

Abstract
A strong public health workforce (PHW) is needed to respond to COVID‐19 and public health (PH) issues worldwide. However, classifying, enumerating, and planning the PHW is challenging. Existing PHW taxonomies and enumerations focus on the existing workforce, and largely ignore workforce competition for public health graduates (PHGs). Such efforts also do not utilize real time data to assess rapid changes to the employment landscape, like those caused by COVID‐19. A job postings analysis can inform workforce planning and educational program design alike. To identify occupations and industries currently seeking PHGs and contrast them with existing taxonomies, authors matched existing PHW taxonomies to standardized occupational classification codes, then compared this with 38,533 coded, US job postings from employers seeking Master's level PHGs from 1 July 2019 to 30 June 2020. Authors also analysed 24,516 postings from March 2019 to October 2019 and compared them with 24,845 postings from March 2020 to October 2020 to assess changing employer demands associated with COVID‐19. We also performed schema matching to align various occupational classification systems. Job postings pre‐COVID and during COVID show considerable but changing demand for PHGs in the US, with 16%–28% of postings outside existing PHW taxonomies, suggesting labour market competition which may compound PHW recruitment and retention challenges.
Keywords: job postings, labour market competition, public health education, public health workforce, taxonomy
1. INTRODUCTION
Well before the onset of the COVID‐19 pandemic, there was a well‐documented healthcare workforce shortage. 1 The World Health Organization (WHO) estimated a shortage of 18 million health workers by 2030 to meet the requirements of the Sustainable Development Goals and universal health coverage targets set by the WHO. Several other direction‐setting policy documents have been published including the European Action Plan for Strengthening Public Health Capacities and Services, 2 the WHO's ‘Comprehensive health labour market framework for universal health coverage’ 3 and the WHO Global Strategy on Human Resources for Health. 4 Concerns regarding workforce shortages due to the migration of healthcare professionals, 5 retirements or attrition of public health (PH) workers, 6 , 7 and lack of information regarding worker supply based on the postgraduate employment outcomes of public health graduates (PHGs) 8 have become even more urgent due to the COVID‐19 pandemic. The WHO Global Strategy recommends gathering workforce data as ‘global public good to be shared in the public domain’. 4
Due to the crucial role of disease prevention in responding to and recovering from the COVID‐19 pandemic, assessing the public health workforce (PHW) remains critically important. Categorizing and enumerating clinical health professionals such as physicians, nurses, midwives, etc., 9 , 10 while challenging, is generally made simpler by the licensing and registration for these occupations. The PHW is more difficult to define, classify, and enumerate due to a lack of a consistent definition of PH professionals; lack of licensure or certification of PH professionals in most cases; and lack of central registries of these professionals in most countries, with the exception of the United Kingdom 11 and Poland, where registration is optional. 12
Even achieving consensus definitions for the PHW is difficult. PH professionals have been defined as ‘people who are involved in protecting and promoting the collective health of whole or specific populations’, 13 or those contributing to the Essential Public Health Operations (EPHOs), 14 Essential PH Services, 15 or Foundational Public Health Services (FPHS), 16 which are different, but related, models describing core functions of PH systems. The workforce is ‘characterized by its diversity and its complexity and includes people from a wide range of occupational backgrounds’. 17 Not only is this workforce diverse in its occupations, it is diverse in its employment settings or sectors. While the ‘core’ PHW has often been defined as existing within government agencies, 18 , 19 it has also been acknowledged that PH work takes place in academia, the voluntary/nongovernmental organization sector (i.e., charities, non‐for‐profit organizations), healthcare, and corporations (for‐profit companies), and that many people contribute to the ‘wider’ PHW, which can include people whose work indirectly contributes to PH efforts. 20 , 21
The PHW is undergoing particular strain in the COVID‐19 context. Especially in the United States, PHW and leadership are being subject to harassment in a highly politicized and polarized COVID‐19 response environment. COVID‐19 associated burnout is compounding an already‐stressed and chronically underfunded workforce that has decreased by approximately 20% since the onset of the Great Recession in 2008. 22 , 23 When employers from outside the PHW, who seek to hire candidates with the skills provided by a PH education, offer higher wages or a better work environment for PHGs, this can entice PHGs away from finding employment in the PHW and can compound PHW shortages, resulting in a workforce crisis.
1.1. Existing taxonomies and enumerations use a needs‐based approach
Several attempts have been made to define and enumerate the PHW, often beginning with creating PHW taxonomies which include categories of occupations—including job functions or titles—which contribute to EPHOs. In workforce research, occupations are categorized or classified, described and quantified using standardized metrics and surveys designed by expert industrial psychologists or labour market researchers. For example, the International Labour Organization (ILO) uses International Standard Classification of Occupations (ISCO‐08) codes 24 (p), the US Bureau of Labor Statistics (BLS) uses Standard Occupational Classification (SOC) codes, 25 and the UK uses its own SOC codes 26 to classify occupations. Although such codes can be imperfect—the WHO global strategy advocates that the ILO revise the ISCO ‘for greater clarity on delineation of health workers and health professions’ 4 —mapping the occupations in a workforce taxonomy to these codes allows researchers to use consistent, standard definitions of workers' roles, and is important for labour market projections and assessment of educational requirements. 4
To create a PHW taxonomy, many researchers use a needs‐based framework—focussing first on the EPHOs and the staff needed to provide them—or use surveys of the existing PHW to determine which occupations exist therein. A recent systematic review article synthesized articles focused on enumerations and definitions of the PHW over a nearly two‐decade period. 27 This article includes a new proposed taxonomy based on a synthesis of occupation‐specific terms and job titles collected from the reviewed articles, which researchers matched to ISCO‐08 codes based on their judgements of job titles. Additionally, while several articles within the systematic review list occupations by name, only two sources highlighted in the review specifically focus on PHW occupational taxonomies, one by the University of Michigan/Centers for Disease Control and Prevention (referred to here as ‘UM’) 19 and one by the Centre for Workforce Intelligence (CfWI) in the United Kingdom. 18 , 20
These workforce taxonomies have primarily been created through a multi‐step, ‘top‐down’ process, beginning with the high‐level definition of EPHOs, 15 , 28 followed by a literature review (often including a ‘job analysis’ of job descriptions provided by current PH professionals), followed by data extraction or qualitative coding, review of key terms by experts, focus groups, and finally pilot testing/surveys of the PHW 29 ; or scoping, literature review, data collection, and stakeholder engagement. 18 The taxonomies generally only include occupations that the researchers defined as contributing to EPHOs, and sometimes define PHW even more narrowly; for example, the UM taxonomy emphasizes occupations in the governmental PHW.
