

While it is clear that children are less susceptible to SARS‐CoV‐2 than adults, 1 their role in spreading the virus is less certain. 1 , 2 This is a relevant topic, since controversies about school opening/closure are still current. 3
After an adolescent presented with COVID‐19 to our institution, we assessed the number of new infections in classmates to evaluate if virus spread had occurred. Written informed consent was provided by the parent or legal guardian. This study is part of a larger paediatric COVID‐19 study approved by the Ethics Committee of our Institution (ID 3078).
Scenario
On 24 September 2020, a 16‐year‐old high‐school student presented to the paediatric emergency department of our institution with pyrexia, headache, anosmia and ageusia, and a nasopharyngeal swab tested positive to SARS‐CoV‐2 by polymerase chain reaction. One week before, two class‐mates presented with ‘flu‐like’ symptoms and had microbiologically confirmed SARS‐CoV‐2 infection.
Epidemiological assessment of the classmates, conducted between 17 and 28 September, showed the following:
The 26 adolescents constituting the usual class during previous years were not divided in subgroups due to logistic problems and the recommended 1‐m distance between each desk was not established due to insufficient space. Windows were kept open during the lessons, but there was no other ventilation system. Students had to wear a surgical mask full‐time while in class. Hand sanitizers were not available within the class. During break and lunchtime, adolescents were requested to have lunch at the own desks in order to reduce the risk of contagion.
Figure 1 shows the results of microbiological assessment by polymerase chain reaction. Nine children (34.6%) had proven infection, with a pattern suggesting a small ‘spatial cluster’. Interestingly, the first row of students was apparently spared. Three of the nine infected adolescents developed no symptoms.
None of the infected adolescents required hospital admission. Of the six symptomatic, all had fever, four (66.6%) had headache and cough, and two had severe asthenia.
Fig 1.
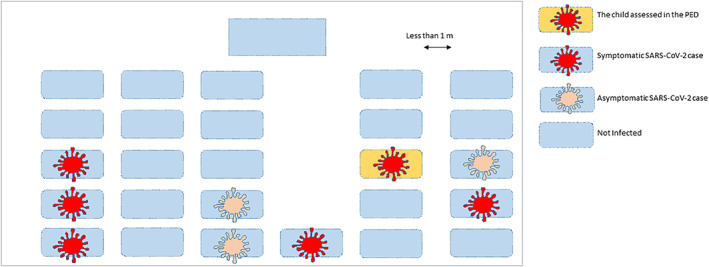
Epidemiological assessment of SARS‐CoV‐2 spread within a high‐school class. The child assessed in the paediatric emergency department; symptomatic SARS‐CoV‐2 case; asymptomatic SARS‐CoV‐2 case; not infected.
Discussion
A recent systematic review and meta‐analysis showed children younger than 14 years old were about half as susceptible to SARS‐CoV‐2 infection as adults, while adolescents appear to have similar susceptibility to adults. 1 However, school closures are controversial. An Australian study showed low transmission within schools on a background of low community transmission, suggesting that clusters in schools might be due to community transmission as much as to transmission within the school. 4 This observation, according to preliminary reports, seems to be true for European schools as well. 3 , 5 In particular, cases of SARS‐CoV‐2 within schools seem to be rare in children younger than 10 years of age. 3 , 4 , 5 However, the same may not be true for older children. Our description shows susceptibility of adolescents to SARS‐CoV‐2 but, more importantly, suggests they can spread the infection if adequate preventive measures are not established. Observing this class, clusters of affected students are possibly related to the lack of proper distancing between students, highlighting the need to establish strict rules that include measures (masking, hand hygiene and distance) to prevent school outbreaks, particularly in adolescents, and avoid unnecessary psychological/mental consequences on child health.
A limitation of our report is the lack of epidemiological assessment of the whole school, including other classes and teachers, nor of the household members of each adolescent, since the aim of this pilot investigation was to assess the spread of the virus within a single class. Active surveillance of similar scenarios, possibly with open access data repositories, is needed, particularly in younger children, who may exhibit different transmission patterns.
Consent for publication was obtained from the parents of the index case.
References
- 1. Viner RM, Mytton OT, Bonell C et al. Susceptibility to SARS‐CoV‐2 infection among children and adolescents compared with adults: A systematic review and meta‐analysis. JAMA Pediatr. 2020: e204573 10.1001/jamapediatrics.2020.4573. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Isaacs D, Britton P, Howard‐Jones A et al. To what extent do children transmit SARS‐CoV‐2 virus? J. Paediatr. Child Health 2020; 56: 978–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Isphording IE, Lipfert M, Pestel N. School Re‐Openings after Summer Breaks in Germany Did Not Increase SARS‐CoV‐2 Cases. 2020. IZA Discussion Paper, IZA DP No. 13790. Available from: http://ftp.iza.org/dp13790.pdf [accessed 29 December 2020].
- 4. Macartney K, Quinn HE, Pillsbury AJ et al. Transmission of SARS‐CoV‐2 in Australian educational settings: A prospective cohort study. Lancet Child Adolesc. Health 2020; 4: 807–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Buonsenso D, De Rose C, Moroni R, Valentini P. SARS‐CoV‐2 infections in Italian schools: Preliminary findings after one month of school opening during the second wave of the pandemic. medRxiv 2020. 10.1101/2020.10.10.20210328. [DOI] [PMC free article] [PubMed] [Google Scholar]