

Abstract
Body-, eating-, and exercise-related social comparison tendencies are implicated in body dissatisfaction and disordered eating among Western women. To date, no published study examines eating- and exercise-related comparisons in a male or non-Western sample. The current series of studies fills these gaps in the literature by translating and validating the existing measure of these comparisons (the 18-item Body, Eating, and Exercise Comparison Orientation Measure [BEECOM]) in samples of Iranian men and women. In Studies 1 and 2, female (n = 284) and male (n = 302) participants completed the translated Farsi BEECOM. Scores were analyzed by exploratory factor analyses (EFA) revealing two different three factor, 15-item scale structures for men and women. In Studies 3 and 4, participants (female n = 384; male n = 253) completed measures of social comparison and psychological functioning in one session. These data were analyzed using confirmatory factor analyses (CFA) and Pearson correlations. Each CFA yielded adequately fitting models. Results support the use of two different 15-item Farsi BEECOM measures with women and men and highlight unique gender differences in social comparison tendencies and correlations with other psychological processes. The resulting F-BEECOM demonstrates strong psychometric properties and will be a useful research tool in Iranian women and men.
Keywords: Social comparison, Scale translation, Psychometrics, Iran
1. Introduction
Social comparison theory (Festinger, 1954) postulates that each individual has a fundamental desire to assess his or her ideas and capacities, and does so by comparing the self to relevant others (Festinger, 1954; Suls, Martin, & Wheeler, 2002). Social comparison is an ubiquitous social phenomenon, a psychological process that serves as a central feature of human life (Buunk & Gibbons, 2007; Suls et al., 2002). People have an innate drive to evaluate themselves in the presence of objective standards; however, when these standards are absent, individuals often draw from their immediate environment, and rely on comparison of their opinions or abilities to those of similar others (Festinger, 1954). Accordingly, targets which are very close to one’s opinions and abilities are salient and frequently used (Lin & Kulik, 2002).
1.1. Appearance-Related Comparison
Social comparison theory applies not only to comparing one’s opinions and abilities, but also to comparing outward appearance; further, there is mounting evidence supporting the negative effect of appearance-related social comparison on body image (Corning, Krumm, & Smitham, 2006; Leahey, Crowther, & Mickelson, 2007). Multiple sociocultural theories of eating disorder development, including the dual-pathway model (Stice, 2001) and tripartite influence model (Thompson, Heinberg, Altabe, & Tantleff-Dunn, 1999), propose that thin-ideal internalization has cascading influences on body dissatisfaction and disordered eating. Research suggests that social comparison is one of the mechanisms through which thin-ideal internalization leads to body dissatisfaction and disordered eating (Fitszimmons-Craft et al., 2014). Driven by sociocultural factors promoting the thin ideal, women engage in social comparison with both familiar and unfamiliar others and identify a discrepancy between their ideal and actual selves (Fitzsimmons-Craft, 2011; Fitzsimmons-Craft, Ciao, & Accurso, 2016) and may aim to address that discrepancy through disordered eating behaviors. Although less frequently studied in men, appearance-related comparison tendencies have negative consequences for both men and women (Myers & Crowther, 2009), and based on available data, women and men may engage in somewhat similar levels of general and appearance-related social comparison behavior (O’Brien et al., 2009; Warren, Schoen, & Schafer, 2010). Importantly, the tendency to engage in appearance-related comparison is associated with poor body image for both genders (Myers & Crowther, 2009).
Multiple brief scales have been developed to assess appearance-related social comparison: the Physical Appearance Comparison Scale (PACS; Thompson, Heinberg, & Tantleff, 1991), Physical Appearance Comparison Scale-Revised (PACS-R; Schaefer & Thompson, 2014), Physical Appearance Comparison Scale- last version (PACS-3; Schaefer & Thompson, 2018), Body Image Comparison Scale (BICS; Faith, Leone, & Allison, 1997), Body Comparison Scale (BCS; Fisher, & Thompson, 1998; Fisher, Dunn, & Thompson, 2002), and Social Comparison to Models (CMS; Thompson et al., 1999). These measures are associated with disordered eating, body dissatisfaction, lower self-esteem, and BMI (Garrusi & Baneshi, 2013; Hamel, Zaitsoff, Taylor, Menna, & Grange, 2012; Schaefer & Thompson, 2014; Schutz, Paxton, & Wertheim, 2002). However, all but two of these studies (Atari, Akbari-Zardkhaneh, Soufiabadi, & Mohammadi, 2015; Garrusi & Baneshi, 2013) examined appearance-related comparisons in Western samples. These intercorrelations merit further exploration to extend their generalizability to non-Western college women and men.
1.2. Eating- and Exercise-Related Comparison
It may be noted that other facets of social comparison contribute to body dissatisfaction and disordered eating. Accordingly, a growing body of literature indicates that along with appearance-related comparison, eating- and exercise-related comparison are associated with disordered eating and predict disordered eating symptoms both cross-sectionally and prospectively (Fitzsimmons-Craft, Bardone-Cone, & Harney, 2012; Fitzsimmons-Craft et al., 2014; Fitzsimmons-Craft et al., 2016). Eating-related comparisons regarding multiple dimensions of the meal experience (e.g., amount, balance, or meal healthfulness) also relate to both increased body dissatisfaction and increased dietary restraint (Fitzsimmons-Craft, 2017) and predict future body dissatisfaction (Fitzsimmons-Craft, Bardone-Cone, Wonderlich, Crosby, Engel, & Bulik, 2015). Exercise-related comparisons have a similar effect, as they correlate with body dissatisfaction and dietary restraint in college-aged women (Fitzsimmons-Craft, Bardone-Cone, et al., 2016), and also predict future body dissatisfaction (Fitzsimmons-Craft et al., 2015). Furthermore, in an experimental study examining exercise-related comparison and body dissatisfaction, Wasilenko and colleagues (2007) decreased participant body satisfaction and exercise duration by placing a fit confederate in a campus gym for participants as a possible (implicit) comparison target to compare physique and exercise intensity while engaging in physical activity.
1.3. The BEECOM: Body, Eating, and Exercise Comparison Orientation Measure
The only existing quantitative measure assessing multiple facets of ED-related social comparison (body-, eating-, and exercise-related comparisons) is the Body, Eating, and Exercise Comparison Orientation Measure (BEECOM; Fitzsimmons-Craft et al., 2012). The original BEECOM consists of three subscales with six items each: body (e.g., “I pay attention to whether or not I am as thin as, or thinner, than my peers”), eating (e.g., “I look at the amount of food my peers leave on their plate in comparison to me when they are finished eating”), and exercise (e.g., “When I am exercising (e.g., at the gym, running outdoors), I pay attention to the length of time that those around me work out”). The scale was initially developed for and normed on U.S. college women without clinical levels of eating pathology. The scale demonstrates adequate internal consistency (α =.93 to .96), construct validity with disordered eating (rs = .60 to .70) and body dissatisfaction (rs = .61 to .75), and two-week test-retest reliability (rs = .85 to .89) among college women in U.S. (Fitzsimmons-Craft et al., 2012). Scores on the measure demonstrate temporal stability and predictive validity over the course of one year by predicting unique variance in body dissatisfaction and disordered eating, over and above body mass index (BMI), general comparison tendencies, and appearance related social comparison as measured by the PACS (Thompson, Heinberg, & Tantleff, 1991; Fitzsimmons-Craft & Bardone-Cone, 2014). The scale was recently adapted for use in clinical and recovering ED female samples (Saunders, Eaton, & Fitzsimmons-Craft, 2019). To date, the BEECOM has not been administered or validated for use with men or non-Western women.
1.4. Body Dissatisfaction and Disordered Eating in Iran
Despite the early beliefs that EDs are culturally embedded syndromes, disordered eating and clinical eating disorders (EDs) are not unique to Western culture (Keel & Klump, 2003). Further, as with Western samples, sociocultural factors are associated with body dissatisfaction in Iranian college men and women (Sahlan et al., under review), including drive for thinness. Estimates of disordered eating and clinical EDs in Iran range from 4% to 11.5% (Garrusi & Baneshi, 2013; Sahlan, Akoury, & Taravatrooy, under review), with nearly a quarter of all Iranian adolescents surveyed demonstrating high ED risk (Rauof, Ebrahimi, Jafarabadi, Malek, & Kheiroddin, 2015). Further, a systematic review showed body dissatisfaction prevalence of 30-75% among Iranians, with girls, college-aged women, and higher-weight individuals demonstrating the highest prevalence (Shoraka, Amirkafi, & Garrusi, 2019). Recent findings also indicated that the regular occurrence of binge eating was 24.7% and 27.5% among Iranian college men and women, respectively (Sahlan, Taravatrooy, Quick, & Mond, 2020). As in Western samples, disordered eating behaviors in Iranian women correlate with multiple psychological symptoms, including low self-esteem and depression (Sahlan, 2016).