1.2. Insufficiencies of current PHW taxonomies
While these taxonomies are an important step in PHW categorization and enumeration, they may leave out relevant occupations due to their focus on the existing PHW and how it is defined. These taxonomies, themselves, also may not be sufficiently robust in describing the landscape of PHW employment because they do not take supply of PHG into account, nor the labour market competition 30 for PHG: ‘partial health workforce policies…designed on the basis of needs‐based estimates and focused on training more health workers’ are ‘not sufficient in addressing health worker shortages’. 3
New research in the United States indicates that PHG may be increasingly finding employment in the for‐profit sector and other fields which may not contribute to EPHOs; assessment of the current PHW and its need for PHG is not enough if it ignores this ‘leaky pipeline’ 31 , 32 , 33 , 34 or loss of PHGs to occupations and sections that do not contribute to the EPHOs.
Additionally, the existing taxonomies do not clearly delineate the occupations which require formal education in PH versus those that do not. Workers included in PHW taxonomies can include everyone from medical doctors and scientists, to nurses, to sanitarians, to typists and office clerks because they are involved in, or support, the delivery of PH services and protections. To ensure we can assure ‘a competent PHW’, 35 it is essential to know how many individuals with formal education in PH (PHGs) are needed in the PHW, and for which specific occupations, then contrast with PHG employment outcomes and detailed data on labour market competition. This manuscript employs a theoretical framework which includes an analysis of both the existing PHW, the supply of PHGs, and employer competition to hire them, adapted from prior healthcare workforce research 30 for this article (Figure 1).
FIGURE 1.
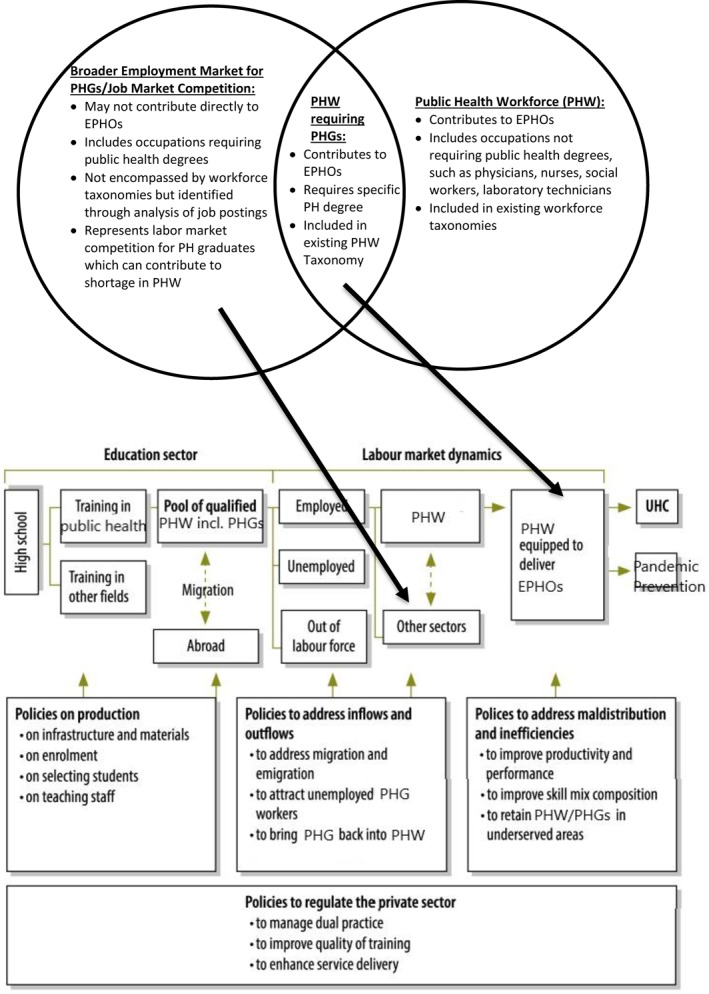
Diagram of labour market dynamics for public health graduates (PHGs)
1.3. Utility of job postings analysis to classify PHW
One method of determining the labour market demand for PHGs is to analyse job postings/advertisements for these graduates, and compare them with the existing definitions and taxonomies for the PHW. Job postings typically include the job title, a description of the employing organization, an overview of job tasks or functions, and a list of required or desired skills, experience, education, or other credentials. Because job descriptions are designed to clearly describe the skills and qualifications needed to perform a job, they are a useful source of insight into current hiring needs. Although job postings are not created for the purposes of workforce research, many studies have been conducted which leverage the rich, text‐based information from job postings—approximately 85% of which are posted on the internet 36 —to infer employer needs and workforce trends. Several research studies on PHW have utilized job descriptions analysis to discern employer demands. 37 , 38 , 39 , 40 , 41
New technologies and methodologies allow for ISCO‐08 and SOC coding of large‐scale job postings data, thereby creating a list of occupations for which employers are currently seeking PHGs. Utilizing job postings data, to contrast with existing taxonomies, also provides data‐driven, ‘real time’ insights more quickly than periodic surveys or expert opinion.
This article seeks to more consistently map the occupations identified in existing PHW taxonomies to ISCO‐08 and US SOC codes, then contrast them with job postings data which illustrate occupations and sectors currently seeking to hire PHGs. By identifying the job postings targeting PHGs which are not part of existing taxonomies, we can reveal new occupations or sectors which may be drawing PHGs away from the occupations that past researchers have defined as contributing to the EPHOs, thus assessing the labour market competition for PHGs. This research can also identify possible workforce gaps, and provide insights to academia to innovate their curricula. Finally, through an analysis of job postings in two time frames, before COVID‐19 and during the COVID‐19 pandemic, we can assess whether demand for PHGs has changed during the COVID‐19 pandemic.
2. METHODS
To assess which jobs seek PHGs aside from those in existing PHW taxonomies, researchers first matched PHW taxonomies with ISCO‐08 codes, then contrasted job postings with the codes; and assessed differences in proportions of postings before and during the COVID‐19 pandemic.
2.1. Mapping existing taxonomies to standardized occupational classifications
The ILO's ISCO‐08 codes classify occupations into 441 categories, while the US Department of Labor's Standard Occupation Classification (referred to here as ‘USSOC’) codes, revised in 2018, include 867 different detailed occupations. 25 The US Department of Labor offers a SOC to ISCO‐08 ‘crosswalk’ to match the codes to one another. 42 The UK's Office for National Statistics (ONS) has its own SOC codes (referred to here as ‘UKSOC’), with 583 unique codes matching to 28,749 job titles and subtypes 26 ; and a UKSOC to ISCO‐08 SOC crosswalk exists.
