

Abstract
Background
When an outbreak emerged, each country needs a coherent and preventive plan to deal with epidemics. In the era of technology, adopting informatics‐based solutions is essential. The main objective of this study is to propose a conceptual framework to provide a rapid and responsive surveillance system against pandemics.
Methods
A three‐step approach was employed in this research to develop a conceptual framework. These three steps comprise (1) literature review, (2) extracting and coding concepts, and determining main themes based on thematic analysis using ATLAS.ti® software, and (3) mapping concepts. Later, all of the results synthesized under expert consultation to design a conceptual framework based on the main themes and identified strategies related to medical informatics.
Results
In the literature review phase, 65 articles were identified as eligible studies for analysis. Through line by line coding in thematic analysis, more than 46 themes were extracted as potential foremost themes. Based on the key themes and strategies were employed by studies, the proposed framework designed in three main components. The most appropriate strategies that can be used in each section were identified based on the demands of each part and the available solutions. These solutions were employed in the final framework.
Conclusion
The presented model in this study can be the first step for a better understanding of the potential of medical informatics solutions in promoting epidemic disease management. It can be applied as a reference model for designing intelligent surveillance systems to prepare for probable future pandemics.
Keywords: civil defence, electronic surveillance system, framework, pandemics, medical informatics
1. INTRODUCTION
According to World Health Organization (WHO), the pandemic is commonly defined as the worldwide spread of a new communicable disease. 1 , 2 The randomness and unpredictability of such diseases is a prominent feature of each new pandemic. This feature causes countries to face inevitable challenges. 3 , 4 , 5 When a disease outbreak began, most people lack natural immunity to fight it. It can cause a rapid transmission of new pandemic across countries over a specific amount of time. 6 The unfamiliar aspects and highly contagious nature of the current COVID‐19 pandemic, have shown that every country requires a coherent and responsive plan to battle against the current pandemic. 7 By the 10 October 2020, there had been 1083140 COVID‐19 deaths worldwide. A high mortality rate of this new virus has raised many concerns about the unpreparedness of countries to use appropriate methods to control, prevent and address unexpected epidemiological conditions. 8 Thus, during a pandemic outbreak, health care system preparedness is essential. In similar epidemics around the world, various countries have taken different approaches based on the last advancement of technologies and health‐IT based solutions. 9
In former pandemics, various digital health strategies have been used with different approaches to control other epidemics such as the Middle East respiratory syndrome, severe acute respiratory syndrome and H1N1 flu. 10 , 11 , 12 For example, a team of scientists from Pakistan invented a smart tool called ID‐Viewer as a decision‐making system for predicting an infectious disease outbreak in 2016. 13 It was employed to detect the dengue epidemic for 20 weeks earlier by gathering and analysing all related information about dengue disease since 2011. 14 In a similar study conducted in 2012, Chinese researchers were able to predict abnormal outbreaks and warn the health system before its emergence by implementation a continuous and intelligent monitoring system to analyse real‐time data of various diseases. 15 , 16
The recent global epidemic has proved that e‐health technologies can be used to control the spread of disease. In a recent report, Healthcare Information and Management Systems Society reported that digital tools such as telemedicine, remote patient monitoring, data analysis methods and even artificial intelligence (AI)‐based solutions could play a significant role in restricting the prevalence of COVID‐19. 17
However, the sudden emergence of the epidemic has proven that just awareness of the latest technologies is not adequate. The most significant point to fight epidemic diseases by applying the latest technologies is to know how to use these tools most appropriately in outbreaks. 18 Consequently, to prepare for combat against the spread of diseases, an appropriate model based on the latest medical informatics solutions is needed. It seems that the time has come to use digital technologies at different levels of the health system based on the experiences of other countries to combat the epidemic of infectious diseases. 19
The main objective of this study is to propose a conceptual framework for designing an appropriate and comprehensive electronic surveillance system for preparedness against the pandemic. Other aims of this study include identifying the most proper solutions in medical informatics that can be used to predict, diagnose, control and manage the COVID‐19 outbreak and other pandemics.
2. METHODS
In this qualitative research, a three‐step approach was applied to outline a conceptual framework. These three steps included (1) literature review, (2) extracting concepts and main themes based on qualitative analysis, and (3) mapping concepts, and synthesizing the results with expert consultation. The qualitative synthesis was conducted based on the Standards for Reporting Qualitative Research checklist, which can help researchers to report their results correctly. 20
2.1. Literature review
The systematic search was performed in four scientific databases, Web of Science, Scopus, PubMed and Science Direct from 2000 to August 2020. The search strategy and keywords are shown in Table A1, Supplementary Appendix. All articles retrieved from database searches entered into Mendeley as the resource management software. The systematic review was conducted based on the preferred reporting items for systematic reviews and meta‐analyses steps. Some inclusion and exclusion criteria were determined for reviewing articles.
Articles included if they were original articles and if they used solutions or strategies to prepare for a sudden outbreak or control of an epidemic disease based on digital health. Solutions regarding social relations, military and cultural measures are not considered. Non‐English papers, letter to editors, commentary papers, book chapters, short briefs, reports, technical reports, any reviews or meta‐analysis were excluded.
After duplication removal, the articles were omitted regarding the type of articles. Next, the remaining studies were reviewed based on titles and abstracts. All titles and abstracts of articles were examined to select eligible studies by reviewers. Marsa Gholamzadeh screened all titles and abstracts to find relevant articles. A second reviewer (Hamidreza Abtahi) reviewed a sample of studies randomly. Following, articles that met our inclusion criteria were selected for full‐text review. After that, the full texts of relevant studies were screened thoroughly by all authors. If there was a disagreement between the authors, the final decision was made by Reza Safdari. Finally, the information of the included articles extracted based on characteristics such as author name, year of publication, title, purpose of the study, country, institution, proposed solution and type of disease and pandemic.
2.2. Qualitative and thematic analysis
Since thematic analysis known as one of the best methods in qualitative analysis, we applied it in our research. 21 Following a systematic investigation, the remained articles met our criteria were imported to ATLAS.ti® software to conduct an inquiry using inductive thematic analysis. It is a free famous software that is mostly used for content analysis by coding and analysing complex textual data. 22
All included articles were imported into the ATLAS.ti® software. All of the studies were screened line by line to code the preliminary idea. By connecting extracted codes, the fundamental themes were extended to achieve a thematic map. All potential themes were depicted in the form of a thematic tree to define themes and sub‐themes. Coding and thematic analysis stages were conducted by one of the authors (Marsa Gholamzadeh) who had experience in analysing and reviewing studies under the supervision of health informatics experts. The information extracted by the researchers was re‐examined to reach an agreement. The next reviewers (Hamidreza Abtahi and Reza Safdari) assessed and verified the extracted information.
2.3. Mapping concepts and designing the conceptual model
Under expert consultation, all of the extracted themes were investigated and integrated. The initial model devised in this step is based on key themes and sub‐themes. Then, in an iterative process, a conceptual framework was defined and redesigned to achieve the optimal model. In the following, the suggested conceptual model and the strategies for outbreak preparedness were described. The different parts of the proposed model are defined based on the solutions available concerning the various branches of medical informatics.
3. RESULTS
3.1. Literature review
Initial searches in scientific databases yielded 397 citations. After removing 71 duplicated articles, 326 citations were screened based on the type of studies. Next, 300 articles remained due to their relevancy in the abstract screening phase. Then, the full‐text of 249 studies were reviewed. Finally, 65 citations were identified as eligible studies to meet our criteria. The process of screening articles is shown in Figure 1. A summary of the included articles based on predefined categories is described in Table 1.
