

Abstract
Blastic plasmacytoid dendritic cell neoplasm (BPDCN) is a rare hematopoietic neoplasm whose immunophenotype remains incompletely characterized, particularly with regards to its distinction from reactive plasmacytoid dendritic cells (PDC). This limitation complicates detection of low-level involvement by BPDCN as well as minimal residual disease (MRD) assessment following therapy. We conducted the current study to characterize the immunophenotype of BPDCN in a cohort of 39 patients, and compared it to that of reactive PDC. We found that, in addition to CD56 expression (97%), BPDCN showed a number of aberrancies, including decreased/negative CD38 (82%), positive CD7 (64%), negative CD2 (81%), negative CD303 (56%), increased HLA-DR (69%) and decreased CD123 (78%) expression. Although BPDCN cells were characterized by CD56 expression, reactive PDC consistently included a CD56+ subset, ranging from 1.3%-20% (median 4.5%) of all PDC, challenging the detection of MRD. These CD56+ reactive PDC were, however, consistently positive for CD2 and CD303, brightly positive for CD38, and negative for CD7, distinctively different from BPDCN. Based on these findings, we set up a ten-color flow cytometry assay for BPDCN and validated it to a sensitivity of 0.01%. This panel was prospectively tested in 19 bone marrow samples from seven patients with BPDCN, and it effectively distinguished BPDCN cells from background reactive PDC in all cases. In summary, by understanding the immunophenotype of reactive and neoplastic PDC, BPDCN can be effectively detected by flow cytometry to a very low level using a panel of markers in addition to CD56. Such an assay could be used for initial bone marrow workup as well as MRD detection after therapy.
Introduction
Blastic plasmacytoid dendritic cell neoplasm (BPDCN) is a rare, clinically aggressive neoplasm derived from non-activated precursors of plasmacytoid dendritic cells (PDC).1,2 Patients often present with a widespread disease involving multiple anatomic sites, most commonly the skin, followed by bone marrow (BM), peripheral blood and lymph nodes.1,3-5 BPDCN can occur at any age, but mostly affects patients in their seventh decade of life.
The diagnosis of BPDCN relies on morphology in combination with immunophenotypic studies.6 BPDCN cells are medium-sized with immature chromatin, resembling lymphoblasts or myeloblasts. They often show cytoplasmic vacuoles and pseudopodia, but these are neither sensitive nor specific features as they may also be present in a variety of other hematolymphoid neoplasms. Immunophenotypically, BPDCN cells are typically positive for CD4, CD56, CD123, HLA-DR, TCL1, and TCF4, and are negative for lineage-specific antigens for B cells (e.g., CD19), T cells (surface and cytoplasmic CD3) as well as myeloid cells (myeloperoxidase).3,8 Monocytic markers such as CD64 are also negative. Our group has recently demonstrated that co-expression of CD123 and TCF4, as determined by immunohistochemistry constitutes a highly reliable marker for BPDCN.9
Despite significant advances in immunophenotypic characterization of BPDCN at baseline, data regarding the distinction between reactive/normal PDC and BPDCN cells remain limited. This limitation raises diagnostic challenges particularly in the evaluation of BM samples with a minimal disease burden, either at presentation in patients with predominantly extramedullary disease or after therapy in patients evaluated for measurable/minimal residual disease (MRD). With advances in treatment options for BPDCN patients and the importance of achievement of disease remission for allogeneic stem cell therapy, the need for reliable and reproducible criteria to assess BM samples for potential low-level BPDCN involvement has gained increased attention. An assay that can reliably distinguish neoplastic PDC from background reactive PDC becomes important. Variable numbers of reactive PDC are detected routinely in the BM by flow cytometry immunophenotyping and/or immunohistochemistry. Similar to their neoplastic counterparts, reactive PDC are positive for CD4, CD123, CD303, HLADR and TCF4, and they lack expression of lineage-specific antigens. CD56, a marker frequently expressed in BPDCN, is the only marker being used to date to distinguish neoplastic from reactive PDC. However, CD56 expression can be found in a small subset of reactive PDC.10-12 Thus, distinguishing CD56+ BPDCN from CD56+ reactive PDC becomes quite challenging in the assessment of post treatment BM specimens, which often contain reactive PDC.