Two of the existing taxonomies, UM 43 and the CfWI Core workforce report 18 , 20 did not include matches to SOC codes in their descriptions. Therefore, the lead researcher matched the job titles, or, when available, job descriptions, to their respective SOC codes, and then to ISCO‐08 codes. For UM, the researcher referenced earlier studies which matched the titles which were later used for the taxonomy with USSOC codes 44 , 45 , 46 and verified the proposed taxonomy with one of the authors of the original taxonomy. We also utilized a SOC‐matching system developed by the US National Institutes of Health to match the available descriptions of the jobs in the UM taxonomy with USSOC codes. 47 In cases where more than one USSOC code matched a job from the UM taxonomy, or where more than one job title from UM matched the same USSOC code, both are included in the table (Table A1). In cases where no USSOC code match could be found, this is indicated in the table.
For the CfWI taxonomy of the Core PHW in the UK, the lead researcher referred to the detailed descriptions of each occupation in the report and attempted to match them to UKSOC 2010 codes using a qualitative approach, and further, utilized the UK ONS Occupation Coding Tool, which matches job titles to UKSOC 2010 codes, 48 which then match to ISCO‐08. Additionally, CfWI included a report on the ‘wider’ PHW, which utilized discussions with various professional association members to determine which other occupations were considered ‘engaged’ in PH. CfWI mapped these to UKSOC 2010 code, which the researcher cross‐matched to ISCO‐08 codes using the UK's ONS crosswalk. 49 For the purpose of this study, we included only those occupations listed as ‘active’ in their engagement (‘public health was explicitly part of their job’).
The taxonomy proposed in the systematic review article 27 was already matched to ISCO‐08 codes by the article's authors.
2.2. Utilizing a job postings database
This manuscript utilizes a commercially available job postings database, maintained by Burning Glass (BG) Technologies. BG is a data vendor which compiles millions of job postings every year using ‘bots’ which search more than 40,000 different sources, tracking 3.4 million job postings at any time. 36 Data from this site has been used in many other workforce studies, 40 , 50 , 51 , 52 including analysis of COVID‐19's impact on the labour market. 40
BG utilizes machine learning and natural language processing technology to match job postings data with the employer's required or desired Classification of Instructional Program (CIP) codes, 53 which are developed by the US Department of Education to categorize areas of academic study; to allow searchability by the level of education required; and to match jobs with industries/sectors and USSOC codes.
We conducted three BG queries. We delimited all queries to job openings posted in the United States, for which, according to the BG algorithms, the employer desired or required a Master's level degree, with any of the CIP codes which match PH degrees, including 51.22 (including General Public Health, Environmental Health, Health/Medical Physics, Occupational Health/Industrial Hygiene, Public Health Education/Promotion, Community Health/Preventive Medicine, Maternal and Child Health, International PH/International Health, Health Services Administration, Behavioural Aspects of Health); 26.1309, Epidemiology; and 26.1102, Biostatistics.
One query was for 40,707 job postings from 1 July 2019 to 30 June 2020, of which 38,533 were USSOC‐coded. The second and third queries were designed to compare jobs across all sectors before and during COVID‐19, including jobs posted 1 March 2020 through 31 October 2020 (n = 24,845, the ‘COVID‐19 era’), and 1 March 2019 through 31 October 2019 (n = 24,516 the ‘pre‐COVID‐19 era’). We compared occupations and sectors from the COVID‐19 using two‐proportion independent sample z tests with α = 0.05.
3. RESULTS
3.1. Mapping existing taxonomies to ISCO‐08 and SOC codes
The three main taxonomies had varying levels of specificity (Table A1). The most detailed was the UM taxonomy, with a total of 69 job titles (three titles not originally in the taxonomy, ‘Pharmacist’, ‘Emergency Medical Services Worker’, and ‘Other Business Support Services’ were added, because they were included in a US PHW survey based on the taxonomy). 54 Matching the UM codes to USSOC and ISCO‐08 codes revealed some discrepancies. There were three titles for which a USSOC code could not be found: ‘population health specialist’, ‘implementation specialist’, and ‘adult protective services/community worker.’ Several titles could map to multiple USSOC codes, and in some cases, several UM codes could map to one SOC code, for example, ‘health officer’, ‘subagency‐level director: Bureau, department, division or branch’, and ‘deputy director (agency or subagency level)’ all match to the USSOC ‘chief executives.’
The CfWI ‘Mapping the Core’ taxonomy encompassed 11 job titles, each of which could include a large number of sub‐titles. When matching the titles to ISCO‐08 codes using the ONS Occupation Coding Tool 48 and subsequently matching UK SOC codes to ISCO‐08 codes, however, multiple titles matched to the same ISCO‐08 codes (e.g., ‘PH consultants and specialists’, ‘Directors of Public Health (DsPH)’, ‘PH managers’, and ‘PH practitioners’ all matched to ISCO‐08 2269, ‘Health professionals not elsewhere classified’).
Some of the CfWI titles were too broad to clearly match to a particular SOC or ISCO‐08 code—for example, ‘information workers’ could refer to individuals who analyse data, but could also mean communications specialists. CfWI also excluded several occupations which appear in other taxonomies, including ‘midwives, general practitioners (GPs), community pharmacists…staff across the NHS and local government fulfilling a PH function as part of their job…staff supporting PH teams (e.g., business support staff, administration staff…).’ 18 The CfWI ‘Understanding the wider PHW’ report, in contrast, lists 75 different UKSOC occupations for which the workers were seen as engaged actively in PH, encompassing 56 ISCO‐08s, but 34 (such as ‘prison guards’, ‘butchers’ and ‘athletes’) matched no occupations in the other taxonomies nor the BG postings and were excluded to reduce confusion.
The taxonomy by Watts et al. 27 included 103 titles, the majority of which were mapped to ISCO‐08 codes by the authors using job titles alone, but multiple titles were matched to the same ISCO‐08 code; removing duplicates, there were 33 unique ISCO‐08 codes, and seven job titles which were not matched to an ISCO‐08 code. Two titles, ‘emergency preparedness’ and ‘quality improvement specialist’ were not matched to ISCO‐08 codes, but could be matched to USSOC codes due to their greater specificity.