1.5. Appearance-Related Social Comparison in Iran
Although Iranian culture encourages the use of body-related comparison (Garrusi & Baneshi, 2013), research examining the social comparison construct in Iran is relatively sparse. To date, with respect to social comparison measures, two different Farsi versions of the PACS (PACS; Thompson et al., 1991, PACS-R; Schaefer & Thompson, 2014) and the Adolescent Comparative Body and Appearance Satisfaction Scale (ACBASS) have been administered with college women, adolescents, and a community sample of men and women in Iran (Atari et al., 2015; Atari, Jamali, Bahrami-Ehsan, & Mohammadi, 2017; Garrusi & Baneshi, 2013). The results indicate that appearance-related social comparison tendencies are significantly correlated with BMI and positive body image cognitions (Atari et al., 2015), with individuals who engage in more appearance-related social comparison reporting higher BMI and more negative body image. Another study with a community sample in Iran reported that appearance-related social comparison (measured by PACS scores; Thompson et al., 1991) predicted disordered eating (Garrusi & Baneshi, 2013). Importantly, sex differences on appearance-related social comparison (i.e., PACS) were unclear in a community sample of men and women, and strong conclusions could not be drawn (Garrusi & Baneshi, 2013). Moreover, the effects of other domains of social comparison (eating- and exercise-related), though identified as important correlates and antecedents to disordered eating in Western samples (Saunders et al., 2019), remain unexplored in Iranian samples.
Among Iranian adolescent boys and girls, ACBASS scores, assessing body-related social comparison tendencies, are negatively correlated with self-esteem and BMI (Atari et al., 2017). However, these findings are not generalizable to college students, and social comparison becomes a more salient and vulnerable behavior during college (Fitzsimmons-Craft, 2017, 2011). This change is likely more pronounced in Iranian culture, given Iranian-specific cultural norms for men and women. For example, college is the first opportunity women in Iran have to take courses with men and to use grooming products to achieve beauty standards. Because of this novel opportunity to interact with women, men in Iran increase their focus on their body upon entrance into college (Sahlan et al., under review). The college environment may put pressure on women and men to focus increasingly more on weight and also appearance-related issues. However, the role of ED-related social comparison on disordered eating behaviors in Iranian men and women remains unstudied.
1.6. Current Study
Given these identified gaps in the literature, we conducted a series of four studies to translate the English version of the BEECOM into Farsi and examine its validity and reliability in male and female Iranian samples by relating BEECOM scores to other measures of psychological functioning previously linked to body-, eating-, and exercise-related comparisons, both those related to disordered eating (body dissatisfaction, eating and weight concerns) and more global psychological functioning (self-esteem). Most of what is known about social comparison comes from Western samples. Accordingly, the translation and validation of a tool to quantify body-, eating-, and exercise-related comparisons in an Iranian, Farsi-speaking male and female sample allows for the identification of social comparison as an additional risk and maintenance factor for EDs in Iranian research and clinical practice.
2. General Method
Four studies were conducted to thoroughly evaluate the psychometric properties of the Farsi version of the BEECOM in female and male college students. In Study 1, exploratory factor analysis (EFA) was used to examine the factor structure of the F-BEECOM in a sample of Iranian women. In Study 2, confirmatory factor analysis (CFA) was used to verify the results of Study 1 in another sample of Iranian women. The validity and reliability of resulting F-BEECOM subscales was also examined. The method of Study 3 and Study 4 mirrored those of Study 1 and Study 2, except EFA (Study 3) and CFA (Study 4) were used to examine and verify the factor structure of the F-BEECOM in two samples of Iranian men. We followed the guidelines and reporting recommendations outlined in Swami and Barron (2019) for the translation and validation of body image measures. These guidelines recommend always conducting an EFA prior to a CFA, regardless of whether prior scale adaption studies have identified a consistent factor structure in other cultural groups (Swami & Barron, 2019; Worthington & Whittaker, 2006).
3. Study 1: Scale Translation and Exploration of Scale Structure in Iranian Women
The aim of Study 1 was to translate the BEECOM into Farsi and to evaluate the resulting scale’s factor structure in a sample of Iranian women.
3.1. Method
3.1.1. Participants.
Participants in Study 1 were 284 Iranian female undergraduate (77.5%, n = 220) and graduate (22.5%, n = 64) students. Participants were recruited using convenience sampling from two large metropolitan universities located in North-Western (University of Tabriz) and Capital (University of Tehran) regions of Iran. Participants in study one ranged in age from 18 to 52 (M = 21.73, SD = 4.04). Participant body mass index (BMI; kg/m2) ranged from 15.47 to 36.72 (M = 21.85, SD = 3.38).
3.1.2. Measures.
3.1.2.1. Demographic information.
Participants provided demographic information including their gender, education status, marital status, age, weight, and height. Weight and height were used by the research team to compute BMI scores for each participant.
3.1.2.2. Body, eating, and exercise comparisons.
The BEECOM (Fitzsimmons-Craft et al., 2012) consists of 18 items and three subscales (Body, Eating, and Exercise), each of which is comprised of six questions. Initial scale development results support a three factor model (Fitzsimmons-Craft et al., 2012). Higher-order factor loadings from .82 to .97 for the three subscales onto a global factor suggest that that the total score may well represent overall eating disorder-related social comparison (Fitzsimmons-Craft et al., 2012). Two-week test-retest reliability was high (rs = .85 to .89) (Fitzsimmons-Craft et al., 2012). Scores on the scale are associated with disordered eating (rs = .53 to .72), body dissatisfaction (rs = .38 to .75), negative affect (rs = .12 to .16), and BMI (rs = .14 to .20) in the literature (Fitzsimmons-Craft et al., 2012; Fitzsimmons-Craft et al., 2015; Saunders, Eaton, & Fitzsimmons-Craft, 2019).
3.1.3. Translation and procedure.
We took a universalist approach to scale translation (Herdman et al., 1997), recognizing that the construct of ED-related social comparison may be expressed differently in an Iranian sample than a Western sample. A universalist approach does not make a priori assumptions about a particular construct across cultural groups. The BEECOM (Fitzsimmons-Craft et al., 2012) was first translated from English into Farsi using the parallel back-translation procedure (Brislin, 1986). Using a combination of back-translation, committee, and pre-test procedures (Cha et al., 2007), the BEECOM was translated into Farsi by first author as well as another Clinical Psychology student, producing two possible versions of the F-BEECOM. A third translator compared these two versions and evaluated linguistic differences. Thereafter, another Clinical Psychologist who finished his M.A. and Ph.D. courses in U.S. and is familiar with Western and non-Western cultures and the corresponding literature compared the resulting version with the original BEECOM items and suggested some minor adjustments to ensure conceptual and item equivalence. The Farsi version was then back-translated by a third Clinical Psychology student and another translator, who were both unfamiliar with the scale. The original sentences of the scale and back-translated sentences were compared by a bilingual translator in Iran to determine if they held the same meaning, to demonstrate a semantic equivalence. All individuals involved in the translation and back-translation procedure were fluent in both Farsi and English. No substantial discrepancies regarding the items were found. The scale in its final Farsi version was then piloted with a small group of college students (male n = 12, female n = 16) to verify the comprehensibility, conceptual equivalence of the items, and operational equivalence of the scale format and instructions. These college students found that all the items were understandable within an Iranian context, the directions were easily followed, and that the questions contained within the measure were relevant to their daily lives. This pilot sample raised no queries that required the scale to undergo further editing.
Upon establishing and pilot-testing the F-BEECOM, potential participants from a broad range of departments (e.g., Psychology, Sociology, Agriculture, and Tourism Management) were approached on campus and given information about the study. In order to reduce the likelihood of sampling bias, the study was advertised as involving general psychology research rather than research relating specifically to disordered eating behaviors. Participants provided written informed consent and those who agreed to participate completed the paper-and-pencil version of the questionnaires, which took about 30 minutes, in the presence of the first author. Confidentiality of participant responses were ensured, as responses were anonymized and could not be linked to individual participants. This study and all studies mentioned below were approved by the ethics review board from a large Iranian university.
