

Abstract
Aim
To investigate the nurses' work environment in university hospitals during the COVID‐19 pandemic in Brazil.
Background
The COVID‐19 pandemic brought challenging times for nurses worldwide. In Brazil, as well as in several countries, nurses are working hard in hospital settings caring for patients infected with the virus, sometimes with unfavourable work environment conditions.
Methods
This study was a convergent embedded mixed methods research. The sample comprised 104 nurses from three Brazilian university hospitals. Data were collected in April–June 2020 from an online questionnaire with a self‐reporting Likert scale survey designed to measure the nurses' perceptions of their work environment. Qualitative data in the form of written comments were also collected through an open question. Data were analysed using descriptive statistics and content analysis.
Results
The quantitative results showed that the responses to ‘I received training on the correct use of personal protective equipment’ and ‘I am afraid of being infected’ items had the best and worst evaluations, respectively. The qualitative findings revealed five themes: feeling of insecurity, lack of personal protective equipment, lack of diagnostic tests, changes in the care flow and fear of the unknown.
Conclusion
The study has highlighted the challenges faced by hospital nurses while caring for patients with COVID‐19.
Implications for Nursing and Nursing Policy
The gaps identified will assist the policymakers and hospital managers in developing policies to enhance the support offered to nurses and improve the care provided to patients with COVID‐19 in university hospitals. The results also indicate the need for attention to the mental health of the professionals due to the increasing workload and treatment of an illness hitherto unknown.
Keywords: coronavirus infections, hospitals, university, nurse's role, organization and administration, pandemics, work environment
Introduction
Since the end of December 2019, an outbreak of a new disease named COVID‐19 (Corona Virus Disease 2019), caused by coronavirus 2 (SARS‐CoV‐2), has been reported in Wuhan, China, and subsequently became a pandemic (Wu et al. 2020). COVID‐19 arrived in Latin America on 25 February 2020, when the Brazilian Ministry of Health confirmed the first case of the disease in the national territory (Rodriguez‐Morales et al. 2020).
In December 2020, Brazil held the third and second place on the global COVID‐19 ranking for confirmed and fatal cases, respectivel, with more than 6 million confirmed cases and 176 000 deaths due to the new coronavirus disease in the country (Center for Systems Science & Engineering of the Johns Hopkins University 2020).
In the global response to the disease, hospital care plays a key role, through the provision of intensive care to patients and a reduction in fatality rates due to COVID‐19 (Wu et al. 2020). For this purpose, investments have been made to expand the staff and the installed capacity of beds and equipment, as well as the reorganization of care processes in the hospital context. In this setting, university hospitals stand out in caring for patients with COVID‐19 as reference centres of medium and high complexity for the Unified Health System in Brazil (Medeiros 2020).
In the hospital environment, the nursing team is responsible for most of the care procedures that the patients receive during their hospitalization. Therefore, nursing has been a protagonist in the care of hospitalized patients with COVID‐19, developing a vital role on innovating practice (Bitencourt et al. 2020; Huang et al. 2020; Medeiros 2020; Rosa et al. 2020).
The 2020 State of the World's Nursing (World Health Organization 2020) highlighted that nurses at the frontline represent 59% of the health workforce and are the critical manpower to prevent the collapse of the healthcare system due to any pandemic crisis. Nurses have always been at the centre of early detection, triage and health promotion during infectious outbreaks, so it is no surprise that they are critical contributors during the COVID‐19 pandemic (Turale et al. 2020) and in the world's acquisition of new skills and knowledge. Furthermore, in most novel infectious diseases, the art and science of nursing care is the mainstay of the treatment plan.
The nursing workforce in Brazil is made up of approximately 1.6 million workers, which represents nearly 50% of the healthcare workforce, divided in three levels of education. From the total of the nursing workforce, 80% are nursing technicians or nursing assistants, and 20% are registered nurses (Machado et al. 2016). Registered nurses are those who are trained in four or five‐year university courses. Nursing technicians receive a diploma after 18 months of education and training in technical schools. Lastly, nursing assistants are those who have a one‐year diploma, but this category has been eliminated to improve the level of education in nursing. The registered nurse supervises the work of the nursing technicians and nursing assistants who work under the direction of the registered nurse in providing bedside care.
Therefore, the search for excellence in institutional results requires knowledge of the characteristics of the nursing work environment, such as, organizational support, access to resources, quality of relationships with the health team, autonomy, as well as the control that nurses hold in solving problems that affect patient care. A work environment with characteristics favourable to the nursing practice is important to improve patient safety and to reduce burnout and the intention of quitting a job among the professionals (Lake et al. 2019; Li et al. 2019; Nelson‐Brantley et al. 2018; Ozer et al. 2017; Santos et al. 2017).
A favourable work environment is even more urgent in face of the COVID‐19 pandemic, since nurses are responsible for taking care of patients, planning and organizing the structural conditions and the nursing staff for the provision of care (Santos et al. 2017). However, unfortunately, the reality has shown the difficulties faced by nurses in their work environment during the COVID‐19 pandemic. As of early June 2020, more than 600 nurses died from the COVID‐19 pandemic due to insufficient personal protective equipment (PPE) (International Council of Nurses 2020). Only Brazil accounts for 30% of the nurses' deaths on the planet (Brazilian Federal Nurses Council 2020), which reveals the importance of studying the nurses' work environment during the COVID‐19 pandemic, especially in the hospital context.