In this study, our aim was to characterize the immunophenotype of BPDCN, with particular focus on the differences between BPDCN and normal/reactive PDC. From understanding these differences, we developed and validated a ten-color clinical-grade flow cytometry immunophenotyping panel and compared its performance to that of orthogonal tools for residual disease evaluation.
Methods
Study group
We identified all patients with BPDCN diagnosed at The University of Texas MD Anderson Cancer Center between 2010 and 2019. All patients fulfilled the diagnostic criteria for BPDCN as defined in the World Health Classification. Patients for whom flow cytometry immunophenotyping had been performed on BM specimens were included in this study. A control group of patients who had BM evaluation by flow cytometry immunophenotyping were also included to study reactive PDC; this group included patients who underwent BM staging for lymphoma or had hematologic diseases other than BPDCN and were in complete remission with or without stem cell transplantation. This study was approved by the University of Texas MD Anderson Cancer Center Institutional Review Board and was conducted in accordance with the Declaration of Helsinki.
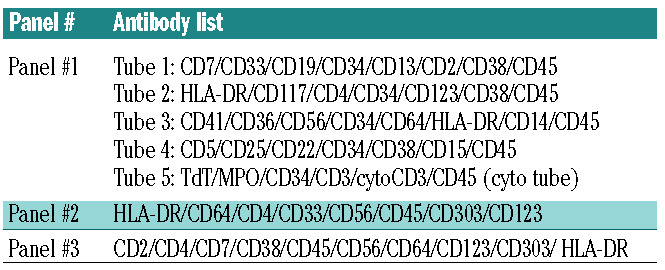
Table 1.
The list of antibodies used in our flow cytometric panels.
Flow cytometric immunophenotypic analysis
BM aspirate specimens were collected in EDTA anticoagulant tubes, and processed within 12 h of collection using a standard lyse/wash technique (PharmLyse™, BD Biosciences, San Diego, CA, USA). For each analysis a minimum of 200,000 events was acquired on FACSCanto II instruments (8-color and 10-color, BD Biosciences).
At the time of initial diagnosis, a comprehensive panel designed for the workup of acute leukemia was performed routinely (panel #1 in Table 1). This panel included lineage-defining markers for B, T, myeloid, and monocytic cells, as well as markers (CD4, CD123, HLA-DR, CD56) necessary for initial screening of BPDCN. When a diagnosis of BPDCN was suspected from panel #1 analysis, an additional panel (panel #2 in Table 1) was used for further characterization and confirmation.
Based on the findings of the current study, a one-tube, ten-color assay (panel #3 in Table 1) was subsequently constructed and validated for distinguishing BPDCN cells from reactive PDC.
Immunohistochemistry
Immunohistochemical studies were performed using formalinfixed, paraffin-embedded BM core biopsy or aspirate clot specimens. 13 TCF4/CD123 double staining was performed using a previously described protocol.9
Results
Immunophenotype of blastic plasmacytoid dendritic cell neoplasm
A total of 39 patients with a diagnosis of BPDCN were studied, including 30 men and 9 women with a median age of 69 years (range, 3-87 years). Flow cytometry immunophenotyping was performed using panel #1 (Table 1) and the more recent cases were also tested using panel #2 (Table 1). The median number of BPDCN cells detected by the flow cytometry was 18% (range, 0.1-91%). The immunophenotype of BPDCN in these 39 cases is summarized in Figure 1 and Online Supplementary Table S1.
