

Abstract
Background
Long‐term effects after COVID‐19 may affect surgical safety. This study aimed to evaluate the literature and produce evidence‐based guidance regarding the period of delay necessary for adequate recovery of patients following COVID‐19 infection before undergoing surgery.
Methods
A rapid review was combined with advice from a working group of 10 clinical experts across Australia and New Zealand. MEDLINE, medRxiv and grey literature were searched to 4 October 2020. The level of evidence was stratified according to the National Health and Medical Research Council evidence hierarchy.
Results
A total of 1020 records were identified, from which 20 studies (12 peer‐reviewed) were included. None were randomized trials. The studies comprised one case–control study (level III‐2 evidence), one prospective cohort study (level III‐2) and 18 case‐series studies (level IV). Follow‐up periods containing observable clinical characteristics ranged from 3 to 16 weeks. New or excessive fatigue and breathlessness were the most frequently reported symptoms. SARS‐CoV‐2 may impact the immune system for multiple months after laboratory confirmation of infection. For patients with past COVID‐19 undergoing elective curative surgery for cancer, risks of pulmonary complications and mortality may be lowest at 4 weeks or later after a positive swab.
Conclusion
After laboratory confirmation of SARS‐CoV‐2 infection, minor surgery should be delayed for at least 4 weeks and major surgery for 8–12 weeks, if patient outcome is not compromised. Comprehensive preoperative and ongoing assessment must be carried out to ensure optimal clinical decision‐making.
Keywords: COVID‐19, inflammation, long‐term, SARS‐CoV‐2, surgery, symptom
A rapid review was combined with advice from a working group of 10 clinical experts across Australia and New Zealand to produce evidence‐based guidance regarding the period of delay necessary for adequate recovery of patients following COVID‐19 infection before undergoing surgery. We found that follow‐up periods containing observable clinical characteristics ranged from 3 to 16 weeks and SARS‐CoV‐2 may impact the immune system for multiple months after laboratory confirmation of infection. Therefore, after laboratory confirmation of SARS‐CoV‐2 infection, minor surgery should be delayed for at least 4 weeks and major surgery for 8–12 weeks, if patient outcome is not compromised; additionally comprehensive preoperative and ongoing assessment must be carried out to ensure optimal clinical decision‐making.
Introduction
Perioperative management has had to adapt to coronavirus disease 2019 (COVID‐19). Triage during the pandemic has required consideration of local COVID‐19 prevalence and hospital resources alongside surgical presentation. 1 Prior COVID‐19 carries considerable surgical risk during the preoperative assessment. 2 High mortality and pulmonary complications associated with perioperative severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) infection 3 have modified both preoperative risk–benefit assessment and postoperative care. Appropriate screening and testing for SARS‐CoV‐2 have become crucial. 4 Ongoing risks of nosocomial spread to both surgical staff and patients have disrupted surgical systems on a global scale. 5
Clinical characteristics associated with laboratory‐confirmed COVID‐19 have mostly been documented in an acute setting. 6 However, long‐term persistence of symptoms has also been reported, 7 , 8 leading to prolongation of the potential timeline of the associated spectrum of disease. 9 , 10 , 11 Cases of clinical recurrence after complete recovery have been described. 12 While the pathophysiology of acute SARS‐CoV‐2 infection is known to include significant inflammation and dysfunctional immune responses, 13 longer‐lasting effects are poorly understood. 14
The potential for long‐term effects after SARS‐CoV‐2 infection has ramifications for perioperative management. Undertaking surgery without allowing adequate time for recovery from COVID‐19, risks compromising patient safety. The necessary recovery period before safely undertaking surgery must be understood to optimize surgical decision‐making. This study aimed to evaluate the literature and produce evidence‐based guidance regarding the period of delay necessary for adequate recovery of patients with COVID‐19 before undertaking surgery.
Methods
In a similar fashion to previous publications, 1 , 4 , 15 , 16 a rapid review of the literature was combined with advice from a working group of clinical experts across Australia and New Zealand. 17 , 18 The working group comprised seven senior surgeons (one urologist and six general surgeons), two senior anaesthetists and a senior medical virologist.
Research questions and inclusion criteria were established a priori (Table 1) 20 and searches for studies of any design in any setting were applied using rapid review methodology. 21 Searches were conducted in MEDLINE and medRxiv databases to identify articles in English published from 31 December 2019 (identification of SARS‐CoV‐2) 22 to 4 October 2020 (Appendix I). No publication restrictions were applied. Grey literature was also searched according to the Grey Matters checklist, 23 including content from international health networks, guideline repositories, surgical and anaesthesia societies, the USA Food and Drug Administration website, and the COVID‐19 Evidence Accelerator. 24 Additional articles were identified by screening the reference lists of any full‐text articles retrieved.
Table 1.
Inclusion criteria for research questions
| Research question 1 | Research question 2 | |
|---|---|---|
| What are the long‐term pathophysiological and functional sequelae of COVID‐19 in patients who have recovered from the acute illness? | What is the impact of prior exposure to COVID‐19 on postoperative surgical outcomes in patients who have recovered from the acute illness? | |
| Population |
|
|
| Intervention | Any elective or emergency operation | |
| Comparator | Not applicable | Patients undergoing surgery who have not been infected with SARS‐CoV‐2 |
| Outcomes |
|
|
| Study type | Studies of any design | |
| Exclusions |
|
|
One reviewer (NAS) screened titles and abstracts and reviewed full texts of relevant articles to extract data into a standard extraction form. Data extracted included study design, setting, population characteristics, clinical observations relating to COVID‐19, and duration of effects after acute SARS‐CoV‐2 infection. Data were synthesized in tabular and narrative formats. Where possible, data were coded according to surgical urgency and complexity. Level of evidence provided by the included studies was stratified according to the National Health and Medical Research Council evidence hierarchy. 25
Results
Study characteristics
A total of 1020 records were identified, from which 94 full‐text articles were retrieved. After applying the specified research criteria, 20 studies were included in the rapid review. Of the 20 studies, 12 contained peer‐reviewed data and eight were non‐refereed publications or conference abstracts. All but one of the studies investigated the long‐term clinical characteristics associated with COVID‐19. One study directly explored the effect of past SARS‐CoV‐2 infection on the postoperative outcomes of recovered patients. Regarding study design and level of evidence, 25 the studies comprised one case–control study (level III‐2 evidence), one prospective cohort study (level III‐2 evidence) and 18 case‐series studies (level IV evidence). No randomized trials were identified that addressed the research questions. Characteristics of the included studies are outlined in Table 2.
Table 2.
