

Abstract
Background
Although women in South Asia and South-east Asia have developed their knowledge regarding modern contraceptive and other family planning techniques, limited information exists on the influence of mass media exposure on the utilization of contraceptives and family planning. The current study examined the association between media exposure and family planning in Myanmar and Philippines.
Methods
The study analyzed data from the 2017 Philippines National Demographic and Health Survey (NDHS) and 2015–16 Myanmar Demographic and Health Survey (MDHS). Three family planning indicators were considered in this study (i.e., contraceptive use, demand satisfied regarding family planning and unmet need for family planning). A binary logistic regression model was fitted to see the effect of media exposure on each family planning indicator in the presence of covariates such as age group, residence, education level, partner education level, socio-economic status, number of living children, age at first marriage, and working status.
Results
The prevalence of contraception use was 57.2% in the Philippines and 55.7% in Myanmar. The prevalence of demand satisfied regarding family planning was 70.5 and 67.1% in the Philippines and Myanmar respectively. Unmet need regarding family planning was 16.6% and 19.9% in the Philippines and Myanmar respectively. After adjusting for the covariates, the results showed that women who were exposed to media were more likely to use contraception in Philippines (aOR = 2.24, 95% CI = 1.42–3.54) and Myanmar (aOR 1.39, 95% CI = 1.15–1.67). Media exposure also had a significant positive effect on demand satisfaction regarding family planning in the Philippines (aOR = 2.19, 95% CI = 1.42–3.37) and Myanmar (aOR = 1.34, 95% CI = 1.09–1.64). However, there was no significant association between media exposure and unmet need in both countries.
Conclusions
The study established a strong association between mass media exposure and the use and demand satisfaction for family planning among married and cohabiting women in Philippines and Myanmar. Using mass media exposure (e.g., local radio, television- electronic; newspapers) to increase both access and usage of contraceptives as well as other family planning methods in these countries could be pivotal towards the attainment of United Nations Sustainable Development Goal 3 (SDG 3) of improving maternal health.
Keywords: DHS, Family planning, Media exposure, Myanmar, Philippines, Women’s health
Background
Globally, it has been observed that family planning issues are highly influenced by the scientific use of mass media, especially television, radio, newspaper, and internet [1]. Similarly, the last three decades have shown that indicators of family planning such as contraceptive use, unmet need for family planning, and demand satisfied regarding family planning have significant association with media exposure [1, 2]. Furthermore, the world has noticed an increased trend regarding these indicators of family planning. For example, worldwide data in 2017 indicates that the rate of contraceptive use among married or in-union women of reproductive age rose to 63% from 35% in 1970. Likewise, an increased trend (78% from 75% in 2000) has also been observed concerning the demand for family planning satisfied by modern methods among married or in-union women. However, 12% of women have an unmet need for family planning, which has declined from 22% in 1970 [3, 4]. A study suggests that the SMS-based communication coverage regarding family planning is higher in Africa than Asia [5]. However, the percentage in terms of contraceptive use in Central and West Africa is very low (25%) and in Asia, the rate is 66.4%, which is considered low compared to Thailand, Vietnam, and Singapore [6–8].
It is evident that women in South Asia and South-East Asia have developed their knowledge regarding modern contraceptive techniques through the proper utilization of mass media [9, 10]. For instance, in India, Pakistan, and Philippines, women who own TV at their homes are more likely to get access in the coverage of contraceptives than women who do not have TV [11–13]. Similarly, exposure of mass media in Myanmar is associated with the age of women at first marriage [14, 15]. A study conducted from 47 DHS data of sub-Saharan Africa indicates that overall, 44.3% family planning related information is available from mass media [16]. Furthermore, in Nigeria, in terms of getting family planning related messages, people with higher socio-economic status have more opportunity of getting access to mass media, especially television and radio, than people with lower socio-economic status [17, 18]. In Indonesia, the exposure of television has increased than radio and print media regarding family planning [19]. Also, in Ethiopia, women’s access to mass media, especially radio, television and newspaper has a significant impact on unmet need for child spacing and limiting births. For instance, data from the year 2005 in Ethiopia proved that women with no access to mass media had higher rate (38.1%) of unmet need for family planning than women with access to mass media (35.8%) [20]. In addition, some covariates like education, partner education, residence, and occupation also had significant impact on family planning. Specifically, urban women were more likely to utilize knowledge about contraceptive use from mass media than rural women. Similarly, educated women were more likely to obtain health related messages through mass media at their homes than healthcare centers [21].
Despite the numerous studies on family planning issues worldwide, these studies have paid more attention to the impact of basic socio-demographic status such as education, economic condition, and decision-making power on family planning rather than recognizing the importance of mass media for awareness building regarding family planning [19, 22–29]. Hence, the literature in Asia regarding media exposure and family planning is sparse. Although there is limited scholarly information on this issue, the influence of media exposure on family planning remains unclear [30, 31]. By utilizing the current DHS data, it is possible to present a valid outcome regarding this prevailing issue. Myanmar and Philippines were targeted for this study because in Myanmar, the contraceptive prevalence rate (CPR) was lower (41.0%) than other Southeast Asian countries (average rate of this region was 62.2% in 2007) [32]. Although the CPR increased at 52.2% in 2016, the rate was lower than a projected target of 60% by 2020 [33]. Rapid population growth, short life expectancy, low level of education, and poor healthcare system are the major loopholes in the process of achieving the goal of population control and ensure a sound maternal and child health by preventing unwanted pregnancies and encouraging birth spacing [14, 34]. Moreover, the rate of unmet need for family planning in Myanmar was very high (19%) than their nearest country, Thailand (3%) [34, 35]. Likewise, the population growth rate was highest in Philippines among the South-East Asia, along with the third highest total fertility rate (TFR) in the region. UN 2015 data indicated that the rate of unmet need of FP was 17.8%, which was higher than other Asian countries [36]. Furthermore, the overall contraceptive prevalence was only 40% among married women in 2017 in Philippines, where the rate of modern contraceptive prevalence increased by only 2% between 2013 and 2017 [37]. Therefore, evidence suggests these countries have challenges to increase the prevalence of contraceptive use and reduce the TFR [38]. This study, therefore, examines the association between media exposure and family planning in both Myanmar and Philippines. By making this assessment between these two countries, researchers and policy makers could get updated view on reproductive health issues for making proper guidelines and efficient programs.