FIGURE 1.
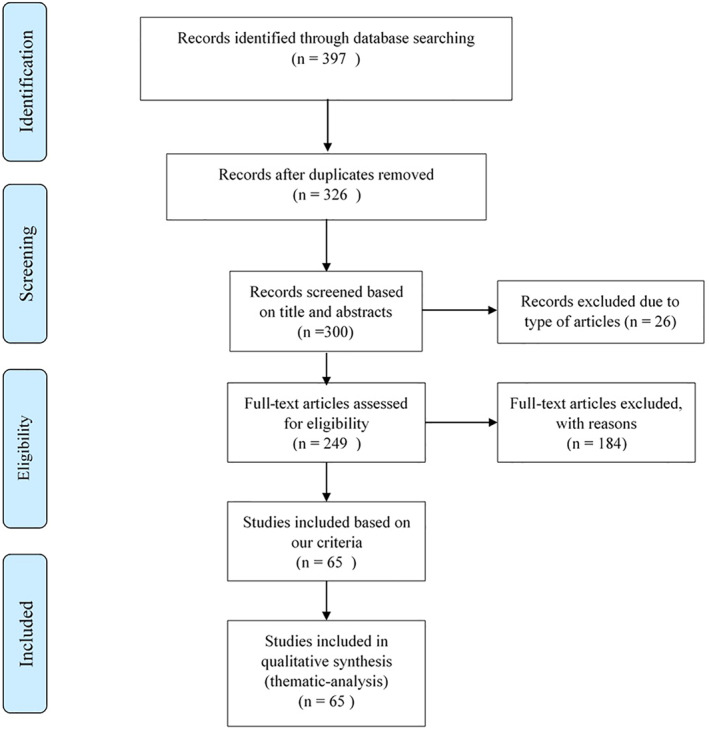
Screening flow based on the preferred reporting items for systematic reviews and meta‐analyses method
TABLE 1.
Summary of reviewed articles
| Author | Year | Journal | Recommended solution | Illness | Main objective | Institution | |
|---|---|---|---|---|---|---|---|
| 1 | Aaby. K et al. | 2006 | J Public Health Manag Pract | Develop Clinic Planning Model Generator or computer program | Pandemic influenza outbreak | To determine points of dispensing (pods) for mass distribution of vaccine | Maryland's Advanced Practice Center for Public Health Emergency Preparedness and Response and the Institute for Systems Research at the University of Maryland. |
| 2 | Abramovich. M et al. | 2017 | American journal of infection control | Computer modelling and simulations using various combinations of variables to determine resource needs | Pandemic influenza outbreak | To model many other hospital preparedness issues | Mayo clinic |
| 3 | Abramovich. M et al. | 2008 | Biosecurity and bioterrorism: biodefense strategy, practice and science | Develop a new tool to estimate the likely healthcare consequences of a pandemic and to aid hospitals in the development of mitigation and response strategies | Influenza outbreak | To plan for a 1918‐like flu pandemic | Not mentioned |
| 4 | Agolory. S et al. | 2008 | PloS one | School preparedness planning and non‐pharmaceutical interventions, including handwashing and use of hand sanitizer | H1N1 pandemic influenza | To mitigate the effects of an influenza outbreak | CDC |
| 5 | Akselrod. H et al. | 2012 | Journal of business continuity & emergency planning | An operational structure that will facilitate the integration of modelling capabilities into action planning for outbreak management | Infectious outbreaks | Real‐time modelling output with anticipated decision points | CDC |
| 6 | Araz. OM | 2013 | Journal of Systems Science and Systems Engineering | A multi‐criteria decision‐making framework, | Not mentioned | Predicting temporal and geographic patterns of disease spread | OMAHA |
| 7 | Araz. OM et al. | 2012 | J Med Syst | Simulation model | H1N1 influenza outbreak, | To prepare university emergency response executives, management, and operational emergency response infrastructure to collaboratively evaluate the university's pandemic influenza emergency response plan | Arizona state university |
| 8 | Buckeridge. D et al. | 2008 | AMIA Annu Symp Proc | To develop quantitative models | Not mentioned | To develop quantitative evidence about the determinants of outbreak detection as a means of supporting manual and automated evidence‐based method selection for public health surveillance. | Not mentioned |
| 9 | Burke. D et al. | 2006 | Academic emergency medicine: official journal of the Society for Academic Emergency Medicine | Agent‐based model | Smallpox epidemic | To evaluate the potential effectiveness of epidemic control strategies that might be deployed in response to a bioterrorist attack | Johns Hopkins |
| 10 | Ceccato. P et al. | 2007 | The American journal of tropical medicine and hygiene | Developing malaria early warning program | Malaria | To define five areas with distinct malaria intensity and seasonality patterns, to guide future interventions and development of an epidemic early warning system. | Brazilian agencies CAPES |
| 11 | Colon‐Gonzalez. F et al. | 2018 | BMC public health | Syndromic surveillance systems | Influenza outbreak | To investigate how the characteristics of different disease outbreaks affected and the time to detection. | University of East Anglia |
| 12 | Cruz. A et al. | 2010 | Annals of emergency medicine | A mobile paediatric emergency response team | H1N1 influenza outbreak, | Describe the implementation of a mobile paediatric emergency response team for mildly ill children with influenza‐like illnesses during the H1N1 swine influenza outbreak. | Not mentioned |
| 13 | Daniel. J et al. | 2005 | MMWR. Morbidity and mortality weekly report | Syndromic surveillance systems | Not mentioned | To identify and report acute illness clusters to health departments | State laboratory institute |
| 14 | Dias. T et al. | 2013 | 2013 BRICS Congress on Computational Intelligence and 11th Brazilian Congress on Computational Intelligence | Development of a semantic platform for decision support based on the DOODA cycle | Dengue | To help dengue epidemics control | Not mentioned |
| 15 | Dopson. S | 2009 | Biosecurity and bioterrorism: biodefense strategy, practice and science | Early Warning Infectious Disease Surveillance program (EWIDS) | Not mentioned | To develop and implement a program to collaborate with states or provinces across international borders, to provide rapid and effective laboratory confirmation, and to expand surveillance capabilities | CDC |
| 16 | Drumright. L et al. | 2015 | BMC Infectious Diseases | Early warning and robust estimation of influenza burden system | Influenza | To inform hospital preparedness and operational, treatment and vaccination policies | Not mentioned |
| 17 | Eichner. M et al. | 2007 | BMC infectious diseases | Complex computer simulations | Not mentioned | To operate with an optimal combination of the competing requirements of precision, realism and generality. | Not mentioned |
| 18 | Ekong. I et al. | 2020 | JMIR mHealth and uHealth | Designing mobile position data contact tracing | COVID‐19 | To survey strategies for digital contact tracing for the COVID‐19 pandemic and to present how using mobile positioning data conforms with Nigeria's data privacy regulations | Not mentioned |
| 19 | Fan. C et al. | 2010 | Canadian Journal of Public Health | Automated Mortality Surveillance System (MSS) | Pandemic H1N1 (ph1n1) influenza | To support evidence‐based decision‐making by physicians and public health. | Not mentioned |
| 20 | Farias. D et al. | 2010 | Disaster Medicine and Public Health Preparedness | Integrated data management system | Influenza A (H1N1) pandemic, | To create a single daily monitoring tool that could integrate multiple information sources | Not mentioned |
| 21 | Gould et al. | 2017 | Public health reports | Prevention‐centric program to one focused on building syndromic surveillance capacity at the state and local level | Various hazardous events and disease outbreaks | Establishing a nationwide integrated public health surveillance system for early detection and assessment of potential bioterrorism‐related illness | CDC |
| 22 | Guo. D et al. | 2014 | 8th International Symposium of the Digital Earth, ISDE 2014 | Cloud computation environment, supports aggregation of massive unstructured and semi‐structured data, integration of various computing model sand algorithms; | Various hazardous events and disease outbreaks | Propose a three‐tier collaborative Spatio‐temporal visual analysis architecture to support emergency management. | Not mentioned |
| 23 | Horad. M et al. | 2005 | International Journal of Hygiene and Environmental Health | To create computer simulation models as ‘what‐if’ tools for disaster preparedness planners. We have recently applied the approach to the issue of hospital surge capacity, and have reached some preliminary conclusions | Rural disaster | To introduce a conceptual framework for a study that applies a rigorous systems approach to rural disaster preparedness and planning | Not mentioned |
| 24 | Hutchins. S et al. | 2008 | Clinical infectious diseases: an official publication of the Infectious Diseases Society of America | Developing an algorithm for clinical evaluation of suspected smallpox disease. | Suspected smallpox | Developed an algorithm to evaluate patients rapidly for suspected smallpox. | CDC |
| 25 | James. A et al. | 2007 | Proceedings. Biological sciences | Developing a super spreading model | severe acute respiratory syndrome (SARS) and Ebola | To increase the probability that an outbreak will eventually cease, rather than continuing indefinitely | Not mentioned |