3.1.4. Statistical analyses.
Prior to analysis, the data were evaluated for multivariate outliers by examining leverage indices for each individual and defining an outlier as a leverage score four times greater than the centered mean leverage value; no outliers were identified. There were no missing data for any of the four studies contained within. For this and study three (below), we adhered to the sample size guidelines of Worthington and Whittaker (2006), which suggest that a sample size ranging from 150-200 participants is sufficient when extracted communalities exceed .50 or factor loadings exceed .60. In the Iranian women EFA sample, all communalities exceeded .51. The factor loadings retained were ≥ .55. The Kaiser-Meyer-Olkin measure of sampling adequacy (seeking values ≥ .80) and Bartlett’s test of sphericity (seeking p < .05) were used to assess data factorability. As we expected three correlated factors, we conducted the EFA using principal axis factoring with promax oblique rotation to examine the factor structure of the F-BEECOM and identify items to retain, appropriate analytic choice for data that violate the assumption of multivariate normality (Fabrigar, Wegener, MacCallum, & Strahan, 1999). As reported below, the data for study one violated the assumption of multivariate normality. The number of factors retained was determined by the Kaiser-Guttman criterion, which specifies that factors with eigenvalues greater than one be retained (Guttman, 1954; Kaiser, 1960), used in conjunction with parallel analysis (Hayton, Allen, & Scarpello, 2004). Items with multiple loadings ≥ .30 or a difference of less than .20 between two loadings were considered to cross-load on multiple factors and removed from the scale (Floyd & Widaman, 1995). We used SPSS 26.0 to conduct the EFAs.
3.2. Results and Discussion
Examination of the factor loadings of the 18 items indicated that three items cross-loaded on more than one factor (see Table 1). Thus, two items from the original BEECOM’s eating-related comparison subscale (Item 3: “During meals, I compare what I am eating to what others are eating” and Item 16: “I pay attention to how much junk food my peers eat compared to me”) and one item from the original BEECOM’s body-related comparison scale (Item 17: “I pay attention to whether or not I am as toned as my peers”) were removed from subsequent analyses. The Kaiser-Meyer-Olkin value of .93 and significant Bartlett’s test of sphericity, χ2(153) = 3303.56, p < .001, provided support for analyzing the Iranian women’s F-BEECOM data in an EFA. Visual examination of the scree plot, identification of eigenvalues greater than 1, and the results from the parallel analysis collectively supported the retention of a three-factor solution that explained 65.37% of the variance in F-BEECOM items. The remaining items loaded strongly onto their primary factors (loading of .55 or higher). The Iranian women’s scale resulting from the EFA consisted of 15 items across three subscales measuring body-, eating-, and exercise-related social comparison. Each of the three factors correlated highly with one another (rs = .58, .58, .57), suggesting the presence of a higher order factor.
Table 1.
EFA factor loadings of BEECOM items for women
| Items | Body | Eating | Exercise |
|---|---|---|---|
| 1. I look at the amount of food my peers leave on their plate in comparison to me when they are finished eating. | .34 | .64 | −.27 |
| 2. I pay attention to whether or not I am as thin as, or thinner, than my peers. | .80 | .03 | −.02 |
| 3. During meals, I compare what I am eating to what others are eating. | .49 | .53 | −.16 |
| 4. In social situations, I think about how my figure “matches up” to the figures of those around me. | .84 | .01 | .04 |
| 5. When I am exercising (e.g., at the gym, running outdoors), I pay attention to the length of time that those around me work out. | .14 | .08 | .60 |
| 6. I pay close attention when I hear peers talking about exercise (in order to determine if I am exercising as much as they are). | −.04 | .04 | .77 |
| 7. I find myself thinking about how my food choices compare with the food choices of my peers | −.13 | .78 | .21 |
| 8. I am quick to notice how healthy (or unhealthy) my peers’ food choices are compared to my own food choices. | −.21 | .81 | .11 |
| 9. I notice how I compare with my peers in terms of specific parts of the body (e.g., stomach, hips, breasts, etc.). | .77 | .02 | .09 |
| 10. When working out around other people, I think about how many calories I am burning in comparison to my peers. | .12 | −.02 | .73 |
| 11. When I go to the dining hall or out to eat, I pay attention to how much I am eating compared to other people. | .18 | .55 | .10 |
| 12. I compare my body shape to that of my peers. | .93 | −.09 | .05 |
| 13. When I see a peer who is wearing revealing clothing, I have thoughts of how my own body compares. | .82 | −.04 | .09 |
| 14. I like to know how often my friends are working out so I can figure out if the number of times I work out “matches up”. | −.07 | .13 | .79 |
| 15. When I exercise (e.g., at the gym, running outdoors), I pay attention to the intensity level of the workouts of those around me. | −.09 | .08 | .88 |
| 16. I pay attention to how much junk food my peers eat compared to me. | .07 | .46 | .28 |
| 17. I pay attention to whether or not I am as toned as my peers. | .38 | −.16 | .57 |
| 18. When I work out, I evaluate how hard my workout was compared to how hard my friends say they worked out. | .09 | −.05 | .83 |
Note: Bold indicates retained item. Please see Appendix A for items in Farsi.
4. Study 2: Confirmation of Factor Structure and Examination of the Reliability and Convergent Validity of the F-BEECOM for Women
The goals of Study 2 were to (1) substantiate the factor structure for women identified by the EFA in Study 1 using confirmatory methods and (2) assess the reliability and convergent validity of the new measure in a separate sample of Iranian women. Convergent validity was also assessed.
4.1. Method
4.1.1. Participants.
Women attending a large Iranian university (total n = 384) at either the undergraduate (75.5%; n = 290) or graduate (24.5%; n = 94) level participated in Study 2. Participants were recruited using convenience sampling from two large metropolitan universities located in North-Western (University of Tabriz) and South-Central (University of Shiraz) regions of Iran. Participants in Study 2 ranged in age from 18 to 54 (M = 21.91, SD = 3.90). Participant BMI (kg/m2) ranged from 15.57 to 36.73 (M = 21.74, SD = 3.42). Self-reported BMI, t(613.80) = 0.41, p = .68, d = .03, and age, t(597.73) = 0.58, p = .56, d = .05, of participants in Study 2 did not differ significantly from the self-reported BMI and age of participants in Study 1.
4.1.2. Measures.
In addition to the F-BEECOM, participants completed standardized measures of body dissatisfaction, disordered eating, and self-esteem.
4.1.2.1. Disordered eating.
The Eating Disorder Examination Questionnaire (EDE-Q) (Fairburn & Beglin, 2008) is widely used to assess body dissatisfaction and eating pathology. The items are rated on a 7-point scale ranging from 0 (No days) to 6 (Every day). Higher scores indicate higher levels of body dissatisfaction and disordered eating. The EDE-Q items have demonstrated strong psychometric properties (Lavender, De Young, & Anderson, 2010; Luce, Crowther, & Pole, 2008). The Farsi version of the EDE-Q (also known as Persian EDE-Q or P-EDE-Q) has been validated and used among both Iranian men and women (Mahmoodi et al., 2016; Sahlan et al., 2020). In the present study, the P-EDE-Q sub-scales demonstrated good internal consistency: restraint (ω = .85), eating concern (ω = .72), shape concern (ω = .88), and weight concern (ω = .79). The P-EDE-Q sub-scale factors each explained between 72% to 88% of the variance in scale scores.
4.1.2.2. Self-esteem.
The Rosenberg Self-Esteem Scale (RSES) (Rosenberg, 1965) is widely used to assess global self-esteem, which is related to self-acceptance and self-assessment (Tafarodi & Milne, 2002). The scale is comprised of 10 items rated on a 4-point Likert ranging from 1 (Strongly disagree) to 4 (Strongly agree). Higher scores indicate higher self-esteem. The scale demonstrates appropriate validity and reliability (Sinclair et al., 2010). The Persian version of the RSES (P-RSES) has been validated among both men and women in Iran (Shapurian, Hojat, & Nayerahmadi, 1987). In the present study, the P-RSES demonstrated good internal consistency: McDonald’s ω = .86 for men and ω = .90 for women.
4.1.3. Procedure.
The procedure for study two matched that of Study 1. In Study 2, participants also completed the P-RSES and P-EDE-Q in addition to the F-BEECOM and providing their demographic information.
4.1.4. Statistical analysis.
Amos 26.0 was used to conduct a CFA to verify the three-factor, 15 item scale derived from the EFA in Study 1. As each of the factors identified by the EFA were highly correlated with each other in Study 1, suggesting the presence of a higher order factor, we included this factor in the models we tested. Two Monte Carlo simulations, with different seed values, were first conducted in MPlus 6.12 to estimate statistical power given our sample size. The Monte Carlo simulations used the factor loadings obtained in Study 1. The Monte Carlo simulations used an estimated sample size of 250 participants given the smaller sample of men in study four below. The Monte Carlo simulation indicated that with a sample size of 250, our estimated power was .99. As this value exceeded Cohen’s (1992) recommendation of .80, we proceeded with our CFA in Study 2 and Study 4.