Materials and methods
Data source and study settings
The study analyzed the 2017 Philippines National Demographic and Health Survey (NDHS) dataset, which took place from August 14 to October 27, 2017, and 2015–16 Myanmar Demographic and Health Survey (MDHS) dataset, which took place from December 7, 2015 to July 7, 2016. These two datasets were selected because they were the most recent dataset available for both countries.
Study design
The 2017 Philippines National Demographic and Health Survey (NDHS), implemented by the Philippine Statistics Authority (PSA), was based on two-stage stratified sample design. It used the Master Sample Frame (MSF) which was designed as well as compiled by the PSA. In the first stage, 1250 primary sampling units (PSUs), distributed by province, were systematically selected. Systematic random sampling from each sampled PSU 20 or 26 housing units were selected at the second stage. Then, from each housing unit, women aged 15–49 were interviewed. To prevent bias replacement, changes in the pre-specified housing units were not allowed. After the data collection, information of 25,074 women were obtained.
The 2015–16 Myanmar Demographic and Health Survey (MDHS) was implemented by the Ministry of Health and Sports (MoHS). This survey followed a two-stage stratified sample design. From the master sample, 442 clusters (123 urban and 319 rural) were selected at the first. At the second stage, by using equal probability systematic sampling from each selected clusters (i.e., a total of 13,260 households), 30 households were selected. Then, from each household, women aged 15–49 were interviewed. After the data collection, data of total 12,885 women were obtained.
The data of women who were married or currently in union and were usual residents and not pregnant, and with education level, including partner’s education level were filtered out from the raw dataset of both countries. This filtered dataset was subsequently analyzed.
Dependent variables
The indicators of family planning selected were contraception use, unmet need for family planning and demand satisfied regarding family planning. The variable contraception use was coded as “Yes” for a woman who was currently using any kind of contraception method, otherwise coded as “No” and the variable unmet need for family planning was coded as “Yes” for a woman who had an unmet need for spacing or unmet need for limiting otherwise “No”. For a woman who had met the need for spacing or met the need for limiting, the indicator demand satisfied regarding family planning was coded as “Yes” otherwise “No”.
Independent variable
The variable media exposure was recoded as ‘Yes’ for a woman who was exposed to either newspaper, radio, television or the internet otherwise “No” for both the countries (Philippines, Myanmar).
A number of covariates were selected for this study based on previous literature [36–46]. These are age group (15–24, 25–29, 30–34, 35–39, 40–49), residence (urban, rural), education level (no education, primary, secondary, higher), partner education level (no education, primary, secondary, higher), socio-economic status (poorest, poorer, middle, richer, richest), number of living children (no children, 1–3, more than 3), age at first marriage (below 20, 20–25, more than 25), and working status (employed, unemployed).
Statistical analysis
After the required filtration of the dataset, chi-square was performed between the confounders and the family planning indicators. The binary logistic regression model was fitted to see the association between media exposure with each family planning indicators in the presence of covariates age group, residence, educational level, partner’s educational level, socio-economic status, number of living children, age at first marriage, and working status. In each model, the covariates were kept regardless of their p-value. Each model was assessed by calculating the area under the ROC curve and were found satisfactory. The analysis was done after considering the sample weight and the complex survey design. All the p-values less than 0.05 were considered significant. The analysis was conducted using software R version 3.6.0.
Results
Sample characteristics
The weighted sample size for Philippines and Myanmar was 4497 and 7047 respectively. For both countries, most of the women were in the age group 40–49 years (see Table 1). For Philippines, 60.2% of the women were from urban areas whereas 26.3% of the women in Myanmar were from urban areas. The sample from Philippines comprised 46.4% of women with a secondary level of education and 41.1% women with partner having secondary level of education whereas the sample of Myanmar comprised 29% women with a secondary level of education and 38.2% women with partner having secondary level of education. The socio-economic status of the women of Philippines was mostly in the richest quintile whereas women from Myanmar have socio-economic status mostly in the middle and poorer quintile. Most of the women of Philippines had age at first marriage within 20–25 while most of the women of Myanmar had age at first marriage below 20. For both countries, most of the women had 1–3 living children. Also, majority of the women from Philippines were employed whereas most of the women of Myanmar were unemployed.
Table 1.
General characteristics of the respondents
| Variable | Philippines (4497) | Myanmar (7047) | ||
|---|---|---|---|---|
| N | Percent | N | Percent | |
| Age group | ||||
| • 15–24 | 543 | 12.1 | 860 | 12.2 |
| • 25–29 | 750 | 16.7 | 1057 | 15 |
| • 30–34 | 765 | 17 | 1353 | 19.2 |
| • 35–39 | 851 | 18.9 | 1395 | 19.8 |
| • 40–49 | 1588 | 35.3 | 2382 | 33.8 |
| Residence | ||||
| • Urban | 2706 | 60.2 | 1854 | 26.3 |
| • Rural | 1791 | 39.8 | 5193 | 73.7 |
| Education level | ||||
| • No education | 51 | 1.1 | 1097 | 15.6 |
| • Primary | 693 | 15.4 | 3348 | 47.4 |
| • Secondary | 2087 | 46.4 | 2041 | 29 |
| • Higher | 1666 | 37.1 | 561 | 8 |
| Partner education level | ||||
| • No education | 59 | 1.3 | 1063 | 15.1 |
| • Primary | 934 | 20.8 | 2850 | 40.4 |
| • Secondary | 1849 | 41.1 | 2689 | 38.2 |
| • Higher | 1655 | 36.8 | 445 | 6.3 |
| Socio-economic status | ||||
| • Poorest | 780 | 17.3 | 1423 | 20.2 |
| • Poorer | 775 | 17.2 | 1446 | 20.5 |
| • Middle | 880 | 19.6 | 1442 | 20.5 |
| • Richer | 1022 | 22.7 | 1373 | 19.5 |
| • Richest | 1040 | 23.2 | 1363 | 19.3 |
| Number of living children | ||||
| • No children | 341 | 7.6 | 496 | 9.9 |
| • 1–3 | 3025 | 67.3 | 5022 | 71.3 |
| • More than 3 | 1131 | 25.2 | 1328 | 18.8 |
| Age at first marriage | ||||
| • Below 20 | 1763 | 39.2 | 3322 | 47.2 |
| • 20–25 | 1909 | 42.5 | 2674 | 37.9 |
| • Above 25 | 825 | 18.3 | 1051 | 14.9 |
| Working status | ||||
| • Employed | 2300 | 51.1 | 2458 | 34.9 |
| • Unemployed | 2197 | 48.9 | 4588 | 65.1 |
The family planning indicator contraception use prevalence was 57.2% in the Philippines and 55.7% in Myanmar (see Fig. 1). The prevalence of demand satisfied regarding family planning was 70.5 and 67.1% in the Philippines and Myanmar respectively. Unmet need regarding family planning was 16.6% and 19.9% in the Philippines and Myanmar respectively.
