

Abstract
The SARS‐CoV‐2 virus that causes COVID‐19 has had a large impact on the lives of many people worldwide. At the peak of confirmed COVID‐19 cases during the first wave in Switzerland (March–April 2020), we conducted a survey in the German‐speaking part of the country (N = 1,585). The results suggest that the implemented measures are accepted. The survey participants are more concerned that other family members could catch the virus compared with themselves, and they are worried about its economic impact. The results suggest that how trust is measured is crucial because general trust and social trust have opposite effects on the participants’ risk perceptions. People with high general trust perceive less risks associated with COVID‐19 compared with people who have low general trust, and people with high social trust perceive more risks compared with people who have low social trust. The results further indicate that perceived risks are important drivers for the acceptance of the government's implemented measures to control COVID‐19 and for more precautionary behavior (i.e., contact with fewer people and more hygienic behavior). Theoretical and practical implications of these findings are discussed.
Keywords: confidence, COVID‐19, hygienic behavior, risk perception, trust
1. INTRODUCTION
A pandemic is one of the major risks that modern societies face (Osterholm, 2005). This has been well known before the emergence of the severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) that causes COVID‐19. However, this virus has made it globally obvious how strongly a pandemic may not only directly influence people's health but also indirectly affect their economic situation and well‐being. Human behavior has a strong impact on how a pandemic develops; only if people show hygienic behavior, keep physical distance, or get vaccinated (when this option is available) can a pandemic be brought under control. Public compliance with health authorities’ recommendations is a key factor contributing to successful risk management in cases of pandemics. COVID‐19 provides an excellent opportunity to examine the factors that shape people's behavior and their acceptance of risk mitigation measures. Such knowledge may not only be important for the successful control of COVID‐19, but it may also be crucial for the prevention or at least the mitigation of future pandemics.
Experts believe that SARS‐CoV‐2 started infecting people in late 2019 in Wuhan, China; even in January 2020, there were only a few reported cases of people who had died due to COVID‐19 (Johns Hopkins University, https://coronavirus.jhu.edu/data/hubei-timeline). Therefore, given the novelty of the virus, not many papers about people's risk perceptions and possible behavior changes caused by COVID‐19 have been published to date. A recent survey conducted from mid‐March to mid‐April 2020 about people's risk perceptions in 10 countries has found relatively high concerns about COVID‐19 (Dryhurst et al., 2020). This study has also found that worldviews influence people's risk perceptions, whereas trust has a significant although only a small effect. However, trust was measured in a very unspecific way (e.g., trust in science), which may have been one reason for the small effect. Furthermore, it has been shown that perceived health concerns constitute a factor that positively influences the adoption of precautionary measures (Zanin, Gentile, Parisi, & Spasiano, 2020). Given the low number of published studies examining people's risk perceptions regarding COVID‐19 and its effects on their behavior, we have to rely on studies examining people's reactions to other pandemics, such as H1N1 or Ebola, both of which affected considerably fewer people compared with COVID‐19.
Trust has been repeatedly proposed as an important factor contributing to public compliance during a pandemic and has been reported to influence people's perceived risks of a pandemic (Condon & Sinha, 2010; Liao, Cowling, Lam, Ng, & Fielding, 2010; Podlesek, Roskar, & Komidar, 2011; Prati, Pietrantoni, & Zani, 2011b; Siegrist & Zingg, 2014). Nonetheless, different types of trust should be distinguished (Siegrist, in press), and it seems plausible that not all types of trust have the same impact on how people perceive and react to a pandemic. Even though trust is often perceived as necessary for successful risk management, some types of trust may be a barrier to the appropriate behavior. For example, it has been argued that trust in the government may even result in a decreased risk perception and lower compliance with risk management measures (Wong & Jensen, 2020). In the present study, we focus on the impacts of general trust, general confidence, and social trust (see Siegrist, in press) on people's perceptions and behaviors.
General trust is the belief that most people are trustworthy most of the time, and it is related to how much someone trusts people whom one meets for the first time (Siegrist, Gutscher, & Earle, 2005; Smith & Mayer, 2018). General trust has been found to be negatively correlated with risk perceptions across a broad range of hazards (Siegrist, Gutscher et al., 2005). People who tend to unconditionally trust others (with whom they have not interacted) perceive fewer risks associated with a number of technological and societal hazards compared with people who show a low level of general trust. General trust has also been found to have a positive influence on cooperation (Yamagishi & Cook, 1993). In a pandemic, all the other people are potential carriers of the virus; therefore, a person should generally perceive other people as posing threats to one's health. We thus assume that people with high levels of general trust perceive less risks and consequently show less risk reduction behavior compared with people who have low levels of general trust.
While general trust is related to a generalized individual (i.e., a stranger) to be relied on, general confidence refers to a generalized object (Keller, Siegrist, Earle, & Gutscher, 2011). General confidence is the belief that most future events will occur as expected and that uncertainty is low. In other words, it is a positive expectation of the future. People with high levels of general confidence perceive fewer risks associated with a number of technological and societal hazards compared with people who have low levels of general confidence (Siegrist, Gutscher et al., 2005). We therefore assume that people with high levels of general confidence perceive less risks compared with people who have low levels of general confidence.
If people lack the necessary knowledge to evaluate the risk of a hazard, trust becomes an important cue regarding whom to believe (Siegrist & Cvetkovich, 2000; Siegrist & Zingg, 2014). People need to rely on experts, government agencies, or other sources to interpret the information. Social trust might be an important factor contributing to people's acceptance of the precautionary measures needed to wipe out a pandemic (Siegrist & Zingg, 2014). An Italian study has shown that people who trust the health ministry, as well as the media, are more likely to adopt the recommended behavior in order to control the H1N1 influenza compared with people who lack trust in the health ministry and the media (Prati, Pietrantoni, & Zani, 2011a). Trust in the government (Quinn et al., 2011; van der Weerd, Timmermans, Beaujean, Oudhoff, & van Steenbergen, 2011) and in medical organizations (Gilles et al., 2011) has also been found to influence people's willingness to be vaccinated against the H1N1 influenza. In the case of COVID‐19, social trust implies people's belief that the information provided by the government is not biased and that there are no conspiracies masterminded by the pharmaceutical industry or politicians.
The affective meaning evoked by a hazard may influence people's risk and benefit perceptions (Finucane, Alhakami, Slovic, & Johnson, 2000), a phenomenon labeled as affect heuristic. The imagery technique has been used to measure people's affect (Slovic, Finucane, Peters, & MacGregor, 2007). In this method, a word or a sentence is presented to participants, who have to provide the first thought or image that comes to their minds. After the elicitation of the associations, participants rate them on a scale ranging from negative to positive. This technique has been employed to measure people's affect related to nuclear power (Keller, Visschers, & Siegrist, 2012; Peters & Slovic, 1996) or gene technology (Connor & Siegrist, 2011). These studies’ results suggest that the valence of the spontaneous associations is linked to people's risk perceptions and acceptance of a technology. The importance of affect for the perceived risk of a pandemic has been shown by an Italian study (Prati & Pietrantoni, 2016), in which the affect evoked by Ebola is correlated with the perceived severity of an illness and the likelihood of an infection. The outbreak of COVID‐19 in several regions in Northern Italy and the healthcare system's near collapse in those locations were frequently in the news in Switzerland. Therefore, we expect people's affect, evoked by COVID‐19, to have an impact on the level of their perceived risk.