| 26 | Kahn. R et al. | 2019 | Prehospital and Disaster Medicine | Developing a simple model to forecast areas at highest risk of a cholera outbreak | Cholera | Determining when and where outbreaks happen and spread | Not mentioned |
| 27 | Lee. E et al. | 2009 | INTERFACES | Developing a fast and practical emergency‐response decision‐support tool | All disasters | To analyse planning strategies, compare the various options, and determine the most cost‐effective combination of dispensing strategies is critical to the ultimate success of any mass dispensing effort | Not mentioned |
| 28 | Li. Y et al. | 2017 | Disaster medicine and public health preparedness | Mobile‐based database with the application‐based server | Infectious outbreaks | To build a database to collect infectious disease information at the scene of a disaster, with rapid acquisition of information regarding the infectious disease and rapid questionnaire customization at the scene of disaster relief by the use of a personal digital assistant (PDA) | Not mentioned |
| 29 | Loonsk. J et al. | 2004 | MMWR. Morbidity and mortality weekly report | Near‐real‐time electronic transmission of data to local, state and federal public health agencies from national regional, and local health data sources | All disasters | To enhance the nation's capability to detect, quantify and localize public health emergencies rapidly | Department of Defence and Veterans Administration medical treatment |
| 30 | Luo. W | 2016 | International journal of health geographics | Geo‐social visualize model | All disasters | To examine the effectiveness of control strategies taking into account geo‐social interaction patterns | Not mentioned |
| 31 | Mahmood. I et al. | 2020 | International Conference on Computational Science | Developing a simulation framework that models population dynamics and the interactions of both humans and mosquitoes | Dengue | To analyse and forecast the transmission and spread of an infectious disease in specific areas | Not mentioned |
| 34 | Murray et al. | 2007 | Developments in Biologicals | Modelling | All disasters | The effectiveness of modelling in outbreak control | Not mentioned |
| 35 | Ndeffo. M et al. | 2011 | PloS one | Our model provides new insights for policymakers in the optimal deployment of limited resources for control in the event of epidemic outbreaks at the landscape scale. | All disasters | To minimize the discounted number of infected individuals during an epidemic by designing a simple SIRS model | Not mentioned |
| 36 | Nguyen et al. | 2018 | BMC public health | Mathematical models that we simulated mechanistically its transmission parameters. | Ebola virus | A multiscale approach showing that individual dynamics were able to reproduce population‐level observations. | Not mentioned |
| 37 | Nuño. M et al. | 2008 | Proceedings of the National Academy of Sciences of the United States of America | On pharmaceutical interventions mathematical model to model a residential care facility | Influenza pandemic | To determine whether an intrinsic ability to control access to these facilities provided a basis for protection against pandemic influenza | Not mentioned |
| 38 | Patroniti. N et al. | 2011 | Intensive care medicine | Set up a national referral network of selected intensive care units (ICU) able to provide advanced respiratory care up to extracorporeal membrane oxygenation (ECMO) for patients with acute respiratory distress syndrome | H1N1 and SARS | To centralize all potentially severe patients and all necessary resources in a limited number of tertiary hospitals to provide advanced treatment options including ECMO | Italian Ministry of Health |
| 39 | Paul. J et al. | 2012 | Journal of Homeland Security and Emergency Management | Graph matching methods | H1N1 | A mixed‐integer programming model (MIP) that analyses patient symptom data available at hospitals to generate patient graph match scores. | Kennesaw state university |
| 40 | Piltch‐Loeb. R et al. | 2014 | Biosecurity and bioterrorism: biodefense strategy, practice and science | Critical incident registry | H1N1 influenza pandemic | To identify the optimal characteristics of a critical incident registry (CIR) for public health emergency preparedness | Not mentioned |
| 41 | Pogreba‐Brown. K et al. | 2013 | Disaster Medicine and Public Health Preparedness | Syndromic surveillance system | All disasters | To develop an onsite syndromic surveillance system for the early detection of public health emergencies and outbreaks at large public events | The Maricopa County Department of Public Health(MCDPH) |
| 42 | Raude. J and Setbon. M | 2011 | PLoS ONE | Factor analyses to provide insight into the nature and predictors of the protective patterns | Influenza outbreak | To protect people from the risk of infection in the case of an avian influenza outbreak, as well as the lay perceptions of the threat that underlie these risk reduction strategies. | Not mentioned |
| 43 | Riley. S and Ferguson. N | 2006 | Proceedings of the National Academy of Sciences of the United States of America | Developing the Markov chain Monte‐Carlo algorithm to generate sociospatial contact networks that were consistent with demographic and commuting data. | Smallpox epidemic | To ensure that widespread community transmission does not occur. | Not mentioned |
| 44 | Rosenfeld. R et al. | 2009 | Journal of public health management and practice: JPHMP | Use of preparedness modelling to enhance the planning for vulnerable and at‐risk populations, all‐hazard emergencies and infectious disease containment strategies | Pandemic influenza | using computer modelling and scenario‐based analyses to better frame problems and opportunities, integrate data sources, expect outcomes and improve multistakeholder decision‐making | CDC |
| 45 | Sacks. J et al. | 2015 | Global health, science and practice | Building the mobile application compare and business intelligence software for real‐time identification of contacts and contact tracers through timestamps and collection of GPS points with their surveillance data. | Ebola virus | To develop a smartphone‐based contact tracing system that is linked to analytics and data visualization software as part of the Ebola response in Guinea | Not mentioned |
| 46 | Schwartz. R and Bayles. B | 2012 | American journal of infection control | Developing university pandemic influenza‐dedicated Web sites as an information source | H1N1 influenza pandemic | Representing information regarding preparedness and response plans against outbreaks at pandemic‐dedicated university Web sites | Not mentioned |
| 47 | Senel. K et al. | 2020 | Disaster Medicine and Public Health Preparedness | Proposing an ‘Single Parameter Estimation’ approach to circumvent potential problems and check the robustness of this new approach by model variation and structured permutation tests. | COVID‐19 | To predict the progress of COVID‐19 worldwide, despite their rather simplistic nature. | Not mentioned |
| 48 | Shearer. F et al. | 2020 | PloS one | Propose a decision support system | Infectious disease | To synthesize the available data to provide enhanced situational awareness, to predict the future course of the pandemic and likely associated social and economic costs, and to plan mitigation strategies | Us army international technology center Pacific (itc‐pac) |
| 49 | Shimoni. Z et al. | 2006 | Medical Hypotheses | Developing automate disease surveillance system with online monitoring, be independent of the medical personnel | Influenza | Acute planning of distribution of medical resources | Not mentioned |
| 50 | Shin. E et al. | 2020 | Studies in health technology and informatics | Developing a Globally Localized Epidemic Knowledgebase (GLEK) that can be utilized for efficient and optimal epidemic surveillance | SARS and Middle East respiratory syndrome | Customizing the local needs by developing best‐tailored intervention | Ministry of Education of the Republic of Korea |