BPDCN cells were positive for CD45, falling into the “blast” gate on CD45/SSC in all cases (39/39, 100%). CD45 expression was often present at a similar level as, or slightly higher than, that of granulocytes (Figure 2A) with the exception of three cases (8%) which showed significantly lower CD45 expression (dimmer than granulocytes) (Figure 2B). HLA-DR as well as CD123 expression was uniformly positive in all cases. Cells were positive for CD4 in all 38 cases assessed, uniform in 34 (89%) and partially in four (11%) cases. BPDCN cells were positive for CD56 in 97% (36/37) of cases, with mostly (92%, 33/36) uniform and occasionally partial (3/36, 8%) expression. The only case in which CD56 was not expressed was a 3year old girl who otherwise had a typical immunophenotype of BPDCN. CD303, a marker which showed a high diagnostic value for BPDCN in some previous studies,14,15 was expressed in 44% (7/16) of cases. Additionally, cells were positive for CD7 in 64% (21/33) of cases, with uniform expression in 11 and partial expression in ten cases. CD38 was variably expressed in 88% (30/34) of cases. Cells were positive for CD2 in 5/27 (19%) cases and all positive cases showed bright expression. CD33 was expressed in 48% (16/33) of cases. CD36 was expressed in 57% (17/30) of cases, with the expression being uniform in seven (41%) and partial in ten (59%) cases. CD117 was partially expressed in three of 34 (9%) cases. CD5 expression was uncommon, only being observed in one of 30 (3%) cases. Partial CD14 without CD64 expression was detected in one (3%, 1/34) case and TdT expression was detected in 25% (4/16) of cases. All cases were negative for CD3 (surface and cytoplasmic), CD13, CD15, CD19, CD22, CD25, CD34, CD41, CD64 and myeloperoxidase.
Figure 1.

The immunophenotype of blastic plasmacytoid dendritic cell neoplasm. The figure summarizes the immunophenotype of blastic plasmacytoid dendritic cell neoplasms in 39 patients. Different colors represent different levels of expression.
Figure 2.

The location of blastic plasmacytoid dendritic cell neoplasm cells on CD45/SSC plots. (A): Most (92%) cases of blastic plasmacytoid dendritic cell neoplasm (BPDCN) show CD45 expression at a level similar to or slightly higher than that detected in granulocytes. (B) A small subset (8%) of cases shows lower CD45 expression. The red population represents BPDCN cells.
Immunophenotype of normal/reactive plasmacytoid dendritic cells
The immunophenotype of normal/reactive PDC was studied in BM samples from 22 patients without BPDCN, including 11 samples that were submitted for lymphoma staging, four cases of B-lymphoblastic leukemia in remission and seven post-transplant samples from patients with B-lymphoblastic leukemia or acute myeloid leukemia. In these cases, normal/reactive PDC represented 0.11% (median) of total nucleated cells (range, 0.01% to 0.43%) as determined by flow cytometry.
Similar to BPDCN cells, normal/reactive PDC were consistently positive for CD123 and HLA-DR and negative for CD64. They were all positive for CD4, CD45, and CD303. Likewise, they were all positive for CD38, which was brightly expressed in all cases, and CD33, which was expressed uniformly in 12 of 21 (57%) cases and partially in the remaining (43%, 9/21). Of note, although positive, CD33 expression in normal/reactive PDC was lower than that of monocytes and basophils (Figure 3D). CD2 expression by normal/reactive PDC showed a bimodal pattern with a spectrum from completely negative cells to positive cells in all cases (Figure 4A). CD7 expression was consistently positive in a small subset of normal/reactive PDC with a median of 13% (range, 0.3% to 21%). Of note, these CD7+ PDC were negative for CD56 (Figure 4A).
The immunophenotype of CD56+ normal/reactive plasmacytoid dendritic cells
CD56 expression was observed in a subset of normal/reactive PDC in all 22 non-BPDCN cases described above, with a median of 4.5% (range, 1.3% to 20%) of total PDC. This CD56+ subset of PDC showed substantial immunophenotypic overlap with BPDCN in PDC-defining markers, including being positive for CD4, CD123, HLADR, and CD303; and the panel (panel #2, Table 1) initially designed for BPDCN was incapable of distinguishing these cells from BPDCN.
This population of CD56+ PDC was further studied with an expanded panel of markers, and demonstrated a remarkably consistent pattern. They were positive for CD2 (100%), negative for CD7 (100%), and showed bright CD38 (100%) expression in all 22 cases tested (Table 2). CD303 expression was also positive in all cases (100%), uniform in 13 (59%) and partial in nine (41%). A representative case of CD56+ reactive PDC is shown in Figure 4A.
Figure 3.