Characteristics of included studies
| Study | Country | Peer‐reviewed or non‐refereed | Study design | Level of evidence† | Research question | Study population | Sample size | Age of study population (years) | Sex of study population (% men) | Length of follow‐up |
|---|---|---|---|---|---|---|---|---|---|---|
| Carfi et al. 7 | Italy | Peer‐reviewed | Retrospective case series; consecutive recruitment; single centre | IV | 1 | Adults hospitalized with COVID‐19: mean LOS 14 (SD 9.7) days | n = 143 | Mean: 57 (SD 14.6; range 19–84) | 63% | Mean 60 (SD 13.6) days after symptom onset |
| Chiesa‐Estomba et al. 26 | Europe | Peer‐reviewed | Prospective case series; consecutive recruitment; multicentre | IV | 1 | Adults (age > 18 years) hospitalized (% not stated) or outpatient‐managed with mild COVID‐19 who had gustatory dysfunction | n = 701 | Mean: 40 (SD 13.0) | 33% | Mean 63 (SD 9.0) days (range 60–76) after symptom onset |
| Ding et al. 27 | China | Peer‐reviewed | Retrospective case series; non‐consecutive recruitment; multicentre | IV | 1 | Patients hospitalized with COVID‐19 pneumonia | n = 53 | Mean: 56 (range 12–89) | 46% | >28 days after symptom onset |
| Garrigues et al. 28 | France | Peer‐reviewed | Retrospective case series; non‐consecutive recruitment; single centre | IV | 1 |
Patients hospitalized (20% in ICU) with COVID‐19; mean LOS 11 (SD 13.4) days |
n = 120 | Mean: 63 (SD 15.7) | 63% | Mean 111 (SD 11.1) days after hospital admission |
| Halpin et al. 29 | UK | Peer‐reviewed | Retrospective case series; non‐consecutive recruitment; multicentre | IV | 1 | Adults (age ≥ 18 years) hospitalized (32% in ICU) with COVID‐19; median LOS 6.5 days for non‐ICU and 12 for ICU patients | n = 100 | Range: 20–93 | 54% | Mean 48 (SD 10.3) days (range 29–71) after hospital discharge |
| Huang et al. 30 | China | Peer‐reviewed | Retrospective case series; non‐consecutive recruitment; single centre | IV | 1 | Adults hospitalized with COVID‐19 who had cardiac symptoms; median LOS not reported | n = 26 | Mean: 38 (range 32–45) | 38% | Median 47 (IQR 36–58) days after onset of cardiac symptoms |
| Li et al. 31 | China | Peer‐reviewed | Prospective case series; recruitment type unclear; multicentre | IV | 1 | Patients with COVID‐19 | n = 145 | Mean: 49 (range 13–80) | 39% | Median 62 days (range 25–95) after symptom onset |
| Liu et al. 32 | China, Germany | Non‐refereed | Prospective concurrent case–control study; recruitment type unclear; multicentre | III‐2 | 1 | Adults hospitalized (43%) or outpatient‐managed with mild (17%) or moderate COVID‐19 | n = 30; age‐ and sex‐matched unexposed cohort: 21 | Mean: 37 | 11% | Median 112 days (range 60–136) after first diagnosis |
| Otte et al. 33 | Germany | Peer‐reviewed | Prospective case series; consecutive recruitment; single centre | IV | 1 | Adults (age ≥ 18 years) outpatient‐managed with COVID‐19 | n = 91 | Mean: 43 (SD 12.7) | 51% | Mean 58 (SD 1.4) days after symptom onset |
| Patelli et al. 34 | Italy | Peer‐reviewed | Retrospective case series; recruitment type unclear; single centre | IV | 1 | Patients hospitalized with COVID‐19 | n = 20 | Mean: 58 (SD 10.0; range 35–86) | Not reported | Mean 40 (SD 13) days after fever remission |
| Puntmann et al. 35 | Germany | Peer‐reviewed | Prospective case series; non‐consecutive recruitment; single centre | IV | 1 | Patients hospitalized (33%) or outpatient‐managed with COVID‐19 | n = 100 | Mean: 49 (SD 14.0) | 53% | Median 71 (IQR 64–92) days after diagnosis |
| Zhao et al. 36 | China | Peer‐reviewed | Retrospective case series; consecutive recruitment; multicentre | IV | 1 | Adults (age ≥ 18 years) hospitalized with COVID‐19: median LOS, 5 days (IQR 2–8) | n = 55 | Mean: 48 years (SD 15.5) | 58% | 64–93 days after hospital discharge |
| Arnold et al. 37 | UK | Non‐refereed | Prospective case series; consecutive recruitment; single centre | IV | 1 | Adults (age ≥ 18 years) hospitalized with COVID‐19: median LOS 5 days (IQR 2–8) | n = 110 | Median: 60 (IQR 46–73) | 56% | Median 83 (IQR 74–88) days after hospital admission; median 90 days (IQR 80–97) after symptom onset |
| Clark et al. 38 | USA | Non‐refereed | Retrospective case series; recruitment type unclear; single centre | IV | 1 | Adult (age > 18 years) collegiate athletes outpatient‐managed with mild or asymptomatic COVID‐19 | n = 22 | Mean: 20 | 41% | Median 52 days from infection |
| Klein et al. 39 | Israel | Non‐refereed | Retrospective case series; non‐consecutive recruitment; single centre | IV | 1 | Adults (age ≥ 18 years) hospitalized (5%) or outpatient‐managed with mild COVID‐19 | n = 112 | Mean: 35 (SD 12.0) | 64% | 6 weeks after two consecutive negative test results for COVID‐19 |
| O'Keefe and Cellai 40 | USA | Non‐refereed | Retrospective case series; non‐consecutive recruitment; single centre | IV | 1 | Adult outpatient‐managed with mild or asymptomatic COVID‐19 | n = 26 | Median: 47.5 (range 23–78) | 33% | Median 38 days (range 21–49) after symptom onset |
| Sahanic et al. 41 | Austria | Non‐refereed | Prospective case series; recruitment type unclear; multicentre | IV | 1 | Patients hospitalized with COVID‐19: mean LOS, 13 days | n = 86 | Mean: 61 | 65% | 6 and 12 weeks after discharge |
| Townsend et al. 42 | Ireland | Non‐refereed | Retrospective case series; consecutive recruitment; single centre | IV | 1 | Patients hospitalized (56%) or outpatient‐managed with COVID‐19 | n = 128 | Mean: 50 (SD 15.0) | 48% | Median 72 (IQR 62–87) days after hospital discharge or a 14‐day timepoint after diagnosis for outpatients |
| Weerahandi et al. 43 | USA | Non‐refereed | Retrospective case series; consecutive recruitment; multicentre | IV | 1 | Adults (age ≥ 18 years) hospitalized with severe COVID‐19: median LOS, 18 days (IQR 10–31) | n = 152 | Median: 62 (IQR 50–67) | 63% | Median 37 days (range 30–43) after hospital discharge |
| COVIDSurg Collaborative 44 | International | Peer‐reviewed | Prospective cohort study; non‐consecutive recruitment; multicentre | III‐2 | 2 | Patients undergoing curative elective cancer surgery with previous positive SARS‐CoV‐2 swab | n = 122; 1–2 weeks from previous positive swab: n = 27; 2–4 weeks from previous positive swab: n = 60; >4 weeks from previous positive swab: n = 35 | <2 weeks: 22% <50, 15% 50–59, 19% 60–69, 30% 70–79, 15% >80; 2–4 weeks: 15% <50, 22% 50–59, 32% 60–69, 25% 70–79, 7% >80; >4 weeks: 23% <50, 26% 50–59, 23% 60–69, 14% 70–79, 14% >80 | <2 weeks: 26%; 2–4 weeks: 37%; >4 weeks: 46% |
22·1% operated on within 2 weeks of diagnosis, 49·2% Between 2 and 4 weeks, and 28·7% after 4 weeks |
According to the National Health and Medical Research Council evidence hierarchy. 25
ICU, intensive care unit; IQR, interquartile range; LOS, length of stay; SD, standard deviation.