A few ‘consensus’ occupations could be clearly identified across the UM, CfWI, and Watts taxonomies. These included ‘health services managers’ (ISCO‐08 1342); ‘environmental and occupational health inspectors’ (3257); ‘environmental and occupational health and hygiene professionals’ (2263, including health educators); ‘social work and counselling professionals’ (2635); ‘biologists, botanists, zoologists and related professionals’ (2131, including epidemiologists, microbiologists); ‘statisticians’ (2120); ‘community health workers’ (3253); ‘nurses’ (2221); ‘systems analysts’ (2511); and ‘medical and pathology laboratory technicians’ (3212), illustrating the interprofessionalism of the PHW.
3.2. Contrasting existing taxonomies with BG data
There were a total of 38,533 SOC‐coded job postings in the US, where a Master's level PHG was sought, in the BG data from 1 July 2019 to 30 June 2020, within 315 different USSOC occupations. We excluded those occupations with 50 or fewer job postings in the data collection, thus analyzing 92 unique SOC coded‐occupations, representing a total of 36,225 postings from the sample. The jobs postings data also included postings by industry/sector.
Overall, there were 32 unique USSOC coded occupations in BG (corresponding to 29 unique ISCO‐08 occupations) which were not included in the UM, CfWI ‘Core’ or ‘Wider’ taxonomies, or Watts taxonomies, representing 10,089 jobs, or 28% of the BG postings. Of these jobs, 4335 were for ‘managers, all other’ (ISCO‐08 1114/USSOC 11‐9199). When these are excluded, 16% of the BG jobs did not match existing taxonomies (See Table 1 and Appendix Table 1). Table 1 compares job titles/occupation naming used in the occupational taxonomies and contrasts them with the number of job postings within each US SOC code/ISCO‐08 code, from the BG data from 2019 to 2020, with the list sorted by number of job postings in BG.
TABLE 1.
Comparison of top 10 most sought jobs for public health graduates, by public health (PH) taxonomy, SOC, and ISCO‐08 codes
| ISCO‐08 code | ISCO‐08 title | USSOC Code | USSOC Title | ‘No two workforces’ 27 titles | UM title 19 | CfWI core title 18 | CfWI ‘wider’ WF title 20 | BG jobs # 2019–2020 |
|---|---|---|---|---|---|---|---|---|
| 1342 | Health services managers | 11‐9111 | Medical and health services managers | Agency leadership, coordinators, directors of PH, health care administrators, health management, health planners, health policy makers, health promotion managers, managers, public health manager | 1.1.5. Program director | PH consultants and specialists | 4636 | |
| 1114 | Senior officials of special‐interest organizations | 11‐9199 | Managers, all other | 4335 | ||||
| 2120 | Mathematicians, actuaries and statisticians | 15‐2041 | Biostatisticians (15‐2041.01)/Statisticians (15‐2014) | Biostatisticians, statisticians | 1.2.23. Statistician | Intelligence and knowledge professionals | 3241 | |
| 2221 | Nursing professionals | 29‐1141 | Registered nurses (including public health nurse) | Health visitors, licensed practical or vocational nurse, nurses, nursing home health aide, nursing technicians, primary healthcare registered nurses, public health nurse, registered nurses, school nurses, social nursing, community health nurses | 1.2.14.1.1. PH or community health nurse | PH nurses; health visitors; school nurses | 1956 | |
| 2519 | Software and applications developers and analysts not elsewhere classified | 15‐1199 | Computer occupations, all other | Intelligence and knowledge professionals | 1833 | |||
| 2120 | Mathematicians, actuaries and statisticians | 15‐2031 | Operations research analysts | Biostatisticians, statisticians | 1340 | |||
| 2131 | Biologists, botanists, zoologists and related professionals | 19‐1041 | Epidemiologists | Biologists, epidemiologists, food safety epidemiologists, health services researchers, microbiology, parasitology, PH scientists, researchers | 1.2.6. Epidemiologist | PH scientists | 1237 | |
| 2310 | University and higher education teachers | 25‐1199 | Postsecondary teachers, all other | Academic PH specialists | PH academics | Higher education teaching professionals | 1223 | |
| 2421 | Management and organization analysts | 13‐1111 | Management analysts | 835 | ||||
| 2263 | Environmental and occupational health and hygiene professionals | 21‐1091 | Health educators | Environmental health experts, environmental PH workers, occupational and environmental health specialists | 1.2.8. Health educator | Environmental health professionals | 810 |
In the 1 July 2019–30 June 2020 BG data, 33,563 were coded by industry/sector; the top industries were health care and social assistance (n = 10,476 postings or 31.2%); educational services (7,606, 22.7%); public administration/government (4,127, 12.3%); finance and insurance (3,312, 9.9%), professional, scientific, and technical services (3,507, 10.4%), manufacturing (2,251, 6.7%), other services (except public administration) (1,089, 3.2%), information (282, 0.8%), administrative and support and waste management and remediation services (264, 0.8%), and retail trade (261, 0.8%; Table 1).
3.3. Comparing pre‐COVID and ‘COVID era’ jobs
There were 24,845 job postings from 1 March 2020 through 1 October 2020 (the ‘COVID era’), and 24,516 postings from 1 March 2019 to 1 October 2019 (‘pre‐COVID’).
Significant differences were observed in the proportion of job postings by industry or sector comparing the two time frames, including a decrease in positions in colleges, universities, and professional schools (p < 0.0001) and general medical and surgical hospitals (p < 0.0001), and increases in insurance carriers (p < 0.0001), and pharmaceutical and medicine manufacturing (p < 0.0001; Table A2).
Comparing COVID‐era and pre‐COVID postings, there were significant increases in postings for epidemiologists and statisticians, medical and health services managers, natural sciences managers (including research managers), sales managers, chief executives, computer occupations, private detectives (a USSOC occupation mapping contact tracers, which does not yet have a USSOC code), architecture and engineering managers (including project managers), biologists, compliance officers, and community health workers. General management occupations, and roles in education and social services declined (See Table A2; Table 2).
TABLE 2.