Differential immunophenotypic characteristics of blastic plasmacytoid dendritic cell neoplasm and reactive plasmacytoid dendritic cells. Blastic plasmacytoid dendritic cell neoplasm (BPDCN) cells often show increased HLA-DR, decreased CD123, decreased CD303, decreased CD38, and positive CD56 expression. Pink: basophils; blue: reactive plasmacytoid dendritic cells (PDC); red, neoplastic PDC; and gray: monocytes. (A) Both basophils and PDC are bright for CD123. Basophils are negative whereas PDC are positive for HLA-DR. In comparison to reactive PDC (blue), neoplastic PDC (red) often show decreased CD123 and increased HLA-DR expression. Monocytes (gray) are also positive for CD123 and HLADR, but their CD123 level is much lower than that of PDC. (B) Neoplastic PDC are positive for CD56 and negative for CD303. CD303 is positive in reactive PDC. (C) Neoplastic PDC often show decreased CD38 expression when compared to reactive PDC. (D) Reactive PDC are positive for CD33, and approximately half of BPDCN cases are negative for CD33.
Of note, the expression of CD56 in normal/reactive PDC is not limited to BM samples. We analyzed a reactive PDC proliferation using immunohistochemistry in a patient who had a self-limited skin lesion, likely an insect bite, which had CD56 expression and had presented a diagnostic challenge at initial encounter (Figure 5).
Differential immunophenotypic characteristics of blastic plasmacytoid dendritic cell neoplasm and reactive plasmacytoid dendritic cells
The immunophenotype of BPDCN was compared to that of reactive PDC. In addition to being “positive” and “negative”, the markers of expression were also scored as “increased” or “decreased/partial” if the intensity difference was greater than one-third on a log scale (Figure 1). This comparison was facilitated by the presence of reactive PDC in some cases of BPDCN at initial diagnosis and in many cases of BPDCN following therapy. Compared with reactive PDC, BPDCN cells showed brighter HLA-DR expression in 25 of 36 (69%) cases (Figure 3A), and lower CD123 expression in 28 of 36 (78%) cases (Figure 3A). In the latter cases, although decreased, CD123 levels in BPDCN were still higher than those of monocytes (Figure 3A). CD303, a marker that is consistently positive in normal/ reactive PDC, was only positive in seven of 16 (44%) BPDCN cases, of which six showed decreased expression and only one (6% in total) had a normal level of CD303 (Figure 3B). In contrast to bright CD38 expression in reactive PDC, CD38 expression was frequently downregulated in BPDCN cells, being decreased in 24 of 34 (70%) and negative in four of 34 (12%) (Figures 1 and 3C). While CD33 expression was positive in all cases of reactive PDC, it was only positive in 48% (16/33) of BPDCN cases.
We next focused on the difference between BPDCN and reactive CD56+ PDC. Unlike CD56+ reactive PDC that were uniformly positive for CD2, bright for CD38 and consistently negative for CD7, BPDCN cells were frequently negative for CD2 (81%), positive for CD7 (64%) and with decreased or negative (82%) expression of CD38 (Figure 4B) (Table 2). In contrast to the 100% positivity of reactive PDC for CD303, only 44% of BPDCN cases were positive. Using a combination of markers (CD2, CD7, CD56, CD303, CD38), none of the 39 BPDCN cases showed an immunophenotype exactly the same as that of CD56+ reactive PDC, which were CD56+/CD2+/CD7- /CD303+/CD38+bright.
Establishment and validation of a flow cytometry assay for minimal residual disease
Based on these findings, a one-tube, ten-color assay C D 2 / C D 7 / C D 3 8 / C D 3 0 3 / C D 1 2 3 / H L A - DR/CD64/CD4/CD45/CD56 was constructed (panel #3, Table 1). Detailed information, including the antibody clones and the fluorochrome attached to each antibody, is listed in Online Supplementary Table S2. CD123, HLA-DR, CD45, and CD64 were included to identify PDC that were CD123bright/HLA-DR+/CD64-/CD45dim+. In patients who received targeted therapy to CD123, an alternative gating strategy was also used to examine PDC that were CD4+CD64-CD56+HLA-DR+CD45dim+. Representative cases to illustrate our gating strategy are shown in Online Supplementary Figures S1 and S2. The sensitivity of this panel was validated to be 0.01% according to the MRD testing guideline from the College of American Pathologists (Online Supplementary Figure S3).