Fig. 1.
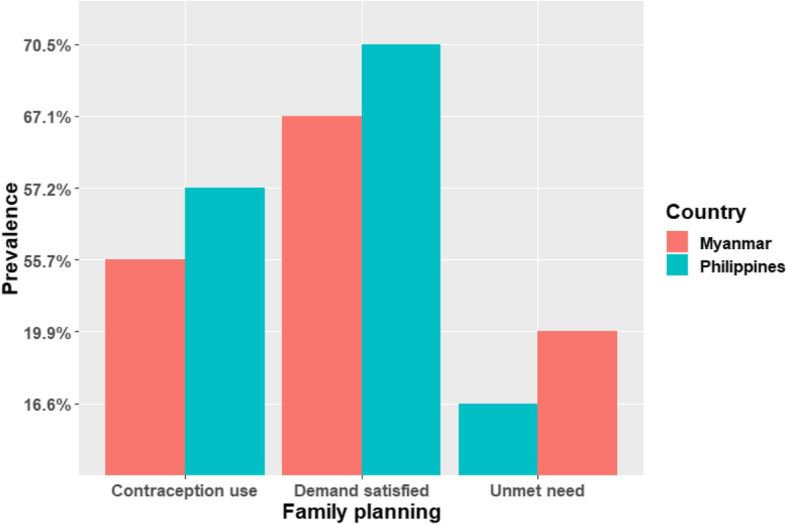
Prevalence of family planning indicators
Chi-square test between the confounding variables and family planning indicators
The results of the chi-square test and the distribution of the family planning indicators across the confounding variables are presented in the Tables 2, 3, 4.
Table 2.
Chi-square test of the association between contraception use and confounders
| Variable | Philippines | Myanmar | ||||
|---|---|---|---|---|---|---|
| Contraception use | p-value | Contraception use | p-value | |||
| Yes | No | Yes | No | |||
| Age group | < 0.01 | |||||
| • 15–24 | 339 | 203 | 580 | 280 | ||
| • 25–29 | 454 | 297 | 710 | 330 | ||
| • 30–34 | 486 | 280 | < 0.01 | 834 | 522 | |
| • 35–39 | 530 | 320 | 923 | 469 | ||
| • 40–49 | 765 | 824 | 880 | 1498 | ||
| Residence | ||||||
| • Urban | 1564 | 1142 | 0.529 | 1170 | 684 | < 0.01 |
| • Rural | 1009 | 782 | 2757 | 2433 | ||
| Education level | < 0.01 | |||||
| • No education | 10 | 41 | 443 | 633 | ||
| • Primary | 355 | 337 | < 0.01 | 1820 | 1527 | |
| • Secondary | 1313 | 774 | 1298 | 743 | ||
| • Higher | 895 | 772 | 366 | 194 | ||
| Partner education level | < 0.01 | |||||
| • No education | 10 | 41 | 429 | 634 | ||
| • Primary | 355 | 337 | < 0.01 | 1595 | 1255 | |
| • Secondary | 1313 | 774 | 1621 | 1068 | ||
| • Higher | 895 | 772 | 283 | 162 | ||
| Socio-economic status | < 0.01 | |||||
| • Poorest | 398 | 381 | 732 | 467 | ||
| • Poorer | 494 | 281 | 774 | 412 | ||
| • Middle | 534 | 346 | < 0.01 | 765 | 391 | |
| • Richer | 610 | 412 | 802 | 339 | ||
| • Richest | 537 | 504 | 854 | 314 | ||
| Number of living children | < 0.01 | |||||
| • No children | 39 | 302 | 266 | 430 | ||
| • 1–3 | 1870 | 1154 | < 0.01 | 3088 | 1934 | |
| • More than 3 | 663 | 468 | 573 | 755 | ||
| Age at first marriage | < 0.01 | |||||
| • Below 20 | 1064 | 698 | 1872 | 1450 | ||
| • 20–25 | 1134 | 775 | < 0.01 | 1552 | 1122 | |
| • Above 25 | 374 | 451 | 503 | 548 | ||
| Working status | 0.66 | |||||
| • Employed | 1241 | 956 | 0.57 | 1381 | 1077 | |
| • Unemployed | 1332 | 968 | 2546 | 2042 | ||
Table 3.
Chi-square test of the association between demand satisfied and confounders
| Variable | Philippines | Myanmar | ||||
|---|---|---|---|---|---|---|
| Demand satisfied | p-value | Demand satisfied | p-value | |||
| Yes | No | Yes | No | |||
| Age group | < 0.01 | |||||
| • 15–24 | 339 | 190 | 580 | 268 | ||
| • 25–29 | 454 | 240 | 710 | 313 | ||
| • 30–34 | 486 | 188 | 0.04 | 834 | 414 | |
| • 35–39 | 530 | 172 | 923 | 334 | ||
| • 40–49 | 765 | 287 | 880 | 594 | ||
| Residence | < 0.01 | |||||
| • Urban | 1564 | 601 | 0.07 | 1170 | 403 | |
| • Rural | 1009 | 476 | 2757 | 1520 | ||
| Education level | < 0.01 | |||||
| • No education | 10 | 13 | 443 | 375 | ||
| • Primary | 355 | 200 | < 0.01 | 1820 | 895 | |
| • Secondary | 1313 | 438 | 1298 | 515 | ||
| • Higher | 895 | 426 | 366 | 138 | ||
| Partner education level | < 0.01 | |||||
| • No education | 23 | 22 | 429 | 393 | ||
| • Primary | 494 | 260 | < 0.01 | 1593 | 748 | |
| • Secondary | 1138 | 387 | 1621 | 677 | ||
| • Higher | 918 | 408 | 283 | 106 | ||
| Socio-economic status | < 0.01 | |||||
| • Poorest | 398 | 238 | 732 | 467 | ||
| • Poorer | 494 | 174 | 774 | 412 | ||
| • Middle | 534 | 203 | < 0.01 | 765 | 391 | |
| • Richer | 610 | 199 | 802 | 339 | ||
| • Richest | 537 | 263 | 854 | 314 | ||
| Number of living children | < 0.01 | |||||
| • No children | 39 | 165 | 266 | 282 | ||
| • 1–3 | 1870 | 663 | < 0.01 | 3088 | 1236 | |
| • More than 3 | 663 | 249 | 573 | 405 | ||
| Age at first marriage | < 0.01 | |||||
| • Below 20 | 1064 | 431 | 1872 | 914 | ||
| • 20–25 | 1134 | 415 | < 0.01 | 1552 | 676 | |
| • Above 25 | 374 | 230 | 503 | 333 | ||
| Working status | 0.37 | |||||
| • Employed | 1241 | 572 | 0.06 | 1381 | 704 | |
| • Unemployed | 1332 | 505 | 2546 | 1219 | ||
Table 4.