Long‐term clinical characteristics of COVID‐19
Studies reporting clinical characteristics persisting after acute SARS‐CoV‐2 infection comprised one case–control study 32 and 18 case‐series studies. 7 , 26 , 27 , 28 , 29 , 30 , 31 , 33 , 34 , 35 , 36 , 37 , 38 , 39 , 40 , 41 , 42 , 43 Median study sample size was 100 (range 20–701, interquartile range 41.5–124). All studies included adult patients, while two case‐series studies also included adolescents. 27 , 31 The case–control study evaluated a mixed population of patients who had required inpatient or outpatient management of COVID‐19. 32 Of the 18 case‐series studies, 10 reported solely on patients who had required hospitalization for COVID‐19. 7 , 27 , 28 , 29 , 30 , 34 , 36 , 37 , 41 , 43 The remainder reported on either mixed populations of patients who had required inpatient or outpatient management for past acute COVID‐19, 26 , 35 , 39 , 42 solely outpatients, 33 , 38 , 40 or did not report if hospital admission had been required. 31 Case‐series studies only of patients who had required hospitalization (Table 3), reported a wider range of clinical characteristics compared to those reported in studies of mixed patient populations (Table 4).
Table 3.
Long‐term clinical characteristics reported in case‐series studies on patients requiring hospitalization for COVID‐19
| Clinical characteristic | Reported proportion of study participants (n; length of follow‐up) |
|---|---|
| At least one ongoing symptom | 87% (n = 143; mean 60 days) 7 |
| Cough |
2% (n = 55; 64–93 days) 36 12% (n = 120; mean 111 days) 28 |
| Breathlessness |
15% (n = 55; 64–93 days) 36 40% (n = 20; mean 40 days) 34 42% (n = 120; mean 111 days) 28 43% (n = 143; mean 60 days) 7 50% (n = 100; mean 48 days) 29 |
| New or excessive fatigue |
16% (n = 55; 64–93 days) 36 43%† (n = 152; median 37 days) 43 53% (n = 143; mean 60 days) 7 55% (n = 120; mean 111 days) 28 64% (n = 100; mean 48 days) 29 |
| Memory disorder | 34% (n = 120; mean 111 days) 28 |
| Attention disorder | 27% (n = 120; mean 111 days) 28 |
| Sleep disorder | 31% (n = 120; mean 111 days) 28 |
| Anosmia |
13% (n = 120; mean 111 days) 28 15% (n = 143; mean 60 days) 7 |
| Ageusia or dysgeusia |
4% (n = 55; 64–93 days) 36 10% (n = 143; mean 60 days) 7 11% (n = 120; mean 111 days) 28 |
| Swallowing issue | 8% (n = 100; mean 48 days) 29 |
| Headache |
9% (n = 143; mean 60 days) 7 18% (n = 55; 64–93 days) 36 |
| Myalgia | 5% (n = 143; mean 60 days) 7 |
| Arthralgia | 27% (n = 143; mean 60 days) 7 |
| Gastrointestinal symptoms | 31% (n = 55; 64–93 days) 36 |
| Diarrhoea | 2% (n = 143; mean 60 days) 7 |
| New‐onset bowel or bladder incontinence | 13% (n = 100; mean 48 days) 29 |
| Chest pain |
11% (n = 120; mean 111 days) 28 22% (n = 143; mean 60 days) 7 42% (n = 26; median 47 days) 30 |
| Myocardial oedema and/or fibrosis (MRI) | 54% (n = 26; median 47 days) 30 |
| Left ventricular dysfunction |
4% (n = 26; median 47 days) 30 |
| Lung fibrosis (CT) | 40% (n = 20; mean 40 days) 34 |
| Abnormal lung function |
26% (n = 55; 64–93 days) 36 |
| Abnormal lung CT |
56% (n = 55; 64–93 days) 36 98% (n = 52; >28 days) 27 |
| Pneumothorax | 4% (n = 52; >28 days) 27 |
| Pleural effusion | 15% (n = 52; >28 days) 27 |
| Bronchiectasis | 45% (n = 52; >28 days) 27 |
| Reduced diffusion capacity | 22%† (n = 86; 12 weeks) 41 |
| Hyperinflation | 38%† (n = 82; 6 weeks) 41 |
| New ongoing need for home oxygen | 14%† (n = 152; median 37 days) 43 |
| Ongoing lymphopenia | 2%† (n = 110; median 83 days) 37 |
| C‐reactive protein >10 mg/L | 2%† (n = 110; median 83 days) 37 |
Non‐refereed data.
CT, computed tomography; MRI, magnetic resonance imaging.
Table 4.
Long‐term clinical characteristics in case‐series studies reporting on mixed patient populations requiring either inpatient or outpatient management for COVID‐19
| Clinical characteristic | Reported proportion of study participants (n; length of follow‐up) |
|---|---|
| Breathlessness |
36% (n = 100; median 71 days) 35 |
| Anosmia or hyposmia |
11% (n = 145; median 62 days) 31 45% (n = 80 symptomatic during acute phase) 33 |
| Ageusia or hypogeusia |
9% (n = 701 symptomatic during acute phase; 60–76 days) 26 |
| Hyposmia and/or hypogeusia | 39% (n = 84; mean 58 days) 33 |
| Chest pain |
17% (n = 100; median 71 days) 35 |
| Myocardial inflammation | 60% (n = 100; median 71 days) 35 |
| At least one ongoing symptom | 57%† (n = 128; median 72 days) 42 |
| Respiratory symptoms | 92%† (n = 26; median 38 days) 40 |
| Cough | 1%† (n = 112; 6 weeks) 39 |
| Low‐grade fever | 12%† (n = 26; median 38 days) 40 |
| New or excessive fatigue | |
| Memory disorder | 5%† (n = 112; 6 weeks) 39 |
| Attention disorder | 1%† (n = 112; 6 weeks) 39 |
| Headache | |
| Myalgia | 5%† (n = 112; 6 weeks) 39 |
| Palpitations | 23%† (n = 26; median 38 days) 40 |
| Gastrointestinal issues | 35%† (n = 26; median 38 days) 40 |
| Diarrhoea | 1%† (n = 112; 6 weeks) 39 |
| Abdominal pain | 1%† (n = 112; 6 weeks) 39 |
Non‐refereed data.