Comparison of COVID VS pre‐COVID Era Industries/Sectors and Jobs
| COVID (1 March 2020–31 Oct. 2020) | Pre‐COVID (1 March 2019–31 Oct. 2019) | |||||
|---|---|---|---|---|---|---|
| NAICS code | Industry | Job postings | % | Job postings % | ||
| 6113 | Colleges, universities, and professional schools | 3757 | 19.9% | 4986 | 25.51% | *** |
| 6221 | General medical and surgical hospitals | 3229 | 17.1% | 3889 | 19.90% | *** |
| 5241 | Insurance carriers | 2854 | 15.1% | 2040 | 10.44% | *** |
| 9211 | Executive, legislative, and other general government support | 1478 | 7.8% | 1528 | 7.82% | |
| 3254 | Pharmaceutical and medicine manufacturing | 1353 | 7.2% | 917 | 4.69% | *** |
| 5417 | Scientific research and development services | 1258 | 6.7% | 1113 | 5.69% | ** |
| 6211 | Offices of physicians | 574 | 3.0% | 793 | 4.06% | *** |
| 6241 | Individual and family services | 381 | 2.0% | 357 | 1.83% | |
| 5416 | Management, scientific, and technical consulting services | 298 | 1.6% | 347 | 1.78% | |
| 8133 | Social advocacy organizations | 290 | 1.5% | 299 | 1.53% | |
| All other | 3407 | 18% | 3276 | 17% | ** | |
| Total | 18,879 | 100% | 19,546 | 100% | ||
Note: A total of 18,879 jobs from 1 March 2020 to 31 Oct. 2020, and 19,546 jobs from 1 March 2019 to 31 Oct. 2019, were assigned NAICS codes in Burning Glass. Seven hundered sixty‐four postings from the COVID era, and 644 from the pre‐COVID era are excluded from the table, but not from the statistical analysis, because they existed in industries with 30 or fewer postings in one of the time points.
***p < 0.0001,**p < 0.01, *p < 0.05.
4. DISCUSSION
This article has sought to consistently map PHW occupations with SOCs, contrast them with jobs requiring PHGs, and finally, illuminate labour market competition for PHGs, while offering insights into COVID‐19's impact on hiring of PHGs. While competition for PHGs has been hinted at in past research, it is more clearly illuminated here, and these findings can be used to both create policies to reduce workforce gaps, and also innovate educational curricula.
Mapping taxonomies to ISCO‐08 and SOC codes, while challenging, provides key insights into PHW labour market dynamics; but these codes do not always clearly align with PH occupations, making it more difficult to gain a complete picture of the PHW. There is clear competition for PHGs outside the PHW as it has been traditionally defined; for example, though the US PHW has often been defined as governmental, government comprised only 12% of job postings for PHGs.
4.1. Mapping to standardized occupational classifications: using new tools
Job analysis—a specific method in industrial psychology—is a critical element in taxonomy creation. New tools exist, which can ensure taxonomies match accurately to SOCs based on complete job descriptions. These include machine learning tools such as the US National Institutes of Health ‘SOCcer’ tool, 47 large‐scale, coded datasets such as BG, or even direct inquiries with the BLS or ONS. The existing taxonomies were mainly created both through discussions with experts in the field and with surveys, by using lists of job titles without complete job descriptions for each occupation, or using job categories which are too broad to match to specific occupations.
The suggestion by Watts and colleagues that differences in taxonomies reflect differences in PH systems is reconfirmed by this investigation. For example, there are several occupations absent from the UM taxonomy, but which appear in other taxonomies or in BG. These include roles in academia, such as ‘postsecondary teachers’ and ‘social science research assistants.’ Conversely, CfWI includes academia as a core part of the PHW. However, while different countries have different taxonomies, we observe there is still some consensus between different taxonomies regarding which occupations are a core part of the PHW.
4.2. Evidence of labour market competition for PHGs
It is notable that there were 24,845 job postings in the ‘COVID era’, and 24,516 postings ‘pre‐COVID era.’ The BLS's monthly Job Openings and Labor Turnover Survey (JOLTS), which tracks the number of monthly job postings in the United States, indicates that there were consistently fewer job postings in 2020 than 2019 each month (e.g., 15.9% fewer job openings in March 2020 compared with March 2019; 30.7% fewer in April, and 26% fewer in May), 55 which suggests that the job market for master's level PHGs has not been as negatively impacted by the COVID‐19 pandemic as compared with the broader job market.
The fact that 4127 positions in Public Administration (government) were posted in the 2019–2020 BG data set is notable because there were 17,948 Master's‐level PHGs in 2019 in the United States. New data show approximately 19% of Master's level PHGs enter into government after graduation, giving approximately 3410 PHGs entering government, a shortfall of approximately 717 PHGs, and preliminary evidence of a long‐suspected labour market mismatch. 32 , 33 , 56 This mismatch—in which not enough PHGs are entering government to fill critical PHW shortages—may have serious repercussions for the ability of the governmental PHW to respond to PH crises including COVID‐19.
The occupations from BG that do not exist in current taxonomies provide researchers with insight into labour market competition. The large percentage of computer‐related occupations in BG outside the taxonomies may reflect employers seeking epidemiology or biostatistics students, such as corporations seeking data scientists. There are also several business‐related occupations (sales, marketing and operations research) which appear in BG but not existing taxonomies, reflecting occupations in the for‐profit sector seeking PHGs—an indicator of job market competition which could negatively impact the ability of PHG to fill a PHW shortage. Conversely, several occupations in PHW taxonomies had very few BG postings, reflecting occupations in the PHW not requiring a PHG.
4.3. COVID‐19 and changes in industry/sector
In addition to ongoing labour market competition, COVID‐19 appears to have impacted the job market for PHGs, and there are several possible explanations for these changes. The insurance industry markedly increased hiring in the COVID era. In the United States, health insurance firms were one of the few sectors to experience fewer financial challenges due to COVID‐19, because elective medical procedures were halted during lockdowns, reducing insurance claims. Hospitals had the opposite challenge; significant revenue comes from elective procedures, cancelled due to COVID‐19. Education sector hiring has declined, reflecting financial challenges. Pharmaceutical firms are growing due to investments in COVID‐19 treatments and vaccines. Finally, hiring in government stayed quite similar, pre‐COVID versus COVID‐era—possibly reflecting funding priorities made by policymakers in the United States during the time period being analysed.
4.4. Recommendations and future PHW research
In order to improve PHW research, we suggest advocacy efforts to BLS and ILO ensure inclusion of codes that encompass critical PH occupations, since several occupations in PH do not match to ISCO‐08 or SOC codes. And while the use of SOCs, by themselves, to enumerate the PHW is controversial due to the ‘ill‐defined’ nature of the workforce 44 , 57 and the fact that simply counting the number of people in an occupation does not illuminate the PHW because many work outside PH (e.g., the vast majority of nurses are not PH nurses), these codes are still helpful in gathering in‐depth occupational information.