Aim
This study aimed to investigate the nurses' work environment in university hospitals during the COVID‐19 pandemic in Brazil.
Methods
Design
This was a convergent embedded mixed methods research, with quantitative and qualitative data collection at the same time, but with a main method and a secondary database (Creswell & Plano Clark 2013). This study focused on the quantitative approach (QUANT) with a cross‐sectional design and incorporation of qualitative data (qual) to complement the information. The Mixed Methods Appraisal Tool (MMAT) was used for assuring the research methodological rigour (Hong et al. 2019).
Sample and setting
The setting consisted of three large‐size university hospitals in Brazil, two in the South and one in the Southeast. These hospitals were selected with the objective of addressing the Brazilian regional diversity, considering the institutions to which the researchers are linked and the existence of an ongoing multicentric project involving members of the research team.
The calculation of the sample size was performed in the Epi‐Info program, version 7.2.3.1. Considering a population of 616, unknown prevalence of 50%, 95% confidence level, and collecting data in three centres, the intended sample size, in order to have a maximum error of 7.5%, was 134 nurses.
Recruitment was carried out by a non‐random convenience sample. All the 616 nurses from the three hospitals received an e‐mail invitation to participate in the study, with weekly follow‐up reminders or reinforcements. According to the time limit, the total number of 104 participants was reached, which can be considered reasonable for online surveys (Nulty 2008; Menon & Muraleedharan 2020), especially considering the context of the COVID‐19 pandemic.
The inclusion criteria for the study were nurses who were working or with the perspective of working in the care of suspected or infected COVID‐19 patients. This inclusion criterion was informed to the participants, in the invitation to answer the online questionnaire. The existence of incomplete information was adopted as exclusion criterion. Nevertheless, no questionnaire was excluded.
Data collection
Data were collected online from April to June 2020. The option for an online questionnaire intended to enhance data collection and facilitate access to a larger number of participants (Hutchinson & Sutherland 2019). Furthermore, it was the most viable strategy considering the restrictions on people circulation and access to hospitals due to the COVID‐19 pandemic.
The data collection instrument was composed of three parts. The first with data on the socio‐professional characterization of the nurses: age, gender, marital status, child(ren), unit, role, training, work shift, another employment contract and length of professional experience (in years). There were also two closed questions: (1) How do you evaluate the experience of working or coming to work in the care of suspected or infected COVID‐19 patients? (negative, neutral, or positive) and (2) How do you perceive the support from nursing management during the pandemic? (bad, medium or good).
In the second part, a self‐made instrument was used because there was not a properly validated instrument available in Portuguese to measure characteristics of the nurses' work during a pandemic, like COVID‐19. The questionnaire was developed based on the Practice Environment Scale of Nursing Work Index (PES‐NWI) (Gasparino & Guirardello 2017; Lake 2002), and a survey used to study the perception of nurses on the care of patients with influenza A (H1N1), during the 2009 pandemic in New Zealand (Honey & Wang 2013).
Before data collection, a pilot test of the questionnaire for face and content validity was performed with two healthcare nurses and two faculty members from the Critical Care Nursing Specialty. The difficulty in completing the instrument and the time required to answer it were evaluated. There were minor suggestions regarding the wording and presentation sequence of the questions. After these reviews, the instrument was sent to the study participants.
The instrument comprised 17 items for which the nurses indicated their level of agreement in relation to the presence of a characteristic in their work environment when caring for suspected or infected COVID‐19 patients. A five‐point Likert scale was used, ranging from 1 (‘strongly disagree’) to 5 (‘strongly agree’). The analysis of the instrument was based on the mean of the scores per item and, subsequently, the general mean value of the instrument. Thus, it is noteworthy that the higher the mean, the better the perception of the work environment during the pandemic.
The third part of the questionnaire contained an optional open‐ended (free text) question about the challenges of the work during the COVID‐19 pandemic. Of the total study participants, 86 nurses answered this question.
Data analysis
The Statistical Package for Social Sciences (SPSS, Inc, Chicago, IL) software was used for data analysis of the quantitative arm of the study. The categorical variables were evaluated using absolute and percentage frequencies. For the continuous variables, measures of position (mean, minimum and maximum) and dispersion (standard deviation) were analysed. The normality of the data was checked using the Kolmogorov–Smirnov test. For the variables that followed normal distribution, the Student's t‐test and ANOVA were used; and, for the data that did not meet normal distribution, the Mann–Whitney and Kruskal–Wallis tests were used.