Figure 4.

Representative cases of reactive and neoplastic CD56+ plasmacytoid dendritic cells. Gray: CD56– reactive plasmacytoid dendritic cells (PDC); blue: CD56+ reactive PDC; red: CD56+ neoplastic PDC. (A) CD56+ reactive PDC are consistently positive for CD2 and CD303, negative for CD7. CD38 expression is bright. (B) In contrast, neoplastic CD56+ neoplastic PDC are often negative for CD2 with decreased to negative CD303 expression. CD7 expression is often positive and CD38 expression level is often decreased. Focusing on CD56– PDC (gray) in both panels (A) and (B), these cells are positive for CD303 and CD38. CD2 shows a bimodal pattern of expression (both negative and positive cells present). A small subset of reactive PDC is CD7+ and these CD7+ reactive PDC are negative for CD56.
Table 2.
The major immunophenotypic differences between CD56-positive reactive plasmacytoid dendritic cells and blastic plasmacytoid dendritic cell neoplasm.

The ten-color MRD panel was tested prospectively in 19 BM samples from seven patients who had a confirmed diagnosis of BPDCN. These 19 samples included one for initial BM diagnosis and 18 samples for evaluation of residual disease during the course of treatment. Using this flow cytometry panel, 12 (63%) samples were positive for BPDCN and the median number of aberrant cells was 0.05% of total nucleated cells (range, 0.008% to 56.5%). Of the 12 positive samples, one was detected as early relapse after stem cell transplant, with 0.01% of aberrant PDC. Of note, all samples had mixed reactive PDC in the background, serving as an internal comparison. All positive cases showed a similar immunophenotype to that identified in the original diagnostic specimen and no significant immunophenotypic shift was observed. For patients who received anti-CD123 targeted therapy, CD123 expression was still maintained in BPDCN as well as normal PDC.
Flow cytometry versus immunohistochemistry in the assessment of minimal residual disease
We compared flow cytometry immunophenotyping and dual-color immunohistochemistry for TCF4/CD123 to determine the relative performance of these assays in BM evaluation in the context of BPDCN after therapy. To achieve this, we first systematically assessed the number, distribution, and morphological characteristics of TCF4/CD123 dual-positive cells in 18 BM samples from patients without BPDCN. In such cases, PDC were few and often scattered, with a broad range of morphological characteristics that ranged from mature plasmacytoid forms to others with increased nucleus-to-cytoplasm ratio and occasional nuclear membrane convolutions. Although occasional loose PDC aggregates were identified, none of the cases had tight PDC aggregates or sheets of PDC. Next, we performed TCF4/CD123 double-stain immunohistochemistry in 14 cases with a history of BPDCN who had been evaluated for residual disease by flow cytometry immunophenotyping. In these cases, TCF4/CD123 highlighted scattered PDC but could not reliably distinguish reactive from neoplastic PDC. As shown in Figure 5, the TCF4/CD123 immunostain highlighted scattered PDC in a case of BPDCN prior to (Figure 6A) and after stem cell transplant in remission (Figure 6B), in both cases accounting for around 1-2% of the total cells in the BM. It is uncertain from the TCF4/CD123 immunostain whether these are aberrant or not. Flow cytometry, on the other hand, was capable of differentiating them: it detected neoplastic PDC mixed with normal PDC in the pre-transplant specimen (Figure 6C), whereas only reactive PDC but no aberrant PDC were detected in the post-transplant specimen (Figure 6D).
Figure 5.

A case of reactive plasmacytoid dendritic cell proliferation positive for CD56 by immunohistochemistry. (A) A skin biopsy shows small clusters of plasmacytoid dendritic cells (PDC), some with plasmacytoid morphology in a self-limited skin lesion, likely caused by an insect bite. The insert shows the low-power view of the skin biopsy. (B) Double staining for CD123/TCF4 highlights scattered and loosely clustered PDC. (C) CD56 immunostaining shows that many PDC are positive.
Figure 6.