A study examining the perception on Ebola in the United States suggests that politically conservative respondents express significantly less support for public health policies managing the Ebola risk compared with liberal respondents (Fischhoff, Wong‐Parodi, Garfin, Holman, & Silver, 2018). Risk management options aiming to reduce the number of people suffering from COVID‐19 always have some undesired negative economic consequences. We assume that people who are more concerned about health and less worried about the economic consequences of COVID‐19 have greater support of government measures aiming to reduce the infection rate and more often show the recommended behavior changes compared with people who are more concerned about economic outcomes and less anxious about health consequences. This does not imply that people cannot perceive both economic and health values as equally important. However, in the short term, risk management has to give more weight to either economic values (e.g., no lockdown) or health values (e.g., lockdown). In this state of uncertainty, it remains unclear whether a stronger weight on either economic or health values is better for the economy or public health, respectively, in the long term. We focus on economic and health values because they are frequently discussed when evaluating or justifying risk management strategies for fighting COVID‐19.
Many countries have experienced rapid changes in the number of infected people in a very short time (Johns Hopkins University, https://coronavirus.jhu.edu). For the present study, we collected data in Switzerland. Therefore, the country's situation during the data collection is crucial for the interpretation of the results. In Switzerland, the first wave of the pandemic peaked on March 23, 2020, with 1,321 people having new positive test results. The Federal Council put some special measures into place on March 16, 2020 (e.g., closure of restaurants, shops—except grocery stores and drugstores—and universities and schools; reduced public transportation; encouragement to work from home; urgent calls to stay home and keep physical distance from other people). The data for our study were collected between March 27 and April 5, 2020, when all these measures aiming to reduce the number of infected people were already in place.
In this study, we aimed to examine how general trust, general confidence, social trust, affect, and values (i.e., economic vs. health values) would influence people's fears associated with COVID‐19. Furthermore, we investigated how these factors would influence people's acceptance of the implemented measures to control the pandemic in Switzerland, their self‐reported hygienic behavior, and the recommended behavior related to avoiding or minimizing contact with other persons. Regarding trust, we hypothesized that general trust and general confidence would be negatively correlated with people's risk perceptions, whereas social trust would have the opposite outcome. The case of people having more negative affect associated with COVID‐19 was expected to result in higher health‐ and economic‐related risk perceptions compared with the case of people having less negative affect. Sociodemographic variables tend to be only weakly correlated with risk perceptions (Siegrist & Arvai, 2020). Considering age, a risk factor, we predicted that age and belonging to a risk group would be positively correlated with perceived health risks, but no association was expected for economic fears. Sex was included as a control variable.
Regarding acceptance of the measures and adoption of the recommended behavior, people who were convinced that the economic and the social aspects of the prevention measures were not sufficiently taken into account were expected to show lower acceptance compared with people who focused more on the health aspects. We further predicted that perceived health risks would be positively associated, and perceived economic risks would be negatively associated with the acceptance of the measures and adoption of the recommended behavior. Concerning trust, we expected people with higher levels of social trust to show more acceptance of the measures/higher adoption of the recommended behavior, while people with higher levels of general trust and general confidence would show less acceptance of the measures/lower adoption of the recommended behavior in comparison to people with low levels of these constructs. Finally, because older people are more at risk, we expected age to be positively correlated with the acceptance of the measures/adoption of the recommended behavior.
2. METHOD
2.1. Participants
The data for this study were collected in the German‐speaking part of Switzerland during end of March and beginning of April 2020, with the support of a professional provider of consumer panels (respondi; Koeln, Germany). The participants were incentivized for responding to the survey. Quota sampling was applied to ensure appropriate sex and age balance in the sample, with five equally distributed age groups (between 20 and 70 years) and equal sex distribution.
A total of 1,654 participants completed the survey. The participants who finished the survey in less than half the median completion time (n = 69; median = 15.6 minutes) were excluded from the analyses because they likely did not fill out the questionnaire conscientiously. The final sample comprised 1,585 participants (50.9% females), between 20 and 70 years old. Of the participants, 39% (n = 614), 51% (n = 817), and 10% (n = 154) belonged to the 20−39, 40−64, and 65−70 age groups, respectively. According to most recent Swiss census data, inhabitants aged 20 years or older are distributed as follows: 33% in the 20−39 age group, 44% in the 40−64 age group, and 23% in the 65 and older age group. Older people are underrepresented in our sample, which was restricted to people who were 70 years old and under (Federal Statistical Office, 2020b). The reason for this is the fact that respondi only allows people in the 20−70 age range to participate in its consumer panels. Regarding the level of education, 5% (n = 72) of the participants had attained the lowest level (i.e., obligatory schools), 61% (n = 968) had reached the middle level (i.e., apprenticeship, college, or higher vocational training), and 34% (n = 545) had obtained the highest level. These data are similar to the Swiss census data, with 11%, 59%, and 30% having attained the lowest, middle, and highest levels of education, respectively (Federal Statistical Office, 2020a).
2.2. Questionnaire
At the start of the questionnaire, the participants were asked whether they had heard of the coronavirus prior to that survey. All participants were then introduced to the topic with this short background information, adapted from the German COVID‐19 Snapshot Monitoring (COSMO Germany)1: “Worldwide, there is an outbreak of respiratory diseases caused by the new coronavirus. This virus was first discovered in Wuhan, Hubei province in China, and has since spread worldwide. There are thousands of confirmed cases and many deaths associated with the new coronavirus, also in Switzerland.” After this introduction, the participants filled out the questionnaire, which covered different topics related to COVID‐19, using various scales. In the following subsections, we focus on the items relevant to this study.
2.2.1. Sociodemographics
The participants were asked various questions regarding their sociodemographic information, such as age, sex, income, education, and canton of residence.
Various illnesses and treatments have been found to increase vulnerability to COVID‐19 (i.e., high blood pressure, diabetes, cardiovascular diseases, chronic respiratory diseases, illnesses/therapies that weaken the immune system, and cancer). The participants were asked to indicate whether they had any preexisting health conditions. For this item, they were provided with a list of health conditions (e.g., high blood pressure, diabetes type II, cancer) that were associated with severe progressions of COVID‐19 and were asked to check each health condition that applied to them (Federal Office of Public Health, 2020). We calculated the objective risk group variable with the value of 1 (n = 399, 25%) if a person had one of these illnesses or was pregnant;2 otherwise, it was calculated with the value of 0 (n = 1,186, 75%).