The qualitative data were analysed through content analysis according to the approach proposed by Graneheim & Lundman (2004). The answers by the nurses were reviewed several times by the research team to obtain an initial idea and general understanding of the data. Subsequently, the written comments were read line by line, and the initial coding was carried out to find the ideas related to the challenges faced by the nurses in caring for suspected or infected COVID‐19 patients. Subcategories were then formed according to the similarities in the initial codes, and categories were later formed according to the differences and similarities between these subcategories. Finally, the main themes were identified and appropriately named. The IRAMUTEQ® software was used to simplify data classification and analysis (Souza et al. 2018).
Quantitative and qualitative data combination was performed through incorporation, which means that the qualitative results were used as support for the interpretation of the main quantitative findings (Creswell & Plano Clark 2013; Hong et al. 2019).
Ethical consideration
All the participants were fully informed about the purpose of the study, voluntary participation, their anonymity and confidentiality. Answering the survey was voluntary through online consent to participate. At any time, the participants had the right to withdraw. The confidentiality of the participants was respected. The Federal University of Santa Maria Ethical Committee approved the study protocol (approval number: 3.993.920).
Results
Quantitative arm
The study was attended by 104 nurses, with a mean age of 38.9 (±8.8) years old and a mean professional experience of 13.69 (±8.99) years. There was a significant relationship in the work environment variable between sector, training, work shift, experience of working or coming to work in the care of suspected or infected COVID‐19 patients, and perception of the support from nursing management during the pandemic. The details of the nurses' demographics are presented in Table 1, as well as their association with the work environment variable. Values in bold indicate statistically significant results.
Table 1.
Nurses' demographics and association with the work environment
| Variable | Sample | Work environment | P |
|---|---|---|---|
| Gender | 0.67 † | ||
| Female | 87 (83.7) | 2.30 ± 0.77 | |
| Male | 17 (16.3) | 3.07 ± 0.62 | |
| Marital status | 0.31 † | ||
| With a partner | 72 (69.2) | 2.97 ± 0.76 | |
| Without a partner | 32 (30.8) | 3.11 ± 0.71 | |
| Children | 0.35 † | ||
| Yes | 63 (60.6) | 2.95 ± 0.77 | |
| No | 41 (39.4) | 3.10 ± 0.70 | |
| Sector | 0.00 ‡ | ||
| Adult Medical‐Surgical Units | 24 (23.1) | 2.68 ± 0.67 | |
| Paediatric or Neonatal Units | 18 (17.3) | 3.03 ± 0.62 | |
| Intensive Care Unit | 20 (19.2) | 3.47 ± 0.74 | |
| Emergency Room | 12 (11.5) | 2.46 ± 0.67 | |
| Operating Room and Recovery Room | 6 (5.8) | 3.20 ± 0.54 | |
| Others | 24 (23.1) | 3.18 ± 0.60 | |
| Role | 0.26 ‡ | ||
| Registered nurse | 82 (78.8) | 2.91 ± 0.74 | |
| Managerial nurse | 13 (12.5) | 3.25 ± 0.78 | |
| Others | 9 (8.7) | 3.53 ± 0.37 | |
| Training | 0.03 ‡ | ||
| University graduate | 12 (11.5) | 2.67 ± 1.20 | |
| Specialization/Residency | 48 (46.2) | 2.92 ± 0,67 | |
| Master's degree | 38 (36.5) | 3.11 ± 0.67 | |
| Doctoral degree | 6 (5.8) | 3.66 ± 0.35 | |
| Work shift | 0.00 † | ||
| Day | 77 (74.0) | 3.13 ± 0.73 | |
| Night | 27 (26.0) | 2.66 ± 0.69 | |
| Another employment contract | 0.09† | ||
| Yes | 9 (8.7) | 3.40 ± 0.43 | |
| No | 95 (91.3) | 2.97 ± 0.76 | |
| Experience of working or coming to work in the care of suspected or infected COVID‐19 patients | 0.01 § | ||
| Negative | 32 (30.8) | 2.75 ± 0.68 | |
| Neutral | 30 (28.8) | 3.06 ± 0.71 | |
| Positive | 42 (40.4) | 3.16 ± 0.80 | |
| Perception of the support from nursing management during the pandemic | 0.00 ‡ | ||
| Bad | 25 (24.0) | 2.30 ± 0.68 | |
| Medium | 30 (28.8) | 2.82 ± 0.54 | |
| Good | 49 (47.1) | 3.48 ± 0.52 |
Student's t‐test.
ANOVA test.
Kruskal–Wallis test.
The overall mean of the instrument used to evaluate the work environment was 3.02. The best evaluated item was ‘I received training on the correct use of PPE’ and the item with the worst evaluation was ‘I am afraid of being infected’. Table 2 lists the nurses' instrument scores. In relation to the variables associated with the practice environment, the nurses working in intensive care, during the day shift, who considered as neutral the experience of working or coming to work in the care of suspected or infected COVID‐19 patients, and who considered as good the support from nursing management during the pandemic, presented a better perception of the environment.
Table 2.