We used the root mean square error of approximation (RMSEA), comparative fit index (CFI), and standardized root mean square residual (SRMR) to evaluate model fit. Prior research supports the use of a CFI value of .95 or higher (Hu & Bentler, 1999), RMSEA value of .08 or lower (Browne & Cudeck, 1993), and SRMR values of .05 or lower (Byrne, 1998) to indicate good model fit. There were no missing data. Omega was calculated to quantify internal consistency for the resulting F-BEECOM and its subscales using JASP 0.11.00. We calculated Pearson product-moment correlations in SPSS 26.0 between F-BEECOM subscales and measures of body dissatisfaction, disordered eating, and self-esteem to assess the F-BEECOM’s construct validity, and calculated average variance extracted (AVE) to assess convergent validity. Average variance extracted is the amount of variance captured by a construct, in this case ED-related social comparison, relative to the amount of variance due to measurement error (Fornell & Larker, 1981). We anticipated moderate, positive correlations between body dissatisfaction, disordered eating, and self-esteem, as has been found in prior work, and expected AVE calculations to exceed .50, indicating that the items converge into a uniform construct (Fornell & Larker, 1981), and supporting convergent validity.
4.2. Results and Discussion
4.2.1. Confirmatory factor analysis.
The data were first evaluated for outliers, skewness, and kurtosis. Mardia’s coefficient of multivariate kurtosis exceeded the critical ratio of 1.96 (critical ratio of 46.12), indicating multivariate non-normality. To address this non-normality, the CFA was performed using maximum likelihood estimation with 1,000 bootstrapped resamples (Hancock & Liu, 2012). The model derived from the CFA fit the data marginally well: robust RMSEA = .08 [90% CI: .07, .09], robust CFI = .95, robust SRMR = .04. Theoretically meaningful modification indices suggested that allowing error variance of items on each factor to correlate would significantly improve model fit. We allowed five pairs of error terms to correlate. Upon applying these modification indices to the model, the CFI and SRMR remained the same and the RMSEA value decreased to meet Browne and Cudek’s (1993) suggested value of less than .08 with a calculated value of .07 [90% CI: 06, 08]. All factor loadings were adequate (.57-.87) and the model explained 93.7% of the variance in eating-related comparisons, 69.3% of the variance in body-related comparisons, and 61.7% of the variance in exercise-related comparisons (see Figure 1). Body-, eating-, and exercise-related comparisons each loaded strongly onto the higher-order ED-related social comparison factor. McDonald’s omega was adequate for each sub-scale, with exercise-related ω = .91, eating-related ω = .91, and body-related ω = .81. The convergent validity captured by this model was also adequate, as the AVE for the 15 items was .61, exceeding the recommended cut-off of .50 (Fornell & Larker, 1981). Women’s scores on the body-, eating-, and exercise-related comparison sub-scales were each significantly and negatively correlated with self-reported self-esteem measured by the P-RSES, significantly and positively correlated with dietary restraint and eating concern (assessing disordered eating), and significantly and positively correlated with weight and shape concern (assessing body dissatisfaction), as measured by the P-EDEQ (see Table 2). These significant correlations indicate construct validity.
Figure 1. CFA factor loadings for women. The correlations between pairs of error terms are not pictured for clarity.
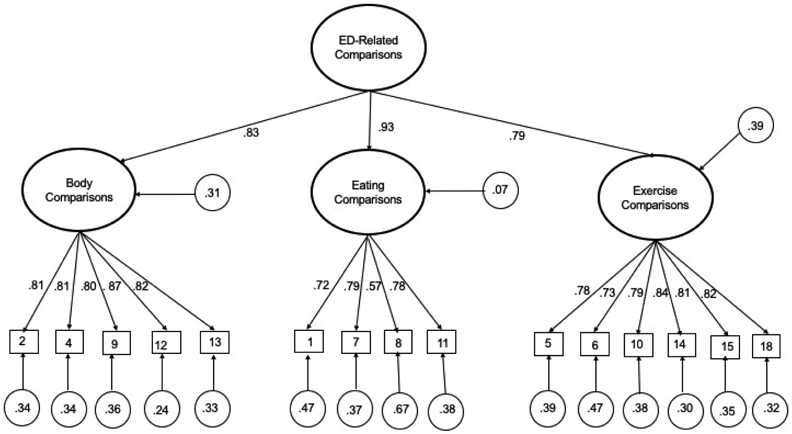
Note: Please see Appendix C for intercorrelations among error terms
Table 2.
Intercorrelations between BEECOM total and sub-scale, EDE-Q, and self-esteem scores for women
| Restraint | Eating Concern |
Shape Concern |
Weight Concern |
Total Eating Pathology |
Self- Esteem |
|
|---|---|---|---|---|---|---|
| Body | .30** | .49** | .47** | .50** | .49** | −.22** |
| Eating | .33** | .46** | .545** | .55** | .54** | −.28** |
| Exercise | .32** | .50** | .52** | .53** | .53** | −.31** |
| ED-Related Comparison Total | .36** | .55** | .59** | .60** | .59** | −.31** |
Note:
p < .01.
5. Study 3: Scale Translation and Exploration of Scale Structure in Iranian Men
The aim of Study 3 was to administer the 18 items of the translated F-BEECOM to a sample of Iranian men and to evaluate the resulting scale’s factor structure.
5.1. Method
5.1.1. Participants.
Participants in study one were 302 Iranian male undergraduate (83.8%, n = 253) and graduate (26.2%, n = 44) students. Recruitment for study three matched that of Study 1. Participants in Study 3 ranged in age from 18 to 35 (M = 21.78, SD = 2.59). Participant body mass index (BMI; kg/m2) ranged from 15.57 to 36.94 (M = 23.01, SD = 3.64).
5.1.2. Measures and procedure.
Participants completed the 18-item F-BEECOM and answered a brief demographic questionnaire. Please see Study 1 for detailed information about the measures and the translation procedure.
5.1.3. Statistical analyses.
Prior to analysis, the data were evaluated for multivariate outliers by examining leverage indices for each individual and defining an outlier as a leverage score four times greater than the centered mean leverage value; no outliers were identified. There were no missing data for any of the four studies contained within. Per Worthington and Whittaker (2006), our sample size was sufficient as our extracted communalities exceed .50 and factor loadings exceed .60. In the Iranian men EFA sample, all communalities exceeded .58. The factor loadings retained were ≥ .54. The analysis procedure followed that of Study 1.
5.2. Results and Discussion
Three items from the original BEECOM’s eating-related comparison subscale (Item 7: “I find myself thinking about how my food choices compare to the food choices of my peers;” Item 8: “I am quick to notice how healthy (or unhealthy) my peers’ food choices are compared to my own food choices;” and Item 11: When I go to the dining hall or out to eat, I pay attention to how much I am eating compared to other people”) cross-loaded on more than one factor (see Table 3), and were removed from subsequent analyses. An additional item from the eating subscale (Item 16: “I pay attention to how much junk food my peers eat compared to me”) loaded highly onto the exercise sub-scale rather than the eating sub-scale and was retained for the exercise sub-scale. The Kaiser-Meyer-Olkin value of .93 and significant Bartlett’s test of sphericity, χ2(153) = 3104.91, p < .001, provided support for analyzing the Iranian men’s F-BEECOM data in an EFA. Visual examination of the scree plot, identification of eigenvalues greater than 1, and the results from the parallel analysis collectively supported the retention of a three-factor solution that explained 62.66% of the variance in F-BEECOM items. Each of the 15 items loaded strongly onto their primary factors (loading of .54 or higher). The Iranian men’s scale resulting from the EFA consisted of 15 items across three subscales measuring body- (six items), eating- (two items), and exercise-related (seven items) social comparison. Each of the three factors correlated highly with one another (rs = .49, .53, .61), suggesting the presence of a higher order factor. Three of these 15 items were different from those retained in the EFA with women (Study 1). Given this difference, we were unable to test for metric invariance by gender in Study 4.
Table 3.