The participants were also asked, “Do you belong to a risk group; in other words, do you think that you are especially at risk in regard to the coronavirus?” The response options were “yes, definitely,” “yes, somewhat,” “no, somewhat not,” and “no, not at all.” A strong association between this subjective risk group variable and the objective risk group variable was observed (γ = 0.84, p < 0.001). Due to the high association between the two measures, the objective risk group variable was used in subsequent analyses.
We asked the participants whether they had been infected with the coronavirus. Only 4 (0.3%) respondents had a medical confirmation of an infection, and 66 respondents (4.2%) indicated that they had experienced the typical symptoms but had no medical confirmation of an infection.
2.2.2. Negative Affect
The participants were asked to indicate two associations—images or thoughts that came to their minds when thinking about the coronavirus. Very different associations were mentioned (e.g., China, Italy, illness, death, pandemic or fear were frequently mentioned). The participants had then to indicate the affect linked to each association using a slider with 11 possible response options, ranging from “very negative affect” (1), “neutral affect” (6) to “very positive affect” (11). The variable was recoded so that higher values indicated more negative affect compared with smaller numbers. For the subsequent analyses, only the affect with the first association was used (M = 8.10, SD = 2.66) because not all participants provided a second association.
2.2.3. Behavior
Several protective behavior items were developed based on the recommendations to increase hygiene measures and enforce social distancing (Federal Council, 2020; Federal Office of Public Health, 2020), leading to two behavioral indexes with protective measures (i.e., physical distancing and hygienic behavior). Six items measured physical contact at home or outside the home that people could control: “guests/neighbors/friends visiting my/our home,” “relatives visiting my/our home,” “cleaning aid at my/our home,” “a personal service provided in my/our home (e.g., hair cutting, cosmetic services, craft activities),” “walking in busy environments (e.g., city or village),” and “staying in larger groups (> five persons).” The participants had to answer these questions in the context of the past seven days, and the response options were “yes,” “no,” and “do not know.” “Yes” was coded as 1 and “no” or “do not know” as 0. A summative index was computed; a larger value would indicate that people spent time with others in more situations compared with a smaller value (M = 0.64, SD = 0.81). There is no reason to believe that these diverse behaviors should be substantially correlated; therefore, for this index number of situations with other people, no Cronbach's alpha is reported.
Seven items measured the participants’ hygienic behavior, as reflected in these practices: “avoidance of touching the face with unwashed hands,” “use of disinfectant for cleaning hands,” “use of disinfectant for cleaning surfaces,” “cleaning hands after touching the mail (letters, parcels),” “cleaning hands after receiving goods,” “washing or disinfecting foods and food packaging,” and “wearing a face mask.” The participants had to answer these questions in the context of the past seven days, and the response options were “yes,” “no,” and “do not know.” “Yes” was coded as 1 and “no” or “do not know” as 0. A scale of hygienic behavior was computed, and a larger value would indicate that people showed more hygienic behavior compared with a smaller value (M = 3.62, SD = 1.66). This scale's Cronbach's α = 0.59.
2.2.4. Risk of Being Infected Compared with Other People's Risk
We were interested in how likely the participants perceived the risk of being infected. We asked this question: “For the following question(s), please think of an average adult person in your community, and compare yourself with this person. Is it less or more likely that you will be infected with this virus compared with this person?” Out of the seven response options, only three were labeled: 1 as less likely, 4 as equally likely, and 7 as more likely.
2.2.5. Risk Perception
The five items that measured the participants’ health risk perceptions and the two items that measured their economic fears are shown in Table I. The participants could indicate the level of their perceived risk on a scale ranging from 1 (no fear) to 7 (very high fear). Only the two extreme points of the scale were also anchored descriptively; the other response categories were only anchored numerically. The health risk perception scale consisted of five items, and its Cronbach's α = 0.87. The mean score was computed (M = 4.33, SD = 1.43). The economic risk perception consisted of two items and had a Cronbach's α = 0.79. The mean score was 4.72 (SD = 1.62).
Table I.
Items Measuring Fears Related to Health and the Economy, Caused by SARS‐CoV‐2
| Related to the new coronavirus, I am afraid … | M | SD | |
|---|---|---|---|
| Health risk perception | … that I will be infected. | 3.47 | 1.75 |
| … that someone from my family or my acquaintances will be infected. | 4.58 | 1.78 | |
| … that there will be fatalities in my social environment. | 4.26 | 1.92 | |
| … that there will be many fatalities in Switzerland. | 4.38 | 1.70 | |
| … that the healthcare system will be overloaded. | 4.97 | 1.62 | |
| Economic risk perception | … of the personal consequences of an economic crisis in Switzerland (e.g., loss of job, short‐time work, falling wage). | 4.51 | 1.94 |
| … of the societal consequences of an economic crisis in Switzerland (e.g., high rate of unemployment, falling wages, falling stock market). | 4.94 | 1.61 |
Note: The possible responses ranged from 1 (no fear) to 7 (very high fear).
2.2.6. Social Trust
The basis of social trust is perceived value similarity (Siegrist, Cvetkovich, & Roth, 2000). We tend to trust organizations that have the same values that are salient to us in a specific situation (Earle & Siegrist, 2006). The following four items were used to measure the participants’ social trust or lack of social trust in the Swiss government and in the pharmaceutical industry, as related to COVID‐19: (1) “The government intentionally exaggerates the hazards associated with the coronavirus.” (2) “The coronavirus has been intentionally brought to people.” (3) “The pharmaceutical industry delays the development of drugs in order to make large profits afterwards.” (4) “We are not openly informed about the pandemic by the authorities; the numbers are fake.” The participants could indicate their agreement with the statements, using a scale ranging from 1 (do not agree at all) to 7 (completely agree). Only the two extreme points of the scale were also anchored descriptively; the other response categories were only anchored numerically. Because all four items were negatively formulated, they were recoded, and the mean was calculated. The scale's Cronbach's α = 0.81 (M = 5.12, SD = 1.52).
2.2.7. Tradeoffs
The measures that aim to reduce the health risks caused by SARS‐CoV‐2 have some undesirable side effects. The following three items measured whether the participants believed that tradeoffs were not sufficiently taken into account: (1) “The risks of the coronavirus are not sufficiently weighed against economic risks (e.g., economic damage caused by the measures against the virus).” (2) “The risks of the coronavirus are not sufficiently weighed against education‐related risks (e.g., pupils who academically lag behind due to closing of schools).” (3) “The risks of the coronavirus are not sufficiently weighed against social risks (e.g., increase of social conflicts at home due to restrictions in going outside).” The participants could indicate their agreement with the statements, using a scale ranging from 1 (do not agree at all) to 7 (completely agree). Only the two extreme points of the scale were also anchored descriptively; the other response categories were only anchored numerically. The scale's Cronbach's α = 0.89. The mean value across the items was used (M = 3.30, SD = 1.63). Higher values indicated the participants’ belief that tradeoffs were not sufficiently taken into account compared with lower values.