To truly assess labour market competition for PHGs, this analysis should be combined with efforts to enumerate the current PHW, assess what proportion of the workforce work in occupations which require PH education (according to SOC‐based educational benchmarks 58 ), compare the current level of PH education within each occupation, and determine expected attrition, 7 then contrast the current PHW with population needs based on EHPOs, and finally determine employment outcomes of PHGs. Such an assessment can allow workforce planners to determine whether there are enough PHGs contributing to EPHOs; this article's analysis can clarify which industries are ‘poaching’ PHGs from EPHO‐related jobs. This can guide policy levers to alter the job market by ensuring competitive wages, reducing barriers to entry into the traditional PHW, 34 and creating more effective recruitment programs for PHGs to compete with new sectors. Additionally, in order to ensure PHGs understand and are committed to their role in contributing to the EPHOs, there can be stronger efforts to connect PHGs to a professional identity which is directly connected to the EPHOs; a professional identity or ethos is also important for the existing PHW. This study illustrates that PHW is comprised of a very diverse range of different occupations, making it more difficult to create a unified professional identity. Efforts towards professionalization, including credentialing, registration, consistent competencies, and a strong professional board or association, can help connect PHGs to a stronger, more unified PHW. 21 Simultaneously, PHGs who do decide to enter the ‘wider’ PHW can advocate for better PH principles wherever they go, bringing the voice of PH to settings beyond traditional PH.
4.5. Uses by academia
Higher education institutions may not wish to see themselves as ‘vocational preparation’ programs whose only role is to respond to employer demands, but if they ignore current employer demand, their curricula may be seen as outdated by their graduates' employers. Universities preparing PHGs can utilize this analysis to discern real‐time job market requirements of employers. The jobs with the fastest increases in hiring during the COVID‐19 era focus on statistics and epidemiology, program management, computer‐related positions, community health workers, and individuals managing clinical trials or research programs. An increased need for Chief Executives highlights the need for leadership training to meet the COVID‐19 pandemic's management challenges or replace retiring PH executives; and ‘private detectives’ may reflect the hiring of contact tracers/disease investigators. Social workers and physicians are needed to provide direct services and to help with prevention efforts for COVID‐19; the increase in market research and compliance may reflect new research around behaviour change communication or enforcement of COVID‐19‐related regulations. The increase in engineering managers might reflect the need to bring PH expertise to the design of buildings to ensure healthy airflow and reduce the transmission of an airborne virus. Ensuing curriculum meets employer demands for leadership, statistics, market research, program and research management, computer programming/data science, business skills, and operations research can ensure PHGs have relevant skills for today's job market.
Career advising for PH students can also be enhanced by referring students to information on the occupations referenced in this taxonomy; each USSOC occupation is described in detail on a comprehensive career guidance website, O*Net Online, 59 which includes alternative job titles, job descriptions, lists of job tasks, technology and tools used, knowledge, skills and abilities, detailed work activities, work context, level of required education or training, credentials or certifications, work styles and values, related occupations, salary ranges and projected labour market growth, providing one of the richest and most accurate sources of occupational data available. A new career guidance intervention could be designed, similar to the UK's PHORCaST program, 60 based on the occupations listed here, which in turn could help encourage students to consider PH studies and contribute to the EPHOs. Universities can also utilize these results to portray to prospective students why a PH degree can offer career satisfaction. 56
4.6. Limitations
The BG data was gathered from the United States. BG does have data collections from Europe, which may help future researchers. BG's coding algorithms are proprietary. It is possible that the jobs in the dataset are not truly reflective of who is hiring PHGs. More research is necessary, including hand‐searching actual job posting samples from BG to validate their methodology. It is possible BG might undercount certain sectors due to the way the jobs are posted online. Jobs posted through government contractors may be miscategorized or undercounted. Also, large‐scale/mass hiring efforts may take place through only a single job posting, which could undercount surge hiring efforts.
BG leaves out qualitative information which might be gleaned by hand‐coding or using a text‐based analysis to discern current skills needed by employers. This can be especially critical for the COVID‐19 era jobs, which may reflect new and emerging occupations without ISCO or SOC codes. Further research, including qualitative analysis or employer surveys, would further illuminate skills requirements. Also, occupations are only one of multiple elements which should be considered when researching the workforce; sector, mission/subject area, and funding source are all factors to consider.
Several occupations, including policy analyst, advocacy, and contact tracing do not map clearly to ISCO‐08 or SOC codes. Some taxonomy occupations are not clearly defined such as ‘population health specialist’, and without a job description, may be impossible to match to a code. More research to finalize the mapping should be conducted, using full job analysis.
This ‘demand side’ approach may illustrate workforce gaps, but should be used in combination with needs‐based workforce and funding assessments for PHW hiring, to gather a more complete picture of PHW gaps.
5. CONCLUSIONS
A complete analysis of the PHW should include the supply of PHGs and labour market competition for them. By understanding who is hiring PHGs, we can intentionally design policies and recruitment initiatives to fill workforce gaps. And while universities offering PH degrees design them to prepare students to contribute to EPHOs, the competencies gained by their students are clearly in demand in fields which may or may not contribute to EPHOs. 32
COVID‐19 has altered the labour market for millions of people, including PHGs. Illuminated the critical role of a trained PHW. By more fully understanding this workforce, leaders can advocate to effectively harness the energy and commitment of new PHGs to contribute to EPHOs to heal our world.
CONFLICT OF INTEREST
Authors declare that they have no conflict of interest and they abide by the ethical policy of the journal.