EFA factor loadings of BEECOM items for men
| Items | Body | Eating | Exercise |
|---|---|---|---|
| 1. I look at the amount of food my peers leave on their plate in comparison to me when they are finished eating. | −.05 | .83 | −.10 |
| 2. I pay attention to whether or not I am as thin as, or thinner, than my peers. | .67 | .38 | −.24 |
| 3. During meals, I compare what I am eating to what others are eating. | .08 | .80 | −.04 |
| 4. In social situations, I think about how my figure “matches up” to the figures of those around me. | .78 | .18 | −.09 |
| 5. When I am exercising (e.g., at the gym, running outdoors), I pay attention to the length of time that those around me work out. | −.02 | .19 | .63 |
| 6. I pay close attention when I hear peers talking about exercise (in order to determine if I am exercising as much as they are). | −.13 | .20 | .75 |
| 7. I find myself thinking about how my food choices compare with the food choices of my peers | −.04 | .53 | .39 |
| 8. I am quick to notice how healthy (or unhealthy) my peers’ food choices are compared to my own food choices. | −.02 | .51 | .31 |
| 9. I notice how I compare with my peers in terms of specific parts of the body (e.g., stomach, hips, breasts, etc.). | .74 | −.11 | .20 |
| 10. When working out around other people, I think about how many calories I am burning in comparison to my peers. | .05 | −.08 | .78 |
| 11. When I go to the dining hall or out to eat, I pay attention to how much I am eating compared to other people. | .40 | .20 | .22 |
| 12. I compare my body shape to that of my peers. | .90 | −.04 | −.05 |
| 13. When I see a peer who is wearing revealing clothing, I have thoughts of how my own body compares. | .86 | −.14 | .09 |
| 14. I like to know how often my friends are working out so I can figure out if the number of times I work out “matches up”. | .02 | −.11 | .86 |
| 15. When I exercise (e.g., at the gym, running outdoors), I pay attention to the intensity level of the workouts of those around me. | .03 | −.06 | .86 |
| 16. I pay attention to how much junk food my peers eat compared to me. | .05 | .17 | .54 |
| 17. I pay attention to whether or not I am as toned as my peers. | .74 | −.06 | .18 |
| 18. When I work out, I evaluate how hard my workout was compared to how hard my friends say they worked out. | .13 | −.14 | .82 |
Note: Bold indicates retained item. Please see Appendix B for items in Farsi.
5. Study 4: Confirmation of Factor Structure and Examination of the Reliability and Convergent Validity of the F-BEECOM for Men
The goals of Study 4 were to (1) substantiate the factor structure for men identified by the EFA in study three using confirmatory methods and (2) assess the reliability and convergent validity of the new measure in a separate sample of Iranian men.
5.1. Method
5.1.1. Participants.
Men attending a large Iranian university (total n = 253) at either the undergraduate (79.1%; n = 200) or graduate (21.9%; n = 53) participated in Study 4. Recruitment mirrored that of Study 2. Participants in Study 4 ranged in age from 18 to 38 (M = 21.87, SD = 3.17). Participant BMI (kg/m2) ranged from 15.85 to 39.18 (M = 22.88, SD = 3.51). One participant failed to provide weight and height information, precluding calculation of his BMI. Self-reported BMI, t(542.18) = 0.43, p = .67, d = .04, and age, t(485.54) = 0.36, p = .71, d = .03, of participants in Study 4 did not differ significantly from the self-reported BMI and age of participants in Study 3.
5.1.2. Measures, procedure, and statistical analysis.
The measures used in Study 4 were the same as in Study 2: F-BEECOM, P-RSES, and P-EDEQ. For this sub-sample of men, each of the measures demonstrated adequate internal consistency. The P-EDE-Q sub-scales yielded McDonald’s omega values above .70: restraint (ω = .81), eating concern (ω = .71), shape concern (men ω = .82), and weight concern men ω = .82). For the P-RSES, McDonald’s ω = .86. The procedure of Study 4 also matched that of Study 2. We conducted the CFA for Study 4 using the same methods and recommended guidelines for fit statistics and convergent validity as described in Study 2.
5.2. Results and Discussion
5.2.1. Confirmatory factor analysis.
The data were first evaluated for outliers, skewness, and kurtosis. Mardia’s coefficient of multivariate kurtosis exceeded the critical ratio of 1.96 (critical ratio of 47.65), indicating multivariate non-normality. To address this non-normality, the CFA was performed with maximum likelihood estimation and 1,000 bootstrapped resamples (Hancock & Liu, 2012). The model derived from the EFA, including a higher order factor given the strength of the correlations between factors, fit the data marginally well: robust RMSEA = .09 [90% CI: .07, .10], robust CFI = .94, robust SRMR = .05. Theoretically meaningful modification indices suggested that allowing error variance of three pairs of items on the exercise factor to correlate would significantly improve model fit. Upon applying these modification indices to the model, the model fit the data well: robust RMSEA = .07 [90% CI: .06, .09], robust CFI = .96, robust SRMR = .04. All factor loadings were adequate (.60-.94) and the model explained 59.9% of the variance in eating-related comparisons, 87.4% of the variance in body-related comparisons, and 70.4% of the variance in exercise-related comparisons (see Figure 2). Body-, eating-, and exercise-related comparisons each loaded strongly onto the higher-order ED-related social comparison factor. Omega was adequate for each sub-scale, with exercise-related ω = .90, eating-related ω = .84, and body-related ω = .90. The convergent validity captured by this model was also adequate, as the AVE for the 15 items was .60, exceeding the recommended cut-off of .50. Men’s scores on the body-, eating-, and exercise-related comparison sub-scales were each significantly and positively correlated with dietary restraint, eating, weight, and shape concern measured by the P-EDEQ (see Table 4), indicating construct validity. Notably, only the body-related social comparison subscale of the BEECOM was significantly related to men’s self-esteem scores.
Figure 2. CFA factor loadings for men.
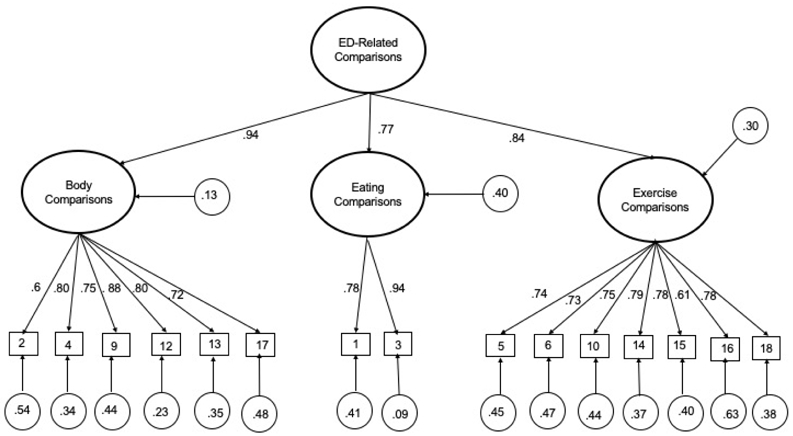
Note: Please see Appendix D for intercorrelations among error terms
Table 4.
Intercorrelations between BEECOM total and sub-scale, dietary restraint, eating, shape, and weight concern, total eating pathology, and self-esteem scores for men
| Restraint | Eating Concern |
Shape Concern |
Weight Concern |
Total Eating Pathology |
Self- Esteem |
|
|---|---|---|---|---|---|---|
| Body | .21** | .25** | .52** | .46** | .42** | −.13* |
| Eating | .20** | .23** | .41** | .41** | .37** | −.04 |
| Exercise | .27** | .26** | .38** | .42** | .40** | −.08 |
| ED-Related Comparison Total | .26** | .29** | .50** | .50** | .49** | −.11 |
Note:
p<.01
p<.05.
6. Discussion
This is the first known study to translate the BEECOM into Farsi and examine the validity and reliability of the F-BEECOM in Iranian men and women. This is therefore the first to examine eating-related and exercise-related comparisons in men and a non-Western sample. Results revealed two different three-factor structures of the F-BEECOM, retaining the body-, eating-, and exercise-related comparison sub-scales with different items removed for men and women due to differences in cross-loading items by gender. This gender difference resulted in two separate scales, and the inability to assess metric invariance. The F-BEECOM scores showed adequate internal consistency and excellent convergent validity for Iranian college men and women. In light of the global-level prevalence of body dissatisfaction (Shoraka et al., 2019) and disordered eating (Garrusi & Baneshi; 2013; Sahlan et al., 2020) in Iran, these findings pave the way for future research in identifying body dissatisfaction and disordered eating risk in this unique cultural group.
Interestingly, all the items of exercise-related comparison sub-scale (for both women and men) and body-related social comparison subscales (for women) loaded strongly onto their primary factors. However, there were also items that did not load onto their respective factors, suggesting the presence of cultural specificity. For example, the results indicated that items focusing on comparing what is eaten in women and eating out in men were related to body-related social comparison, eating-related social comparison, as well as exercise--related social comparison. Further, items focused on comparing food choices, noticing healthy (or unhealthy) food choices in men, being toned in women, and junk foods in both men and women were implicated in exercise-related comparisons. This may be reflective of prior findings that both indicate that athletic-ideal internalization is higher in Iran than in most Western societies (e.g., Sahlan, under review; Schaefer et al., 2018) and that exercise-related behaviors implicated in disordered eating symptoms are on the rise among Iranian college women and men (Rauof et al., 2015; Sahlan et al., 2020).
