community in the same period could have affected the risk of transmission and one cannot exclude that had the risk of transmission been higher, the prevalence of SARS‐CoV‐2 would also have been higher. Irrespective of the incidence, we would advocate implementing a return to play plan for SARS‐CoV‐2 infected athletes.
It is uncertain whether these results from elite football can be extrapolated to other types of professional sport. Environmental factors can influence the transmission of viral infections and it could be speculated that as football is an outdoor sport, it might differ from indoor sports regarding the risk of transmission from one player to another. Further, this study was conducted in the Danish spring and summer and the transmission rate might be different during autumn and winter. 10 Lastly, the degree of close physical contact varies greatly depending on the type of sport; this could play a role in the risk of transmission of SARS‐CoV‐2.
Based on the result of this study, a controlled reopening of professional football appears safe for the players as there is only a low risk of contracting SARS‐CoV‐2 infection. However, this is on the premise that a strict protocol is implemented, including thorough surveillance of possible spread, with clubs and players acting responsibly and complying with guidelines and recommendations.
ACKNOWLEDGEMENTS
Lars Pedersen, Jens Lindberg, and Hanne Rasmusen have received consulting fees as members of Danish League's COVID‐19 expert group.
Pedersen L, Lindberg J, Lind RR, Rasmusen H. Reopening elite sport during the COVID‐19 pandemic: Experiences from a controlled return to elite football in Denmark. Scand J Med Sci Sport. 2021;31:936–939. 10.1111/sms.13915
REFERENCES
- 1. Divisionsforeningen . Protocol for the resumption of training and match play across all professional football competition in Denmark during the current SARS‐CoV‐2 pandemic. https://divisionsforeningen.dk/protocol/. Accessed October 7, 2020.
- 2. Hoser MJ, Mansukoski HK, Morrical SW, Eboigbodin KE. Strand Invasion Based Amplification (SIBA®): a novel isothermal DNA amplification technology demonstrating high specificity and sensitivity for a single molecule of target analyte. PLoS ONE. 2014;9(11):e112656. 10.1371/journal.pone.0112656 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Corman VM, Landt O, Kaiser M, et al. Detection of 2019 novel coronavirus (2019‐nCoV) by real‐time RT‐PCR. Euro Surveill. 2020;25(3):2000045. 10.2807/1560-7917.ES.2020.25.3.2000045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Statens Serum Institut . https://www.ssi.dk/sygdomme‐beredskab‐og‐forskning/sygdomsovervaagning/c/covid19‐overvaagning/arkiv‐med‐overvaagningsdata‐for‐covid19. Accessed September 15, 2020.
- 5. Iversen K, Bundgaard H, Hasselbalch RB, et al. Risk of COVID‐19 in health‐care workers in Denmark: an observational cohort study. Lancet Infect Dis. 2020;20(12):1401‐1408. 10.1016/S1473-3099(20)30589-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Bundgaard H, Bundgaard JS, Raaschou‐Pedersen DET, et al. Effectiveness of adding a mask recommendation to other public health measures to prevent SARS‐CoV‐2 infection in Danish mask wearers: a randomized controlled trial. Ann Intern Med. 2020. 10.7326/M20-6817 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Rivett L, Sridhar S, Sparkes D, et al. Screening of healthcare workers for SARS‐CoV‐2 highlights the role of asymptomatic carriage in COVID‐19 transmission. eLife. 2020;9:e58728. 10.7554/eLife.58728 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Sutton D, Fuchs K, D'Alton M, Goffman D. Universal screening for SARS‐CoV‐2 in women admitted for delivery. N Engl J Med. 2020;382(22):2163‐2164. 10.1056/NEJMc2009316 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Meyer T, Mack D, Donde K, et al. Successful return to professional men's football (soccer) competition after the COVID‐19 shutdown: a cohort study in the German Bundesliga. Br J Sports Med. 2020;55(1):62‐66. 10.1136/bjsports-2020-103150 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Moriyama M, Hugentobler WJ, Iwasaki A. Seasonality of respiratory viral infections. Annu Rev Virol. 2020;7(1):83‐101. 10.1146/annurev-virology-012420-022445 [DOI] [PubMed] [Google Scholar]