Descriptive Measures of the Work Environment
| Work environment | Mean | SD | Variation† |
|---|---|---|---|
| I received training on the correct use of personal protective equipment | 4.23 | 1.25 | 1–5 |
| The institution where I work offers training and/or qualification courses on COVID‐19 | 4.00 | 1.14 | 1–5 |
| I can work as a team and develop a collaborative practice with health professionals | 3.78 | 1.11 | 1–5 |
| There is standardization of care rules and procedures | 3.47 | 1.43 | 1–5 |
| I have access to sufficient personal protective equipment to protect me | 3.40 | 1.25 | 1–5 |
| The managers of the institution are attentive and concerned with health professionals | 3.25 | 1.35 | 1–5 |
| I have sufficient materials and supplies at my disposal to provide nursing care | 3.22 | 1.23 | 1–5 |
| I work with enough nursing staff to provide quality care to patients | 3.13 | 1.44 | 1–5 |
| The physical environment of the unit is adequate and safe for me to perform my duties | 3.05 | 1.15 | 1–5 |
| There was an increase in my workload | 2.80 | 1.35 | 1–5 |
| The support services provide necessary support for a timely diagnosis | 2.69 | 1.30 | 1–5 |
| I consider my wage adequate/compatible with my demand/risks at work | 2.63 | 1.28 | 1–5 |
| I take part in decisions about patient care flow | 2.59 | 1.40 | 1–5 |
| I feel overloaded and tired | 2.47 | 1.11 | 1–5 |
| I am aware of or took part in the discussions on the contingency plan adopted by the institution where I work | 2.47 | 1.34 | 1–5 |
| I participated or was consulted about changes and definitions of workflows, routine, and standardizations | 2.39 | 1.29 | 1–5 |
| I am afraid of being infected | 1.83 | 1.21 | 1–5 |
| General | 3.02 | 0.63 | 1.83–4.23 |
SD, Standard Deviation.
Min.–max.
Qualitative arm
Five main themes were developed from the valid answers about the challenges faced by nurses in their work environment during the COVID‐19 pandemic. Theme 1 was ‘Feeling of insecurity’, as it portrays the discomfort and stress resulting from the care provided to suspected patients or to those diagnosed with COVID‐19. Theme 2 is entitled ‘Lack of personal protective equipment’, as it highlights the insufficient quantity of these materials in the institution. Theme 3 received the title of ‘Lack of tests’, given the elements that refer to the unavailability of tests for health professionals and the population at large. Theme 4, ‘Changes in the care flow’, portrays the difficulty in adapting to the new care flows. In Theme 5, ‘Fear of the unknown’, the testimonies of the participants express the fear of providing care in the face of a disease that is still little known and the challenge of managing emotions in the workplace. Figure 1 presents examples on excerpts (direct quotations) from participants answers to support the themes.
Figure 1.
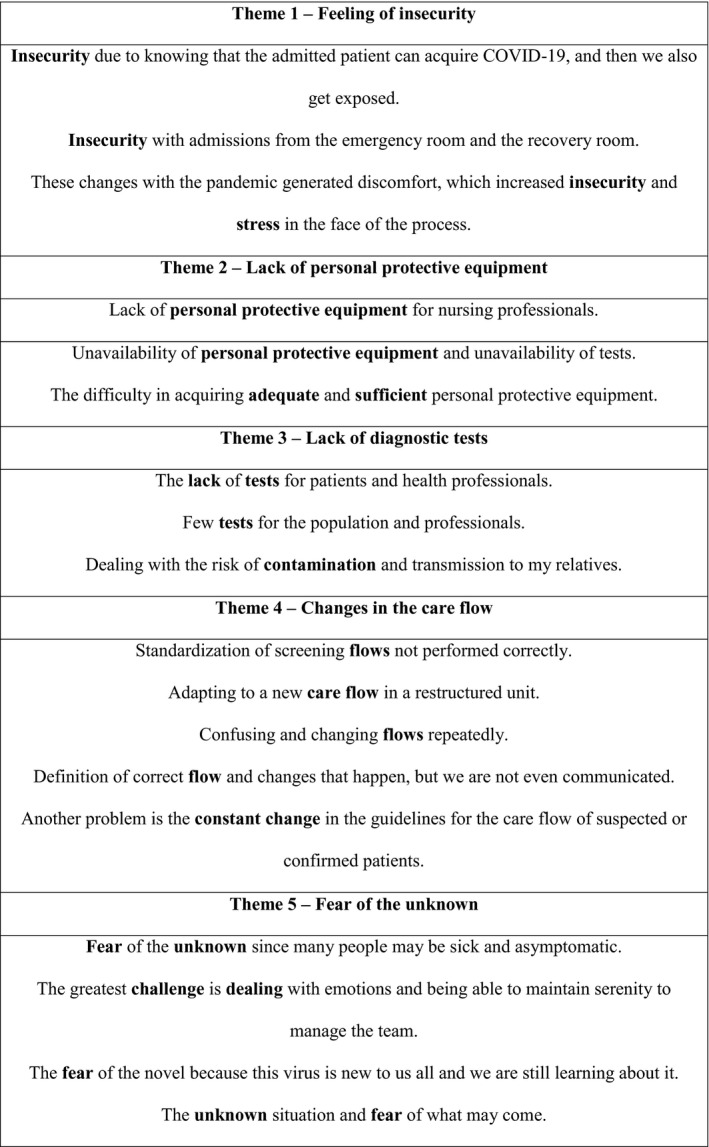
Representative quotations from participants answers to each theme.