Chi-square test of the association between unmet need and confounders
| Variable | Philippines | Myanmar | ||||
|---|---|---|---|---|---|---|
| Unmet need | p-value | Unmet need | p-value | |||
| Yes | No | Yes | No | |||
| Age group | < 0.01 | |||||
| • 15–24 | 89 | 439 | 125 | 723 | ||
| • 25–29 | 100 | 594 | 156 | 867 | ||
| • 30–34 | 97 | 577 | < 0.01 | 202 | 1046 | |
| • 35–39 | 87 | 615 | 184 | 1073 | ||
| • 40–49 | 233 | 818 | 498 | 976 | ||
| Residence | < 0.01 | |||||
| • Urban | 337 | 1829 | 0.20 | 246 | 1326 | |
| • Rural | 270 | 1214 | 919 | 3359 | ||
| Education level | < 0.01 | |||||
| • No education | 7 | 16 | 261 | 557 | ||
| • Primary | 128 | 427 | 0.01 | 570 | 2146 | |
| • Secondary | 261 | 1490 | 283 | 1529 | ||
| • Higher | 211 | 1110 | 51 | 453 | ||
| Partner education level | < 0.01 | |||||
| • No education | 13 | 31 | 263 | 558 | ||
| • Primary | 151 | 603 | 0.07 | 484 | 1858 | |
| • Secondary | 227 | 1298 | 371 | 1926 | ||
| • Higher | 216 | 1110 | 47 | 342 | ||
| Socio-economic status | < 0.01 | |||||
| • Poorest | 134 | 501 | 292 | 907 | ||
| • Poorer | 107 | 560 | 247 | 939 | ||
| • Middle | 122 | 615 | 0.08 | 232 | 924 | |
| • Richer | 104 | 705 | 218 | 923 | ||
| • Richest | 139 | 661 | 176 | 992 | ||
| Number of living children | < 0.01 | |||||
| • No children | 15 | 189 | 59 | 489 | ||
| • 1–3 | 385 | 2148 | < 0.01 | 778 | 3546 | |
| • More than 3 | 207 | 706 | 328 | 650 | ||
| Age at first marriage | 0.001 | |||||
| • Below 20 | 278 | 1217 | 616 | 2170 | ||
| • 20–25 | 231 | 1318 | 0.32 | 417 | 1811 | |
| • Above 25 | 97 | 508 | 133 | 703 | ||
| Working status | 0.50 | |||||
| • Employed | 324 | 1489 | 0.18 | 404 | 1681 | |
| • Unemployed | 283 | 1554 | 762 | 3003 | ||
Binary logistic regression models between family planning indicators and media exposure
After adjusting for the covariates, the results showed that media exposure has a significant effect on contraception use for both Philippines and Myanmar (see Table 5). In Philippines, media exposed women are significantly 1.27 times more likely to use any contraception method than women who are not media exposed. Similarly, in Myanmar, media exposed women are significantly 39% more likely to use any contraception method than women who are not media exposed.
Table 5.
Association between media exposure and contraceptive use after adjusting for the covariates
| Variable | Philippines | Myanmar | ||||||
|---|---|---|---|---|---|---|---|---|
| aOR | 95% CI | P-value | ROC curve | aOR | 95% CI | P-value | ROC curve | |
| Media Exposure | ||||||||
| • Yes | 2.27 | 1.45 -3.56 | < 0.001* | 68.2% | 1.39 | 1.15–1.67 | 0.001* | 69.7% |
| • No | Ref. | Ref. | ||||||
Note: Reference category of contraception use is ‘No’
CI Confidence interval, aOR Adjusted odds ratio
*significant
Media exposure also has a significant effect on family planning indicator demand satisfied in the presence of all the covariates for both countries (see Table 6). In Philippines media exposed women are significantly 1.15 times more likely to have demand satisfied regarding family planning than the women who are not media exposed. Similarly, in Myanmar media exposed women are 34% more likely to have demand satisfied regarding family planning than the women who are not media exposed.
Table 6.
Association between media exposure and demand satisfied regarding family planning after adjusting for covariates
| Variable | Philippines | Myanmar | ||||||
|---|---|---|---|---|---|---|---|---|
| aOR | 95% CI | P-value | ROC curve | aOR | 95% CI | P-value | ROC curve | |
| Media Exposure | ||||||||
| • Yes | 2.15 | 1.41 -3.27 | < 0.001* | 65.5% | 1.34 | 1.09 –1.64 | 0.006* | 64.4% |
| • No | Ref. | Ref. | ||||||
Note: Reference category of demand satisfied is ‘No’
CI Confidence interval, aOR Adjusted odds ratio
*significant
But in the presence of all the covariates, the result shows that media exposure has no significant effect on family planning indicator unmet need for both countries (see Table 7).
Table 7.