Within the case‐series studies, new or excessive fatigue and breathlessness were the most commonly reported symptoms, followed by dysfunction in smell (anosmia or hyposmia) or taste (ageusia or hypogeusia), cough and chest pain (Tables 3 and 4). Regarding non‐specific clinical characteristics, rates of new or excessive fatigue ranged from 16–65% within individual study populations, 7 , 28 , 29 , 36 , 39 , 40 , 42 , 43 chest pain occurred in 1–42% of participants, 7 , 28 , 30 , 35 , 39 two studies reported myalgia in 5% of participants, 7 , 39 one study reported arthralgia in 27% of participants 7 and one study reported low‐grade fever in 12% of participants. 40 Regarding respiratory symptoms, breathlessness was reported in 15–50% of participants, 7 , 28 , 29 , 34 , 35 , 36 , 39 , 41 cough in 1–15% of participants 28 , 36 , 39 , 41 and one study reported general respiratory symptoms in 92% of participants. 40 Abnormal pulmonary investigation or imaging findings were reported in five studies. 27 , 34 , 36 , 41 , 43 Issues with smell and taste were reported at rates of 11–45% 7 , 28 , 31 , 39 and 7–11%, 7 , 26 , 28 , 36 , 39 respectively, within individual study populations, with one study describing issues with smell and/or taste in 39% of participants. 33 Other symptoms of potential neurological origin included headache, reported in 4–50% of participants 7 , 36 , 39 , 40 ; memory issues, reported in 5–34% of participants 28 , 39 ; and attention disorder, in 1–27% of participants. 28 , 39 One study reported sleep disorder in 31% of paticipants 28 and another reported new‐onset bowel or bladder incontinence in 13%. 29 Regarding gastrointestinal symptoms, general gastrointestinal issues were reported in 31–35% of participants, 36 , 40 diarrhoea was reported in 1–2% 39 and one study reported abdominal pain in 1% of participants. 7 , 39 Regarding cardiac issues, palpitations of unspecified severity were reported in 23% of participants in one study 40 and three studies reported abnormalities on investigation or imaging. 30 , 35 , 41 Two studies reported at least one ongoing symptom in 57% 42 and 87% 7 of their respective study populations.
The follow‐up periods in which clinical characteristics were observed ranged from approximately 3–16 weeks in the case‐series studies. Starting timepoints varied, with eight studies beginning with the onset of symptoms, 7 , 26 , 27 , 30 , 31 , 33 , 37 , 40 five beginning with hospital discharge, 29 , 36 , 41 , 42 , 43 two beginning with diagnosis, 35 , 38 one with hospital admission, 28 one with fever remission, 34 and one study beginning with consecutive negative test results. 39 Symptoms did not evolve in a predictable way with increasing follow‐up time.
The case–control study examined serum immunological changes in peripheral blood mononuclear cells – at various timepoints from first diagnosis (median 112 days, range 60–136 days) – in 49 patients with previous mild or moderate COVID‐19 compared with 27 matched participants without SARS‐CoV‐2 infection. 32 The patients with past COVID‐19 had lower numbers of invariant natural killer T (NKT) cells and NKT‐like cells compared with the control group without past SARS‐CoV‐2 infection. In addition, these patients had greater numbers of regulatory T‐cells, increased T‐cell immunoglobulin and mucin domain‐3 expression on CD4 and CD8 T cells, increased programmed death‐ligand 1 expression on B cells, and decreased cytotoxic potential of T cells and NKT‐like cells. However, CD4 and CD8 T‐cells showed increased Ki67 expression and were able to produce effector cytokines on T‐cell receptor stimulation.
Effect of past COVID‐19 on postoperative outcomes
Only one study directly investigated the effect of past SARS‐CoV‐2 infection on postoperative outcomes. 44 This was a subgroup analysis of the COVIDSurg–Cancer study of patients undergoing curative elective cancer surgery. The study examined patients in which SARS‐CoV‐2 RNA had been detected in a respiratory swab but who were not suspected of active infection at the time of surgery. The study found that past COVID‐19 was associated with increased odds of pulmonary complications compared to no prior infection, and when analysed by time from positive swab to surgery, both pulmonary complications and mortality were lowest 4 weeks after the swab. Nevertheless, more than 70% of included patients had had their surgeries within 4 weeks of confirmed SARS‐CoV‐2 infection.
In addition to this study, five expert consensus guidance documents also provided data around alterations to surgical management for surgical patients who had recovered from COVID‐19. 45 , 46 , 47 , 48 , 49 Within these guidelines, there was notable heterogeneity in the advice provided. Some stated that after a positive SARS‐CoV‐2 test, surgery should be delayed until patients are no longer infectious and have demonstrated recovery from COVID‐19. 47 , 48 Some advised deferral for at least 2–4 weeks, 49 while others recommended a minimum of 8 weeks without symptoms before all but minor elective procedures. 45 There was consensus; however, regarding the need for comprehensive preoperative re‐evaluation, including clinical review of the cardiac and respiratory systems and exercise capacity. 45 , 46 , 47 For patients experiencing ongoing symptoms after laboratory recovery from acute SARS‐CoV‐2 infection, it was advised that a multisystem and multidisciplinary approach is taken to assessment and rehabilitation. 50
Discussion
This study evaluates the long‐term effects after SARS‐CoV‐2 infection that have been reported so far in the literature, in addition to potential impacts on surgery and perioperative care. On the basis of a rapid review, evidence‐based recommendations have been produced regarding the period of delay necessary to allow for adequate recovery of surgical patients after COVID‐19 (Table 5). 20 Articles were sourced from peer‐reviewed, non‐refereed and grey literature, given the uniqueness of the topic. Lower levels of evidence predominated. Case‐series studies formed the majority of the literature around the long‐term clinical characteristics associated with COVID‐19. The sole case–control study described immune signatures in patients recovering from SARS‐CoV‐2 infection, and found that the cellular immune systems of these patients may be impacted for multiple months after laboratory confirmation of infection. 32 Only one study directly investigated the effect of past COVID‐19 on postoperative outcomes, suggesting that care of cancer patients with past SARS‐CoV‐2 infection may be optimized by delaying elective curative surgery by at least 4 weeks after a positive swab. 44
Table 5.