2.2.8. Acceptance Measures
When the data were collected, various measures that aimed to reduce the spread of the virus were already in place. The participants could indicate their level of agreement with the following statements about the measures taken in Switzerland, using a scale ranging from 1 (do not agree at all) to 7 (completely agree): (1) “In my view, it is justified that in Switzerland the schools have been closed.” (2) “… the restaurants and the bars have been closed.” (3) “… one is discouraged from leaving the house.” (4) “… all shops, with the exception of grocery shops and pharmacies, have been closed.” Only the two extreme points of the scale were also anchored descriptively; the other response categories were only anchored numerically. The four‐item scale's Cronbach's α = 0.88. The mean value was calculated for each participant (M = 5.74, SD = 1.42).
2.2.9. General Trust
For the measurement of general trust, a scale that was previously used for explaining people's risk perception was applied (Siegrist, Gutscher et al., 2005). This scale integrated various items from other studies (Glaeser, Laibson, Scheinkman, & Soutter, 2000; Rotter, 1967; Yamagishi, 1988). The following six items were used to measure general trust: (1) “If given the chance, most people would try to take advantage of you.” (2) “Most people are too busy looking out for themselves to be helpful.” (3) “You can't trust strangers anymore.” (4) “When dealing with strangers, one is better off using caution before trusting them.” (5) “Most people are basically honest.” (6) “Most people tell a lie when they can benefit from doing so.” The participants could indicate their agreement with the statements, using a scale ranging from 1 (do not agree at all) to 7 (completely agree). Only the two extreme points of the scale were also anchored descriptively; the other response categories were only anchored numerically. Items 1, 2, 3, 4, and 6 were recoded, so higher values expressed higher levels of trust, and lower values expressed lower levels of trust. The scale's Cronbach's α = 0.84. The mean across the six items was calculated (M = 3.79, SD = 1.18).
2.2.10. General Confidence
General confidence is a psychological buffer for coping with uncertainty (Keller et al., 2011). The following items from this study by Keller et al. (2011) were used to measure the construct: (1) “In the future, society will be functioning as well as today.” (2) “Our society is well equipped to solve future problems.” (3) “The future safety and security of our population are assured.” (4) “Our society has a bright future.” (5) “Nowadays, things seem to be getting more and more out of control.”3 The last item was recoded, so higher values expressed higher levels of confidence, and lower values expressed lower levels of confidence. The participants could indicate their agreement with the statements, using a scale ranging from 1 (do not agree at all) to 7 (completely agree). Only the two extreme points of the scale were also anchored descriptively; the other response categories were only anchored numerically. The scale's Cronbach's α = 0.82. The mean of the items was used for further analyses (M = 4.17, SD = 1.14).
3. RESULTS
3.1. Own risk compared with others’ risk
We were interested in how the participants perceived their own risk of being infected by SARS‐CoV‐2. They had to think about an average adult person in their community and indicate whether they perceived their likelihood of being infected as lower, equal, or higher compared with such a person. The responses to this question are shown in Fig. 1. Nearly half of the respondents (44.5%) perceived their own risk as equal to that of an average adult person. A similar number of participants (44.1%) perceived themselves as less likely to be infected than an average adult person, and only 11.4% perceived themselves as more likely to be infected.
Fig 1.
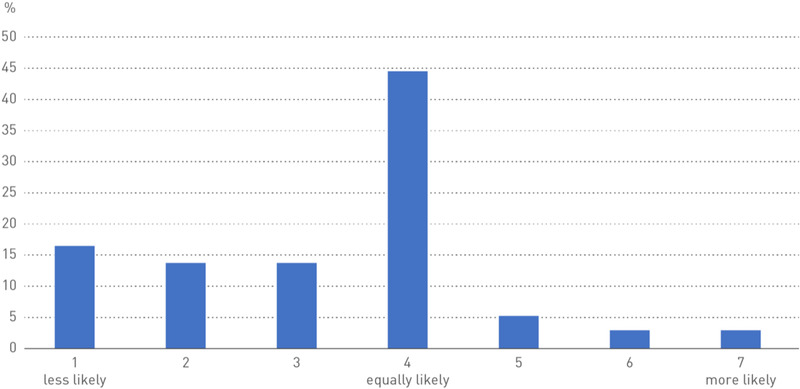
Responses (in percentages) to the question, “For the following question(s), please think of an average adult person in your community, and compare yourself with this person. Is it less or more likely that you will be infected with this virus compared with this person?”.
3.2. Correlations between constructs
Given the large sample size, a p‐value = 0.01 was used as the significance level. The correlations (as shown in Table II) indicated that people who accepted the measures implemented by the Swiss government demonstrated more hygienic behavior and had contact with fewer people compared with people who were against the measures. Furthermore, general confidence and general trust were negatively correlated with health and economic fears caused by COVID‐19. Finally, the variables (health risk perception, concerns that the wrong tradeoffs were made, social trust, and economic fears) that were expected to explain the acceptance of the government measures were substantially correlated with such acceptance.
Table II.
Correlations Between Self‐Reported Behavior, Acceptance of Implemented Measures, Different Types of Trust, Affect, and Risk Perceptions
| 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | 9. | |
|---|---|---|---|---|---|---|---|---|---|
| 1. Number of situations involving contact with other people | |||||||||
| 2. Hygienic behavior | −0.10** | ||||||||
| 3. Acceptance measures | −0.20** | 0.24** | |||||||
| 4. General confidence | −0.02 | 0.03 | 0.14** | ||||||
| 5. General trust | −0.04 | −0.06 | −0.03 | 0.33** | |||||
| 6. Social trust | −0.16** | 0.02 | 0.37** | 0.33** | 0.34** | ||||
| 7. Health risk perception | −0.13** | 0.24** | 0.48** | −0.10** | −0.20** | 0.09** | |||
| 8. Economic fears | −0.02 | 0.09* | 0.08* | −0.22** | −0.20** | −0.08* | 0.43** | ||
| 9. False tradeoffs | 0.13** | −0.05 | −0.44** | −0.28** | −0.24** | −0.63** | −0.09** | 0.20** | |
| 10. Negative affect | −0.01 | −0.02 | 0.07* | −0.08* | −0.03 | 0.01 | 0.20** | 0.13** | 0.00 |
Note: N = 1,585.
p < 0.01; **p < 0.001.
3.3. Perceived health and economic risks
As shown in Table I, on average, the participants were not too concerned about being infected; they were more concerned that someone else in the family would be infected. The highest levels of fear were related to an overload of the healthcare system and to the economic consequences.
Linear regression analyses were used to examine the predictors of perceived health risks and economic risks associated with SARS‐CoV‐2. The model for perceived health risks was significant, F(8,1576) = 29.66, p < 0.001, and explained 13% of the variance. The results are shown in Table III. Females perceived significantly more health risks compared with males, but age was not a significant predictor. The participants who belonged to a high‐risk group, had illnesses that had been found to increase the mortality risk, or were pregnant perceived significantly higher health risks compared with the participants who did not belong to a high‐risk group. General trust was negatively associated with perceived health risks. The participants who tended to trust other people perceived less health risks related to SARS‐CoV‐2 compared with the participants who were not inclined to trust other people. The participants who trusted the government and the pharmaceutical industry in regard to SARS‐CoV‐2 perceived more risks compared with the participants who had low levels of social trust. Finally, the negative affect linked to the association that spontaneously came to people's minds when asked to think about the coronavirus was significantly related to perceived health risks. More negative associations resulted in a higher level of perceived risks compared with less negative associations.
