

To the Editor:
A 22‐year‐old healthy male with no medication use received the Pfizer‐BioNTech BNT16B2b2 mRNA vaccine through his work as an emergency department employee. On day three, post‐vaccination, he experienced widespread petechiae (Figure 1) and gum bleeding, which prompted his presentation. He was current on his vaccines, including yearly influenza, with no history of adverse reactions. He denied respiratory and gastrointestinal complaints or a history of infection. He had no personal or family history of bleeding or autoimmune disease. Vital signs and the remainder of his exam were normal. Laboratory tests revealed normal white‐cell count, hemoglobin, and severe thrombocytopenia with a platelet count of 2 × 109/L.
FIGURE 1.
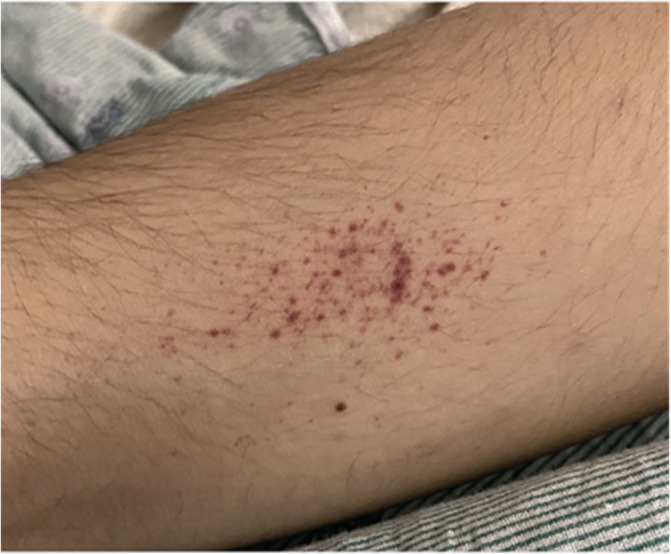
Purpuric lesions on the patient's upper extremity
Two months prior to receiving the vaccine, the patient was evaluated at an outpatient clinic for upper respiratory symptoms. His PCR assay returned negative for SARS‐CoV‐2, and complete blood count was unremarkable with a normal platelet count of 145 × 109/L (reference range, 140–400 × 109/L). The upper respiratory symptoms resolved within a few days, and the patient had no further complaints. However, as a precautionary measure, one‐week post outpatient evaluation, he was again tested for SARS‐CoV‐2, which returned negative.
At the emergency department on day 3, post‐vaccination, the following labs were normal or negative: prothrombin time, partial thromboplastin time, fibrinogen, BUN, creatine, electrolytes, bilirubin, LDH, alkaline phosphatase, albumin, globulin, total protein, and haptoglobin. The aspartate aminotransferase (42) and alanine aminotransferase (90) were mildly elevated; however, they normalized the next day. Additionally, he tested negative for HIV, Hepatitis B, Hepatitis C antibody, and Epstein–Barr Virus serology. A nasopharyngeal swab also returned negative for SARS‐CoV‐2 antigen. The patient was then admitted and given dexamethasone 40 mg daily for 4 days, a platelet transfusion, and intravenous immunoglobulin at 1 g/kg for 2 days. 1
Immunologic studies performed on day 6 for Rheumatoid factor, antibodies for Cyclic Citrullinated Peptide, Anti Centromere, Chromatin IgG, dsDNA, Jo1, Ribosomal P Protein, Ribonucleoprotein, Scleroderma, Smith, Sjogren's Syndrome B, Sm/Rnp IgG, Antinuclear Antibody (<1:80, normal <1:80) were normal. However, Sjogren's Syndrome A antibody (2.8) was elevated (normal <1 AI).
On day six, post‐vaccination, petechiae and oral bleeding decreased, and the patient was discharged with a platelet count of 28 × 109/L. Based on the presentation, a platelet count <100 × 109/L, and the exclusion of alternative causes, a diagnosis of ITP was made. 1
At follow up, on day 11, the patient's platelet count normalized to 173 × 109/L, and the patient tested positive for plasma IIb/IIIa and Ia/IIa platelet autoantibodies. Sjogren's Syndrome A antibody decreased from 2.8 on day 6 to 1.5 (normal <1 AI). Moreover, complement C3 (94) was normal (reference range, 79–152 mg/dL), while complement C4 (10.9 mg/dL) was low (reference range, 16–38 mg/dL).