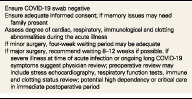
Recommendations from the working group on delaying surgery for patients recovering from COVID‐19 20
| Ensure COVID‐19 swab negative |
| Ensure adequate informed consent; if memory issues may need family present |
| Assess degree of cardiac, respiratory, immunological and clotting abnormalities during the acute illness |
| If minor surgery, four‐week waiting period may be adequate |
| If major surgery, recommend waiting 8–12 weeks if possible. If severe illness at time of acute infection or ongoing long COVID‐19 symptoms suggest physician review; preoperative review may include stress echocardiography, respiratory function tests, immune and clotting status review; potential high dependency or critical care in immediate postoperative period |
Clinical implications
Preoperative assessment of surgical patients can improve outcomes, identify potential anaesthetic difficulties and determine surgical risk. 51 During preoperative evaluation, increased surgical risks associated with perioperative SARS‐CoV‐2 infection need to be considered against the risks of delaying surgery for individual patients. 3 There is strong evidence demonstrating an association between surgery on COVID‐19 patients and significant rates of postoperative complications, particularly of a pulmonary or thrombotic nature. 2 , 3 The difficulty of this decision‐making process is further compounded by the fact that COVID‐19 may be more important than other surgical risk factors in preoperative evaluation. 2 Conditions such as diabetes and obesity that may affect surgical risk and worsen outcomes after acute illness, must still be considered in the presence of SARS‐CoV‐2 infection.
This review provides the best available evidence on the persistent clinical manifestations and immunological dysregulation associated with COVID‐19. It recommends that a complex risk–benefit deliberation should be undertaken within 4 weeks of laboratory confirmation of SARS‐CoV‐2 infection when considering patients for minor surgery, and from 8–12 weeks when considering patients for major surgery (Table 5). For patients who have severe illness during either the acute phase of SARS‐CoV‐2 infection or the ongoing disease process, it is advised that they are reviewed preoperatively by a physician and undergo investigations including stress echocardiography, respiratory function tests, and immune and clotting status review. For certain patients with severe disease, admission to high dependency or critical care units in the immediate postoperative period may be required. Further, given some studies reported lasting issues with cognition and memory, 28 , 39 preoperative processes of ensuring adequate informed consent may also need to be considered, such as the preoperative provision of written information or obtaining consent in the presence of a patient's next of kin.
The findings from this study have direct implications for systems of surgical and perioperative care. Delay of non‐urgent operations to minimize transmission of SARS‐CoV‐2 in the early stages of the pandemic resulted in long‐lasting disruption to surgical systems worldwide. 5 To avoid similar effects arising from the need to delay surgery in patients recovering from COVID‐19, cases must be considered on an individual basis using a data‐driven approach incorporating resource supply and local COVID‐19 prevalence. 1 More intensive surveillance must occur for patients with both COVID‐19 and cancer 52 to ensure clinical decision‐making accounts for current circumstances and unnecessary delay is avoided. Where possible, if surgery is delayed after confirmation of SARS‐CoV‐2 infection, nonoperative management strategies that do not worsen patient outcomes should be considered by the treating surgical team. 1
Limitations
The primary limitation of this study was the inclusion of evidence from non‐refereed and grey literature. Given the novelty of the topic; however, widely accepted methods 21 , 23 were used to rigorously evaluate this literature along with peer‐reviewed sources, which allowed us to extract data that may otherwise have been missed. The rapid evolution of the evidence base associated with the increased data‐sharing during the COVID‐19 pandemic 53 means that new relevant data may soon be available. 8 The process of selecting relevant studies and data extraction was conducted by a single reviewer, leading to potential selection bias; however, all synthesized data were reviewed by a working group of clinical experts prior to the formulation of the evidence‐based recommendations. Collaboration between researchers and expert clinicians also ensured enhanced clinical relevance of the evidence presented within the final report. Not all included studies provided baseline measures of patient quality of life or symptoms existing prior to SARS‐CoV‐2 infection, which added a degree of bias to the association of certain clinical profiles with the long‐term effects of COVID‐19. Similarly, the symptoms outlined, particularly those of a psychological nature, rely on subjective patient reports, thus carrying the possibility of misestimation. Likewise, symptom aetiology may be attributed to COVID‐19 when in reality it may be multifactorial, with many of the lifestyle changes associated with the pandemic also playing a role. 8
Conclusions
This rapid review synthesizes the available data around the long‐term clinical manifestations of COVID‐19 and associated impacts on postoperative care. Utilizing these findings alongside input from a working group of clinical experts, evidence‐based guidance regarding delaying surgery for patients recovering from COVID‐19 was developed. Given persistent clinical manifestations and immunological dysregulation, minor surgery should be delayed for at least 4 weeks and major surgery for 8–12 weeks after laboratory confirmation of SARS‐CoV‐2 infection, where it does not compromise patient outcome. Methods must be implemented to ensure adequate informed consent if COVID‐19 results in ongoing issues with memory or cognition. Comprehensive preoperative and ongoing assessment must be carried out to ensure optimal clinical decision‐making. As SARS‐CoV‐2 does not conform to previous knowledge of respiratory viruses, future research of COVID‐19 via studies of strong design is required to clarify the direct, long‐term effects of SARS‐CoV‐2 infection on both preoperative risk profile and postoperative outcomes.
Author contributions
Joshua Kovoor: Conceptualization; investigation; writing‐original draft; writing‐review and editing. N. Ann Scott: Data curation; formal analysis; investigation; methodology; writing‐original draft; writing‐review and editing. David Tivey: Conceptualization; investigation; methodology; supervision; writing‐review and editing. Wendy Babidge: Conceptualization; formal analysis; investigation; supervision; writing‐review and editing. David Scott: Conceptualization; investigation; supervision; writing‐review and editing. Vanessa Beavis: Conceptualization; investigation; supervision; writing‐review and editing. Jen Kok: Conceptualization; investigation; supervision; writing‐review and editing. Conceptualization; investigation; supervision; writing‐review and editing. R Padbury: Conceptualization; investigation; supervision; writing‐review and editing. Thomas Hugh: Conceptualization; investigation; supervision; writing‐review and editing. Peter Hewett: Conceptualization; investigation; supervision; writing‐review and editing. Trevor Collinson: Conceptualization; investigation; supervision; writing‐review and editing. Guy Maddern: Conceptualization; investigation; supervision; writing‐review and editing.
Conflicts of interest
None declared.
Acknowledgements
The authors would like to thank Kaitryn Campbell for assistance with the literature searches and Kristin Weidenbach for copyediting the final version of this report. Funding was provided by Royal Australasian College of Surgeons, Research Audit and Academic Surgery.