Table III.
Results of a Linear Regression Analysis with Perceived Health Risk and Economic Fears as Dependent Variables
| Perceived Health Risk | Perceived Economic Fears | |||||||
|---|---|---|---|---|---|---|---|---|
| B | SE | Beta 3 | t | B | SE | Beta 3 | t | |
| Constant | 4.50 | 0.29 | 15.67** | 3.73 | 0.33 | 11.35** | ||
| Sex 1 | 0.28 | 0.07 | 0.10 | 4.13** | 0.26 | 0.08 | 0.08 | 3.31* |
| Age | −0.01 | 0.003 | −0.05 | −2.09 | 0.01 | 0.03 | 0.07 | 2.71* |
| Risk group 2 | 0.34 | 0.08 | 0.10 | 4.17** | 0.08 | 0.09 | 0.02 | 0.82 |
| General confidence | −0.08 | 0.03 | −0.06 | −2.41 | −0.20 | 0.04 | −0.14 | −5.46** |
| General trust | −0.29 | 0.03 | −0.24 | −9.34** | −0.22 | 0.04 | −0.16 | −6.20** |
| False tradeoffs | −0.07 | 0.03 | −0.08 | −2.48 | 0.23 | 0.03 | 0.23 | 7.51** |
| Social trust | 0.14 | 0.03 | 0.15 | 4.70** | 0.17 | 0.03 | 0.16 | 5.06** |
| Negative affect | 0.10 | 0.01 | 0.18 | 7.64** | 0.07 | 0.01 | 0.11 | 4.62** |
Note: N = 1,585.
p < 0.01; **p < 0.001.
R 2 = 0.13 for perceived health risk and R 2 = 0.12 for perceived economic fears.
Sex: man coded as 0, woman coded as 1.
Belonging to objective risk group: no coded as 0, yes coded as 1.
Standardized coefficients.
The same set of predictors was used to explain perceived risks related to the economy. The model was significant, F(8,1576) = 27.91, p < 0.001, and explained 12% of the variance. The results are shown in Table III. Females perceived significantly more economic risks compared with males. Age was positively correlated with perceived economic risks. The participants with higher values on the general confidence and the general trust scales perceived fewer economic risks compared with the participants who had lower values on the two scales. The participants with high levels of social trust related to the government and the pharmaceutical industry perceived more economic risks compared with the participants who had low levels of social trust. The more negative the affect evoked by SARS‐CoV‐2, the more risk for the economy was perceived.
3.4. Acceptance of measures
Similar to other countries, Switzerland implemented various measures to reduce the infection rate. During the survey period, schools were closed, group gatherings of more than five people were not allowed, and only food shops and pharmacies were open. Furthermore, the government asked people to stay home and not leave the house unless necessary. However, no complete lockdown was imposed. A linear regression analysis was utilized to examine which predictors explained the acceptance of the measures implemented in Switzerland. The model was significant, F(9,1575) = 123.61, p < 0.001, and explained 41% of the variance. The results are shown in Table IV. The participants’ risk perception was the most important predictor of the acceptance of the measures implemented to prevent the spread of SARS‐CoV‐2. The second most important predictor comprised perceived tradeoffs. In other words, the participants who thought that the measures’ negative side effects were not sufficiently taken into account showed lower acceptance of the measures compared with the participants who did not share these beliefs. General confidence had a significant positive association with the acceptance of the measures. The participants with higher general trust showed less acceptance of the measures compared with those who had lower general trust. Social trust was a positive predictor of the acceptance of the measures. The participants who trusted in the government and in the pharmaceutical companies regarding COVID‐19 showed more acceptance compared with the participants who lacked social trust.
Table IV.
Results of a Linear Regression Analysis with Acceptance of Implemented Measures for Decreasing the Infection Rate as the Dependent Variable
| Unstandardized B | SE | Beta 3 | t | |
|---|---|---|---|---|
| Constant | 4.12 | 0.25 | 16.81** | |
| Sex 1 | 0.12 | 0.06 | 0.04 | 2.09 |
| Age | 0.001 | 0.002 | 0.01 | 0.40 |
| Risk group 2 | −0.06 | 0.07 | −0.02 | −0.90 |
| General confidence | 0.10 | 0.03 | 0.08 | 3.65** |
| General trust | −0.12 | 0.03 | −0.10 | −4.52** |
| Health risk perception | 0.45 | 0.02 | 0.45 | 20.06** |
| Economic risk perception | −0.05 | 0.02 | −0.05 | −2.32 |
| False tradeoffs | −0.26 | 0.02 | −0.30 | −11.48** |
| Social trust | 0.14 | 0.03 | 0.15 | 5.60** |
Note: R 2 = 0.41; N = 1,585.
p < 0.01; **p < 0.001.
Sex: man coded as 0, woman coded as 1.
Belonging to objective risk group: no coded as 0, yes coded as 1.
Standardized coefficients.
3.5. Behavior
To slow down the infection rate, contact with other people should be decreased, and hygienic behavior should be increased. The index consisted of six items measuring contact with other people (e.g., relatives visiting my/our home). The majority of the participants (n = 839, 53%) had a value of 0 for this index, indicating very few contacts. Only 3% of the participants had a value above 2 for this index, with a theoretical maximum of 6. Given the skewed distribution of this variable, a dummy variable was created, with the value of 0 or 1, where 1 indicated at least one positive response to one of the six items. A logistic regression analysis was conducted to examine which predictors were associated with the number of situations in which the participants had contacts with other people. The model was significant, χ 2(9) = 37.51, p < 0.001, and Nagelkerke R 2 = 0.03. The results are shown in Table V. Health risk perception was negatively associated with the number of contacts. The participants with a higher health risk perception related to SARS‐CoV‐2 had fewer contacts compared with those who had a lower health risk perception.
Table V.
Results of a Logistic Regression Analysis with the Dummy Variable (Number of Situations with Other People) as the Dependent Variable
| B | SE | p | |
|---|---|---|---|
| Constant | 0.89 | 0.46 | 0.05 |
| Sex 1 | −0.08 | 0.10 | 0.47 |
| Age | −0.01 | 0.004 | 0.01 |
| Risk group 2 | 0.10 | 0.12 | 0.43 |
| General confidence | 0.04 | 0.05 | 0.47 |
| General trust | −0.02 | 0.05 | 0.72 |
| Health risk perception | −0.17 | 0.04 | <0.001 |
| Economic risk perception | 0.05 | 0.04 | 0.21 |
| False tradeoffs | 0.05 | 0.04 | 0.25 |
| Social trust | −0.06 | 0.05 | 0.23 |
Note: Nagelkerke R 2 = .03; N = 1,585.
Sex: man coded as 0, woman coded as 1.