Association between media exposure and unmet need for family planning after adjusting for the covariates
| Variable | Philippines | Myanmar | ||||||
|---|---|---|---|---|---|---|---|---|
| aOR | 95% CI | P-value | ROC curve | aOR | 95% CI | P-value | ROC curve | |
| Media Exposure | ||||||||
| • Yes | 0.79 | 0.55–1.15 | 0.23ns | 60.6% | 0.87 | 0.72 –1.06 | 0.18ns | 65.4% |
| • No | Ref. | Ref. | ||||||
Note: Reference category of unmet need is ‘No’
CI Confidence interval, aOR Adjusted odds ratio, ns not significant
Discussion
We examined the association between mass media exposure and family planning and compared the assessment in both countries so that researchers and policy makers could get an utter view for making proper guidelines and efficient programs. Using data from the Demographic and Health Survey in Philippines and Myanmar, the regression analysis was fitted to show the effect of mass media exposure on the various family planning indicators. After adjusting for covariates, the study revealed that mass media exposure has a significant effect on contraception use in both countries. In the Philippines, the results indicate that women who had media exposure were approximately 2 times more likely to use any contraceptive methods as opposed to their counterparts who were not exposed to mass media. Similarly, in Myanmar, mass media exposed women were 39% more likely to use any contraceptive method than women who were not exposed to mass media. This finding supports other studies that have documented the influence of mass media communication interventions on contraceptive use [2–9]. Additionally, studies [10–12] have claimed that mass media remains a vital source of information and has the capacity to raise awareness, increase knowledge level, and influence attitudes towards family planning. This same evidence aligns with another work [13] in Kenya that revealed that access to media messages influences the use of contraceptives, intention to use contraceptives, and even desire for future births.
Other studies have demonstrated that mass media impacts women empowerment, including their ability to take household decisions on contraception [47–51]. For example, sexual partners who access diverse media platforms (e.g., television, radio, newspapers), communicate more about safer sexual practices and subsequently use contraceptives (e.g., condoms), and/or other family planning methods. Thus, exposure to media could improve knowledge and attitudes through behaviour modification associated with consistent use of some contraceptives and other family planning methods. Some behaviours and communication change models emphasize that knowledge is one key prerequisite for a positive behavioural change [14–17, 52].
Another important finding in our study is the effect of mass media exposure on demand satisfied regarding family planning. Surprisingly, there is little published data on this aspect and its association with mass media. The current study reveals that mass media exposure also has a significant effect on satisfaction of demands in the presence of all the covariates for both countries. For both countries, geographical disparities or heterogeneity (e.g., population density, ageing pattern) in attitudes and norms, differentials in employment, and other socio-economic parameters (e.g., household wealth index) might mirror the accessibility of media platforms relative to information or messages on general and reproductive health care, including contraception and family planning methods toward demand satisfaction [53–55]. For instance, the regional groups in Myanmar show geographic inequalities in access to modern contraception or accessibility and quality of family planning services [53]. It is more likely that indicators such as physical distance, staying in hilly areas, and network access and/ or availability of media outlets might limit appropriate information or messages related to reproductive healthcare and services. This limitation could influence the demand satisfaction of the populace towards contraception and other family planning methods in the country [56]. Further, media information related concerns about the side effects, health consequences, and inconvenience of methods might negatively influence demand and satisfaction on contraceptive usage. The unpleasant thoughts of side effects, method-related and health concerns might be reasons that may account for low patronage or possibly discontinuation of use [57, 58].
Although extensive research has been carried out on family planning, little or no study emphasizes the satisfied demands of women who have been exposed to mass media. However, few studies [18, 19] have documented that women’s exposure to media is one of the two important factors that influence contraceptive use and promote health-related behaviour such as reproductive preferences. Other studies that hold a similar view with the current study are earlier works of Hailemariam [20] at an individual level and those of Abulmageed [21] at a national level, which found a relationship between mass media exposure and reduction in fertility levels. Ultimately, this narrative holds the view that the use of mass media positively increases the awareness about the need for fertility control [59].
This pioneering investigation of the effect of media exposure and family planning as an indicator of unmet needs for both Philippines and Myanmar, after adjusting for all the covariates, shows that media exposure has no significant effect on the unmet needs for both countries. However, this finding contradicts previous research [22, 23] that reported that exposure to newspaper/ magazine had a significant effect on unmet needs for family planning whereas those who had no information had a higher likelihood of their needs being unmet. The current finding is surprising because unmet needs for contraceptive and family planning methods is relatively higher in low-income developing countries like Philippines and Myanmar with low socio-economic indicators (e.g., poverty, low education) [60]. Therefore, in relatively low-income countries, the likelihood of few media establishments could restrict young people’s capacity because of low media education or information related to accessing contraceptives or seeking sexual and reproductive health services [61, 62]. Besides, the growing trend of premarital sexual relationship and unintended pregnancies noted in many South-East Asian countries (e.g., Indonesia, Myanmar, Nepal, Pakistan, Philippines) requires a greater need for contraceptives among the sexually active population [41, 63]. Methodological variations and the type of media exposure studied in previous studies might account for the inconsistencies. The theoretical implication is that mass media communication campaigns are highly capable of influencing family planning methods in both countries.
Strength and limitations
This study is the first to investigate the effect of mass media exposure on family planning indicators in Philippines and Myanmar. It also provides insights into the effects of media exposure on demand satisfaction on family planning methods and on unmet needs for both countries that previous studies have ignored. The study is not without some limitations. First, the use of the large DHS dataset from cross-sectional perspective restricts causality from the noted outcomes. Second, because of the research design used, the possibility of social desirability associated with self-reporting and recall bias from the respondents cannot be ruled out. Also, the effects of the type of mass media exposure of the sample were not captured in the current study. Other limitations might include the alterations in the coding of the study variables, which could potentially generate data extraction errors. However, no substantial modifications were done during coding and extraction within the current study [47]. Despite these limitations, the sample size allows for generalizability of findings in the studied countries because data used were nationally representative.
Conclusions
The study established a strong association between mass media exposure and the use of contraceptive and family planning as well as demand satisfaction among the sexually active population in Philippines and Myanmar. Using mass media exposure (e.g., local radio, television- electronic; newspapers) to increase both access and usage of contraceptives as well as other family planning methods in these countries could be pivotal towards the attainment of United Nations Sustainable Development Goal 3 (MDG 3) of improving maternal health. Therefore, the dissemination of contraceptive use and other family planning information through media channels could help minimize neonatal and infant deaths, unsafe abortions, and maternal deaths often noticed in low-income countries like Philippines and Myanmar. Continuous education or advocacy on reproductive health matters (i.e., on contraception/ family planning) using the mass media could serve as a public health strategy for health-promoting behaviours. Public-private-sector partnership for the establishment of media houses in these countries is encouraged. Future studies could target the influence of the type of media exposure on contraception and/ or family planning methods possibly through longitudinal designs to establish clear patterns or trends for effective reproductive health interventions and policy direction.