| 51 | Stein. M et al. | 2012 | BMC public health | Developing the asiaflucap Simulator which was built in MS Excel© and contains a user‐friendly interface which allows users to select mild or severe pandemic scenarios, change resource parameters and run simulations for one or multiple regions | H1N1 | To implement response measures or interventions described in plans and trained in exercises based on the available resource capacity | National Institute for Public Health and the Environment (RIVM) |
| 52 | Steward. D et al. | 2007 | Journal of medical systems | Simulation model | All disasters | Preparation and evaluation of the model | Not mentioned |
| 53 | Suganthe. R and Sreekanth. G | 2016 | Journal of Medical Imaging and Health Informatics | Epidemic routing (ER) protocol within the cluster | All disasters | To decrease a Delay Tolerant Network environment typically contains comparatively sparse nodes which leads to a network partition. | Not mentioned |
| 54 | Tiwari. S et al. | 2020 | Disaster Medicine and Public Health Preparedness | Developing a prediction model with machine learning methods | COVID‐19 | The objective of this paper is to prepare the government and citizens of India to take or implement the control measures proactively to reduce the impact of coronavirus disease 2019 (COVID‐19). | Not mentioned |
| 55 | Tizzoni. M et al. | 2014 | PLoS computational biology | Modelling Human mobility as a large‐scale spatial‐transmission model of infectious diseases | Influenza‐like‐illness epidemic | Correctly modelling and quantifying human mobility | Not mentioned |
| 56 | Todkill. D et al. | 2017 | Prehospital and Disaster Medicine | Presenting Ambulance data syndromic surveillance system (ADSSS) | All disasters | Feasibility of ambulance Data Syndromic Surveillance System (ADSSS) and utility in enhancing the existing suite of PHE syndromic surveillance systems | Mfph public health England, |
| 57 | Turner. A et al. | 2018 | Disaster medicine and public health preparedness | Developing an Infectious disease network (IDN) | Ebola virus disease (EVD) | To provide a coordinated response and utilize appropriate personal protective equipment (PPE) for the transport or treatment of a suspected or confirmed serious communicable disease patient. | Georgia Department of Public Health |
| 58 | Vokinger. N et al. | 2020 | Swiss medical weekly | Developing a mobile‐based framework for applications | COVID‐19 | Building on an existing trustworthiness checklist for digital health applications to contribute to controlling the current epidemic or mitigating its effects. | Institute for Implementation Science in Health Care |
| 59 | Wallace. D et al. | 2006 | Resuscitation | Designing robotic patient simulators or Simulation resource utilization | Influenza | To resuscitate simulators and actors during a drill and compares the times required to perform procedures on simulator patients to published values for real patients. | Kings county hospital center |
| 60 | Wang. J et al. | 2008 | Journal of public health (Oxford, England) | Data‐based analysis to find link and association | Severe acute respiratory syndrome (sars) | To develop a mathematically rigorous and scientifically meaningful SARS modelling framework that accounts for the crucial epidemic associations | Beijing Center for Disease Control |
| 61 | Wu. J et al. | 2011 | Experimental Biology and Medicine | Developing mathematical models of infectious diseases | Influenza pandemics 2009 | Developing mathematical models have been widely used in the past decade to aid pandemic planning by allowing detailed predictions of the speed of the influenza pandemic and the likely effectiveness of alternative control strategies | Harvard Center for Communicable Disease Dynamics |
| 62 | Yaylali. E et al. | 2014 | Public health reports | Simulation model ‐Markov modelling | 2009 H1N1 outbreak | To provide sophisticated techniques that can model the system, simulate, and optimize complex systems, even under uncertainty. | CDC and North Carolina Preparedness and Emergency Response Research Center |
| 63 | Zaric. G et al. | 2002 | IMA Journal of mathematics applied in medicine and biology | Computational analyses or some reallocation of resources over the time horizon of the problem | All disasters | To develop a dynamic resource allocation model in which a limited budget for epidemic control is allocated over multiple periods that affect multiple populations. | Not mentioned |
| 64 | Zhan. Y et al. | 2010 | 2010 International Conference on Management and Service Science, MASS 2010 | Developing a GIS and decision support model | All disasters | To assist government authorities to identify evacuation strategy shortly after the outbreak of disasters, and proposes a GIS‐based urban emergency decision support model for large‐scale crowd evacuation. | Not mentioned |
| 65 | Zhang. X et al. 23 | 2020 | Wuhan Daxue Xuebao (Xinxi Kexue Ban)/Geomatics and Information Science of Wuhan University | Integration of vertical system and horizontal system, based on the idea of ‘let data run more, rely on accurate information, and outperform viruses with electromagnetic waves’. | COVID‐19 | Providing a solution to increase speed for efficient management of time, data, information and resources in disease outbreaks | Geomatics and Information Science of Wuhan University |
Abbreviations: CDC, Centers for Disease Control and Prevention; GIS, geographic information system.
The analysis of the most significant features of the reviewed articles is represented in Table 2. Regarding the country, the United States has used medical informatics solutions more than any other country to control pandemics. On the other hand, the analysis revealed that most of the efforts devoted to controlling the spread of influenza outbreaks (41.54%) and employing medical informatics solutions. The trend of published articles regarding our objective had steady growth until the COVID‐19 outbreak in 2020. Though, eight articles were published regarding outbreak preparedness from the beginning of 2020 up to 2 August 2020.
TABLE 2.
Analysis of some characteristics of included articles
| Article type | Frequency | Percentage |
|---|---|---|
| Conference proceedings | 8 | 12.7% |
| Journal | 55 | 87.3% |
| Year of publication | ||
| 2000–2004 | 2 | 3.2% |
| 2005–2008 | 18 | 28.6% |
| 2009–2012 | 16 | 25.4% |
| 2013–2016 | 11 | 17.5% |
| 2017–2020 | 16 | 25.4% |
| Country | ||
| USA | 17 | 27.0% |
| UK | 5 | 7.9% |
| Canada | 3 | 4.8% |
| China | 3 | 4.8% |
| Georgia | 3 | 4.8% |
| Germany | 2 | 3.2% |
| Argentina | 1 | 1.6% |
| Brazil | 1 | 1.6% |
| More than two European countries | 1 | 1.6% |
| France | 1 | 1.6% |
| Guinea | 1 | 1.6% |
| India | 1 | 1.6% |
| Israel | 1 | 1.6% |
| Italy | 1 | 1.6% |
| Korea | 1 | 1.6% |
| Montgomery | 1 | 1.6% |
| Mozambique | 1 | 1.6% |
| Switzerland | 1 | 1.6% |
| Not mentioned | 18 | 28.6% |
| Problems | ||
| All disasters | 15 | 23.08% |
| H1N1 and Influenza outbreak | 27 | 41.54% |
| COVID‐19 | 5 | 7.69% |
| Ebola virus disease | 4 | 6.15% |
| Severe acute respiratory syndrome | 1 | 1.54% |
| Smallpox epidemic | 3 | 4.62% |
| Dengue | 2 | 3.08% |
| Middle East respiratory syndrome | 1 | 1.54% |
| Cholera | 1 | 1.54% |
| Malaria | 1 | 1.54% |
| Rural disaster | 1 | 1.54% |
| Other infectious diseases | 4 | 6.15% |
Based on the central idea of our research, all studies were examined based on their tactics and strategies related to the medical informatics disciplines. Overall, all of the employed strategies can be devoted to 19 categories. These categories are represented based on their frequency and percentage in Table 3. It is worth noting that most studies used a combination of different techniques and did not focus on just one specific solution but most strategies were related to developing AI‐based models.