Quantitative and qualitative combination
The combination of the quantitative (QUANT) and qualitative (qual) approaches by incorporation allows for the identification of convergences and divergences among the findings of the study. Some main examples are presented below.
The ‘I am afraid of being infected’ item (1.83 ± 1.21) has the worst evaluation, confirming Themes 1, 2, 3 and 5 from the qualitative results. This shows the insecurity of the nurses and fear in the care of patients with a suspected or confirmed diagnosis of COVID‐19.
Despite the ‘I have access to sufficient personal protective equipment to protect me’ item being among the five items with the best evaluation (3.40 ± 1.25), Theme 2 indicates lack of personal protective equipment. This divergence can be related to the differences among institutions and even to the variability and dynamics of access to these supplies in the care context, especially in a time of constant demand.
The evaluation of the ‘I participated or was consulted about changes and definitions of workflows, routine and standardizations’ item (2.39 ± 1.29) helps to understand the citation of changes in the care flow as a challenge for nurses in Theme 4.
There is convergence between the ‘The support services provide necessary support for a timely diagnosis’ item and the qualitative results (Themes 1, 3 and 5). It was one of the worst evaluated items, and the respondents stated that there is lack of tests for patients and professionals, which increases the risk of contamination, as well as the feelings of insecurity and fear.
Discussion
As far as it is known, this is the first study on the work environment of hospital nurses during the COVID‐19 pandemic in Brazil. The main favourable aspects were the provision of qualification courses on PPE and COVID‐19 and the existence of teamwork. Among the unfavourable aspects, the fear of being infected and the little participation in decisions about the care flow stood out, as well as the lack of tests by the support services to diagnose the disease among professionals and patients.
Although they received training on the use of PPE, the distress of the professionals is related to the unavailability or low quality of these materials. A study with 103 health professionals working in a hospital in Wuhan, who were infected by the virus, found that 87 considered having acquired the virus while performing their duties, with 43 of these workers attributing contamination due to the lack of PPE, or even due to the low quality of those devices (Jin et al. 2020). The highest viral load of SARS‐CoV‐2 is present in sputum and in the secretions of the upper airways; it is extremely necessary to provide PPE of sufficient quality to ensure the protection of professionals on the front lines of the battle against the disease (Cook 2019). According to the findings of another study in European countries, 64.5% of the nurses suffered from protective equipment shortages (Danielis et al. 2020).
The increase in demand and the consequent lack of PPE can lead health managers to discuss the rational use and possible reuse of these materials. However, this practice is questionable since, during the disinfection process, changes in the material can occur, thus reducing its effectiveness and putting the professional at risk. In Italy, one of the most affected countries by the COVID‐19 pandemic, the Italian Association of Industrial Hygienists, has made a caveat that, if there is proof of the effectiveness of disinfection, the material can be reused strictly in emergency situations and never on a routine basis (Spinazzè et al. 2020).
These unprecedented working conditions have expanded the sources of emotional suffering experienced by the professionals, since they place them in situations of ethical and moral dilemma. By providing care to the patient without appropriate precautions, they put at risk not only their lives, but that of the other patients under their care, as well as that of their co‐workers and loved ones; while refusing to provide care, they run the risk of becoming criminally responsible for this action, despite being backed by class councils (Brazilian Federal Nurses Council 2020).
Another item that obtained a good evaluation was the existence of standardization of operational rules and procedures. Nevertheless, although the participants highlight the importance of these standardization processes, they reiterate that the constant change in these flows and the fact that they do not take part in these decisions negatively interfere in their work environment.
Considering that COVID‐19 is a new virus, as science advances and makes discoveries, changes in operational standards and protocols are necessary to offer better care to patients and to ensure the protection of the professionals. In this sense, the nurses indicated little participation in the discussions about changes in workflows and in the contingency plan adopted by the institution to fight against COVID‐19. This can be related to the speed of dissemination of the new coronavirus, which required a rapid response from these hospitals, contributing to the centralization of decision‐making in the institutional managers. However, open communication and dialogical leadership in times of crisis are important to direct the healthcare actions and keep them motivated (Moura 2019; Stoller 2020).
In the quantitative results, teamwork and collaborative practice with health professionals was well evaluated by the nurses. Nursing teamwork is a key instrument in the professional practice, as it is the most appropriate way to obtain satisfactory results; and, in order to sustain it effectively, we need the cooperation of all those involved in the process (Goh et al. 2020).
In a period of crisis in public health, as currently experienced, health professionals end up having to work longer and with greater overload, which generates great physical and psychological stress. In this sense, it is important that they are and feel supported. Clear leadership guidelines and collaborative teamwork entail favourable working conditions, in addition to reducing tensions due to the situation (Gan et al. 2020). Managing information and ensuring that everybody was always ‘on the same page’ in the rapidly changing environment was a critical factor during the COVID‐19 pandemic (Magro et al. 2020).