Belonging to objective risk group: no coded as 0, yes coded as 1.
The linear regression model explaining hygienic behavior was significant, F(9,1575) = 13.49, p < 0.001, and explained 7% of the variance. The results are shown in Table VI. Age and perceived risks were the two significant predictors. Older participants and participants with a higher health risk perception showed more hygienic behavior compared with younger participants and participants who had a lower health risk perception.
Table VI.
Results of a Linear Regression Analysis with Hygienic Behavior as the Dependent Variable
| Unstandardized B | SE | Beta 3 | t | |
|---|---|---|---|---|
| Constant | 2.11 | 0.36 | 5.85** | |
| Sex 1 | −0.02 | 0.08 | −0.01 | −0.19 |
| Age | 0.01 | 0.003 | 0.10 | 3.73** |
| Risk group 2 | −0.05 | 0.10 | −0.01 | −0.53 |
| General confidence | 0.10 | 0.04 | 0.07 | 2.49 |
| General trust | −0.05 | 0.04 | −0.04 | −1.31 |
| Health risk perception | 0.30 | 0.03 | 0.25 | 8.96** |
| Economic risk perception | −0.02 | 0.03 | −0.02 | −0.63 |
| False tradeoffs | −0.03 | 0.03 | −0.03 | −1.02 |
| Social trust | −0.05 | 0.04 | −0.05 | −1.49 |
Note: R 2 = 0.07; N = 1,585.
p < 0.01; **p < 0.001.
Sex: man coded as 0, woman coded as 1.
Belonging to objective risk group: no coded as 0, yes coded as 1.
Standardized coefficients.
4. DISCUSSION
The data for this study were collected in Switzerland during the period when the highest number of people had positive test results. Before the data collection started, a large number of measures had been implemented, with a strong impact on public and personal lives (e.g., closure of schools, restaurants, and shops). This situation has provided an ideal opportunity to examine the factors that influence people's perception of and behavior during a pandemic. In our study, the participants are less afraid of being infected by the virus. They are more fearful that their family members could be infected, and that the healthcare system would be overloaded. Given that the healthcare system was never overloaded during the initial phase of the pandemic in Switzerland, this fear may decrease; as a result, support for risk management strategies and compliance with government measures may be lower as the pandemic continues.
Trust has been suggested as an important factor that influences people's perception and behavior during a pandemic (Siegrist & Zingg, 2014). Most of the support for such a claim does not come from studies conducted during a pandemic, however. One of the few relevant studies examined the impact of trust on a community under stress, specifically its collective action, during the SARS outbreak in 2003 (Fong & Chang, 2011). This cited study's results suggest that trust is only associated with perceived measures in the absence of an outbreak, but trust is less important in cities with an outbreak. Trust in science is not associated with people's risk perceptions related to COVID‐19 (Dryhurst et al., 2020). However, our study's findings indicate that trust is important during an outbreak of a pandemic. These seemingly contradicting results are déjà vu in risk perception research (Siegrist, in press). The impact of trust strongly depends on what type of trust is measured. Based on theoretical considerations, we have hypothesized that in the case of COVID‐19, general trust, as well as social trust, might be important. General trust has a negative impact on people's risk perceptions and thus an indirect effect on people's acceptance of the government's implemented measures and on their risk reduction behavior. People with high levels of trust tend to believe in the benevolence of others. Other people should be perceived as potential carriers of SARS‐CoV‐2 in order to adopt physical distancing behavior, which may present a conflict for people with a high level of general trust because they may be unable to easily perceive others as representing a risk factor. Our finding that trust may not be generally positive for implementing risk prevention measures is in line with the findings from the literature on flooding risks, suggesting that trust in the authorities may prevent people from implementing precautionary measures (Wachinger, Renn, Begg, & Kuhlicke, 2013). In addition to general trust, we have also measured social trust. Social trust is related to whether the government honestly informs the public about a pandemic. Whether people believe the government's assertion that COVID‐19 has not been intentionally brought to them and that pharmaceutical companies act in the public interest regarding COVID‐19 is also part of the social trust construct. The participants with high levels of social trust indicate more health and economic fears and more acceptance of the implemented measures compared with the participants who have low levels of social trust. Our results therefore suggest that social trust and general trust have opposite effects.
Health risk perception is the strongest predictor of people's acceptance of the implemented measures and of their behavior. The participants with a higher health risk perception show hygienic behavior more often and interact with fewer people compared with the participants who have a lower health risk perception. The impact of risk perception on people's risk‐related behavior seems plausible. However, it should be noted that in many studies on risk perception and behavior, no such relations could be observed (Kellens, Terpstra, & De Maeyer, 2013; Siegrist & Gutscher, 2006). This could be the case because participants may show nonadaptive risk management behavior due to their lack of knowledge on the correct behavior or the extremely high barrier to such behavior (e.g., costs, inconvenience). It is therefore important to note that in the case of the initial outbreak of COVID‐19 in Switzerland, risk perception seems to be a highly relevant factor contributing to acceptance of and compliance with the recommended protective measures. Nonetheless, these results may also imply that if people become familiar with COVID‐19, they may perceive less health risks. This would be in line with past studies showing that familiar hazards are perceived as less risky compared with unfamiliar and novel hazards (Siegrist, Keller, & Kiers, 2005; Slovic, 1987). This may have negative effects on people's risk mitigation behavior; they may show less strict hygienic behavior and may interact with more people, which will increase their risk, of course.
According to the affect heuristic, images associated with a hazard may have an impact on people's risk perceptions (Slovic & Peters, 2006; Slovic, Finucane, Peters, & MacGregor, 2004). Regarding COVID‐19, images of coffins containing COVID‐19 victims from Bergamo, Northern Italy, as well as of overworked care unit workers from Northern Italian hospitals, have been dominant in the Swiss media and may have shaped people's risk perceptions. We have found significant associations between the valence of the first spontaneous association that comes to the participants’ minds when asked about the coronavirus and their risk perceptions. The present study's results therefore provide further support for the importance of the affect heuristic for people's risk perceptions.
People may underestimate their own risk of contracting the virus. The prevalent finding about many people's belief that they are less likely to be affected by a personal risk compared with their peers has been labeled optimistic bias (Weinstein, 1989). In the present study, we also find such an optimistic bias against the likelihood of being infected by SARS‐CoV‐2. Furthermore, females perceive significantly more health risks compared with males, but age is not a significant predictor. These results are remarkable because males are more at risk than females, and older persons are more at risk compared with younger ones (Penna, Mercurio, Tocchetti, & Pagliaro, 2020). An optimistic bias in people's risk perception might be a challenge for risk communication. If most people think that they are less vulnerable than others, few people may be motivated to show risk reduction behavior.
As in many other countries, in Switzerland, the discussions about the measures that should be taken to control COVID‐19 have been dominated by epidemiologists and health concerns. Especially in the beginning of the pandemic, there were less discussions about the economic costs of the government measures and whether the undesirable side effects of some measures might be riskier than the virus. In the general population, on average, people do not believe that economic or social risks have not been sufficiently considered when implementing the measures. Nevertheless, people who believe that false tradeoffs have been made (i.e., a strong focus on health and less on the economy) show less acceptance of the implemented measures compared with people who think otherwise.