TABLE 3.
Applied medical informatics‐based solutions with their frequency
| Applied solutions | Frequency | Percentage |
|---|---|---|
| Emergency response system | 31 | 47.7% |
| Computational methods | 30 | 46.2% |
| Outbreak prediction models | 26 | 40.0% |
| Resource allocation systems | 23 | 35.4% |
| AI‐based algorithms | 22 | 33.8% |
| Epidemiological model | 20 | 30.8% |
| Database and registry systems | 18 | 27.7% |
| Warning system | 17 | 26.2% |
| Simulation models | 17 | 26.2% |
| Patient management systems | 14 | 21.5% |
| Geographic positioning | 12 | 18.5% |
| Geographic transmission model | 10 | 15.4% |
| Clinical decision support system (CDSS) | 9 | 13.8% |
| Syndromic surveillance systems | 8 | 12.3% |
| Network of information | 8 | 12.3% |
| Mobile‐based system | 4 | 6.2% |
| Providing preparedness information | 2 | 3.1% |
| Cloud computing | 1 | 1.5% |
| Computerized network protocol | 1 | 1.5% |
3.2. Thematic analysis outcomes
After coding all the themes and sub‐themes, more than 46 themes were extracted as potential main themes. By integrating all of the potential themes, the mapped network of themes is devised and illustrated in Figure 2. Conclusively, all of the themes are summarized regarding recommended and applied strategies in three main categories. These categories were used to devise a conceptual model:
Epidemiological solutions and surveillance systems
Research‐based solution to manage and predict an outbreak
Clinical care planning, inpatient and outpatient management strategies
FIGURE 2.
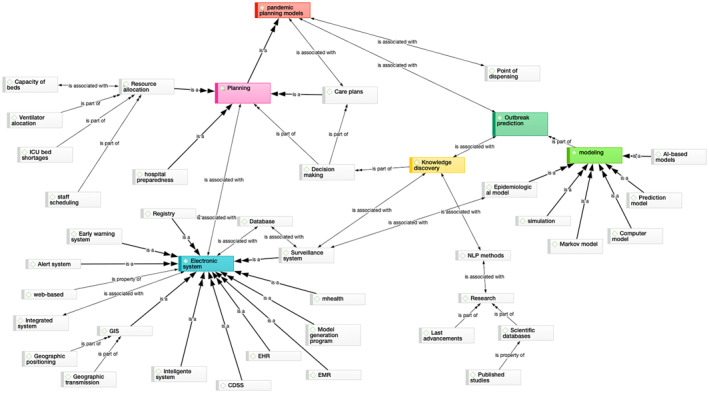
Thematic map of main concepts extracted from the literature review
3.3. Suggested conceptual framework
The most appropriate solutions that can be used in each section are identified based on the integration of the requirements and the available solutions in the proposed model. In the following, the most suitable model for better epidemic management is designed in each section using the identified solutions.
3.3.1. Epidemiological subsystem
Analysis of articles showed that mathematical models have the potential to aid clinical decision‐makers to forecast the next epidemic and prepare for a proper pandemic. Besides, the thematic analysis revealed that predictive modelling was the most common solution to develop an early warning system. It has the potential to predict outbreaks for providing emergency response. Analysis of studies showed that outbreak prediction models, AI‐based algorithms and early warning systems, in combination with geographical positioning strategies can be adopted in this section. The schematic model of this subsystem is represented in Figure 3.
FIGURE 3.
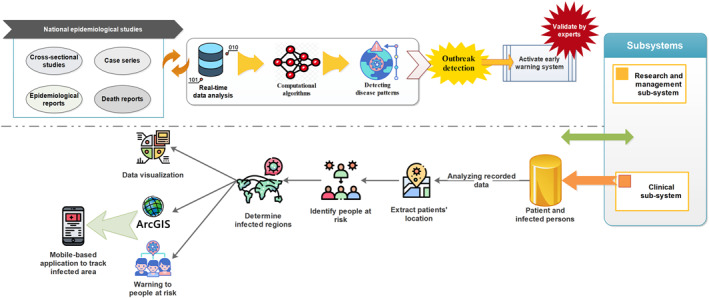
The epidemiological subsystem model
The first part of this model is an intelligent subsystem that investigates and interprets all recorded data in cross‐sectional studies, death reports and case reports continuously to detect an abnormal pattern of a particular disease using built‐in AI‐based algorithms. In case of occurrence of an abnormal pattern, the system would be placed in alert mode. Later, the subsystem of outbreak prediction will activate. Once epidemiologists confirm the outbreak, a survival system begins to run. Then the subsystems concerning clinical care and outbreak management will start to operate. The results of the epidemiological subsystem can also be used by clinical researchers for further studies. By integrating this subsystem with geographic systems, a model can be designed to visualize how the disease is transmitted, identifying infected areas and finding people at risk. Through analysing the obtained data and connecting the results to mobile applications, it is also possible to inform people who live in high‐risk areas.
3.3.2. Research and management subsystem
During the disease outbreak, one of the challenges was considered by most articles is how to allocate health and human resources during the epidemic. Therefore, it is necessary to consider a subsystem to manage the proper allocation of resources to the health system. Reviewing literature showed that after a new disease outbreak, resource allocations could be handled by defining appropriate heuristic algorithms and analysing real‐time data. The schematic model of the suggested subsystem is represented in Figure 4.
FIGURE 4.
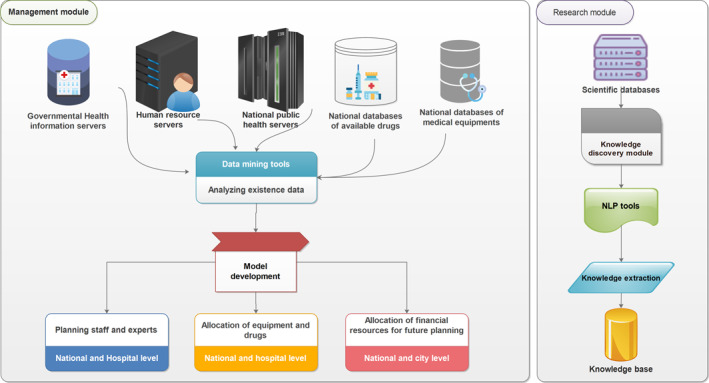
The research and management subsystem model; NLP, natural language process
Fair and efficient resource allocation is one of the biggest challenges for health care managers in the recent epidemic, COVID‐19. Even one of the most notable problems in developed countries was allocating well‐equipped health resources such as beds and staff to the areas that need them most as soon as possible. Therefore, in an epidemic, efficient resource allocation could be provided by applying machine learning algorithms. Such algorithms provide a health system. Such algorithms enable health systems to make the best decisions about allocating the most appropriate facilities by using real‐time data analysis and learning from past experiences in low‐ and middle‐income countries. The developed model in Figure 4 refers to the smart allocation model which will be created based on machine learning methods.