The F-BEECOM subscales and its global score were associated with body dissatisfaction and disordered eating which aligned with prior literature in U.S. college women (Fitzsimmons-Craft et al., 2012; Fitzsimmons-Craft et al., 2014; Fitzsimmons-Craft et al., 2015). In prior research with a community sample in Iran, body-related comparison predicted disordered eating (Garrusi & Baneshi, 2013). The current findings extend this body of literature, as multiple types of social comparisons were salient among and related to disordered eating cognitions among not only Iranian college-aged women but also men. This is of special importance, as clinical indicators (Luce & Crowther, 1999) of disordered eating among college women in Iran are increasing (4%; Sahlan et al., under review) and nearly match or exceed those seen in Western societies among college-aged samples (5-6%; Habashy & Culbert, 2019; Quick & Byrd-Bredbenner, 2013). In recent research, both Iranian college men and women reported binge eating, dietary restriction, and laxative misuse, and men endorsed greater self-induced vomiting and driven exercise than women (Sahlan et al., 2020). This behavior is likely maintained by continued engagement in body-, eating-, and exercise-related social comparison, as these comparisons have been implicated as both a risk and maintenance factor for disordered eating in U.S. college women (Fitzsimmons-Craft et al., 2016). However, future research should examine the prospective and predictive power of these comparisons as risk and maintenance factors; such conclusions cannot be drawn from the current, cross-sectional data. The current findings extend those from Western samples; multiple domains of social comparison (i.e., body, eating, exercise) appear to be maintenance and risk factors for body dissatisfaction and disordered eating in Iranian college students, despite the differences in cultural norms.
With respect to the F-BEECOM subscales and their association with self-esteem across genders in Iran, it appears that engaging in social comparison about eating and exercise is related to general self-esteem in Iranian women but not men. This finding aligns with prior literature correlating higher social comparison tendencies with lower self-esteem in women (Corning et al., 2006; Gibbons & Buunk, 1999; Pokrajac-Bulian et al., 2008; Schutz et al., 2002). College women who have lower self-esteem are more likely to compare not only their bodies and appearance but also their eating and exercise patterns with others in their day-to-day environments. Only body-related social comparison was related to self-esteem in Iranian men, which is surprising. Accordingly, it may illustrate that a different and as yet unmeasured psychological mechanism (i.e., affect) is implicated in the relation between eating- and exercise-related comparisons and self-esteem in this understudied population.
6.1. Limitations and Future Directions
Some limitations of the current study should be addressed in the future. First, this research relied on convenience samples of Iranian college students, which may have introduced sampling bias (e.g., participants may have self-selected or declined to participate based on the salience of the assessed constructs to them; students who are frequently present on campus and have the time to volunteer for a study may not represent the entire student body). Second, social comparison among university students may diverge substantially from the general population, preventing the generalization of the results to all Iranian adults. Additional data concerning the students’ socio-economic status, religiosity, attitudes towards hijab/modest dress, or place of origin, may have further informed our findings. This limitation in study design makes further conclusions on differences between Iranian college students and general population impossible. Although we also administered items that address the thin-ideal, and not the athletic-ideal, to a sample of men, these items were retained and psychometrically sound measures of male body-related comparison tendencies. It is likely necessary for further revisions of the scale for Iranian men, to account for both uniquely male aspects of social comparison and uniquely Iranian aspects of social comparison. Further, test-retest reliability of the F-BEECOM was not examined to establish whether the scale is stable over time, but given prior research (Fitzsimmons-Craft et al., 2012), scores on the F-BEECOM are likely consistent over time. Finally, no scale was used to examine discriminant validity of the F-BEECOM scores.
Accordingly, future studies should replicate this study in a random community sample of adolescent and adult Iranians and examine how differences in age, income, regions of origin, education, religiosity, attitudes towards hijab/modest dress, and other factors affect the relation between ED-related social comparison and body dissatisfaction and disordered eating. Likewise, validation of the F-BEECOM in a clinical sample of eating disordered Iranians is a necessary next step to assess the appropriateness of using the scale in clinical settings. Future research into the interrelations between eating- and exercise-related comparisons and self-esteem in men is also important. Lastly, including another scale to examine discriminant validity of the BEECOM scores would be strengthen future studies.
To help contextualize the current findings, we recommend future inquiries into (1) Iranian mainstream and social media to elucidate the presence of mainstream Western body ideals therein; (2) Iranians’ attitudes towards the hijab/modest dress mandate and its influences on body image and social comparison, in order to disentangle the effects the hijab from religiosity or reduced body scrutiny; (3) the relationships between these variables using experimental or longitudinal designs, to establish causal chains.
6.2. Conclusion
These limitations notwithstanding, the current study examines the validity and reliability of the F-BEECOM and points to the importance of considering social comparison as a risk and maintenance factor for body dissatisfaction and disordered eating in both women and men from Iran. While further investigation is needed, the findings lend support to the idea that in Iran, as in Western samples, ED-related social comparison (body-, eating-, and exercise-related) is strongly correlated with disordered eating outcomes in both men and women. If occurring, these comparisons should be addressed in a clinical setting, regardless of the client’s cultural background.
Appendix
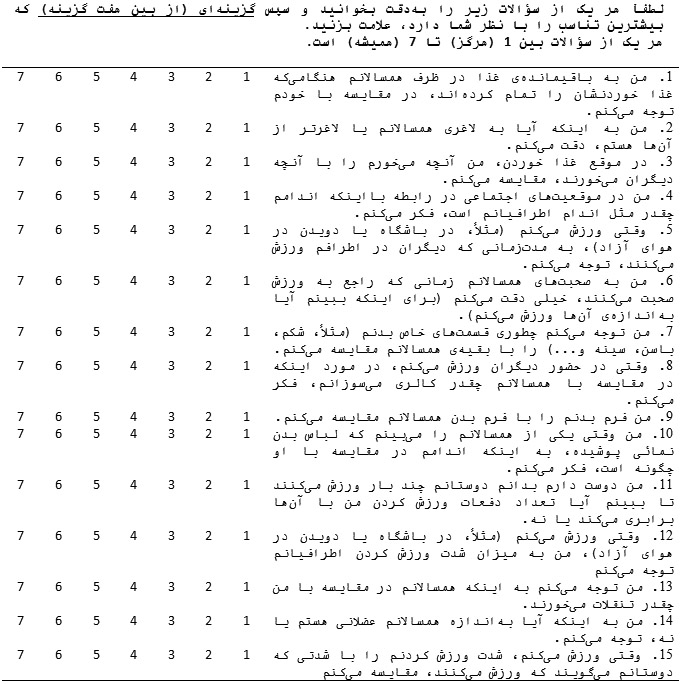
Appendix A.
Translated 15 items in Farsi among women.
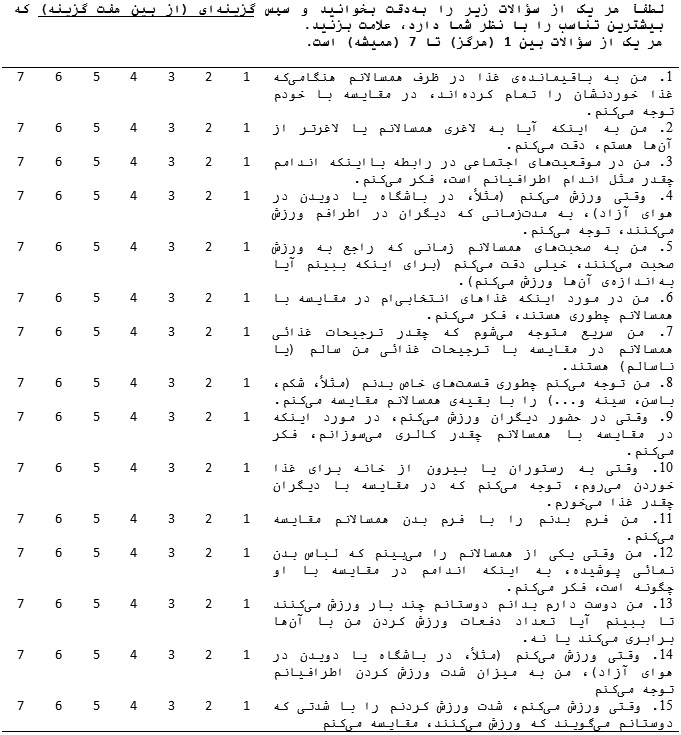 |
Appendix B.
Translated 15 items in Farsi among men.
 |
Appendix C.
Error term correlations in Women’s CFA
| Pair of Items | r |
|---|---|
| Item 1 and Item 8 | .14* |
| Item 2 and Item 4 | .19* |
| Item 2 and Item 9 | .20** |
| Item 5 and Item 6 | .26*** |
| Item 6 and Item 15 | .12* |
Note:
p < .001
p < .01
p < .05.
Appendix D.
Error term correlations in Men’s CFA
Note:
p < .001
p < .01
p < .05.