A previous study highlights that teamwork, companionship and help from professional colleagues in daily activities can influence the perception of nursing professionals about the workload, mitigating the difficulties of the work environment (Feldhaus 2019). Thus, it is possible to consider that the work context to which the professionals are exposed mobilizes them to develop a collaborative practice and to cultivate a collective spirit of mutual help.
The item with the worst evaluation was ‘I am afraid of being infected’. This result is linked with the following themes: ‘Feeling of insecurity’ and ‘Fear of the unknown’.
The perception of fear was one of the main converged findings from the quantitative and qualitative data combination. As the majority of nurses indicated that they had received training on COVID‐19, it can be inferred that their fear is not related to lack of training, but to insecurity in the face of a disease that has been proved to be potentially fatal and represents the most important public health problem worldwide in the last 100 years. This feeling is also worsened by the lack of medications and vaccines capable of helping to combat COVID‐19 (Medeiros 2020).
Another item that has been shown to negatively interfere in the nurses work environment refers to the lack of diagnostic tests for professionals and patients. The accomplishment of tests to identify individuals infected with SARS‐CoV‐2 is essential to help control the pandemic. In some countries, large‐scale testing has been at the heart of successful strategies to halt the spread of the virus. In others, due to the limited availability of tests, because of the scarcity of financial resources or logistic difficulties in transportation, priority was given to individuals in risk groups (Cheng et al. 2020). This highlights the importance of planning future strategies focused on using technology more smartly to deliver health and nursing care, prudent use of scarce resources, triaging of large numbers of patients and the way in which patients, their friends and relatives interact with the nurses (Rosa et al. 2020).
In Singapore, an engineering model was used to evaluate the behaviours necessary to minimize the risk of intra‐hospital dissemination, aiming to protect health professionals against occupational infection by COVID‐19. Among the measures of organizational scope, segregation was used among the professionals who care for suspected or confirmed COVID‐19 patients and those who manage other patients. The objective of this action was to avoid cross‐transmission and to segment tasks according to risk (Gan et al. 2020). Considering the worldwide scarcity of supplies for mass testing of patients and workers, the more precautionary measures are taken, the lower the risk of contagion among professionals and patients.
Limitation of the study
This study comes with several limitations. Firstly, convenience sampling was used to present partial results from a major multicentric project. Secondly, online data collection makes it difficult to control samples and populations, since anyone can complete the questionnaire and there is a greater possibility of people interested in the subject to bias sample composition. Finally, it is necessary to consider that the study was developed at the beginning of the COVID‐19 pandemic in Brazil. Despite these limitations, the findings of this study are vital in serving as baseline knowledge.
Conclusion
This study has enabled us to identify the repercussions of the COVID‐19 pandemic in the work environment of nurses in Brazilian university hospitals. The accomplishment of qualification courses on PPE and COVID‐19 and the existence of teamwork were the main favourable aspects found. Among the unfavourable aspects, we can highlight fear of being infected, limited participation in decisions regarding care flows and lack of tests to diagnose the disease among professionals and patients.
Implications for Nursing and Nursing Policy
This study conducted in three Brazilian university hospitals presents the nurses' perceptions of their work environment taking care of patients during the COVID‐19 pandemic. The findings of this study have several implications for nursing research and health policy for improvement of the Nursing working conditions.
The gaps identified will assist policymakers and hospital managers in developing policies to enhance the support offered to nurses and improve the care provided to patients with COVID‐19 in university hospitals. In view of the setting found, it is proposed to return the results to Nursing management and to the continuing education service of the hospitals addressed in the study as a way of evaluating the actions developed to deal with the COVID‐19 pandemic. The research findings may support the discussion and planning of improvement opportunities for the continuation of the fight against this pandemic. Furthermore, the research also encourages the development of new studies, mainly in other Brazilian settings, to analyse how the COVID‐19 pandemic has impacted on the work environment of nurses in the hospital context.
The results also indicated the need for attention to the mental health of the professionals due to the increasing workload and the treatment of an illness hitherto unknown. Health work in normal situations is emotionally distressing. In a situation like the current one, demands related to mental health have increased considerably. Routinely, the nursing work includes situations of stress, anxiety and even depression, which are directly related to frustration, physical and mental exhaustion, feelings of helplessness and professional insecurity experienced during the pandemic, mainly by young professionals with no experience in the care of critically‐ill patients.
Author contributions
JLGS, SC and APB designed the study
JLGS, APB, IA, DDL and SC collected the data
JLGS, FHA, EO and JAL analysed the data
JLGS, SC, APB and ALE supervised the study
JLGS, AP, FHA, IA, DDL, JAL, ALE and SC involved in manuscript writing
JLGS, AP, FHA, IA, DDL, JAL, ALE and SC involved in critical revisions for important intellectual content.
Santos J.L.G.d., Balsanelli A.P., Freitas E.d.O., Menegon F.H.A., Carneiro I.A., Lazzari D.D., Menezes J.A.L.D., Erdmann A.L.& Camponogara S. (2021) Work environment of hospital nurses during the COVID‐19 pandemic in Brazil. Int. Nurs. Rev. 68, 228–237
Conflict of interest: The study has no conflict of interest.