Given the importance of understanding the latest scientific evidence and the pattern of disease outbreak, a separate section is set up to extract the necessary knowledge under the management system for the automated extraction of information from published literature. Biomedical text extraction or the use of natural language process techniques can be used in this section to find the latest published literature and achievements through biomedical databases. Researchers and physicians can use this tool to enjoy the benefits of easier access to the latest scientific evidence and automating data abstraction in a short time. Extracted and classified knowledge can also be used to enhance the quality of outbreak control or as a source of knowledge in other subsystems.
3.3.3. Clinical care subsystem
In an epidemic event, patient treatment and follow‐up are the most significant issue to decrease the mortality rate. Hence, the clinical care subsystem is explained in the following based on the most useful strategies applied in reviewed articles. In a thematic analysis of the most influential ideas, clinical care planning was one of the most repetitive concepts extracted in the qualitative analysis stage of this research.
The most common solutions that appeared in the analysis regarding this section include (1) implementing electronic health records for patient management, (2) using decision support systems and computerized physician order entry tool to make better decisions and prevent medical errors, and (3) model generation. Moreover, telemedicine can be utilized in clinical care planning. Due to the importance of the clinical system and its complexities, this system is better designed in two subsystems of monitoring outpatients and inpatients.
3.3.4. Outpatient care subsystem
The proposed system can be designed in such a way that the rapid alert system is activated when the disease is detected. By activating the alert status, this system will automatically give the necessary alerts to medical centres. Additionally, the latest treatment protocols will be provided to specialists in the form of embedded knowledge in such a framework.
As it is apparent in Figure 5, an appropriate strategy can be employed in this section to identify people at risk using knowledge obtained from evidence, and regular monitoring of epidemiological data. The early screening module is one of the main parts of the proposed framework.
FIGURE 5.
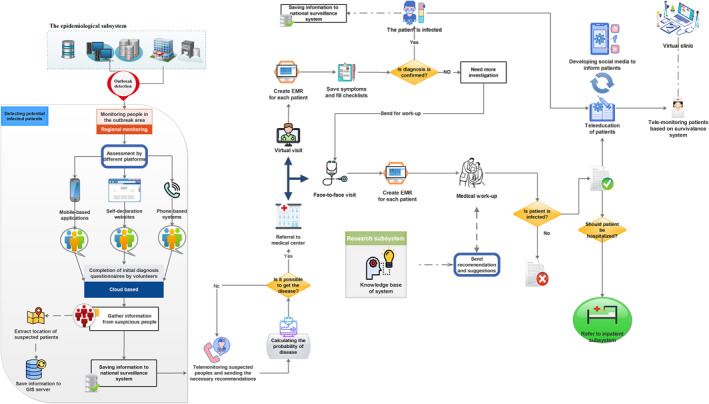
The outpatient subsystem model
As soon as the imminent alert system is activated, the infected geographical areas could be recognized. The necessary warning messages can then be sent to residents of high‐risk areas to prevent further outbreaks. Early screening of patients could be conducted in infected areas by applying different methods such as developing self‐assessment websites and mobile‐based applications, and telephone‐based counselling. Accordingly, all of the people who were at the risk of exposure can be determined. Taking such an approach can also be effective in reducing the prevalence of COVID‐19 in low‐ and middle‐income countries.
If the person is suspected of having the disease, he/she will be assessed based on standard checklists by health care providers. Then, the risk of disease in each person will be calculated. If the risk of disease is high, the patient will be monitored remotely through regular telephone consultation. For more investigation, the patient will be referred to medical centres if he needs it. Then, a medical record will be created for him. If he needs to be hospitalized, his information will be referred to the hospital subsystem. In a viral illness, the patient must be quarantined. To better communicate, secure social networks can be designed for patients to discuss their problems and share their experiences. These social networks should be managed under the supervision of health professionals to prevent the spread of untruths.
Developing telemedicine programs is crucial to monitor non hospitalized patients in severe communicable diseases like COVID‐19. So, monitoring patients through telemonitoring programs and virtual clinics could reduce disease transmission. It can be helpful in better controlling the spread of diseases such as COVID‐19.
Self‐monitoring of people who have some symptoms is possible by employing such a system. Through telemonitoring, if the patient has the initial symptoms of the disease, it can first be followed remotely. After an initial investigation, the system referred the patient to medical centres if it is required. According to other studies, tele‐education can be used to better educate patients for the prevention and control of the disease using social networks and distance education.
3.3.5. Inpatient care subsystem
In the proposed model, once the patient's referred, the information is automatically entered into the system to create a file for the patient. During patient monitoring, control, and follow‐up, all recorded information is continuously analysed to extract the disease pattern. At the same time, due to the connection of the system to the knowledge base, patients are followed according to the treatment protocols based on standard treatment steps. Physicians are also asked to enter their new findings concerning the disease in the relevant section. These new achievements could be added to the knowledge‐base after expert approval. The details of the suggested strategy are shown in Figure 6.
FIGURE 6.
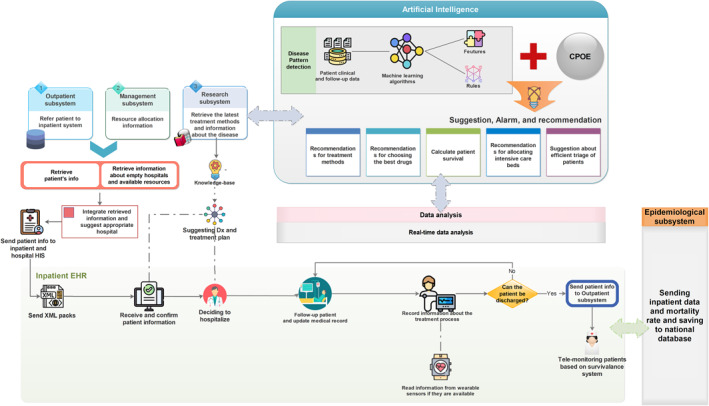
The inpatient subsystem model
At the time of hospitalization, the knowledge regarding the disease symptoms and its characteristics are extracted for better management and disease control using machine learning algorithms and real‐time data analysis. The knowledge can be used for appropriate resource allocations in critically ill patients, prescribing the most effective drugs and prioritizing patients.
4. DISCUSSION
Through this survey, the published articles regarding medical informatics application for preparedness against disease outbreak were investigated to extract topics of interest. The evidence showed that more developed countries such as the United States have more tendency to apply medical informatics strategies to fight epidemics more efficiently. Through this survey, the highest frequency of epidemics related to the influenza outbreak. However, this result was expected due to the worldwide outbreak of influenza.
Based on the experiences of countries in similar diseases epidemic, it is possible to control the spread of the virus more effectively with the appropriate use of modern technologies. 24 , 25 Hence, valuable experiences and applied strategies were explored through thematic analysis. According to the extracted main themes, we devised an appropriate conceptual framework for better prevalence control. After identifying the main themes, solutions concerning medical informatics were specified in each section. A suggested model according to these strategies was represented in terms of sub‐systems. The proposed model can be summarized in the form of an ultimate model represented in Figure 7. This notation ties well with previous studies wherein effective preparedness should include prevention, control and management planning. 26 , 27 , 28 , 29
FIGURE 7.