Acknowledgments
We are grateful to MEASURE DHS for granting us free access to use the data for our study. We also appreciate the effort of Mr. Ebenezer Agbaglo, a budding linguist in the Department of English, University of Cape Coast, who took the pain to copyedit this manuscript.
Abbreviations
- NDHS
National Demographic and Health Survey
- MDHS
Demographic and Health Survey
- aOR
Adjusted odds ratio
- CI
Confidence interval
- SDG
Sustainable Development Goal
- PSA
Philippine Statistics Authority
Authors’ contributions
Conception and design of study: PD; analysis and/or interpretation of data: PD; drafting the manuscript: PD, NS, HA, TES, JEH, BOA and AS; revising the manuscript critically for important intellectual content; PD, NS, HA, TES, JEH, BOA and AS. All authors have read and approved the final manuscript.
Authors’ information
Department of Statistics, University of Dhaka, Bangladesh (PD); Department of Public Health, North South University, Bangladesh (NS); Institute of Social Welfare and Research, University of Dhaka, Bangladesh (HA); Bachelor of Science in Anatomy, University of Ilorin, Nigeria (TE); Department of Health, Physical Education, and Recreation, University of Cape Coast, Cape Coast, Ghana (JEH); Neurocognition and Action-Biomechanics-Research Group, Faculty of Psychology and Sport Sciences, Bielefeld University, Bielefeld-Germany (JEH), School of Public Health, Faculty of Health, University of Technology Sydney, Australia (BOA); Department of Population and Health, University of Cape Coast, Cape Coast, Ghana (AS); College of Public Health, Medical and Veterinary Sciences, James Cook University, Townsville, Queensland, Australia (AS).
Funding
Not Applicable.
Availability of data and materials
The dataset supporting the conclusions of this article is available online at https://dhsprogram.com/data/
Ethics approval and consent to participate
This was a secondary analysis of data and therefore no further approval was required for this study since the data is secondary and is available in the public domain. However, the source of data (DHS) reports that ethical clearance were obtained from the Ethics Committee of ORC Macro Inc. as well as Ethics Boards in Myanmar and Philippines. The DHS follows the standards for ensuring the protection of respondents’ privacy. Inner City Fund (ICF) International ensured that the survey complies with the U.S. Department of Health and Human Services regulations for the respect of human subjects.
Consent for publication
Not Applicable.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Pranta Das, Email: pranta.du.stat@gmail.com.
Nandeeta Samad, Email: nandeeta6@gmail.com.
Hasan Al Banna, Email: symumshuvro001@gmail.com.
Temitayo Eniola Sodunke, Email: temmy4tayo@yahoo.com.
John Elvis Hagan, Jr, Email: elvis.hagan@ucc.edu.gh.
Bright Opoku Ahinkorah, Email: brightahinkorah@gmail.com.
Abdul-Aziz Seidu, Email: abdul-aziz.seidu@stu.ucc.edu.gh.
References
- 1.Vijaykumar S. Communicating safe motherhood: strategic messaging in a globalized world. J Marriage Fam. 2008;44:2–3, 173-199. doi: 10.1080/01494920802177378. [DOI] [Google Scholar]
- 2.Naugle DA, Hornik RC. Systematic review of the effectiveness of mass media interventions for child survival in low- and middle-income countries. J Health Commun. 2014;19(sup1):190–215. doi: 10.1080/10810730.2014.918217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.World Family Planning Report . Department of Economic and Social Affairs. United Nations. 2017. [Google Scholar]
- 4.Alkema L, Kantorova V, Menozzi C, Biddlecom A. National, regional, and global rates and trends in contraceptive prevalence and unmet need for family planning between 1990 and 2015: a systematic and comprehensive analysis. Lancet. 2013;381(9878):1642–1652. doi: 10.1016/S0140-6736(12)62204-1. [DOI] [PubMed] [Google Scholar]
- 5.Hu Y, Huang R, Ghose B, Tang S. SMS-based family planning communication and its association with modern contraception and maternal healthcare use in selected low-middle-income countries. BMC Med Inform Decis Mak. 2020;20(1):218. doi: 10.1186/s12911-020-01228-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Utami Ds NKAD, Wirawan DN, Ani LS. Sociodemographic factors and current contraceptive use among ever-married women of reproductive age: Analysis of the 2017 Indonesia Demographic and Health Survey data. J Prev Med Public Health. 2019;7(2):95–102. doi: 10.15562/phpma.v7i2.211. [DOI] [Google Scholar]
- 7.Ogini AB, Ahonsi BA, Adebajo S. Trend and determinants of unmet need for family planning services among currently married women and sexually active unmarried women aged 15–49 in Nigeria (2003—2013). Afr Popul Stud. 2015;29(1) Available at: http://aps.journals.ac.za/pub/article/view/694.
- 8.Chakraborty NM, Murphy C, Paudel M, Sharma S. Knowledge and perceptions of the intrauterine device among family planning providers in Nepal: a cross-sectional analysis by cadre and sector. BMC Health Serv Res. 2015;15:39. doi: 10.1186/s12913-015-0701-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Majumder N, Ram F. Contraceptive use among poor and non-poor in Asian countries: a comparative study. Soc Sci Spectr. 2015;1(2):87–105. [Google Scholar]
- 10.Ayanore MA, Pavlova M, Groot W. Unmet reproductive health needs among women in some West African countries: a systematic review of outcome measures and determinants. Reprod Health. 2016;13:–5. 10.1186/s12978-015-0104-x PMID: 26774502; PMCID: PMC4715869. [DOI] [PMC free article] [PubMed]
- 11.Bakht MB, Arif Z, Zafar S, Nawaz MA. Influence of media on contraceptive use: a cross-sectional study in four Asian countries. J Ayub Med Coll Abbottabad. 2013;25(3–4):3–8. [PubMed] [Google Scholar]
- 12.Ansary R, Anisujjaman M. Factors determining pattern of unmet need for family planning in Uttar Pradesh, India. Int Res J Social Sci. 2012;1(4):16–23. [Google Scholar]
- 13.Khandeparkar K, Roy P, Motiani M. The effect of media exposure on contraceptive adoption across “poverty line”. Int J Pharm Healthc Mark. 2015;9(3):219–236. doi: 10.1108/IJPHM-06-2014-0034. [DOI] [Google Scholar]
- 14.Chan N, Sawangdee Y, Pattaravanich U, et al. Birth cohorts, marriage patterns, and contraceptive methods used among women in contemporary Myanmar. J Health Res. 2020;34(3):209–219. doi: 10.1108/JHR-06-2019-0127. [DOI] [Google Scholar]
- 15.Thein SS, Thepthien B. Unmet need for family planning among Myanmar migrant women in Bangkok, Thailand. Br J Midwifery. 2020;28(3). 10.12968/bjom.2020.28.3.182.