Reference
- Atari M, Akbari-Zardkhaneh S, Soufiabadi M, & Mohammadi L (2015). Cross-cultural adaptation of the physical appearance comparison scale-revised in Iran. International Journal of Body, Mind and Culture, 2(2), 115–124. doi: 10.22122/ijbmc.v2i2.27 [DOI] [Google Scholar]
- Atari M, Jamali R, Bahrami-Ehsan H, & Mohammadi L (2017). Development and validation of Adolescent Comparative Body and Appearance Satisfaction Scale (ACBASS). Current Psychology, 36(3), 637–648. doi: 10.1007/s12144-016-9452-0 [DOI] [Google Scholar]
- Brislin RW (1986). The wording and translation of research instruments. In Lonner W & Berry J (Eds.), Field methods in cross-cultural research (pp. 137–164). Beverly Hills, CA: Sage. [Google Scholar]
- Browne MW, & Cudeck R (1993). Alternative ways of assessing model fit. Sage Focus Editions, 154, 136–136. [Google Scholar]
- Buunk AP, & Gibbons FX (2007). Social comparison: The end of a theory and the emergence of a field. Organizational Behavior and Human Decision Processes, 102(1), 3–21. https://psycnet.apa.org/doi/10.1016/j.obhdp.2006.09.007 [Google Scholar]
- Byrne BM (1998), Structural equation modeling with LISREL, PRELIS and SIMPLIS: Basic concepts, applications and programming. Mahwah, New Jersey: Lawrence Erlbaum Associates. [Google Scholar]
- Cha ES, Kim KH, & Erlen JA (2007). Translation of scales in cross-cultural research: Issues and techniques. Journal of Advanced Nursing, 58, 386–395. doi: 10.1111/j.1365-2648-2007.04242.x [DOI] [PubMed] [Google Scholar]
- Cohen J (1992). A power primer. Psychological Bulletin, 112(1), 155–159. [DOI] [PubMed] [Google Scholar]
- Corning AF, Krumm AJ, & Smitham LA (2006). Differential social comparison processes in women with and without eating disorder symptoms. Journal of Counseling Psychology, 53(3), 338–349. doi: 10.1037/0022-0167.53.3.338 [DOI] [Google Scholar]
- Fairburn CG, & Beglin SJ (2008). Eating Disorder Examination Questionnaire (EDE-Q 6.0). In Fairburn CG (Ed.), Cognitive behavior therapy and eating disorders (pp. 309–313). New York: Guilford Press. [Google Scholar]
- Faith MS, Leone MA, & Allison DB (1997). The effects of self-generated comparison targets, BMI, and social comparison tendencies on body image appraisal. Eating Disorders, 5(2), 128–140. doi: 10.1080/10640269708249216 [DOI] [Google Scholar]
- Fabrigar LR, Wegener DT, MacCallum RC, Strahan EJ (1999). Evaluating the use of exploratory factor analysis in psychological research. Psychological Methods, 4, 272–299. doi: 10.1037/1082-989X.4.3.272 [DOI] [Google Scholar]
- Festinger L (1954). A theory of social comparison processes. Human Relations, 7, 117–140. https://psycnet.apa.org/doi/10.1177/001872675400700202 [Google Scholar]
- Fisher E, & Thompson JK (1998). Social comparison and body image: An investigation of body comparison processes using multidimensional scaling. Unpublished manuscript, University of South Florida. [Google Scholar]
- Fisher E, Dunn M, & Thompson JK (2002). Social comparison and body image: An investigation of body comparison processes using multidimensional scaling. Journal of Social and Clinical Psychology, 21(5), 566–579. doi: 10.1521/jscp.21.5.566.22618 [DOI] [Google Scholar]
- Fitzsimmons-Craft EE (2017). Eating disorder-related social comparison in college women's everyday lives. International Journal of Eating Disorders, 50(8), 893–905. doi: 10.1002/eat.22725 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fitzsimmons-Craft EE (2011). Social psychological theories of disordered eating in college women: Review and integration. Clinical Psychology Review, 31(7), 1224–1237. 10.1016/j.cpr.2011.07.011 [DOI] [PubMed] [Google Scholar]
- Fitzsimmons-Craft EE & Bardone-Cone AM (2014). One-year temporal stability and predictive and incremental validity of the Body, Eating, and Exercise Comparison Orientation Measure (BEECOM) among college women. Body Image, 11, 27–35. doi: 10.1016/j.bodyim.2013.09.003 [DOI] [PubMed] [Google Scholar]
- Fitzsimmons-Craft EE, Bardone-Cone AM, Bulik CM, Wonderlich SA, Crosby RD, & Engel SG (2014). Examining an elaborated sociocultural model of disordered eating among college women: The roles of social comparison and body surveillance. Body Image, 11(4), 488–500. doi: 10.1016/j.bodyim.2014.07.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fitzsimmons-Craft EE, Bardone-Cone AM, & Harney MB (2012). Development and validation of the Body, Eating, and Exercise Comparison Orientation Measure (BEECOM) among college women. Body Image, 9(4), 476–487. doi/ 10.1016/j.bodyim.2012.07.007 [DOI] [PubMed] [Google Scholar]
- Fitzsimmons-Craft EE, Bardone-Cone AM, Wonderlich SA, Crosby RD, Engel SG, & Bulik CM (2015). The relationships among social comparisons, body surveillance, and body dissatisfaction in the natural environment. Behavior Therapy, 46(2), 257–271. doi: 10.1016/j.beth.2014.09.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fitzsimmons‐Craft EE, Ciao AC, & Accurso EC (2016). A naturalistic examination of social comparisons and disordered eating thoughts, urges, and behaviors in college women. International Journal of Eating Disorders, 49(2), 141–150. 10.1002/eat.22486 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Floyd FJ, & Widaman KF (1995). Factor analysis in the development and refinement of clinical assessment instruments. Psychological Assessment, 7(3), 286–299. [Google Scholar]
- Fornell C, & Larcker DF (1981). Evaluating structural equation models with unobserved variables and measurement error. Journal of Marketing Research, 18(1), 39–50. [Google Scholar]
- Garrusi B, & Baneshi MR (2013). Eating disorders and their associated risk factors among Iranian population - a community based study. Global Journal of Health Science, 5(1), 193–202. doi: 10.5539/gjhs.v5n1p193 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibbons FX, & Buunk BP (1999). Individual differences in social comparison: Development of a scale of social comparison orientation. Journal of Personality and Social Psychology, 76(1), 129–142. doi: 10.1037/0022-3514.76.1.129 [DOI] [PubMed] [Google Scholar]
- Guttman L (1954). Some necessary conditions for common-factor analysis. Psychometrika, 19(2), 149–161. [Google Scholar]
- Habashy J, & Culbert KM (2019). The role of distinct facets of perfectionism and sociocultural idealization of thinness on disordered eating symptoms. Journal of Social and Clinical Psychology, 38(4), 343–365. 10.1521/jscp.2019.38.4.343 [DOI] [Google Scholar]
- Hamel AE, Zaitsoff SL, Taylor A, Menna R, & Grange DL (2012). Body-related social comparison and disordered eating among adolescent females with an eating disorder, depressive disorder, and healthy controls. Nutrients, 4(9), 1260–1272. 10.3390/nu4091260 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayton JC, Allen DG, & Scarpello V (2004). Factor retention decisions in exploratory factor analysis: A tutorial on parallel analysis. Organizational Research Methods, 7, 191–205, 10.1177/1094428104263675 [DOI] [Google Scholar]
- Herdman M, Fox-Rushby J, & Badia X (1997). ‘Equivalence’and the translation and adaptation of health-related quality of life questionnaires. Quality of Life Research, 6(3), 237–247. doi: 10.1023/a1026410721664 [DOI] [PubMed] [Google Scholar]
- Hu L, & Bentler PM (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1–55. 10.1080/10705519909540118 [DOI] [Google Scholar]
- Kaiser HF (1960). The application of electronic computers to factor analysis. Educational and Psychological Measurement, 20(1), 141–151. [Google Scholar]
- Keel PK, & Klump KL (2003). Are eating disorders culture-bound syndromes? Implications for conceptualizing their etiology. Psychological Bulletin, 129(5), 747–769. doi: 10.1037/0033-2909.129.5.747 [DOI] [PubMed] [Google Scholar]
- Lavender JM, De Young KP, & Anderson DA (2010). Eating Disorder Examination Questionnaire (EDE-Q): Norms for undergraduate men. Eating Behaviors, 11(2), 119–121. doi: 10.1016/j.eatbeh.2009.09.005 [DOI] [PubMed] [Google Scholar]