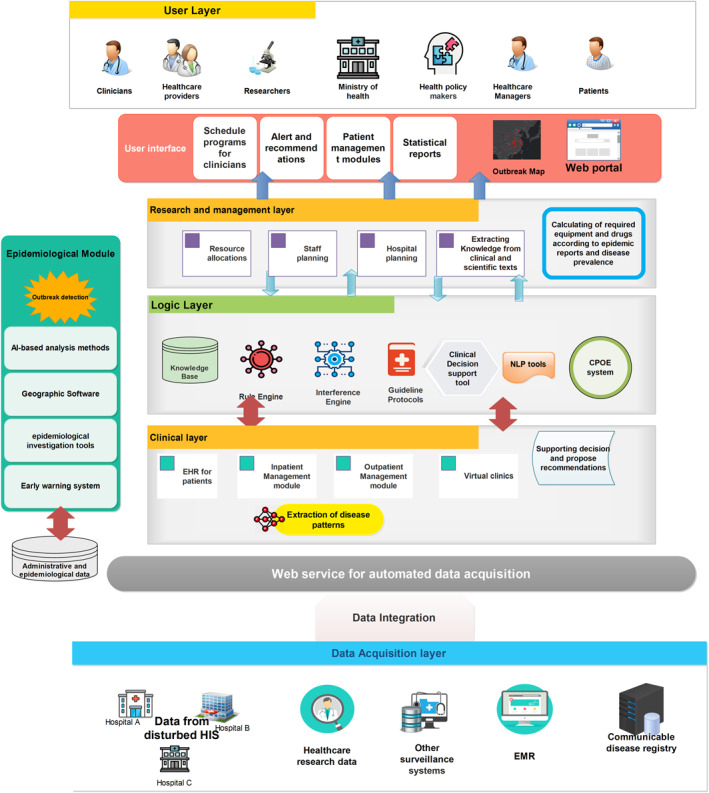
Overall conceptual model
From the medical informatics view, AI‐based strategies are the most common technique applied in studies. By applying AI methods, researchers developed intelligent systems such as early warning applications, prediction models, epidemiological systems and intelligent surveillance systems to help healthcare organizations to fight outbreaks easier. Most of these systems were related to disease management after the emergence of the outbreak. Thus, developing an integrated intelligent system could fight disease outbreak at organizational and clinical levels can be accounted for a research gap. Such a system should be fighting against pandemic before and after a disease outbreak.
The proposed framework is a type of intelligent clinical surveillance system for real‐time monitoring of infectious and epidemic diseases such as COVID‐19, which is equipped with patient monitoring systems, prevention and analytical tools for further research and study. Because this model is customized for contagious disease monitoring, we tried to define the proposed system in such a way it can prevent, control, and follow patients at the national level. Similarly, Oppenheim et al. 30 declared that an outbreak preparedness plan involves early detection, disease management and control, surveillance, case findings, patient treatment and management. The final system should be designed in such a way to benefit all of the patients and health care providers in clinical fields. Based on the main categories identified through thematic analysis, as a result of analysing the main concepts presented in the studies, solutions appropriate to each section have been proposed in each part. As shown in Figure 7, the proposed model is a four‐layer model. These layers comprise the user interface layer, the logic layer, the application layer and the data layer. Despite each layer of the layered architecture pattern has a specific role and responsibility, all layers have interacted with each other to pass the information up to the presentation layer. Layered architecture pattern is the most common architecture pattern for developing web‐based applications in healthcare settings. 31
Analysis of related articles showed that the most common strategy applied by researchers was designing early warning systems. In line with previous studies, it is apparent that the first step of ‘preparation’ is the continuous investigation and prevention of further outbreaks. 27 Accordingly, the popularity of mathematical models to forecast epidemic diseases has been increased to better help policy‐makers in decision‐making with the development of AI‐based methods in other studies. 32 Consequently, outbreak investigation and prediction are considered as a prerequisite of preparedness to activate other subsystems in the form of an early detection system in the epidemiological section.
In an epidemic, physicians should be aware of the best available evidence as soon as possible. Meanwhile, the work of the medical staff increases during the outbreak of the disease. Therefore, limited time is a common challenge in critical situations. As in the Coronavirus pandemic, the workload of healthcare providers has increased, and health care providers have to work in heavy workload conditions. 33 , 34 To address this challenge, an AI‐based technique such as text mining in the research and management section was considered to retrieve the required evidence as soon as possible. Recently, some studies were conducted to extract valuable knowledge from published literature and summarizing the most up‐to‐date research using natural language processing. 35 This solution can enable clinicians to access information from a huge amount of scientific evidence published recently. 36
Allocation of the appropriate resources and well‐coordinated care during the time of the outbreak is one of the main themes and strategies extracted through our analysis. It accounted for another challenge that we usually face in an outbreak. 37 Thus, an intelligent procedure was considered in our proposed model using data mining mechanisms to solve this problem.
Case findings and accurate diagnosis are crucial in controlling the outbreak of an epidemic. 38 Hence, a systematic process in patient management and clinical care planning is embedded to find infected people in the proposed model. The next important issue is related to the continuous care of infected patients. Thus, establishing a standard of care for triage and treatment could be remarkably efficient during a disease outbreak in disease control and enhance patient safety. 39 Patient management is also considered in two parts for an effective clinical care program. It comprises outpatient and inpatient modules using solutions such as applying decision support systems, implementing electronic health records, remote monitoring and utilizing data mining tools in the presented model.
The proposed model tries to provide a framework to prepare for a sudden outbreak of disease by considering usable medical informatics methods. This model could provide deeper insights into the designing of a surveillance system for public health professionals from a medical informatics perspective. Such a framework can be optimized to be applied in different situations. Moreover, this study is the first stage of further research to validate the framework through focus group discussions, Delphi survey, or expert consensus. Once the model is validated, it can be considered as a reference framework in developing surveillance systems to prepare for the next epidemic.
There are several limitations to this research. The proposed framework was designed from the author's point of view. However, this is only a proposed model for further studies and a new perspective on the control of communicable diseases regarding medical informatics solutions. Also, this is a non‐validated model, and its validation will be examined in future studies.
ETHICS STATEMENT
The study involves only a review of literature without involving humans and/or animals. The authors have no ethical conflicts to disclose.
CONFLICT OF INTERESTS
The author(s) declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
AUTHORS CONTRIBUTION
Reza Safdari: Conception and design of study, Acquisition of data, Analysis and/or interpretation of data, Revising the manuscript critically for important intellectual content. Hamidreza Abtahi: Conception and design of study, Acquisition of data, Draughting the manuscript. Marsa Gholamzadeh: Conception and design of study, Acquisition of data, Analysis and/or interpretation of data, Draughting the manuscript, Revising the manuscript critically for important intellectual content. Approval of the version of the manuscript to be published
Supporting information
Supplementary Material
Supplementary Material
ACKNOWLEGMENT
Not relevant. No funding to declare.
DATA AVAILABILITY STATEMENT
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.