The data for this study were collected in the German‐speaking part of Switzerland. The stage of the pandemic, the measures implemented by the government, the social context, and the economic situation of a country may influence people's risk perceptions and whether they accept the measures. Additional studies are needed to test the generalizability of our findings. We only collected data about self‐reported behavior, not actual behavior. Furthermore, during our study, restaurants were closed, many places where people usually meet were closed, and public transportation was substantially reduced. It was thus more difficult to meet other people or go out in public. This may be one of the reasons why our model provides a much better explanation of people's acceptance of the measures but is less appropriate for explaining their number of contacts with other people. The regression model for hygienic behavior has limited explanatory power. One possible reason for this rather poor model fit may be the low Cronbach's alpha for the hygienic behavior scale. Another limitation of the present study is the use of a cross‐sectional design for testing causal relations. Finally, all items measuring social trust are negatively formulated. We do not think, however, that this influenced our results.
Risk perception, social trust, and the right balance between health and economic concerns seem to be important factors contributing to successful risk management during a pandemic. Building the basis for social trust already begins before a pandemic. Ill‐prepared government agencies may not be in a good position to be trusted by the public. Perceived risks are important for people's acceptance of government measures and their adoption of the recommended behavior changes regarding physical distancing from others or increased hygienic behavior. However, if people do not perceive any risks for themselves or if they perceive the measures as riskier than COVID‐19, they may be unwilling to follow public recommendations. In such a situation, governments might be tempted to heighten public risk perceptions by emphasizing single events (e.g., one young person died of COVID‐19). However, in our view, this is a risky strategy because communication whose only aim is to increase people's risk perceptions may undermine social trust at the end. Such persuasion strategies may result in less support of government measures due to a lack of social trust, instead of the intended opposite outcome.
Footnotes
Pregnancy was coded as a risk factor because of its impact on the immune system, as well as some physicians’ advice for pregnant women to take precautionary measures regarding infection with SARS‐CoV‐2.
Due to a programming error, one item (“Altogether, we live in a safe and secure time.”) of the original confidence scale was not included in the survey.
REFERENCES
- Condon, B. J. , & Sinha, T. (2010). Who is that masked person: The use of face masks on Mexico City public transportation during the Influenza A (H1N1) outbreak. Health Policy, 95(1), 50–56. [DOI] [PubMed] [Google Scholar]
- Connor, M. , & Siegrist, M. (2011). The power of association: Its impact on willingness to buy GM food. Human and Ecological Risk Assessment, 17, 1142–1155. [Google Scholar]
- Dryhurst, S. , Schneider, C. R. , Kerr, J. , Freeman, A. L. J. , Recchia, G. , van der Bles, A. M. , … van der Linden, S. (2020). Risk perceptions of COVID‐19 around the world. Journal of Risk Research, 23(7–8), 994–1006. [Google Scholar]
- Earle, T. C. , & Siegrist, M. (2006). Morality information, performance information, and the distinction between trust and confidence. Journal of Applied Social Psychology, 36, 383–416. [Google Scholar]
- Federal Council . (2020). Coronavirus: Bundesrat erklärt die “ausserordentliche Lage” und verschärft die Massnahmen [Federal Council announces the ‘extraordinary situation’ and tightens measures] [Press release]. Retrieved from https://www.admin.ch/gov/de/start/dokumentation/medienmitteilungen.msg-id-78454.html
- Federal Office of Public Health . (2020). Neues Coronavirus: Besonders gefährdete Personen [New corona virus: Risk factors]. Retrieved from https://www.bag.admin.ch/bag/de/home/krankheiten/ausbrueche-epidemien-pandemien/aktuelle-ausbrueche-epidemien/novel-cov/besonders-gefaehrdete-menschen.html
- Federal Statistical Office . (2020a). Bildungsstand der Bevölkerung . Retrieved from https://www.bfs.admin.ch/bfs/de/home/statistiken/wirtschaftliche-soziale-situation-bevoelkerung/gleichstellung-frau-mann/bildung/bildungsstand.assetdetail.12527185.html
- Federal Statistical Office . (2020b). Demographic balance by age . Retrieved from https://www.bfs.admin.ch/bfs/en/home/statistics/population/effectif-change/population.assetdetail.14087718.html
- Finucane, M. L. , Alhakami, A. , Slovic, P. , & Johnson, S. M. (2000). The affect heuristic in judgments of risks and benefits. Journal of Behavioral Decision Making, 13(1), 1–17. [Google Scholar]
- Fischhoff, B. , Wong‐Parodi, G. , Garfin, D. R. , Holman, E. A. , & Silver, R. C. (2018). Public understanding of Ebola risks: Mastering an unfamiliar threat. Risk Analysis, 38(1), 71–83. 10.1111/risa.12794 [DOI] [PubMed] [Google Scholar]
- Fong, E. , & Chang, L. Y. (2011). Community under stress: Trust, reciprocity, and community collective efficacy during SARS outbreak. Journal of Community Health, 36(5), 797–810. 10.1007/s10900-011-9378-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gilles, I. , Bangerter, A. , Clemence, A. , Green, E. G. T. , Krings, F. , Staerkle, C. , & Wagner‐Egger, P. (2011). Trust in medical organizations predicts pandemic (H1N1) 2009 vaccination behavior and perceived efficacy of protection measures in the Swiss public. European Journal of Epidemiology, 26(3), 203–210. 10.1007/s10654-011-9577-2 [DOI] [PubMed] [Google Scholar]
- Glaeser, E. L. , Laibson, D. I. , Scheinkman, J. A. , & Soutter, C. L. (2000). Measuring trust. Quarterly Journal of Economics, 115, 811–846. [Google Scholar]
- Kellens, W. , Terpstra, T. , & De Maeyer, P. (2013). Perception and communication of flood risks: A systematic review of empirical research. Risk Analysis, 33, 24–49. [DOI] [PubMed] [Google Scholar]
- Keller, C. , Siegrist, M. , Earle, T. C. , & Gutscher, H. (2011). The general confidence scale: Coping with environmental uncertainty and threat. Journal of Applied Social Psychology, 41(9), 2200–2229. 10.1111/j.1559-1816.2011.00811.x [DOI] [Google Scholar]