Supporting information
Supplementary Material 1
Supplementary Material 2
ACKNOWLEDGEMENTS
Daniel Russ, PhD, at the US National Institutes of Health, for extensive assistance with SOCcer system. Kristy Sherrer, MS, University of Los Angeles Fielding School of Public Health, Los Angeles, CA, USA preliminary review; Cedric JJP Slock for workforce research framing information.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- 1. Liu JX, Goryakin Y, Maeda A, Bruckner T, Scheffler R. Global health workforce labor market projections for 2030. Hum Resour Health. 2017;15(1):11. 10.1186/s12960-017-0187-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Kroezen M, Van Hoegaerden M, Batenburg R. The joint action on health workforce planning and forecasting: results of a European programme to improve health workforce policies. Health Pol. 2018;122(2):87‐93. 10.1016/j.healthpol.2017.12.002 [DOI] [PubMed] [Google Scholar]
- 3. WHO . A comprehensive health labour market framework for universal health coverage. WHO, 2020. https://www.who.int/bulletin/volumes/91/11/13‐118927/en/. Accessed November 27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. WHO . Global strategy on human resources for health: workforce 2030. WHO, 2020. http://www.who.int/hrh/resources/pub_globstrathrh‐2030/en/. Accessed November 19. [Google Scholar]
- 5. Glinos IA. Health professional mobility in the European Union: exploring the equity and efficiency of free movement. Health Pol. 2015;119(12):1529‐1536. 10.1016/j.healthpol.2015.08.010 [DOI] [PubMed] [Google Scholar]
- 6. Draper DA. Public Health Workforce Shortages Imperil Nation's Health. 2008(4):8. [PubMed] [Google Scholar]
- 7. Liss‐Levinson R, Bharthapudi K, Leider JP, Sellers K. Loving and leaving public health: predictors of intentions to quit among state health agency workers. J Public Health Manag Pract JPHMP. 2015;21(Suppl 6):S91‐S101. 10.1097/PHH.0000000000000317 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Krasna H, Gershuni O, Sherrer K, Czabanowska K. Post‐graduate employment outcomes of undergraduate and graduate public health students: a scoping review. Publ Health Rep. 2020. In Press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. WHO . A universal truth: No health without a workforce. WHO, 2020. https://www.who.int/workforcealliance/knowledge/resources/hrhreport2013/en/. Accessed November 19. [Google Scholar]
- 10. Gale Academic OneFile . Document ‐ headcount and FTE data in the European health workforce monitoring and planning process. 2020. https://go‐gale‐com.ezproxy.cul.columbia.edu/ps/i.do?p=AONE&u=columbiau&id=GALE%7CA461871414&v=2.1&it=r&sid=summon. Accessed November 19. [Google Scholar]
- 11. UK public health register. 2020. https://ukphr.org/. Accessed November 27. [Google Scholar]
- 12. Absolwentów Rejestr. PZH. Published January. 2019;15. https://www.pzh.gov.pl/rejestr‐absolwentow/. Accessed December 3, 2020. [Google Scholar]
- 13. Global Public Health A New Era. Oxford University Press; 2020. https://oxford.universitypressscholarship.com/view/10.1093/acprof:oso/9780199236626.001.0001/acprof‐9780199236626. Accessed November 23. [Google Scholar]
- 14. The 10 essential public health operations, 2020. https://www.euro.who.int/en/health‐topics/Health‐systems/public‐health‐services/policy/the‐10‐essential‐public‐health‐operations. Accessed November 20. [Google Scholar]
- 15. CDC ‐ public health system and the 10 essential public health services ‐ OSTLTS, 2019. https://www.cdc.gov/publichealthgateway/publichealthservices/essentialhealthservices.html. Accessed November 17. [Google Scholar]
- 16. The Public Health National Center for Innovations . Foundational Public Health Services (FPHS): building a strong foundation of public health infrastructure FPHS. 2020. https://phnci.org/national‐frameworks/fphs. Accessed December 25. [Google Scholar]
- 17. Beaglehole R, Dal Poz MR. Public health workforce: challenges and policy issues. Hum Resour Health. 2003;1(1):4. 10.1186/1478-4491-1-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Centre for Workforce Intelligence . Mapping the Core Public Health Workforce; 2014:81. https://www.gov.uk/government/publications/mapping‐the‐core‐public‐health‐workforce. Accessed December 25, 2020. [Google Scholar]
- 19. Boulton ML, Beck AJ, Coronado F, et al. Public health workforce taxonomy. Am J Prev Med. 2014;47(5Supplement 3):S314‐S323. 10.1016/j.amepre.2014.07.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. The wider public health workforce: the next major public health workforce. Perspect Public Health. 2016;136(1):13‐15. 10.1177/1757913915618312 [DOI] [PubMed] [Google Scholar]
- 21. Czabanowska K, Martin‐Moreno J, Gray S, et al. Roadmap to professionalizing the public health workforce (working paper). Public Health Services Division of Health Systems and Public Health World Health Organization Regional Office for Europe, WHO. 2019. [Google Scholar]
- 22. Newman S. Local health department job losses and program cuts: findings from the 2013 profile study. National Association of City‐County Health Officials. 2013. Published July. https://www.naccho.org/uploads/downloadable‐resources/Survey‐Findings‐Brief‐8‐13‐13‐3.pdf [Google Scholar]
- 23. NEHA COVID‐19 environmental health workforce needs assessment II report, 2020. https://www.neha.org/sites/default/files/flipping_book/neha‐covid‐19‐eh‐workforce‐needs‐assessment‐ii‐report/index.html. Accessed November 26. [Google Scholar]
- 24. ISCO . International standard classification of occupations. 2020. https://www.ilo.org/public/english/bureau/stat/isco/isco08/index.htm. Accessed August 27. [Google Scholar]
- 25. U.S.Bureau of Labor Statistics . SOC User Guide, on Behalf of the Office of Management and Budget (OMB) and the Standard Occupational Classification Policy Committee (SOCPC); 2018. Published online 2018. https://www.bls.gov/soc/2018/soc_2018_user_guide.pdf [Google Scholar]
- 26. SOC 2010 ‐ office for national statistics, 2020. https://www.ons.gov.uk/methodology/classificationsandstandards/standardoccupationalclassificationsoc/soc2010. Accessed November 22. [Google Scholar]
- 27. Watts RD, Bowles DC, Ryan E, Fisher C, Li IW. No two workforces are the same: a systematic review of enumerations and definitions of public health workforces. Front Public Health. 2020;8. 10.3389/fpubh.2020.588092 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Self‐assessments of the Essential Public Health Operations in the WHO European Region 2007–2015 (2017). https://www.euro.who.int/en/health‐topics/Health‐systems/public‐health‐services/publications/2017/self‐assessments‐of‐the‐essential‐public‐health‐operations‐in‐the‐who‐european‐region‐20072015‐2017. Accessed November 19, 2020. [Google Scholar]
- 29. Toward standardized, comparable public health systems data: a taxonomic description of essential public health work | hsr, 2020. https://www.hsr.org/node/441446. Accessed November 20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Vujicic M, Zurn P. The dynamics of the health labour market. Int J Health Plann Manag. 2006;21(2):101‐115. 10.1002/hpm.834 [DOI] [PubMed] [Google Scholar]