Search strategy
| # | Searches | Results (4 October 2020) |
|---|---|---|
| 1 | *Coronavirus Infections/ | 28 966 |
| 2 | (COVID‐19 OR COVID19).mp. | 55 103 |
| 3 | ((pneumonia OR COVID* OR coronavirus* OR corona virus* OR ncov* OR 2019‐ncov OR sars*) AND (hubei OR wuhan OR beijing OR shanghai)).ti,kf. | 925 |
| 4 | Wuhan virus*.ti,kf. | 8 |
| 5 | (19nCoV OR 2019‐nCoV OR 2019nCoV).ti,kf. | 726 |
| 6 | (nCoV* OR n‐CoV*).ti,kf. | 804 |
| 7 | (“CoV 2” OR CoV2).ti,kf. | 13 275 |
| 8 | (OC43 OR NL63 OR 229E OR HKU1 OR HCoV* OR Sars‐coronavirus*).ti,kf. | 1343 |
| 9 | (2019‐novel CoV OR Sars‐coronavirus2 OR Sars‐coronavirus‐2 OR SARS‐like coronavirus* OR ((novel OR new OR nouveau) adj2 (CoV OR nCoV OR COVID OR coronavirus* OR corona virus OR Pandemi*2)) OR (coronavirus* AND pneumonia)).ti,kf. | 3334 |
| 10 | COVID‐19.rx,px,ox. OR severe acute respiratory syndrome coronavirus 2.os. | 26 764 |
| 11 | severe acute respiratory syndrome coronavirus 2.ti,kf. | 1245 |
| 12 | (SARSCoV* OR SARS‐CoV* OR SARS2 OR SARS‐2).ti,kf. | 14 065 |
| 13 | (novel coronavirus* OR novel corona virus* OR novel CoV).ti,kf. | 2086 |
| 14 | ((coronavirus* OR corona virus*) adj2 “2019”).ti,kf. | 5035 |
| 15 | ((coronavirus* OR corona virus*) adj2 “19”).ti,kf. | 940 |
| 16 | (coronavirus 2 OR corona virus 2).ti,kf. | 1371 |
| 17 | COVID*.ti,kf. | 48 101 |
| 18 | OR/1–17 | 63 813 |
| 19 | (201 911* OR 202*).dp. OR 20191101:20301231.(ep). OR 20191101:20301231.(dt) | 1 400 591 |
| 20 | 18 AND 19 | 58 365 |
| 21 | *Coronavirus Infections/su [surgery] | 44 |
| 22 | exp *Specialties, Surgical/ | 156 391 |
| 23 | exp *Surgical Procedures, Operative/ | 2 012 842 |
| 24 | (intraoperat* OR intra‐operat* OR operation? OR operative* OR preoperat* OR pre‐operat* OR peroperat* OR per‐operat* OR perioperat* OR peri‐operat* OR postoperat* OR post‐operat* OR presurg* OR pre‐surg* OR perisurg* OR peri‐surg* OR postsurg* OR post‐surg* OR reoperat* OR re‐operat* OR surgeries OR surgery OR surgeon? OR surgical*).ti,kf. | 1 017 840 |
| 25 | OR/21–24 | 2 666 199 |
| 26 | *Failure to Rescue, Health Care/ OR *Hospitalization/ OR exp. *Intensive Care Units/ OR exp. *Mortality/ OR *Patient Admission/ | 151 536 |
| 27 | exp *Specialties, Surgical/ae, co, mo [adverse effects, complications, mortality] | 1154 |
| 28 | exp *Surgical Procedures, Operative/ae, co, mo [adverse effects, complications, mortality] | 256 808 |
| 29 | (admission? OR admitted OR admitting OR adverse* OR complication? OR complicat* OR death* OR fatal OR fatalit* OR hospitalis* OR hospitaliz* OR icu? OR ((coronary OR intensive* OR respiratory) adj2 (care OR unit?)) OR mortalit*).ti,kf. | 789 014 |
| 30 | (ae OR co OR mo).fs. | 3 929 637 |
| 31 | OR/26–30 | 4 397 057 |
| 32 | *Brain Ischemia/ OR exp. *Intracranial Hemorrhages/ OR exp *Stroke/ OR *Stroke Rehabilitation/ | 178 858 |
| 33 | (stroke* OR poststroke? OR post‐stroke? OR CVA OR CVAs).ti,kf. | 123 321 |
| 34 | ((cerebrovascular* OR cerebro‐vascular* OR cerebral vascular*) adj2 (apoplex* OR accident* OR infarct*)).ti,kf. | 2235 |
| 35 | ((brain OR cerebral OR intracerebral OR intra‐cerebral OR arachnoid OR subarachnoid OR sub‐arachnoid OR intracranial* OR intra‐cranial* OR cranial*) adj2 (infarct* OR isch?emi* OR h?emorrhag*)).ti,kf. | 60 590 |
| 36 | ((postacute OR post‐acute OR chronic) adj5 (stroke* OR poststroke? OR post‐stroke?)).ti,kf. | 2513 |
| 37 | (((postacute OR post‐acute OR chronic) adj5 (hemipare* OR paretic OR paresis OR phase? OR stage? OR state? OR condition? OR paraly* OR spastic*)) AND (stroke* OR poststroke? OR post‐stroke?)).ti,kf. | 363 |
| 38 | exp *Heart Diseases/ | 967 223 |
| 39 | ((cardiac* OR heart? OR myocardia* OR myo‐cardia*) adj2 (attack? OR event? OR failure? OR infarct* OR ruptur*)).ti,kf. | 193 632 |
| 40 | *Lung/pa, pp | 24 203 |
| 41 | exp *Lung Injury/ | 33 043 |
| 42 | ((lung? adj2 (damag* OR injur*)) OR pulmonary function*).ti,kf. | 25 199 |
| 43 | *Respiratory Distress Syndrome, Adult/ | 15 345 |
| 44 | (((acute OR syndrome?) adj (respiratory distress OR respiratory failure)) OR ARDS OR ARDSS).ti,kf. | 12 995 |
| 45 | *Venous Thrombosis/ OR *Upper Extremity Deep Vein Thrombosis/ | 20 802 |
| 46 | ((deep adj (vein OR venous) adj (thrombos?s OR thrombus)) OR deep thrombophlebitis OR deep thrombo‐phlebitis OR DVT OR DVTs).ti,kf. | 12 115 |
| 47 | exp *Pulmonary Embolism/ | 28 762 |
| 48 | ((lung? OR pulmonary) adj (embol* OR infarct* OR micro‐embol* OR microembol* OR thrombo‐embol* OR thromboembol*)).ti,kf. | 23 406 |
| 49 | OR/26–48 | 5 216 331 |
| 50 | exp *Intraoperative Complications/ | 25 785 |
| 51 | exp *Postoperative Complications/ | 291 232 |
| 52 | OR/50–51 | 309 653 |
| 53 | exp animals/ | 23 471 581 |
| 54 | exp animal experimentation/ OR exp. animal experiment/ | 9487 |
| 55 | exp models animal/ | 573 370 |
| 56 | nonhuman/ | 0 |
| 57 | exp vertebrate/ OR exp. vertebrates/ | 22 807 589 |
| 58 | OR/53–57 | 23 473 525 |
| 59 | exp humans/ | 18 732 734 |
| 60 | exp human experimentation/ OR exp. human experiment/ | 12 488 |
| 61 | OR/59–60 | 18 733 389 |
| 62 | 58 NOT 61 | 4 740 761 |
| 63 | (20 AND 52) OR (20 AND 25 AND 49) | 796 |
| 64 | 63 NOT 62 | 795 |
| 65 | limit 64 to English language | 767 |
| 66 | *Long Term Adverse Effects/ | 373 |
| 67 | ((duration? OR follow‐up* OR followup* OR long‐term* OR longterm* OR persistent* OR post‐recover* OR postrecover*) adj2 (complication? OR consequence? OR (adverse* adj effect?) OR implication? OR outcome? OR sequelae OR symptom?)).ti,kf. | 27 460 |
| 68 | *Recovery of Function/ | 12 977 |
| 69 | ((recover* OR return*) adj2 (baseline? OR base‐line? OR disease? OR function* OR health* OR patient* OR usual)).ti,kf. | 9251 |
| 70 | OR/66–69 | 47 842 |
| 71 | 20 AND 70 | 126 |
| 72 | 71 NOT 62 | 126 |
| 73 | limit 72 to English language | 125 |
J. G. Kovoor BHlthMedSc (Hons); N. A. Scott BSc (Hons), PhD; D. R. Tivey BSc (Hons), PhD; W. J. Babidge BApp Sci (Hons), PhD; D. A. Scott PhD, FANZCA; V. S. Beavis MBBS, FANZCA; J. Kok PhD, FRCPA; A. D. MacCormick PhD, FRACS; R. T. A. Padbury PhD, FRACS; T. J. Hugh MD, FRACS; P. J. Hewett MBBS, FRACS; T. G. Collinson MS, FRACS; G. J. Maddern PhD, FRACS; M. Frydenberg MBBS, FRACS.