Immunostain and flow cytometric analysis of a case of blastic plasmacytoid dendritic cell neoplasm before and after transplantation. (A, B) Immunostain using a dual-color TCF4/CD123 double stain showed scattered plasmacytoid dendritic cells (PDC) in both samples, before (A) and after (B) transplantation. (C, D) Flow cytometric analysis showed that a subset of PDC (red) in the pre-transplant sample (C) was aberrant (decreased CD38, negative CD2, decreased CD303 expression) whereas all PDC in the post-transplant sample (D) showed a normal immunophenotype. CD56+ reactive PDC are highlighted blue in (C) and (D).
Discussion
In this study, we investigated the immunophenotype of BPDCN in a large cohort of 39 patients and compared it to that of reactive PDC. This study is the first to go beyond a simple characterization of the BPDCN immunophenotype, but to understand the immunophenotypic aberrancy/alterations of BPDCN. Of particular interest, we show that CD56 is expressed in a small subset of normal/reactive PDC and therefore, CD56 alone is insufficient to differentiate BPDCN from reactive PDC, especially when the tumor burden is low. Through further characterization of these CD56+ normal PDC, we identified a combination of markers that can detect BPDCN and distinguish neoplastic from non-neoplastic PDC in BM with a sensitivity of 0.01%.
The diagnosis of BPDCN at the time of initial presentation, typically with a high tumor burden, is often straightforward as BPDCN cells show a distinct immunophenotype, being positive for HLA-DR, CD123 (bright), CD4, CD56, and absence of myeloperoxidase and monocytic markers as well as B- and T-cell lineage-defining markers. The neoplastic infiltrate can be further confirmed by immunohistochemical studies using CD123, TCL1 or a more specific TCF4/CD123 double stain. Basophils often have a similar level of CD123 expression but they are negative for HLA-DR. Monocytes, some hematopoietic precursors and acute myeloid leukemia blasts are positive for both CD123 and HLA-DR,16 but their level of CD123 expression is substantially lower than that of PDC.
More challenging is the evaluation of MRD status after treatment or staging assessment of BM specimens with a low tumor burden. This challenge is attributable to the immunophenotypic overlap between BPDCN cells and reactive PDC, especially, the CD56+ subset of reactive PDC. In fact, an initial panel designed for BPDCN MRD detection (panel #2, Table 1) failed to distinguish BPDCN from normal PDC. An immunohistochemical study with TCF4/CD123 was able to highlight PDC, but was incapable of differentiating BPDCN from reactive PDC. These problems prompted us to study the immunophenotype of reactive PDC, and explore the immunophenotypic difference between neoplastic and reactive PDC.
Although both reactive PDC and BPDCN cells were uniformly positive for CD123 and HLA-DR, BPDCN cells tended to have brighter HLA-DR and lower CD123 expression. While all reactive PDC were positive for CD33, 52% of BPDCN cases did not express this marker. All reactive PDC were positive for CD2 with a bimodal pattern, whereas only 19% of BPDCN cases were positive for CD2. With regards to other lymphoid antigens, CD7 expression in BPDCN was very frequent (64%), whereas CD5 was only observed in less than 5% of cases. CD303, a marker considered specific for PDC, was reported to be expressed in 90%,14 63%17 and 53%18 of BPDCN cases as determined by immunohistochemistry. According to flow cytometry analysis, CD303 was expressed in 75%15 and 64%19 of cases. Of note, various anti-CD303 antibodies have been used in previous studies, including clone DDX0043 (Dendritics, Dardilly, France),14,17 rabbit anticytoplasmic CD303,18 and AC144.15 In our study, using clone 201A from Biolegend, all reactive PDC were positive for CD303, whereas only 44% of BPDCN cases were positive. Of the CD303+ BPDCN cases, many showed a decreased level of expression compared to that of the internal control-normal PDC. Recently, Huang and colleagues reported decreased or absent CD303 expression in early stages of plasmacytotoid maturation in their series of myeloid neoplasms with PDC differentiation.20 The lower CD303 intensity in BPDCN might reflect the immaturity of tumor cells as they derived from less mature/precursors of PDC. Nonetheless, this altered level of expression of CD303 in BPDCN facilitates the identification of neoplastic cells in a background of normal PDC, and contributes to MRD detection.