- 16.Babalola S, Figueroa ME, Krenn S. Association of mass media communication with contraceptive use in sub-Saharan Africa: a meta-analysis of demographic and health surveys. J Health Commun. 2017;22(11):885–895. doi: 10.1080/10810730.2017.1373874. [DOI] [PubMed] [Google Scholar]
- 17.Ajaero CK, Odimegwu C, Ajaero ID, Nwachukwu CA. Access to mass media messages, and use of family planning in Nigeria: a spatio-demographic analysis from the 2013 DHS. BMC Public Health. 2016;16:427. doi: 10.1186/s12889-016-2979-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Konkor I, Sano Y, Antabe R, Kansanga M, Luginaah I. Exposure to mass media family planning messages among post-delivery women in Nigeria: testing the structural influence model of health communication. Eur J Contracept Reprod Health Care. 2019;24(1):18–23. doi: 10.1080/13625187.2018.1563679. [DOI] [PubMed] [Google Scholar]
- 19.Ardiansyah B. Effect of mass media on family planning choices in Indonesia. 2016. [Google Scholar]
- 20.Hailemariam A, Haddis F. Factors affecting unmet need for family planning in southern nations, nationalities and peoples region, Ethiopia. Ethiop J Health Sci. 2011;21(2):77–89. doi: 10.4314/ejhs.v21i2.69048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Abulmageed SS, Elnimeiri MK. Sociodemographic and cultural determinants of seeking family planning knowledge and practice among a Sudanese community. Int J Community Med Public Health. 2018;5(8):3248–3256. doi: 10.18203/2394-6040.ijcmph20183053. [DOI] [Google Scholar]
- 22.Min KT, Bhula R. Socioeconomic and demographic determinants of contraceptive use among currently married women in Myanmar. 2019. [Google Scholar]
- 23.Islam AZ, Mostofa MG, Islam MA. Factors affecting unmet need for contraception among currently married fecund young women in Bangladesh. Eur J Contracept Reprod Health Care. 2016;21(6):443–448. doi: 10.1080/13625187.2016.1234034. [DOI] [PubMed] [Google Scholar]
- 24.Lwin MM, Munsawaengsub C, Nanthamongkokchai S. Factors influencing family planning practice among reproductive age married women in Hlaing township, Myanmar. J Med Assoc Thail. 2013;96(Suppl 5):S98–106. [PubMed] [Google Scholar]
- 25.Jirapongsuwan A, Latt KT, Siri S, Munsawaengsub C. Family planning practice among rural reproductive-age married women in Myanmar. Asia Pac J Public Health. 2016;28(4):303–312. doi: 10.1177/1010539516645159. [DOI] [PubMed] [Google Scholar]
- 26.Wai KM, Shibanuma A, Oo NN, Fillman TJ, Saw YM, Jimba M. Are husbands involving in their spouses’ utilization of maternal care services?: A cross-sectional study in Yangon, Myanmar. PLoS One. 2015;10(12):e0144135. doi: 10.1371/journal.pone.0144135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kamal SM. Socioeconomic factors associated with contraceptive use and method choice in urban slums of Bangladesh. Asia Pac J Public Health. 2015;27(2):NP2661–NP2676. doi: 10.1177/1010539511421194. [DOI] [PubMed] [Google Scholar]
- 28.Mon MM, Liabsuetrakul T. Predictors of contraceptive use among married youths and their husbands in a rural area of Myanmar. Asia Pac J Public Health. 2012;24(1):151–160. doi: 10.1177/1010539510381918. [DOI] [PubMed] [Google Scholar]
- 29.Colleran H, Mace R. Social network- and community-level influences on contraceptive use: evidence from rural Poland. Proc Biol Sci. 2015;282(1807):20150398. doi: 10.1098/rspb.2015.0398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Mutumba M, Wekesa E, Stephenson R. Community influences on modern contraceptive use among young women in low and middle-income countries: a cross-sectional multi-country analysis. BMC Public Health. 2018;18(1):430. doi: 10.1186/s12889-018-5331-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Soe K, Holland P, Mateus C. Association between maternal education and childhood mortalities in Myanmar. Asia Pac J Public Health. 2019;31(8):689–700. doi: 10.1177/1010539519888299. [DOI] [PubMed] [Google Scholar]
- 32.United Nation . World contraceptive use. 2011. [Google Scholar]
- 33.Tin NK, Williamson J, Sonneveldt E. Setting the stage for strengthen annual monitoring of family planning program performance at the state/national level in Myanmar. 2019;3:154. 10.12688/gatesopenres.13012.2. [DOI] [PMC free article] [PubMed]
- 34.Ministry of health . Health in Myanmar, 2013. Naypyidaw: Ministry of Health; 2014. [Google Scholar]
- 35.Ministry of Immigration and Population . Summary of the provisional result. 2014. [Google Scholar]
- 36.United Nation. Trends in contraception use worldwide 2015 (ST/ESA/SER.A/349). Available at: https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/undesa_pd_report_2015_trends_contraceptive_use.pdf. Accessed 20 Nov 2020.