Previous studies reported only mild or moderate adverse events following the Covid‐19 vaccine. 2 , 3 , 4 To our knowledge, outside of a report in the press, 5 , 6 this is the first case published in the medical literature of an individual, with no other cause identified and no associated illness, experiencing ITP after receiving the Pfizer‐BioNTech vaccine. The temporal relationship of the patient's presentation 3 days post‐vaccine administration suggests, but does not prove, the vaccine may be linked to the patient's ITP. Additionally, the rapid and severe drop in platelet count to 2 × 109/L is reminiscent of the abrupt onset observed in drug‐induced thrombocytopenia, which further suggests a recent etiology. 7
However, it must be noted that the incidence of ITP is about 3.3 per 100 000 adults/year. 8 Therefore, it is also plausible that this patient's diagnosis was purely coincidental, given that the United States has administered over 12 million vaccines to date. 9 Additionally, 43 448 participants were included in the Pfizer‐BioNTech trial, and no ITP was reported. 2 Moreover, considering the low complement C4 (10.9 mg/dL), mildly elevated SSA Ab (1.5), and 2 months prior, the platelet count (145 × 109/L) was near the lower limit, it is difficult to exclude alternative causes, such as an underlying autoimmune condition with pre‐existing ITP. In this scenario, the ITP became clinically apparent following the vaccine, though this patient never manifested symptoms suggestive of autoimmune disease.
This case was reported to the FDA's Vaccine Adverse Events Reporting System (VAERS) and is valuable both for post‐approval pharmacovigilance and as a foundation for clinicians to evaluate future patients with suspected ITP. Rare vaccination events are important, but do not diminish the enormous utility of vaccination and the well‐documented safety profile 2 of the Pfizer‐BioNTech BNT16B2b2 mRNA vaccine.
CONFLICT OF INTEREST
The authors report no conflict of interest.
DATA AVAILABILITY STATEMENT
Data sharing not applicable ‐ no new data generated
REFERENCES
- 1. Neunert C, Terrell DR, Arnold DM, et al. American Society of Hematology 2019 guidelines for immune thrombocytopenia. Blood Adv. 2019;3(23):3829‐3866. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Polack FP, Thomas SJ, Kitchin N, et al. Safety and efficacy of the BNT162b2 mRNA Covid‐19 vaccine. N Engl J Med. 2020;383:2603‐2615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Walsh EE, Frenck RW Jr, Falsey AR, et al. Safety and immunogenicity of two RNA‐based Covid‐19 vaccine candidates. N Engl J Med. 2020;383(25):2439‐2450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Jackson LA, Anderson EJ, Rouphael NG, et al. An mRNA vaccine against SARS‐CoV‐2 ‐ preliminary report. N Engl J Med. 2020;383(20):1920‐1931. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Grady D, Mazzei P. Doctor's death after Covid vaccine is being investigated. The New York Times . 2021. https://www.nytimes.com/2021/01/12/health/covid-vaccine-death.html.
- 6. Weintraub K. Death of Florida doctor after receiving COVID‐19 vaccine under investigation. USA Today .
- 7. George JN, Aster RH. Drug‐induced thrombocytopenia: pathogenesis, evaluation, and management. Hematology Am Soc Hematol Educ Prog. 2009;2009:153‐158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Terrell DR, Beebe LA, Vesely SK, et al. The incidence of immune thrombocytopenic purpura in children and adults: a critical review of published reports. Am J Hematol. 2010;85(3):174‐180. [DOI] [PubMed] [Google Scholar]
- 9. CDC . COVID‐19 vaccines. 2021. https://www.cdc.gov/coronavirus/2019-ncov/vaccines/index.html.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing not applicable ‐ no new data generated