We further confirmed that CD56 was normally expressed in a subset of normal PDC, ranging from 1.3% to 20% of total PDC. A similar observation was previously made in peripheral blood and BM samples from healthy people.10-12 These CD56+ PDC have been proposed to be precursors as well as the cell of origin of BPDCN. We show here that the CD56+ subset of normal PDC are positive for CD2 and CD303, negative for CD7,10-12 and retained a high level of CD38. This immunophenotypic pattern is distinctively different from that of CD56+ BPDCN cells, which are often CD2– (81%), CD7+ (64%), CD303– (56%), and show decreased or negative CD38 expression (82%). Based on the immunophenotypic differences, we designed a new flow cytometric panel composed of these markers. This panel was capable of detecting BPDCN cells to a level of 0.01% and, prospectively tested in 19 BM samples from seven patients, was able to reliably distinguish BPDCN cells from reactive PDC in all samples. Of note, every BM sample contained reactive PDC, which served as internal controls for comparison. Other markers that could be explored in the future to distinguish BPDCN cells from normal PDC include CD5, CD13, CD22, and CD33. BCL2 is also potentially valuable as it is expressed in BPDCN but often negative in reactive PDC.5
In this study, the flow cytometry assay for MRD detection was not compared to mutational analysis for a number of reasons. First, not every case of BPDCN had detectable mutations using our current next-generation sequencing analysis covering 81 frequently mutated genes in myeloid/lymphoid neoplasms. Second, the mutations frequently found in BPDCN, such as TET2, ASXL1, TP53 and NRAS, are also commonly found in myeloid neoplasms. It is well known that myeloid neoplasms such as myelodysplastic syndrome and chronic myelomonocytic leukemia frequently co-occur with BPDCN.8,21 Thus the detection of these mutations by next-generation sequencing cannot differentiate a BPDCN clone and a myeloid clone in such cases. Last, the sensitivity of next-generation sequencing is about 1%, which is unable to reach the 0.01% level of sensitivity of flow cytometry.
In summary, we have provided the immunophenotypic characteristics of BPDCN in detail in this study. We have also defined “immunophenotypic aberrancies” of BPDCN in comparison with normal/reactive PDC. It is imperative to recognize that reactive PDC usually include a small subset of CD56+ cells, which should not be misinterpreted as BPDCN. These CD56+ PDC have an immunophenotypic profile distinctively different from that of BPDCN, which allowed us to develop a flow cytometric assay that has a high sensitivity and specificity for the detection of MRD. Such laboratory tests are much in need in the era of targeted therapy and precision medicine. This flow cytometry panel is valuable for disease monitoring during treatment and also enables early detection of relapse in BPDCN patients who have undergone allogeneic stem cell transplant, allowing for early intervention. The significance of positive MRD prior to and following stem cell transplantation is of great interest in BPDCN, and deserves future studies.
Supplementary Material
References
- 1.Khoury JD. Blastic plasmacytoid dendritic cell neoplasm. Curr Hematol Malig Rep. 2018;13(6):477-483. [DOI] [PubMed] [Google Scholar]
- 2.Beird HC, Khan M, Wang F, et al. Features of non-activation dendritic state and immune deficiency in blastic plasmacytoid dendritic cell neoplasm (BPDCN). Blood Cancer J. 2019;9(12):99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Facchetti F, Petrella T, Pileri S. Blastic plasmacytoid dendritic cell neoplasm. In: Swerdlow S, Campo E, Harris N., et al., eds. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. Revised 4th edition. Lyon, 2017:174-177. [Google Scholar]
- 4.Venugopal S, Zhou S, El Jamal SM, Lane AA, Mascarenhas J. Blastic plasmacytoid dendritic cell neoplasm-current insights. Clin Lymphoma Myeloma Leuk. 2019;19(9):545-554. [DOI] [PubMed] [Google Scholar]