Sources of funding: The present work was carried out with the support of the Coordination for the Improvement of Higher Level – Brazil (CAPES) with financing code 001 and also by the National Council for Scientific and Technological Development (CNPQ) under case number 402392/2020‐5.
References
- Bitencourt, J.V.O.V. , et al. (2020) Nurse's protagonism in structuring and managing a specific unit for COVID‐19. Texto & Contexto Enfermagem, 29, e20200213. 10.1590/1980-265x-tce-2020-0213. [DOI] [Google Scholar]
- Brazilian Federal Council of Nursing . (2020) Brazil accounts for 30% of deaths of nursing professionals by covid‐19. (in Portuguese). Available at: http://biblioteca.cofen.gov.br/wp‐content/uploads/2019/11/C%C3%B3digo‐de‐%C3%89tica‐dos‐profssionais‐de‐Enfermagem.pdf (accessed 20 July 2020). [Google Scholar]
- Center for Systems Science and Engineering of Johns Hopkins University (2020) Modeling the spread of 2019‐nCoV. Available at: https://systems.jhu.edu/wp‐content/uploads/2020/01/Gardner‐JHU_nCoV‐Modeling‐Report_Jan‐26.pdf accessed 05 December 2020. [Google Scholar]
- Cheng, M.P. , et al. (2020) Diagnostic testing for severe acute respiratory syndrome‐related coronavirus 2: a narrative review. Annals of Internal Medicine, 172 (11), 726–34. 10.7326/M20-1301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cook, T.M. (2019) Personal protective equipment during the coronavirus disease (COVID) 2019 pandemic – a narrative review. Anaesthesia, 75, 920–927. 10.1111/anae.15071. [DOI] [PubMed] [Google Scholar]
- Creswell, J.W. & Plano Clark, V.L. (2013) Pesquisa de métodos mistos. Penso, Porto Alegre. [Google Scholar]
- Danielis, M. , Palese, A. , Terzoni, S. & Destrebecq, A.L.L. (2020) How hospitals, Intensive Care Units and nursing care of critically ill patients have changed during the Covid‐19 outbreak? Results from an exploratory research in some European countries. Assistenza infermieristica e ricerca, 39 (3), 130‐138 10.1702/3454.34430. [DOI] [PubMed] [Google Scholar]
- Feldhaus, C. , et al. (2019) Association between workload and absenteeism in nursing technicians. Texto & Contexto Enfermagem, 28, e20180307. 10.1590/1980-265x-tce-2018-0307. [DOI] [Google Scholar]
- Gan, W.H. , Lim, J.W. & Koh, D. (2020) Preventing intra‐hospital infection and transmission of coronavirus disease 2019 in health‐care workers. Safety and Health at Work, 11 (2), 241–243. 10.1016/j.shaw.2020.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gasparino, R.C. & Guirardello, E.B. (2017) Validation of the Practice Environment Scale to the Brazilian culture. Journal of Nursing Management, 25 (5), 375–383. 10.1111/jonm.12475. [DOI] [PubMed] [Google Scholar]
- Goh, P.Q.L. , et al. (2020) Nursing teamwork in general ward settings: A mixed‐methods exploratory study among enrolled and registered nurses. Journal of Clinical Nursing, 29, 3802–3811. 10.1111/jocn.15410. [DOI] [PubMed] [Google Scholar]
- Graneheim, U.H. & Lundman, B. (2004) Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthines. Journal of the Nurse Education Today, 24 (2), 105–112. 10.1016/j.nedt.2003.10.001. [DOI] [PubMed] [Google Scholar]
- Honey, M. & Wang, W. (2013) New Zealand nurses perceptions of caring for patients with influenza A (H1N1). Nursing Critical Care, 18 (2), 63–69. 10.1111/j.1478-5153.2012.00520.x. [DOI] [PubMed] [Google Scholar]
- Hong, Q.N. , et al. (2019) Improving the content validity of the mixed methods appraisal tool: a modified e‐Delphi study. Journal of Clinical Epidemiology, 111, 49–59. 10.1002/nur.21976 [DOI] [PubMed] [Google Scholar]
- Huang, L.H. , Chen, C.M. , Chen, S.F. & Wang, H.H. (2020) Roles of nurses and National Nurses Associations in combating COVID‐19: Taiwan experience. International Nursing Review, 67 (3), 318–322. 10.1111/inr.12609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hutchinson, M.K. & Sutherland, M.A. (2019) Conducting surveys with multidisciplinary health care providers: Current challenges and creative approaches to sampling, recruitment, and data collection. Research in Nursing & Health, 42 (6), 458–466. 10.1002/nur.21976. [DOI] [PubMed] [Google Scholar]
- International Council of Nurses (2020) More than 600 nurses die from COVID‐19 worldwide. Available at: https://www.icn.ch/news/more‐600‐nurses‐die‐covid‐19‐worldwide accessed 5 June 2020. [Google Scholar]