References
- 1. Babidge WJ, Tivey DR, Kovoor JG et al. Surgery triage during the COVID‐19 pandemic. ANZ J. Surg. 2020; 90: 1558–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Doglietto F, Vezzoli M, Gheza F et al. Factors associated with surgical mortality and complications among patients with and without coronavirus disease 2019 (COVID‐19) in Italy. JAMA Surg. 2020; 155: 1–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. COVIDSurg Collaborative . Mortality and pulmonary complications in patients undergoing surgery with perioperative SARS‐CoV‐2 infection: an international cohort study. Lancet 2020; 396: 27–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Kovoor JG, Tivey DR, Williamson P et al. Screening and testing for COVID‐19 before surgery. ANZ J. Surg. 2020; 90: 1845–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. COVIDSurg Collaborative . Elective surgery cancellations due to the COVID‐19 pandemic: global predictive modelling to inform surgical recovery plans. Br. J. Surg. 2020; 107: 1440–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Guan WJ, Ni ZY, Hu Y et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020; 382: 1708–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Carfi A, Bernabei R, Landi F, Gemelli Against COVID‐19 Post‐Acute Care Study Group . Persistent symptoms in patients after acute COVID‐19. JAMA 2020; 324: 603–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Huang C, Huang L, Wang Y et al. 6‐month consequences of COVID‐19 in patients discharged from hospital: a cohort study. Lancet 2021; 397: 220–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Datta SD, Talwar A, Lee JT. A proposed framework and timeline of the spectrum of disease due to SARS‐CoV‐2 infection: illness beyond acute infection and public health implications. JAMA 2020; 324: 2251–2. [DOI] [PubMed] [Google Scholar]
- 10. National Institute for Health and Care Excellence, Royal College of General Practitioners, Healthcare Improvement Scotland SIGN . COVID‐19 Rapid Guideline: Managing the Long‐Term Effects of COVID‐19. [Updated 18 Dec 2020; Cited 29 Dec 2020.] Available from URL: https://www.nice.org.uk/guidance/ng188
- 11. Cortinovis M, Perico N, Remuzzi G. Long‐term follow‐up of recovered patients with COVID‐19. Lancet 2021; 397: 173–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Gousseff M, Penot P, Gallay L et al. Clinical recurrences of COVID‐19 symptoms after recovery: viral relapse, reinfection or inflammatory rebound? J. Infect. 2020; 81: 816–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Tay MZ, Poh CM, Renia L, MacAry PA, Ng LFP. The trinity of COVID‐19: immunity, inflammation and intervention. Nat. Rev. Immunol. 2020; 20: 363–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Mahase E. Covid‐19: what do we know about "long covid"? BMJ 2020; 370: m2815. [DOI] [PubMed] [Google Scholar]
- 15. Tan L, Kovoor JG, Williamson P et al. Personal protective equipment and evidence‐based advice for surgical departments during COVID‐19. ANZ J. Surg. 2020; 90: 1566–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Tivey DR, Davis SS, Kovoor JG et al. Safe surgery during the coronavirus disease 2019 crisis. ANZ J. Surg. 2020; 90: 1553–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Maddern GJ. Evidence, not eminence, in coronavirus disease 2019. ANZ J. Surg. 2020; 90: 1537. [DOI] [PubMed] [Google Scholar]
- 18. Kovoor JG, Tivey DR, Babidge WJ, Maddern GJ. COVID‐19: a test of evidence‐based surgery. BJS 2020; 108: e5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Greenhalgh T, Knight M, A'Court C, Buxton M, Husain L. Management of post‐acute covid‐19 in primary care. BMJ 2020; 370: m3026. [DOI] [PubMed] [Google Scholar]
- 20. Royal Australasian College of Surgeons . Delaying Surgery for Patients Recovering from COVID‐19: A Rapid Review Commissioned by RACS. [Cited 14 Jan 2021.] Available from URL: https://www.surgeons.org/-/media/Project/RACS/surgeons-org/files/news/covid19-information-hub/2021-01-11-RACS-Post-covid-delay-to-surgery-report.pdf?rev=f3af8dee5c9447d0bb9f00bfb5cec2dc&hash=F90FD9A387E07501ECC72B020DFC62CC
- 21. Watt A, Cameron A, Sturm L et al. Rapid versus full systematic reviews: validity in clinical practice? ANZ J. Surg. 2008; 78: 1037–40. [DOI] [PubMed] [Google Scholar]
- 22. World Health Organization . Pneumonia of Unknown Cause – China. [Cited 24 Nov 2020.] Available from URL: https://www.who.int/csr/don/05-january-2020-pneumonia-of-unkown-cause-china/en
- 23. Canadian Agency for Drugs and Technologies in Health (CADTH) . Grey Matters: A Practical Tool for Searching Health‐Related Grey Literature. [Updated 8 May 2019; Cited 24 Nov 2020.] Available from URL: https://www.cadth.ca/resources/finding-evidence/grey-matters
- 24. Reagan‐Udall Foundation for the FDA . COVID‐19 Evidence Accelerator. [Cited 24 Nov 2020.] Available from URL: https://www.evidenceaccelerator.org/
- 25. Merlin T, Weston A, Tooher R. Extending an evidence hierarchy to include topics other than treatment: revising the Australian 'levels of evidence'. BMC Med. Res. Methodol. 2009; 9: 34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Chiesa‐Estomba CM, Lechien JR, Barillari MR, Saussez S. Patterns of gustatory recovery in patients affected by the COVID‐19 outbreak. Virol. Sin. 2020; 35: 833–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Ding X, Xu J, Zhou J, Long Q. Chest CT findings of COVID‐19 pneumonia by duration of symptoms. Eur. J. Radiol. 2020; 127: 109009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Garrigues E, Janvier P, Kherabi Y et al. Post‐discharge persistent symptoms and health‐related quality of life after hospitalization for COVID‐19. J. Infect. 2020; 81: e4–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Halpin SJ, McIvor C, Whyatt G et al. Postdischarge symptoms and rehabilitation needs in survivors of COVID‐19 infection: a cross‐sectional evaluation. J. Med. Virol. 2021; 93: 1013–22. [DOI] [PubMed] [Google Scholar]