REFERENCES
- 1. Fineberg HV. Pandemic preparedness and response—lessons from the H1N1 influenza of 2009. N. Engl J Med. 2014;370(14):1335‐1342. [DOI] [PubMed] [Google Scholar]
- 2. Kelly H. The classical definition of a pandemic is not elusive. Bull World Health Organ. 2011;89:540‐541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Din A, Khan A, Baleanu D. Stationary distribution and extinction of stochastic coronavirus (COVID‐19) epidemic model. Chaos, Solitons and Fractals. 2020;139(October 2020):110036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Cohn SK. Pandemics: waves of disease, waves of hate from the Plague of Athens to A.I.D.S. Hist J. 2012;85(230):535‐555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Chen Y, Cook AR, Lim AXL. Randomness of dengue outbreaks on the equator. Emerg Infect Dis. 2015;21(9):1651‐1653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Nikolich‐Zugich J, Knox KS, Rios CT, Natt B, Bhattacharya D, Fain MJ. SARS‐CoV‐2 and COVID‐19 in older adults: what we may expect regarding pathogenesis, immune responses, and outcomes. Geroscience. 2020;42(2):1‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Contreras GW, MEP M. Getting ready for the next pandemic COVID‐19: why we need to be more prepared and less scared. Int J Emerg Manag. 2020;18(2):87‐89. [DOI] [PubMed] [Google Scholar]
- 8. Binagwaho A. We need compassionate leadership management based on evidence to defeat COVID‐19. Int J Health Policy Manag. 2020;9(10):413‐414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Vokinger KN, Nittas V, Witt CM, Fabrikant SI, von Wyl von Wyl. Digital health and the COVID‐19 epidemic: an assessment framework for apps from an epidemiological and legal perspective. Swiss Med Wkly. 2020;150:w20282. 10.4414/smw.2020.20282 [DOI] [PubMed] [Google Scholar]
- 10. Nuño M, Reichert TA, Chowell G, Gumel AB. Protecting residential care facilities from pandemic influenza. Proc Natl Acad Sci USA. 2008;105(30):10625–10630. 10.1073/pnas.0712014105 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Schwartz RD, Bayles BR. US university response to H1N1: a study of access to online preparedness and response information. Am J Infect Contr. 2012;40(2):170‐174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Stein ML, Rudge JW, Coker R, et al. Development of a resource modelling tool to support decision makers in pandemic influenza preparedness: The AsiaFluCap Simulator. BMC Publ Health. 2012;12(1). 10.1186/1471-2458-12-870 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Ali MA, Ahsan Z, Amin M, Latif S, Ayyaz A, Ayyaz MN. A visual analytics architecture for infectious diseases surveillance and response management in Pakistan. Publ Health. 2016;134:72–85. 10.1016/j.puhe.2016.01.006 [DOI] [PubMed] [Google Scholar]
- 14. Beard R, Wentz E, Scotch M. A systematic review of spatial decision support systems in public health informatics supporting the identification of high risk areas for zoonotic disease outbreaks. Int J Health Geogr. 2018;17(1):38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Tsai C‐T, Sung F‐C, Chen PS, Lin S‐C. Exploring the spatial and temporal relationships between mosquito population dynamics and dengue outbreaks based on climatic factors. Stoch Environ Res Risk Assess. 2012;26(5):671‐680. [Google Scholar]
- 16. Zhang H, Wang L, Lai S, Li Z, Sun Q, Zhang P. Surveillance and early warning systems of infectious disease in China: from 2012 to 2014. Int J Health Plan Manag. 2017;32(3):329‐338. [DOI] [PubMed] [Google Scholar]
- 17. Jiancheng Ye. The Role of Health Technology and Informatics in a Global Public Health Emergency: Practices and Implications From the COVID‐19 Pandemic. JMIR Medical Informatics. 2020;8(7):e19866. 10.2196/19866 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Qing Ye, Zhou J, Hong Wu. Using Information Technology to Manage the COVID‐19 Pandemic: Development of a Technical Framework Based on Practical Experience in China. JMIR Med Inform. 2020;8(6):e19515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Hussain AA, Bouachir O, Al‐Turjman F, Aloqaily M. AI Techniques for COVID‐19. IEEE Access. 2020;8:128776–128795. 10.1109/access.2020.3007939 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Peditto K. Reporting qualitative research: standards, challenges, and implications for health design. HERD: Health Environments Research & Design Journal. 2018;11(2):16–19. 10.1177/1937586718772615 [DOI] [PubMed] [Google Scholar]
- 21. Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis: striving to meet the trustworthiness criteria. Int J Qual Methods. 2017;16(1):1609406917733847. 10.1177/1609406917733847 [DOI] [Google Scholar]
- 22. Soratto J, Pires DEPd, Friese S. Thematic content analysis using ATLAS. ti software: potentialities for researches in health. Rev Bras Enferm. 2020;73(3). 10.1590/0034-7167-2019-0250 [DOI] [PubMed] [Google Scholar]
- 23. Zhang X, Lin H, Wang J, et al. Scientific and technological strategies proposal for the construction of digital public health emergency management system in China. Wuhan Daxue Xuebao (Xinxi Kexue Ban)/Geomatics Inf Sci Wuhan Univ. 2020;45(5):633‐639. 10.13203/j.whugis20200151 [DOI] [Google Scholar]
- 24. Christaki E. New technologies in predicting, preventing and controlling emerging infectious diseases. Virulence. 2015;6(6):558–565. 10.1080/21505594.2015.1040975 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Kummitha RKR. Smart technologies for fighting pandemics: the techno‐ and human‐ driven approaches in controlling the virus transmission. Gov Inf Q. 2020;37(2):1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Akselrod H, Mercon M, Kirkeby Risoe P, Schlegelmilch J, McGovern J, Bogucki S. Creating a process for incorporating epidemiological modelling into outbreak management decisions. J Bus continuity Emerg Plan. 2012;6(1):68‐83. [PubMed] [Google Scholar]
- 27. Ameli J. Communicable Diseases and Outbreak Control. Turk J Emerg Med. 2016;9(15):20‐26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Fast SM, González MC, Wilson JM, Markuzon N. Modelling the propagation of social response during a disease outbreak. J R Soc Interface. 2015;12(104):1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Tiwari S, Kumar S, Guleria K. Outbreak Trends of Coronavirus Disease–2019 in India: a Prediction. Disaster Med Public Health Prep. 2020;14(5):e33–e38. 10.1017/dmp.2020.115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Oppenheim B, Gallivan M, Madhav NK, et al. Assessing global preparedness for the next pandemic: development and application of an Epidemic Preparedness Index. BMJ Glob Health. 2019;4(1):e001157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Westfechtel B, Munch BP, Conradi R. A layered architecture for uniform version management. IEEE Transactions on Software Engineering. 2001;27(12):1111–1133. 10.1109/32.988710 [DOI] [Google Scholar]
- 32. Murray AG, Raynard RS. Modelling for disease preparedness and response. Dev Biol (Basel). 2007;129:41–51. [PubMed] [Google Scholar]
- 33. Shah K, Chaudhari G, Kamrai D, Lail A, Patel RS. How essential is to focus on physician's health and burnout in coronavirus (COVID‐19) pandemic? Cureus. 2020;12(4):e7538‐e7538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Unadkat S, Farquhar M. Doctors’ wellbeing: self‐care during the covid‐19 pandemic. BMJ. 2020;368:m1150. [DOI] [PubMed] [Google Scholar]
- 35. Nasar Z, Jaffry SW, Malik MK. Information extraction from scientific articles: a survey. Scientometrics. 2018;117(3):1931‐1990. [Google Scholar]
- 36. Kilicoglu H. Biomedical text mining for research rigor and integrity: tasks, challenges, directions. Briefings Bioinforma. 2017;19(6):1400‐1414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Belfroid E, Timen A, van Steenbergen JE, Huis A, Hulscher MEJL. Which recommendations are considered essential for outbreak preparedness by first responders? BMC Infect Dis. 2017;17(1):195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Kelly‐Cirino CD, Nkengasong J, Kettler H, et al. Importance of diagnostics in epidemic and pandemic preparedness. BMJ Glob Health. 2019;4(Suppl 2):e001179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Lee MH, Lee GA, Lee SH, Park Y‐H. A systematic review on the causes of the transmission and control measures of outbreaks in long‐term care facilities: back to basics of infection control. PloS One. 2020;15(3):e0229911‐e0229911. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Material
Supplementary Material
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.