- Jin, Y. , et al. (2020) Perceived infection transmission routes, infection control practices, psychosocial changes, and management of COVID‐19 infected healthcare workers in a tertiary acute care hospital in Wuhan: a cross‐sectional survey. Military Medical Research, 7 (24), 1–13. 10.1186/s40779-020-00254-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lake, E.T. (2002) Development of the practice environment scale of the Nursing Work Index. Journal of Nursing Management, 25 (5), 375–383. 10.1002/nur.10032. [DOI] [PubMed] [Google Scholar]
- Lake, E.T. , et al. (2019) A meta‐analysis of the associations between the nurse work environment in hospitals and 4 sets of outcomes. Medical Care, 57 (5), 353–361. 10.1097/MLR.0000000000001109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li, B. , Li, Z. & Wan, Q. (2019) Effects of work practice environment, work engagement and work pressure on turnover intention among community health nurses: mediated moderation model. Journal of Advanced Nursing, 75, 3485–3494. 10.1111/jan.14130. [DOI] [PubMed] [Google Scholar]
- Machado, M.H. , et al. (2016) Características gerais da Enfermagem: o perfil sócio demográfico (in Portuguese). Enfermagem Em Foco, 7, 1–6. 10.21675/2357-707X.2016.v7.nESP.686. [DOI] [Google Scholar]
- Magro, F. , et al. (2020) Managing a tertiary orthopedic hospital during the COVID‐19 epidemic, main challenges and solutions adopted. International Journal of Environmental Research and Public Health, 17 (13), 4818. 10.3390/ijerph17134818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Medeiros, E.A.S. (2020) Health professionals fight against COVID‐19. Acta paulista Enfermagem, 33, e‐EDT20200003. [Google Scholar]
- Menon, V. & Muraleedharan, A. (2020) Internet‐based surveys: relevance, methodological considerations and troubleshooting strategies. General Psychiatry, 33 (5), e100264. 10.1136/gpsych-2020-100264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moura, A.A. , et al. (2019) Charismatic leadership among nursing professionals: an integrative review. Revista Brasileira de Enfermagem, 72 (Suppl 1), 315–320. 10.1590/0034-7167-2017-0743. [DOI] [PubMed] [Google Scholar]
- Nelson‐Brantley, H.V. , Park, S.H. & Bergquist, S. (2018) Characteristics of the nursing practice environment associated with lower unit‐level RN turnover. Journal of Nursing Adminstration, 48 (1), 31–37. 10.1097/NNA.0000000000000567. [DOI] [PubMed] [Google Scholar]
- Nulty, D.D. (2008) The adequacy of response rates to online and paper surveys: what can be done? Assessment & Evaluation in Higher Education, 33 (3), 301–314. 10.1080/02602930701293231. [DOI] [Google Scholar]
- Ozer, O. , Santas, F. , Santas, G. & Sahin, D.S.S. (2017) Impact of nurses' perceptions of work environment and communication satisfaction on their intention to quit. International Journal of Nursing Practice, 23, e12596. 10.1111/ijn.12596. [DOI] [PubMed] [Google Scholar]
- Rodriguez‐Morales, A.J. , et al. (2020) COVID‐19 in Latin America: The implications of the first confirmed case in Brazil. Travel Medicine and Infectious Disease, 35, 101613. 10.1016/j.tmaid.2020.101613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosa, W.E. , et al. (2020) Leveraging nurse practitioner capacities to achieve global health for all: COVID‐19 and beyond. International Nursing Review, 67 (4), 554–559. 10.1111/inr.12632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Santos, J.L.G. , et al. (2017) The nurse’s work environment in a hospital emergency service. Revista da Rede de Enfermagem do Nordeste, 18 (2), 195–203. 10.15253/2175-6783.2017000200008. [DOI] [Google Scholar]
- Souza, M.A.R. , et al. (2018). The use of IRAMUTEQ software for data analysis in qualitative research. Revista da Escola de Enfermagem da USP, 52, e03353. 10.1590/s1980-220x2017015003353. [DOI] [PubMed] [Google Scholar]
- Spinazzè, A. , Cattaneo, A. & Cavallo, D.M. (2020) COVID‐19 Outbreak in Italy: Protecting Worker Health and the Response of the Italian Industrial Hygienists Association. Annals of work exposures and health, 64 (6), 559–564. 10.1093/annweh/wxaa044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stoller, J.K. (2020) Reflections on leadership in the time of COVID‐19. BMJ Leader, 4, 77–79. 10.1136/leader-2020-000244. [DOI] [Google Scholar]
- Turale, S. , Meechamnan, C. & Kunaviktikul, W. (2020) Challenging times: Ethics, nursing and the COVID‐19 pandemic. International Nursing Review, 67 (3), 164–167. 10.1111/inr.12598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization . State of the World’s Nursing Report – 2020. https://www.who.int/publications/i/item/9789240003279 (accessed 20 July 2020). [Google Scholar]
- Wu, F. , et al. (2020) A new coronavirus associated with human respiratory disease in China. Nature, 579, 265–269. 10.1038/s41586-020-2008-3. [DOI] [PMC free article] [PubMed] [Google Scholar]