- 30. Huang L, Zhao P, Tang D et al. Cardiac involvement in patients recovered from COVID‐2019 identified using magnetic resonance imaging. JACC Cardiovasc. Imaging 2020; 13: 2330–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Li J, Long X, Zhu C et al. Olfactory dysfunction in recovered coronavirus disease 2019 (COVID‐19) patients. Mov. Disord. 2020; 35: 1100–1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Liu J, Yang X, Wang H et al. The analysis of the long‐term impact of SARS‐CoV‐2 on the cellular immune system in individuals recovering from COVID‐19 reveals a profound NKT cell impairment. medRxiv 2020. 10.1101/2020.08.21.20179358:2020.08.21.20179358. [DOI] [Google Scholar]
- 33. Otte MS, Eckel HNC, Poluschkin L, Klussmann JP, Luers JC. Olfactory dysfunction in patients after recovering from COVID‐19. Acta Otolaryngol. 2020; 140: 1032–5. [DOI] [PubMed] [Google Scholar]
- 34. Patelli G, Paganoni S, Besana F et al. Preliminary detection of lung hypoperfusion in discharged Covid‐19 patients during recovery. Eur. J. Radiol. 2020; 129: 109121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Puntmann VO, Carerj ML, Wieters I et al. Outcomes of cardiovascular magnetic resonance imaging in patients recently recovered from coronavirus disease 2019 (COVID‐19). JAMA Cardiol. 2020; 5: 1265–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Zhao YM, Shang YM, Song WB et al. Follow‐up study of the pulmonary function and related physiological characteristics of COVID‐19 survivors three months after recovery. EClinicalMedicine 2020; 25: 100463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Arnold DT, Hamilton FW, Milne A et al. Patient outcomes after hospitalisation with COVID‐19 and implications for follow‐up; results from a prospective UK cohort. medRxiv 2020. 10.1101/2020.08.12.20173526:2020.08.12.20173526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Clark DE, Parikh A, Dendy JM et al. COVID‐19 myocardial pathology evaluated through scrEening cardiac magnetic resonance (COMPETE CMR). medRxiv 2020. 10.1101/2020.08.31.20185140. [DOI] [Google Scholar]
- 39. Klein H, Asseo K, Karni N et al. Onset, duration, and persistence of taste and smell changes and other COVID‐19 symptoms: longitudinal study in Israeli patients. medRxiv 2020. 10.1101/2020.09.25.20201343:2020.09.25.20201343. [DOI] [Google Scholar]
- 40. O'Keefe JB, Cellai M. Characterization of prolonged COVID‐19 symptoms and patient comorbidities in an outpatient telemedicine cohort. medRxiv 2020. 10.1101/2020.07.05.20146886:2020.07.05.20146886. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Sahanic S, Sonnweber T, Pizzini A et al. Persisting pulmonary impairment following severe SARS‐CoV‐2 infection, preliminary results from the CovILD study. European Respiratory Society International Congress. Virtual, 2020.
- 42. Townsend L, Dyer AH, Jones K et al. Persistent fatigue following SARS‐CoV‐2 infection is common and independent of severity of initial infection. medRxiv 2020. 10.1101/2020.07.29.20164293:2020.07.29.20164293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Weerahandi H, Hochman KA, Simon E et al. Post‐discharge health status and symptoms in patients with severe COVID‐19. medRxiv 2020. 10.1101/2020.08.11.20172742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. COVIDSurg Collaborative . Delaying surgery for patients with a previous SARS‐CoV‐2 infection. Br. J. Surg. 2020; 107: e601–2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Royal Australasian College of Surgeons . Guidance on delay to elective surgery post recovery from SARS‐CoV‐2 infection (5 August 2020). [Updated 5 Aug 2020; Cited 25 Nov 2020.] Available from URL: https://www.surgeons.org/-/media/Project/RACS/surgeons-org/files/news/covid19-information-hub/Perioperative-Guidance-post-COVID-infection.pdf?rev=7592ce808e8c4ac19dc2c8856bde48fa&hash=216BF43F414EA0293F1C717E4A79E43A.
- 46. American College of Surgeons, American Society of Anesthesiologists, Association of periOperative Registered Nurses, American Hospital Association . Joint Statement: Roadmap for Maintaining Essential Surgery during COVID‐19 Pandemic. [Updated 10 Aug 2020; Cited 25 Nov 2020.] Available from URL: https://www.asahq.org/about-asa/newsroom/news-releases/2020/08/joint-statement-roadmap-for-maintaining-essential-surgery-during-covid-19-pandemic
- 47. Anesthesia Patient Safety Foundation . COVID‐19 and Anesthesia FAQ. [Updated 4 Aug 2020; Cited 25 Nov 2020.] Available from URL: https://www.apsf.org/COVID-19-and-anesthesia-faq/
- 48. Healthcare Improvement Scotland . COVID‐19 Position Statement: Reducing the Risk of Postoperative Mortality Due to COVID‐19 in Patients Undergoing Elective Surgery. [Updated 21 Aug 2020; Cited 25 Nov 2020.] Available from URL: https://www.sign.ac.uk/media/1744/elective-surgery_v111.pdf
- 49. Patel V, Jimenez E, Cornwell L et al. Cardiac surgery during the coronavirus disease 2019 pandemic: perioperative considerations and triage recommendations. J. Am. Heart Assoc. 2020; 9: e017042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Barker‐Davies RM, O'Sullivan O, Senaratne KPP et al. The Stanford hall consensus statement for post‐COVID‐19 rehabilitation. Br. J. Sports Med. 2020; 54: 949–59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Garcia‐Miguel FJ, Serrano‐Aguilar PG, Lopez‐Bastida J. Preoperative assessment. Lancet 2003; 362: 1749–57. [DOI] [PubMed] [Google Scholar]
- 52. Liang W, Guan W, Chen R et al. Cancer patients in SARS‐CoV‐2 infection: a nationwide analysis in China. Lancet Oncol. 2020; 21: 335–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Glasziou PP, Sanders S, Hoffmann T. Waste in covid‐19 research. BMJ 2020; 369: m1847. [DOI] [PubMed] [Google Scholar]