- 31. Krasna H, Kornfeld J, Cushman L, Ni S, Antoniou P, March D. The new public health workforce: employment outcomes of public health graduate students. J Public Health Manag Pract. 2019;27:12–19. 10.1097/PHH.0000000000000976 [DOI] [PubMed] [Google Scholar]
- 32. Plepys C, Krasna H, Leider J, Burke E, Blakely C, Magana L. First‐destination outcomes for 2015‐2018 public health graduates: focus on employment. Am J Publ Health. 2020;111(3):475–484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Yeager VA, Beitsch LM, Hasbrouck L. A mismatch between the educational pipeline and public health workforce: can it Be reconciled? Publ Health Rep. 2016;131(3):507‐509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Yeager VA, Beitsch LM, Johnson SM, Halverson PK. Public health graduates and employment in governmental public health: factors that facilitate and deter working in this setting. J Public Health Manag Pract. 2019;27:4–11. 10.1097/PHH.0000000000001052 [DOI] [PubMed] [Google Scholar]
- 35. Martin‐Moreno JM. Self‐assessment tool for the evaluation of essential public health operations in the WHO European Region (2015); 113, 2015. https://www.euro.who.int/en/publications/abstracts/self-assessment-tool-for-the-evaluation-of-essential-public-health-operations-in-the-who-european-region-2015. Accessed Feb. 16, 2021. [Google Scholar]
- 36. “Labor InsightTM real‐time labor market information tool.” burning Glass technologies, 2020. https://www.burning‐glass.com/job‐market‐data/. Accessed November 2. [Google Scholar]
- 37. Krasna H, Czabanowska K, Jiang S, et al. The future of careers at the intersection of climate change and public health: what can job postings and an employer survey tell us? Int J Environ Res Publ Health. 2020;17(4):1310. 10.3390/ijerph17041310 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Keralis JM, Riggin‐Pathak BL, Majeski T, et al. Mapping the global health employment market: an analysis of global health jobs. BMC Publ Health. 2018;18(1):293. 10.1186/s12889-018-5195-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Frankenfeld CL. Trends in employer postings for epidemiology jobs: an analysis of PublicHealthJobs.net data from 2003 to 2016. Ann Epidemiol. 2017;27(9):553‐557. 10.1016/j.annepidem.2017.08.007e1. [DOI] [PubMed] [Google Scholar]
- 40. Kahn LB, Lange F, Wiczer DG. Labor Demand in the Time Of COVID‐19: Evidence from Vacancy Postings and UI Claims. National Bureau of Economic Research. 2020. 10.3386/w27061 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Watts RD, Bowles DC, Fisher C, Li IW. Public health job advertisements in Australia and New Zealand: a changing landscape. Aust N Z J Publ Health. 2019;43(6):522‐528. 10.1111/1753-6405.12931 [DOI] [PubMed] [Google Scholar]
- 42. Bureau of Labor Statistics . Crosswalk between the international standard classification of occupations (ISCO‐08) and the 2010 standard occupational classification (SOC). 2020. https://www.bls.gov/soc/isco_soc_crosswalk_process.pdf. Accessed November 21. [Google Scholar]
- 43. Beck AJ, Coronado F, Boulton ML, Merrill JA. The public health workforce taxonomy: revisions and recommendations for implementation. J Publ Health Manag Pract. 2017;00(00). 10.1097/PHH.0000000000000690 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Gebbie K, Merrill J, Sanders L, Gebbie EN, Chen DW. Public Health Workforce Enumeration: Beware the “Quick Fix”. J. Public Health Management Practice. 2007;13(1):72‐79. [DOI] [PubMed] [Google Scholar]
- 45. Gebbie KM, Raziano A, Elliott S. Public health workforce enumeration. Am J Publ Health. 2009;99(5):786‐787. 10.2105/AJPH.2008.137539 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Gebbie KM. The Public Health Work Force: Enumeration 2000. U.S. Department of Health and Human Services, Health Resources and Services Administration, Bureau of Health Professions, National Center for Health Workforce Information and Analysis. 2000. [Google Scholar]
- 47. Russ DE, Ho K‐Y, Colt JS, et al. Computer‐based coding of free‐text job descriptions to efficiently identify occupations in epidemiological studies. Occup Environ Med. 2016;73(6):417‐424. 10.1136/oemed-2015-103152 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. ONS. ONS Occupation Coding Tool . Office for National Statistics. 2020. https://onsdigital.github.io/dp‐classification‐tools/standard‐occupational‐classification/ONS_SOC_occupation_coding_tool.html. Accessed November 22. [Google Scholar]
- 49. Classifying the standard occupational classification 2020 (SOC 2020) to the international standard classification of occupations (ISCO‐08) ‐ office for national statistics, 2020. https://www.ons.gov.uk/methodology/classificationsandstandards/standardoccupationalclassificationsoc/soc2020/classifyingthestandardoccupationalclassification2020soc2020totheinternationalstandardclassificationofoccupationsisco08. Accessed November 22. [Google Scholar]
- 50. Morgan P, Leach B, Himmerick K, Everett C. Job openings for PAs by specialty. J Am Acad PAs. 2018;31(1):45‐47. 10.1097/01.JAA.0000527701.08322.18 [DOI] [PubMed] [Google Scholar]
- 51. Deming DJ, Noray KL. STEM Careers and the Changing Skill Requirements of Work. National Bureau of Economic Research. 2018. 10.3386/w25065 [DOI] [Google Scholar]
- 52. Deming D, Kahn L. Skill Requirements across Firms and Labor Markets: Evidence from Job Postings for Professionals. National Bureau of Economic Research. 2017. [Google Scholar]
- 53. CIP user site, 2019. https://nces.ed.gov/ipeds/cipcode/resources.aspx?y=55. Accessed December 16. [Google Scholar]
- 54. Sellers K, Leider JP, Harper E, et al. The public health workforce Interests and needs survey: the first national survey of state health agency employees. J Public Health Manag Pract JPHMP. 2015;21(Suppl 6):S13‐S27. 10.1097/PHH.0000000000000331 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Effects of COVID‐19 Pandemic on Job Openings and Labor Turnover News Release and Data : U.S. Bureau of Labor Statistics, 2020. https://www.bls.gov/covid19/effects‐of‐covid‐19‐pandemic‐on‐job‐openings‐and‐labor‐turnover‐data.htm. Accessed November 7. [Google Scholar]
- 56. Beck AJ, Leider JP, Krasna H, Resnick BA. Monetary and nonmonetary costs and benefits of a public health master's degree in the 21st century. Am J Publ Health. 2020;110(7):978‐985. 10.2105/AJPH.2020.305648 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Moore J. Studying an ill‐defined workforce: public health workforce research. J Public Health Manag Pract. 2009;15(6 Suppl):S48‐S53. 10.1097/PHH.0b013e3181b23978 [DOI] [PubMed] [Google Scholar]
- 58. Leider JP, Harper E, Bharthapudi K, Castrucci BC. Educational attainment of the public health workforce and its implications for workforce development. J Public Health Manag Pract. 2015;21(Suppl 6):S56‐S68. 10.1097/PHH.0000000000000306 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. O*NET OnLine, 2020. https://www.onetonline.org/. Accessed August 21. [Google Scholar]
- 60. Wright J. PHORCaSTING insights on public health careers. Perspect Public Health. 2011;131(1):20‐21. 10.1177/17579139111310011202 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Material 1
Supplementary Material 2
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.