- 37.Philippine Statistics Authority (PSA) and ICF . Philippines national demographic and health survey 2017: key indicators. Quezon City and Rockville: PSA and ICF; 2018. [Google Scholar]
- 38.Nagai M, Bellizzi S, Murray J, Kitong J, Cabral EI, Sobel HL. Opportunities lost: Barriers to increasing the use of effective contraception in the Philippines. PLoS One. 2019;14(7):e0218187. doi: 10.1371/journal.pone.0218187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Aung T, Hom NM, Sudhinaraset M. Increasing family planning in Myanmar: the role of the private sector and social franchise programs. BMC Womens Health. 2017;17(1):46. doi: 10.1186/s12905-017-0400-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Aung T, Thet MM, Sudhinaraset M, Diamond-Smith N. Impact of a social franchise intervention program on the adoption of long and short acting family planning methods in hard to reach communities in Myanmar. J Public Health (Oxf) 2019;41(1):192–200. doi: 10.1093/pubmed/fdy005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Najafi-Sharjabad F, Zainiyah Syed Yahya S, Abdul Rahman H, Hanafiah Juni M, Abdul Manaf R. Barriers of modern contraceptive practices among Asian women: a mini literature review. Global J Health Sci. 2013;5(5):181–192. doi: 10.5539/gjhs.v5n5p181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Miradora KG. Determinants of modern contraceptive use in the Philippines. Int J Pol Stu. 2017;8(1) Available at: researchgate.net/profile/Katrina_Miradora/publication/320444306_Determinants_of_Modern_Contraceptive_Use_in_the_Philippines/links/59e5d10d0f7e9b0e1ab25219/Determinants-of-Modern-Contraceptive-Use-in-the-Philippines.pdf.
- 43.Mello MM, Powlowski M, Nañagas JM, Bossert T. The role of law in public health: the case of family planning in the Philippines. Soc Sci Med. 2006;63(2):384–396. doi: 10.1016/j.socscimed.2006.01.010. [DOI] [PubMed] [Google Scholar]
- 44.Gupta N, Katende C, Bessinger RE. Associations of mass media exposure with family planning attitudes and practices in Uganda. Stud Fam Plan. 2003;34(1):19–31. doi: 10.1111/j.1728-4465.2003.00019.x. [DOI] [PubMed] [Google Scholar]
- 45.Jacobs J, et al. Mass media exposure and modern contraceptive use among married west African adolescents. Eur J Contracept Reprod Health Care. 2017;22(6):439–449. doi: 10.1080/13625187.2017.1409889. [DOI] [PubMed] [Google Scholar]
- 46.Tiruneh FN, et al. Factors associated with contraceptive use and intention to use contraceptives among married women in Ethiopia. Women Health. 2016;56(1):1–22. doi: 10.1080/03630242.2015.1074640. [DOI] [PubMed] [Google Scholar]
- 47.Seidu AA, Hagan JE, Agbemavi W, Ahinkorah BO, Nartey EB, Budu E, et al. Not just numbers: Beyond counting caesarean deliveries to understanding their determinants in Ghana using a population based cross-sectional study. BMC Pregnancy Childbirth. 2020;20(1):1–10. doi: 10.1186/s12884-019-2665-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Nair S, Dixit A, Ghule M, Battala M, Gajanan V, Dasgupta A, Begum S, Averbach S, Donta B, Silverman J, Saggurti N. Health care providers’ perspectives on delivering gender equity focused family planning program for young married couples in a cluster randomized controlled trial in rural Maharashtra, India. Gates Open Res. 2019;3. [DOI] [PMC free article] [PubMed]
- 49.Jensen R, Oster E. The power of TV: Cable television and women's status in India. Q J Econ. 2009;124(3):1057–94.
- 50.Mądra-Sawicka M, Nord JH, Paliszkiewicz J, Lee TR. Digital Media: Empowerment and Equality. Inform. 2020;11(4):225.
- 51.Leong C, Pan SL, Bahri S, Fauzi A. Social media empowerment in social movements: power activation and power accrual in digital activism. Eur J Inform Systems. 2019;28(2):173–204.
- 52.Servaes J, Malikhao P. Advocacy strategies for health communication. Public Relat Rev. 2010;36(1):42–9.
- 53.Aung MS, Soe PP, Moh MM. Predictors of modern contraceptive use and fertility preferences among men in Myanmar: further analysis of the 2015-16 demographic and health survey. Int J Community Med Public Health. 2019;6(10):4209. doi: 10.18203/2394-6040.ijcmph20194477. [DOI] [Google Scholar]
- 54.MacQuarrie KLD, Edmeades J, Steinhaus M, Head SK. Men and contraception: trends in attitudes and use. Rockville: ICF; 2015. [Google Scholar]
- 55.United States Agency for International Development . Essential considerations for engaging men and boys for improved family planning outcomes. Washington, D.C: Office of Population and Reproductive Health, Bureau for Global Health; 2018. [Google Scholar]
- 56.Tang K, Zhao Y, Li B, Zhang S, Lee SH. Health inequity on access to services in the ethic minorityregions of Northestern Myanmar: a cross-sectional study. BMJ. 2017;7:e017770. doi: 10.1136/bmjopen-2017-017770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Malik S, Courtney K. Higher education and women’s empowerment in Pakistan. Gend Educ. 2011;23(1):29–45.
- 58.Claringbold L, Sanci L, Temple-Smith M. Factors influencing young women's contraceptive choices. Aust J Gen Pract. 2019;48(6):389. [DOI] [PubMed]
- 59.Hornik R, McAnany E. Theories and evidence: mass media effects and fertility change. Commun Theory. 2001;11(4):454–471. doi: 10.1111/j.1468-2885.2001.tb00253.x. [DOI] [Google Scholar]
- 60.Wulifan JK, Brenner S, Jahn A, De Allegri M. A scoping review on determinants of unmet need for family planning among women of reproductive age in low and middle income countries. BMC women's health. 2015;16(1):1–5. [DOI] [PMC free article] [PubMed]
- 61.Chapagain M. Conjugal power relations and couples’ participation in reproductive health decision-making: exploring the links in Nepal. Gend Techn Dev. 2006;10(2):159–89.
- 62.Landau SC, Tapias MP, McGhee BT. Birth control within reach: a national survey on women's attitudes toward and interest in pharmacy access to hormonal contraception. Contraception. 2006;74(6):463–70. [DOI] [PubMed]
- 63.Wong LP. An exploration of knowledge, attitudes and behaviours of young multiethnic Muslim-majority society in Malaysia in relation to reproductive and premarital sexual practices. BMC Public Health. 2012;12(1):865. doi: 10.1186/1471-2458-12-865. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The dataset supporting the conclusions of this article is available online at https://dhsprogram.com/data/