- Leahey TM, Crowther JH, & Mickelson KD (2007). The frequency, nature, and effects of naturally occurring appearance-focused social comparisons. Behavior Therapy, 38(2), 132–143. 10.1016/j.beth.2006.06.004 [DOI] [PubMed] [Google Scholar]
- Lin LF, & Kulik JA (2002). Social comparison and women's body satisfaction. Basic and Applied Social Psychology, 24(2), 115–123. doi: 10.1207/S15324834BASP2402_4 [DOI] [Google Scholar]
- Luce KH, & Crowther JH (1999). The reliability of the Eating Disorder Examination-Self-report questionnaire version (EDE-Q). International Journal of Eating Disorders, 25(3), 349–351. doi: [DOI] [PubMed] [Google Scholar]
- Luce KH, Crowther JH, & Pole M (2008). Eating Disorder Examination Questionnaire (EDE-Q): Norms for undergraduate women. International Journal of Eating Disorders, 41(3), 273–276. doi: 10.1002/eat.20504 [DOI] [PubMed] [Google Scholar]
- Mahmoodi M, Moloodi R, Ghaderi A, Babai Z, Saleh Z, Alasti H, & Mohammadpour Z (2016). The Persian version of Eating Disorder Examination Questionnaire and Clinical Impairment Assessment: Norms and psychometric properties for undergraduate women. Iranian Journal of Psychiatry, 11(2), 67–74. PMID: 27437002; PMCID: PMC4947222 [PMC free article] [PubMed] [Google Scholar]
- Myers TA, & Crowther JH (2009). Social comparison as a predictor of body dissatisfaction: A meta-analytic review. Journal of Abnormal Psychology, 118(4), 683. https://psycnet.apa.org/doi/10.1037/a0016763 [DOI] [PubMed] [Google Scholar]
- O’Brien KS, Caputi P, Minto R, Peoples G, Hooper C, Kell S, & Sawley E (2009). Upward and downward physical appearance comparisons: Development of scales and examination of predictive qualities. Body Image, 6(3), 201–206. 10.1016/j.bodyim.2009.03.003 [DOI] [PubMed] [Google Scholar]
- Pokrajac-Bulian A, Ambrosi-Randić N, & Kukić M (2008). Thin-ideal internalization and comparison process as mediators of social influence and psychological functioning in the development of disturbed eating habits in Croatian college females. Psihologijske Teme, 17(2), 221–245. https://hrcak.srce.hr/32440 [Google Scholar]
- Prior KL, Erceg-Hurn DM, Raykos BC, Egan SJ, Byrne S, & McEvoy PM (2018). Validation of the clinical perfectionism questionnaire in an eating disorder sample: A bifactor approach. International Journal of Eating Disorders, 51(10), 1176–1184. doi: 10.1002/eat.22892 [DOI] [PubMed] [Google Scholar]
- Quick VM, & Byrd-Bredbenner C (2013). Eating Disorders Examination Questionnaire (EDE-Q): Norms for US college students. Eating and Weight Disorders, 18(1), 29–35. doi: 10.1007/s40519-013-0015-1 [DOI] [PubMed] [Google Scholar]
- Raouf M, Ebrahimi H, Jafarabadi MA, Malek A, & Kheiroddin JB (2015). Prevalence of eating disorders among adolescents in the northwest of Iran. Iranian Red Crescent Medical Journal, 17(10), e19331. doi: 10.5812/ircmj.19331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenberg M (1965). Society and the adolescent self-image. Princeton, NJ: Princeton University Press. doi: 10.1126/science.148.3671.804 [DOI] [Google Scholar]
- Sahlan RN (2016). Comparison of overvaluation of weight and shape, self-esteem, weight bias internalization in obese women patients with and without binge eating disorder and a normal-weight control group. MSc thesis (unpublished), Iran University of Medical Sciences, Tehran, Iran. [Google Scholar]
- Sahlan RN, Akoury LM, & Taravatrooy F Validation of the Farsi version of the Sociocultural Attitudes Towards Appearance Questionnaire-4 (F-SATAQ-4) in a sample of male and female students from Iran. Under review. [DOI] [PubMed] [Google Scholar]
- Sahlan RN, Taravatrooy F, Quick V, & Mond JM (2020). Eating-disordered behavior among male and female college students in Iran. Eating Behaviors, 37, 101378. doi: 10.1016/j.eatbeh.2020.101378 [DOI] [PubMed] [Google Scholar]
- Saunders JF, Eaton AA, & Fitzsimmons-Craft EE (2019). Body-, eating-, and exercise-related comparisons during eating disorder recovery and validation of the BEECOM-R. Psychology of Women Quarterly, 43(4), 494–508. 0361684319851718. doi: 10.1177/0361684319851718 [DOI] [Google Scholar]
- Schaefer LM, Burke NL, Anderson LM, Thompson JK, Heinberg LJ, Bardone-Cone AM, Paxton SJ (2018). Comparing internalization of appearance ideals and appearance-related pressures among women from the United States, Italy, England, and Australia. Eating and Weight Disorders, 24, 947–951. doi: 10.1007/s40519-018-0544-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schaefer LM, & Thompson JK (2018). The development and validation of the Physical Appearance Comparison Scale–3 (PACS-3). Psychological Assessment, 30(10), 1330–1341. 10.1037/pas0000576 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schaefer LM, & Thompson JK (2014). The development and validation of the Physical Appearance Comparison Scale-Revised (PACS-R). Eating Behaviors, 15(2), 209–217. 10.1016/j.eatbeh.2014.01.001 [DOI] [PubMed] [Google Scholar]
- Schutz HK, Paxton SJ, & Wertheim EH (2002). Investigation of body comparison among adolescent girls. Journal of Applied Social Psychology, 32(9), 1906–1937. doi: 10.1111/j.1559-1816.2002.tb00264.x [DOI] [Google Scholar]
- Shapurian R, Hojat M, & Nayerahmadi H (1987). Psychometric Characteristics and dimensionality of a Persian version of Rosenberg Self-Esteem Scale. Perceptual and Motor Skills, 65(1), 27–34. doi: 10.2466/pms.1987.65.1.27 [DOI] [PubMed] [Google Scholar]
- Shoraka H, Amirkafi A, & Garrusi B (2019). Review of body image and some of contributing factors in Iranian population. International Journal of Preventive Medicine, 10, 19–19. doi: 10.4103/ijpvm.IJPVM_293_18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sinclair SJ, Blais MA, Gansler DA, Sandberg E, Bistis K, & LoCicero A (2010). Psychometric properties of the Rosenberg Self-Esteem Scale: Overall and across demographic groups living within the United States. Evaluation and Health Professions, 33(1), 56–80. doi: 10.1177/0163278709356187 [DOI] [PubMed] [Google Scholar]
- Stice E (2001). A prospective test of the dual-pathway model of bulimic pathology: Mediating effects of dieting and negative affect. Journal of Abnormal Psychology, 110(1), 124–130. doi: 10.1037//0021-843x.110.1.124 [DOI] [PubMed] [Google Scholar]
- Suls J, Martin R, & Wheeler L (2002). Social comparison: Why, with whom, and with what effect? Current Directions in Psychological Science, 11(5), 159–163. 10.1111/1467-8721.00191 [DOI] [Google Scholar]
- Swami V, & Barron D (2019). Translation and validation of body image instruments: Challenges, good practice guidelines, and reporting recommendations for test adaptation. Body Image, 31, 204–220. doi: 10.1016/j.bodyim.2018.08.014 [DOI] [PubMed] [Google Scholar]
- Tafarodi RW, & Milne AB (2002). Decomposing global self-esteem. Journal of Personality, 70(4), 443–484. doi: 10.1111/1467-6494.05017 [DOI] [PubMed] [Google Scholar]
- Thompson JK, Heinberg LJ, Altabe M, & Tantleff-Dunn S (1999). Exacting beauty: Theory, assessment, and treatment of body image disturbance. Washington DC: American Psychological Association. doi: doi: 10.1037/10312-000. [DOI] [Google Scholar]
- Thompson JK, Heinberg L, & Tantleff S (1991). The Physical Appearance Comparison Scale (PACS). The Behavior Therapist, 14(174). https://scholarcommons.usf.edu/psy_facpub/2116 [Google Scholar]
- Warren CS, Schoen A, & Schafer KJ (2010). Media internalization and social comparison as predictors of eating pathology among Latino adolescents: The moderating effect of gender and generational status. Sex Roles, 63(9-10), 712–724. 10.1007/s11199-010-9876-1 [DOI] [Google Scholar]
- Wasilenko KA, Kulik JA, & Wanic RA (2007). Effects of social comparisons with peers on women’s body satisfaction and exercise behavior. International Journal of Eating Disorders, 40, 740–745. doi: 10.1002/eat.20433 [DOI] [PubMed] [Google Scholar]
- Worthington R, & Whittaker T (2006). Scale development research: A content analysis and recommendations for best practice. The Counseling Psychologist, 34, 806–838. doi: 10.1177/0011000006288127 [DOI] [Google Scholar]