- 5.Sapienza MR, Pileri A, Derenzini E, et al. Blastic plasmacytoid dendritic cell neoplasm: state of the art and prospects. Cancers (Basel). 2019;11(5). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Garnache-Ottou F, Vidal C, Biichle S, et al. How should we diagnose and treat blastic plasmacytoid dendritic cell neoplasm patients? Blood Adv. 2019;3(24):4238-4251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lyapichev KA, Sukswai N, Konoplev S, Khoury JD. Blastic plasmacytoid dendritic cell neoplasm with unusual lymphoid features and macrovacuoles. Ann Hematol. 2019;98(9):2221-2222. [DOI] [PubMed] [Google Scholar]
- 8.Alayed K, Patel KP, Konoplev S, et al. TET2 mutations, myelodysplastic features, and a distinct immunoprofile characterize blastic plasmacytoid dendritic cell neoplasm in the bone marrow. Am J Hematol. 2013;88(12): 1055-1061. [DOI] [PubMed] [Google Scholar]
- 9.Sukswai N Aung PP Yin CC,et al. Dual expression of TCF4 and CD123 is highly sensitive and specific for blastic plasmacytoid dendritic cell neoplasm. Am J Surg Pathol. 2019;43(10):1429-1437. [DOI] [PubMed] [Google Scholar]
- 10.Comeau MR, Van der Vuurst de Vries AR, Maliszewski CR, Galibert L. CD123bright plasmacytoid predendritic cells: progenitors undergoing cell fate conversion? J Immunol. 2002;169(1):75-83. [DOI] [PubMed] [Google Scholar]
- 11.Osaki Y, Yokohama A, Saito A, et al. Characterization of CD56+ dendritic-like cells: a normal counterpart of blastic plasmacytoid dendritic cell neoplasm? PLoS One. 2013;8(11):e81722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Petrella T, Comeau MR, Maynadie M, et al. 'Agranular CD4+ CD56+ hematodermic neoplasm' (blastic NK-cell lymphoma) originates from a population of CD56+ precursor cells related to plasmacytoid monocytes. Am J Surg Pathol. 2002;26(7):852-662. [DOI] [PubMed] [Google Scholar]
- 13.Khoury JD, Wang WL, Prieto VG, et al. Validation of Immunohistochemical assays for integral biomarkers in the NCI-MATCH EAY131 clinical trial. Clin Cancer Res. 2018;24(3):521-531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Boiocchi L, Lonardi S, Vermi W, Fisogni S, Facchetti F. BDCA-2 (CD303): a highly specific marker for normal and neoplastic plasmacytoid dendritic cells. Blood. 2013;122(2):296-297. [DOI] [PubMed] [Google Scholar]
- 15.Garnache-Ottou F, Feuillard J, Ferrand C, et al. Extended diagnostic criteria for plasmacytoid dendritic cell leukaemia. Br J Haematol. 2009;145(5):624-636. [DOI] [PubMed] [Google Scholar]
- 16.Arcangeli S, Rotiroti MC, Bardelli M, et al. Balance of Anti-CD123 chimeric antigen receptor binding affinity and density for the targeting of acute myeloid leukemia. Mol Ther. 2017;25(8):1933-1945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Julia F, Dalle S, Duru G, et al. Blastic plasmacytoid dendritic cell neoplasms: clinicoimmunohistochemical correlations in a series of 91 patients. Am J Surg Pathol. 2014;38(5):673-680. [DOI] [PubMed] [Google Scholar]
- 18.Jaye DL, Geigerman CM, Herling M, Eastburn K, Waller EK, Jones D. Expression of the plasmacytoid dendritic cell marker BDCA-2 supports a spectrum of maturation among CD4+ CD56+ hematodermic neoplasms. Mod Pathol. 2006;19(12):1555-1562. [DOI] [PubMed] [Google Scholar]
- 19.Tsagarakis NJ, Kentrou NA, Papadimitriou KA, et al. Acute lymphoplasmacytoid dendritic cell (DC2) leukemia: results from the Hellenic Dendritic Cell Leukemia Study Group. Leuk Res. 2010;34(4):438-446. [DOI] [PubMed] [Google Scholar]
- 20.Huang Y, Wang Y, Chang Y, et al. Myeloid neoplasms with elevated plasmacytoid dendritic cell differentiation reflect the maturation process of dendritic cells. Cytometry A. 2020;97(1):61-69. [DOI] [PubMed] [Google Scholar]
- 21.Brunetti L, Di Battista V, Venanzi A, et al. Blastic plasmacytoid dendritic cell neoplasm and chronic myelomonocytic leukemia: a shared clonal origin. Leukemia. 2017;31(5):1238-1240. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.