- Keller, C. , Visschers, V. , & Siegrist, M. (2012). Affective imagery and acceptance of replacing nuclear power plants. Risk Analysis, 32, 464–477. [DOI] [PubMed] [Google Scholar]
- Liao, Q. Y. , Cowling, B. , Lam, W. T. , Ng, M. W. , & Fielding, R. (2010). Situational awareness and health protective responses to pandemic influenza A (H1N1) in Hong Kong: A cross‐sectional study. Plos One, 5(10). 10.1371/journal.pone.0013350 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Osterholm, M. T. (2005). Preparing for the next pandemic. New England Journal of Medicine, 352(18), 1839–1842. 10.1056/NEJMp058068 [DOI] [PubMed] [Google Scholar]
- Penna, C. , Mercurio, V. , Tocchetti, C. G. , & Pagliaro, P. (2020). Sex‐related differences in COVID‐19 lethality. British Journal of Pharmacology, 177(19), 4375–4385. 10.1111/bph.15207 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peters, E. , & Slovic, P. (1996). The role of affect and worldviews as orienting dispositions in the perception and acceptance of nuclear power. Journal of Applied Social Psychology, 26(16), 1427–1453. [Google Scholar]
- Podlesek, A. , Roskar, S. , & Komidar, L. (2011). Some factors affecting the decision on non‐mandatory vaccination in an influenza pandemic: Comparison of pandemic (H1n1) and seasonal influenza vaccination. Zdravstveno Varstvo, 50(4), 227–238. [Google Scholar]
- Prati, G. , & Pietrantoni, L. (2016). Knowledge, risk perceptions, and xenophobic attitudes: Evidence from Italy during the Ebola outbreak. Risk Analysis, 36(10), 2000–2010. 10.1111/risa.12537 [DOI] [PubMed] [Google Scholar]
- Prati, G. , Pietrantoni, L. , & Zani, B. (2011a). Compliance with recommendations for pandemic influenza H1N1 2009: The role of trust and personal beliefs. Health Education Research, 26(5), 761–769. 10.1093/her/cyr035 [DOI] [PubMed] [Google Scholar]
- Prati, G. , Pietrantoni, L. , & Zani, B. (2011b). A social‐cognitive model of pandemic influenza H1N1 risk perception and recommended behaviors in Italy. Risk Analysis, 31(4), 645–656. 10.1111/J.1539-6924.2010.01529.X [DOI] [PubMed] [Google Scholar]
- Quinn, S. C. , Kumar, S. , Freimuth, V. S. , Musa, D. , Casteneda‐Angarita, N. , & Kidwell, K. (2011). Racial disparities in exposure, susceptibility, and access to health care in the US H1N1 influenza pandemic. American Journal of Public Health, 101(2), 285–293. 10.2105/Ajph.2009.188029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rotter, J. B. (1967). A new scale for the measurement of interpersonal trust. Journal of Personality, 35(4), 651–665. [DOI] [PubMed] [Google Scholar]
- Siegrist, M. (in press). Trust and risk perception: A critical review of the literature. Risk Analysis, 10.1111/risa.13325 [DOI] [PubMed] [Google Scholar]
- Siegrist, M. , & Arvai, J. (2020). Risk perception: Reflections on 40 years of research. Risk Analysis, 40, 2191–2206. 10.1111/risa.13599 [DOI] [PubMed] [Google Scholar]
- Siegrist, M. , & Cvetkovich, G. (2000). Perception of hazards: The role of social trust and knowledge. Risk Analysis, 20(5), 713–719. [DOI] [PubMed] [Google Scholar]
- Siegrist, M. , Cvetkovich, G. , & Roth, C. (2000). Salient value similarity, social trust, and risk/benefit perception. Risk Analysis, 20(3), 353–362. [DOI] [PubMed] [Google Scholar]
- Siegrist, M. , & Gutscher, H. (2006). Flooding risks: A comparison of lay people's perceptions and expert's assessments in Switzerland. Risk Analysis, 26(4), 971–979. [DOI] [PubMed] [Google Scholar]
- Siegrist, M. , Gutscher, H. , & Earle, T. C. (2005). Perception of risk: The influence of general trust, and general confidence. Journal of Risk Research, 8(2), 145–156. [Google Scholar]
- Siegrist, M. , Keller, C. , & Kiers, H. A. L. (2005). A new look at the psychometric paradigm of perception of hazards. Risk Analysis, 25(1), 211–222. [DOI] [PubMed] [Google Scholar]
- Siegrist, M. , & Zingg, A. (2014). The role of public trust during pandemics implications for crisis communication. European Psychologist, 19(1), 23–32. 10.1027/1016-9040/a000169 [DOI] [Google Scholar]
- Slovic, P. (1987). Perception of risk. Science, 236(4799), 280–285. [DOI] [PubMed] [Google Scholar]
- Slovic, P. , Finucane, M. L. , Peters, E. , & MacGregor, D. G. (2004). Risk as analysis and risk as feelings: Some thoughts about affect, reason, risk, and rationality. Risk Analysis, 24(2), 311–322. [DOI] [PubMed] [Google Scholar]
- Slovic, P. , Finucane, M. L. , Peters, E. , & MacGregor, D. G. (2007). The affect heuristic. European Journal of Operational Research, 177(3), 1333–1352. 10.1016/j.ejor.2005.04.006 [DOI] [Google Scholar]
- Slovic, P. , & Peters, E. (2006). Risk perception and affect. Current Directions in Psychological Science, 15(6), 322–325. 10.1111/J.1467-8721.2006.00461.X [DOI] [Google Scholar]
- Smith, E. K. , & Mayer, A. (2018). A social trap for the climate? Collective action, trust and climate change risk perception in 35 countries. Global Environmental Change‐Human and Policy Dimensions, 49, 140–153. 10.1016/j.gloenvcha.2018.02.014 [DOI] [Google Scholar]
- van der Weerd, W. , Timmermans, D. R. M. , Beaujean, D. J. M. A. , Oudhoff, J. , & van Steenbergen, J. E. (2011). Monitoring the level of government trust, risk perception and intention of the general public to adopt protective measures during the influenza A (H1N1) pandemic in the Netherlands. BMC Public Health, 11(1). 10.1186/1471-2458-11-575 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wachinger, G. , Renn, O. , Begg, C. , & Kuhlicke, C. (2013). The risk perception paradox‐implications for governance and communication of natural hazards. Risk Analysis, 33(6), 1049–1065. 10.1111/j.1539-6924.2012.01942.x [DOI] [PubMed] [Google Scholar]
- Weinstein, N. D. (1989). Optimistic biases about personal risks. Science, 246(4935), 1232–1233. [DOI] [PubMed] [Google Scholar]
- Wong, C. M. L. , & Jensen, O. (2020). The paradox of trust: Perceived risk and public compliance during the COVID‐19 pandemic in Singapore. Journal of Risk Research, 23(7–8), 1021–1030. [Google Scholar]
- Yamagishi, T. (1988). The provision of a sanctioning system in the United States and Japan. Social Psychology Quarterly, 51, 265–271. [Google Scholar]
- Yamagishi, T. , & Cook, K. S. (1993). Generalized exchange and social dilemmas. Social Psychology Quarterly, 56(4), 235–248. [Google Scholar]
- Zanin, G. M. , Gentile, E. , Parisi, A. , & Spasiano, D. (2020). A preliminary evaluation of the public risk perception related to the COVID‐19 health emergency in Italy. International Journal of Environmental Research and Public Health, 17(9), 3024. 10.3390/ijerph17093024 [DOI] [PMC free article] [PubMed] [Google Scholar]